Role Relationship Patterns
At the end of the chapter, the reader will be able to:
1 Define role as a framework for role performance and role relationships.
2 Discuss the professional roles of the nurse.
3 Describe the components of professional role socialization in professional nursing education.
4 Describe interprofessional education.
5 Discuss professional role development as a registered nurse.
6 Identify factors needed to create supportive work environments for nurses.
7 Discuss professional role relationship behaviors with colleagues.
8 Describe professional role behaviors supporting nurse-client relationships.
This chapter explores the concept of role and role relationships in nursing practice from two perspectives: (a) professional nursing role; and (b) role as a functional health pattern, and nursing diagnosis. Key concepts of professional socialization, professional communication, and professional development are addressed.
Basic concepts
Role is defined as the traditional pattern of behavior and self-expression performed by or expected of an individual within a given society. People develop social and professional roles throughout life. Some are conferred at birth (ascribed roles) and some are attained (acquired roles) during a lifetime. People can have several social roles at the same time (Chaudhary & Sriram, 2001). For example, Marge is a professional nurse, a mother, a wife, a daughter, a lay minister in her church, and president of the parent-teacher association at her children’s school. Each role carries different expectations. When the expectations of one role interfere with the discharge of other important life roles, conflict, burnout, or both can occur.
Role relationships
Roles have performance and relationship dimensions that affect how people relate to one another. Social customs and expected professional standards of practice reinforce the performance aspect of role relationships. For example, consider the different professional role expectations of a lawyer, a physician, and a dentist. Each profession has a different set of skills and professional role competencies based on their education and training.
Behavioral expectations in role relationships are reciprocal as role perceptions and expectations influence communication content and delivery. Consider your own “role” as a nursing student and how it has influenced your relationships and communication with clinical instructors, your clients, professional peers, your friends, and other significant people in your life. What do others expect of you, simply because you are now a nursing student?
Roles provide guides for behavior that are in part socially regulated and in part individually determined. Standards for individual role performance reflect personal, social, cultural, gender, institutional, and family expectations. Role relationships are recognizable through membership in a community or through differences in work responsibilities, cooperative activities, education, and social affiliations. Stronger role expectations may be held for people in public roles, for example, elected politicians, ministers, and teachers because of the trust people have in them as a function of their role. Changes in social circumstances such as marriage, widowhood, retirement, job promotions, or birth of a child can alter personal and societal interpretations of individual and professional roles. Exercise 7-1 is designed to help you focus on the complexity of different life roles.
Professional nursing roles
Nursing roles are developed from and linked to the discipline of nursing. The criteria (Box 7-1) for describing a professional discipline, originally developed by Flexner (1915), still hold true today. In their seminal work on nursing as a discipline, Donaldson and Crowley (1978) identify three key themes that distinguish and delimit the discipline of professional nursing:
1. Concern with principles and laws that govern the life processes, well-being, and optimum functioning of human beings
2. Concern with the patterning of human behavior in interaction with the environment in critical life situations
3. Concern with the processes by which positive changes in health status are affected (p. 113)
Willis, Grace, and Roy (2008) identify a similar unifying focus for the discipline related to facilitating meaning, choice, quality of life, humanization, and healing through nursing interventions.The robustness of nursing as a professional discipline is evidenced in the fact that its core descriptors as a discipline are as salient today as they were elegantly described in 1978. Clearly, the nursing role is much more complex than it was in 1978. Evidence for expanded roles is found in the transition of nursing education from the hospital training to increasing levels of educational preparation and practice certifications required of professional nurses. Nursing content and skill sets necessarily change in relation to new and different health care situations; the fundamental essence of nursing as a discipline remains constant.
Role behaviors in professional nursing
Anthony and Landeen (2009) note, “Nursing education has a history of tension and inter-reliance with historical events that encompasses nursing practice, human and social needs, geo- and socio-political processes” (p. 2). At no time in recent history has there been such a complex accumulation of historical events directly and indirectly impacting health care delivery and nursing education. Professional nursing roles have evolved and expanded to reflect the increasing complexities of health care, globalization, changing client demographic characteristics and diversity, and the exponential growth of health information technology (Hegarty, Condon, Walsh, & Sweeney, 2009). With the rapid changes in health care, there is no single role descriptor to explain how professional nursing roles fit in to the health care hierarchy, or will do so in the future. Figure 7-1 identifies the evolving role competencies required of contemporary nurses, identified by the Institute of Medicine (2003).
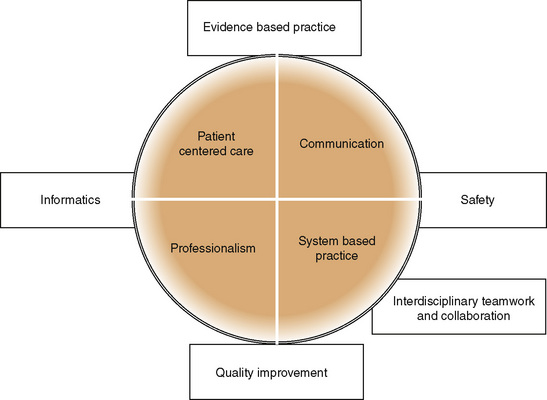
Figure 7-1 Professional nursing role: core competencies for health professionals. Adapted from Institute of Medicine (IOM): Health professions education: a bridge to quality (pp. 45–46). Washington, DC, 2003, National Academies Press, 2003.
Types of Professional Roles: The significance of the professional nurse’s role is emphasized in the Joint Commission’s first white paper, entitled Health Care at the Crossroads (2002), which states, “… in the end, nurses are the primary source of care and support for patients at the most vulnerable points in their lives” (p. 4). Clinical skills related to health promotion, risk reduction, and collaboration with clients and health care providers in primary care are recognized as modern hallmarks of clinical role competence. As providers of care, nurses delegate and supervise related care activities for allied professional staff. Nurses provide leadership and coordination in health care improvement through advocacy and education, and participate in research. Proficiency in biotechnology and health information technology has become an expected competency required of professional nurses (American Association of Colleges of Nursing [AACN], 2008; Gugerty, 2007). Regardless of setting, nurse-client relationships and professional communication provide a primary means through which nurses implement professional roles in providing quality health care and contribute to shaping the health care delivery system.
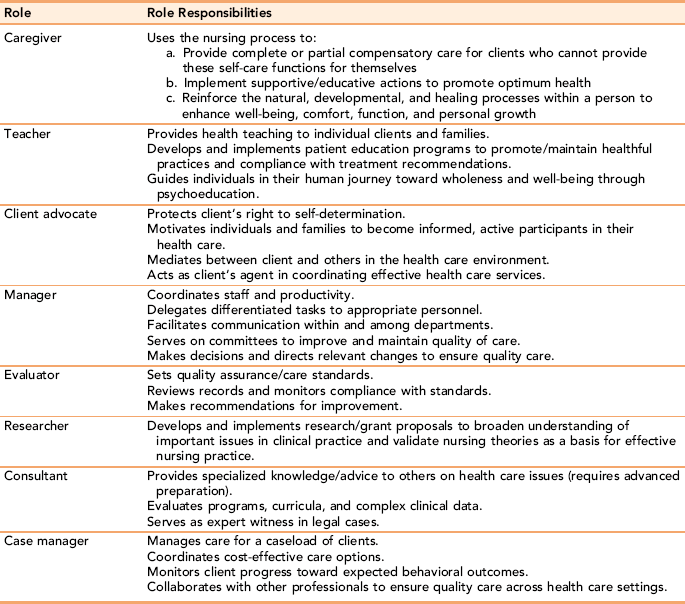
Table 7-1 identifies the many different types of roles associated with professional nursing practice. Nursing roles are adapted for practice in prisons, schools, home care, shopping malls, and faith-based settings. Nurses provide care individually and as part of multidisciplinary health care teams with the military, during disasters, in the juvenile justice system, with the homeless, in the fields with migrant workers, and in clinics for the uninsured. Increasingly, nurses are assuming active advocacy roles to inform policy makers, educators, other health care providers and consumers to increase and protect the funding, accessibility, and availability of quality health services. Exercise 7-2 is designed to help you look at the different role responsibilities of practicing nurses.
Advanced Practice Roles: Advanced practice nurses are registered nurses with a baccalaureate degree in nursing and an advanced degree in a selected clinical nursing specialty with relevant clinical experience. Certification and state licensing requirements vary according to state for practice in advanced practice roles. Box 7-2 identifies the four categories of advanced practice nursing in contemporary health care.
Expanded advanced practice roles can include “entrepreneur, recruiter, editor, publisher, ethicist, labor relations expert, nurse anesthetist, lobbyist, [and] culture broker” (Roberson, 1992, p. 4). Many advanced practice nurses (nurse practitioners and some clinical specialists) have prescriptive authority. In addition to clinical roles, advanced practice nurses function in research, educational, and administrative roles. Each expanded role requires specialized competency training to manage care independently in an advanced specialty role. Exercise 7-3 helps you to explore the different specialty areas available for professional nurses in advanced practice.
Nursing education and professional role performance
The nursing profession has evolved from a primarily apprenticeship model to one with sophisticated educational models and multiple training options. All registered nurses currently are educationally prepared in colleges and universities, at associate’s degree, baccalaureate, master’s, and doctoral levels (Erickson & Ditomassi, 2005). Educational career ladders are available for nurses to advance from bedside nurses to advanced practice levels involved with research, clinical expertise, consultation, education, and administration. Hegyvary (2007) asserts that there is no form of self-investment more significant than education for realizing one’s full potential as a nurse.
New models in nursing education
In 2003, the American Association of Colleges of Nursing (AACN) introduced two new models of professional education. They were developed in response to expanded clinical roles in nursing practice, the Institute of Medicine’s Report on Medical Errors, and to offset nursing faculty shortages. The clinical nurse leader (CNL) role prepares students with a baccalaureate degree in another field to become an advanced nurse generalist. An accelerated generalist nursing curriculum combines baccalaureate and master’s level courses, which emphasize clinical leadership skills, and training in health care systems management at the clinical unit level. The CNL “designs, implements, and evaluates client care by coordinating, delegating and supervising the care provided by the health care team, including licensed nurses, technicians, and other health professionals” (AACN, 2003, paragraph 2). Students who satisfactorily complete program requirements are awarded a generic master’s degree. Graduates can sit for the NCLEX professional nursing licensing examination and are eligible for certification as a CNL. To practice as an advanced practice nurse in a clinical specialty, the CNL must complete master’s-level preparation in an advanced practice specialty.
A second professional role, Doctor of Nursing Practice (DNP), represents a terminal degree in advanced clinical nursing practice. It is designed for nurses who want a clinical rather than research-focused doctorate. The curriculum combines advanced nursing practice competencies with a solid foundation in clinical science, evidence-based practice methods, system leadership, information technology, health policy, and interdisciplinary collaboration (American Association of Colleges of Nursing, AACN, 2004). According to Mundinger (2005), the DNP degree will expand and complement current master’s specialty education and roles.
Interprofessional education: The Institute of Medicine (2003), in its landmark report, Health Professions Education: A Bridge to Quality, calls for health professionals to develop competencies in working together in interdisciplinary teams. The report identifies “working in interdisciplinary teams” as one of five core competencies needed in today’s health care delivery. Promoting interdisciplinary education and providing shared learning opportunities is an important way to develop the respect and integration students need to function in interdisciplinary health care teams.
Interprofessional education is defined as “occasions when two or more professions learn from and about each other to improve collaboration and the quality of care” (Oandasan & Reeves, 2005, p. 24). This does not mean that nursing and other health care professional roles are interchangeable. Nursing, medicine, dentistry, pharmacy and social work are distinct health disciplines that prepare clinicians to assume different practice roles using discipline specific practice standards. Helping students understand the natural interdependence between professions required for today’s interdisciplinary care, whereas at the same time recognizing the unique knowledge and skill set of each discipline, is a critical foundation for interprofessional training. Students gain firsthand understanding of the professional values held by other disciplines and collectively identify with important health care issues. In the process of sharing knowledge and experience, students learn the tools of collaborative problem solving (Fronek et al., 2009).
The goal of interprofessional education is to provide students with the knowledge, skills, and attitudes needed to effectively collaborate and improve the quality of health care through interdisciplinary problem solving. Skills to enhance teamwork and to clarify roles in providing client-centered care are important in both discipline-specific and interprofessional learning (Pecukonis, Doyle, & Bliss, 2008).
The impetus for interprofessional education comes from many sources. The Pew Health Professions Commission (1993) recommends revision of health professions curricula to include shared interprofessional learning in academic settings, and the AACN (2008) recently identified “interprofessional communication and collaboration for improving patient health outcomes” (p. 3) as one of nine essential outcomes expected of nursing graduates. The Joint Commission suggests that safe, effective clinical care requires an interdisciplinary collaborative team approach (Walsh, Gordon, Marshall, Wilson, & Hunt, 2005).
Introducing interprofessional courses as part of the basic nursing curriculum helps students articulate their own professional roles, and understand how collaboration and teamwork can more effectively resolve complex issues to enhance clinical outcomes (Margalit, Thompson, Visovsky, et al., 2009). Students can learn trust and respect for each discipline’s competencies, and the team building collaborative skills through direct experience with each other’s clinical practices. Collaborative interactions modeled by interdisciplinary faculty add to the learning experience.
Learning about Interdisciplinary Collaboration: Rodts and Lamb (2008) state that “any new role requires an understanding of what it is and what it is not” (p. 131). An interdisciplinary, collaborative role is no different. Nursing students must have a solid understanding of their own discipline’s specific roles and responsibilities so that they can articulate them clearly to professionals in other disciplines. To maintain nursing’s integrity as a profession, the profession must retain control of its knowledge base, skills, and accountability for practice. At the same time, nurses must be willing to work collaboratively with other professionals as part of an interdisciplinary team. Figure 7-1 identifies core competencies needed in today’s health care delivery system.
Although interdisciplinary collaboration is still in its infancy as an integral part of professional curriculums, shared elective classes involving interdisciplinary education for two or more disciplines are increasing at the baccalaureate and graduate level (Herbert, 2005). Frequent topics covered in interprofessional electives include ethics, death and dying, emergency preparedness, gerontology, and legal issues. In preparing courses, Aveyard, Edwards, and West (2005) suggest topics need to be “both enhanced by an interdisciplinary approach and not hindered by a lack of detailed attention to field-specific content” (p. 64). As student nurses, you have a unique opportunity to help make the nursing discipline visible as a key player and carve out nursing’s role in the evolution of interdisciplinary collaboration as a primary care strategy.
Nursing values and role socialization
Although the core values and fundamental features of professional nursing remain constant, the scope of practice and implementation of associated professional nursing roles continues to evolve as we enter the 21st century.
Professional role socialization
Essential Values and Professional Behaviors: The AACN (1986) first published examples of the essential values, attitudes, personal qualities, and professional behaviors associated with the profession of nursing and later refined them in 2008 (see Table 7-2). Key elements of the professional nursing role include the acquisition, development, and integration of health-related psychomotor, social, and cognitive skills, and the achievement of a sense of self as a professional nurse within an ethical, competency-based framework.
TABLE 7-2
Values and Qualities of Professionalism in Nursing
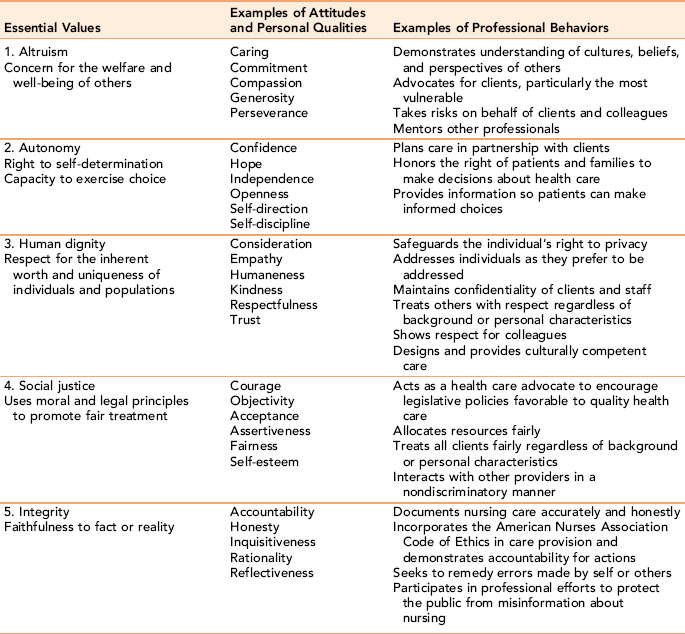
Adapted from American Association of College and University Education for Professional Nursing: Final report, Washington, DC, 1986, American Association of Colleges of Nursing; and American Association of Colleges of Nursing: Essentials of baccalaureate nursing education for professional nursing practice (pp. 27–28), Washington, DC, 2008, Author.
Role socialization refers to the process through which a student nurse learns the professional norms, values, and skills associated with the professional nursing role, and acquires identity features of the profession. It is an interactive developmental process that starts when students enter a nursing program and begin to learn the “pure” form of nursing knowledge. Initially, nursing students are absorbed in learning the basic knowledge required of the professional role. They are dependent on textbooks and their instructor to help them find the one “right answer” to health care problems. As students become comfortable with foundational nursing knowledge, they begin to consider multiple options as they integrate professional judgment into clinical care planning. Students are able to apply scientific knowledge to practice in a realistic manner and “to relate new material to their previous knowledge base” (Cohen, 1981, p. 18).
The next phase involves internalizing the culture, that is, the values, standards, and role behaviors associated with professional nursing. Pecukonis, Doyle, and Bliss (2008) note that “each discipline possesses its own professional culture that shapes the educational experience; determines curriculum content, core values, dress, salience of symbols” (p. 417). Student nurses are accountable for presenting themselves as professionals to other health providers and the public. For example, professional appearance is important. Although a common dress code for professional nurses is “scrubs,” attire should be neat, clean, and properly fitted. The professional “image” of the nurse is an unspoken factor in how others perceive the profession.
Nursing faculty and clinical preceptors serve as important socializing agents, helping students learn the values, traditions, norms, and competencies of the nursing profession (Neil et al., 1998). A clinical preceptor is an experienced nurse, chosen for clinical competence and charged with supporting, guiding, and participating in the evaluation of student clinical competence (Paton, Thompson-Isherwood, & Thirsk, 2009). Clients/families, mentors, and peers serve as informal socializing agents in ways that can contribute to a student’s understanding of the professional nursing role. As preceptors, other nurses and clinical faculty model desirable nursing role behaviors; students begin to identify with them and learn the normative expectations associated with the professional nursing role.

The last phase of the socialization process focuses on an internalization of professional norms and values as an integral part of self. With increasing clinical experience, nursing students become self-directed and committed to the role of professional nurse.
Professional role development as a registered nurse
Professional role development does not end with graduation and licensure as a registered nurse. After graduation, standard means of continued professional development include continuing education, staff development, conference attendance, academic education, specialized training, and research activities. Professional learning occurs through informal means such as consultation, professional reading, experiential learning, giving presentations, and self-directed activities. At advanced practice levels, nurses are required to complete a certain level of continuing education activities within designated time frames to maintain their specialty certification.
From Novice to Expert: Process of Skill Acquisition: Patricia Benner (1984, 2000; Norman, 2008) describes five developmental stages of increasing proficiency associated with the professional nursing role: novice, advanced beginner, competence, proficiency, and expert. The first developmental stage is referred to as the novice stage. With limited nursing experience, novice nurses need structure and tend to compare clinical findings with the textbook picture because they lack the practice experience to do otherwise. Theoretical knowledge and confidence in the expertise of more practiced nurses serve as guides to practice. Veteran nurses can re-experience the novice stage any time that nurse makes a career change and enters a new clinical area or specialty, never having had experience with a particular client population (Thomas, 2003).
In stage 2, the advanced beginner stage, nurses understand the basic elements of practice and can organize and prioritize clinical tasks. Although clinical analysis of health care situations occurs at a higher level than strict association with the textbook picture, the advanced beginner is only able to partially grasp the unique complexity of each client’s situation.
Stage 3, the competence stage, occurs 1 to 2 years into nursing practice. The competent nurse is able to easily “manage the many contingencies of clinical nursing” (Benner, 1984, p. 27). Nurses in this stage begin to practice the “art” of nursing. The nurse views the clinical picture from a broader perspective and is more confident about his or her role in health care.
Stage 4, the proficiency stage, occurs 3 to 5 years into practice. Nurses in this stage are self-confident about their clinical skills and perform them with competence, speed, and flexibility. The proficient nurse sees the clinical situation as a whole, has well-developed psychosocial skills, and knows from experience what needs to be modified in response to a given situation (Benner, 1984). Stage 5, expert, is marked by a high level of clinical skill and the capacity to respond authentically and creatively to client needs and concerns. Expert nurses can recognize the unexpected and work with it creatively. They demonstrate mastery of technology, sensitivity in interpersonal relationships, and specialized nursing skills in all aspects of their caregiving. Being an expert nurse is not an end point; nurses have the professional and ethical responsibility to continuously upgrade and refine their clinical skills through professional development and clinical skill training. Table 7-3 identifies behaviors associated with different levels of Benner’s model (Norman, 2008).
TABLE 7-3
Benner’s Stages of Clinical Competence
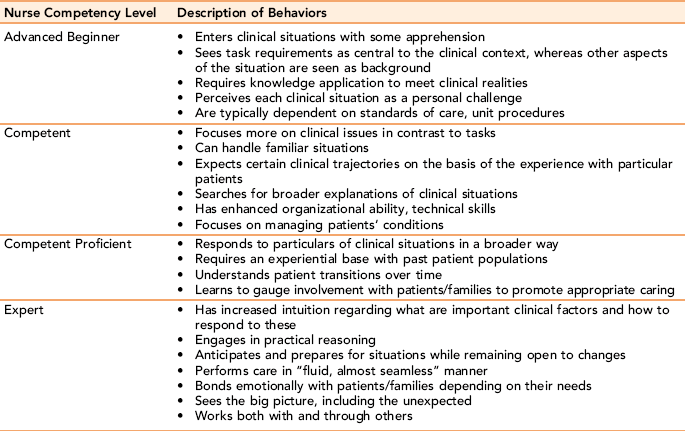
From Norman V: Uncovering and recognizing nurse caring from clinical narratives, Holistic Nursing Practice 22(6):324, 2008, by permission.
Mentoring: Expert or seasoned nurses often serve as mentors for their less-experienced colleagues. Mentoring is defined as a special type of professional relationship in which an experienced nurse or clinician (mentor) assumes a role responsibility for guiding the professional growth and advancement of a less-experienced person (protégé). Yonge, Billay, Myrick, and Luhanga (2007) make several distinctions between mentorship and preceptorship. A mentoring relationship can last over several months or years, whereas the assigned relationship between a preceptor and less experienced nurse is a short-term relationship with a defined end date focused on clinical teaching and role modeling. The mentor relationship is broader and more personal. Nurses choose a mentor rather than having one assigned.
Each mentoring experience is unique because of the people and situations involved. Excellent mentors demonstrate role expertise and model the highest levels of personal professionalism. They share values and tips for success, and provide support, structure, and challenges to the mentee or protégé. In many instances, they help facilitate contacts with significant people. Benefits to the mentor include satisfaction in seeing the achievements of the mentee and expansion of clinical excellence through interacting others. Hoffman, Harris, and Rosenfield (2008) suggest that mentoring of students in interprofessional education should contain the following elements:
Networking: Networking is an essential component of personal role development, and ultimately of advancing the status of professional nursing roles in health care delivery systems. Professional networking is defined as “establishing and using contacts for information, support, and other assistance in order to achieve career goals” (Puetz, 2007, p. 577). Nurses can use networking when they are in the market for a new job, need a referral, want to receive or share information about an area of interest, or need assistance with making a career choice. For example, if you want to write an article, you might want to discuss your ideas and get guidance from someone who is published.
Networking contacts can be with peers from as close as the nursing unit on the floor below, or people you meet at an international professional conference. Participating in activities of nursing organizations or continuing education events provides fertile opportunities for networking. Having business cards with you and following up with a thank-you e-mail or note is helpful.
Networking can offer professional opportunities for developing new ideas and receiving feedback that might not otherwise be available. Through networking contacts, nurses can communicate their expertise and share their ideas while gathering information from their contacts. This give and take of information is often the bridge to developing or strengthening collaborative relationships with others in the field. For example, extensive networking among oncology nurses was the impetus for the formation of the Oncology Nursing Society. Networking is closely associated with coordination and collaboration activities, and is destined to become increasingly important in determining the future impact of advanced practice nursing.
Applications
Professional role behaviors with colleagues
Developing productive role relationships with other professionals does not just happen. Professional role behaviors and strong relationships with nursing and other professional colleagues include full acceptance of one’s fair share of the workload. Masters (2005) asserts that if nurses are to engage in interprofessional work relationships, they must be able to clearly articulate professional nursing values. Development of supportive, dependable relationships with coworkers—with those you dislike as well as with those you can work with easily—is essential. Maintaining zero tolerance for gossip and criticism helps establish you as a professional with ethical integrity and worthy of trust.
Respecting the views of other disciplines and communicating in an organized, thoughtful manner has an impact on how practitioners from other disciplines perceive the nurse’s role and value as competent health care professionals. Using critical thinking, focused communication skills, and professional behaviors in interactions with professional colleagues is just as important as it is with clients and their families.
How nurses present their ideas in writing and speaking is critical. If you use e-mails to communicate, remember that your e-mail is a reflection of you as a professional person. Use complete, well-thought-out sentences, and check punctuation, grammar, and spelling. Likewise, voice-mail messages should be professional in content and delivery.
Verbal communication with professional colleagues
When communicating with professional colleagues, it is important to remain sensitive to the tasks at hand, and to develop an understanding of how the work of different disciplines affects the nurse’s work and contributes to overall treatment goals. Collaboration in joint decision making and coordination of care with colleagues requires knowing when to hold and when to let go of ideas and opinions. Most of the time, decisions are not either/or processes, but it is easy to lose sight of alternative options. Placing issues in order of priority is a useful organizing strategy for assessing, defining, and clarifying problems. Persistence and a good sense of humor are essential characteristics of honest interpersonal relationships with professional peers.
E-mail or memos can provide quick routine information that does not require discussion. Face-to-face interaction or telephone conversations are preferred for communicating in the professional environment about difficult or emotional issues that could be misinterpreted. Serving as an informed resource to other providers helps build rapport and encourages others to work with you to achieve relevant treatment and organizational goals.
Self-awareness
Self-awareness is an essential aspect of effective professional relationships with colleagues and a necessary antecedent to the full development of the professional role in nursing. Malloch and Porter-O’Grady (2005) assert that “knowing from the internal self what needs to be done and living those beliefs and values in the real world marks the leader’s journey” (p. 101).
Professional self-awareness promotes recognition of the need for continuing education, the acceptance of accountability for one’s own actions, the capacity to be assertive with professional colleagues, and the capability of serving as a client advocate when the situation warrants it, even if it is uncomfortable to do so. Exercises 7-4 and 7-5 are designed to help you explore the use of personal strengths in professional role development.
Professional rights
All health professionals, including nurses, have rights as well as significant responsibilities in interprofessional relationships with colleagues. Box 7-3 lists the American Nurses Association (2002) Bill of Rights for Registered Nurses. Rights carry with them corresponding responsibilities. Think about your professional collegial relationships and your dual professional commitment to self and others. Think about the professional values identified in this textbook, and reexamine the components of professionalism. Each of those components is basically a professional responsibility. Add your ideas for rights next to those responsibilities. Exchange ideas about professional rights and responsibilities with others.
Creating supportive work environments
A responsive work environment that values nurses and is committed to quality client-centered care attracts nurses and improves clinical outcomes for clients. Likewise, nurses who are enthusiastic, competent, dependable, adaptable, and responsible are key variables in creating a satisfying, quality work environment. In a study of what types of environmental support create satisfaction for professional nurses, Kramer and Schmalenberg (2002) uncovered the following factors chosen by the majority of the nurses surveyed:
• Working with other nurses who are clinically competent
• Good nurse-physician relationships and communication
• Nurse autonomy and accountability
• Supportive nurse manager-supervisor
• Control over nursing practice and practice environment
• Support for education (in-service, continuing education, etc.)
In an effort to develop and support work environments favorable to nurses, the American Nurses Association, through its American Nurses Credentialing Center (ANCC), developed the Magnet Recognition Program in 1993. Over the years, magnet recognition has become “the global standard for excellence in nursing practice” (Morgan, 2009, p. 105).
Magnet recognition
The magnet recognition program recognizes nursing excellence in health care institutions and agencies, and identifies them as work environments that act as a “magnet” for professional nurses desiring to work there because of the institutions’ excellence (American Nurses Credentialing Center [ANCC] 2004). In 2008, the magnet model was redesigned to include five interactive elements known to support excellence in nursing practice work environments (see Figure 7-2). Characteristics of a magnet culture include:
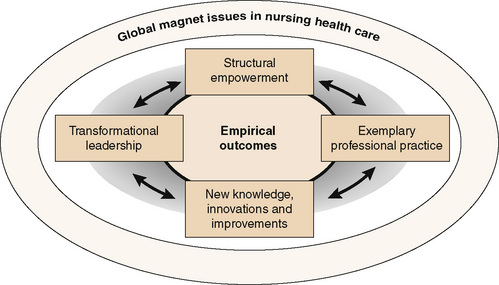
Figure 7-2 Magnet model components. (Developed from Morgan S: The magnet (TM) model as a framework for excellence, Journal of Nursing Care Quality 24(2):105–108, 2009 (p. 106).
• Positive interdisciplinary professional relationships
• Control over and autonomy in nursing practice
• Client-centered care for clients and families
• Adequate staffing and nurse-manager support (ANCC, 2006).
A magnet health care facility is characterized as one in which nurses have a high level of job satisfaction and lower staff nurse turnover, exemplary professional practice, and demonstrate commitment at every nursing level to effective, efficient, quality care (American Nurses Credentialing Center). Nurses in a magnet work environment are valued and have a strong voice in decision making about care delivery. They are encouraged and rewarded for involvement in shaping research-based nursing practice. Staffing ratios are viewed as appropriate, and the hospital demonstrates excellent treatment outcomes and client satisfaction. Communication among health professionals is open, and there is an appropriate mix of health care personnel to ensure quality care. Exercise 7-6 can help you think about how you would see yourself in the professional nursing role in the future.
Becoming key players in a global health care arena
Malloch and Porter-O’Grady (2005) suggest that we are living in an information-based societal infrastructure that is primarily relational and that functions horizontally in a global world without boundaries. Professional nursing requires an expanded set of skill competencies in the 21st century, as presented in Table 7-4.
TABLE 7-4
Old versus New Skill Sets for Professional Nurses in the 21st Century
| Employee | Knowledge Worker |
| Functional analysis | Conceptual synthesis |
| Manual dexterity | Competent integrated care |
| Fixed skill set | Mobile skill set |
| Process, value-based practice | Outcome-based practice |
| Individual practice | Interdisciplinary team performance |
Modified from Mallach K, Porter-O’Grady T: A new vessel for leadership: new rules for a new age. In The quantum leader: applications for the new world of work, Sudbury, MA, 2005, Jones and Bartlett.
Making the role of the professional nurse visible in the 21st century is a task that nurses must undertake to strengthen the public’s recognition of the nursing profession in an interdisciplinary health care delivery system. Although nurses are the largest professional group in the health care workforce (Hassmiller & Cozine, 2006), their role is not as visible as it should be. Neither physicians nor nurses seem to fully appreciate the depth of the nurse’s contribution to health care delivery (Coombs, 2004). In some ways, the work of the nurse is invisible until a crisis such as the nursing shortage brings the work of nurses to the forefront of people’s attention. Individual nurses and nursing organizations need to work together to strengthen the professional nursing role.
In addition to defining our professional roles in ways that are understandable, nurses need to project a positive activist image of the professional nursing role within their communities by
• Developing partnerships with clients, health care professionals, policy makers, and community agencies in the care of vulnerable populations
• Reflecting on and documenting what nurses do and the broad scope of services they provide for the public
• Participating as members of interdisciplinary teams and multidisciplinary groups with defined expertise as nurses to address significant health care issues from a nursing perspective
• Maintaining competence and acting in a professional manner
• Advocating for systems of care that provide adequate accessible health care for all people
• Developing and participating in continuing education programs to ensure continued competence as a professional nurse
• Promoting the public and professional understanding of the professional nursing role
• Contributing to ethical discussions that support principled practices in clinical settings
Professional role behaviors in nurse-client relationships
A nurse’s first professional role responsibility is to the client. Acting in a professional manner at all times is essential to maintaining the integrity of nursing as a profession. Expected professional role behaviors in nurse-client relationships emphasize the following qualities:
• An ability to view clients as individual, holistic beings
• Respect for the basic human dignity of all clients, regardless of differences from oneself
• An attitude of cultural openness and tolerance for divergent ways of thinking
• Sensitivity to individual clients’ ability to access health care and adhere to prescribed regimens
• An understanding of the impact that illness and/or disability may have on clients
• Adherence to nursing standards of care
• Use of research evidence to improve nursing practice (Masters, 2005, pp. 156–157)
Role relationships with a client can affect the quality of nursing care in the nurse-client relationship when the worth of the client as a person, for example, is judged on the basis of socioeconomic status, level of education, ethnicity, health state, or level of consciousness. Perceptions of role relationships can affect effective treatment decision making. For example, roles become important when questioning a health care provider’s professional judgment is not considered an appropriate behavior in the client’s culture, or when the family, rather than the client, is culturally expected to make important health care decisions.
Professional performance behaviors in the nurse-client relationship include much more than simple caring; they require a sound knowledge base, as well as specific technical and interpersonal competencies. On a daily basis, nurses must collect and process multiple, often indistinct pieces of behavioral data. Nurses work creatively with clients and families to come up with workable solutions that are realistic and in tune with the client’s beliefs, values, and preferences. Through words and behaviors in relationship with other health care providers and agencies, nurses consistently serve as advocates for their clients and family members.
Today’s nurse functions in a high-tech, managed health care environment in which the human caring aspects of nursing are easier to overlook. Unique challenges to the nurse-client relationship include shorter client contacts, decreased continuity, technology, and lower levels of trust in relation to these factors. Yet, the nurse-client relationship will become increasingly important in helping clients feel cared for in a health care environment that sometimes neglects the psychosocial needs of clients in favor of cost-effectiveness and efficient use of time.
In today’s health care environment, clients are expected to take an active role in self-management of their condition to whatever extent is possible. The expectation is for an equal partnership, with clients having shared power and authority as joint decision makers in their health care. With a client-centered model of health care delivery, the client’s thoughts, concerns, and questions are welcomed and encouraged. Every decision related to the client’s diagnosis and treatment should be a shared determination made with the medical team based on combined input and joint responsibility for implementing the recommendations. This use of the client’s self-knowledge and inner resources allows nurses to more effectively respond to client needs.
Client Rights and Responsibilities: The American Hospital Association (AHA, 2003) has developed a brochure outlining the rights and responsibilities of patient care partnership in lieu of its former Patient’s Bill of Rights. It is accessible in multiple languages on the AHA Web site. Hospitals today have copies of comprehensive patient rights posted on their Web site. Written copies are given to clients on admission. A sample listing of common patient rights and responsibilities is provided in Box 7-4.
Advocacy roles in the nurse-client relationship
Merriam-Webster’s Dictionary (2009) defines advocate as “one that pleads the cause of another; one that supports or promotes the interests of another.” Nurses are advocates for clients every time they protect, defend, and support a client’s rights, and/or intervene on behalf of clients who cannot do so for themselves. The ANA (2001) affirms advocacy as an essential role in its Code of Ethics for Nurses, stating, “The nurse promotes, advocates for, and strives to protect the health, safety and rights of the patient.”
Clients who benefit from advocacy fall into two categories: those who need advocacy because of vulnerability caused by their illness, and those who have trouble successfully navigating the health care system. Nursing actions that constitute client advocacy include facilitating access to essential health care services for clients, ensuring quality care, protecting client rights, and acting as a liaison between clients and the health care system to procure quality care.
A key means of employing client advocacy is the nurse-client relationship (Negarandeh, Oskouie, Fhmadi, Nikravesh, & Hallberg, 2006). Within the relationship, nurses listen carefully to clients, help them foresee potential difficulties, answer questions honestly, and apply the clinical knowledge and skills identified in Box 7-5 for the benefit of the client.
The goal of advocacy support is to empower clients and to help them attain the services they need for self-management of health issues. Examples of individuals needing advocacy include survivors of domestic violence, chronically mentally ill clients, pregnant teenagers, the homeless, frail elders—in fact, virtually anyone unable to act cogently on their own behalf. As health care services in the public sector become scarcer because of economic considerations, advocacy becomes an even greater emphasis. Several authors (Welchman and Griener, 2005; Mahlin, 2010) argue that nursing’s professional organizations need to take up the gauntlet to collectively advocate for resolution of systemic client care issues in health care settings. For more information on nurse involvement in advocacy at the community level, see Chapter 24.

Advocacy should support client autonomy. Zomorodi and Foley (2009) note the importance of differentiating advocacy strategies from paternalism in which the nurse decides what is best for the client. Clients need to be in control of their own destiny, even when the decision reached is not what you as the nurse would recommend for the client’s health and well-being. You need to recognize when to speak for the client and when to encourage the client to speak up. In general, encouraging clients to take responsibility to speak on their own behalf is more effective.
To be effective, the nurse’s advocacy efforts should be systematically implemented and related to client identified needs, beliefs and values, and preferences. Questions you might ask include: (a) What does the client believe is the most pressing problem? (b) What supports (e.g., family, minister, rabbi, social services) are in place? (c) What health or social services is the client familiar with or resistant to considering? A client’s sense of powerlessness can decrease when the answers to these questions become the starting points for developing realistic solutions to difficult problems. When advocacy efforts include referrals to community resources, factors to be considered include compatibility with the client’s expressed need, financial resources, accessibility (time as well as place), and ease of contact.
Client advocacy sometimes provides a connective link between ethics and the law. Nurses must be willing and able to take a stand in situations involving poor medical management of a client. This is not easy, when risk to employment or possibility of censure is associated with this form of client advocacy. On the other hand, being too cautious or having misplaced loyalties to colleagues that interfere with appropriate protective advocacy can become a legal as well as an ethical issue. Sometimes, the only person willing to defend or promote the cause of the client is the nurse.
In the following case example, a client admitted to postanesthesia care unit (PACU) suddenly had a significant change in his vital signs. The nurse called the operating room (OR), but the surgeon was scrubbing for the next operation and said he would call her later.
Exercise 7-7 provides a clinical situation in which the nurse’s advocacy role is in conflict with traditional nursing and medical advice. Sometimes the nurse serves as dual advocate for the client and a family member. For example, in a child abuse situation, nurses act as an advocate of the child by taking the steps necessary to provide a protective and safe environment for the child, including reporting abuse situations. The same nurse can be an advocate for the parents by referring them to appropriate community resources and helping them develop more productive methods for coping with situational stressors.
Role performance as a nursing diagnosis
Role performance disturbance has been designated by NANDA (2009) as a nursing diagnosis. Healthy People 2010 identifies quality of life as a priority goal. Quality of life and role performance are interconnected. How effectively a person is able to function within expected roles influences his or her reputation within society and affects his or her sense of self-esteem. That role relationships and performance matter to people as essential elements of their well-being is evidenced in the emergence of symptoms of depression, feelings of emptiness, and even suicidal thoughts when a significant personal or professional role ceases to exist. Examples of lost role relationships include job loss, divorce, retirement, death of a significant person, and a chronic or debilitating illness.
For clients, significant changes in their behavioral ability to function in expected roles as a result of illness, disability, or other life changes can be devastating. Alterations in normal roles, compromised role performance, and changes in role relationships are common sources of frustration and emotional pain to clients and families. The effects of alteration in role performance and role relationships within the family and work environment are such an important dimension of self-concept that they warrant a nursing diagnosis: ineffective role performance.
Nurses need to be sensitive to the changes in role relationships that even a minor illness or injury produces. An altered health status can change an individual’s social role from one of independent self-sufficiency to one of vulnerability and dependence on others. For example, when lack of physical stamina after a heart attack prevents a woman from fulfilling her customary caregiving roles in the home, she can experience a loss of self-confidence and personal value that can affect her rehabilitation (Arnold, 1997).
Most people do not assume the sick role voluntarily. At the hospital door, the client forsakes, either temporarily or permanently, recognized social roles in the family, work situation, and community. Regardless of how competent the person may be in other life roles, questions about role performance inevitably arise when illness strikes. Often, clients must learn new role behaviors that are unfamiliar and unsettling to previously held self-concepts. Illness or disability, whether actual or perceived, also strain family equilibrium and coping abilities. Sometimes alterations in role performance are intimately associated with the illness and will never be regained.
Clients and their families need the compassionate support of the nurse to incorporate the meaning of role changes occasioned by their illness or disability into an otherwise basically healthy self-concept. Asking open-ended, focused questions about the client’s family relationships, work, and social roles helps the nurse to accurately assess potential alterations in role relationships in personal, social, and work relationships (Box 7-6). The questions should be asked in a conversational manner at a pace the client can tolerate.
With shortened hospital stays, potential role changes should be addressed as part of discharge planning or follow-up in the community, or both. Nurses working in long-term rehabilitation settings can help their clients look at transferable skills and personal strength they may possess that could be used in a different way, for example, good communication skills, persistence, patience, and so on. Many times clients are not aware of transferable skills that can be put to good use when previous capabilities are no longer available to them. Exercise 7-8 can help you understand the nature of transferable skills.
Health is a value-laden concept for many people. Preconceived notions of role disruption for an ill or disabled person occur more commonly when the illness is protracted, recurrent, or seriously role disruptive. Even when the person is fully capable of resuming previous role responsibilities after a documented extended illness, it is not uncommon for them to find that they are being “laid off” when they return to work.
Nurses need to help clients learn how to respond to subtle and not-so-subtle discriminatory actions associated with people’s lack of understanding of the client’s health situation.
Summary
How nurses perceive their professional role and how they function as a nurse in that role has a sizable effect on the success of interpersonal communication in the nurse-client relationship. The professional nursing role should be evidenced in every aspect of nursing care, but nowhere more fully than in the nurse-client relationship. A professional nurse’s first role responsibility is to the client. Because hospitals no longer are the primary settings for nursing practice, nurse practice roles take place in nontraditional and traditional community based health care settings. Advanced practice roles include the nurse practitioner, clinical nurse specialist, certified nurse-midwife, and nurse anesthetist. Two new roles, the CNL and the DNP, were introduced in 2003. A new concept in nursing education is interdisciplinary course
Nurses learn professional role behaviors through the process of professional role socialization. Professional development as a nurse is a lifelong commitment. Benner’s five developmental stages of increasing proficiency describe the nurse’s progression from novice to expert. Mentorship and continuing education assist nurses in maintaining their competency and professional role development. Interdisciplinary collaboration and health care teams have stimulated the development of shared elective classes involving two or more disciplines, for example, nursing and medicine or pharmacy.
Role performance disturbance has been designated by NANDA (2009) as a nursing diagnosis. Quality of life and role performance are interconnected. Examples of lost role relationships include job loss, divorce, retirement, death of a significant person, and a chronic or debilitating illness. Clients and their families need the compassionate support of the nurse to incorporate the meaning of role changes occasioned by their illness or disability into an otherwise basically healthy self-concept. Nurses can help clients and families identify and use transferable skills learned in previous roles in different ways.
References
American Association of Colleges of Nursing. Values, qualities, and behaviors associated with professionalism in nursing practice. Washington, DC: Author, 1986.
American Association of Colleges of Nursing. The essentials of baccalaureate education for professional nursing practice. Washington, DC: Author, 2008.
American Association of Colleges of Nursing Working paper on the role of the clinical nurse leader, 2003. Available online:, http://www.aacn.nche.edu/Publications/WhitePapers/ClinicalNurseLeader.htm. [Accessed August 28, 2009].
American Association of Colleges of Nursing AACN position statement on the practice doctorate in nursing, Washington, DC, American Association of Colleges of Nursing, 2004. Available online:, http://www.aacn.nche.edu/DNP/DNPPositionStatement.htm. [Accessed August 28, 2009].
American Hospital Association The patient care partnership; understanding expectations, rights and responsibilities, Atlanta, Author, 2003. Available online:, http://www.aha.org/aha/issues/Communicating-With-Patients/pt-care-partnership.html. [Accessed December 30, 2009].
American Nurses Association. Know your rights: ANA’s Bill of Rights arms nurses with critical information. Am Nurse. 2002;34(6):16.
American Nurses Association. Code of ethics for nurses with interpretive statements. Silver Spring, MD: American Nurses Publishing, 2001.
American Nurses Credentialing Center. Magnet recognition program: recognizing excellence in nursing services: application manual. Silver Spring, MD: Author, 2004.
American Nurses Credentialing Center, Objectives of the magnet recognition program. In ANCC Magnet Recognition Program, revised April 6, 2006. Available online:, http://www.nursingworld.org/ancc/magnet/index.html.
Anthony, S., Landeen, J. Evolution of Canadian nursing curricula: a critical retrospective analysis of power and caring. Int J Nurs Educ Scholarsh. 2009;6(1, Article 18):1–14.
Arnold, E. The stress connection: women and coronary heart disease. Crit Care Nurs Clin North Am. 1997;9(4):565–575.
Aveyard, H., Edwards, S., West, S. Core topics of health care ethics: the identification of core topics for interprofessional education. J Interprof Care. 2005;19(1):63–69.
Benner, P. From novice to expert: excellence and power in clinical nursing practice. Menlo Park, CA: Addison-Wesley, 1984.
Benner, P. From novice to expert: excellence and power in clinical nursing practice, comm ed. New York: Prentice Hall, 2000.
Bishop, A.H., Scudder, J.R., Jr. Nursing ethics: therapeutic caring presence. Boston: Jones and Bartlett, 1996.
Chaudhary, N., Sriram, S. Dialogues of the self. Culture & Psychology. 2001;7(3):379–392.
Cohen, H. The nurse’s quest for a professional identity. Menlo Park, CA: Addison-Wesley, 1981.
Coombs, M.A. Power and conflict between doctors and nurses: breaking through the inner circle in clinical care. London: Routledge, 2004.
Donaldson, S.K., Crowley, D.M. The discipline of nursing. Nurs Outlook. 1978;26(2):113–120.
Erickson, J., Ditomassi, M. The clinical nurse leader: new in name only. J Nurs Edu. 2005;44(3):99–100.
Flexner, A., Is social work a profession?. Proceedings of the National Conference on Social Work, 1915. [New York].
Fronek, P., Kendall, M., Ungerer, G., Malt, J., Eugard, E., Geraghty, T. Towards healthy professional-client relationships: the value of an interprofessional training course. J Interprof Care. 2009;23(1):16–29.
Gugerty, B. Nursing at a crossroads—education, research, training, and informatics. J Healthc Inf Manag. 2007;21(1):12–14.
Hassmiller, S., Cozine, M. Addressing the nurse shortage to improve the quality of patient care. Health Aff. 2006;25(1):268–274.
Hegarty, J., Condon, C., Walsh, E., Sweeney, J. The undergraduate education of nurses: looking to the future. Int J Nurs Educ Scholarsh. 2009;6(1, Article 17):1–11.
Hegyvary, S. An agenda for nursing as a means to improve health. J Nurs Scholarsh. 2007;39(2):103–104.
Herbert, C., Changing the culture: interprofessional education for collaborative patient centered practice in Canada. J Interprof Care, 2005;Suppl 1:1–4.
Hoffman, S., Harris, A., Rosenfield, D. Why mentorship matters: students, staff and sustainability in interprofessional education. J Interprof Care. 2008;22(1):103–105.
Institute of Medicine (IOM). Health professions education: a bridge to quality. Washington, DC: National Academies Press, 2003.
Joint Commission. The Health care at the crossroads: addressing the evolving nursing crisis. Washington, DC: Author, 2002.
Kramer, M., Schmalenberg, C. Staff nurses identify essentials of magnetism. In: McClure M., Hinshaw A.S., eds. Magnet hospitals revisited: attraction and retention of professional nurses. Washington, DC: American Nurses Publication, 2002.
Mahlin, M. Individual patient advocacy, collective responsibility and activism within professional organizations. Nurs Ethics. 2010;17(2):247–254.
Malloch, K., Porter-O’Grady, T. The quantum leader: applications for the new world of work. Sudbury, MA: Jones and Bartlett, 2005.
Margalit, R., Thompson, S., Visovsky, C., et al. From professional silos to interprofessional education: campuswide focus on quality of care. Qual Manag Health Care. 2009;18(3):165–173.
Masters, K. Role development in professional nursing practice. Sudbury, MA: Jones and Bartlett, 2005.
Merriam-Websters Dictionary. Available online: http://www.merriam-webster.com/dictionary/advocate. [Accessed December 30, 2009].
Morgan, S. The magnet (TM) model as a framework for excellence. J Nurs Care Qual. 2009;24(2):105–108.
Mundinger, M. Who’s who in nursing: bringing clarity to the doctor of nursing practice: 2005. Nurs Outlook. 2005;53(4):173–176.
NANDA Nursing diagnosis 2009–2011. Definitions and classification (NANDA nursing diagnosis). Ames Iowa: John Wiley & Sons Ltd, 2009.
Negarandeh, R., Oskouie, F., Fhmadi, F., Nikravesh, M., Hallberg, I.R., Patient advocacy: barriers and facilitators. BMC Nursing, 2006;5:3. Available online:, http://www.biomedcentral.com/1472-6955/5/3. [Accessed September 9, 2009].
Neil, K., McCoy, A., Parry, C., et al. The clinical experiences of novice students in nursing. Nursing Education. 1998;23(4):16–21.
Oandasan, I., Reeves, S. Key elements for interprofessional education. Part I: The learner, the educator and the learning context. J Interprof Care. 2005;19:21–38.
O’Connell, M. Personal communication, 2009. [June].
Odom, J. The nurse as patient advocate. J Perianesth Nurs. 2002;17(2):75–76.
Paton, B., Thompson-Isherwood, R., Thirsk, L. Preceptors matter: an evolving framework. J Nurs Educ. 2009;48(4):213–216.
Pecukonis, E., Doyle, O., Bliss, D. Reducing barriers to interprofessional training: Promoting interprofessional cultural competence. J Interprof Care. 2008;22(4I):417–428.
Pew Health Professions Commission. Health professions education for the future: schools in service to the nation. San Francisco: Pew Commission, 1993.
Puetz, B. Networking. Public Health Nurs. 2007;24(6):577–579.
Roberson, M. Our diversity gives us strength: comment and opinion. Am Nurse. 1992;24(5):4.
Rodts, M., Lamb, K. Transforming your professional self: encouraging lifelong personal and professional growth. Orthop Nurs. 2008;27(2):125–131.
Thomas, J. Changing career paths: from expert to novice. Orthop Nurs. 2003;22(5):332–334.
Walsh, C.L., Gordon, M.F., Marshall, M., Wilson, F., Hunt, T. Interprofessional capability: a developing framework for interprofessional education. Nurse Educator Practitioner. 2005;5:230–237.
Welchman, J., Griener, G. Patient advocacy and professional associations: individual and collective responsibilities. Nurs Ethics. 2005;12(3):296–304.
Willis, D.G., Grace, P.J., Roy, C. A central unifying focus for the discipline: facilitating humanization, meaning, choice, quality of life, and healing in living and dying. Adv Nurs Sci. 2008;31(1):E28–E40.
Yonge, O., Billay, D., Myrick, F., Luhanga, F. Preceptorship and mentorship: not merely a matter of semantics. Int J Nurs Educ Scholarsh. 2007;4(1, Article 19):1–13.
Zomorodi, M., Foley, B.J. The nature of advocacy vs. paternalism in nursing: clarifying the ‘thin line’. J Ad Nurs. 2009;65(8):1746–1752.