Chapter 32 Primary Lesions of the Deep Digital Flexor Tendon within the Hoof Capsule
Anatomy
Within the hoof capsule the deep digital flexor tendon (DDFT) is molded to the palmar (plantar) surface of the navicular bone and separated from it by the navicular bursa. Proximally the DDFT is intimately related to the distal digital annular ligament on its palmar aspect. The distal recess of the navicular bursa separates the DDFT and the distal sesamoidean impar ligament (DSIL). The DDFT has a terminal fanlike expansion containing cartilage that occupies the entire space between the medial and lateral palmar processes of the distal phalanx. It inserts on the facies flexoria and semilunar crest of the distal phalanx. The dorsal portion of the DDFT joins with the DSIL immediately before insertion on the facies flexoria of the distal phalanx. There are parallel fibers of dense connective tissue, separated by loose connective tissue, within which are many sensory nerves and numerous blood vessels.1 A prominent line (tidemark) indicates the transition from nonmineralized tendon and ligament to mineralized regions of the DDFT and DSIL before attachment to the distal phalanx.2
Within the digit the DDFT induces axial compression of the articular surfaces of the proximal and distal interphalangeal joints.2,3 It has an important role in stabilizing the distal interphalangeal joint. The anatomical arrangement of the collateral ligaments of the navicular bone facilitates compression of the articular surfaces of the navicular bone into those of the middle and distal phalanges.2 The DDFT has a dorsal fibrocartilaginous pad that supports pressure of the tuberositas flexoria, the transverse prominence on the proximopalmar aspect of the middle phalanx.3
The relationship of the DDFT to the navicular bone varies with the phase of the stride. During the full weight-bearing stance of the stride the DDFT is only in contact with the distal aspect of the bone, whereas in the propulsion phase the DDFT bends over the distal scutum (the fibrocartilaginous insertion of the straight sesamoidean ligament on the middle phalanx) and comes into full contact with the navicular bone. Tension in the DDFT is maximal, and active muscle contraction and the elasticity in the tendon and in its accessory ligament result in extension of the distal interphalangeal joint.3 At the beginning of the swing phase of the stride the tension in the DDFT contributes passively to induce flexion of the interphalangeal joints. During extension of the distal interphalangeal joint, which is maximum at the propulsion phase of the stride, pull on the DDFT creates a shear force between the DDFT and the DSIL.2
Pathophysiology
Primary lesions of the DDFT have only recently been recognized clinically, and only limited information concerning pathophysiology is available. A progressive increase in proteoglycans with age was seen in the distal aspects of the DDFT and DSIL, which may be an adaptation to stress.2 It was suggested that horses with low, weak heels may be more susceptible to these changes. Similar but more extensive changes were seen in two horses with navicular disease. Lesions within the DDFT within the foot were identified in fewer than 10% of horses with unknown history in a post mortem study of superficial digital flexor tendon and DDFT lesions in the metacarpal region and digit.4
In a post mortem study of 38 horses with suspected navicular disease, one horse had a core lesion of the DDFT with no associated pathological condition of the navicular bone5; four additional horses had histological evidence of focal regions of necrosis within the tendon concurrent with other pathological conditions of the navicular bone. Surface fibrillation was a common finding in horses with navicular disease but not in age-matched controls. No lesions of the DDFT were described in the age-matched controls. Pool et al6 considered lesions in the DDFT to be secondary to navicular disease. Inflammation at the intersection of the DDFT and DSIL was recognized in the Quarter Horse in association with other signs compatible with navicular disease.7 It was considered that these lesions may be involved with the pathogenesis of navicular disease.
A variety of different types of lesions of the DDFT have been identified using magnetic resonance imaging (MRI) and confirmed post mortem.8-11 These include partial or full-thickness sagittal plane splits, dorsal abrasions, fibrillation, and core lesions. Core lesions within the tendon or on the dorsal surface, full-thickness parasagittal splits can be seen alone and are considered primary lesions of the DDFT, whereas fibrillation and small isolated incomplete parasagittal splits are commonly seen in association with other lesions of the podotrochlear apparatus.12-14 Core lesions or full-thickness splits usually occur extending proximally from the proximal aspect of the navicular bursa or distal to the navicular bone. Isolated incomplete parasagittal plane splits, minor dorsal abrasions, and fibrillation are seen most commonly from the proximal level of the navicular bursa distally.
In recent studies comparing MRI and histopathology in groups of horses with chronic foot pain and age-matched control horses, the incidence of DDFT lesions was considerably higher than previously recognized.8-11 Degenerative changes of the DDFT were seen in both groups but were of greater severity in the lame horses. Thickening of septae, with ghosting and occlusion of blood vessels, and fibrocartilaginous and chondroid metaplasia were characteristic findings, which may predispose to fibrillation and dorsal splits of the tendon. Such changes have also been identified in the proximity of necrotic core lesions. The presence of degenerative changes within the DDFT was not age related. With all types of lesions of the DDFT there was a notable absence of acute inflammatory reaction.
Primary deep digital flexor (DDF) tendonitis may be the result of repetitive overstress or an acute-onset traumatic tear, possibly superimposed on preexisting degenerative change. The identification of severe core lesions in young horses that have done relatively little work suggests that some horses may have an inherent predisposition to injury.
Rupture of the DDFT secondary to previous neurectomy of the palmar digital nerves is considered a separate condition; however, it is likely that a preexisting, unrecognized pathological condition of the DDFT predisposes to rupture (see Chapter 70).
Dystrophic or ectopic mineralization within the DDFT was identified radiologically, at the level of the navicular bone and immediately proximal to it, but its clinical significance has been speculative.15 Entheseous new bone at the site of insertion of the DDFT on the facies flexoria and semilunar crest of the distal phalanx was described associated with lameness and unassociated with navicular disease.16 Nuclear scintigraphic examination of horses with palmar foot pain has revealed horses with linear increased radiopharmaceutical uptake (IRU) in the DDFT in pool phase images or focal regions of IRU in the region of insertion of the DDFT on the distal phalanx,17,18 either alone or in association with a region of increased uptake in the navicular bone. This has correlated well with lesions identified using MRI.
History and Clinical Signs
Lameness associated with primary DDF tendonitis within the hoof capsule has been identified most commonly in horses that jump,12-14 but it has also been seen in general-purpose riding horses. Lameness usually is unilateral, acute in onset, and moderate to severe in intensity. In horses with severe lameness, the horse may point the affected limb at rest. In mild to moderate injuries, lameness may resolve with rest but recur with work and progressively worsen.
There are generally no clinically significant palpable abnormalities of the limb, unless the lesion extends proximally into the pastern region. There is also no response to pressure applied to the foot with hoof testers. Lameness is often worse on a soft surface, especially on a circle, and in some horses is apparent only under these circumstances. A core lesion in the lateral lobe results in lameness worst with the lame limb on the outside of a circle, whereas a medial lobe lesion usually results in lameness worst with the lame limb on the inside of a circle. The response to distal limb flexion is variable; flexion of the nonlame limb may exacerbate lameness in the lame limb. Extension of the distal interphalangeal joint using the board or wedge test may accentuate the lameness.
Local Analgesia
Perineural analgesia of the palmar digital nerves immediately proximal to the cartilages of the foot usually, but not invariably, improves lameness; however, rarely is lameness fully alleviated. Perineural analgesia of the palmar nerves at the level of the base of the proximal sesamoid bones usually abolishes the lameness. Intraarticular analgesia of the distal interphalangeal joint results in rapid improvement in lameness in some horses, but in others lameness persists unchanged. There has been no correlation between the analgesic response and the proximodistal site of the lesion.12 Analgesia of the navicular bursa often results in improvement in lameness but rarely alleviates it fully. Intrathecal analgesia of the digital flexor tendon sheath may result in improvement in lameness, but this technique is not specific for DDFT lesions and does not reliably alter lameness associated with lesions confined to the insertion.
Diagnostic Imaging
Radiography
In some lateromedial radiographic images of the foot a faint outline of the DDFT can be seen; the clinical significance of this finding is unknown. Occasionally a focus of mineralization is seen within the DDFT, at the level of or proximal to the navicular bone, and usually reflects chronic DDFT injury. In a well-positioned, high-detail lateromedial image, entheseous new bone or a radiolucent focus may be identified on the facies flexoria of the distal phalanx. This finding has been seen more commonly in heavier Warmblood breeds16 than in Thoroughbred and cross-bred horses and has been correlated with increased bone activity identified by nuclear scintigraphy.
Ultrasonography
Diagnostic ultrasonographic imaging of the DDFT within the hoof capsule is not easy because of the horny hoof capsule and the difficulties in orientating the ultrasound transducer perpendicular to the line of the tendon fibers. Thus it is easy to create artifacts. The proximal part of the DDFT may be imaged using a 6.5-MHz transducer positioned between the bulbs of the heel, unless the heel is very contracted. The region of the DDFT overlying the navicular bone and close to its insertion is potentially seen by a solar approach, placing the transducer (7.5 MHz) on the frog. The frog must be sufficiently soft; this generally is achieved by soaking the foot by bandaging a water-soaked sponge on the foot for several hours. If the horn is exceptionally hard, soaking may have to be continued for several days. The horn must also be pared to provide a relatively flat site for placement of the ultrasound transducer. This is difficult to achieve if the horse has a very narrow foot with a deep frog cleft and sulci. Only the region of the DDFT in the midsagittal plane can be successfully imaged. Orientation is achieved most easily in longitudinal images.
A normal DDFT has linear, parallel echoes, and its margins are well defined.20 An anechoic region representing fluid in the navicular bursa is interposed between the DDFT and the echoic line of the palmar aspect of the navicular bone. Lesions are characterized by enlargement of the tendon and thus loss of its parallel margins. Fiber pattern cannot be assessed, but the presence of mineralization can be detected. Lesions extending into the pastern region may be seen as core lesions, but false-negative results may occur. However, identification of a core lesion in the pastern is generally associated with a lesion that extends further distally.
Nuclear Scintigraphy
Pool and bone phase nuclear scintigraphic lateral and solar images of the foot have been used to identify a region of IRU either at the site of insertion of the DDFT on the facies flexoria of the distal phalanx or further proximally within the DDFT12,18 (Figures 32-1 and 32-2). Superimposition of a lateromedial radiographic image and a lateral scintigraphic image helps to accurately locate the site of increased radiopharmaceutical uptake. Although the bone phase solar (palmar) view may be more sensitive for identification of abnormal modeling associated with insertional stress, false-positive results may occur.17
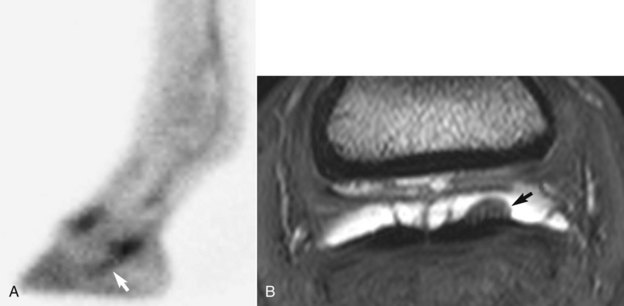
Fig. 32-1 A, Lateral pool phase scintigraphic image of the left front foot of a 9-year-old event horse with a history of acute-onset severe lameness after competing. Lameness had persisted despite rest for 3 weeks. Lameness was improved by perineural analgesia of the palmar digital nerves or intraarticular analgesia of the distal interphalangeal joint, but it was not affected by analgesia of the navicular bursa. There is linear increased radiopharmaceutical uptake (arrow) in the region of the deep digital flexor tendon (DDFT). Magnetic resonance imaging demonstrated multifocal lesions of the DDFT. B, Transverse three-dimensional T2*-weighted gradient-echo magnetic resonance image of the same foot in A, at the level of the middle phalanx. Medial is to the left. There is a lesion of the dorsal aspect of the lateral lobe of the DDFT, with granulation tissue (arrow) protruding into the distended navicular bursa.
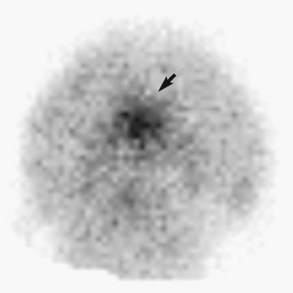
Fig. 32-2 Solar (palmar) bone phase scintigraphic image of the left front foot of a 7-year-old show jumper with acute-onset, chronic left forelimb lameness that was alleviated by perineural analgesia of the palmar digital nerves. There is a focal region of intensely increased radiopharmaceutical uptake in the distal phalanx at the site of the insertion of the deep digital flexor tendon (DDFT) (arrow). Post mortem examination revealed focal bone necrosis and reactive bone at this site associated with the insertion of the DDFT.
The results from pool phase lateral images have correlated well with findings using MRI, arthroscopic evaluation of the DDFT through the navicular bursa, and post mortem studies. However, the presence of IRU at the DDFT insertion on the distal phalanx does not necessarily reflect an insertional injury; tendon lesions may be restricted to proximal to the navicular bone.18
Computed Tomography
Computed tomography (CT) can only be performed with the horse under general anesthesia but has the potential to give information about the size, shape, and internal architecture of the DDFT within the hoof capsule. Therefore it is an accurate method of diagnosis of primary DDFT lesions. Lesions have been identified in one or both of the two lobes of the DDFT and were seen as an enlargement of the DDFT with an increase or decrease in density21,22 (Figure 32-3). Thirteen of 78 horses examined using CT had abnormalities of the DDFT within the hoof.21 Correlation of an abnormal CT scan result with abnormalities verified at post mortem examination has been described without clinical details.21 The use of a contrast agent can facilitate identification of relevant lesions and may be helpful in determining the chronicity of the lesion. CT also provides the opportunity to perform image-guided intervention, such as injection of a core lesion.22
Magnetic Resonance Imaging
MRI can be performed either with the horse under general anesthesia or in a standing sedated horse, and offers the optimal method of diagnosis of primary DDFT lesions12-14,23 (Figures 32-4 and 32-5). Lesions are seen best in sagittal and transverse planes. Most core lesions are visible in T1- and T2-weighted images and fat-suppressed images and are characterized by increased signal intensity extending a variable distance proximodistally, often associated with enlargement of a cross-sectional area of the affected lobe. Fat-suppressed two-dimensional fast spin-echo or three-dimensional gradient-echo sequences also are useful for detection of bone pathology at the insertion. Dorsal core lesions within the navicular bursa are often covered dorsally by granulation-like tissue.
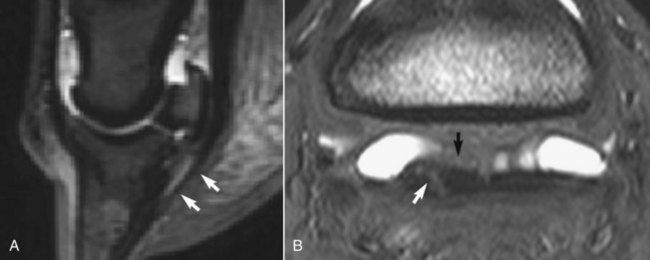
Fig. 32-4 A, Sagittal short tau inversion recovery magnetic resonance image of a left front foot. There is swelling of the distal aspect of the deep digital flexor tendon (DDFT), which has diffuse increase in signal intensity. B, Transverse three-dimensional T2*-weighted, gradient-echo magnetic resonance image of the left front foot of a 9-year-old medium-level dressage horse, with lameness improved by palmar digital analgesia and abolished by perineural analgesia of the palmar (abaxial sesamoid) nerves. There is a core lesion of the DDFT characterized by increased signal intensity (white arrow) and some soft tissue proliferation within the navicular bursa (black arrow).

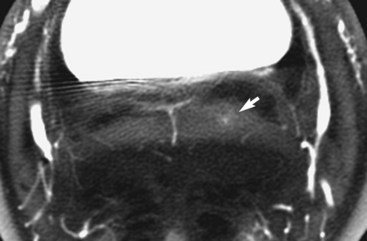
Fig. 32-5 Sagittal spoiled gradient-echo magnetic resonance image of the right front foot of an advanced event horse with acute-onset severe lameness that was alleviated by perineural analgesia of the palmar digital nerves and improved by intraarticular analgesia of the distal interphalangeal joint. The deep digital flexor tendon (DDFT) is enlarged and has increased signal intensity proximal to the navicular bone (arrow). This correlated with an extensive core lesion at post mortem examination. Increased signal intensity in the DDFT and distal sesamoidean impar ligament distal to the navicular bone reflects the magic angle effect.
Most primary DDFT lesions have been identified immediately proximal to the navicular bone, extending a variable distance proximally, to as far as the proximal aspect of the proximal phalanx.14 Such lesions are often not detectable using ultrasonography. A smaller proportion of lesions have been identified at the insertion of the DDFT. Lesions usually are restricted to either the medial or the lateral lobe, but occasionally they occur in both lobes. Core lesions or dorsal fiber disruption, sometimes with herniation of fibers and granulation tissue into the navicular bursa, are most common. Focal, full-thickness, sagittal plane splits have also been seen at the level of the navicular bone in association with abnormal signal intensity in the palmar cortex of the bone. Seventy-five of 347 horses (21.6%) with palmar foot pain of previously undetermined cause had primary DDFT injuries diagnosed using MRI.19 A further 40 horses had combined lesions of the navicular bone and DDFT.
Correlation of the results of MRI examination of cadaver specimens from horses with clinically suspected DDFT lesions and post mortem examination has been good9-11 (see Figure 32-5). Collagen necrosis and chondroid metaplasia within the DDFT have been seen in regions of increased signal intensity.9-11 Care must be taken in the interpretation of sagittal plane images in the region of insertion of the DDFT in T1- and T2-weighted high-field magnetic resonance images because there is increased signal intensity in normal horses. This is related in part to the composition of the tendon but also to the magic angle effect, which results from orientation of fibers at approximately 55 degrees to the static magnetic field (see Figure 32-5).
Surgical Exploration
Endoscopic examination of the digital flexor tendon sheath and the navicular bursa allows visual evaluation of the surface of the DDFT and assessment of its integrity by probing (see Chapter 24). Some dorsal core lesions of the DDFT are associated with extensive surface fibrillation of the tendon and inflammation of the synovial lining of the navicular bursa with villous proliferation. However, this technique is invasive and provides only limited information about the internal architecture of the tendon, although it does offer the option of surgical debridement of dorsal lesions.
Treatment
Successful treatment of horses with core lesions of the DDFT remains a challenge. Core necrosis can ultimately repair by fibroplasia; however, long-term follow-up studies to date indicate a high rate of recurrent lameness after prolonged periods (6-12 months) of box rest and controlled exercise and corrective trimming and shoeing.19,24 Lesions often reduce in size, but usually there is persistent high signal intensity on T1-weighted magnetic resonance images. Twenty-nine per cent of 84 horses returned to full athletic function for a period of more than 6 months and up to 4 years.24 In a separate study 25% of 55 horses returned to full athletic function. Lesion type or proximodistal location did not appear to influence prognosis.25 Longer-term follow-up evaluation indicates that rest for a minimum of 12 to 18 months may result in an improved outcome.26,27 Surgical debridement of dorsal core lesions within the navicular bursa was successful in 54% of 63 horses,28,29 but with relatively short follow-up time. This technique is only of use for dorsal lesions, not central core lesions or large splits in the DDFT. Complications have included recurrent lameness associated with adhesion formation within the navicular bursa. CT-guided injections of the DDFT have been performed using a variety of preparations (A cell, platelet-rich plasma, stem cells), but long-term follow-up information is not yet available. Short-term improvement may be seen after medication of the navicular bursa and/or digital flexor tendon sheath with corticosteroids, but repeated injections may predispose to progression of lesions.