Chapter 26 Infections of the gastrointestinal tract
Normal flora
In healthy, fasting individuals, the stomach is either sterile or may contain only a few organisms, because of its low pH and enzymes. The diet has a major effect on the gut flora. The small intestine may be colonized with streptococci, lactobacilli and yeasts (especially Candida albicans); the proportions of these and other organisms vary, depending on dietary habits. In the ileum, a typical Gram-negative flora (e.g. Bacteroides spp. and Enterobacteriaceae) is seen, and the large intestine has a dense population of varied flora. These include members of the Enterobacteriaceae, Enterococcus faecalis, Bacteroides spp., Clostridium spp., bifidobacteria and anaerobic streptococci. The anaerobes outweigh the aerobes by far and comprise the vast majority of the bacteria in the large intestine. Roughly 20% of the faeces contains bacteria, approximately 1011 organisms per gram. As in the oral cavity, the gastrointestinal tract harbours a vast multitude of unculturable, and yet to be discovered organisms.
Important pathogens
Gastrointestinal infections are a major cause of morbidity and mortality worldwide. For example, recent studies have revealed that, globally, severe diarrhoea and dehydration are responsible each year for the death of 1 575 000 children under the age of 5. Most of these diseases are preventable and are caused by poor food, and personal hygiene, poor sanitation and lack of quality pipeborne water systems.
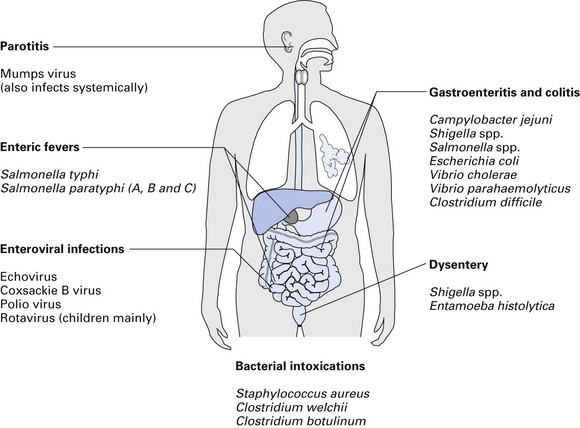
A diverse array of infections of the gastrointestinal tract is caused by an equally varied population of microbial agents (Fig. 26.1). The agents of diarrhoeal diseases, including those that are considered common agents of food poisoning, are listed in Table 26.1. The common bacterial diarrhoeal diseases in the developed world include those caused by:
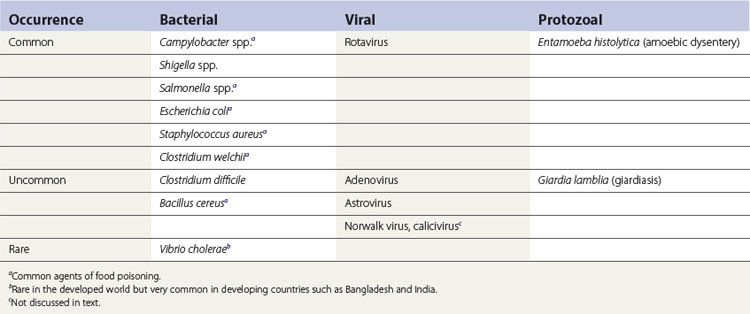
Cholera caused by Vibrio cholerae is noteworthy as a common diarrhoeal disease in the developing world, together with the foregoing.
Less common diseases include infections caused by Clostridium difficile and Bacillus cereus.
Common diarrhoeal diseases
Campylobacter
Campylobacter coli and Campylobacter jejuni are among the most common diarrhoea-inducing agents in the western world. They are curved, slender, Gram-negative bacilli present in the gut as well as in the oral cavity.
Pathogenesis and epidemiology
Symptoms vary from mild to severe, with any part of the small or large intestine affected. Dogs and cats are probable sources of infection, but mass-produced poultry is the most common source. Eating contaminated food is a common cause of infection; note that campylobacters do not multiply in food. Patients may become symptomless carriers after recovery.
Shigella
Shigella causes bacillary dysentery, as opposed to amoebic dysentery caused by intestinal amoebae. It is an important cause of morbidity and death in young children, particularly in the developing world.
Aetiology
The genus Shigella contains four species: Shigella dysenteriae, Shigella flexneri, Shigella boydii and Shigella sonnei.
Pathogenesis and epidemiology
Infection is by ingestion of organisms. Once ingested, the bacteria attach to the mucosal villus epithelium, enter and multiply in these cells. The resultant death of the infected cells initiates an inflammatory reaction in the submucosa and lamina propria. Finally, necrosis and ulceration of the villus epithelium ensue, making the stools bloody and mucous. This type of severe reaction is usually due to Shigella dysenteriae, which is known to produce a potent enterotoxin and a cytotoxin. This infection may be life-threatening.
Dysentery due to other shigellae is generally milder and varies from asymptomatic excretion to a severe attack of diarrhoea with abdominal pain. Shigella sonnei is the usual agent of dysentery in the UK, while Shigella boydii is common in the Middle East and South-East Asia.
Spread of the disease is from hand to mouth. It usually occurs in nursery schools where the index case (i.e. the person with the disease) contaminates hands at the toilet, and further contaminates lavatory handles and hand towels if personal hygiene is deficient. Subsequent handling of these bacteria-laden fomites (inanimate surfaces acting as vehicles of disease transfer) by healthy individuals results in hand-to-mouth transmission of the agents, leading to the disease. Thus, ‘food, flies and fomites’ are classical means of spread.
Diagnosis
The diagnosis is made by examination of stool sample and culture on MacConkey’s agar and selective media such as desoxycholate-citrate agar (DCA). Pale, non-lactose-fermenting (NLF) colonies are then isolated and identified by biochemical tests; serological identification is performed subsequently.
Salmonella
A large number of different Salmonella species exist, together with an even more bewildering number (about 1500) of serotypes. Of these, about 14 are important pathogens. The common diarrhoea-causing organism is Salmonella typhimurium. The other major pathogens of this group are Salmonella typhi and Salmonella paratyphi-A, -B and -C, which cause enteric fever, a septicaemic illness in which diarrhoea is a late feature of the disease.
Pathogenesis and epidemiology
The genesis of salmonella food poisoning is ill understood. Patients have mild gastrointestinal disturbances with an incubation period of about 1–2 days. Abdominal pain, diarrhoea (with or without fever) and vomiting are commonly present. Septicaemia is rare.
The organism is found in domestic animals and poultry and is spread via the faecal–oral route. On entering the gastrointestinal tract, the salmonellae may either produce an enterotoxin (similar to toxigenic E. coli) or invade the mucosa of small intestine (like shigellae).
Diagnosis
Examination of stool sample and culture on MacConkey (indicator) medium and selective media such as DCA or Wilson–Blair medium; pale, NLF colonies on MacConkey medium and black, shiny colonies on Wilson–Blair medium. Subsequent identification is by biochemical tests and determination of serological status. The major antigens that are useful for the serotyping of salmonellae are the ‘O’ (somatic or body antigen) and the ‘H’ (flagellar) antigens.
Treatment
Treatment is rarely necessary. Antibiotics are contraindicated except in septicaemic cases; antibiotic therapy prolongs the carriage of the organism in the convalescent phase.
Prevention
Prevention includes control of animal food quality, good farming and abattoir practices, rigorous kitchen hygiene and good personal hygiene among food handlers, and exclusion of known human carriers (‘excretors’) from food handling. However, the best form of prevention is thorough cooking of food and avoidance of consumption of raw or partly cooked eggs and other animal-derived food.
Escherichia coli
E. coli is a normal commensal of the gastrointestinal tract, but certain strains, for some unknown reason, can behave as pathogens. As described in Chapter 15, they produce enterotoxins, and the enteroinvasive strains have the ability to invade the gut mucosa.
Pathogenesis and epidemiology
There are two types of E. coli diarrhoea:
Infantile gastroenteritis
Accompanied by acute and profuse diarrhoea, this infection has an incubation period of 1–3 days. The disease is mainly caused by enteropathogenic E. coli (EPEC), but in a minority of cases, enterotoxigenic E. coli (ETEC) strains contribute (Chapter 15). It is common in the developing world because of poor sanitation and poverty; infection spreads directly from case to case and via fomites (see above for shigellae), and in some cases, the mother may be the source of infection.
Diagnosis
Treatment
In infantile diarrhoea, treatment is by rehydration and correction of fluid loss and electrolyte balance. No antibiotics are necessary for either of the E. coli diarrhoeas. Traveller’s diarrhoea is self-limiting.
Prevention
Haemorrhagic syndromes
Though not diarrhoeogenic, two important haemorrhagic syndromes caused by E. coli are noteworthy here. Haemorrhagic colitis is seen in children and adults, while haemolytic uraemic syndrome is mainly seen in children – both produce outbreaks and sporadic infections; death may be the outcome in either. The agent is E. coli (mainly of the serotype O157) that produces cytotoxins VT1 and VT2 (demonstrated in the laboratory by their cytopathic effect on cultured monkey kidney cells called Vero cells); due to their verotoxigenicity, these E. coli strains are known as VTEC (Chapter 15). These toxins are also called Shiga-like toxins. The main source of infection is beef.
Staphylococcus aureus
Staphylococcus aureus is a common cause of diarrhoea due to food poisoning. Symptoms ensue very quickly after the food intake, as the Staphylococcus aureus enterotoxin is preformed in food.
Pathogenesis and epidemiology
The Staphylococcus aureus enterotoxin has a local action on the gut mucosa, with resultant nausea and vomiting (and occasional diarrhoea) within a few hours after the food intake. Cooked food, which is not stored at 4°C or frozen immediately but left at room temperature, is the usual source of infection. The organism reaches the food from a staphylococcal lesion on the skin of a food handler and, if left at ambient or warm temperatures, may multiply in food and liberate the enterotoxin. The toxin is relatively heat-resistant; on heating contaminated food, the Staphylococcus aureus cells usually die, leaving the active toxin in the food, which is ingested. Milk or milk products such as cream or custard may also act as sources of toxin.
Clostridium welchii
Clostridium welchii, responsible for gas gangrene (see Chapter 13), also causes food poisoning.
Pathogenesis and epidemiology
Heat-resistant spores of C. welchii survive in contaminated food during the heating procedure, and subsequently multiply in deep, relatively anaerobic parts of the food (e.g. in meat pies). After the food is ingested, sporulation (spore formation) occurs in the gastrointestinal tract, and an enterotoxin is produced, which alters the membrane permeability of the small intestine, causing diarrhoea.
Cholera
Though rare in the West, cholera is a relatively common disease in some parts of the world, especially in South-East Asia (e.g. Bangladesh). It is mainly caused by V. cholerae O1.
Pathogenesis and epidemiology
V. cholerae infects only humans and is transmitted via the faecal–oral route. Contaminated food and water are the main reservoirs of infection. Human carriers are frequently asymptomatic and may be incubating or convalescing from the disease. Once ingested, the organism colonizes the small intestine and secretes a protein exotoxin (an enterotoxin).
A large number of cholera vibrios (about 1 billion) need to be ingested for them to survive the acids of the stomach. They then adhere to the brush border of the intestine (by secreting a mucinase that dissolves the protective glycoprotein of the intestinal cells), multiply and secrete the enterotoxin (choleragen). The toxin stimulates the activity of the enzyme, adenyl cyclase, of the intestinal cells and increases the flow of water and electrolytes into the bowel lumen, leading to a massive, watery diarrhoea without inflammatory cells. Morbidity and death are due to dehydration and electrolyte imbalance. If fluid balance is adjusted promptly, the diarrhoea is self-limiting in about 7 days.
Clinical features
The hallmark of cholera is non-bloody, frothy and colourless diarrhoea: ‘rice-water stools’. The incubation period varies from 6 h to 5 days. There is no abdominal pain, and symptoms are mainly due to dehydration, which also brings about cardiac and renal failure. The mortality rate is about 40% without treatment.
Diagnosis
Diagnosis is by culture of faeces on selective media, e.g. thiosulphate-citrate-bile salts (TCBS) agar.
Less common and uncommon diarrhoeal diseases
Clostridium difficile
The agent of antibiotic-associated pseudomembranous colitis, a mild and self-limiting disease. Rarely, life-threatening fulminant infection may set in.
Pathogenesis and epidemiology
The organism is a normal commensal of the gut in some 3% of the population. Antibiotics (especially clindamycin, cephalosporins and, less frequently, ampicillin) suppress drug-sensitive normal flora, allowing Clostridium difficile to multiply and produce two toxins: an enterotoxin and a cytotoxin. These initiate the diarrhoea and the resultant pseudomembranes (yellow-white plaques) on the colon visualized by sigmoidoscopy.
Outbreaks are commonly reported in long-stay wards and hospitals.
Diagnosis
Clinical diagnosis is by proctosigmoidoscopy to detect the pseudomembranes. The toxin in stool samples can be detected by its toxic effect on cultured cells.
Bacillus cereus
Bacillus cereus is an aerobic, spore-forming Gram-positive bacillus commonly found in soil, air and dust.
Pathogenesis and epidemiology
The organisms can contaminate rice and soups, or survive cooking by sporulation. When the food is stored at room temperature, reheated or fried quickly, the spores germinate into vegetative forms, multiply and liberate an enterotoxin. The latter, when ingested with contaminated food, causes diarrhoea either within 1–2 h (short incubation) or within 6–18 h (long incubation). The disease is commonly associated with Chinese restaurants because of their bulk use of rice.
Enteric fever
The term ‘enteric fever’ is given to typhoid and paratyphoid infections caused by Salmonella typhi and Salmonella paratyphi-A, -B and -C, respectively; Salmonella paratyphi-A and -C are common in the tropics, while type B is common in Europe. Both diseases are due to salmonellae that are significantly more virulent and hence invasive than those responsible for food poisoning.
Clinical features
Typhoid fever
The onset of typhoid fever is slow, with fever and constipation (compare diarrhoea and vomiting of Salmonella enteritidis). After the first week (following the 2- to 3-week incubation period), the bacteria enter the blood stream (i.e. bacteraemia), with resultant high fever, delirium and tender abdomen with ‘rose spots’ (rose-coloured papules on the abdomen). The disease begins to resolve by the third week, but severe complications such as intestinal haemorrhage or perforations may occur if the disease is not promptly treated. About 3% of typhoid patients become chronic carriers of the organism, a favourite reservoir of which is the gall bladder.
Pathogenesis and epidemiology
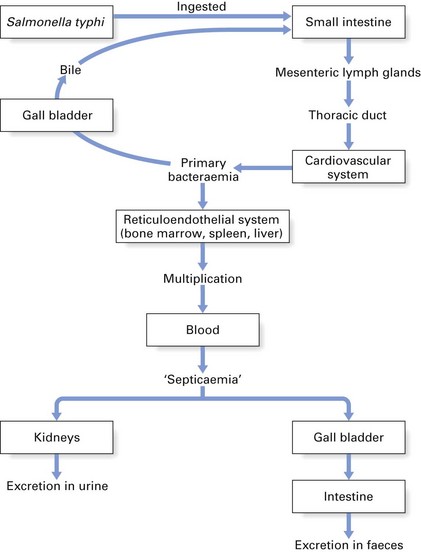
In typhoid fever, the organism takes a complicated route inside the body after entering the alimentary tract (Fig. 26.2). The pathogenicity of salmonellae appears to depend both on their ability to survive and grow inside macrophages and on the potency of their endotoxin (O antigen of the lipopolysaccharide). Further, the typhoid bacilli possess a glycolipid, the virulence (Vi) antigen, that protects the organism from phagocytosis.
The reservoir of infection is the human gut, during both the acute and the carrier phases of the infection (which may last up to 2 months after the acute illness). Spread occurs via water, food or the faecal–oral route. Small numbers of Salmonella typhi can cause typhoid fever, whereas large doses of Salmonella paratyphi are required to initiate paratyphoid fever.
Diagnosis
Diagnosis is by isolation of the organisms from blood (first week of disease), stools and urine (second and third weeks) in selective media such as MacConkey’s agar, DCA or bismuth sulphite agar or in fluid enrichment media. Identification is by biochemical tests (e.g. API test) and serology (screening for H and O antigens by appropriate antisera). Further typing with bacteriophages (phage-typing) can be performed.
Widal test
When Salmonella typhi cannot be isolated, the diagnosis can be made serologically by demonstrating a rise in antibody titre in the patient’s serum. This classic test, called the Widal test, consists of demonstrating antibodies to flagellar H antigen (using formalized bacteria) and somatic O antigen (using boiled bacteria) of Salmonella typhi and Salmonella paratyphi-A and -B. Interpretation of the test is difficult if the patient has been immunized with typhoid vaccine.
Treatment
Chloramphenicol, co-trimoxazole and ciprofloxacin are useful drugs, both in the treatment of acute typhoid fever and of the carrier state.
Prevention
Good personal hygiene and public health measures, i.e. safe water supplies, adequate sewage disposal and supervision of food processing and handling, are of great importance. Carriers of the organism should not be employed in the food industry. Immunization is useful. Two types of vaccine are available for travellers to – or those living in – endemic areas:
Non-bacterial causes of diarrhoea
The foregoing lists the major causes of bacterial diarrhoea. It is important to realize that there are a number of viral and protozoal agents that may cause diarrhoea. These major non-bacterial causes of diarrhoea are briefly outlined below (and see Table 26.1).
Infantile gastroenteritis due to rotavirus
Apart from E. coli diarrhoea in children, the major cause of infantile gastroenteritis is rotavirus infection. This infection, seen mainly in older children and sometimes in adults, may be accompanied by respiratory illness. Laboratory diagnosis is by electron microscopy of stools for viral particles or enzyme-linked immunosorbent assay (ELISA) for antigen in stools.
Protozoal diarrhoeal diseases
Amoebiasis (amoebic dysentery)
Caused by Entamoeba histolytica, the symptoms of amoebic dysentery vary from fulminating colitis to absence of symptoms. The disease is common in the tropics and is usually acquired via food contaminated by the cysts of the organism.
Giardiasis
Infection with Giardia lamblia, a flagellate protozoan with a pear-shaped body, gives rise to symptoms of abdominal discomfort, flatulence and diarrhoea; malabsorption and steatorrhoea may develop in chronic infection. Both children and adults are affected, and it is a common bowel pathogen in countries throughout the world.
Probiotics and gastrointestinal infections
Probiotics are defined as substances secreted by one microorganism that stimulate the growth of another. The use of probiotics to prevent and treat a variety of diarrhoeal diseases as well as to maintain general gastrointestinal health has gained favour in recent years. However, the overall efficacy of these treatments and the mechanisms by which probiotics ameliorate gastrointestinal infections are mostly unknown.
Probiotic bacteria currently used include:
Probiotics may be delivered to the host via capsules, in powder format or laced in food (such as the lactobacilli) in various milk-related manufactured products.
Mechanisms of action
Postulated mechanisms by which probiotics may help the host include:
Key facts
Britton R.A., Versalovic J. Probiotics and gastrointestinal infections. Interdisciplinary Perspectives on Infectious Diseases. 2008. Article ID 290769. doi:10.1155/2008/290769
Mims C., Playfair J., Roitt I., Wakelin D., Williams R. Gastrointestinal tract infections, Ch. 20. Medical microbiology, 2nd ed. London: Mosby. 1998.
Shanson D.C. Infections of the gastrointestinal tract, Ch. 15. Microbiology in clinical practice, 3rd ed. Oxford: Butterworth-Heinemann. 1999.
Review questions (answers on p. 354)
Please indicate which answers are true, and which are false.