Developing Therapeutic Communication Skills
At the end of the chapter, the reader will be able to:
1 Discuss the concept of therapeutic communication.
2 Describe the characteristics of client-centered communication.
3 Apply communication strategies and skills in client-centered relationships.
4 Discuss active listening responses used in therapeutic communication.
5 Discuss the use of verbal responses as a communication strategy.
6 Describe other forms of communication used in nurse-client relationships.
Communication is an important cornerstone of all clinical encounters. This chapter focuses on therapeutic communication skills and strategies that nurses need to support, educate, and empower people to effectively cope with their health-related issues. The chapter reviews the purpose and components of therapeutic communication, using a client-centered focus. Applications describe active listening responses, verbal communication strategies, and other communication techniques applicable in nurse-client relationships.
Basic concepts
Therapeutic communication, a term first coined by Jurgen Ruesch in 1961, refers to an interactive dynamic process entered into by nurse and client for the purpose of achieving identified health-related goals. It takes place within the context of a healing conversation, and encompasses both verbal and nonverbal components. Therapeutic communication skills serve as fundamental building blocks for the development of effective therapeutic relationships.
It differs from “social chit chat” in that it promotes the client’s personal development (Peplau, 1960, p. 964). Therapeutic communication is the primary means through which nurse and client exchange information about health matters, plan treatment approaches, reach consensus about treatment decisions, conduct treatment activities, and evaluate clinical outcomes. It is the basis for developing the working partnerships between client and health providers needed to support improved treatment outcomes.
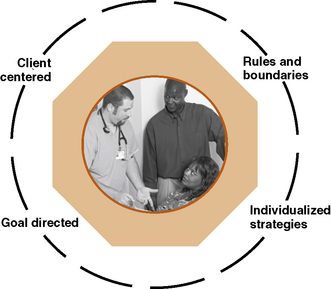
Each therapeutic conversation is unique because the people holding them are different (Caughan & Long, 2000). Communication techniques are similar to those used spontaneously in social situations, with notable modifications. Therapeutic conversations have a specific health related purpose. They take place within a defined health care format and are time limited. These conversations are subject to federal guidelines and professional standards regarding confidentiality and protected information. Characteristics of therapeutic communication are displayed in Figure 10-1. Therapeutic communication is client centered and uses a deliberate, health-focused dialogue. Direct interaction comes to an end when health goals are achieved, clients are discharged, or clients are referred to a different care setting.
Purpose of therapeutic communication
Therapeutic conversations offer a safe, empathetic way for clients to explore the meaning of their illness experience and to learn the best ways of coping with it. Therapeutic conversations tell the story of a personal illness, with nurse and client both contributing to the telling of it.
Quality clinical communication is essential to achieving positive health outcomes and client satisfaction. Interpersonal communication skills influence the completeness of diagnostic information, compliance with treatment, and client satisfaction with care. “Good” clinical experiences typically involve human communication encounters in which human needs are respected and the humanity of the clinician is transparent. With “negative” clinical encounters, clients experience disconnects with the knowledge and interpersonal care the client or family expects from the provider. Poor communication is implicated as a key factor in clinical safety errors and malpractice allegations.
Essential components
Fundamental components of communication—sender, receiver, message, channels, and context—are also applied to therapeutic communication. Therapeutic communication is a reciprocal process that begins with active listening (Bush, 2001). Active listening combines verbal and nonverbal components of a message into an integrated, meaningful whole.
Active listening is a dynamic process in which a nurse hears a client’s message, decodes its meaning, asks questions for clarification, and provides feedback to the client. Active listening allows people to offer presence and to bear witness to one another (Kagan, 2008). Attentive listening for the client’s perspective without making judgments and also using listening responses increase understanding.
The goal of active listening is to fully understand what the client is trying to communicate through his or her story. As you ask clarifying questions and share your own thinking process about what you are hearing, you are developing a more in-depth understanding of the health care situation from the client’s perspective.
Included in each participant’s communicated message are important nonverbal instructions (metacommunication) about the interpretation of the message. If a nurse sits down in a relaxed position with good eye contact and actively listens, the verbal and nonverbal message of interest is congruent. The same verbal message, delivered while looking at the clock or a watch, provides a nonverbal message that the nurse doesn’t have time to listen. When verbal and the nonverbal messages are congruent, the message is credible. If the two are incongruent, it creates doubt in the mind of the listener, and the message is suspect. If you notice nonverbal behaviors that seem to contradict words, or the client seems sad or distracted, you might want to call the client’s attention to the discrepancy with a simple statement, such as, “You seemed quite animated yesterday; I notice that you seem a little subdued today. Is something going on that we should talk about?”
Verbal responses refer to the spoken words people use to communicate with each other. Unlike the written word, they cannot be erased, although they can be explained, or modified. Words are the primary means through which nurse and client will organize data about problems, explore different options, make meaning of experiences, and dialogue with each other. The meaning of words resides in the person who uses them, not in the words themselves. When languages or word connotations differ, meaning changes. Nurses should pay close attention to the client’s verbal expression and forms of language (Kettunen, Poskiparta, & Liimatainen, 2001) and mirror them, when possible. Verbal responses should be clear, complete, and easily understandable. Choice of words is important. Words should neither overstate nor understate the situation. Words are not the sole source of meaning. Nadzam (2009) notes, “Communication is not just about what a person says, but how he or she says it” (p. 184). Nurses also need to be sensitive to what is left out of the message, as well as to what is included. How words are used should not cast doubt on the implications of the message. Straightforward messages are trustworthy. Vague messages are not.
Both words and nonverbal behaviors are subject to misinterpretation. Nurses need to check in with clients to ensure the accuracy of their perceptions. You can simply say, “I’d just like to check in with you to make sure that I understand. Are you saying that… ?”
Factors that affect communication
Readiness to engage in therapeutic relationships is influenced by personal and environmental factors that the nurse should take into consideration when relating to clients and families. Eye contact, genuine respect for the client, and clear, concise messages are fundamental tools. Words that respect a person’s culture, spiritual beliefs, and educational level capture the client’s attention. Conversely, words that disregard or dismiss the fundamental personhood of the client or family as being less important than that of the health care provider cause unnecessary damage.

Whether you are sitting or standing, your posture should be relaxed, with the upper part of your body inclined slightly toward the client.
People communicate nonverbally through body language, eye contact, and level of attention. The nurse consciously uses body language, gestures, and minimal verbal cues to encourage further communication. Physical cues are used to accentuate words or connect with people nonverbally, as well as verbally (Box 10-1).
Communication breaks down when the nurse or client do not share the same understanding of messages. Barriers to effective communication occur in clients when they are:
• Preoccupied with pain, physical discomfort, worry, or contradictory personal beliefs
• Unable to understand the nurse’s use of language or terminology
• Struggling with an emotionally laden topic
• Feeling defensive, insecure, or judged
• Confused by the complexity of the message—too many issues, tangential comments
• Deprived of privacy, especially if the topic is a sensitive one
• Have hearing or cognitive deficits that compromise receiving accurate messages
Barriers within the nurse occur when the nurse is not fully engaged with the client for the following reasons:
• Preoccupation with personal agendas
• Being in a hurry to complete physical care
• Making assumptions about client motivations
• Defensiveness or personal insecurity about being able to help the client
Exercise 10-1 is designed to help students identify difficult communication issues in nursing practice.
Professional self-awareness
Client-centered communication requires greater self-awareness. Nurses must become aware of their behaviors and responses, and recognize the sometimes unintentional effects these may have on the communication process.
Knowing your own biases and values is critical. Communication can be limited by a nurse’s standards concerning, for example, different sexual preferences, alcoholism, and teenage pregnancy. Nurses may feel intimidated by clients who have higher social status, education, or influence, and respond in subtle ways to these differences. Caring for clients who refuse to comply with treatment or who have given up can be a communication challenge for the nurse.
Self-awareness of personal prejudices and stereotypes allows nurses to separate the person from the behavior or problem, and to maintain the patience, neutrality, and understanding needed for therapeutic communication. Nurses have an ethical and professional responsibility to resolve personal issues so that countertransference feelings do not affect communication.
Environmental factors
Privacy, space, and timing are important factors that nurses need to consider. Clients need privacy, free from interruption and elimination of noise for meaningful conversations. “Noise” refers to any distraction, which interferes with being able to pay full attention to the discussion (Weiten, Lloyd, Dunn & Hammer, 2009). For example, TV or music can be distracting.
People require different amounts of personal space for conversation (Hall, 1959). Therapeutic conversations typically take place within a social distance (3–4 feet is optimal). Culture, personal preference, nature of the relationship, and the topic will influence personal space needs. Clients experiencing high anxiety may need more physical space, whereas clients experiencing a sudden physical injury or undergoing a painful procedure appreciate having the nurse in closer proximity. Sitting at eye level with bedridden clients is helpful.

Timing is critical. Planning communication for periods when the client is able to participate physically and emotionally is both time-efficient and respectful of the client’s needs. Clients must be given enough time to absorb material, to share their impressions, and to ask questions.
Client behavior can cue the nurse about emotional readiness and available energy. The presence of pain or variations in energy levels, anger, or anxiety will require extra time to inquire about the change in the client’s behavior and its meaning, before proceeding with the health care dialogue.
Client-centered communication
Client-centered care and collaborative partnerships in current health care deliverables require a broader span of communication skills. In the past, healing relationships were important sources of clinician information and expertise, which was shared with clients. Today, clients are viewed as equally important informational resources and collaborators in health care. Clients expect emotional support and guidance to assume greater personal responsibility for their health care. They not only require their clinicians to be technically competent; they expect them to be sensitive and accommodating of their concerns and treatment preferences. Clients want to be listened to, involved in their own care, and able to choose between treatment options. Epstein and Street (2007) identify six core, overlapping functions of patient-centered communication needed to achieve beneficial health outcomes.
Client-centered communication is an interactive reciprocal exchange of ideas in which nurses try to understand what it is like to be this person in this situation with this illness. Each client and family has its unique set of values, patterns of behavior, and preferences that must be taken into account. How clients communicate with the nurse varies, based on culture and social background factors. Client readiness to learn, personal ways of relating to others, physical and emotional conditions, life experiences, and place in the life cycle are related factors in planning and implementing contemporary care through therapeutic communication.
Client-centered conversations are structured to be person focused rather than problem focused. They include discussions needed for collaborative decision making and teaching clients self-management skills. Talking about complex health problems with a trained health professional allows clients and families to hear themselves, as they put health concerns into words. The feedback provided by the health professional ideally helps clients realistically sort out priorities and determine the actions they want to take in effectively coping with their health circumstances.
Active listening in client-centered conversations
Active listening is an intentional form of listening, which contributes to fewer incidents of misunderstanding, more accurate information, and stronger health relationships (Straka, 1997). Listening responses in a client-centered health environment ask about all relevant client health concerns, and take into account the client’s values, preferences, and expectations related to treatment goals, priorities, and attitudes about treatment suggestions. Queries might include open-ended questions such as “What is important to you now?” or “What are you hoping will happen with this treatment?” Sufficient information to support client decision-making and self-management of health problems is expected. Validation of client preferences might consist of asking the client, “How does the idea of __________ sound to you?” or “How easy will it be for you to learn to use your crutches?” Adding these questions may seem time consuming. If the answers lead to greater compliance and client satisfaction, then it may be more time efficient.
Applications
Applying concepts of client-centered communication
Building rapport
A client-centered communication process starts with the first encounter. Your initial presentation of yourself will influence the communication that follows. Your client should have your full attention. Entering the client’s space with an open, welcoming facial expression, respectful tone, and direct eye contact declares your interest and intent to know this person.
Communication involves the whole self. Your posture immediately gives a message to the client, either inviting trust or conveying disinterest. Whether you are sitting or standing, your posture should be relaxed, facing the client and leaning slightly forward.
Introduce yourself and identify the client by name before beginning conversation. Introductions are important, especially if many health professionals are involved in the client’s care (Van Servellen, 2009). When more than the client is involved in a discussion, expand the introductions if you are meeting other people for first time. It is important to center your attention on the client, but not ignore other family members. Speak directly to the client, but include family members with eye contact, physical cues, and so forth. Eye contact is an important inclusive gesture.
Keep in mind that clients will vary in their ability to effectively communicate their feelings, preferences, and concerns (Epstein & Street, 2007). Even their willingness to treat their clinicians as partner rather than absolute authority can reflect personality features, communication style, socioeconomic status, previous life experiences, and education level. Considering these factors allows you to phrase questions and interpret answers in meaningful ways.
Being fully present, providing relevant information, and listening to client concerns help build rapport through personalized communication. Clients who feel safe, accepted, and validated by their nurses find it easier to collaborate with them. Although rapport building begins with the initial encounter, it continues as a thread throughout the nurse-client relationship. Remember that clients are looking to you for not only competence, but for sincerity and genuine interest in them as individuals.
A client-centered communication process seeks to understand critical links between the client’s life experiences and values, and their current health problems. Nurses should strive to understand the whole person, including information from and about family members affected by the client’s illness.
The goal of client-centered communication is to find common ground related to identification of client problems, priorities, and treatment goals. Nurses need to understand what aspects of care are most important to a client and family, and what helps or hinders their capability to self-manage their health problems. Clients need to understand the full range of therapeutic choices available to them in treating and self-managing their illness.
The idea of health care as a shared partnership in which the client is an equal stakeholder and communicator in ensuring quality health care is relatively new. Building rapport requires:
• Empathetic objectivity, which allows you to experience clients as they are, not the way you would like them to be
• A “here and now” focus on the current issues and client concerns
• Demonstration of respect, and asking questions about cultural and social differences that can influence treatment
• Authentic interest in the client and a confident manner that communicates competence
• The capability to consider competing goals and alternative ways to meet them
Exercise 10-2 is designed to increase the student’s understanding of communication strategies using a client-centered focus.
Observation
There are different “channels” of nonverbal communication (e.g., facial expressions, vocal tones, gestures and body positions, body movements, touch, and personal space). Take note of whether cues such as the client’s facial expression, body movements, posture, and breathing rate support or negate the meaning of the spoken message.
Burgoon, Guerrero, & Floyd (2009) note up to 65% of interpersonal communication is nonverbal. Clients cannot always put their concerns into words. Some are not aware of them. Others experience powerful emotions that make verbalizing personal concerns difficult. Watch for nonverbal cues from the client. Changes in body language and nonverbal cues noted when the nurse or clinician is speaking can indicate discomfort with the message. The client who declares that he is ready for surgery and seems calm may be sending a different message through the tense muscles the nurse accidentally touches. This body language cue suggests that the client may be worried about the surgery. Environmental cues such as a half-eaten lunch or noncompliance with treatment can provide nonverbal evidence that a client is in distress. Calling attention to conflicting verbal and nonverbal responses is useful if done in a spirit of tentative inquiry. You might note that the client seems nervous or is not paying attention to what you are saying. Inquire about your perception: “I’m wondering what you are feeling right now, about what I am saying,” or “I noticed when I mentioned __________, your expression changed.” (Weiten, Lloyd, Dunn, & Hammer, 2009). Nonverbal behaviors and signals are culture bound so they may mean different things in different cultures (Samovar, Porter, & McDaniel, 2009). Exercise 10-3 provides practice with observing and interpreting the meaning of nonverbal behaviors.
Asking questions
A client-centered interview begins with encouraging clients to tell their story in an authentic way (Platt & Gaspar, 2001). Applicable questions are a primary means of helping clients tell their story, obtaining relevant information, and reducing misunderstandings. There are different ways of asking questions. Questions fall into three categories: open ended, closed ended, and circular.
Open-Ended Questions
Open-ended questions encourage the client to take the initiative. An open-ended question is similar to an essay question on a test. It is open to interpretation and cannot be answered by “yes,” “no,” or a one-word response. Questions are designed to permit the client to express the problem or health need in his or her own words. They usually begin with words such as “what,” “why, “how,” “can you describe for me…” etc. Telling the story of an illness rather than listing discrete facts helps the client and nurse link the context of a health disruption with symptoms and provides more complete information. Open-ended questions ask the client to think and reflect on their situation. They help connect relevant elements of the client’s experience (e.g., relationships, impact of the illness on self or others, environmental barriers, potential resources). Open-ended questions are used to elicit the client’s thoughts and perspectives without influencing the direction of an acceptable response. For example,
“Can you tell me what brought you to the clinic (hospital) today?”
“What has it been like for you since the accident?”
These questions are general, rather than specific, and open to a variety of answers. An open-ended question is usually just the introduction, requiring further dialogue about relevant topics. Ending the dialogue with a general open-ended question, such as “Is there anything else that is concerning you right now?” can provide relevant information that might otherwise be overlooked. Look for tone of voice, body movements, and so on as clues to the level of anxiety. Exercise 10-4 provides an opportunity to practice the use of open-ended questions.
Focused Questions
Focused questions require more than a yes or no answer, but place limitations on the topic to be addressed. Emergencies or other circumstances requiring immediate answers involve the use of focused or closed-ended questions. Focused questions can clarify the timing and sequence of symptoms, and concentrate on details about a client’s health concerns, for example, when symptoms began, what other symptoms the client is having, or what the client has done to date to resolve the problem. Clients with limited verbal skills sometimes respond better to focused questions because they require less interpretation. Examples include:
Focused questions can be used to help clients prioritize immediate concerns; for example, “Of all the concerns we have talked about today, which is the most difficult for you?”
Circular questions are a form of focused questions that give attention to the interpersonal context in which an illness occurs. They identify differences in the impact of an illness on individual family members or changes in relationship brought about by the health circumstances (see Chapter 13).
Closed-Ended Questions
Closed-ended questions narrow the focus of the question to a single answer, for example, yes, no, or simple phrase answer. They are useful in emergency situations, when the goal is to obtain information quickly, and the context or client’s emotional reactions are of secondary importance in the immediate situation. Examples of closed-ended questions include:
What the nurse listens for
Box 10-2 identifies what the nurse listens for in client-centered conversations. Therapeutic communication involves both intrapersonal and interpersonal processes. As Myers (2000) suggests, “Any actual dialogue has an inner, subjectively experienced component” (p. 151). Intrapersonal communication refers to the internal processing that goes on within a person about the underlying feeling or core idea associated with the verbal message. It is not usually intentionally expressed.
Listening for themes requires observing and understanding what the client is not saying, as well as what the person actually reveals. Identifying the underlying themes presented in a therapeutic conversation can relieve anxiety and provide direction for individualized nursing interventions. For example, the client may say to the nurse, “I’m worried about my surgery tomorrow.” This is one way of framing the problem. If the same client presents his concern as “I’m not sure I will make it through the surgery tomorrow,” the underlying theme of the communication changes from a generalized worry to a more personal theme of survival. Alternatively, a client might say, “I don’t know whether my husband should stay tomorrow when I have my surgery. It is going to be a long procedure, and he gets so worried.” The theme (focus) expresses her concern about her relationship with her husband. In each communication, the client expresses a distinct theme of concern related to a statement, but the emphasis in each requires a different response.
Emotional objectivity in making sense of client themes is essential. “Objectivity here refers to seeing what an experience is for another person, not how it fits or relates to other experiences, not what causes it, why it exists, or what purposes it serves. It is an attempt to see attitudes and concepts, beliefs and values of an individual as they are to him at the moment he expresses them—not what they were or will become” (Moustakas, 1974, p. 78). Exercise 10-5 provides practice in listening for themes.
Communication patterns
Communication patterns provide a different type of information. Some clients exaggerate information; others characteristically leave out highly relevant details. Some talk a lot, using dramatic language and multiple examples; others say very little and have to be encouraged to provide details. Evaluation of the client’s present overall pattern of interaction with others includes strengths and limitations, family communication dynamics, and developmental and educational levels. Culture, role, ways of handling conflict, and ways of dealing with emotions reflect and influence communication patterns. Being respectful of the client’s communication pattern involves accepting the client’s communication style as a part of who the person is, and not expecting the person to be different. For example, AJ is a client with chronic mental illness. She frequently interrupts and presents with a loud, ebullient opinion on most things. This is AJ’s communication pattern. To engage successfully with her, you would need to listen, while accepting her way of communicating as a part of who she is, without getting lost in detail.
Using intuitive feelings
Intuitive feelings can emerge as a personal listening response from within the nurse during the course of a conversation with a client or family. Personal ways of knowing represent a body-centered way of listening to feelings about underlying issues and concerns (Klagsbrun, 2001). For example, if a nurse has no particular personal reason for reacting to the client with anger, fear, or sadness, this inner response may reflect a client’s unexpressed feeling. Behavioral reactions that the nurse feels are out of proportion to the situation (e.g., complete calm before surgery, excessive anger, noncompliance or passive compliance with no questions asked, guarded verbalizations, incongruent facial expressions or body language, or social withdrawal) can be danger signals that need further exploration.
Active listening responses
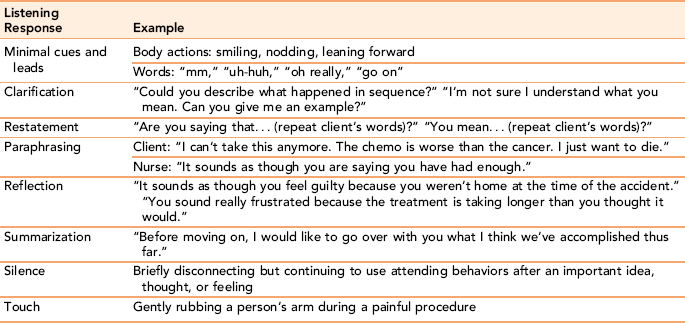
Active listening responses show the client that the nurse is fully present as a professional partner in helping the client understand a change in health status and the best ways to cope with it (Keller & Baker, 2000). Minimal verbal cues, clarification, restatement, paraphrasing, reflection, summarization, silence, and touch are examples of skilled listening responses nurses can use to guide therapeutic interventions (Table 10-1).
Minimal cues and leads
Simple, encouraging leads communicate interest. Minimal cues transmitted through body actions (e.g., smiling, nodding, and leaning forward) encourage clients to continue with their story. By not detracting from the client’s message and by giving permission to tell the story as the client sees it, minimal cues promote client comfort in sharing intimate information. Short phrases such as “Go on” or “And then?” or “Can you say more about… ?” are useful prompts. Exercise 10-6 provides an opportunity to see the influence of minimal cues and leads on communication.
Clarification
Clarification seeks to understand the message of the client by asking for more information or for elaboration on a point. The strategy is most useful when parts of a client’s communication are ambiguous or not easily understood. Failure to ask for clarification when part of the communication is poorly understood means that the nurse will act on incomplete or inaccurate information.
Clarification listening responses are expressed as a question or statement followed by a restatement or paraphrasing of part of the communicated message; for example, “You stated earlier that you were concerned about your blood pressure. Tell me more about what concerns you.” The tone of voice used with a clarification response should be neutral, not accusatory or demanding. Practice this response in Exercise 10-7.
Restatement
Restatement is an active listening strategy used to broaden a client’s perspective or when the nurse needs to provide a sharper focus on a specific part of the communication. Restatement is particularly effective when the client overgeneralizes or seems stuck in a repetitive line of thinking. To challenge the validity of the client’s statement directly could be counterproductive, whereas repeating parts of the message in the form of a query serves a similar purpose without raising defenses; for example, “Let me see if I have this right…” (Coulehan et al., 2001). Restating a self-critical or irrational part of the message in a questioning manner focuses the client’s attention on the possibility of an inaccurate or global assertion.
Paraphrasing
Paraphrasing is a response strategy used to check whether the nurse’s translation of the client’s words is an accurate interpretation of the message. The strategy involves the nurse taking the client’s original message and transforming it into his or her own words, without losing the meaning. The paraphrase is shorter and more specific than the client’s initial statement so that the focus is on the core elements of the original statement.
Reflection
Reflection as a listening response focuses on the emotional implications of a message. This listening response helps the client clarify important feelings and experience them with their appropriate intensity in relation to a particular situation or event. There are several ways to use reflection, for example:
• Reflection on vocal tone: “I can sense anger and frustration in your voice as you describe your accident.”
• Linking feelings with content: “It sounds like you feel ___________ because _____________.”
• Linking current feelings with past experiences: “It seems as if this experience reminds you of feelings you had with other health care providers where you didn’t feel understood.”
Reflection as a listening response gives clients permission to have feelings and helps them to identify feelings they may not be aware of in new and unfamiliar circumstances. Sometimes nursing students feel they are putting words into the client’s mouth when they “choose” an emotion from their perception of the client’s message. This would be true if you were choosing an emotion out of thin air, but not when the nurse empathetically considers the client’s situation and presents the underlying feelings present in the client’s narrative, without interpreting its meaning. Exercise 10-8 provides practice in using paraphrasing and reflection as listening responses.
Summarization
Summarization is an active listening skill used to review content and process. Summarization pulls several ideas and feelings together, either from one interaction or a series of interactions, into a few succinct sentences. This would be followed by a comment seeking validation, such as “Tell me if my understanding of this agrees with yours.” A summary statement is useful as a bridge to changing the topic or focus of the conversation. The summarization should be completed before the end of the conversation. A summary statement should not be delivered as the nurse leaves the room. Exercise 10-9 is designed to provide insight into the use of summarization as a listening response.
Silence
Silence, used deliberately and judiciously, is a powerful listening response. Intentional pauses can allow the client to think. A short pause also lets the nurse step back momentarily and process what he or she has heard before responding. Too often a quick response addresses only a small part of the message or gives the client an insufficient opportunity to formulate an idea fully.
Silence can be used to emphasize important points that you want the client to reflect on. By pausing briefly after presenting a key idea and before proceeding to the next topic, you can encourage a client to notice vital elements. When a client falls silent, it can mean many things: something has touched the client, the client is angry or does not know how to respond, or the client is thinking. A verbal comment to validate meaning is helpful. Exercise 10-10 provides practice with the use of silences.
Not all listening responses are helpful. Nurses need to recognize when their responses are interfering with objectivity or inviting premature closure. Table 10-2 provides definitions of negative listening responses that block communication. Exercise 10-11 provides practice with using active listening responses.
TABLE 10-2
| Category of Response | Explanation of Category | Examples |
| False reassurance | Using pseudocomforting phrases in an attempt to offer reassurance | “It will be okay.” “Everything will work out.” |
| Giving advice | Making a decision for a client; offering personal opinions; telling a client what to do (using phrases such as “ought to,” “should”) | “If I were you, I would…” “I feel you should…” |
| False inferences | Making an unsubstantiated assumption about what a client means; interpreting the client’s behavior without asking for validation; jumping to conclusions | “What you really mean is you don’t like your physician.” “Subconsciously, you are blaming your husband for the accident.” |
| Moralizing | Expressing your own values about what is right and wrong, especially on a topic that concerns the client | “Abortion is wrong.” “It is wrong to refuse to have the operation.” |
| Value judgments | Conveying your approval or disapproval about the client’s behavior or about what the client has said using words such as “good,” “bad,” or “nice” | “I’m glad you decided to…” “That really wasn’t a nice way to behave.” “She’s a good patient.” |
| Social responses | Polite, superficial comments that do not focus on what the client is feeling or trying to say; use of clichés | “Isn’t that nice?” “Hospital rules, you know?” “Just do what the doctor says.” “It’s a beautiful day.” |
Verbal responses
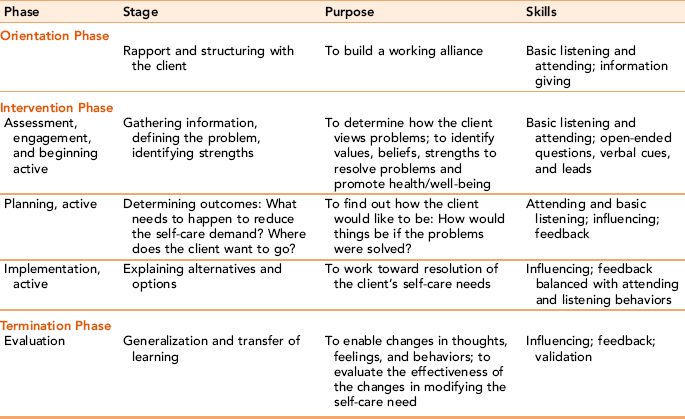
Active listening and verbal responses are inseparable from each other. Each informs and reinforces the other. Table 10-3 presents a summary of the therapeutic interviewing skills presented in this chapter as they apply to the phases of the nurse-client relationship. With shorter time frames for client contact, nurses need to verbally connect with clients, beginning with the first encounter.
As the relationship develops, the quality of verbal and listening responses ensure that care remains client centered. Most clients are not looking for brilliant answers from the nurse, but rather seek feedback and support that suggests a compassionate understanding of their particular dilemma. No matter what level of communication exists in the relationship, the same needs—“hear me,” “touch me,” “respond to me,” “feel my pain and experience my joys with me”—are fundamental themes. These are the themes addressed by client-centered communication.
Nurses use verbal responses to teach, encourage, support, provide and gather information, in guiding a client toward goal achievement. Words help clients assess the healthy elements of their personality (their strengths) and enables them to use these elements in coping with their current health problems. Accurate, appropriate language is critical for informed consent.
Verbal response strategies include mirroring, focusing, metaphors, humor, reframing, feedback, and validation, all of which are designed to strengthen the coping abilities of the client, alone or in relationship with others. Nurses use observation, validation, and patterns of knowing to gauge the effectiveness of verbal interventions. On the basis of the client’s reaction, the nurse may decide to use simpler language or to try a different strategy in collaboratively working with a client.
When making verbal responses or providing information, do not overload the client with too many ideas or details. If you find you are doing most of the talking, you need to back up and use listening responses to elicit the client’s perspective. People can absorb only so much information at one time, particularly if they are tired, fearful, or discouraged. Introducing new ideas one at a time allows the client to process data more efficiently. Repeating key ideas and reinforcing information with concrete examples facilitates understanding and provides an additional opportunity for the client to ask questions. Paying attention to nonverbal response cues from the client that support understanding or that reflect a need for further attention is an important dimension of successful communication.
Matching responses
Regardless of content, the nurse’s verbal responses should match the client’s message in level of depth, meaning, and language (Johnson, 1980). The client needs to lead the way to any exploration of deeper feeling. If the client makes a serious statement, the nurse should not respond with a flip remark. Likewise, a superficial statement does not warrant an intense response. Responses that encourage a client to explore feelings about limitations or strengths at a slightly deeper but related level of conversation are likely to meet with more success.
Verbal response should neither expand nor diminish the meaning of the client’s remarks. Notice the differences in the nature of the following responses to a client.
Using understandable language
Using simple, clear-cut words, keeping the client’s developmental and educational level in mind, and speaking with a general spirit of inquiry and concern for the client stimulates trust. Verbal messages should address core issues in a comprehensible, concise manner, taking into account the guidelines for effective verbal expressions, listed in Box 10-3.
Avoid using jargon or clinical language that clients may have trouble understanding. Unless clients can associate new ideas with familiar words and ideas that have meaning to him or her, the nurse might as well be talking in a different language. Clients may not tell the nurse that they do not understand for fear of offending the nurse or revealing personal deficits. Giving information that fails to take into account a client’s previous experiences, or assumes that clients have knowledge they do not possess, tends to fall on deaf ears. Frequent validation with the client related to content helps reduce this problem.
Focusing
In the past, nurses had more time to talk with clients. In today’s health care delivery system, nurses must make every second count. It is important for nurses and clients to select the most pressing health care topics for discussion. For example, the nurse can redirect the conversation to immediate nursing needs.
Sensitivity to client need and preferences, and client readiness are factors to take into consideration. You should not force a client to focus on an issue that he or she is not yet willing to discuss unless it is an emergency situation. You can always go back to a topic when the client is more receptive. For example, you might say, “I can understand that this is a difficult topic for you, but I am here for you if you would like to discuss [identified topic] later.”
Presenting reality
Presenting reality to a client who is misinterpreting it can be helpful as long as the client does not perceive that the nurse is criticizing the client’s perception of reality. A simple statement such as “I know that you feel very strongly about ___________, but I don’t see it that way” is an effective way for the nurse to express a different interpretation of the situation. Another strategy is to put into words the underlying feeling implied but not directly stated.
Giving feedback
Feedback is a message given by the nurse to the client in response to a message or observed behavior. Feedback can focus on the content, the relationship between people and events, the feelings generated by the message, or parts of the communication that are not clear. Feedback should be specific and directed to the behavior. It should not be an analysis of the client’s motivations.
Feedback responses reassure the client that the nurse is directing full attention to what the client is communicating through words or nonverbal behavior. Verbal feedback provides the receiver’s understanding of the sender’s message and personal reaction to it. Effective feedback offers a neutral mirror, which allows a client to view a problem or behavior from a different perspective. Feedback is most relevant when it only addresses the topics under discussion and does not go beyond the data presented by the client.
Effective feedback is specific rather than general. Telling a client he or she is shy or easily intimidated is less helpful than saying, “I noticed when the anesthesiologist was in here that you didn’t ask her any of the questions you had about your anesthesia tomorrow. Let’s look at what you might want to know and how you can get the information you need.” With this response, the nurse provides precise information about an observed behavior and offers a solution. The client is more likely to respond with validation or correction, and the nurse can provide specific guidance.
Feedback can be about the nurse’s observations of nonverbal behaviors; for example, “You seem (angry, upset, confused, pleased, sad, etc.).” It can be framed as a question, requiring the client to elaborate; for example, “I want to be sure that we have the same understanding of what we have talked about. Can you summarize for me what we have discussed?”
Not all feedback is equally relevant, nor is it always uniformly accepted. The benchmark for deciding whether feedback is appropriate is to ask, “Does the feedback advance the goals of the relationship?” and “Does it consider the individualized needs of the client?” If the answer to either question is “no,” then the feedback may be accurate but inappropriate for the moment.
Timing of feedback is important. Feedback given as soon as possible after a behavior is observed is most effective. Other factors (e.g., a client’s readiness to hear feedback, privacy, and the availability of support from others) contribute to effectiveness. Providing feedback about behaviors over which the client has little control only increases the client’s feelings of low self-esteem and leads to frustration. Feedback should be to the point and empathetic.
Effective feedback is clear, honest, and reflective. Feedback supported with realistic examples is believable, whereas feedback without documentation to support it can lack credibility. To illustrate from your nursing school experience, if you were told that you would have no trouble passing any of the exams in nursing school, you would wonder whether the statement was true. However, if your instructor said, “On the basis of past performance and the fact that your score on the entrance exams was high, I think you should have little problem with our tests as long as you study,” you would have more confidence in the statement.
Nonverbal feedback registers the other’s reaction to the sender’s message through facial expressions such as surprise, boredom, or hostility. When you receive nonverbal messages suggesting uncertainty, concern, or inattention, use a listening response to fully inquire about what the client is having trouble understanding. Feedback can have a surprise twist leading to an unexpected conclusion, as shown in the following example.
Asking for validation
Meanings are in people, not in the words themselves. Validation is a special form of feedback, used to ensure that both participants have the same basic understanding of messages. Simply asking clients whether they understand what was said is not an adequate method of validating message content. Instead, you might ask, “How do you feel about what I just said?” or “I’m curious what your thoughts are about what I just told you.” If the client does not have any response, you can suggest that the client can respond later, “Many people do find they have reactions or questions about [the issue] after they have had a chance to think about it. I would be glad to discuss this further.” Validation can provide new information that helps the nurse frame comments that match the client’s need.
Other forms of communication
Touch, the first of our senses to develop, and the last to leave, is a nurturing form of communication and validation. Intentional comforting touch benefits the nurse, as well as the client (Connor & Howett, 2009). Touch is a powerful listening response used when words would break a mood or when verbalization would fail to convey the empathy or depth of feeling between nurse and client (Straneva, 2000). A hand placed on a frightened mother’s shoulder or a squeeze of the hand can speak far more eloquently than words in times of deep emotion. Touch stimulates comfort, security, and a sense of feeling valued (Sundin & Jansson, 2003). Clients in pain, those who feel repulsive to others because of altered appearance, lonely and dying clients, and those experiencing sensory deprivation or feeling confused respond positively to the nurse who is unafraid to enter their world and touch them. Children and the elderly are comforted by touch.
How you touch a client in providing everyday nursing care is a form of communication. For example, gentle massage of a painful area helps clients relax. Holding the hand of a client with dementia can reduce agitation. Gently rubbing a client’s forehead or stroking the head is comforting to very ill clients.

People vary in their comfort with touch. Touch is used as a common form of communication in some cultures, whereas in others, it is reserved for religious purposes, or seldom used as a form of communication (Samovar, Porter, & McDaniel, 2009). Before touching a client, assess the client’s receptiveness to touch. Observation of the client will provide some indication, but you may need to ask for validation. If the client is paranoid, out of touch with reality, verbally inappropriate, or mistrustful, touch is contraindicated as a listening response.
Specialized communication strategies
Familiar images promote understanding. Metaphors can help clients and families process difficult new information by connecting it with familiar images from ordinary life experience. For example, Arroliga et al. (2002) describe chronic lung disease as “emphysema is like having lungs similar to ‘swiss cheese,’” and the airways in asthma are “different sized drainpipes that can get clogged up and need to be unclogged” (p. 377). These are familiar images that the client can appreciate and connect with a disease that is harder to comprehend.
In health care situations, metaphors need to be used carefully. Periyakoil (2008) suggests that using war or sports metaphors with clients experiencing advanced metastatic cancer can result in an unintended impact when the client can no longer fight the valiant battle or win the game by playing according to prescribed moves.
Humor
Humor is a powerful therapeutic communication technique when used with deliberate intent for a specific therapeutic purpose. Humor recognizes the incongruities in a situation, or an absurdity present in human nature or conduct (Random House Dictionary, 2009). Humor allows taboo topics to be raised without creating hostility or discomfort.
Humor and laughter have healing purposes. Laughter generates energy and activates β-endorphins, a neurotransmitter that creates natural highs and reduces stress hormones (Hassed, 2001). Humorous remarks are best delivered as simple statements that contain positive kernels of truth and are conveyed with calmness. The surprise element in humor can cut through an overly intense situation and put it into perspective.
Humor is most effective when rapport is well established and a level of trust exists between the nurse and client (McGhee, 1998). When humor is used, it should focus on the idea, event, or situation, or something other than the client’s personal characteristics. Humor that ridicules is not funny. Some clients respond well to humor; others are insulted or perplexed by it. Humor is less effective when the client is tired or emotionally vulnerable. Instead, that client may need structure and calming support.
Humor should fit the situation, not dominate it. The following factors contribute to its successful use:
Reframing
Bandler and Grindler (1997) define reframing as “changing the frame in which a person perceives events in order to change the meaning” (p. 1). Reframing offers a different positive interpretation designed to broaden the client’s perspective.
Reframing strategies should accentuate client strengths. The new frame must fit the current situation and be understandable to the client; otherwise, it will not work.
Reframing a situation is helpful when blame is a component of a family’s response to the client’s illness, for example, with alcoholism. Helping a family view the alcoholism as a disease rather than as a reaction to family members permits necessary detachment.
Cognitive behavioral strategies
Reality often is not the problem; rather it lies with negative thinking that creates emotional responses and influences behavior. Cognitive behavioral communication strategies are helpful in helping clients challenge self-defeating thoughts that threaten productive engagement in recovery. Once the nurse helps clients identify negative thoughts, clients are taught to challenge the validity of those thoughts and/or to replace them with a positive thought. By interrupting negative thinking patterns and replacing them with positive thoughts, people can modify behavior.
Applying the cognitive behavioral therapy model (Box 10-4), the activating event (A) is Jack’s prescription for depressive symptoms associated with cancer. His belief (B) that using psychotropic medication is a sign of weakness and that he should be able to get along as well without it gets in the way of his being able to resolve his depressive symptoms. This belief affects his efforts to cope with his cancer. The consequence (C) of going off the medication is a return of his depressive symptoms. In this case example, how would you help the client receive the help he needs for his emotional well-being?
Using technology in communication
Increasingly, nurses are using technology to communicate with clients and families. Although technology can never replace face-to-face time with clients, voice mail, e-mail, and telehealth virtual home visits help connect clients with care providers and provide critical information. Currently, technology is used as a form of communication to augment onsite communication. For example, routine laboratory results, appointment scheduling, and links to information on the Web can be transmitted through technology. Present-day technology allows people to use the Internet as a communication means to share common experiences with others who have a disease condition, to consult with experts about symptoms and treatment, and to learn up-to-date information about their condition.
The electronic nurse-client relationship begins when the nurse comes online or begins speaking to the client on the phone (Sharpe, 2001). From that point forward, the nurse needs to follow defined standards of nursing care, using communication principles identified in this chapter. At the end of each telehealth encounter, nurses need to provide their clients with clear directions and contact information should additional assistance be required. Confidentiality and protection of identifiable client information is an essential component of telehealth conversations.
Telephone communication is an essential communication link. Periodic informational telephone calls enhance family involvement in the long-term care of clients. Over time, some families lose interest or find it too painful to continue active commitment. Interest and support from the nurse reminds families that they are not simply nonessential, interchangeable parts in their loved one’s life; their input is important.
Summary
This chapter discusses basic therapeutic communication strategies nurses can use with clients across clinical settings. Nurses use active listening responses such as paraphrasing, reflection, clarification, silence, summarization, and touch to elicit complete information. Observation is a primary source of information, but all nonverbal behaviors need to be validated with clients for accuracy.
Open-ended questions give the nurse the most information because they allow clients to express ideas and feelings as they are experiencing them. Focused or closed-ended questions are appropriate in emergency clinical situations, when precise information is needed quickly.
Nurses use verbal communication strategies that fit the client’s communication patterns in terms of level, meaning, and language to help clients meet treatment goals. Other strategies include use of metaphors, reframing, humor, confirming responses, feedback, and validation. Feedback provides a client with needed information.
References
Arroliga, A.C., Newman, S., Longworth, D.L., et al. Metaphorical medicine: using metaphors to enhance communication with patients who have pulmonary disease. Ann Intern Med. 2002;137(5 Part 1):376–379.
Bandler, R., Cahill Grindler, J. Reframing. Palo Alto, CA: Science and Behavior Books, 1997.
Bush, K. Do you really listen to patients? RN. 2001;64(3):35–37.
Burgoon, J.K., Guerrero, L.K., Floyd, K. Nonverbal Communication. Boston, MA: Allyn and Bacon, 2009.
Caughan, G., Long, A. Communication is the essence of nursing care: 2. Ethical foundations. Br J Nurs. 2000;9(15):979–984.
Chesla, C. Reconciling technologic and family care in critical-care nursing. Image J Nurs Sch. 1996;28(3):199–203.
Connor, A., Howett, M. A conceptual model of intentional comfort touch. J Holist Nurs. 2009;27(2):127–135.
Coulehan, J.L., Platt, F.W., Egener, B., et al. Let me see if I have this right…: words that help build empathy. Ann Intern Med. 2001;135:221–227.
Definition of humor Random House Dictionary, New York, Random House, Inc, 2009. dictionary.com.. [Available online at:].
Epstein, R.M., Street, R.L., Jr. Patient-centered communication in cancer care: promoting healing and reducing suffering. Bethesda, MD: National Cancer Institute, 2007. [(NIH Publication No. 07-6225)].
Hall, E. The silent language. New York: Doubleday, 1959.
Hassed, C. How humour keeps you well. Aust Fam Physician. 2001;30(1):25–28.
Johnson, M. Self-disclosure: a variable in the nurse-client relationship. J Psychiatr Nurs. 1980;18(1):17–20.
Kagan, P. Feeling listened to: a lived experience of human becoming. Nurs Sci Q. 2008;21(1):59–67.
Keller, V., Baker, L. Communicate with care. RN. 2000;63(1):32–33.
Kettunen, T., Poskiparta, M., Liimatainen, L. Empowering counseling—a case study: nurse-patient encounter in a hospital. Health Educ Res. 2001;16:227–238.
Klagsbrun, J. Listening and focusing: holistic health care tools for nurses. Nurs Clin North Am. 2001;36(1):115–130.
Majanovic-Shane, A. Metaphor: a propositional comment and an invitation to intimacy. Paper presented at the Second Conference for Sociocultural Research, Geneva, Switzerland September 1996, 1996. Available online:, www.speakeasy.org/~anamshane/intima.pdf.
McGhee, P. Rx laughter. RN. 1998;61(7):50–53.
Moustakas, C. Finding yourself: finding others. Englewood Cliffs, NJ: Prentice Hall, 1974.
Myers, S. Empathetic listening: reports on the experience of being heard. J Humanist Psychol. 2000;40(2):148–174.
Nadzam, D. Nurses’ role in communication and patient safety. J Nurs Care Qual. 2009;24(3):184–188.
Peplau, H. Talking with patients. Am J Nurs. 1960;60(7):964–966.
Periyakoil, V. Using metaphors in medicine. J Palliat Med. 2008;11(6):842–844.
Platt, F.W., Gaspar, D.L. Tell me about yourself”; the patient-centered interview. Ann Intern Med. 2001;134(11):1079–1085.
Ruesch, J. Therapeutic communication. New York: Norton, 1961.
Samovar, L., Porter, R., McDaniel, E. Communication between Cultures. Boston MA: Wadsworth Cengage Learning, 2009.
Sharpe, C. Telenursing: nursing practice in cyberspace. Westport, CT: Auburn House, 2001.
Straka, D.A. Are you listening—have you heard? Adv Pract Nurs Q. 1997;3(2):80–81.
Straneva, J.A. Therapeutic touch: coming of age. Holist Nurs Pract. 2000;14(3):1–13.
Sundin, K., Jansson, L. Understanding and being understood” as a creative caring phenomenon: in care of patients with stroke and aphasia. J Clin Nurs. 2003;12:107–116.
Van Servellen, G. Talking the talk to improve your skills. Nursing. 2009;39(12):22–23.
Weiten, W., Lloyd, M., Dun, S., et al. Psychology applied to modern life: adjustment in the 21st centtury. Belmont CA: Wadsworth Cengage Learning, 2009.