Chapter 58Angular Limb Deformities
 Diagnosis and Conservative Management
Diagnosis and Conservative Management
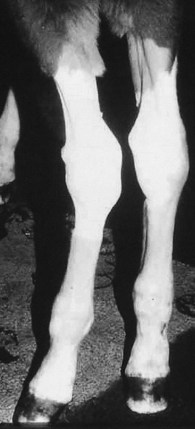
Angular limb deformities are considered lateral or medial deviations to the long axis of the limb in the dorsal (frontal) plane. A lateral deviation distal to the carpus, termed carpus valgus, is the most common. Tarsus valgus and fetlock varus (a medial deviation) are the next most common, respectively. The toed-in or toed-out appearance that often accompanies an angular deformity is a concurrent rotational deformity and should not be confused with the angular deformity. An outward (external) rotation is usually observed concurrently with a valgus deformity, and an inward (internal) rotation is seen with a varus deformity. No confirmed breed or sex predilection is known, but subjectively there may be some genetic predisposition. For a foal to be born with a mild bilateral carpal valgus and toed-out appearance is considered normal by most clinicians, and as the foal grows and the chest widens, the limbs straighten progressively.
Angular limb deformities usually are congenital, but they can be developmental, and have numerous causes. An acquired angular deformity is defined as worsening or failure of correction of the normal slight carpus valgus conformation in a neonatal foal. The cause and the severity and progression of the deformity are vital pieces of information that should be acquired before a treatment plan is formulated. Treatment is predicated by these factors. Foals are like molding plastic. The conformation changes slowly with growth. Genetics, nutrition, amount of exercise or weight bearing, and veterinary interventions all influence the conformation of the adult horse. Some of these factors can be influenced as a young horse matures, and small adjustments often need to be made to the treatment plan as the animal grows. The foal should always be evaluated with the amount of remaining growth in mind and not just its present status. Because the greatest impact on conformation is made during periods of rapid growth, early recognition and regular reevaluations are extremely important to achieve a positive outcome.
Growth rates are most rapid in the neonate and slow considerably within the first year. Most of the growth from the distal radial and tibial physes occurs within the first 6 months of age. Most of the growth from the distal aspect of the third metacarpal bone (McIII) and the third metatarsal bone (MtIII) occurs within the first 3 months of age. Minimal changes take place beyond these times. Radiology alone cannot be used to determine the end of bone growth, because a physis is radiologically apparent long after clinically relevant growth has abated. In a normal foal, carpus valgus should be corrected to within 5 to 7 degrees of normal by 4 months of age and should be almost straight by 8 to 10 months of age.
Examination of the Foal
It is critical to determine the extent and cause of the deformity before developing a management plan. Foals should be examined while they are standing and walking and radiographically. Occasionally foals are assessed in lateral recumbency.
Deformities can be assessed subjectively by visual examination. The foal should stand as squarely as possible, with the foot directly below the proximal part of the limb. Deviations from this stance exacerbate any deformities that truly exist. Because most foals stand still only transiently, repositioning the foal several times to evaluate each limb independently is often necessary. This allows observation of how the foal stands most frequently in a relaxed position. The clinician stands directly in front of the dorsum of the long bones for evaluation of the forelimbs, not necessarily at the front of the toe. The orientation of the toe may be affected by a concurrent rotational deformity, which confounds interpretation. Hindlimbs should be evaluated similarly but directly from behind. The forelimbs can also be evaluated by standing shoulder to shoulder with the foal, looking down the limb toward the ground.
All limbs also should be evaluated with the foal walking away from and toward the clinician. Breakover is determined for each foot, which may be helpful in deciding the most appropriate way to manage the foal. The entire assessment of a foal should be graded and recorded on video or on paper for future reference.
Radiology provides an objective assessment of angular deformity, but sequential radiographic examinatoins may be unreliable if the obliquity varies. Differences in radiographic projection can result in a misinterpretation of worsening or improvement, which is particularly true when trying to quantify small differences in the angle. Long, narrow (18 × 43 cm) cassettes should be used to measure the angle of the deformity, by evaluating the intersection of a line representing the long axis of the proximal and distal aspects of the long bones from the joint in question. This is more accurate in the carpus and fetlock than in the tarsus. Radiology is essential to identify cuboidal injury or malformation. Such a deformity dramatically worsens the foal’s prognosis. Foals with angular deformity resulting from cuboidal bone abnormalities usually have compromised range of motion, but this often is detected best with the foal in lateral recumbency.
Periarticular Laxity
Periarticular laxity is the major cause of congenital angular limb deformities and often improves dramatically within the first 4 weeks of life, without any intervention, as the periarticular tissues become less elastic. The improvement is most dramatic in a windswept foal, which has a tarsus valgus of one limb and a concurrent varus of the other. Limited exercise is all that is required for these foals to become normal.
Infrequently the deformity can be so severe, particularly in the fetlock, that the foal is unable to bear weight on the sole of its foot. Immediate treatment is required to establish normal weight bearing. Custom-made glue-on shoes are particularly useful to prevent abnormal breakover and to keep the foot flat on the ground. If the foal has excessive laxity of the lateral collateral ligaments and a tendency to break over on the lateral side of the foot, a lateral extension shoe is used to maintain appropriate alignment of the limb. The foal should initially be restricted to a stall before turnout in a small paddock or round pen with just the mare. Soft tissues become progressively stronger, and normal activity can be permitted within a relatively short time. Allowing premature excessive exercise can lead to proximal sesamoid bone fractures (see Chapter 36) and other injuries. Glue-on shoes are usually required for several weeks, but they then should be removed to prevent contracture of the foot. External coaptation also should be avoided if possible. Splints are used only to maintain joint alignment if absolutely necessary. Splints are contraindicated to try to pull or push a limb straight. Rigid support from a splint or cast usually leads to greater soft tissue laxity. Trying to support a limb results in continued laxity and soft tissue wounds from bandaging. Every foal must be managed on an individual basis with the goal of achieving normal weight bearing and function while providing the minimal amount of support necessary.
Asymmetrical Physeal Growth
Asymmetrical growth of a distal physis is a cause of angular limb deformity. Greater growth from the distal physis of the radius medially compared with growth laterally results in carpus valgus. Continued asymmetrical growth precludes the normal correction anticipated with resolution of periarticular laxity. Greater growth from the lateral aspect of the distal physes of the McIII or the MtIII results in fetlock varus. With time and limited exercise (stall or small paddock turnout, alone with the mare) substantial self-correction occurs for most foals with angular deformities. Radiology can be used to evaluate objectively the degree of deformity and the difference in physeal growth, but it is not always required.
Fetlock varus is often overlooked and affects the left hind fetlock most commonly, possibly because of in utero positioning. Because growth at the distal physis of the McIII and the MtIII terminates within a few months, early recognition of this deformity is critical.
Trauma-Related Deformities
Developmental causes of angular deformities are likely secondary to excessive or asymmetrical weight bearing and can be more serious than congenital abnormalities. Incomplete ossification of the cuboidal bones in a foal can result in cuboidal bone crush and a secondary angular limb deformity. The lateral carpal bones most commonly are affected, resulting in carpus valgus. Although the deformity is clearly apparent, the health and function of the joint is most critical. The carpi and tarsi of any premature or dysmature foal should be examined radiologically. Because ossification is incomplete, abnormal cuboidal bones appear round or in other shapes, and if crushing exists, the bones are wedge shaped, overlap opposing bones, or are fractured. If the foal’s activity can be managed strictly in a hospital situation, no further support is recommended. Limited, strictly controlled exercise encourages appropriate ossification. If the foal’s activity cannot be strictly managed and the foal has moderate strength, sleeve casts are recommended to prevent cuboidal bone crush. Sleeve casts should be changed or removed in 10 to 14 days in a growing foal. Radiological reevaluation every 2 weeks helps determine the length of time a cast is required.
Foals can also develop angular limb deformities secondary to lameness in the contralateral limb. If foals become non–weight bearing on a single limb, they adopt a tripod-like stance by bringing the contralateral limb more medial and toeing in. Over several weeks this results in asymmetrical bony growth of the nonlame limb and varus deformity of all joints, with internal rotation of the distal aspect of the limb. A dorsolateral toe extension can be placed on the foot of the nonlame limb to try to encourage a more abducted stance, but resolution of the primary lameness is the best way to prevent the contralateral limb deformity from occurring. Once the deformity has occurred, correction is improbable.
Conservative Management
In most situations, judicious minimal intervention is all that is required to correct angular limb deformities. This includes limited small paddock exercise and careful attention to the foot. Trimming the foot and using shoe extensions can influence a foal’s ability to self-correct an angular limb deformity by affecting the weight bearing and tracking of the limb. A foal younger than 4 months of age with mild carpus valgus likely requires no specific intervention. A foal with a moderate carpus valgus, toed-out appearance would benefit from shoes with dorsomedial extensions. This encourages the foal to adduct the limb and turn in more when breaking over. The result is more physiologically normal strain on the limbs, which should result in a straighter limb. A similar external appearance can be achieved by overtrimming the lateral hoof wall, but the effect is not the same. Although trimming the foot in this manner may give the appearance of an immediate benefit, it may have a negative long-term effect of an unbalanced foot, compensating for a limb with a deformity. This method has, however, been used for years with apparent success.
More aggressive intervention is infrequently required. Surgical intervention should be reserved for those foals that are not improving fast enough for the amount of growth potential remaining. Therefore frequent reevaluation to monitor progress of a foal with an angular limb deformity is critical. Surgical intervention has a greater effect on a young foal because of the more rapid growth; thus early surgical intervention should be considered for a foal with a severe deformity.
Surgical Management
A high proportion of foals with angular limb deformities are treated successfully conservatively, but surgical intervention is warranted if a deviation is severe or if deformity persists despite adequate management, including restriction of exercise and corrective farriery. Various surgical techniques aimed at accelerating or decreasing the growth on a particular side of the growth plate have been described.1-7 Surgical technique depends on the age of the foal, the degree of angular limb deformity, the anatomical site, and whether the deformity is varus or valgus (Figure 58-1).
Before surgery, all the limbs should be assessed from the front, from the back, and while standing next to the limbs. Good-quality radiographs, which include a substantial length of the bones proximal and distal to the deviation, should be obtained to assess bone structure (Figure 58-2) and to determine the pivot point and pivot point angle of the deviation. The pivot point is the intersection of two lines drawn parallel to the long axis of the bones proximal and distal to the articulation in question (Figure 58-3). The pivot point indicates the origin of the deviation and helps to determine whether the cuboidal bones, in the case of the carpus and tarsus, are involved in the deviation, or if deviation is caused by disproportionate physeal growth only. Abnormalities in the structure of these bones can have a substantial influence on the effect of the procedure and the future athletic potential of the horse. The pivot point angle is the angle formed by the intersection of these two lines and indicates the severity of the condition.8

Fig. 58-2 Dorsopalmar radiographic image of a carpus with mild incomplete ossification of the carpal bones and valgus deformity. Medial is to the right.

Fig. 58-3 Dorsopalmar radiographic image of a carpus with valgus deformity. Lateral is to the right. Lines are drawn parallel to the long axis of the radius (A) and third metacarpal bone (B). The point at which these lines intersect is known as the pivot point (PP), and the angle between them is the pivot point angle (PPA).
Hemicircumferential periosteal transection and elevation, or periosteal stripping, aims to accelerate growth on the concave side of the limb, laterally for valgus and medially for varus deformities.1 Previous work on chicken radii had shown that a circumferential division of the periosteum, rather than a longitudinal one, resulted in increased bone growth. The proposal was that the periosteum functioned as a fibroelastic tube that spanned the diaphysis, provided an even tension between both epiphyses, and was responsible for the regulation of growth.1,9 A horizontal or circumferential division of the periosteum would result in a release of tension at the level of the growth plate, resulting in the induction of new bone production on the side of the division.
The procedure has been thoroughly described.4-6 Hemicircumferential periosteal transection and elevation is performed with the foal in lateral recumbency under general anesthesia, with the concave side of the affected limb uppermost. If the procedure is going to be performed bilaterally, dorsal recumbency is recommended. The position of the physis is identified using a 20-gauge needle. For a carpus valgus deformity, a 4- to 6-cm longitudinal incision is made between the common and lateral digital extensor tendons starting just proximal to the medial physis. The incision is extended through to the periosteum. Using a curved scalpel blade (No. 12), a horizontal incision is made 1 to 2 cm proximal and parallel to the physis, at the distal end of the initial incision (parallel to the skin incision), forming an inverted T. The periosteal flaps are elevated with the aid of a periosteal elevator and then allowed to return to the normal position. It is important to transect the remnant of the ulna, or if the ulna is ossified, it should be removed with the aid of rongeurs. In foals with hindlimb tarsus valgus the veterinarian should bear in mind that a fibular remnant may be present. The incision is closed routinely and the area is bandaged for 10 to 14 days. The foal is kept in a large stall or small paddock until the deformity has been corrected.
Hemicircumferential periosteal transection and elevation has been reported to exert its effects for up to 2 months, but the procedure can be repeated if further correction is needed.4 There are no reports of overcorrection of the deformity, although one of the Editors (MWR) is aware of a few foals in which transphyseal bridging techniques on the opposite of the limb were necessary after hemicircumferential periosteal transection, giving the distinct appearance that overcorrection occurred. Early reports suggested an approximately 80% success rate1,3; however, more recent work indicates less favorable results.10-12 A large retrospective study in Thoroughbred racehorses investigated racing performance after hemicircumferential periosteal transection and elevation.10 A lower percentage of treated horses were able to start a race and had a lower starts percentile ranking number compared with half-siblings. Most of the foals appeared to respond favorably to hemicircumferential periosteal transection and elevation based on external appearance of the limbs, but preexisting conditions, such as abnormal cuboidal bone formation from incomplete ossification or osteoarthritis secondary to abnormal loading of the limb before correction, may have influenced subsequent performance.
The technique of physeal stimulation, a modification of hemicircumferential transection and elevation, was reported to be successful.13 Briefly, a needle is inserted into the physis on the concave portion of the limb (for example, the distal lateral aspect of the radial physes for foals with carpus valgus limb deformity) and numerous needle punctures are made into the physis, but deep to the periosteum, in a fan-shaped fashion.13 I have no experience with this technique.
Angular limb deformities are probably the most common orthopedic problem affecting Thoroughbred foals.1014 Early surgical intervention was previously recommended to take maximum advantage of the growth potential of the physis, to try to provide foals with excellent conformation, and to enhance sale value and possibly potential performance. Based on current knowledge, it now seems likely that a large number of foals with mild angular limb deformities underwent unnecessary surgery. The reported success for correction of angular limb deformities, particularly in the carpus, after hemicircumferential periosteal transection and elevation has been recently challenged. Foals with carpus valgus that underwent hemicircumferential periosteal transection and elevation were no more likely to improve than were those managed with stall rest and corrective farriery.11,12 Although the efficacy or need to perform hemicircumferential periosteal transection and elevation when treating foals with mild to moderate carpus valgus deviations is a matter of current debate, the same cannot be said necessarily for other regions of the limb, such as the tarsus and fetlocks, without further investigation.
Transphyseal bridging is performed on the convex side of a deformity to decrease the growth rate on that side of the physis. Traditionally, transphyseal bridging has been performed in young foals with severe deformities or in foals in which most of the growth in a particular physis has subsided. Transphyseal bridging has been performed successfully using cortical screws with cerclage wire in a figure eight, with a small dynamic compression plate, or with orthopedic staples.4-6
The foal is positioned in lateral recumbency under general anesthesia, with the convex side of the affected limb uppermost, or in dorsal recumbency. The position of the physis is identified and checked radiologically using a 20-gauge needle inserted into the physis. Stab incisions are made for placement of cortical screws and cerclage wire; one incision is made in the center of the epiphysis and the other approximately 2 cm proximal to the physis. Once the subcutaneous tissues between both incisions have been bluntly dissected, a 4.5- or 3.5-mm cortex screw is placed through each incision, slightly angled toward the physis. Screw size depends on the size of the foal, but 4.5-mm screws are preferred. Before complete tightening of the screws, a loop of 18-gauge wire is fed through the proximal incision and positioned around the distal screw head. The wire is then tightened over the proximal screw head, forming a figure eight. Once the wire has been tightened, the screws are tightened and the incisions are closed routinely. When performing this procedure in the distal aspect of the tibia, the clinician should be aware of the contour of the tarsocrural joint, because placing the epiphyseal screw into the joint is possible. The screw should be angled more sharply toward the physis than in the distal aspect of the radius. Postoperatively the foal should be kept in a large stall and monitored closely. Follow-up radiographs are strongly recommended to assess the amount of correction. Prompt removal of the implants is essential, because overcorrection of the deformity is possible.
A surgical alternative to transphyseal bridging has been described and is currently known as the transphyseal screw technique.4,7 A single screw, either 3.5 mm or 4.5 mm in diameter, is inserted in neutral fashion across the growth plate through a small stab incision in order to create the desired compression on the convex side of the deformity, as with transphyseal bridging (Figure 58-4). This technique has been successful in achieving adequate correction of angular limb deformities, with the advantage of a better cosmetic result. Postoperative care for horses treated with a transphyseal screw is similar to that for transphyseal bridging. Prompt removal of the screw just before correction is achieved is encouraged because overcorrection is possible and there is a lag phase between screw removal and continued growth on the operated side.

Fig. 58-4 Dorsoplantar radiographic image of a tarsus with valgus deformity after a transphyseal screw procedure.
In foals and young horses with an angular limb deformity that persists after physeal closure, corrective ostectomy or osteotomy can be performed. A step ostectomy (sagittal plane) or step osteotomy (dorsal plane) is preferred to a closing wedge ostectomy, because limb length is preserved and interfragmentary compression between the bone pieces is better.4 These techniques are generally considered to be salvage procedures.
Tarsus valgus deformities frequently go unrecognized by both owners and veterinarians, possibly from lack of observation of the foal from behind and the inherent offset position of the tarsus.15,16 Early recognition and sometimes more aggressive surgical management of tarsal angular limb deformities are critical to achieve satisfactory results. Although the distal tibial physis has a tremendous growth rate until 4 months of age, foals younger than 2 months of age responded more favorably to hemicircumferential periosteal transection and elevation than older foals. Transphyseal bridging was more effective than hemicircumferential periosteal transection and elevation, especially in foals older than 2 months of age.15 This is a substantial change from the previous perception that hemicircumferential periosteal transection and elevation alone were adequate when managing most tarsus valgus deformities in foals 4 to 6 months of age. Early recognition of incomplete ossification of the tarsal bones (Figure 58-5) is crucial, because the condition, if unrecognized, leads to collapse of the third or central tarsal bones, resulting in osteoarthritis.15,16 Of 22 foals with incomplete ossification of the tarsal bones, 73% had tarsus valgus deformities. Only 32% of the foals were able to achieve the intended use.16
