Professional Guides to Action in Interpersonal Relationships
At the end of the chapter, the reader will be able to:
1 Describe the use of professional standards of care and professional performance standards in nurse-client relationships.
2 Identify regulatory bodies and state laws guiding the conduct of professional nursing practice.
3 Discuss legal standards used in nursing practice.
4 Discuss ethical standards and issues of professional nursing practice.
5 Apply the nursing process and SBAR format to structure professional nursing care.
6 Discuss client privacy, Health Insurance Portability and Accountability Act of 1996 (HIPAA) regulations, confidentiality, and informed consent as guides to action in nurse-client relationships.
This chapter introduces the student to the professional, legal, and ethical standards of practice that provide essential parameters for professional therapeutic activities occurring within the nurse-client relationship. Included in this chapter is an overview of the nursing process, which is used to sequence nursing actions in the nurse-client relationship and as a guide to chart client progress.
Basic concepts
Standards as guides to action in clinical nursing practice
All legitimate professions have standards of conduct. Nursing’s professional, legal, and ethical standards identify principles of professional nursing practice and govern its actions. Professional nurses, regardless of setting, are expected to follow these standards in their clinical practice, research, and education. The Code of Ethics for Nurses (ANA, 2001) establishes principled guidelines designed to protect the integrity of clients related to their care, health, safety, and rights. Nurses are held to federal and state regulatory laws for hospital and other health care facilities, and to the nursing standards, policies, and procedures of the health care facility in which they are employed (Guido, 2009). Professional nursing practice is legally regulated through state licensure, with additional education and national certification required for advanced practice. The American Nurses Credentialing Center (ANCC) certifies nurses for advanced practice in a nursing specialty once the applicant completes all requirements for national certification. Each state sets forth professional nursing standards and interpretive guidelines through its Nurse Practice Act. Professional, ethical, and legal standards are complementary but distinct guides to action in nurse-client relationships. They each reflect societal values.
Professional standards of care and nursing performance standards
The national professional organization for registered nurses (ANA), publishes standards of care and nursing performance that help ensure professional nursing competence and safe ethical clinical practice. Professional standards of practice serve the dual purpose of providing a standardized benchmark for evaluating the quality of their nursing care and offering the consumer a common means of understanding nursing as a professional service relationship. They inform the public what they can expect from professional nurses.
Specified competencies identified in nursing standards represent a uniform legal yardstick against which care can be measured. In legal situations, professional standards of practice would be used as a first-line defense, in conjunction with what a “reasonable and prudent nurse” would do in a similar nursing situation, to determine nursing accountability. Failure to adhere to established nursing practice and professional performance standards could result in a negative civil judgment against a professional nurse.
The Joint Commission (TJC, 2007) mandates that written nursing policies with specific standards of care be available on all nursing units. Professional standards of practice provide definitions of the minimum competencies needed for quality professional nursing practice Presented as principled statements, they designate the knowledge and clinical skills required of nurses to practice competently and safely.
Professional performance standards describe a competent level of professional role behaviors related to quality of care, practice evaluation, continuing education, collegiality, collaboration, ethics, research, resource utilization, and leadership. Nurses are expected to competently perform professional role behaviors consistent with published standards and appropriate to their education, position, and the practice setting. They are expected to refrain from performing any nursing activities for which they are not trained.
Professional nurses are accountable for adhering to professional standards regardless of their particular nursing role or the acuity of individual nursing circumstances. Additional specialty practice guidelines provide a customized set of standards for care of specific populations (e.g., children, the elderly, and psychiatric patients) and specialty areas of clinical practice (e.g., acute care or perioperative nursing).
Nursing’s Social Policy Statement: Nursing’s Social Policy Statement spells out the discipline’s covenant with society and contractual obligations for care (LaSala, 2009). Nursing is conceptualized as a dynamic profession, operating within a social context, and being responsive to the ever-changing nature of societal health care needs. The American Nurses Association Social Policy Statement (American Nurses Association, 2003) describes the social values and assumptions inherent in professional nursing practice and identifies nursing’s stewardship commitment to society. The ANA recently published a revised edition of Nursing’s Social Policy Statement: The Essence of the Profession in 2010 (American Nurses Association, 2010).
Regulatory bodies: state boards of nursing: Each state has its own Board of Nursing. The National Council of State Boards of Nursing states, “Boards of Nursing are state governmental agencies that are responsible for the regulation of nursing practice in each respective state. Boards of Nursing are authorized to enforce the Nurse Practice Act, develop administrative rules/regulations and other responsibilities per the Nurse Practice Act” (National Council of State Boards of Nursing, 2008).
In addition to issuing professional licenses to practice nursing, the state Board of Nursing is responsible for establishing and maintaining standards for safe nursing care in that state, and monitoring nurses’ compliance with state laws governing their practice. Each state Board of Nursing has the authority to take disciplinary action against the licenses of those nurses who have exhibited unsafe nursing practice.
Nurse Practice Acts: Nurse Practice Acts are the most important statutory laws governing the provision of professional nursing care through the nurse-client relationship. Nurse Practice Acts are legal documents that communicate professional nursing’s scope of practice, and outline nurses’ rights, responsibilities, and licensing requirements in providing care to individual clients, families, and communities. Nurses appointed by the governor to serve on a state Board of Nursing develop the statutes’ governing nursing practice in each state.
Each state’s Board of Nursing develops and executes its own Nurse Practice Act. If a nurse practices in one state and then moves to another, the nurse has to follow the Nurse Practice Act guidelines in his or her new state of residence. Because all Nurse Practice Acts reflect standards of nursing care developed by the ANA, they do not usually differ significantly, but nurses are advised to have a working knowledge of the Nurse Practice Act in each state of planned employment.
Nurse Practice Acts authorize state boards of nursing to interpret the legal boundaries of safe nursing practice and give them the authority to punish violations, with suspension or loss of professional licensure.
Scope of Practice: Scope of practice is a broad term referring to the legal and ethical boundaries of practice for professional nurses The ANA (2010) recently published its latest revised edition of Nursing: Scope and Standards of Nursing. In addition to national standards, each state’s Board of Nursing establishes the scope of nursing practice within its state. Scope of practice is defined in written state statutes. Scope of practice in most states reflects different levels of nursing practice, based on the nurse’s education, special skill training, supervised experience, state and national professional credentials, and appropriate professional experience.
Scope of practice includes a broad range of nursing activities such as providing direct care, effectively managing emergency and crisis situations, administering medications, monitoring changes in client conditions, teaching and coaching clients and their families, prioritizing and coordinating care, delegating of nursing tasks, and supervision of unlicensed personnel.
Professional Licensure: The registered nurse’s professional license ensures that each individual nurse has successfully completed an accredited nursing program and can demonstrate the knowledge, skills, and competencies to function as a health provider of safe, effective nursing care. All graduates must pass a national licensure examination (National Council Licensure Examination [NCLEX]) that tests core nursing knowledge before being granted a professional RN license to practice nursing. Practicing nursing without a license can result in legal prosecution.
Nursing licensure helps maintain standards for nursing. Although the NCLEX is a national examination, each nurse must apply for RN state licensure through the state Board of Nursing in his or her state of residence to practice as a registered nurse.
Compact State Recognition Model: In 2000, the National Council of State Boards of Nursing (NCSBN) developed a mutual recognition model of nurse licensure, permitting registered nurses licensed and residing in a compact state to practice in other compact states without obtaining a second license. The multistate license is issued by the compact state in which the nurse resides. The registered nurse is held to the state’s nursing practice laws and regulations in which he or she is actually practicing at the time. The multistate license is valid only between compact states. Over the past few years, more than half the nation’s state boards of nursing have enacted the RN and LPN/VN nurse licensure compact legislation. This legislation is particularly helpful for nurses working in states with large rural populations and few nurses.
Legal standards
Professional nurses are held legally accountable for all aspects of the nursing care they provide to clients and families, including documentation and referral. As the registered nurse’s professional responsibilities have increased in depth and complexity, requiring greater levels of clinical judgment, so has the potential for legal liability (Aiken, 2004). Of special relevance to the nurse-client relationship are issues of professional liability, informed consent, and confidentiality.
Classifications of Laws in Health Care: Nurses need to take into consideration two types of law related to the care they provide for clients and families. Statutory laws are legislated laws, drafted and enacted at federal or state levels. Medicare and Medicaid amendments to the Social Security Act are examples of federal statutory laws. Nurse practice acts are examples of statutory laws enacted at the state level (Aiken, 2004).
Civil laws are developed through court decisions, which are created through precedents, rather than written statutes. Most infractions for malpractice and negligence are covered by civil law and are referred to as torts. A tort is defined as a private civil action that causes personal injuries to a private party. Deliberate intent is not present. Four elements are necessary to qualify for a claim of malpractice or negligence.
• The professional duty was owed to client (professional relationship)
• A breach of duty occurred in which the nurse failed to conform to an accepted standard of care
• Causality in which a failure to act by professional was a proximate cause of the resulting injury
• Actual damage or injuries resulted from breach of duty (Dimond, 2008).
Definitions of negligent actions and related examples are found in Table 2-1.
TABLE 2-1
Definition and Examples of Negligent Actions
| Definition of Negligent Action | Example |
| Performing a nursing action that a prudent nurse would not perform | Carrying out a physician’s order that would have been questioned by other reasonably prudent nurses in similar circumstances |
| Failing to perform a nursing action that a reasonably prudent nurse would perform | Failing to report suspected physical or sexual child abuse |
| Failure to provide routine or customary care | Failing to check vital signs before and after surgery; failing to perform postpartum checks on a client |
| Exhibiting conduct that a reasonably prudent nurse would recognize as posing an unreasonable risk to a client | Failing to give accurate information in a manner that the client can understand regarding choice of treatment and known adverse effects; sharing confidential information with a client’s family or workplace without the client’s permission |
| Failing to protect a client from unnecessary harm | Not putting up the guardrails on a bed with a newly diagnosed client suffering from a stroke; allowing unlicensed personnel to do a nursing procedure without appropriate experience or supervision |
The nurse is bound legally by the principles of civil tort law to provide reasonable standard of care, defined as a level of care that a reasonably prudent nurse would provide in a similar situation (Catalano, 2008). If taken to court, this standard would be the benchmark against which the nurse’s actions would be judged.
Criminal law is reserved for cases in which there was intentional misconduct, and/or the action taken by the health care provider represents a serious violation of professional standards of care (Scott, 2006). The most common violation of nurses related to criminal law is failure to renew a professional nursing license, which, in effect, means that a nurse is practicing nursing without a license (Calalano, 2008).
Legal Liability in Nurse-Client Relationships: In the nurse-client relationship, the nurse is responsible for maintaining the professional conduct of the relationship. Examples of unprofessional conduct in the nurse-client relationship include:
• Breaching client confidentiality
• Verbally or physically abusing a client
• Assuming nursing responsibility for actions without having sufficient preparation
• Delegating care to unlicensed personnel, which could result in client injury
• Following a doctor’s order that would result in client harm
• Failing to assess, report, or document changes in client health status
• Failing to obtain informed consent
• Failure to question a physician’s orders, if they are not clear
• Failure to provide required health teaching
• Failure to provide for client safety (e.g., not putting the side rails up on a client with a stroke)
Scott (2006) claims that effective and frequent communication with clients and other providers is one of the best ways to avoid and/or minimize the possibility of claims of malpractice or negligence. In-depth communication provided in simple layperson’s language about what the nurse is doing, the status of the client’s health care, the meaning of diagnostic tests for client care, and so forth allows clients to make more informed choices and leads to greater satisfaction.
Ethical standards and issues
Nurses have an ethical accountability to the clients they serve that extends beyond their legal responsibility in everyday nursing situations. Ethical issues of particular relevance to the nurse-client relationship relate to caring for clients in ambulatory managed care settings, the rights of clients participating in research, caring for mature minors, client education, right to die issues, transfer to long-term care of elderly clients, and telehealth nursing (Guido, 2009).
American Nurses Association Code of Ethics: The revised ANA Code of Ethics for Nurses (ANA, 2001) with interpretive statements provides ethical guidelines for nurses designed to protect client rights, provide a mechanism for professional accountability, and educate professionals about sound ethical conduct. The new provisions of the Code of Ethics for Nurses are identified in Box 2-1. Similar codes of ethics for nurses exist in other nations. For example, in Canada, nursing practice is guided by the Canadian Nurses Association Code of Ethics for Registered Nurses (1997).
The ANA Code of Ethics for Nurses provides a broad conceptual framework outlining the principled behaviors and value beliefs expected of professional nurses in delivering health care to individuals, families, and communities. Ethical standards of behavior require a clear understanding of the multidimensional aspects of an ethical dilemma, including intangible human factors that make each situation unique (e.g., personal and cultural values or resources).
When an ethical dilemma cannot be resolved through interpersonal negotiation, an ethics committee composed of biomedical experts reviews the case and makes recommendations (Otto, 2000). Of particular importance to the nurse-client relationship are ethical directives related to the nurse’s primary commitment to
Exercise 2-1 provides an opportunity to consider the many elements in an ethical nursing dilemma.
Advance Directives: In 1991, the U.S. Congress passed the Patient Self-Determination Act. This legislation requires health care institutions to inform their clients, on admission, of their right to choose whether to have life-prolonging treatment should they become mentally or physically unable to make this decision (Westley & Briggs, 2004). An advance directive is a legal document, executed by a competent client or legal proxy, specifically identifying individual preferences for the level of care at end of life, related to treatment, medications, hydration, and nutrition (Basanta, 2002). Advance directives allow individuals to specify what actions should be taken on their behalf should they be unable to make health-related decisions. Types of advance directives are identified in Table 2-2. Because life-threatening medical emergencies can occur at any time, all adults—even the healthiest—can benefit from having advance directives in place concerning preferred end-of-life care. Advance directives can be revoked or revised at any time by its author. Exercise 2-2 provides an opportunity to understand the use of advance directives in clinical practice.
TABLE 2-2
| Living will | Documents the client’s preferences for medical treatment, artificial life support, nutrition, use of antibiotics, pain medication) should the client be unable or incompetent to state them (Legal status of living wills varies from state to state.) |
| Medical power of attorney for health care decisions | Legal document with designation of a proxy who is authorized to make health care decisions for a person should the individual be unable to express his or her wishes |
| Durable power of attorney | Legal document with designation of a proxy authorized to make financial decisions and to represent the client’s interests should the client be unable to do so; durable power of attorney can be revoked in writing at any time, as long as the client is competent |
| Do-not-resuscitate (DNR) orders | Written directions about not resuscitating the client if the client’s breathing or heartbeat stops |
| Durable mental health power of attorney | Legal document with designation of a proxy who is authorized to make mental health care decisions for a person should the individual be unable to do so because of mental symptoms |
Psychiatric advance directives are legal, written documents used by people with mental illness to indicate their preference for treatment in the event that they are unable to make decisions about treatment because of mental symptoms (Vuckovich, 2003). A psychiatric advance directive specifies the person who the client wants to accept legal responsibility for making clinical decisions if the client is unable to do so. The document can identify the client’s preferences for medication, treatment, and treatment setting. Having an advance directive in place helps decrease family anxiety and provides direction for health care, endorsed by the client.
Applications
The most common configuration for collecting, organizing, and analyzing data, and for sharing information with other professionals is the nursing process. The nursing process is an interpersonal, client-centered process. Assessment data, nursing diagnosis, and goals for treatment are systematically documented on treatment plans that can be easily shared with nurses and other health professionals.
Using the nursing process in nurse-client relationships
The nursing process is the primary framework used to structure and organize nursing care. Nurses use the nursing process to apply problem-solving strategies to complex health problems and to develop individualized care plans. The Joint Commission has identified six interrelated elements required of the nursing care plan; these are presented in Box 2-2.
The nursing process consists of five progressive phases: assessment, problem identification and diagnosis, outcome identification and planning, implementation, and evaluation. As a dynamic, systematic clinical management tool, it functions as a primary means of directing the sequence, planning, implementation, and evaluation of nursing care to achieve specific health goals. Communication plays an important role in all aspects of the nursing process by
• Helping clients to promote, maintain, or restore health, or to achieve a peaceful death
• Facilitating client management of difficult health care issues through communication
• Providing quality nursing care in a safe and efficient manner
The nursing process is closely aligned with meeting professional nursing standards in the total care of the client. Table 2-3 illustrates the relationship.
TABLE 2-3
Relationship of the Nursing Process to Professional Nursing Standards in the Nurse-Client Relationship
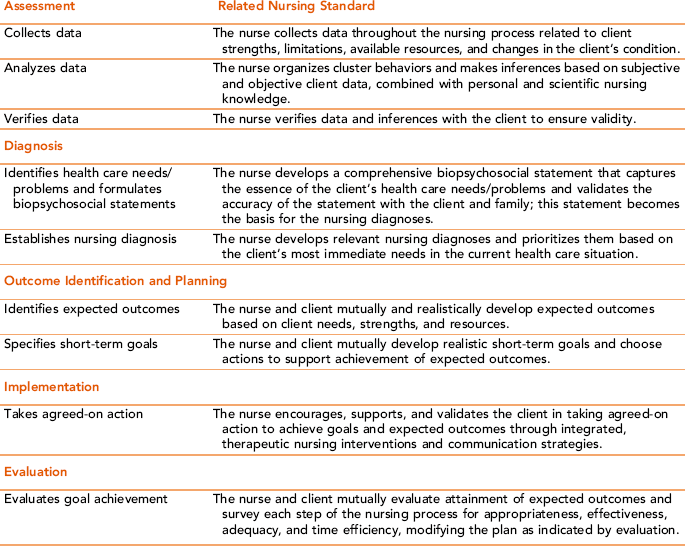
The nursing process begins with the nurse’s first encounter with a client and family, and ends with discharge, referral, or both. There is an ordered sequence of nursing activities, with each activity linked to the trustworthiness of the activity that preceded it. Although the sequence of activities follows a distinctive order, each phase is flexible, flowing into and overlapping with other phases of the nursing process. For example, in providing a designated nursing intervention, the nurse might discover a more complex need than what was originally assessed. This could require a modification in the nursing diagnosis, identified outcome, intervention, or the need for a referral.
The nursing process is not complete until treatment outcomes and client responses are documented on the client’s chart using correct spelling and terminology. Nurses are expected to report all relevant data to appropriate health care personnel at regular intervals and when there is a change in the client’s condition.
Assessment
A client-centered approach to assessment uses a systematic, dynamic process to gather data about the client seeking service. The assessment process begins when when you first meet the client and family. Introducing yourself and explaining the purpose of the assessment interview helps put the client at ease and sets the stage for the information that needs to be gathered. The next step is to ask the client to tell his or her story as it relates to the current request for nursing services. A simple statement, such as “Can you tell me what prompted you to seek treatment at this time?” usually is sufficient to start the conversation. Clients sometimes seek treatment for reasons that one would not ordinarily expect, so this type of open-ended question provides valuable information that otherwise might not emerge so quickly.
The intake assessment, usually completed on admission to the health care agency, serves as baseline data. Using open-ended and focused questions, you should collect data about
• The current problem for which the client seeks treatment
• The client’s perception of his or her health patterns
• Presence of other health risk and protective factors
• Relevant social, occupational, and family history
• The client’s medical and psychiatric history (e.g., previous hospitalizations, family history, medical and psychiatric treatment, and medications)
Assessment of client needs should take the client’s entire experience of an illness or injury into account, rather than simply focusing on clinical data related to the diagnosis. This is what is meant by “patient-centered” care. The behavior, attitude, and appearance of the client also are important sources of information. For example, does the client appear anxious, angry, apathetic, lethargic, cooperative, or uncooperative?
Assessment data should reflect behavioral observation and information from as many sources as is needed for complete accuracy. Sources of data include interview, history, physical assessment, review of records, family interviews, and in some instances, contact with previous health care providers, schools, or other referral sources. As new information becomes available, nurses are expected to refine and update the original assessment.
Two types of data are collected during an assessment interview. Subjective data refers to the client’s perception of data and what the client or family says about the data (e.g., “I have a severe pain in my chest”). Client data about alternative forms of treatment, medications, and previously used care systems are relevant pieces of information. Objective data refers to data that are directly observable or verifiable through physical examination or tests (e.g., an abnormal electrocardiogram). Combined, these data will present a complete picture of the client’s health problem.
Observations of the client’s appearance and nonverbal behaviors can help nurses make inferences. An inference is an educated guess about the meaning of an observed behavior or statement. To be sure that the inference represents a correct interpretation of an observation or statement, you must validate the data with the client. For example, if a client is withdrawn and distractible, the nurse may infer that the client is struggling with an internal emotional issue. To validate this inference, you might comment, “You seem withdrawn, as though something is troubling you. Is that true for you right now?”
You also can use data cues, defined as small pieces of data that would not reveal much when taken by themselves but, when considered within the total assessment picture, can lead the nurse to ask further questions (Avant, 1991). For example, hesitancy about a certain topic, complaints of hunger or thirst, dry skin, or agitation is a data cue that can help nurses to seek a fuller explanation.
The assessment should consider more than client problems. Appraisal of client strengths is an important dimension of the assessment process as it provides a built-in resource asset for resolving health problems. Identifying client strengths is particularly important in today’s health care environment, when clients have to assume much more responsibility for their health care than previously. Analysis of the client’s support systems including level of utilization, availability, and social role is relevant data, as is the client’s spiritual or philosophical beliefs and values. Environmental, economic, and legal factors also should be included when related to the client’s health and well-being.
Throughout the assessment phase, you will need to validate the information you receive from the client and significant others to make sure that the data are complete and accurate. Ask the client for confirmation that your perceptions and problem analysis are correct periodically throughout the assessment interview, and summarize your impressions at the end. An assessment summary should highlight important elements in ways that are easily understood and retrievable by everyone involved in the client’s care. After the summary, you should thank the client or health informant for giving you the information, with a brief explanation of what will happen with this information. Respectful, regular communication represents an important intersection between the nurse-client relationship and the nursing process.
Once the assessment is complete, the next step is to analyze the information and identify gaps in the data collection or content. One way to do this is to compare individual client data with normal health standards, behavior patterns, and developmental norms. Gordon’s 11 Functional Health Patterns (Box 2-3) provide a useful structure for clustering assessment data and help direct the choice of nursing diagnoses. The determination of whether a pattern is functional or dysfunctional is based on established norms for age and sociocultural standards (Gordon, 2007).
In each clinical situation, you should take individual differences and preferences into consideration. For example, maintaining a sufficient intake of food needs to be assessed in terms of what is adequate intake for an individual on the basis of age, activity, height-to-weight ratio, and current health status. Nutritional needs for an active teenager are greater than those for an older, sedentary adult. The nurse would ask different specific questions of a client with diabetes, anorexia, or obesity regarding nutritional intake and food choices than of those for whom potential deviations would not appear to be an issue.
Environmental factors such as socioeconomic status and culture can influence the nature of a client’s health care needs. For example, diet choices and lack of prenatal care can represent financial constraints, rather than preference. Lack of knowledge about health care options, access, and experience are additional issues that nurses need to consider.
Documentation of relevant problems, observations, and assessments form the basis for planning care. A direct relationship among assessment data, nursing diagnosis, treatment goals, and intervention strategies should exist. Health care concerns judged potentially responsive to nursing intervention form the basis for the selection of nursing diagnoses.
Planning
The planning phase begins with the development and prioritization of relevant nursing diagnoses related to identified nursing problems. Nursing diagnoses is the term used to describe the client’s human responses to medical diagnoses (Carpenito-Moyet, 2008). They should complement, not compete, with the actual medical diagnosis of a health problem.
The nursing diagnosis consists of three parts: problem, cause, and evidence (North American Nursing Diagnosis Association [NANDA], 2005).
• Problem: A statement identifying a health problem or alteration in a client’s health status, requiring nursing intervention. Using a list of the most recent NANDA diagnoses, you would pick a NANDA diagnosis that best represents the identified problem or potential problem.
• Cause: A statement specifying the probable causative or risk factors contributing to the existence or maintenance of the health care problem. The cause of a problem can be psychosocial, physiologic, situational, cultural, or environmental in nature. The phrase “related to” (R/T) serves to connect the problem and causative statements. Example: “Impaired communication related to a cerebrovascular accident.”
• Evidence: A statement identifying the clinical evidence (behaviors, signs, symptoms) that support the diagnosis. An example of a nursing diagnosis statement would be “Impaired verbal communication related to a cerebrovascular accident, as manifested by incomplete sentences and slurred words.”
The nursing diagnosis should be written in such clear, precise language that any member of the interdisciplinary health care team can look at the statement and be able to identify relevant client issues.
Nurses use Maslow’s Hierarchy of Needs (see Chapter 1) to prioritize goals and objectives. Examples of nursing problems associated with each level of Maslow’s hierarchy are included in Table 2-4. Priority attention should be given to the most immediate, life-threatening problems. You also should consider what the client sees as his or her priorities, and incorporate this information in your prioritization. Otherwise, you and your client may be working at cross-purposes.
TABLE 2-4
Identifying Nursing Problems Associated with Maslow’s Hierarchy of Needs
| Physiologic survival needs | Circulation, food, intake/output, physical comfort, rest |
| Safety/Security needs | Domestic abuse, fear, anxiety, environmental hazards, housing |
| Love and belonging | Lack of social support, loss of significant person or pet, grief |
| Self-esteem needs | Loss of a job, inability to perform normal activities, change in position or expectations |
| Self-actualization | Inability to achieve personal goals |
Nurses may be able to address more than one nursing diagnosis at a time, because attention to several interconnected nursing diagnoses can often serve the same outcome. In addition to identifying and prioritizing nursing diagnoses, nurses are expected to monitor progress and look for potential complications accompanying nursing diagnoses. Examples of monitoring include vital signs, hydration, potential fluid imbalances, electrolytes, intravenous (IV) infusions associated with health issues requiring nursing diagnosis for resolution. Clearly written nursing diagnoses helps to ensure continuity and an ordered approach to meeting the individualized needs of the client (Carpenito-Moyet, 2008). Exercise 2-3 provides practice in considering cultural, age, and gender-related themes when using the nursing process with different types of clients.
Outcome Identification
Shaughnessy (1997) defines a health care outcome as “the change in health status between a baseline time point and a final time point” (p. 1225). The outcome refers to the result or end product of an identified nursing action. Some outcomes are unexpected. When this circumstance occurs, either the assessment failed to reveal a critical piece of data, the diagnosis or other issue was not validated with the client or family, the associated risks or plans for continuity of care were not factored into the treatment goals, or the treatment plan was not executed as collaboratively developed by the stakeholders in the process. Sometimes factors beyond the control of the client and health care provider interfere, for example, a change in the client’s physical or mental status. At any point in the process, ongoing assessment data can be used to revise the diagnosis, the plan itself, or implementation to meet the emerging needs in the clinical situation.
Clients should be involved in a shared decision-making process with health care providers in choosing relevant goals and outcomes (Kerr, 2009). Evidence of shared decision making can be documented with a simple statement, such as “Client states that she is satisfied that she made the right decision to decline surgery at this time.”
Outcome criteria need to take into account the client’s culture and life situation, present mental status, strengths and limitations, and available resources. Important client values and preferences should be factored into the development of relevant outcome criteria. Time limits need to be realistic so that the client can be successful.
Outcomes should be client-centered (e.g., “The client will…”) and described in specific, measurable terms. An appropriate treatment outcome for a client after surgery might be: “The client will show no signs of infection as evidenced by the incision being well-approximated and free of redness and swelling, normal temperature, and white blood cell count within normal limits by 9/21/09.” Nursing outcomes should be
• Documented in measurable terms
• Developed collaboratively with the client and other health providers
Each treatment outcome specifies the action or behavior that the client will demonstrate once the health problem is resolved. Outcome criteria are stated as long- and short-term treatment goals. Using measurable action verbs to describe what the client will be doing to achieve a short-term goal is key to effective identification of treatment outcomes; for example, “The client will take his medicine, as prescribed” is measurable: He either takes his medicine or he does not. Other measurable verbs include “perform,” “identify,” “discuss,” and “demonstrate.” Broad-spectrum verbs such as “understand,” “know,” and “learn” are not easily measurable and should not be used. Note the conditions or circumstances for outcome achievement “as prescribed” is specifically identified. Documentation of clinical outcomes should include client response.
Planning
The care plan serves as the structural framework for providing safe quality care. Each care plan should be individualized to reflect client values, clinical needs, and preferences. The care plan provides for continuity of care and supplies a concrete basis for supportive documentation of client response. The care plan is dynamic, meaning that it needs to be continuously updated as the client’s condition and health needs change.

Implementation
During the implementation phase, the client and nurse manage the care plan through specified nursing interventions and corresponding client actions. McCloskey and Bulechek (2000) define nursing intervention as “any treatment, based upon clinical judgment and knowledge, that a nurse performs to enhance patient/client outcomes. Nursing interventions include both direct and indirect care, nurse-initiated, physician-initiated, and other provider-initiated treatments” (p. xix). Interventions appropriate to the purposes of the nurse-client relationship include giving direct physical, psychological, social, and spiritual support; health teaching; collaborating with other health professionals on behalf of the client; continuing to make ongoing assessments; documenting client responses; and updating or revising the care plan as needed.
Nursing interventions can be classified as independent, dependent, or collaborative (Snyder, Egan, & Nojima, 1996). Independent interventions are those that nurses can provide without a physician’s order or direction from another health professional. Independent nursing interventions are permitted under Nurse Practice Acts and are protected through professional licensure and law. Many forms of direct care assistance, health education, health promotion strategies, and counseling fall into this category, and nurses are particularly well equipped to provide these functions. Dependent interventions require an oral or a written order from a physician to implement. For example, in most states, staff nurses cannot administer a medication without having a physician order it. The nurse is accountable for using appropriate knowledge, judgment, and competence in administering the medication at physician orders—and for questioning a physician about a problematic medical order. Thus, a nurse would not automatically carry out a physician’s order without considering first the appropriateness of the medication or without knowing appropriate dosage, mode of action, side effects, and potential adverse reactions. Collaborative interventions are those performed by the nurse and other health care team members with the mutual goal of providing the most appropriate and effective care to clients (McCloskey & Bulechek, 2000). Box 2-4 identifies factors the nurse should consider in developing nursing interventions.
Evaluation
In the evaluation phase, the nurse and client mutually examine the client’s progress or lack of progress toward achievement of treatment outcomes, mutually determined during the planning phase. When treatment goals are not achieved, or there is a lack of progress, the nurse needs to ask the following questions:
• Were the assessment data collected appropriate and complete?
• Was the nursing diagnosis appropriate?
• Were the treatment outcomes realistic and achievable in the time frame allotted?
• Were the nursing interventions chosen appropriate to the needs of the situation and the capabilities of the client?
• Was there any variable within the client, situation, or family that was overlooked and should have been addressed?
Issues and circumstances that can influence the achievement of treatment outcomes include the effectiveness, time efficiency, appropriateness, and adequacy of the nursing actions selected for implementation, economic barriers or assets, the motivation of the client, family obstruction or support, and obstacles in the setting, which could not have been anticipated. The nurse and client review progress, determine necessary modifications or need for referral, and terminate the relationship. Exercise 2-4 provides an opportunity to practice developing a care plan.
Documentation
Nurses are responsible for careful, accurate, and timely documentation of nursing assessments, the care given, and the behavioral responses of the client. This documentation represents a permanent record of the client’s health care experience. In the eyes of the law, failure to document in written form any of these elements means the actions were not taken.
Two common models for documenting nursing care are the Nursing Outcomes Classification (NOC) and Nursing Interventions Classification (NIC) systems, which complement the function of the other. The NOC model is linked to the problem (nursing diagnosis), whereas the NIC intervention classification is linked to the related or contributing factors (Marrs & Lowery, 2006). These classification systems help standardize the language used to describe the nursing process. Frisch (2001) observed, “Nurses documenting practice using these systems are accomplishing three important things: appropriate documentation of care, identification of work as within the scope of professional nursing, and building a body of knowledge for nurses on the use of specific interventions” (pp. 11–12).
Clients need to trust that their health care provider is accurately and appropriately representing their voice and experience in medical care records. The medical record of care and treatment is also used to direct and improve client-centered care. Although nursing documentation usually covers documentation of biophysical issues, important aspects of nursing care related to the client’s perspective, spiritual state, and learning needs are not always adequately noted (Laitinen, Kaunonen & Astedt-Kurki, 2010). Statements related to accommodations made for cultural, religious, and spiritual practices and preferences should be included in the record of care.
Verbal Reporting: Using the SBAR as a Communication Tool
Nurses need to verbally communicate assessment data and changes in health status to physicians, nurse colleagues, and others involved in the client’s care on a regular basis. The SBAR format is a standardized assessment reporting format that helps nurses communicate a clear, succinct overview of critical information in an organized, thoughtful way. This can be especially important when communicating with physicians by phone (Rodgers, 2007). When communicating by phone, it is useful to have the client’s chart in front of you.
SBAR is an acronym used to describe the
Situation (What is going on with the patient?)
Background (What is the key clinical background or context?)
Assessment (What do I think the problem is?)
Recommendation (What do I recommend or what do I want you to do?) (Guise & Lowe, 2006, p. 313)
Table 2-5 provides a sample of how nurses can use this structured format in communicating assessment data and changes in health status effectively.
TABLE 2-5
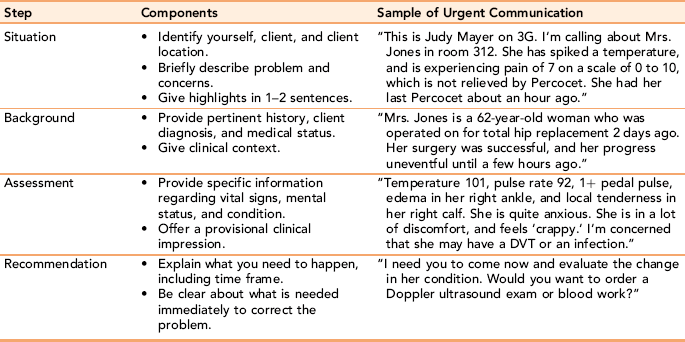
Developed in consultation with Barbara Dobish, RN, MS, Assistant Professor, University of Maryland, March 10, 2010.
The Joint Commission, the Institute for Health Care Improvement, and the AACN all support the use of SBAR as a desirable structured communication format. Given these approvals, Pope et al. (2008) suggest that the SBAR should be considered a “best practice” communication tool. In addition to using SBAR when there is a change in a client’s health status, this communication format is used between shifts between nurse colleagues, between nurses and physicians during rounds, transfer and handoffs from one care setting or unit to another, and presurgery handoffs (Dunsford, 2009).
A distinct advantage of using SBAR as a primary communication tool between physicians and nurses is that it cuts down on professional differences in communication styles (Haig, Sutton, & Whittington, 2006). In addition to communication with professional colleagues at regular intervals or when a client’s condition changes, nurses are accountable for orally informing ancillary clinical staff about the meaning of changes in the client’s condition. They are responsible for appropriately supervising their care of the client, and for questioning unclear or controversial orders made by a physician. (See Chapter 22 and 24 for more information and related exercises).
Protecting the client’s privacy
Jones (1998) states: “Privacy refers to a client’s right to have control over personal information whereas confidentiality refers to the obligation not to divulge anything said in a nurse-client relationship” (p. 5). As data is increasingly stored and transmitted through electronic record keeping, issues related to maintaining client privacy are under greater scrutiny. Institutional policies and federal law provide specific guidelines that all health care providers are required to follow. Kerr (2009) refers to the nurse’s obligation to protect a client’s privacy as a “sacred trust” (p. 315). The client’s right to have personal control over personal information is upheld through federal HIPAA regulations. The ANA Code of Ethics (2003) specifically addresses the nurse’s responsibility to safeguard the client’s right to privacy.
HIPAA Regulatory Compliance
In the United States, the first federal legislation dealing with privacy of medical records was part of P.L. 104-191, the Health Insurance Portability and Accountability Act of 1996 (U.S. Department of Health and Human Services [DHHS], 2003). HIPAA regulations protect the privacy of the client’s medical record and the client’s right to have control over his or her identifiable information in health care records. Health care providers must provide clients with a written notice of their privacy practices and procedures. Key elements of the HIPAA privacy regulations are presented in Box 2-5.
HIPAA privacy rules govern the use and disbursement of individually identifiable health information, and give individuals the right to determine and restrict access to their health information. Clients have the right to access medical records, request copies, and/or request amendments to health information contained in the record. The Fair Health Information Practices Act of 1997 stipulates civil and criminal penalties for not allowing clients to review their medical records (Milton, 2009).
HIPAA regulations protect the confidentiality, accuracy, and availability of all electronic protected information, whether created, received, or transmitted. Strict maintenance of written records in a protected, private environment is required. Other potential issues of concern about privacy involve cell phones, picture taking, use of hand held devices, use of fax machines, internet user ID and passwords, and use of RFID technologies or electronic monitoring devices (Kerr, 2009).
Health care providers must get written authorization from clients before disclosing or sharing any personal medical information. Client authorization is not required in situations concerning the public’s health, criminal and legal matters, quality assurance, and aggregate record reviews for accreditation. In addition, “information can and must be shared between healthcare providers who have a legitimate need to know in order to provide safe and appropriate care” (Brooke, 2009, p. 11). This provision typically refers to emergency situations such as in the case of a client who is unable because of a psychotic state to give accurate information, or to sign a release of information form in the emergency department. HIPAA provisions allow nurses to gather information about the client’s medical condition or drug history in an emergency for the purpose of providing immediate treatment, without having the client’s written permission. When this occurs, it is important to document in the client’s chart the immediacy of the need to obtain the required information.
The Office of Civil Rights enforces HIPAA regulations. Agencies and providers face severe penalties for violations, with improper disclosure of medical information punishable by fines or imprisonment. Study your agency’s policies to determine to whom and under what conditions personal health information can be released. More information can be obtained through their web site (www.hhs.gov/ocr).
Protecting Client Privacy in Clinical Situations
In addition to informational privacy, which is a legal mandate, informal protection of the client’s right to control the access of others to one’s person in clinical situations is an ethical responsibility. The client and family usually view protecting the client’s privacy in the clinical setting as a measure of respect. Simple strategies that nurses can use to protect the client’s right to privacy in clinical situations include:
• Providing privacy for the client and family when disturbing matters are to be discussed
• Explaining procedures to clients before implementing them
• Entering another person’s personal space with warning (e.g., knocking or calling the client’s name) and, preferably, waiting for permission to enter
• Providing an identified space for the client’s personal belongings
• Encouraging the inclusion of personal and familiar objects on the client’s nightstand
• Decreasing direct eye contact during hands-on care
• Minimizing body exposure to what is absolutely necessary for care
• Using only the necessary number of people during any procedure
Confidentiality
Protecting the privacy of client information and confidentiality are related, but separate concepts. Confidentiality is defined as providing only the information needed to provide care for the client to other health professionals who are directly involved in the care of the client. Kerr (2009) notes that “a violation occurs when information deemed private, and divulged in confidence, is shared with others” (p. 315). The need to share information with other health professionals directly involved in care on a “need to know” basis should be made clear to the client as they enter the clinical setting. Other than these individuals, the nurse must have the client’s written permission to share his or her private communication, unless the withholding of information would result in harm to the client or someone else, or in cases where abuse is suspected. Confidential information about the client cannot be shared with the family or other interested parties without the client or designated legal surrogate’s written permission. Shared confidential information, unrelated to identified health care needs, should not be communicated or charted in the client’s medical record.
Confidentiality within the nurse-client relationship involves the nurse’s legal responsibility to guard against invasion of the client’s privacy related to the following:
• Releasing information about the client to unauthorized parties
• Unwanted visitations in the hospital
• Discussing client problems in public places or with people not directly involved in the client’s care
• Taking pictures of the client without consent or using the photographs without the client’s permission
• Performing procedures such as testing for HIV without the client’s permission
• Publishing data about a client in any way that makes the client identifiable without the client’s permission (Cournoyer, 2001)
Professional Sharing of Confidential Information: Nursing reports and interdisciplinary team case conferences are acceptable forums for the discussion of health related communications shared by clients or families. Other venues include change-of-shift reports, one-on-one conversations with other health professionals about specific client care issues, and client-approved consultations with client families. Discussion of client care should take place in a private room with the door closed. Only relevant information specifically related to client assessment or treatment should be shared. Discussing private information casually with other health professionals without the client’s permission is an abuse of confidentiality. The ethical responsibility to maintain client confidentiality continues even after the client is discharged from care.
Mandatory Reporting: Mandatory reporting of personal health information related to certain communicable or sexually transmitted diseases, child and elder abuse, and the potential for serious harm to another individual are considered exceptions to sharing of confidential information. Required mandatory disclosures may differ slightly from state to state. In general, nurses are required to report all notifiable infectious diseases and abuse to appropriate state and local reporting agencies. This duty to report supersedes the client’s right to confidentiality or privileged communication with a health provider. Relevant client data should be released only to the appropriate local, state, or federal agency and as confidential information. The information provided must be the minimum amount needed to accomplish the purposes of disclosure, and the client needs to be informed about what information will be disclosed, to whom, and for what reason(s).
Informed Consent
Informed consent is more than a signature on a form indicating a client’s willingness to undergo a treatment or procedure (Neary, Cahill, Kirwan, Kiely, & Redmond, 2008). Informed consent is defined as a focused communication process in which the professional nurse or physician discloses all relevant information related to a procedure or treatment, with full opportunity for dialogue, questions, and expressions of concern, before asking the client or health care agent for the client to sign a legal consent form. Unless there is a life-threatening emergency, all clients have the right to give informed consent. For legal consent to be valid, it must contain three elements (Northrop & Kelly, 1987):
• The client must have full disclosure about the risks, benefits, cost, potential side effects or adverse reactions of the proposed treatment or procedure, and should be provided with information about other treatment alternatives, if available.
• The client must have the capacity and competency to understand the information and to make an informed choice.
Before initiating an informed consent process, nurses need to assess the adequacy of a client’s “hearing, sight, mental status, literacy level, and ability to understand the process or procedure” (Plawecki & Plawecki, 2009, p. 3). Essential disclosures needed to help ensure informed consent include:
• The nature and purpose of the proposed treatment or procedure
• The risks and benefits of not receiving or undergoing a treatment or procedure
• The client has the right to refuse treatment or discontinue it without penalty, unless it is an emergency situation
Clients should be given ample opportunity to ask questions and to express concerns. They should never feel coerced or pressured into consenting to treatment, as allowing a client to sign a consent form without fully understanding the meaning of what he or she is signing will invalidate the consent (Brooke, 2009). Ending the conversation leading to the actual signing of the consent form should always include the question, “Is there anything else that you think might be helpful in making your decision?” This type of dialogue gives the client permission to ask a question or address a concern that the nurse may not have given thought to in the informed consent discussion.
Guidelines Governing Legal Consent: Only legally competent adults can give legal consent; adults who are mentally retarded, developmentally disabled, or cognitively impaired cannot give legal consent (White, 2000). Evaluation of competency is made on an individual basis (e.g., in the case of emancipated adolescents no longer under their parent’s control, brain-injured clients, or clients with early dementia) to determine the extent to which they understand what they are signing.
Legislation exists in all states, such that a legal guardian or personal health care agent can provide consent for the medical treatment of adults who lack the capacity to consent on their own behalf. In most cases, legal guardians or parents must give legal consent for minor children, defined as those younger than 18, unless the youth is legally considered an emancipated minor. Minors can also give consent in cases of immediate emergencies.
Emancipated minors are mentally competent adolescents younger than 18 who petition the courts for adult status. To be considered, adolescents must be financially responsible for themselves, and no longer living with their parents. Other criteria include being married, having a child, and/or being in military service.
Summary
This chapter addresses the professional, legal, and ethical standards nurses use to guide their actions in the nurse-client relationship. Standards of professional practice provide a measurement benchmark, used to assess nursing competence in clinical situations regardless of specialty. Nurses are bound legally by the principles of tort law to provide a reasonable standard of care. This means that the nurse is obligated to provide a level of care that a reasonably prudent nurse with similar education and experience would provide in a similar situation. The ANA Code of Ethics for Nurses provides a conceptual framework for identifying the moral dimensions of nursing practice; it is an important guide to choice of actions in nurse-client relationships. Each state’s Nurse Practice Acts defines the scope of nursing practice for nurses practicing in that state. Multistate licensure in a compact state allows registered nurses licensed and residing in a compact state to practice in other compact states without obtaining a second license.
The nursing process serves as a clinical management framework. It consists of sequential, overlapping phases: assessment, planning (including diagnosis and development of outcome criteria), implementation, and evaluation. The client is an active participant and decision maker in all phases. Nurses use the SBAR format to communicate essential information to other health professionals involved in the client’s care.
Nurses are legally and ethically responsible for protecting the client’s privacy. Privacy and confidentiality are related but separate concepts nurses use to protect a client’s freedom of choice about sharing personal information with others. Privacy refers to a client’s right to have control over personal information; confidentiality refers to the obligation not to divulge private information from a nurse-client relationship. HIPAA regulations, mandated by federal law govern the use and disbursement of personally identifiable health information, and give individuals the right to determine and restrict access to their health information.
References
Aiken, T.D. Legal, ethical, and political issues in nursing. Philadelphia: FA Davis Company, 2004.
American Nurses Association. Code of ethics for nurses with interpretive statements. Washington, DC: Author, 2001. [(approved revised)].
American Nurses Association. Nursing’s Social Policy Statement, 2nd ed. Washington, DC: Author, 2003.
American Nurses Association. Nursing’s Social Policy Statement: The Essence of the Profession. Washington, DC: Author, 2010.
American Nurses Association. Nursing: scope and standards of practice. Washington, DC: Author, 2010.
Avant, K. Paths to concept development in nursing diagnosis. Nurs Diagn. 1991;2(3):105–110.
Basanta, W.E. Advance directives and life sustaining treatment: a legal primer. Hematol Oncol Clin North Am. 2002;16(6):1381–1396.
Brooke, P. Legal questions. Nursing. 2009;39(4):10–11.
Canadian Nurses Association The code of ethics for registered nurses, Alberta, Canada, Author, 1997. Available online:, http://www.cna-nurses.ca/CNA/practice/ethics/code/default_e.aspx.
Carpenito-Moyet, L.J. Handbook of nursing diagnoses, ed 12. Philadelphia: Lippincott Williams & Wilkins, 2008.
Catalano, J. Nursing now: today’s issues, tomorrow’s trends, ed 5. Philadelphia: FA Davis, 2008.
Cournoyer, C. Legal relationships in nursing practice. In: Creasia J., Parker B., eds. Conceptual foundations: the bridge to professional nursing practice. St. Louis: Mosby, 2001.
Dimond, B. Legal aspects of nursing, ed 5. Essex, United Kingdom: Pearson Education Limited, 2008.
Dunsford, J. Structured communication: improving patient safety with SBAR. Nurs Womens Health. 2009;13(5):384–390.
Frisch, N., Nursing as a context for alternative/complementary modalities. Online J Issues Nurs, 2001;6(2):2. http://www.nursingworld.org/ojin/topic15/tpc15_2.htm. [[serial online] Available online:].
Gordon, M. Manual of nursing diagnoses, ed 11. Sudbury, MA: Jones and Bartlett Publishers, 2007.
Guido, G. Legal and ethical issues in nursing, ed 5. Saddle River, NJ: Prentice Hall, 2009.
Guise, J.M., Lowe, N. Do you speak SBAR? J Obstet Gynecol Neonatal Nurs. 2006;25(3):313–314.
Haig, K., Sutton, S., Whittington, J. SBAR: a shared mental model for improving communication between clinicians. J Qual Patient Saf. 2006;32(3):167–175.
Joint Commission on Accreditation of Health Care Organizations. Accreditation manual for hospitals. Chicago: Author, 1991.
Joint Commission on Accreditation of Health Care Organizations. Hospital accreditation standards. Oakbrook Terrace, IL: Joint Commission Resources, 2007.
Jones, D. Adjunctive therapies: issues and interventions in psychiatric nursing practice, ed 4. New Westminster, British Columbia, Canada: Douglas College, 1998.
Kerr, P. Protecting patient education in an electronic age: A sacred trust. Urol Nurs. 2009;29(5):315–319.
Laitinen, H., Kaunonen, M., Astedt-Kurki, P. Patient-focused documentation expressed by nurses. J Clin Nurs. 2010;19(1):489–497.
LaSala, C. Moral accountability and integrity in nursing practice. Nurs Clin North Am. 2009;44:423–434.
Marrs, J., Lowry, L. Nursing theory and practice: connecting the dots. Nurs Sci Q. 2006;19:44–50.
McCloskey J.C., Bulechek G.M., eds. Nursing interventions classification (NIC), ed 3, St Louis: Mosby, 2000.
Milton, C. Information sharing: transparency, nursing ethics, and practice implications with electronic medical records. Nurs Sci Q. 2009;22(3):214–219.
NANDA. Nursing diagnoses: definitions & classification. Philadelphia: NANDA International, 2005.
National Council of State Boards of Nursing (NCSBN). Available online: https://www.ncsbn.org/boards.htm. [Accessed September 5, 2008].
Neary, P., Cahill, R., Kirwan, W., et al. What a signature adds to the consent process. Surg Endosc. 2008;22(12):2698–2704.
Northrop, C., Kelly, M. Legal issues in nursing. St Louis: Mosby, 1987.
Otto, S. A nurse’s lifeline: a nursing ethics committee offers the chance to review and learn from ethical dilemmas. Am J Nurs. 2000;100(12):57–59.
Plawecki, L., Plawecki, H. Simply stated: informed consent can be a very complex task. J Gerontol Nurs. 2009;35(2):3–4.
Pope, B., Rodzen, L., Spross, G. Raising the SBAR: how better communication improves patient outcomes. Nursing. 2008;38(3):41–43.
Rodgers, K.L. Using the SBAR communication technique to improve nurse-physician phone communication. AAACN Viewpoint. 2007. [March/April 7–9].
Scott, R. Legal aspects of documenting patient care for rehabilitation professionals, ed 3. Sudbury, MA: Jones & Bartlett, 2006.
Shapiro, S. Evaluating clinical decision rules. Western J Nurs Res. 2005;271(5):655–664.
Shaughnessy, P. Outcomes across the care continuum: home health care. Med Care. 1997;35(12):1225–1226.
Snyder, M., Egan, E.C., Nojima, Y. Defining nursing interventions. Image J Nurs Sch. 1996;28(2):137–141.
U.S. Department of Health and Human Services (DHHS) Summary of the HIPAA privacy rule, 2003. Retrieved July 1, 2010, from, http://www.hhs.gov/ocr/privacy/hipaa/understanding/summary/index.Html.
Vuckovich, P. Psychiatric advance directives. J Am Psychiatr Nurses Assoc. 2003;9(2):55–59.
Westley, C., Briggs, L. Stages of change model to improve communication about advance care planning. Nurs Forum. 2004;39(3):5–12.