Chapter 113The Finnish Horse and Other Scandinavian Cold-Blooded Trotters
History of the Breeds
The Finnhorse is the only original horse breed in Finland. Sweden and Norway also have similar cold-blooded breeds. The Finnhorse has been known for about 1000 years and originally was used for farm and forest work and in the army. The Stud Book of the Finnhorse was founded in 1907 for draft and carriage horses but is now divided into four parts for racing trotters, riding horses, draft horses, and small pony-type horses. Seventy-five percent of the registered Finnhorses are trotters. The Finnhorse is heavy and well muscled, with a short neck and usually a heavy head. The average height is 155 to 160 cm, but pony-sized Finnhorses exist. Swedish and Norwegian cold-blooded horses are slightly lighter and smaller than Finnhorses, with an average height of 150 to 160 cm.
Trotting competitions are the main use of Finnhorses. In Scandinavia all harness races are for trotters; there are no pacing races. The first records of trotting races are from 1817, when races were arranged on the ice of the river Aura in Turku. The first races with official timing took place in 1862 in Viipuri. In the early years the trotting races were arranged by the state to support and develop horse breeding in Finland. In the first races the distance was 2138 m, and they were on a straight track. The horses raced individually, and prizes were given according to the times. The first official Finnish record was from 1865 by the mare Brita. The average time for 1000 m was 1.51.3 (1 minute 51.3 seconds, equivalent to a mile in 2 minutes 59 seconds). Today the record is held by Viesker and is 1.19.9 (2:08.5). Betting was first introduced in 1928 but developed slowly until the 1960s, after which rapid growth followed.
In Sweden, racing also was started in the early nineteenth century on roads and icetracks. The first permanent tracks were built in the early twentieth century. The first official record in Sweden was in 1829, 1.37.6 (2:37), held by a Norwegian horse, Sleipner Varg. Today the record is 1.17.9 (2:05) by a Swedish stallion, Jarvsofaks. When racing became more popular, Swedish and Norwegian horsemen started trading horses across the border, and the Swedish and Norwegian breeds began to merge together. Today the breeds are genetically alike, and they now are considered to be the same breed. Sweden and Norway have a close collaboration in breeding and racing, and their horses race in the same races.
Today the races are held at modern dirt tracks, and in the same events there are separate races for Finnhorses and Standardbreds (STBs). The Finnhorses are allowed to race first at the age of 3 years, but not uncommonly they start racing as late as 5 or 6 years of age. They are allowed to race until 16 years of age, and a Finnhorse usually is considered to be best from 7 to 10 years of age. Some stakes races are held for 4- and 5-year-olds, but the main events are for older horses. The biggest event for Finnhorses is the Kuninkuusravit, the Royal Trot, which is held annually in July or August at a different track in Finland each year. The race is one of the major sporting events in Finland, attracting about 50,000 people. Separate races are held for mares and stallions; geldings are excluded. To be allowed to race in the Kuninkuusravit, the horse has to be approved for public breeding and has to be entered in the Stud Book, which requires inspection and approval by a special board. The horses race three times in 2 days over distances of 1609 m, 2100 m, and 3100 m, and the final result is based on the total time for all three races. To win the royal title is the greatest honor a Finnhorse can ever achieve; the best stallions have won the title five times (Vieteri, Vekseli, and Viesker), and the best mares, four times (Suhina and Valomerkki). This is good proof of stamina and endurance, which are typical for the Finnhorse at its best.
In Sweden and Norway horses usually start racing at 3 years of age and are allowed to race until the age of 15. Stakes races are open to Swedish and Norwegian horses, and big races are held for 3- and 4-year-olds and for older horses. Finnish horses are not allowed in these races, and only a few races are held in which all Scandinavian horses race together.
Training a Cold-Blooded Trotter
Traditionally the horses have been bred and trained by farmers, and many remain home bred and trained. There are no sales for Finnhorses, Swedish, or Norwegian trotters. Most horses are broken at 2 years of age, spend the next summer at pasture, and then start more serious training in the winter at 3 years of age, often with a summer break. Farm and forest work has historically been part of the training to build up strength. Speed work is not done at all at this stage, and traditionally some trainers have never used speed work. Horses started racing at 5 to 6 years of age and raced themselves to condition. However, many professional trainers now train cold-blooded horses, and the horses are better prepared for the races and start racing younger. The race times for the beginners are faster, which has caused problems for many old-school trainers. Many Finnhorses are not natural trotters, and building them up to speed takes time and training. If fast speeds are demanded too early, gait abnormalities develop at higher speeds, and horses lose complete control of the trotting action while appearing sound at a slower trot.
Training cold-blooded trotters takes much more time than for STBs, making training more expensive and leading to problems in getting new owners and trainers. In all Scandinavian countries, fewer cold-blood races are held than STB races, and they are concentrated in the north. Nonetheless, cold-blood racing is supported by the central racing organizations of each country and continues to thrive.
Racetracks and Weather Conditions
The racetracks in Scandinavia are 1000-m oval dirt tracks, and the horses race counterclockwise. The climate is cold in the winter, and the tracks freeze and get covered by snow (Figure 113-1). In winter temporary tracks also are made on ice for smaller races with no betting. The variable climate causes track problems. In late autumn when the track is frozen but not yet covered by snow, the surface can be treacherous. Snowfall makes the tracks smooth but not hard, and provided the horse is shod properly, the track is not slippery. In the springtime, when the snow begins to melt, the track conditions vary throughout the day, being hard in the morning after a night frost, becoming good for a few hours when the frost melts, and then becoming wet and soft the rest of the day. Keeping the track in good condition requires much skill.

Because of the long winter, much of the training has to be done on snowy or icy surfaces. Snow is a good surface on which to train a horse, but special shoeing with studs is essential so that the horses do not slip. In the winter many trainers do much of the speed work in snow, which can be deep. The training speeds can be lower because of the resistance, but the training effect is equal or even better than when the training is done on the track. Snow provides a soft and smooth surface, acting as a shock absorber. Many horses with lameness problems race better in winter because of the training in snow. Horses also are trained on the ice of lakes, which is also a good surface. The surface of the ice gives slightly, and shoes with studs can get a good grip. The worst training surface is ground that is frozen hard like asphalt; this type of surface causes many lameness problems.
Shoeing Considerations
In the winter (November to April) special requirements for shoeing are needed to prevent the horses from slipping on ice. Studs, 5 to 15 mm in length with sharp tips that offer a good grip on the ice or snow, are screwed into the shoes. Four to 15 studs are used per shoe; more studs usually are used in the hind shoes. It is important to have enough studs for the horse to avoid slipping slightly at every step, causing joint and muscle soreness. A risk of interference injuries exists, and some horses with poor action cannot race in the winter. Forelimb heel injuries are common if a horse breaks stride. Elbow boots may be necessary to protect the elbows from stud-induced trauma. Some lameness problems get worse during the winter, because traction from the studs stops the feet abruptly. Hock-related lameness is often worse during the winter, and tendon and suspensory ligament (SL) problems increase.
The shoeing of racing Finnhorses is otherwise much like that of STBs, but many Finnhorses are not natural trotters and tend to gallop or pace, so many trainers use special shoeing to help the horse to balance. Young horses often need heavy front shoes with toe weights and bell (overreach) boots when they are learning to trot. The total weight per foot can be up to 500 to 800 g, and this predisposes the horses to lameness, particularly tendon and SL injuries. Improvements in breeding have decreased the number of horses with severe balancing problems. On the hind feet Finnhorses usually wear normal STB shoes. The lateral branch of the shoe is often longer and bent slightly outward (trailer) to make the hind action wider and therefore avoid interference between the forelimbs and hindlimbs. Although many STBs race unshod, this is rare in Finnhorses.
Conformation and Lameness
The Finnhorse is a heavy, draft-type horse compared with other racehorses. The forehand is heavier than the rear of the horse and is combined with a heavy head and a thick and short neck, causing much stress to the forelimbs. Finnhorses often stand back at the knee, and this sometimes is combined with lateral deviation of the carpus (offset knees). Forelimb tendon, SL, and carpal injuries are not uncommon. The hindlimbs are usually conformed better in Finnhorses than the forelimbs. The most common faults are sickle hocks and cow hocks, which can cause curbs or other lameness problems in the tarsal area. Fetlock conformation is often good, and most Finnhorses have big hooves with good-quality horn.
Lameness Examination
Many Finnhorses complete a racing career without serious lameness problems and require substantially less veterinary treatment than STBs, perhaps because of slower racing speeds. The lameness examination for a Finnish horse is similar to that for a STB racehorse, and similar problems occur. Clinical history is particularly important, and the following questions should be asked:
The veterinarian should assess the type and use of the horse and its conformation, muscular development, and general condition and should systematically palpate all the limbs, because concurrent lameness in several limbs often occurs.
Many horses are trained with sleighs in the winter and are harnessed with collars. If the collar is not fitted properly, it can cause shoulder musculature soreness. Soreness of the shoulder or scapular musculature also can point to other problems in the forelimbs, especially when the lameness is bilateral. Inflammation of the carpal sheath is common because of the heavy front of Finnhorses and the conformation of the carpi and invariably is associated with palpable distention. Proximal suspensory desmitis (PSD) sometimes occurs, and pain may be induced by palpation of the proximal metacarpal region.
The second (McII) and fourth (McIV) metacarpal bones in Finnhorses are sometimes thick and prominent, but this is not usually relevant (Figure 113-2), although thick metacarpal bones are sometimes seen in horses with PSD or tenosynovitis of the carpal sheath. Ossification of the cartilages of the foot usually can be felt by thickening and loss of elasticity in the region of the coronet, but pain is seldom evident on palpation.
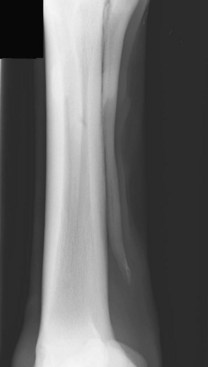
Fig. 113-2 Dorsomedial-plantarolateral oblique radiographic image of the metacarpal region. The second metacarpal bone is enlarged, which usually has no clinical significance.
In the hindlimbs special emphasis needs to be given to palpation of the tarsus. Tarsal pain is common in Finnhorses with poor conformation. Curbs are common in younger horses (3 to 6 years of age), and distal hock joint pain is common in older horses. The Churchill test works well in Finnhorses. Stifle lameness is not common in Finnhorses, and upward fixation of the patella is rare. Osteochondrosis of the lateral trochlear ridge of the femur occurs occasionally in foals and young horses, sometimes with large defects that respond poorly to arthroscopic debridement.
The gait and response to flexion tests can be evaluated properly only when the horse is calm and well controlled by the handler. It is essential that the horse trots straight and not too fast. Many horses are too eager and excited and need to be sedated or tranquilized mildly for flexion tests. Acepromazine (0.01 to 0.025 mg/kg) or romifidine (0.01 to 0.03 mg/kg) is suitable. Sedation is especially important for Finnhorse stallions, which are often difficult to handle, and sometimes two leaders are necessary to control the horse and keep it trotting straight. Horses used for riding can be examined in a circle on the lunge, but trotters are seldom taught to lunge.
When flexion tests are performed, it is essential for the veterinarian always to examine all limbs and not only those that are suspected to be lame. The tests always should be done in a similar manner and order. When doing flexion tests, the clinician should note all reactions. We do not think false-positive reactions exist, only reactions of different grades. The clinician needs to collect all the information and decide which reactions are clinically significant. Proximal and distal limb flexion tests are done separately in the forelimbs and hindlimbs, using a force of approximately 40 kPa for 60 seconds.
In general, all the trotting Finnhorses also are examined at the track at high speeds. Many action problems, especially in the young horses, show only at high speeds. The horse is harnessed in a higher sulky than normal, so the driver of the vehicle does not obscure the horse. The veterinarian drives a car behind or beside the horse at the racetrack. Examining the horse from the car is more helpful than driving the horse, because the clinician can be some distance away from the horse to see the action more clearly, and abnormalities can be assessed more easily.
Diagnostic analgesia is used as in STBs. The clinician must keep in mind that high-speed lameness seldom can be resolved totally by analgesic techniques. Every block changes the horse’s action, and when the veterinarian does several blocks on the same horse, assessing the meaning of each block is difficult. When examining a horse with high-speed lameness, the clinician must believe what vision, touch, and experience indicate.
Imaging Considerations
In Finnhorse trotters, radiological changes are found much less commonly than in STBs. Carpal chip fractures are rare in Finnhorses, and sclerosis of the third carpal bone is unusual. Osteochondrosis is also rare in the Finnhorse, though the prevalence has been increasing slightly in the past decade. Because osteochondrosis is unusual, radiographic examination of young Finnhorses is not performed routinely if clinical signs are absent. Controlling osteochondrosis in Finnhorses is attempted by obtaining radiographs of all stallions that are proposed for public breeding. Stallions with osteochondrosis generally are not accepted. Ossification of the cartilages of the foot is a common radiological finding in Finnhorses. Navicular disease is a rare diagnosis. Enlargement of the McII and the McIV is common and often does not cause clinical signs. Flakelike fragments adjacent to the McII usually result from interference.
Ultrasonography is invaluable for assessing soft tissue injuries and may be more useful than radiography in examining the splint bones, because splint bone problems often are associated with carpal canal syndrome or PSD.
Undiagnosed Lameness
Some young trotting Finnhorses trot soundly at slow speeds and show no signs of lameness during a lameness examination, but when asked for speed, the horses lose the action completely. Loss of rhythm causes this; the horse simply cannot trot at higher speeds. This often happens to talented horses that have early speed with little training but do not have the strength to maintain it. The training regimen must be aimed at building strength, especially in the hindlimbs. Horses are trotted in 1- to 3-minute intervals with resistance from a special resistance cart, in deep snow, or uphill. Training takes a long time, sometimes up to a year, until these horses learn to trot again, and some horses never recover. Because the main racing events are for aged horses, time is not as big a factor for Finnhorses as for STBs. It is quite possible for a horse to recover completely and become a top-class racehorse at an older age.
Lameness Conditions Typical of Finnhorses
Carpal synovitis is common in Finnhorses, and signs are similar to those seen in STBs. In the early stages a horse warms out of lameness quickly. Often horses with carpal problems begin to roll over and may try to pace or gallop instead of trotting. The horse may trot if the shoes are weighted more, but this may accentuate the primary problem. Without treatment the lameness worsens, and the horse begins to hang on a line and gradually becomes overtly lame. Radiological changes rarely are seen, probably because of the slower racing speeds compared with those of Thoroughbreds and STBs. Treatment consists of intraarticular medication with hyaluronan, polysulfated glycosaminoglycans (PSGAGs), or corticosteroids, alone or in combination, together with rest for several weeks. Recently the use of autologous conditioned serum (ACS) has been increasing in treating joint lameness with good results.
Carpal canal syndrome is also common in Finnhorses, sometimes simultaneously with carpitis, sometimes on its own. Ultrasonography is useful for confirming the diagnosis. The treatment is usually rest combined with intrathecal administration of hyaluronan or corticosteroids. Some horses do not respond to conservative therapy, and surgical treatment using tenoscopy may be necessary. Osteochondromas of the distal caudal aspect of the radius are seen tenoscopically, often accompanied by lesions of the deep digital flexor tendon (DDFT). The severity of these osteochondromas is difficult to assess radiologically, and often the diagnosis is made by tenoscopy. Surgical removal of the osteochondroma and debridement of torn fibers of the DDFT result in a good prognosis for racing.
Tarsal lameness is common in Finnhorses and is the most frequent cause of hindlimb lameness, usually because of distal hock joint pain. Mild lameness in horses is not noticed easily at slow speeds, but with increasing speed the horse begins to drag the affected limb, and the rear end moves to the opposite shaft. The horse usually hangs on the line on the side of the affected limb. Radiological evidence of osteoarthritis may or may not be apparent. Radiological changes are seen less frequently than in STBs. Intraarticular treatments with corticosteroids, hyaluronan, or PSGAGs are used widely. Treatment with intravenous (IV) tiludronate is often beneficial. In some horses cunean tenectomy can be useful.
Superficial digital flexor (SDF) tendonitis and suspensory desmitis are common. SDF tendonitis usually occurs in forelimbs, and poor conformation or overweighting the shoes may be predisposing factors. In the hindlimb, tendon injuries are usually traumatic. Suspensory desmitis occurs more frequently in forelimbs than hindlimbs, probably because of the heavy front conformation. Suspensory branch injuries are most common.
Finnhorses cope better with chronic suspensory desmitis than do STBs because of the lower racing speeds, longer rest periods, ability of the horses to race at an older age, and thus better opportunities to heal. Suspensory desmitis is sometimes associated with splint bone fractures or exostoses.
Treatment of Finnhorses with SDF tendonitis and suspensory desmitis is most often conservative, with long rest periods. Tendon splitting or desmotomy of the accessory ligament of the SDF tendon (SDFT) sometimes is used for tendonitis. Hot firing has been a traditional treatment for Finnhorses with tendonitis and desmitis for many decades, and some veterinarians still use it in some horses, though with mixed success. Stem cell treatments are used as in other breeds.
Curbs (soft tissue enlargement in the plantar tarsal and proximal plantar metatarsal regions) often are seen in young horses (3 to 5 years old) in early training, especially those with sickle hocks (see Chapter 78). Curbs seldom cause spontaneous lameness. Usually the signs show first at higher speeds, when the cranial phase of the stride in the affected limb is shortened, and the horse begins to drag the limb. Ultrasonographically, peritendonous and periligamentous inflammation is the most common finding (Figure 113-3). Injuries of the SDFT or the DDFT are rarely seen. Most veterinarians treat horses with curbs symptomatically, without ultrasonographic examination to determine the structure involved. Treatments include rest, corticosteroid or dimethyl sulfoxide injections, or pin firing. Cryotherapy is not used as widely as pin firing. The prognosis with all treatments is very good.

Fig. 113-3 Transverse ultrasonographic image of the plantar distal aspect of the hock. Medial is to the left. There is extensive subcutaneous heterogeneous echogenic material (arrows) plantar to the superficial digital flexor tendon in a horse with curb.
Ossification of the cartilages of the foot (sidebones) is a common finding in the front feet of heavy horses, occurring in 80% of Finnhorses. The condition is more common in females than in males and positively correlates with the size of the horse. The grade of the ossification is usually mild, but extensive ossification sometimes occurs. The cause is unclear, but a heritable component exists. In a recent study evaluating ossification of the cartilages of the foot in 964 Finnhorses, females had more ossification than males, and this difference increased with age.1 The ossification in the medial cartilages progressed significantly with age in females but not in males, and in lateral cartilages the increase in ossification with age was evident in both sexes.1 Estimates of heritability for the ossification parameters varied slightly between the cartilages as well as between the front feet.1 For total ossification, the estimates of heritability varied from 0.31 (right lateral) to 0.50 (left medial) and were slightly higher for ossification at the base of the cartilages.1 High genetic correlations were found for total ossification between the medial and lateral cartilages in the foot and for parallel ossification parameters between the right and left feet.1 The authors concluded that the estimates of heritability were relatively high, and both cartilages and front feet have a similar genetic tendency to ossify.1 The cartilages start ossifying at an early age, unassociated with training of the horse. Other contributory factors may include hoof conformation, shoeing, and concussion.
The clinical relevance of sidebones is questionable. Most horses with mild or moderate ossification show no clinical signs. Ossification is detected only by radiology. With extensive ossification the cartilages are palpable proximal to the coronary band. Palpation does not induce pain. In general, horses with large sidebones show some clinical signs, especially on hard ground. Lameness at slow speeds is rare, but at high speeds with increased concussion the forelimb stride is shortened and the horse breaks to pace or gallop. In a study of 21 Finnhorses with ossification of the cartilages of the front feet, there was no significant relationship between height of the ossifications measured radiologically and increased radiopharmaceutical uptake (IRU) in the cartilages of the foot. Separate centers of ossification were not associated with IRU.2 Intense IRU was seen unilaterally in four horses, medially in one horse, and laterally in three. In two of these horses a unilateral palmar digital nerve block relieved the mild lameness.2 In the other two horses no obvious lameness was seen, but both had a history of being stiff or having locomotion problems during high-speed trot.2 In two horses with IRU in the lateral cartilage of the foot, an incomplete fusion line was found radiologically between a large separate center of ossification and the base. The third horse had extensive ossification with bony protrusions, suggestive of chronic enthesopathy in a narrow foot.2 In all cartilages of the foot with intense IRU and/or lameness, the ossified part of the cartilage was wider and more irregular compared with other ossifications.2 The authors concluded that IRU and a different radiological appearance of affected cartilages from that of unaffected cartilages within the same horse were definite signs of clinical relevance. Obscure locomotion problems were more commonly associated with ossification of the cartilages than true lameness.2
The diagnosis is confirmed radiologically, using dorsopalmar images. Osteoarthritis of the distal interphalangeal joint and navicular disease may cause similar clinical signs and may be present concurrently with sidebones.
The treatment options are limited, because the condition persists. Shoeing with egg bar shoes, often combined with thick pads, is helpful in some horses. Most horses with sidebones can race with moderate-to-good success when shod properly and raced only on good surfaces. Because of the hereditary background, all Finnhorse stallions that are used for public breeding have to be free of sidebones, radiologically, before being accepted.
Splints are fairly common in the forelimbs of young, growing horses, and affected horses are usually treated conservatively with rest. Most splints resolve spontaneously, but local corticosteroid injections or cryotherapy sometimes is used. Interference injury may result in a flake of bone detached from the McII. These fragments do not heal with rest and horses respond poorly to corticosteroid injections or cryotherapy. Surgical removal is usually necessary.
Chronic tenosynovitis of the digital flexor tendon sheath (DFTS) is a common cause of lameness in aged cold-blooded trotters and usually develops gradually, with mild or moderate swelling and no lameness for long periods. In time the DFTS becomes fibrotic, and masses and adhesions develop. At this stage constriction by the palmar annular ligament (PAL) may occur. Many horses can perform well despite chronic tenosynovitis, especially in hindlimbs. Intrathecal administration of hyaluronan, with or without corticosteroids, is used for horses with acute tenosynovitis. Frequent corticosteroid injections often seem to increase tenosynovial masses. Physiotherapy and especially shockwave therapy are often beneficial in treating Finnhorses with chronic tenosynovitis, not only for controlling pain but also for helping to keep the DFTS as elastic as possible. Tenoscopy and transection of the PAL is used if the condition is advanced. Cold-blooded horses with chronic tenosynovitis seem to respond more poorly to treatment than do STBs with similar lesions. This may be because Finnhorses are often older and of greater weight.
In young Finnhorses, bilateral hindlimb fetlock pain is fairly common and causes a short and stiff hindlimb stride when they start to trot, which improves with exercise early in the condition. When both hind fetlocks are blocked simultaneously, the action changes completely. Pain is considered to be associated with subchondral bone remodeling of the distal aspect of the MtIII. A variety of treatments have been used, including shockwave therapy, joint lavage, and intraarticular treatment with PSGAGs, hyaluronan, or corticosteroids, often combined with parenteral administration of NSAIDs. In some Finnhorses IV tiludronate infusion is more beneficial than intraarticular treatments. If lameness is severe, surgical drilling of the subchondral bone is performed. Horses remain lame for several months, but the long-term prognosis is reasonable.
Osteochondrosis is rare in Finnhorses, but when it does occur, osteochondrosis most often is seen in the cranial aspect of the intermediate ridge of the tibia and causes effusion of the tarsocrural joint. Treatment is removal of the fragment(s) by arthroscopy. The femoropatellar joint is another typical predilection site for osteochondrosis in Finnhorses, and osteochondrosis of this joint causes clinical signs in young horses. Finnhorses with large defects of the lateral trochlear ridge of the femur have a guarded or poor prognosis.