Losses and Endings
Communication Skills at End of Life
At the end of the chapter, the reader will be able to:
1 Describe the concept of loss.
2 Describe the stages of death and dying.
3 Discuss the concept of palliative care.
4 Discuss theory-based concepts of grief and grieving
5 Define grief and describe common patterns of grieving.
6 Describe the nurse’s role in palliative care.
7 Discuss key issues and approaches in end-of-life (EOL) care.
8 Identify cultural and spiritual needs in EOL care.
9 Describe supportive strategies for children.
This chapter examines the nurse-client relationship in the context of palliative and EOL care. The chapter identifies theory frameworks related to the stages of dying and the process of grief and grieving. The Application section discusses the process of identifying and responding to client and family needs in EOL care. This chapter spotlights the communication issues in the care nurses provide to dying clients and as they meet the needs of grieving families. Helping clinicians recognize and cope with the high stress of providing quality EOL care is also addressed.
Basic concepts
Corless (2001) defines loss as “a generic term that signifies absence of an object, position, ability or attribute” (p. 352). Important losses occur as part of everyone’s personal experience. Anything or anyone in whom we invest time, energy, or a part of ourselves can be experienced as a loss. When people suffer the loss of someone or something important to them, there is a loss of their sense of “wholeness” and a break in the person’s expected life story (Attig, 2004). The loss remains in that person’s mind, even with the passage of time (Levine, 2005). When a fresh loss occurs, previous losses are remembered. Consider the theme of loss in each of the following normal life experiences:
• A wife loses a 35-year-old marriage through divorce
• A couple loses their dream home through foreclosure
The feelings associated with loss differ only in the intensity with which one experiences them. Mark Twain noted: “Nothing that grieves us can be called little; by the eternal laws of proportion a child’s loss of a doll and a king’s loss of a crown are events of the same size” (Mark Twain Quotations, 2002). Some losses are unfinished; others occur simultaneously or sequentially.
Multiple losses occurring over a short period intensify the experience. Older adults will experience the deaths of friends and family members with greater frequency. One loss can precipitate multiple losses. For example, the client with Alzheimer’s disease doesn’t simply lose memory. Accompanying cognitive loss are profound losses of role, communication, independence, and loss of identity. Lifestyle changes are required to accommodate for the cognitive loss.
Multiple losses complicate the grieving process and usually take longer to resolve. Helping people focus on one relationship at a time instead of trying to address the losses together is helpful. Acknowledgment of the differences between single and multiple loss helps put the enormity of multiple losses into perspective (Mercer & Evans, 2006). Exercise 8-1 is designed to help you understand the dimensions of personal loss.
Death: the final loss
Death is associated with loss; it signals the end of all that life holds on this earth: successes, failures, relationships, careers, laughter, and pain. More than a biological event, dying has spiritual, social, and cultural features that help people make sense of its meaning. Dobratz (2002) describes a human life pattern in dying patients that is “shaped by self-integration, inner cognition, creation of personal meanings, and connection to others and a higher being” (p. 139).
Silveira and Schneider (2004) suggest that “planning for the end of life is planning for the unknown” (p. 349). Although death is a necessary part of the circle of life, dying is often feared, even if people believe in an afterlife. As Chenitz (1992), a nurse dying of AIDS noted, “Like many people with AIDS, I am not afraid of death. I am afraid of dying. The dying process and how that will be handled is of great concern to me” (p. 454).
When asked, most clients identify fear of pain and of experiencing their last phase of life unaccompanied as their two principal fears (Pashby, 2010). Clients and families need to know that help is always available from someone knowledgeable, who cares about them, and is willing to anticipate and respond to their personal care needs as they appear.
Nurses are not immune from these fears. It is often difficult for nurses to maintain a balance between their own sensitivity to death and well-being, and providing the empathy and support needed by clients and families. This is why self-awareness about death and dying issues is so important in providing palliative care.
Theoretical framework: stages of dying
Elisabeth Kübler-Ross (1969) provides a five-stage framework for understanding the process of dying. Not every person experiences each stage.
Denial
Kübler-Ross (1969) characterizes denial stage as the “No, not me” stage. Nurses should be sensitive to the client’s need for denial. Some people remain in the denial stage throughout their illness; their right to do so should be respected.
Anger
Kübler-Ross (1969) refers to anger as the “Why me?” stage, associated with feelings about the unfairness of life, or anger with God. Feelings get projected on those closest to the client. The client lashes out at family, friends, and staff members. Those closest to the client may need support in recognizing that the anger is not a personal attack.
Bargaining
Kübler-Ross (1969) refers to the bargaining stage as the “Yes, me, but … I need just a little more time.” The bargaining stage involves pleading for time extension or special consideration. Bargaining is not a futile exercise. Sometimes the extra energy a person gets by trying to postpone death can provide a meaningful moment for client and family; consider the father, wanting to stay alive for his daughter’s wedding. By supporting hope and avoiding challenges to the client’s reality, the nurse facilitates the process of living while dying.
Depression
Kübler-Ross (1969) characterizes the depression stage as the “Yes, me” stage, accompanied by depressive feelings. Mood swings and depressive feelings are hard for families to tolerate, but very common. Nursing strategies in this stage include helping clients to accept depression as being a normal response, and being present to clients and families as an empathetic, listening witness to their experience.
Acceptance
Pashby (2010) notes that the theoretical stages seem to mirror the physiologic decline experienced at the EOL. Clients who are weak and bedridden with declining consciousness as death approaches come more readily to the final stage of acceptance. The acceptance stage is characterized by an acknowledgment of the inevitable EOL. As the client approaches death, there is a gradual detachment from the world, and the person is almost “void of feeling” (Kübler-Ross, 1969, p. 124). Because of this, there can be a sense of peace.
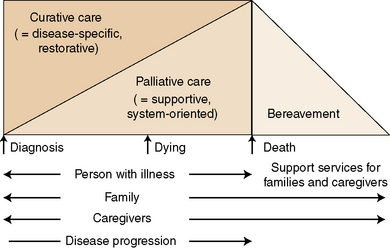
Palliative care
Palliative care is defined as “a clinical approach designed to improve the quality of life for clients and families coping with a life threatening illness” (Davies & Higginson, 2004, p. 14). It is recognized as a philosophy of care and as an emerging practice discipline. The dimensions of palliative care identified by the World Health Organization (WHO) are presented in Box 8-1.
Clients are admitted to palliative care services when the client has a life-limiting disease with care needs that will go beyond traditional modes of medical intervention (Galanos, 2004; Morrison & Meier, 2004). Palliative care is unique in that it includes involved family members and the client with the life-limiting disease as one integrated unit of care. Clients initially admitted to palliative care services may still be receiving active treatment for their disease process to control symptoms and improve quality of life (McIlfatrick, 2007). Palliative care can augment treatment with attention directed to providing the secondary psychosocial, practical, and spiritual support services and assistance people need regarding EOL decisions and care. As the disease or disability progresses, palliative care still supports living while dying, but the focus becomes symptom management and movement toward achieving a good death, rather than active treatment. Table 8-1 identifies proposed quality measures for palliative care in the critically ill.
TABLE 8-1
Quality Measures for Palliative and End-of-Life Care by Domain
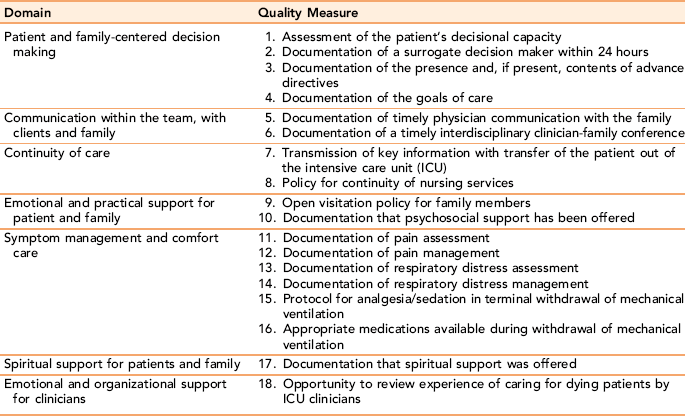
From Mularski R, Curtis J, Billings J et al: Proposed quality measures for palliative care in the critically ill: a consensus from the Robert Wood Johnson Foundation care group, Critical Care Medicine 34(11 suppl):S406, 2006.
Palliative care strategies are designed to help clients and families understand the dying process as a part of life and to assist terminally ill clients to achieve the best quality of life in the time left to them. The basic axiom for palliative EOL care is to follow what clients actually want for themselves (Silveira & Schneider, 2004). Palliative care is dedicated to supporting families as resources and as units of care themselves. After the client’s death, palliative care offers grief support for family members.
Palliative care and hospice are related concepts. A fundamental difference between the two approaches is that the palliative care team can admit and serve patients still receiving curative treatment, with no time restrictions regarding prognosis. Hospice clients must have a prognosis of 6 months or less, and cannot be receiving active medical treatment. Hospice is considered part of the continuum of palliative care; it offers a quality care environment in the last segment of life.
Nursing initiatives
Nurses have taken a leadership role in developing guidelines for quality EOL care through national initiatives. Nationally recognized nursing experts, funded by the American Association of Colleges of Nursing (AACN) and the City of Hope, have developed the End-of-Life Nursing Education Consortium (ELNEC), a national education initiative to improve EOL care in the United States. The ELNEC project targets undergraduate and graduate nursing faculty, continuing education providers, staff development educators, and pediatric and oncology specialty nurses in EOL care (AACN, 2006). Specific EOL training allows nurses to teach others and to enter into the lives of many more people facing EOL as skilled, compassionate professionals with specialized care tools (Malloy, Paice, Virani, Ferrell, & Bednash, 2008).
Concepts of grief and grieving
The concept of grief describes the personal emotions and adaptive process a person goes through in recovering from loss. Common feelings include sadness and an acute awareness of the void accompanied by recurring, wavelike feelings of sadness and loss. Certain situations, time alone, holidays, and anniversaries allow grief feelings to resurface.
Theory-based frameworks of grieving
Eric Lindemann (1944/1994) pioneered the concept of grief work based on interviews with bereaved persons suffering a sudden tragic loss. He described patterns of grief, and the physical and emotional changes that accompany significant losses. Lindemann observed that grief can occur immediately after a loss, or it can be delayed. He summarized three components of support: (a) open, empathetic communication; (b) honesty; and (c) tolerance of emotional expression as being important in grieving. When the symptoms of grief are exaggerated or absent, it is considered pathologic or complicated grief. People experiencing complicated grief may require psychological treatment to resolve their grief and move into life again.
Engel’s Contributions
George Engel’s (1964) concepts built on Lindemann’s work. He described three sequential phases of grief work: (a) shock and disbelief, (b) developing awareness, and (c) restitution.
In the shock and disbelief phase, a newly bereaved person may feel alienated or detached from normal—“literally numb with shock; no tears, no feelings, just absolute numbness” (Lendrum & Syme, 1992, pp. 24–25). Seeing or hearing the lost person, or sensing his or her presence is a normal, temporary altered sensory experience related to the loss, which should not be confused with psychotic hallucinations.
In the immediate aftermath of death, families and friends surround a person with support and opportunities to talk. This support diminishes over time. The developing awareness phase occurs slowly as the void created by the loss fully enters consciousness. There is a loss of energy, not the kind that requires sleep, but rather a desire to accomplish things without having either the organizational capacity or energy to follow through with related tasks.
Listening, identifying feelings, and having an empathetic willingness to repeatedly hear the client’s story without needing to give advice or interpretation are helpful nursing interventions (Jeffries, 2005).
The restitution phase is characterized by adaptation to a new life without the deceased. There is a resurgence of hope and a renewed energy to fashion a new life. With successful grieving, the loss is not forgotten, but the pain diminishes, and is replaced with memories that enrich and give energy to life. John Thomas (2010) describes his sense of new beginnings:
• Has one foot planted firmly in this life and the other seeking a firm footing in the spiritual realm
• Is identified with life and love rather than loss and grief
• Walks with the stride of renewal rather than the shuffle of grief; a vigorous man with an appreciation for beauty and quality
• Is confident about the future without needing a tangible GPS
• Can still embrace life knowing that the pain of loss is intense
• Can be alone without being lonely
• Faced grief head-on and reached a deeper core of self and spirituality
• Has much to give in many arenas living a life that honors my past and sharing the blessing derived from it
Contemporary models of grieving
Florczak (2008) states, “The newer worldview considers loss to be a unique, intersubjective process in which the individual maintains connections with the absent and the meaning of the experience continually changes” (p. 8). The past is not forgotten, and there is a continuous spiritual connection with the deceased, which illuminates different features of self and possibilities for fuller engagement with life. Features of past experiences with the loved one are rewoven into the fabric of a person’s life in a new form. Contemporary authors Neimeyer (2001) and Attig (2001) emphasize meaning construction as a central issue in grief work.
Patterns of grieving
Acute grief occurs as “somatic distress that occurs in waves with feelings of tightness in the throat, shortness of breath, an empty feeling in the abdomen, a sense of heaviness and lack of muscular power, and intense mental pain” (Lindemann, 1994, p. 155). Sudden traumatic deaths are more likely to stimulate acute grief reactions.
When the death is untimely (as with an accident or fatal heart attack), out of normal sequence (as in the case of a child’s death), or complicated by stigma (as with death from addiction or suicide), the challenge for the family is greater. Survivors feel more guilt, anger, and helplessness.
Suicide survivors are at a disadvantage. Survivors typically overestimate their ability to influence the suicidal behavior or outcome. They are reluctant to discuss death details because of shame or perceived stigma. Survivors usually need more support. Often they get less because people don’t know how to talk to them about suicides (Harvard Women’s Health Watch, 2009). Suicide survivor support groups can offer the specialized help that many survivors need after a suicide (Felgelman, 2008).
Anticipatory Grief
Anticipatory grief is an emotional response that occurs before the actual death around a family member with a degenerative or terminal disorder. It also is experienced by a person anticipating his or her own death. Symptoms can be similar to those experienced after death and can be colored by ambivalent feelings.
Chronic Sorrow
Chronic sorrow is an ill-defined form of grief, occurring while a person is still alive, in relation to a limiting disease, or as an ongoing loss of potential in a loved one (Bowes, Lowes, Warner, & Gregory, 2009). It has been identified in parents of disabled or mentally ill children, spouses of dementia victims, and adults with a permanent disability or severe chronic illness.
Chronic sorrow is an intermittent grief process. In between, there are periods of emotional neutrality and positive emotions. It presents as a recurring sadness, particularly during exacerbations of symptoms, or comparisons with healthy people. Key distinctions between chronic sorrow and other forms of grieving include an inability to achieve closure and its discontinuous nature. Clients and family members may not be aware that they are grieving because they don’t recognize having an ongoing incomplete loss as a legitimate loss to be grieved (Lafond, 2002). Providing timely support for families when there is a resurgence of symptoms can reduce stress.
Complicated Grieving
Complicated grieving represents a form of grief, distinguished by being unusually intense, significantly longer in duration, or incapacitating. A history of depression, substance abuse, death of a parent or sibling during childhood, prolonged conflict or dependence on the deceased person, or a succession of deaths within a short period predispose a person to complicated grief. Statements such as “I never recovered from my son’s death,” or “I feel like my life ended when my husband died” may indicate the presence of complicated grief.
Symptoms can appear as an absence of grief in situations where it would be expected, for example, a marine who displays no emotion over the deaths of war comrades. When deaths and important losses are not mourned, the feelings don’t just disappear; they reappear in unexpected ways sometimes years later. Subsequent losses trigger an extreme reaction to a current loss. Complicated grief can result in clinical symptoms such as depression or anxiety disorders that require professional help. Exercise 8-3 provides a personal opportunity to reflect on the grieving process.
Applications
Nursing roles in palliative care
Implementing palliative care concepts
Palliative care operates as a 24-hour resource, providing comprehensive, holistic services to clients and families in hospitals, people’s homes, nursing homes, and outpatient settings. Ideally, palliative services are integrated at all levels of care, and are adapted to a client’s specific cultural, social, and economic circumstances. Palliative care can be used concurrently with disease-modifying care, with the level of comfort care increasing according to client need (Savory & Marco, 2009).
The palliative care team is interdisciplinary, consisting of physicians, nurses, social workers, psychologists, and clergy specially trained in palliative care. In addition to supportive care for clients and families, team members provide education and consultation about EOL care for hospital staff. The treatment focus of palliative care is on pain control, physical symptom management, and easing the secondary psychosocial and spiritual distress experienced by clients with a terminal illness. If the client has had a special relationship with a physician, before admission to palliative care, the client or nurse can contact them. In some cases, the physician will stay involved; this can be a major source of comfort for clients and families.
Nurses play a pivotal role as professional coordinators, direct providers of care, and advocates for client autonomy and control in EOL care. They are in a key position to help families maintain family integrity, and to support their efforts in managing the process of living until death and in preparing for the death of their loved one. Quality indicators for EOL care are displayed in Figure 8-1.
Nurses must be aware of their own EOL experiences, including attitudes, expectations, and feelings about death and the process of dying. Miller (2001) notes, “As you become more clear about who you are and why you do what you do, you will become more receptive to whomever you are with” (p. 23). Exercise 8-4 is designed to promote self-awareness.
Key issues and approaches in end-of-life care
Clients and families face difficult, irreversible decisions in the last phase of life. Decisions related to discontinuation of fluids, antibiotics, blood transfusions, and ventilator support require a clear understanding of a complex care situation. Thelan (2005) defines end-of-life decision making as “the process that healthcare providers, patients and patients’ families go through when considering what treatments will or will not be used to treat a life threatening illness” (p. 29).
EOL decisions should be transparent, meaning that all parties involved in the decision should fully understand the implications of their decision. For example, to make an informed decision about use of life supports for terminal clients, clients and families need to know whether further treatments will enhance or diminish quality of life, their potential impact on life expectancy, whether the treatment is known to be effective or is an investigative treatment, and what types of adverse effects the client is likely to experience.
When the client is fully competent, he or she should make all treatment decisions. Ideally, EOL care choices should be made before a life-threatening illness occurs, or as early as possible after diagnosis (Kirchhoff, 2002). The nurse’s role is to provide the client with full information, and to serve as his or her advocate in support of the person’s right to make decisions about treatment and care (ANA, 1991; Erlen, 2005). Box 8-2 provides guidelines for talking with families about care options at EOL when an advance directive or durable power of attorney is not in effect.
Using advance directives
Miscommunication is a common underlying theme in creating confusion and delaying appropriate decisions about EOL care (Lang & Quill, 2004). Preferences are best expressed in advance directives (see Chapter 2), with discussions taking place in a compassionate, gentle manner, paced at the client/family’s pace and level of understanding. Studies of family use of advance directives demonstrate significantly lower stress in families using them (Davis et al., 2005). In the hospital, advance directives should be kept in the front of the client’s chart.
Pain control and management
Pain control and management is an essential component of quality EOL care. Standards for pain management established by the Joint Commission (2010) require that every inpatient be routinely assessed for pain, with documentation of appropriate monitoring, and pain management. The American Pain Society (APS), Joint Commission, and Veteran’s Administration have identified pain as the fifth vital sign with a nursing expectation of pain evaluation together with the standard vital signs (temperature, pulse, respiration, and blood pressure).
Pain is a subjective assessment, assessed verbally with the client and/or observed in client behavior. Routine assessments can identify previously unreported incidences of pain symptoms (Morrison & Meier, 2004).
• Character of the pain (sharp, dull, burning, persistent, changes with movement, direct or referred pain)
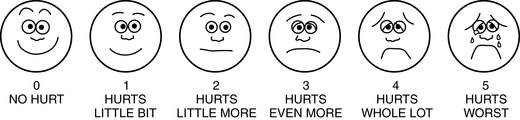
• Intensity—using a 0 to 10 numerical rating scale, with 0 being no pain and 10 being unbearable pain; assess children and clients having limited English with the Wong–Baker FACES Pain Rating Scale (Figure 8-2).
Behavioral indicators include abrupt changes in activity, crying, inability to be consoled, listlessness or unwillingness to move, rubbing a body part, wincing, or facial grimacing (Atkinson, Chesters, & Heinz, 2009).
Having appropriate pain control for moderate-to-severe pain usually requires the use of opioids. Misperceptions about pain-relieving opioids are a major, unnecessary barrier to adequate pain control. Families will attribute signs and symptoms of approaching death such as increased lethargy, confusion, and declining appetite to side effects of opioids. With or without pain medication, actively dying clients become less responsive as death approaches. Although clients may experience drowsiness with initial dosing, this side effect quickly disappears.
Nurses should educate the family and client about the differences between disease progression and adverse effects related to opioids (Pashby, 2010). Essential information includes action, dosing intervals, side effects, and role pain control in client comfort and quality of life.
A second unfortunate barrier is fear of addiction (Clary & Lawson, 2009). All clients, including addicts, are entitled to appropriate and adequate pain management of severe pain. People do not become addicted from taking legally prescribed opioid medications for pain associated with terminal illness. There is a fundamental difference between taking essential medication for pain control on a prescribed scheduled basis and addictive uses. Addicted clients may require larger doses of pain medication because of cross-tolerance. Once the family understands the mechanisms and goals of pain control, and is assured that the client will not die or become addicted from its appropriate use, most will support its use in EOL care.
Clients approaching death can experience “breakthrough” pain, which occurs episodically as severe pain spikes. When breakthrough pain occurs, rescue medications, which are faster acting, can be used. Touch and light massage are helpful adjuncts for pain relief.
Communication in end-of-life care
Curtis (2004) suggests that communication skill is equal to or supersedes clinical skill in EOL care. Everyone experiences a death differently; it is the uniqueness of each person’s experience that the nurse attempts to tap into and facilitate through conversation. Conversations with clients and families provide nurses with insights about personal values and preferences regarding EOL care, and provide a forum to answer difficult questions in a supportive environment.
The quality of the relationship between nurse, patient, and family members is a key factor in how the last phase of life is experienced and negotiated (Mok & Chiu, 2004; Olthuis et al., 2006). EOL interactions help people find meaning, achieve emotional closure, and provide the best means for helping clients and families make complex life decisions. Listening and responding to clients as they cope with difficult issues around dying is easier said than done (Larson & Tobin, 2000). The challenge for nurses is to remain in a relationship with clients and families even when one feels inadequate to the task.
Schim and Raspa (2007) believe that the process of dying is a narrative: “Life-altering happenings are expressed through stories” (p. 202). Personal reflections are critical sources of assessment data. Once rapport is established, Pashby (2010) suggests nurses can ask clients how they learned of their diagnosis. She notes that a terminal diagnosis is usually a “Technicolor Moment” that the person remembers vividly and appreciates talking about. Other questions such as “What has changed for you since the diagnosis?” or “What is it like for you now?” provide additional data. Giving voice to the experience helps clients to consider its personal meaning and provides the nurse with a more complete picture of each person’s distinctive concerns and goals.
Although most dying clients know that they are dying, it is not unusual for a client to ask in the course of conversation, “Am I going to die?” Before answering, find out more about the origin of the question. A useful listening response is, “What is your sense of it?” Box 8-3 provides guidelines for communicating with terminally ill clients.
Morgan (2001) suggests using a basic social process between nurse and client in palliative care, which she labeled protective coping and adjustment. The process involves nursing interactions that protect, maintain, and safeguard the integrity of clients, whereas at the same time helping them to determine and act on actions that are in their own best interests.
Communicating with Families
Family members have different levels of readiness to engage in discussions about the dying process. It is “normal” for an impending death to have a different impact on each family member, because each has had a unique relationship with the dying person. Conversations with families need not be long in duration, but regularity is important. Box 8-4 identifies family communication needs at EOL.
Common concerns include discontinuing life support; conflicts among family members about care; tensions between the client, family, and/or physician and family about treatment; where death should occur (home, hospital, hospice); if/when hospice should be engaged; and other concerns. Active listening can produce a creative outcome.
Creating Family Memories
Clients and families need to talk about things other than the disease process and treatments. Nurses can help make this happen. There are spiritual stories, cultural stories, funny stories, developmental stories, narratives of advocacy, and family stories. Each reinforces the bonds and affirms the depth of meaning a family holds with a dying person. The moments of laughter, foibles, and shared experiences are connections that need to be remembered.
Providing Information
Nurses are key informants about client status and changes in the client’s condition. There are fundamental differences in the level of information an individual or family will desire. The response of the client should determine the content and pace of sharing information. Talking with families about care details and potential outcomes should happen often, but even more frequently when the client’s health status begins to decline or show a change.
Ideally, one nurse serves as the primary contact for the client and family, and acts as a liaison between providers and clients. This nurse keeps other health team members informed of new issues, and shares their input into planning and evaluation of care with the family. Using precise language, giving full and truthful information about the client’s condition, and admitting to uncertainty, when it exists, are important dimensions of EOL information giving.
Family Conferences
Family conferences are effective tools to alleviate family anxiety about the dying process, reduce unnecessary conflict between family members, and assist family members with important decision-making processes. Principles related to EOL care, as presented in Box 8-5, offer guidelines for discussions. Gavrin (2007) notes, “the analog of informed consent is informed refusal” (p. S86). This concept becomes important to clients and families as a component of decision making related to withdrawing or withholding life support in EOL care. Although a physician commonly leads the discussion, nurses often present data and answer questions. Data sharing should be compassionate, accurate, and presented in language understandable to the family. Contradictory recommendations and incomplete information add to a family’s confusion and cause unnecessary distress (Wright, Wurr, Tomlinson, & Miller, 2009). A coordinated approach prevents fragmentary and inconsistent care.
Curtis (2004) recommends that there be a higher ratio of family member–to–health care provider speaking time, and that there be follow-up communication using a consistent physician-nurse team approach. Helping clients and families understand the importance of advance directives and do not resuscitate (DNR) orders can prevent later conflicts when tensions arise near the time of death (Boyle, Miller, & Forbes-Thompson, 2005). Nurses are invaluable resources in clarifying meanings with clients or individual family members after the conference.
Addressing cultural and spiritual needs in end-of-life care
Different cultures have distinctive communication and care standards for clients with life-threatening conditions, some of which are identified in Box 8-6 (Searight & Gafford, 2005). Other distinctions include: (a) type of care that provides comfort to the dying person; (b) understanding of the causes of illness and death; (c) appropriate care of the body and burial rites; and (d) expression of grief responses (Doolen & York, 2007; LaVera et al., 2002).
Asking clients/families directly about their cultural values and issues as a starting point helps ensure cultural safety for clients and families. A simple question such as “Can you tell me about how your family/culture/spiritual beliefs views serious illness or treatment?” provides a framework for discussion. When cultural differences are considered, it is important to avoid stereotyping, as each person’s interpretation of their culture is unique. Once cultural needs are identified, every effort should be taken to honor their meaning to clients and families by incorporating them in care.
Spiritual needs
Glass, Cluxton, and Rancour (2001) note, “The transition from life to death is as sacred as the transition experienced at birth” (p. 49). The dying process, grief, and death itself herald a spiritual crisis—a crisis of faith, hope, and meaning for many people. Spiritual pain occurs when a person’s sense of purpose is challenged or one’s existence is threatened (Millspaugh, 2005).
Spirituality becomes a priority for many people at EOL (Williams, 2006). It is not unusual for clients who have previously declined spiritual interventions to desire them as they move into the final phase of life. Spiritual beliefs and religious rituals provide a tangible vehicle for individuals and families to express and experience meaning and purpose. Religious practices and rituals relevant to EOL can be important to clients even if the person no longer formally practices the religion. Facilitating these practices touches the client’s inner core and helps the person move toward a peaceful death (Bryson, 2004).
Most people welcome an inquiry about their spiritual well-being (Morrison & Meier, 2004). People having a strong relationship with God and/or religious beliefs will usually indicate this connection. To elicit more information about its nature, an appropriate question is: “Is there anything I should know about your spiritual or religious views?” The answer can tell you what is important related to their current circumstances. Steinhauser et al. (2006) suggest that using the probe “Are you at peace?” is a useful way to ask the client about spiritual concerns without being intrusive. Nurses can ask the client and/or family if they would like a visit from an appropriate clergy or hospital chaplain, facilitate the initial contact if the answer is yes and provide essential information about the client’s condition and/or family concerns (Barclay & Lie, 2007).
Not all people attach their concept of spirituality to a particular belief system. Instead, they define their spirituality from an existential perspective. Attig (2001) describes this sense of spirituality as follows:
That within us that reaches beyond present circumstances, soars in extraordinary experiences, strives for excellence and a better life, struggles to overcome adversity, and searches for meaning and transcendent understanding. (p. 37)
When individuals frame their spirituality from an existential perspective, it is appropriate to explore spirituality sources in terms of meaningful relationships. Asking a question such as “Can you tell me about the relationship you had with someone whom you loved who has died?” helps start the conversation. A follow-up question relates to how the client feels about the person now. The value of this intervention is that it emphasizes that the person’s life held meaning for this other person. This line of questioning indirectly tells the person that they too will be remembered after death (Pashby, 2010).
People benefit from telling stories about how they view their life and validate its meaning. A life review helps people consider the deeper values and purpose of their lives, the experience of joy and sorrow. As one person stated, “I lived my life as best I could. I have no regrets.” A follow-up listening response to help the person put into words what he or she reflect on the meaning of a life well lived might be: “Tell me more about this.”
Whatever form spiritual distress takes, it is essential for the nurse to address it. Spiritual issues that trouble clients relate to forgiveness, unresolved guilt issues, expressions of love, saying good-bye to important people, and existential questions about the meaning of life, the hereafter, and concern for their family.
Clary and Lawson (2009) suggest that the EOL offers a final opportunity for people to experience spiritual growth. The most important intervention nurses can provide is to actively and respectfully listen to each client’s search for clarity about their spirituality with compassion and a desire to understand. Helping clients think through spiritual preferences and assisting them to identify resources that can give them strength, courage, purpose, and encouragement to cope with their situation is highly valued. Providing explicit attention to inclusion of appropriate spiritual advisors, prayer, and scripture reading can be helpful to faith-based clients and families coping with a terminal condition.
Nurses need to take an honest look at their own spirituality. Self-awareness allows nurses to enter their client’s spiritual world from an authentic position, without imposing personal values and beliefs. Exercise 8-5 is designed to help nurses understand the value of reflecting on a purposeful life.
Supportive strategies for children
When a child is diagnosed with a terminal illness or condition, the effect on parents is devastating and can last a lifetime. It can influence role functioning, friendships, and treatment of siblings (Hinds, Schum, Baker, & Wolfe, 2005). Children are such an integral part of their parent’s identity that issues of parental protectiveness, guilt, caregiving, balancing family demands, and helplessness must be addressed in the course of providing direct care for the child. When caring for children, there are always two clients to consider: the parent(s) and the child.
Parents are the major anchoring force for most children, so supporting them as primary caregivers for their child is important. They need to be recognized as the expert and primary advocate for their child. Some may not feel they are up to the task, but with appropriate support surprise themselves. Critical to parent satisfaction is knowledge that everything possible was done for their child; that they received accurate, timely information and support; and that preventable suffering was not permitted.
Parents often maintain hope for the child’s survival even with a terminal diagnosis. This is because of a belief that it is not the natural order of things for a child to die, and because terminal symptom profiles for children are less predictable. Nurses can help identify situations in which there is a mismatch between a child’s condition and a parent’s understanding of that condition (Field & Behrman, 2002). They can help decrease parental anxiety by explaining changes in the child’s appearance, and observing signs of distress in parents and siblings related to the child’s progressive deterioration. If the child or family requires additional counseling to reduce stress, nurses can make appropriate referrals. Table 8-2 identifies common goals and provides examples of supportive care for children.
TABLE 8-2
Common Goals and Examples of Supportive Care for Children
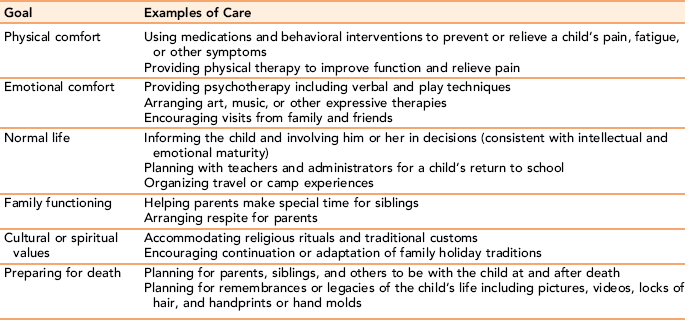
From Field M, Behrman R: When children die: improving palliative and end of life care for children and their families (p. 128). Washington DC, 2002, National Academies Press.
Talking with children about death
Developmental level is a key factor in the child’s attitude toward death. A child younger than 5 years has no clear concept of what death means. As a child matures, the finality of death becomes more real. Death is difficult for children because they don’t have the cognitive development and life experiences to process them completely. Until children reach the formal operations stage of cognitive development, they can have fantasies about the circumstances surrounding the death, and their part in it.
Children don’t express their grief in the same way as adults. Acting out, anger, fear, and crying are common responses, which appear spontaneously. One minute the child may be playing, the next he or she is angry or withdrawn. Preschoolers may repeatedly ask when someone close to them will be coming home even if parents tell them the person has died. Developmentally, they don’t understand the permanence of death. Elementary school children accept the permanence of death, but view it in a concrete manner. Adolescents are aware of death as a final act.
Regardless of age, parents can help their children understand the impending death or loss of a relative by explaining in a concrete, direct way what has happened, using clear, concrete language suitable to the child’s developmental level. Children should be encouraged to talk about changes in the health of a parent or the impending death of a central person in their lives. Questions should be answered directly and honestly at the child’s developmental level of comprehension. Check in with the child to find out how the child is coping at regular intervals.
The National Cancer Institute (2010) identifies three key concerns of children:
Parents can anticipate that these will be issues for children, and create opportunities for children to ask these questions. For example, if a child around the same age or a sibling dies, a child may be fearful that something similar will happen to him or her. Maintaining daily routines in the child’s life after the death of a parent or primary caregiver is critical. Children need to know that they are safe and will be taken care of by the remaining adults in their life. If changes are needed, children should have ample time to make the adjustment rather than have a sudden move thrust on them without discussion. Children need physical contact, reassurance, and relevant discussions about the person who has died. If parents are unable to provide the level of communication a child needs, nurses can help them with appropriate referrals.
Sometimes a family will want to exclude young children from contact with or knowledge about a person who is likely to die soon. Usually children are aware of what is happening (Loomis, 2009). Encouraging family members to talk with children about changes in their relative’s condition using clear, simple terms and allowing them to express their feelings freely is important. Drawing a picture or sending a note can be a useful way for the child to connect with a critically ill relative, if direct contact is not advised. With preparation, adolescents can benefit from being allowed to visit with the client.
Helping clients achieve a good death
The Institute of Medicine (1997) defines a good death as “one that is free from unavoidable distress and suffering for patients, families and caregivers; in general accord with patients’ and families’ wishes; and reasonably consistent with clinical, cultural, and ethical standards” (p. 82). Death is a deeply personal experience. In a study of what constitutes a good death from the perspective of families, clients, and professionals, Steinhauser et al. (2000) identified six elements:
Maintaining a sense of control over what happens during the dying process and who is present at the end, having access to spiritual, emotional, and knowledgeable supports and being afforded hope, dignity, and privacy are also client/family values associated with a good death (Côté & Peplar, 2005; Kirchhoff, 2002; Smith, 2000). Exercise 8-6 provides you with the opportunity to personally think about what constitutes a good death.
Signs of approaching death
As death approaches, there are subtle but significant changes in a person’s behavior. With some people, changes are progressive and swift. With others, there is gradual downward spiral. Common symptoms include long periods of sleeping or coma, decreased urinary output, changes in vital signs, disorientation, restlessness and agitation, severe dyspnea (breathlessness), skin temperature, and color. Dying clients experience profound weakness such that they cannot independently complete even basic hygiene.
The process of watching someone die is frightening to families. Family members feel increasingly helpless in being able to properly meet client needs. They need anticipatory guidance about what to expect and concrete suggestions about ways to connect with their loved one. The American Cancer Society Web site offers an excellent description of typical changes in the client when death is near and a clear outline of what caregivers can do to provide comfort to the client. The Internet is an invaluable resource for general information and for family-to-family support. Recommended sites should be carefully screened for accuracy and appropriateness.
Direct comfort care is essential. Practical suggestions for care and availability are critical components of care as clients approach death. Nurses can recommend simple care measures such as positioning, mouth and hygiene care, and so forth, to support family member efforts. They can provide immediate assessment data and explain its meaning. Nurses can encourage out-of-town family to visit, refer caregivers to support groups, and offer resource referrals for respite care. Most important, they can listen.
A common concern is the client’s loss of appetite and interest in food. Most stop eating. Explaining that this is a natural process that occurs as the body begins to shut down in preparation for death helps with family understanding (Reid, McKenna, Fitsimons, & McCance, 2009). As death approaches, clients become increasingly unresponsive to voice and stimulus. Because hearing is the last sense to go, talking with the dying person in a soft voice, playing calming music, and using gentle touch can soothe the client in a meaningful way.
Creating a care environment in which the dying person feels valued, comforted, and treated as a unique individual (Volker & Limerick, 2007) is vital, even when the client is no longer cognizant of what is happening. Flexibility in allowing family and/or significant others open access to the client, while taking care that the visits are not taxing for the client, reduces family anxiety and can be comforting for all concerned. As clients weaken, they typically want to engage with fewer family and friends. Nurses can act as gatekeepers in helping clients balance their own needs for relationship with the needs of others, and helping everyone concerned to engage with each other in a meaningful way.
Communication strategies
Presence is an important form of communication with dying clients and families. Casarett, Kutner, and Abrahm (2001) assert that simply by being with a family and bearing witness to the family’s expression of grief, health care providers provide important emotional and practical support.
Most families find it difficult to leave a dying client, even for a short period. Assuring family members that the nurse will check on the client frequently, and will call the family immediately if change occurs, gives families permission to take a brief respite from the client.
Caring of the client after death
Respect for the dignity of the client continues after death. If the family is present at time of death, allowing uninterrupted private time with the client, before initiating postmortem care is important. If the family is not present, all excess equipment and trash should be removed from the room. You can offer presence and emotional support as you escort the family into the room. Some families will want privacy; others will appreciate having the presence of the nurse or chaplain. Family preference should be honored.
If the family is not immediately present, the client’s belongings should be placed in a bag and given to the family after the visitation. Provide soft lighting, chairs for the family, and tissues. The client’s head should be elevated at a 30-degree angle, in a natural position. Hair should be combed, exposed body parts cleaned, and dentures replaced, if possible. The tone of the room and the positioning of the client should “give a sense of peace for the family” (Marthaler, 2005, p. 217). It is important for the nurse to allow the family as much time as they need with the client. The nurse can obtain signatures to release the client to the funeral home after the family has spent some time with the client.
Nurses can offer healing presence for the family after death.
Stress issues for nurses in palliative care settings
Nurses deeply invest themselves in the care and comfort of clients and families facing death, and can experience grief when the client dies. Disenfranchised grieving is a term applied to the grief nurses can experience after the death of a client with whom they have had an important relationship (Brosche, 2007; Rushton et al., 2006). Unacknowledged grieving in professional nurses can be cumulative. Unlike their clients, who live through one loss at a time, nurses can experience several losses a week while caring for terminally ill clients and their families (Brunelli, 2005).
Nurses can experience compassion fatigue, a syndrome associated with serious spiritual, physical, and emotional depletion related to caring for clients that can affect the nurse’s ability to care for other clients (Worley, 2005). Unrelieved compassion fatigue can result in burnout and a nurse’s decision to leave nursing.
Another source of stress is the moral distress associated with helping clients and families resolve conflicts about EOL care (Rushton et al., 2006). For example, the use of technology and life support, and use of phase I or II clinical trial drugs with terminally ill clients can create significant ethical dilemmas for nurses caring for these clients. Support groups in which nurses can successfully address and resolve the secondary stress of continuously caring for terminally ill clients and some of the ethical issues involved with that care are helpful to nurses.
Summary
This chapter describes the stages of death and dying, and theory frameworks of Eric Lindeman and George Engel for understanding grief and grieving. Palliative care is discussed as a philosophy of care and an emerging discipline focused on making EOL care a quality life experience. A good death is defined as a peaceful death experienced with dignity and respect; one that wholly honors the client’s values and wishes at the EOL. Nurses can offer compassionate communication, presence, and anticipatory guidance to ease the grief of loss. Seven domains of quality indicators for palliative and EOL care are identified as pain and symptom control, transparent decision making, communication, emotional and practical support, spiritual support, and continuity of care.
Nursing strategies are designed to help clients cope with the secondary psychological and spiritual aspects of having a terminal illness such that they achieve the best quality of life in the time left to them. Talking with clients about advance directives is a professional responsibility of the nurse, and it reduces unnecessary conflict among family members at this critical time in a person’s life.
Talking with children about terminal illness and death in a relative, or in coping with a terminal diagnosis themselves should take into consideration the child’s developmental level. Questions should be answered honestly and empathetically. Nurses can help families understand the behavioral changes signaling the body’s natural shutdown of systems as death approaches. Providing support for clinicians is considered a quality indicator in EOL care. When not addressed, the disenfranchised grief that nurses experience with providing EOL care to multiple clients can lead to compassion fatigue, burnout, and moral distress.
References
American Association of Colleges of Nursing End-of-Life Nursing Education Consortium (ELNEC) fact sheet, updated March 2006, Washington, DC, Author, 2006. Available online:, http://www.aacn.nche.edu/ELNEC/about.htm. [Accessed July 25, 2020].
American Nurses Association, ANA position statements: nursing and the patient self determination acts. ANA Nursubg World 1991. Available online:, www.nursingworld.org/readroom/position/ethics/etsdet.html.
Atkinson, P., Chesters, A., Heinz, P. Pain management and sedation for children in the emergency department. Br Med J. 2009;339:b4234.
Attig, T. Relearning the world: making and finding meanings. In: Neimeyer R., ed. Meaning reconstruction and the experience of loss. Washington, DC: American Psychological Association; 2001:33–53.
Attig, T. Meanings of death seen through the lens of grieving. Death Stud. 2004;28:341–360.
Barclay, L., Lie, D. New guidelines issued for family support in patient-centered ICU. Crit Care Med. 2007;37:605–622.
Bowes, S., Lowes, L., Warner, J., et al. Chronic sorrow in parents of children with type 1 diabetes. J Adv Nurs. 2009;65(5):992–1000.
Boyle, D., Miller, P., Forbes-Thompson, S. Communication and end-of-life care in the intensive care unit. Crit Care Nurs Q. 2005;28(4):302–316.
Brosche, T. A grief team within a healthcare system. Dimens Crit Care Nurs. 2007;26(1):21–28.
Brunelli, T. A concept analysis: the grieving process for nurses. Nurs Forum. 2005;40(4):123–128.
Bryson, K.A. Spirituality, meaning, and trancendence. Palliat Support Care. 2004;2(3):321–328.
Casarett, D., Kutner, J., Abrahm, J. Life after death: a practical approach to grief and bereavement. Ann Intern Med. 2001;134(3):208–215.
Chenitz, W.C. Living with AIDS. In: Flaskerud J.H., Ungvarski P.J., eds. HIV/AIDS: a guide to nursing care. Philadelphia: WB Saunders, 1992.
Clary, P., Lawson, P. Pharmacologic pearls for end of life care. Am Fam Physician. 2009;79(12):1059–1065.
Corless, I. Bereavement. In: Ferrell B., Coyle N., eds. Textbook of palliative nursing. New York: Oxford University Press, 2001.
Côté, J., Peplar, C. A focus for nursing intervention: realistic acceptance or helping illusions. Int J Nurs Pract. 2005;11:39–43.
Curtis, J.R. Communicating about end-of-life care with patients and families in the intensive care unit. Crit Care Clin. 2004;20:363–380.
Davies E., Higginson J., eds. Palliative care: the solid facts. Milan: European Office of the World Health Organization, 2004.
Davis, B., Burns, J., Rezac, D., et al. Family stress and advance directives: a comparative study. Am J Hosp Palliat Care. 2005;7(4):219–229.
Dobratz, M. The pattern of becoming: self in death and dying. Nurs Sci Q. 2002;15(2):137–142.
Doolen, J., York, N. Cultural differences with end of life care in the critical care unit. Dimens Crit Care Nurs. 2007;26(5):194–198.
Engel, G. Grief and grieving. Am J Nurs. 1964;64(7):93–96.
Erlen, J. When patients and families disagree. Orthop Nurs. 2005;24(4):279–282.
Felgelman, B., et al. Surviving after suicide loss: the healing potential of suicide survivor support groups. Illness, Crisis and Loss. 2008;16(4):285–304.
Field, M., Behrman, R. When children die: improving palliative and end of life care for children and their families. Washington, DC: The National Academies Press, 2002.
Florczak, K. The persistent yet everchanging nature of grieving a loss. Nurs Sci Q. 2008;21(1):7–11.
Galanos, A. Hospital-based palliative care units: answering a growing need. N C Med J. 2004;65(4):217–220.
Glass, E., Cluxton, D., Rancour, P., et al. Principles of patient and family assessment. In: Ferrell B., Coyle N., eds. Textbook of palliative nursing. New York: Oxford University Press, 2001.
Gavrin, J. Ethical considerations at the end of life in the intensive care unit. Crit Care Med. 2007;35(2):S85–S94. [L].
Harvard Womens Health Watch Left behind after suicide, 2009. Available at:, www.health.harvard.edu. [July;].
Hinds, P., Schum, L., Baker, J., et al. Key factors affecting dying children and their families. J Palliat Med. 2005;8(Suppl 1):S70–S78.
Institute of Medicine. Field M.J., Cassel C.K., eds. Approaching death: improving care at the end of life. Washington: DC: National Academy Press, 1997.
Jeffries, J. Helping grieving people: a handbook for care providers. New York: Brunner-Routledge, 2005.
Joint Commission. The Approaches to pain management: an essential guide for clinical leaders, ed 2. Oakbrook Terrace, IL: Joint Commission Resources, 2010.
Kirchhoff, K.T. Promoting a peaceful death in the ICU. Critical Care Clinics of North America. 2002;14:201–206.
Kübler-Ross, E. On death and dying: What the dying have to teach doctors, nurses, clergy, and their own families. New York: Scribner, 1969.
Lafond, V. Grieving mental illness: a guide for patients and their caregivers, ed 2. Toronto: University of Toronto Press, 2002.
Lang, F., Quill, T. Making decisions with families at the end of life. Am Fam Physician. 2004;70(4):719–723.
LaPorte Matzo M., Witt-Sherman D., eds. Palliative care nursing: quality care to the end of life, ed 2, New York: Springer, 2006.
Larson, D., Tobin, D. End-of-life conversations: evolving practice and theory. JAMA. 2000;284(12):1573–1578.
LaVera, M., Crawley, M., Marshall, P., et al. Strategies for culturally effective end of life care. Ann Intern Med. 2002;136(9):673–677.
Lee, K.J., Dupree, C. Staff experiences with end-of-life care in the pediatric intensive care unit. J Palliat Med. 2008;11(7):986–990.
Lendrum, S., Syme, G. Gift of tears: a practice approach to loss and bereavement counseling. London: Routledge, 1992.
Levine, S. Unattended sorrow: recovering from loss and reviving the heart. Emmaus, PA: Rodale, 2005.
Lindemann, E. Symptomatology and management of acute grief. Am J Psychiatry. 1994;151(6 sesquicentennial Suppl):155–160. [(Originally published in 1944)].
Loomis, B. End of life issues: difficult decisions and dealing with grief. Nurs Clin North Am. 2009;44:223–231.
Malloy, P., Paice, J., Virani, R., et al. End-of life-nursing education consortium: 5 years of educating graduate nursing faculty in excellent palliative care. J Prof Nurs. 2008;24(6):352–357.
Mark Twain Quotations, Newspaper Collections, & Related Resources, 2002. Available online:, www.twainquotes.com.
Marthaler, M.T. End of life care: practical tips. Dimens Crit Care Nurs. 2005;24(5):215–218.
McIlfatrick, S. Assessing palliative care needs: views of patients, informal carers and healthcare professionals. J Adv Nurs. 2007;57(1):77–86.
Mercer, D., Evans, J. The impact of multiple losses on the grieving process: an exploratory study. Journal of Loss and Trauma. 2006;11:219–227.
Miller, J. The art of being a healing presence. Ft. Wayne, IN: Willowgreen Publishing, 2001.
Millspaugh, D. Assessment and response to spiritual pain: part I. J Palliat Med. 2005;8(5):919–923.
Mok, E., Chiu, P. Nurse-patient relationships in palliative care. J Adv Nurs. 2004;48(5):475–483.
Morgan, A. A grounded theory of nurse-client interactions in palliative care nursing. J Clin Nurs. 2001;10(4):583–584.
Morrison, R.S., Meier, D.E. Palliative care. N Engl J Med. 2004;350:2582–2590.
Mularski, R., Curtis, J., Billings, A., et al. Proposed quality measures for palliative care in the critically ill: a consensus from the Robert Wood Johnson Foundation Critical Care Workgroup. Crit Care Med. 2006;34:S404–S411.
National Cancer InstituteNational Institutes of Health. Children and grief. Available online: http://www.cancer.gov/cancertopics/pdq/supportivecare/bereavement/Patient/page9, 2010. [Accessed January 9].
National Consensus Project for Quality Palliative Care Clinical practice guidelines for quality palliative care, 2004. Available online:, http://www.nationalconsensusproject.org.
Neimeyer R.A., ed. Meaning reconstruction and the experience of loss. Washington, DC: American Psychological Association, 2001.
Olthuis, G., Dekkers, W., Leget, C., et al. The caring relationship in hospice care: an analysis based on the ethics of the caring conversation. Nurs Ethics. 2006;13(1):29–40.
Pashby, N., 2010. [(Expert Hospice Nurse): Personal Communication, Odenton, MD, January 15].
Reid, J., McKenna, H., Fitsimons, D., et al. Fighting over food: patient and family understanding of cancer cachexia. Oncol Nurs Forum. 2009;36(4):439–445.
Rushton, C.H., Reder, E., Hall, B., et al. Interdisciplinary interventions to improve pediatric palliative care and reduce health care professional suffering. J Palliat Med. 2006;9:922–933.
Savory, E., Marco, C. End of life issues in the acute and critically ill patient. Scandanavian Journal of Trauma Resuscitation Emergency Medicine. 2009;17:21.
Schim, S., Raspa, R. Cross disciplinary boundaries in end-of-life education. J Prof Nurs. 2007;23(4):201–207.
Searight, H., Gafford, J. Cultural diversity at the end of life: issues and guidelines for family physicians. Am Fam Physician. 2005;71(3):515–522.
Silveira, M., Schneider, C. Common sense and compassion: planning for the end of life. Clinics Family Practice. 2004;6(2):349–368.
Smith, R. A good death. BMJ. 2000;320:129–130.
Steinhauser, K.E., Clipp, E.C., McNeilly, M., et al. In search of a good death: observations of patients, families, and providers. Ann Intern Med. 2000;132(10):825–832.
Steinhauser, K.E., Voils, C., Clipp, E., et al. Are you at peace?: one item to probe spiritual concerns at the end of life. Arch Intern Med. 2006;166(1):101–105.
Thelan, M. End of life decision making in intensive care. Crit Care Nurse. 2005;25(6):28–37.
Thomas, J. My Saints Alive: A Journey of Life, Loss, and Love, 2010. [Unpublished Manuscript, Charlottesville, VA, September].
Volker, D., Limerick, M. What constitutes a dignified death? The voice of oncology advanced practice nurses. Clin Nurse Spec. 2007;21(5):241–247.
Williams, A.L. Perspectives on spirituality at the end of life: a metasummary. Palliat Support Care. 2006;4:407–417.
World Health Organization WHO definition of palliative care, 2008. Available online:, http://www.who.int/cancer/palliative/definition/en/. [Accessed February 28, 2009].
Worley, C.A. The art of caring: compassion fatigue (from the editor). Dermatol Nurs. 2005;17(6):416.
Wright, B., Wurr, K., Tomlinson, H., et al. Clinical dilemmas in children with life-limiting illnesses: decision making and the law. Palliat Med. 2009;23:238–247.