Chapter 49Diagnosis and Management of Pelvic Fractures in the Thoroughbred Racehorse
Injuries to the pelvis of the horse have historically been considered uncommon.1-3 They have also previously been described as invariably resulting from external trauma.4 Pelvic fractures are now recognized as a common cause of lameness in the racing Thoroughbred (TB). Stover et al5 confirmed a high incidence of stress fractures in the pelvis of American racing TBs examined at post mortem. Similarly in a clinical study performed in Newmarket, England, pelvic fractures were found to be common in the young racing TB.6,7 We now realize that pelvic fractures in the TB are most often the end stage of a cycle of bone fatigue and injury, commonly called stress-related bone injury. This has focused attention on early detection before the development of a full-blown displaced fracture. This section outlines steps to aid in early detection and management strategies subsequent to diagnosis.
Pelvic Anatomy
The pelvis comprises the symmetrical halves and the sacrum in the midline. The left and right halves of the pelvis are joined in the ventral midline at the pubic symphysis. Although technically a joint, this becomes mineralized with age and is a bony union in most horses. A second joint occurs on each side between the pelvis and the head of the femur, forming the coxofemoral joint. The third joint is that between the ventral surface of the pelvis and the sacrum, the sacroiliac joint. Only the coxofemoral joint has any substantial degree of movement. The sacroiliac joint does have a synovial membrane, but it is largely immobile in many horses. In most horses the sacroiliac joint is spanned by dense bands of fibrous connective tissue, and despite having a cartilage surface, little or no movement takes place in the normal sacroiliac joint. Each half of the pelvis comprises three bones, which meet at the acetabulum, the ilium cranially, the ischium caudally, and the pubis medially. The ilium has a large wing of bone extending from the tuber sacrale in the midline to the tuber coxae at the lateral extremity. The blade of the ilium narrows to form the shaft, which extends back to form the cranial segment of the coxofemoral joint. Caudal to the coxofemoral joint, and forming its caudal margin, is the ischium. Joining the two acetabula, forming the floor of the pelvis with its contralateral counterpart, is the pubis. The bones of the pelvis form a large fulcrum on which most of the gluteal muscle mass originates, to exert considerable propulsive forces on the hindlimbs. Although the pelvis can fracture anywhere as a result of external trauma or a fall, as is common with many other stress injuries, the forces involved in locomotion create predilection sites for stress fractures. These sites are associated with the concentration of forces involved in load bearing at speed and the biomechanics, innate structure, and form of the bone.
Diagnostic Techniques
Clinical Examination
A thorough working knowledge of the anatomy of the equine pelvis is essential for clinical examination to be useful. Because of the large muscle mass over the horse’s hindquarters, only the bony extremities of the pelvis can be palpated. However, it is often possible to gain information about horses with pelvic injuries by studying the position of these bony landmarks. For example, the normal position and angle of the tuber coxae in the racehorse are often disturbed in horses with fracture or sacroiliac joint instability. The position of the tubera coxae can be assessed by viewing the horse from behind, with an assistant placing fingertips on the craniodorsal extremity of the tubera coxae (Figure 49-1). It is important that the horse stands completely level, with both hind feet together, for this test to be meaningful. Some horses, however, show asymmetry viewed in this way that is not linked to lameness. Similarly, careful palpation of the tubera sacrale can give information about the possible involvement of the sacral wing of the ilium or disruption of the sacroiliac joint.
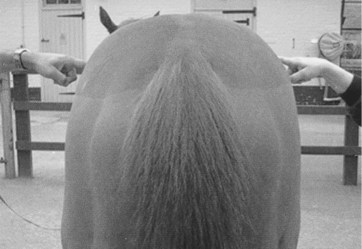
Fig. 49-1 Assessment of the position of the bony pelvis by fingertip levels placed on the dorsal extremity of the tubera coxae on either side.
Ventral displacement of one tuber sacrale is commonly encountered in ilial wing fractures, where the overlap of the fracture fragments seems to allow the tuber sacrale to move ventrally. Often a pain response is associated with palpation of a horse with tuber sacrale displacement, and sometimes movement of the bone itself may be felt if the fracture is complete. Fracture of a tuber coxae is often produced by external trauma, usually after a fall, but can also occur as a stress-related athletic injury. This usually results in a cranioventral displacement of the fracture fragment because of the distractive forces of associated musculature. The tuber coxae in these horses can often be felt situated in the sublumbar fossa, and the remnant fracture bed can be palpated at the original site. Fractures of the ischium can sometimes be felt by manual palpation, although the extensive muscle spasm and protective boarding that are associated with these fractures often preclude this examination. Usually there is hemorrhage and swelling in the acute phase, but a clear loss of muscle mass or even a “hollow” in the caudal contour of the rump may develop with time as inflammation subsides. Finally, muscle tone in the tail and anus should be evaluated because fractures involving the sacrum can involve neural elements that supply these structures and cause flaccid paralysis of the tail, rectum, anal ring, and vulva (in a filly), that is, the cauda equina syndrome (Figure 49-2). Bilateral ilial wing fractures can produce the same neurological appearance associated with severe nerve root damage consequent on movement of the pelvis in relation to the sacrum.
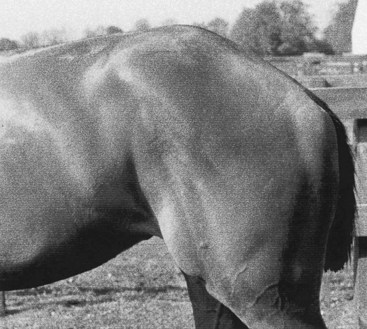
Fig. 49-2 A horse with a sacral fracture. Note the abrupt angle change just behind the tubera sacrale, where the sacrum and coccyx have moved ventrally. The tail has complete flaccid paralysis. This filly had urine and fecal retention.
Rectal examination allows direct manual assessment of the integrity of the pubis, internal surface of the wing of the ilium, and ventral border of the sacroiliac joint. Sometimes an obvious, sharp discontinuity in the bone surface can be felt, particularly in horses with fracture of the pubis. Gentle rocking of the horse by an assistant, while the clinician maintains digital contact with the bone surface of the pelvis per rectum, sometimes allows an appreciation of relative movement of adjacent bones or, more commonly, a sensation of crepitus. In horses with fracture of the ilial wing, a soft asymmetrical swelling can often be felt at the fracture site, representing a subfascial hematoma. The more serious and potentially fatal hemorrhage that occurs when an iliac artery is severed by the sharp dorsal edge of the fractured ilium often cannot be detected per rectum. If not immediately fatal, this free blood often percolates ventrally to cause massive swelling and edema of the thigh musculature.
Some horses have several stress fractures identified scintigraphically, only one of which may have initially collapsed, leading to overt lameness. Progressive collapse of the pelvis may then occur during the convalescent period, as incomplete fractures become complete and displaced because of bone resorption and weakening of the fracture site. The degree of lameness seen in these horses varies enormously, depending on the type and extent of the fracture, and is considered separately in the following discussions of each class of fracture.
Diagnostic Ultrasonography
Ultrasonography is useful for diagnosing pelvic fractures and has proved especially useful in demonstrating fractures of the ilial wing (Figure 49-3), ilial shaft, tuber coxae, and ischium. Ultrasonography is quick, easy, and within the capability of clinicians with a suitable ultrasound machine. Ultrasonography may eliminate the requirement for a horse to travel to a referral center for diagnosis, and the risk associated with radiography under general anesthesia can be avoided. Ultrasonography has obvious limitations. For example, adequate imaging of the sacral wing, sacroiliac joint, and the femoral head is not possible. Fractures with minimal displacement or poorly developed callus are also difficult to image, as are incomplete fractures involving the ventral surface of the ilium. For this reason, ultrasonography should not be regarded as a standalone imaging modality for identifying a fracture of the pelvis but should be used with a thorough clinical examination and, if available, scintigraphy. In many horses, the exact site and extent of the fracture can be determined, which allow improved prognostic and management advice to be given. The healing process can be monitored by serial examinations, allowing the management program to be tailored to the individual horse (see Figure 49-3, B and C). A longitudinal- or sector-array ultrasound transducer can be used, provided it has a deep enough penetration to see the bone surface (i.e., a 3.5- or 5-MHz transducer). The muscle mass lying above the bone structures acts as a natural “standoff,” bringing the bone surfaces into the focal zone of the ultrasound beam. A separate standoff may be required to evaluate the position of the tubera sacrale and to detect any displacement. In thin-coated horses, no clipping is required, provided adequate saturation of the coat is achieved by degreasing with a detergent solution (chlorhexidine) or by soaking in surgical spirit, followed by application of a coupling gel before scanning. Horses with thicker hair coats must be clipped to obtain images of adequate quality. Images can be difficult to produce in horses with large amounts of subcutaneous fat because of the attenuating properties of this tissue. Numerous blood vessels running through the musculature can create acoustic shadows, which may be confused with a discontinuity of the bone surface. Identifying the bony landmarks such as the tubera sacrale, tubera coxae, cranial and caudal margins of the ilial wing, and greater trochanters of the femur allow anatomical orientation. A dry pelvic specimen is also useful in orientation. Both sides of the pelvis should be evaluated because the normal side can be used for comparison. However, keep in mind that bilateral ilial wing stress fractures occur and both sides may be abnormal. For recording and reference purposes, the area of the ilial wing imaged is referred to as line A, B, or C, and the distance from the tuber sacrale is measured. Scans aligned longitudinally along the ilial shaft are referred to as line D. This simple system is useful, especially in follow-up examinations. A systematic method for recording ultrasonographic findings has been published elsewhere.8
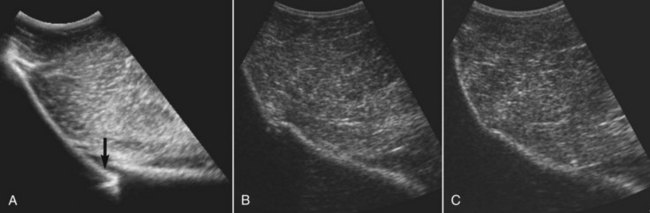
Fig. 49-3 A, Ultrasonographic image of the right ilial wing obtained using a 3- to 5-MHz transducer. There is a stress fracture of the ilial wing (arrow). The fracture appears as a discontinuity in the pelvis surface, with some comminution evident. Adjacent to the fracture is irregular echogenic material (callus), and just dorsal to the fracture is an anechogenic defect in the muscle (hemorrhage). Healing can be monitored by serial ultrasonographic examination, here at 63 days (B) and 109 days (C) following injury.
Radiography
Radiography of the pelvis is easily carried out in a foal when it can be performed under heavy sedation, for example, with a combination of detomidine and butorphanol, with the foal allowed to stand again shortly after the procedure. Standard projections include a ventrodorsal image with the foal lying on its back and a lateral image with the foal lying on its side on top of the cassette. A grid is mandatory to reduce scattered radiation produced by the large mass of soft tissue covering the pelvis. Radiography in adult horses is considerably more difficult. General anesthesia is required for thorough radiographic examination of the pelvis for numerous reasons, including the safety of the horse, personnel, and radiographic equipment. Administering general anesthesia to a horse suspected of having a pelvic fracture is contraindicated because of the possibility of the horse displacing the fracture on recovery. Fracture displacement can lead to fatal hemorrhage or worsening of clinical signs, which is particularly true in horses with an incomplete fracture of the wing and shaft of the ilium. It is also difficult to get high-quality radiographs of the pelvic bones without extensive previous starvation of the horse to allow emptying of the gastrointestinal tract. Small, incomplete, pelvic stress fractures are extremely difficult to see radiologically. Three techniques for standing radiography in the horse have been described.9-11 However, in my experience this has proved difficult, presents real risks of damage to the equipment, and is a substantial radiation hazard to attending personnel. The standing examination is also limited to examination of the acetabulum and ilial shaft, and images of the ilial wing are obscured by the sublumbar and overlying dorsal lumbar musculature. Image quality obtained in this way is also often poor; however, it may permit detection of substantially displaced fractures. Although radiography used to be the imaging technique of choice for assessing horses with pelvic fractures, it has been replaced by combined ultrasonographic and scintigraphic evaluation in many hospitals.
Scintigraphy
Scintigraphy is considered the most sensitive method of assessing acute bone damage in the horse (see Chapter 19).3,12-17 Special techniques for examining the pelvis have also been described, including an oblique image of the ilium, which is useful in diagnosing incomplete stress fractures in this site.16 Sacroiliac joint luxation has also been described as a scintigraphic diagnosis, the appearance of which is extremely similar to the ilial wing fractures observed by others.3 Equine scintigraphic techniques applicable to the pelvis, as well as numerous examples of normal and most types of pathology, have also been published in detail elsewhere.17 To examine the equine pelvis fully using a gamma camera, dorsal images of the entire pelvis are mandatory. The lateral image of the pelvis tends to be difficult to interpret because of the areas of focal greater radiopharmaceutical uptake (RU) observed at tubera coxae and the coxofemoral joints in a normal horse. The massive muscle mass interposed between the slender bones of the ilial shaft and the gamma camera results in extensive shielding and poor images. Radioactive urine in the underlying bladder contributes to extensive background radiation, further decreasing image quality. Movement is a key factor in limiting image quality, but motion correction software can be used to minimize this complication. However, the lateral oblique image described by Hornof et al16 usually gives better images of the ilial wing and shaft. A caudal oblique image is also used by some to give better images of the coxofemoral joint and acetabulum. A method for scintigraphic examination of the pelvis using a hand-held probe has also been described.18 If a pelvic fracture is strongly suspected and initial scintigraphic examination is performed within 3 to 5 days of injury and is negative, a follow-up examination should be performed at least 10 days from the time of injury. Early fractures, even those with associated displacement, may not be evident scintigraphically for several days after injury.
Fractures of the Tuber Coxae
Fractures of a tuber coxae are often described as a knocked-down hip. They are relatively common and fairly straightforward to diagnose by clinical examination of the bony landmarks of the pelvis. They may occur after direct trauma or a fall but also as an athletic injury in training or racing.
Clinical Signs
On the first day of injury, the horse is moderately to severely lame, even at the walk. Often the horse shows intense muscle spasm and guarding of the affected hindquarter. The horse may sweat and scrape the ground, which can mimic signs of colic. The affected tuber coxae is often displaced cranioventrally and is palpable in the region of the sublumbar fossa. The parent bed from which the fragment originated is often palpable in the original site of the tuber coxae. Lameness rapidly resolves, and many horses are walking sound after only 24 to 48 hours, but they will still trot lame. Hemorrhage often occurs, which may present as a subcutaneous hematoma. Occasionally the sharp spiculated end of the ilium wears through the overlying skin, leading to development of an open fracture, which can be extremely difficult to treat because the skin overlying the sharp fragment will not heal and infection becomes a problem.
Radiographic Examination
A technique to evaluate the tubera coxae in the standing horse was recently described, but strict attention to limiting radiation exposure to attending personnel should be followed.11 A medial 50° dorsal-lateroventral oblique radiographic image is obtained with the horse standing, sedated in stocks with the horse bearing weight on the affected limb and resting the unaffected limb, if possible.11
Scintigraphic Examination
Scintigraphic examination is probably not indicated in most horses because the clinical diagnosis is straightforward. If performed, scintigraphic examination reveals clinically significant focal increased radiopharmaceutical uptake (IRU) associated with the displaced tuber coxae and also a fairly obvious distortion of the normal anatomy of the pelvis on the dorsal image. In the Editors’ experience, photopenic regions associated with ventral displacement of the fracture fragments may be present.
Ultrasonographic Examination
Directly after injury, horses with a tuber coxae fracture have clinical signs similar to those with other fractures of the pelvis, and an ultrasonographic examination helps to confirm the diagnosis and to define better the limits of the fracture. The fracture is easily seen as a disruption to the normally smooth and continuous contour of the ilial wing as it approaches the tuber coxae. A standoff may be required for better imaging of the bone immediately beneath the skin. It is important to perform a thorough examination of all the bony structures in case there are fractures in other regions of the pelvis.
Fractures of the Ilial Wing
Fractures of the ilial wing appear to be among the most commonly encountered type of athletic stress fractures in the skeletally immature TB racehorse.17-20
Clinical Signs
A horse with a complete ilial wing fracture often shows lameness, but the initial lameness varies from lame at the walk to grade 1 to 4 of 5 at the trot. Lameness often resolves rapidly within 24 to 48 hours, and the horse then has a slight gait abnormality, walking with the back hunched up, but with no overt lameness. A horse with an ilial wing fracture often plaits with the hindlimbs at the trot and has a shortened stride . Although a complete fracture may be present on only one side, evidence of a subclinical stress fracture in the same site on the contralateral limb is common, and this may contribute to the peculiar gait shown by the horse. Obviously, pain from both sacroiliac joints considerably affects the freedom of movement of the hindlimbs. A horse with bilateral lesions may appear to have signs of exertional rhabdomyolysis, but plasma creatine kinase levels are often normal or only slightly increased (500 to 1500 IU/L).
. Although a complete fracture may be present on only one side, evidence of a subclinical stress fracture in the same site on the contralateral limb is common, and this may contribute to the peculiar gait shown by the horse. Obviously, pain from both sacroiliac joints considerably affects the freedom of movement of the hindlimbs. A horse with bilateral lesions may appear to have signs of exertional rhabdomyolysis, but plasma creatine kinase levels are often normal or only slightly increased (500 to 1500 IU/L).
Incomplete fractures may occur on one or both sides, and this can often show as poor propulsion and a poor hindlimb action rather than overt lameness. In a horse with a complete fracture, ventral displacement of the ipsilateral tuber sacrale is often apparent and can be detected by careful digital examination of the midline of the spine and both tubera sacrale. Firm pressure in the previous site of the tuber sacrale often evinces a marked pain response, with associated muscle spasm over the sacroiliac joint region. Palpating the tip of the tuber sacrale in its ventrally displaced position is sometimes possible. Often fairly profound muscle wastage is associated with this injury in the first 2 weeks, and this contributes substantially to the apparent asymmetry of the horse when viewed from behind. Bilateral complete fractures lead to profound stiffness, unwillingness to walk, and boarding of the muscles of the pelvis in response to digital manipulation. They can lead to collapse and inability to rise, with substantial neurological deficits in severe injuries.
Scintigraphic Examination
Scintigraphy usually reveals marked focal IRU associated with the ilial wing, usually 10 to 15 cm from the midline (Figure 49-4). IRU may be bilateral or unilateral. A clear fracture line and the displacement of the ilial wing are sometimes visible. The lateral oblique image16 is particularly useful in determining whether the fracture extends to the cranial and caudal cortices of the ilial wing, although masking of the normal greater RU associated with the tubera coxae, caused by lack of attenuation of the gamma rays by overlying muscle as the bone approaches the skin surface, may be needed to highlight these changes (see Figure 49-4, B).
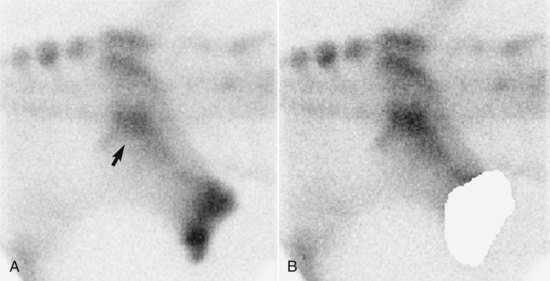
Fig. 49-4 A, Dorsal lateral oblique delayed (bone) phase scintigraphic image over the right side of the pelvis of a horse with a stress fracture of the ilial wing. Cranial is to the right. Focal increased radiopharmaceutical uptake (IRU) (arrow) appears about one fourth of the way between the tuber sacrale and tuber coxae, the most common predilection site for stress fractures of the ilial wing. Masking of areas of apparent greater RU, which are the consequence of normal bone with little attenuating soft tissue cover (tuber coxae), allows better recognition of the pathology otherwise obscured by “count capture” (B).
(Courtesy Animal Health Trust, Newmarket, U.K.)
Ultrasonographic Examination
The normal ultrasonographic appearance of the ilial wing is a smooth and regular concave hyperechoic line, extending between the tuber sacrale and the ipsilateral tuber coxae. Acoustic shadowing and refraction artifacts can be created by the many blood vessels within the musculature and must not be confused with disruption to the bone contour. Ilial wing fractures appear as a disruption to the ilial wing contour, with changes ranging from a clear fracture gap to small irregular echogenic areas on the dorsal surface, representing prodromal periosteal new bone formation. The fractures normally run sagitally and involve the bone dorsal to or in proximity with the sacroiliac joint. The bone abnormalities often appear more severe toward the caudal margin of the fracture. Sometimes hemorrhage at the site of fracture appears as an anechoic defect in the normal heterogeneous echogenicity of skeletal muscle (see Figure 49-3, A).
Fractures of the Ilial Shaft
The ilial shaft is a common site for fracture after a fall or as a spontaneous athletically induced injury.
Clinical Signs
Fracture of the ilial shaft is extremely painful, producing non–weight-bearing lameness, and is often associated with shock from extreme pain and rapid blood loss. The tubera coxae often are markedly asymmetrical when viewed from behind, although encouraging the horse to bear weight equally to allow this examination to be carried out can be difficult. Sometimes with incomplete or minimally displaced fractures, no displacement of the tuber coxae is apparent initially, but in these horses the pelvis often collapses early in convalescence, at which time asymmetry becomes obvious. Collapse of the pelvis can often make the fracture less painful for the horse for reasons that are unclear. Rectal examination is often useful, and gentle rocking of the horse while the arm is inserted in the rectum often allows clear crepitus to be felt with the fingertips on the ilial shaft of the affected side. A hematoma next to the fractured ilium can also be easily palpated in many horses. Not uncommonly, horses damage the iliac arteries with the sharp edges of the comminuted fracture fragments, and this can result in severe and sometimes fatal hemorrhage.
Horses usually do not resent palpation and flexion of the distal aspect of the limb, although forced abduction of the limb, including the hock and stifle, may elicit a painful response. Palpation of the hindquarters usually results in intense muscle spasm and guarding on the affected side. Bizarre consequences of the severe lameness and change in functional anatomy after some of these fractures are not uncommon and include permanent upward fixation of the patella, contracture of the hamstring group of muscles, and spastic hyperextension of the tarsus. These complications invariably result in a grave prognosis.
Scintigraphic Examination
Many horses are too lame to allow transport to an equine clinic for scintigraphic examination, and a combination of clinical signs and ultrasonographic findings can establish the diagnosis. If scintigraphy is performed, a caudal oblique image is often extremely useful in illustrating the extent and nature of the fracture. Because pelvic anatomy is directly visible on a scintigraphic image, the displacement of the fracture fragments and ilial wing is often easily appreciated.
Ultrasonographic Examination
The ilial shaft is examined by aligning the ultrasound beam in a craniocaudal direction and following the ilial shaft from the flat surface of the ilial wing toward the greater trochanter of the femur. With ultrasonography, a displaced ilial shaft fracture is easily detected as a discontinuity to the bone surface. Passive movement of the limb may show independent movement of the fracture margins in real-time scanning. Hypoechogenic areas may be present around the fracture line and represent hemorrhage into the musculature. As with other fractures, if displacement is minimal, an ultrasonographic examination may fail to detect any pathological condition.
Fractures of the Pubis and Ischium
Discrete fractures of the ischium are relatively uncommon. The horse usually has unilateral lameness with obvious swelling over the caudal aspect of the thigh. A fall or rearing over backward is often noted in the history, but these fractures can also develop as a spontaneous athletic injury. Often palpable crepitus and a marked pain response on firm digital pressure to the site are apparent. The tail may be held to one side because of muscle spasm associated with the painful lesion. Often focal sweating occurs on a patch of skin on the back of the thigh, presumably resulting from nerve damage. With time, the acute swelling subsides, and a “caved-in” appearance of the caudal aspect of the upper thigh may develop when viewed from the side.
Fractures of the pubis are uncommon and usually only encountered with other multiple pelvic fractures or after a fall.
Scintigraphic Examination
Scintigraphy shows focal IRU associated with the ischium and sometimes clear displacement of a segment of bone. Isolated fractures of the pubis can be difficult to see because of the mass of bone and muscle interposed between the fracture site and the gamma camera. For this reason, a hand-held probe, used per rectum, can give useful information. A bladder artifact produced by delayed excretion of urine may give the appearance of an IRU in this site.
Ultrasonographic Examination
The pubis is the least rewarding of the pelvic bones to examine by ultrasonography. A rectal probe is required, and only marked changes are detectable. The ultrasonographic examination is limited by the small degree of probe movement that is possible within the rectum, coupled with the irregular normal contour of the bone at this site.
Part of the ischium is also examined internally using a rectal transducer. This approach may be the only way to detect any ultrasonographic changes associated with an acetabular fracture. The caudal-most portion of the ischium and the ischiatic tuberosity can be examined percutaneously. Normally a smooth concave contour extends caudally from the greater trochanter of the femur. Ultrasonographic changes similar to those described in other sites where bone damage has taken place can be seen in this area. Comparing the contralateral ischium with the fractured one is useful.
Fractures Involving the Acetabulum
Horses with fractures of the ilial shaft and ischium that involve the acetabulum have the poorest prognosis of all for return to athletic function as a racehorse and normally develop osteoarthritis (OA) of the coxofemoral joint, which results in permanent and progressive lameness. Acetabular fractures commonly result from trauma, often subsequent to slipping over or being cast. This is one of the more frequent causes of lameness in a horse found not bearing weight on a hindlimb in the stable or paddock, with no obvious inciting cause.
Clinical Examination
The horse is extremely lame and is often unwilling to move. The horse has extremely short protraction of the hindlimbs at the walk and often hops rather than attempting to bear weight. Both Editors have observed that horses willing to walk with fractures or severe OA of the coxofemoral joint often have a shortened caudal phase of the stride, differentiating this area of pain from many others in the hindlimb. Pain occurs on abduction of the limb, and often firm palpation of the muscle mass around the coxofemoral joint causes muscle spasm and pain. Crepitus may be felt with displaced fractures if the hand is applied to the greater trochanter of the femur while the horse is walked, although commonly these fractures are incomplete and crepitus is not apparent. Crepitus may also be felt if the horse is rocked during rectal examination with the hand on the pelvic brim. In horses younger than 2 years of age, separation of the femoral head can occur from trauma and produces similar clinical signs to a comminuted acetabular fracture.
Scintigraphic Examination
Scintigraphic examination reveals focal IRU associated with the coxofemoral joint, greater trochanter of the femur, and ilial shaft on the affected side. The IRU is particularly visible on a caudal oblique image in which both coxofemoral joints can usually be seen using a large field of view gamma camera. OA of the coxofemoral joint contributes substantially to IRU in horses with a chronic fracture. These fractures are not associated with intense focal IRU initially, and early examination may give false-negative results. At least 1 week is required before scintigraphic abnormalities are detectable, and often this time period is necessary to allow humane transport of the horse. If the clinician is doubtful, the scan should be repeated 14 days later, when bone uptake will be maximal.16 Separation of the femoral head, which occurs infrequently in yearlings usually after a fall, produces similar scintigraphic changes, with moderate IRU associated with the coxofemoral joint.
Ultrasonographic Examination
Because of the great depth of the acetabulum and the many changing bone contours, the acetabulum is probably the most difficult area of the pelvis to image by ultrasonography. Subtle pathological conditions may well be missed. The greater trochanter of the femur provides a good landmark by which to orient the image. The normal acetabular region is represented as a smooth and regular hyperechoic line of the acetabular rim. The greater trochanter of the femur is close to the skin surface as a hyperechoic line extending down and toward the acetabular rim. In some horses, a hypoechogenic region represents the joint space. In foals and immature animals, a hyperechoic convex line extends from the greater trochanter and represents the femoral head.
A fracture can appear as a discontinuity or irregular roughening of the acetabular rim and will be particularly obvious if greater degrees of callus are present.
Principles of Treatment of Horses with Pelvic Fractures
Surgical repair of pelvic fractures is not currently a realistic option in the adult horse. The period of box rest required for bony union ranges from 2 to 3 months, judged by monitoring fracture healing with ultrasonography. The end result in terms of the functional anatomy of the pelvis depends on the degree of displacement in the initial insult and the extent of subsequent distraction of the fracture fragments by subsequent muscle contracture. For example, tuber coxae fracture fragments heal by becoming adherent to the cranial wing of the pelvis through fibrous union. Despite the fact that the position of the tuber coxae often changes by several centimeters and the tuber coxae comes to rest in the sublumbar fossa, many horses make a full return to athletic function and race with success. Fractures of the sacral wing of the ilium are often nondisplaced and can make an extremely good, smooth bone union after healing (see Figure 49-3). Often an abnormal angle is apparent on the ilial surface because of distraction of the fragments by muscle contraction before healing. Although the abnormal angulation of the pelvic blade cannot help the stability of the sacroiliac joint immediately beneath the fracture, many affected horses go on to train and race successfully. In a review of 20 horses with ilial fractures, 15 horses made a full recovery to advanced race training, and 11 of these raced successfully.6 Involvement of the ilial shaft considerably worsens the prognosis for racing, although many heal adequately to allow retirement to stud. Some general principles of the care and management of horses apply equally to the different types of pelvic fractures and can be outlined as follows:
Horses should remain tied up for no more than 1 month. Many horses cope with being tied up without problems, but while they are tied up, horses should be fed from the floor several times a day and be held by an attendant while they eat. This encourages drainage of bronchial secretions from the trachea and may help to prevent pleuritis and pleuropneumonia, which can develop with prolonged periods of being tied up.21 During the period that NSAIDs are administered by mouth, any increase in rectal temperature will be masked. For this reason it is vital to take regular (every 48 hours) blood samples to assess changes in white blood cell count, serum amyloid protein A (SAA), and fibrinogen level, which may signal an early onset of pneumonia or pleuritis. Subsequent to NSAID therapy, rectal temperature should be monitored twice daily. When a horse is untied after 1 month, the fracture fragments possibly still can displace, leading to fatal hemorrhage. However, displacement is rare, and the clinician must balance the potential risk to the horse against the humanitarian aspects of keeping a horse tied up continuously for more than 1 month. Although I feel strongly about tying up horses with pelvic fractures, others feel differently, and many horses with pelvic fractures have been managed successfully without being tied up.
Careful thought should be given to each individual horse to make sure that the horse’s future is worthwhile, in terms of quality of life for the horse and the economic realities of the situation, before subjecting a horse to a prolonged and, by necessity, painful convalescent period.
Prognosis in foals with acetabular fractures is considerably better than in adult horses. Treating a foal with an acetabular fracture is definitely worthwhile because at this age the pelvis appears capable of healing with much less chance of the development of OA in the coxofemoral joint when compared with adult horses. Foals are treated with 12 weeks of box rest initially and progressive turnout in a nursery paddock.
Separation of the femoral head in a young horse carries a hopeless prognosis and, if confirmed, should lead to immediate euthanasia.