Introduction to: Discussion, questions and answers
These questions ask you to examine issues concerning the applications of the scientific method to various aspects of health sciences research. Unlike the multiple choice and true or false questions, these discussion questions do not necessarily have a single correct answer. Rather, they are aimed at promoting a critical, integrative view of conducting research.
Our first discussion question involves theories and examines the relationships between theories, models, hypotheses and empirical observations. Theories are conceptual frameworks (as we discussed in Ch. 1) integrating a range of related observations and explanatory hypotheses. We may deduce empirically testable hypotheses from our theories.
On the basis of observations, in particular when the observations are carried out under controlled conditions, we establish the probable truth of our hypotheses, and thereby support or falsify the theories which were originally the sources for the hypotheses.
Some theories include models which represent specific aspects of a theory. Models are used to explain real situations and predict novel empirical outcomes. Models can be as follows:
1.
Physical models. These models are constructed from materials, for example a ‘pump’ model of the heart for showing how the circulatory system works, or a construction of the DNA molecule to show how different nucleotides are organized in order to replicate genetic information.
2.
Mathematical models. These models contain a series of equations that represent our theoretical interpretations of real-life situations. For example, epidemiologists may employ mathematical models to predict how a given epidemic might spread in a population, or a physiologist may employ a mathematical model of neuronal membranes to predict the behaviour of action potentials in a neurone. When our theories and related models are sufficiently detailed and well formed, we may use these in simulation research. We now use computers, which are capable of carrying out the complex calculations necessary for the simulation of a real-life situation and predicting numerical outcomes.
3.
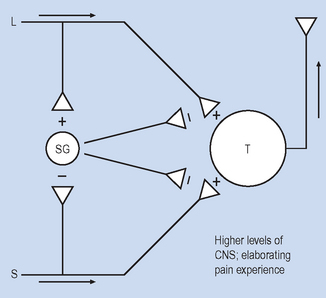
‘Paper and pencil’ models. Often, our theories are not sufficiently detailed to allow precise numerical predictions. Here the models are ‘sketches’ of a particular system, defining the key elements of the model and showing how these elements interact to produce various outcomes. Such models enable us to make testable predictions concerning the effects of variables as shown by the following model (
Fig. D1.1) of the ‘gate control theory’ of pain (
Melzack & Wall 1965). (Note that for teaching purposes this model is an incomplete and modified representation of the original. If you are interested in understanding pain problems, you should consult Melzack & Wall’s original work.)
Elements of the systems
(a)
L: ‘Large’-diameter axons of receptors, which convey information concerning mechanical stimuli, such as pressure and vibration.
(b)
S: ‘Small’-diameter axons of receptors, which convey information concerning noxious (tissue-damaging) stimuli.
(c)
SG: Neurones within the substantia gelatinosa (SG) of the spinal cord. These receive converging information from L and S axons. The SG neurones control, or gate through pre-synaptic inhibition, the information flowing through to the T neurones.
(d)
T: Transmission neurones in the spinal cord, which receive information from both L and S axons. The pattern of activity of T neurones is projected to higher levels of the central nervous system (CNS), where this information is elaborated into the experience of pain.
(e)
Δ: Synapses, which may be either excitatory (+) or inhibitory (−). Excitatory synapses increase, while inhibitory synapses decrease the activity of the post-synaptic neurones.
(f)
→: Arrows showing the direction of the information flow; in this case from the periphery towards the spinal cord and, subsequently, to higher levels of the CNS. The activity of large fibres (L) stimulates the gating mechanism (SG) which serves to inhibit nociceptive information conveyed by S axons to the T neurones.
The above model is an attempt to produce a representation of the events which take place in the mammalian nervous system when receiving and processing nociceptive input at a spinal cord level. The ‘gate control’ model integrates a broad range of research in the neurosciences and has been applied to explain aspects of pain control in clinical settings.
Questions
After this rather prolonged introduction to the model, we are ready to ask questions about how it may be applied to explaining and predicting observations about pain.
1.
Use the above model to describe what happens in the nervous system during noxious (tissue-damaging) stimulation.
2.
How would we use controlled observations to demonstrate that small (S), rather than large (L), neurones convey nociceptive information? (Assume that we have instrumentation for measuring the activity of single neurones in response to different kinds of stimuli.)
3.
Explain how we would use evidence obtained by recording the activity of single neurones to demonstrate that T neurones are in fact involved in nociception.
4.
Describe the effects of large (L) and small (S) axons on the activity of SG neurones.
5.
Explain the mechanism by which SG neurones function as a ‘pain-gating’ system.
6.
Propose a hypothesis for predicting the effects of selectively damaging T neurones on subsequent pain experience.
7.
Propose a hypothesis for predicting the effects of damaging large axons (L) on subsequent pain experience.
8.
A virus is identified which damages SG neur-ones. As a hypothetical case, imagine that people who have this virus report greatly reduced pain sensitivity. What would be the implication of this observation for the validity of the gate control theory of pain?
9.
Would you discard the gate control theory on the bases of the hypothetical observations described in question 8? Explain.
10.
A clinical technique called transcutaneous electrical nerve stimulation (TENS) for relieving pain involves the gentle peripheral electrical
stimulation of painful areas. Explain in terms of the model how TENS might work to reduce pain. (Hint: TENS does not directly reduce the activity of S axons.)
Answers
1.
Small-diameter S axons convey nociceptive information towards spinal cord neurones, including the SG and the T neurones. The SG neurones are inhibited through nociceptive inputs while the T neurones are excited by the stimulation. Information concerning tissue damage is then conveyed by the axons of the T neurones to higher levels of the CNS. There it is elaborated into the experience of pain.
2.
By showing that the activity of T neurones is correlated to the levels of peripheral noxious stimulation.
3.
Mechanical stimuli – show that S axons are not responsive while L axons change rate of activity. Noxious stimuli – show that S axons change rate of activity while L remain unresponsive.
4.
Large axons excite (increase the rate of activity of SG neurones) while small axons inhibit the rate of activity of the SG neurones.
5.
The SG neurones inhibit the effect of the S axons on the T neurones. As L axons excite the SG neurones, the action of L fibres is to ‘close’ the pain gate. The S fibres ‘open’ the pain gate by inhibiting the SG neurones. In effect, the model is telling us that mechanical stimulation, such as gently scrubbing an injured area, will reduce nociceptive input. Conversely, noxious stimulation seems to maintain the effects of subsequent nociceptive inputs.
6.
The T neurones are crucial for transmitting nociceptive information to higher levels of the CNS. Hypothesis: selectively damaging T neurones will reduce or eliminate pain experience following nociceptive stimulation.
7.
Damage to L axons will result in reduced excitatory stimulation of the SG neurones, opening the spinal gate to noxious stimulation. Hypothesis: damaging L axons would increase the pain experienced following nociceptive stimulation.
8.
As the model proposes that SG neurones are involved in the gating of noxious stimuli, we would predict that damage to the SG neurones would increase pain sensitivity. Reduced pain sensitivity is evidence which would falsify the gate control theory.
9.
Probably not; as we discussed in the context of Lakatos’ ideas. Theories have a ‘protective belt’ of assumptions, which means that a single empirical falsification need not result in the rejection of the theory. In this case, we may look for additional effects of the virus; say in destroying CNS tissue involved in elaborating pain experience. However, in the long run, such disconfirmations will lead to discarding the theory.
10.
In terms of the model, TENS works by stimulating the L axons, and thereby ‘closing’ the pain gate, as outlined in questions 4 and 5.