Communicating with Families
At the end of the chapter, the reader will be able to:
1 Define family and identify its components.
2 Compare and contrast theoretical frameworks used to study family relationships.
3 Apply family-centered concepts to the care of the family in clinical settings, using standardized family assessment tools.
4 Apply the nursing process to the care of families in clinical settings.
5 Identify nursing interventions for families in the intensive care unit (ICU).
6 Identify nursing interventions for families in the community.
The purpose of this chapter is to describe family-centered relationships and communication strategies that nurses can use to support family integrity in health care settings. The chapter identifies family theory frameworks, which provide a common language for describing family relationships. Practical assessment and intervention strategies address family issues that affect a client’s recovery, and support self-management of chronic health conditions, or peaceful death in clinical practice.
Basic concepts
Wright and Leahey (2009) state, “A family is who they say they are” (p. 70). Identified family members may or may not be blood related. Strong emotional ties and durability of membership characterize family relationships regardless of how uniquely they are defined. Even when family members are alienated, or distanced geographically, they “can never truly relinquish family membership” (Goldenberg & Goldenberg, 2008, p. 3).
Some people identify their family as those with whom they have close relationships and who care for them (Kristjanson & Aoun, 2004). Each family member relates to the other and to crisis affecting the family in unique ways. Communication, even when reactive, is designed to maintain the integrity of the family. Understanding the family as a system is relevant in today’s health care environment, as the family is an essential part of the health care team.
The family represents the primary sociocultural system, in which children learn values and behavior patterns (Novilla, Barnes, De La Cruz, & Williams, 2006). Family health beliefs, past family experience with illness or injury, family loyalties and conflicts are important pieces of information that help explain client and family responses to health disruptions.
Families have a profound influence on sick clients as advisors, caretakers, supporters, and sometimes irritants. Clients who are very young, very old, and those requiring assistance with self-management of chronic illness are particularly dependent on their families.
Learning about the family’s dynamics provides:
• Awareness of family relationships that can be rallied for support, or that may need special attention because of a negative impact on the client’s situation
• Awareness of who else in the family has had a similar illness or medical problem and family coping strategies
• Awareness of cultural and family factors that influence a client’s attitudes, beliefs, and willingness to take action related to health care (Cole-Kelly & Seaburn, 1999).
Family composition
There is significant diversity in the composition of families, family beliefs and values, how they communicate with each other, ethnic heritage, life experiences, commitment to individual family members, and connections with the community (Schor, 2003). Box 13-1 identifies different types of family composition.
Families today are much more complex than in past generations. Modern definitions of family include “declared commitment” family households without marriage (Levine, 2004). Single-parent families must accomplish the same developmental tasks as two-parent families, but in many cases, they do it without the support of the other partner or sufficient financial resources.
Blended families have a different life experience than those in an intact family because their family structure is more complex. Children may be members of more than one family unit, linked biologically, physically, and emotionally to people who may or may not be part of their daily lives. Their “family” may include two or more sets of grandparents, step- or half-brothers and sisters, and multiple aunts and uncles (Byng-Hall, 2000). The child may spend extended periods in separate households, each with a full set of family expectations that may or may not be similar. Blended families can offer a rich experience for everyone concerned, but they are more complex because of multiple connections. Table 13-1 displays some of the differences between biological and blended families. Issues for blended families include discipline, money, use of time, birth of an infant, death of a stepparent, inclusion at graduation, and marriage and health care decisions.
TABLE 13-1
Comparing Differences Between Biological and Blended Families
| Biological Families | Blended Families |
| Family is created without loss. | Family is born of loss. |
| There are shared family traditions. | There are two sets of family traditions. |
| One set of family rules evolves. | Family rules are varied and complicated. |
| Children arrive one at a time. | Instant parenthood of children at different ages occurs. |
| Biological parents live together. | Biological parents live apart. |
Theoretical frameworks
Kurt von Bertalanffy’s (1968) general systems theory provides a conceptual foundation for family system models (Barker, 1998). A systems perspective examines the interdependence among all parts of the system and how they support the system as a functional whole. Systems’ thinking maintains that the whole is greater than the sum of its parts with each part reciprocally influencing its function. If one part of the system changes or fails, it affects the functioning of the whole. A clock is a useful metaphor. It displays time correctly, but only if all parts work together. If any part of the clock breaks down, the clock no longer tells accurate time.
A system interacts with other systems in the environment. An interactional process occurs when “inputs” are introduced into the system in the form of information, energy, and resources. Within each system, the information is processed internally as the system actively processes and interprets its meaning. The transformation process of raw data into desired outputs is referred to as throughput. The output refers to the result or product that leaves the system. Each system is separated from its environment by boundaries that control the exchange of information, energy, and resources into and out of the system. Evaluation of the output and feedback loops from the environment inform the system of changes needed to achieve effective outputs. Figure 13-1 identifies the relational components of a human system’s interaction with the environment, using von Bertalanffy’s model.
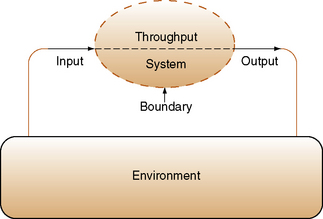
Applied to the human system, individuals take in food, liquids, and oxygen to nourish the body (inputs). Within the body, a transformational process occurs through enzymes and other metabolic processes (throughputs). so that the body can use them. This interactional process results in the human organism’s growth, health, and capacity to interact with the external environment (outputs). Nonusable outputs excreted from the body include urine, feces, sweat, and carbon dioxide. A person’s skin represents an important boundary between the environment and the human system.
Family systems have boundaries that regulate information coming into and leaving the family system. Family systems theory helps explain how families strive for harmony and balance (homeostasis), how the family is able to maintain its continuity despite challenges, (morphostasis), and how the family is able to change and grow over time in response to challenges (morphogenesis). Feedback loops describe the patterns of interaction that facilitate movement toward morphogenesis, or morphostasis. They impact goal setting in behavior systems. The systems principle of equifinality describes how the same outcome or end state can be reached through different pathways. This principle helps explain why some individuals at high risk for poor outcomes do not develop maladaptive behaviors (Cicchetti & Blender, 2006). Hierarchy is the term used to describe the complex layers of smaller systems that exist within a system. Subsystems refer to the smaller parts within the system, and suprasystems help describe the larger economic, social, and political systems in which the family system exists.
Bowen’s systems theory
Murray Bowen (1978) family systems theory conceptualizes the family as an interactive emotional unit. He believed that family members assume reciprocal family roles, develop automatic communication patterns, and react to each other in predictable connected ways, particularly when family anxiety is high. Once anxiety heightens within the system, an emotional process gets activated (Nichols & Schwartz, 2009) and dysfunctional communication patterns can emerge. For example, if one person is overly responsible, another family member is less likely to assume normal responsibility. Until one family member is willing to challenge the dysfunction of an emotional system by refusing to play his or her reactive part, the negative emotional energy fueling a family’s dysfunctional communication pattern persists.
Bowen developed eight interlocking concepts to explain his theoretical construct of the family system (Bowen Center, 2004; Gilbert, 2006). He viewed self-differentiation as the fundamental means of reducing chronic anxiety within the family system and enhancing effective problem solving. Self-differentiation emphasizes thinking rather than feeling in communication.
• Self-differentiation refers to a person’s capacity to define himself/herself within the family system as an individual having legitimate needs and wants. It requires making “I” statements based on rational thinking rather than emotional reactivity. Self-differentiation takes into consideration the views of others but is not dominated by them. Poorly differentiated people are so dependent on the approval of others that they discount their own needs.
• Multigenerational transmission refers to the emotional transmission of behavioral patterns, roles, and communication response styles from generation to generation. It explains why family patterns tend to repeat behaviors in marriages, child rearing, choice of occupation, and emotional responses across generations without understanding why it happens.
• Nuclear family emotional system refers to the way family members relate to one another within their immediate family when stressed. Family anxiety shows up in one of four patterns: (1) dysfunction in one spouse, (2) marital conflict, (3) dysfunctional symptoms in one or more of the children, or (4) emotional distancing.
• Triangles refer to a defensive way of reducing, neutralizing, or defusing heightened anxiety between two family members by drawing a third person or object into the relationship (Glasscock & Hales, 1998). If the original triangle fails to contain or stabilize the anxiety, it can expand into a series of “interlocking” triangles, for example, into school issues or an affair.
• Family projection process refers to an unconscious casting of unresolved anxiety in the family on a particular family member, usually a child. The projection can be positive or negative, and it can become a self-fulfilling prophecy as the child incorporates the anxiety of the parent as part of his or her self-identity.
• Sibling position, a concept originally developed by Walter Toman (1992), refers to a belief that sibling positions shape relationships and influence a person’s expression of behavioral characteristics. Each sibling position has its own strengths and weaknesses. This concept helps explain why siblings in the same family can exhibit very different characteristics. For example:
• Oldest or only children are more serious, assume leadership roles, and like to be in control. They may experience more trouble with staying connected with others, or depending on them.
• Youngest siblings are characterized as being followers, spontaneous and fun loving, with a stronger sense of humor. They are more likely to be interested in quality of life and relationships.
• Middle child positions embrace characteristics of oldest and youngest; they are likely to be adventuresome and independent, but not leaders. The child in the middle position may feel neglected or take on the role of peacemaker.
• An age differential of 6 years or more, illness, life circumstances, gender, and personality can modify typical sibling position characteristics. Children in well-differentiated families are less likely to be affected by sibling position characteristics than those in fused family systems. Complementary matches, for example, oldest/youngest work best in marriage and work situations. When two people occupy the same sibling position, issues can arise. For example, competitiveness in two oldest or only child marital partners, or difficulty making decisions with two youngest pairings is not uncommon.
• Although sibling position is a factor in explaining different relational behaviors, it is not useful as a descriptor of life functioning as a person occupying any sibling position can be successful or unsuccessful (Gilbert, 2006).
• Emotional cutoff refers to a person’s withdrawal from other family members as a means of avoiding family issues that create anxiety. Emotional cutoffs range from total avoidance to remaining in physical contact, but in a superficial manner. Emotional cutoffs contain a negative anxiety that drains personal energy. The problems creating the emotional cutoff persist.
• Societal emotional process refers to parallels that Bowen found between the family system and the emotional system operating at the institutional level in society. As anxiety grows within a society, many of the same polarizations, lack of self-differentiation, and emotion-based thinking dominate behavior and system outcomes.
Family legacies have a powerful influence on family relationships and in shaping parenting practices. Knowledge of family relationships helps explain behaviors that would not be clear without having a family context. Helping families gain clarity about how their family heritage can be used as an asset in health care and/or what areas need work strengthens the potential for effective family-centered care.
Minuchin’s structural model
Family structure models, pioneered by Salvador Minuchin (1974), emphasize the structure (subsystems, hierarchies, and boundaries) of the family unit as the basis for understanding family function. Family structure refers to how the family is constructed legally and emotionally. The concept of hierarchy describes how families organize themselves into various smaller units, referred to as the subsystems that comprise the larger family system.
Subsystems are organized by position, gender, generation, interest, or function to accomplish the goals of the family through related tasks. Common subsystems include spousal, parental, and sibling units. Family members typically belong to several subsystems simultaneously (Goldenberg & Goldenberg, 2008). Their behaviors in each subsystem reflect the nature of the relationship, for example, an adult feeling like a child when visiting parents. Being in multiple subsystems can generate conflict when the expectations of one subsystem interfere with those of another, for example, being a parent while having caregiving responsibility as a daughter for a frail elder and finding time for the spousal subsystem.
Boundaries, defined as invisible limits surrounding the family unit, protect the integrity of the family system. Boundaries draw a line in the sand by identifying what belongs within the family system and what is external to it. They define the level of participation between family members (Nichols & Schwartz, 2009). Clear generational boundaries provide security for family members, for example, setting legitimate limits with children and balancing individual needs with caring for the needs of chronically ill family members.
Boundaries regulate the flow of information into and out of the family. Permeable boundaries welcome interactions with others and allow information to flow freely. Families with clear, permeable boundaries are better able to balance the demands of the illness with other family needs and can communicate more effectively with care providers (Dalton & Kitzmann, 2008). Diffuse boundaries lead to family overinvolvement, whereas rigid boundaries are operative in families with little interaction between members and family secrets. Rigid boundaries restrict flow of information. Interaction with outsiders is discouraged or heavily regulated. Diffuse boundaries are found in enmeshed families.
Exercise 13-1 provides an opportunity to look at the communication process of family from a structural functional perspective. Structural and functional aspects of families determine the nature of interactions between family members. Family interactions offer protective and health-promoting support for members in crisis when they function well, and are an area of concern when they function ineffectively.
The family performs its functions through subsystem alliances and coalitions to maintain the system as a whole (homeostasis). Wright and Leahey (2009) describe two ways of examining family functioning: instrumental and expressive. Both are important descriptors of family functioning.
• Instrumental functioning refers to task activities of daily living (e.g., eating, sleeping, or caring for a sick member).
• Expressive functioning looks at the communication, problem-solving skills, roles, beliefs, spheres of influence, and power that govern how individual members interact with one another.
Assessment of a family’s structure and function for strengths and weaknesses, and comparing current functionality with previous functioning helps focus nursing interventions and supports.
Duvall’s developmental framework
Evelyn Duvall (1958) proposed a family life stage framework for understanding issues that normal families experience based on expected family development through the life span, each with its own set of tasks. Her model describes the life cycle of a family, using the age of the oldest child in the family as the benchmark for determining the family’s developmental stage. Developmental tasks represent the challenges and growth responsibilities each family experiences at different life stages (Table 13-2).
TABLE 13-2
Duvall’s Family Life Cycle and Related Developmental Tasks
| State Family Life Cycle Stage | Family Development Tasks |
| I. Beginning families (married couples without children) | Establishing a mutually satisfying marriage; adjusting to pregnancy and the promise of parenthood; fitting into the kin network |
| II. Child-bearing families (oldest child birth through 30 months) | Having, adjusting to, and encouraging the development of infants; establishing a satisfying home for both parents and infants |
| III. Families with preschool-age children (oldest child 2.5–6 years of age) | Adapting to the critical needs and interests of preschool-age children in stimulating, growth-promoting ways; coping with energy depletion and lack of privacy as parents |
| IV. Families with school-age children (oldest child 6–13 years of age) | Fitting into the community of school-age families in constructive ways; encouraging children’s educational achievement |
| V. Families with teenagers (oldest child 13–20 years of age) | Balancing freedom with responsibility as teenagers mature and emancipate themselves; establishing postparental interests and careers as growing parents |
| VI. Families launching young adults (first child leaving home through last child leaving home) | Releasing young adults into work, college, marriage with appropriate rituals and assistance; maintaining supportive home base |
| VII. Middle-age parents (empty nest to retirement) | Rebuilding the marriage relationship; maintaining kin ties with older and younger generations |
| VIII. Family during retirement and aging (retirement) | Adjusting to retirement; closing the family home or adapting it to aging; coping with bereavement and living alone |
From Duvall EM, Miller BC: Marriage and family development, ed 6, Boston, 1985, Allyn and Bacon. Copyright © 1985 by Pearson Education. Adapted by permission of the publisher. by Pearson Education. Adapted by permission of the publisher.
Duvall’s stages of family development are helpful in guiding nurses about possible concerns families may have at different stages of family development. It helps nurses appreciate a family’s current developmental needs that may coincide with their family member’s illness or injury. Nurses can provide information about natural family development as a basis for discussion of the limitations imposed by the health deviation.
Duvall (1958) identified nine family characteristics indicative of successful family development:
2. Satisfactory ways of earning and spending money
3. Mutually acceptable patterns in the division of labor
4. Continuity of mutually satisfying sexual relationships
5. An open system of communication
6. Workable relationships with relatives
7. Ways of interacting with the larger social community
Developmental family theory helps nurses appreciate the family’s current developmental needs that may coincide with their family member’s illness or injury. This knowledge helps nurses craft a developmentally appropriate level of involvement for each family system (Leon, 2008). Families benefit from information about normal developmental patterns and typical limitations imposed by a health deviation. For example, hair loss for the adolescent having chemotherapy can be devastating because of the heightened attention to appearance during this developmental stage. Anticipatory guidance about natural developmental milestones and associated behaviors is helpful.
Mccubbin’s resiliency model of family coping
McCubbin’s Resiliency Model of Family Stress, Adjustment, and Adaptation is considered the most extensively studied model of family coping with traumatic and chronic illness (McCubbin, McCubbin, Thompson, et al, 1993; Clark, 1999). In this model, A (an event) interacts with B (resources) and with C (family’s perception of the event) to produce X (the crisis). An expansion of this model adds the concepts of “pileup of demands, family system resources, and postcrisis behavior” (McCubbin, McCubbin, & Thompson et al., 1998, p. 49). With any serious illness, most people experience a roller coaster emotional response that parallels the course of the illness—optimism and hope when things are going well, disappointment and anger when they are not.
Protective factors related to stress adaptation include good problem-solving skills and flexibility to try different constructive actions. Successful coping built on family capabilities, strengths, and resources leads to positive adaptation. Unsuccessful coping strategies result in maladaptive behaviors (Greeff & Human, 2004). Exercise 13-2 provides an opportunity to look at the differences between positive and negative family interactions.
Pile-up demands (McCubbin et al., 1998) from the environment such as job loss, unexpected expenses, overcrowded housing conditions, and limited caregiving skills can place children and vulnerable adults at risk for significant stress. Family violence, substance abuse, neglect, and dysfunction are on the rise as families become more and more stressed while trying to cope with the demands of chronically ill clients. Nurses must be able to recognize families who are providing unsafe environments for individual family members or who have reached dangerous stress levels themselves.
Recognizing Families at Risk
Medalie and Cole-Kelly (2002) describe the course of chronic illness as being a series of health crises with relatively stable times in between. Knowledge of risk factors for family coping is an important dimension of providing family-centered care for the person with chronic illness and the family caring for the family member. Equally essential is knowledge and an assessment of family assets. Assets can include support from other family members, shared family activities, connections with supportive people in the community, and parental involvement in child care and school activities.
An atmosphere of openness to family concerns helps families feel comfortable in sharing painful feelings of anger or guilt. Psychosocial screening for risk factors should include asking relevant questions about family relationships, domestic violence, maternal depression, substance abuse, and suicidal ideation. There are brief written screening tools for depression and stress that nurses can also use. Individuals found to be at risk through screening can be referred to appropriate resources.
Just talking about the impact of a significant illness on family roles and function is helpful for families. Relevant questions should focus on how each family member is coping with the situation, what types of changes are needed in family functioning to cope with the illness over time, and the degree to which the family is able to meet the requirements of the crisis situation. Exercise 13-3 examines coping strategies that families use in crisis situations.
The McCubbin model is helpful in assessing and responding to a family’s psychosocial needs around the serious illness of a family member, particularly a child. Families of seriously ill children face many competing demands—care for the ill child, attention to other children, balancing work responsibilities, and having any kind of a normal life for themselves. Using this model, the nurse might inquire about how the family is able to work together in dealing with the challenges of the current illness.
Providing timely information and promoting connections with community supports and parent-to-parent networks is helpful. When significant problems exist, referring families to professionals able to deal with these complex problems and notifying protective service authorities become essential roles. Nurses are considered reporting agents in most states and, therefore, are required by law to report suspicion of child physical or sexual abuse to child protection agencies.
Family Resilience
Resilience refers to the ability to cope positively with adversity. It is recognized as a protective factor in times of family stress. Family resilience is associated with a healthy family atmosphere of positive support, warmth, and affection. Walsh (1996) identifies four characteristics found in resilient families:
• Capacity to derive meaning from adversity
• The capacity to affirm strengths and consider alternative possibilities
• Transcendent and spiritual beliefs that allow families to connect with a larger purpose and commitment to help others
Serious illness or injury creates many challenges to family integrity, all occurring within a short period. In addition to fear and anxiety about the illness itself, the internal image of what the family is and the meaning it holds for each person within it is challenged. In some cases, the experience strengthens the family unit. In others, it leads to disruption of family functioning. Normal life routines are suspended. Families automatically become involved in the client’s care as participant, critic, support, or advocate with health care providers.
Nurses can support family resilience by providing emotional support for individual family members and vital updated information about the client’s condition. Psychosocial support makes a difference. Families need attention, repeated information, and assurances (Van Horn & Kautz, 2007). Other strategies include encouraging collaboration among family members, reinforcing a sense of teamwork. Referrals to support groups for peer support of shared experiences and verbalizing observations of personal and family strengths are helpful.
Applications
Family-centered care allows health care providers to have a more uniform understanding of the client and family’s knowledge, preferences, and values in health care as the basis for shared decision making. This information allows them to provide consistent information to all those involved in the client’s care, and to identify any barriers that might arise with the care plan.
The health events of one family member affect the whole family. Trotter and Martin (2007) note, “Families share genetic susceptibilities, environments, and behaviors, all of which interact to cause different levels of health and disease” (p. 561). Families bear a bulk of the care and/or support of client self-management of chronic health conditions. They are instrumental in helping clients appreciate the need for diagnosis and treatment, and in encouraging the patient to seek treatment. Family members are involved in a client’s health care decisions ranging from treatment options to critical decisions about end of life care. Families play a pivotal advocacy role in treatment by monitoring and insisting on quality care actions for an individual family member.
The challenges for the nurse in family-centered care are:
• To understand the impact of the medical crisis on family functioning and dynamics
• To appreciate and respond empathetically to the emotional intensity of the experience for the family
• To determine the appropriate level of family involvement in holistic care of the client, based on an understanding of fundamental family system concepts (Leon & Knapp, 2008)
Assessment
For immediate health care purposes, family is defined as the significant people in the client’s environment who are capable and willing to provide family-type support. This definition of family includes members who may not be related by blood, marriage, or adoption (Medalie & Cole-Kelly, 2002). Regardless of how it occurs, any health disruption becomes a family event. Even when the family is not directly involved in the client’s care, they will have feelings about it—individually or collectively—that support or sabotage the effectiveness of treatment and the client’s quality of life (Bell, 2000). Box 13-2 lists sample indicators that could warrant family assessment and nursing intervention.
Assessment tools
Wright and Leahey’s (2009) 15-minute interview, consisting of the genogram, ecomap, therapeutic questions, and commendations provide a comprehensive look at family relationships. Assessment tools such as the genogram, ecomap, and family time lines are used to track family patterns. The structured format of these tools focuses on getting relational data quickly and can sensitize clinicians to systemic family issues that affect patterns of health and illness (Gerson, McGoldrick, & Petry, 2008).
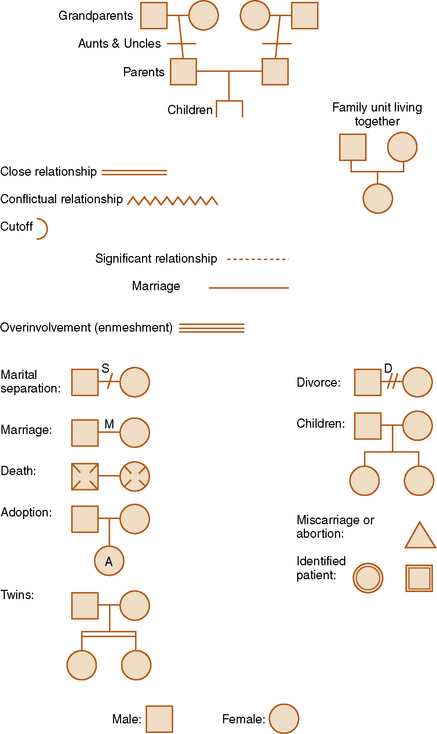
Genograms
Most family members enjoy constructing a genogram and learn about themselves in the process (Cole-Kelly & Seaburn, 1999). A genogram uses a standardized set of connections to graphically record basic information about family members and their relationships over three generations. Genograms are updated and/or revised as new information emerges.
There are three parts to genogram construction: mapping the family structure, recording family information, and describing the nature of family relationships. Figure 13-2 identifies the symbols used to map family structure, with different symbols representing pregnancies, miscarriages, marriages, deaths, and other nodal family events. Male family members are drawn on the left of the horizontal line as a square and female members on the right as a circle. The oldest sibling is placed on the left, with younger siblings following from left to right, in order of birth. In the case of multiple marriages, the earliest is placed on the left and the most recent on the right. Lines drawn between significant family members identify the strength of relational patterns that are overly close, close, distant, cut off, or conflicted. An example of a family genogram is presented in Figure 13-3. Exercise 13-4 provides practice with developing a family genogram.
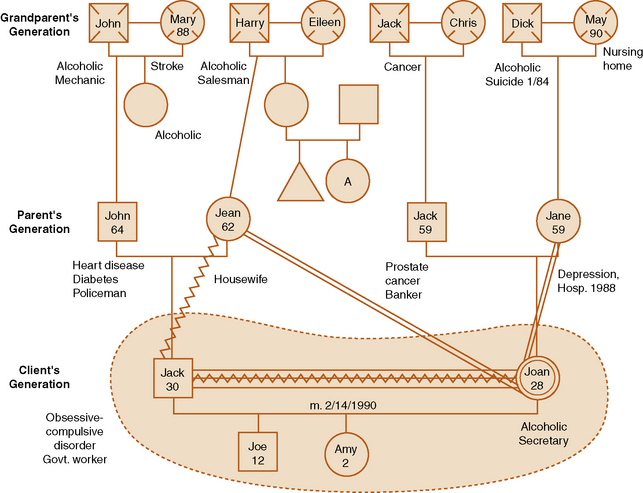
The genogram explores the basic dynamics of a multigenerational family. Its multigenerational format, which traces family structure and relationships through three generations is based on the assumption that family relationship patterns are systemic, repetitive, and adaptive. Data about ages, birth and death dates, miscarriages, relevant illnesses, immigration, geographical location of current members, occupations and employment status, educational levels, patterns of family members entering or leaving the family unit, religious affiliation or change, and military service are written near the symbols for each person. The recorded information about family members allows families and health professionals to simultaneously analyze complex family interaction patterns in a supportive environment. The impact of multiple generations on family relationships is more readily visible.
The genogram offers much more than a simple diagram of family relationship. Formal and informal learning about appropriate social behaviors and roles takes place within the family of origin. People learn role behaviors and responsibilities expected in different life stages experientially, by way of role modeling, and through direct instruction.
As you help a client construct a family genogram, you can ask questions regarding family thoughts about the role of gender, spiritual beliefs, or cultural values in shaping personal identity, managing conflict, and handling life issues (McCormick & Hardy, 2008). For example, girls are exposed to different role behaviors and social expectations than their male siblings. Although they are less rigid than in previous generations, the differences persist. Both men and women carry these understandings into “contemporary” family relationships when they marry. Fundamental differences in family rules and role expectations especially about parenting, handling of finances, and the nature of male and female complementary roles can lead to conflict and misunderstandings if not identified, shared, and dealt with. Exercise 13-5 provides an opportunity to trace gender role development and socialization within a family and how it affects adult communication and behaviors.
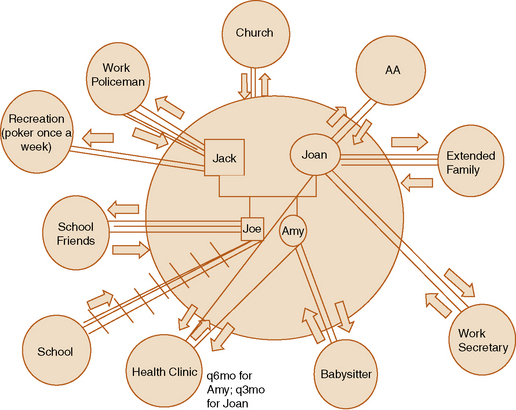
Ecomaps
An ecomap is essentially a sociogram, illustrating the shared relationships between family members and the external environment (Rempel, Neufeld, & Kushner, 2007). Beginning with an individual family unit or client, the diagram extends to include significant social and community-based systems with whom they have a relationship. These data identify at a glance the family’s interaction with environmental supports, and their use of resources available through friends and community systems. Adding the ecomap is an important dimension of family assessment, providing awareness of community supports that could be or are not being used to assist families. Ecomaps can point out resource deficiencies and conflicts in support services that can be corrected.
An ecomap starts with an inner circle representing the family unit, labeled with relevant family names. Smaller circles outside the family circle represent significant people, agencies, and social institutions with whom the family interacts on a regular basis. Examples include school, work, church, neighborhood friends, recreation activities, health care facilities or home care, and extended family.
Lines are drawn from the inner family circle to outer circles indicating the strength of the contact and relationship. Straight lines indicate relation, with additional lines used to indicate the strength of the relationship. Dotted lines suggest tenuous relationships. Stressful relationships are represented with slashes placed through the relationship line. Directional arrows indicate the flow of the relational energy. Figure 13-4 shows an example of an ecomap. Exercise 13-6 provides an opportunity to construct an ecomap.
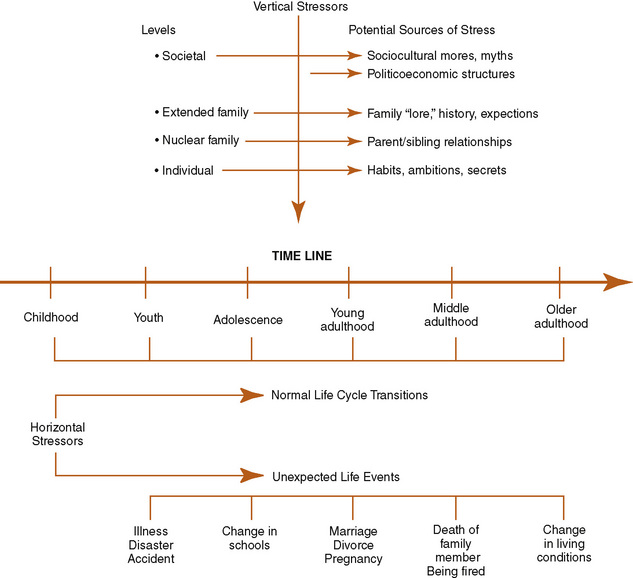
Family Time Lines
A family systems framework acknowledges that each family is unique with its own set of expertise, knowledge, and skills. Vertical and horizontal stressors affect the family systems level of functioning in both positive and negative ways. Medical crises tend to exacerbate unresolved issues, which can create additional challenges for nurses (Leon & Knapp, 2008).
Time lines offer a visual diagram that captures significant family stressors, life events, health, and developmental patterns through the life cycle. Family history and patterns developed through multigenerational transmission are represented as vertical lines. Horizontal lines indicate timing of life events occurring over the current life span. These include such milestones as marriages, graduations, and unexpected life events such as disasters, war, illness, death of person or pet, moves, births, and so forth (Figure 13-5). Time lines are useful in looking at how the family history, developmental stage, and concurrent life events might interact with the current health concern.
Applying the nursing process
The nurse-family relationship in client care depends on a reciprocal relationship between the nurses and family in which both are equal partners and sources of information. Nurses should begin offering information to the family as soon as the client is admitted to the hospital or service agency. Orientation to the unit, location of the cafeteria and restrooms, parking options, nearby lodging, and access to the hospitalist or physician are important data points.
The initial encounter sets the tone for the relationship. How nurses interact with each family member may be as important as what they choose to say. Begin with formal introductions and explain the purpose of gathering assessment data. Even this early in the relationship, you should listen carefully for family expectations and general anxiety that may be revealed more through behavior than through words.
Gathering assessment data
Inquiring about the relationship the family member has with the identified client is an initial step nurses can take in establishing a relationship with the family. For example, you can initially say, “I would like to understand more about the effect of your husband’s heart attack on the family.” This simple statement frames the information needed. It also serves as a reminder that each family member plays a role in the health care scenario and has associated support needs that the nurse needs to consider (Vandall-Walker, Jensen, & Oberle, 2007). Box 13-3 illustrates a framework for a family assessment with a client entering cardiac rehabilitation.
Family participation in the data assessment process enhances the therapeutic relationship and completeness of the data. It is important to inquire about the family’s cultural identity, rituals, values, level of family involvement, decision making, and traditional behaviors as it relates to the health care of the client (Leon & Knapp, 2008).
Knowledge of a family’s past medical experiences, particularly whether they were positive or negative, the family’s medical beliefs, major family events a family is struggling with concurrently, plus family expectations for treatment and care are essential pieces of family assessment data. Suggested questions include:
• How does the family view the current health crisis?
• What is each family member’s most immediate concern?
• Has anyone else in the family experienced a similar problem?
• What do family members believe would be most helpful to the client at this time?
• How does the family explain the reasons for the illness or injury?
• Are there any other recent changes or sources of stress in the family that make the current situation worse (pile up of demands?)
• How has the family handled the problem to date?
• What would the family like to achieve with the nurse’s help in resolving issues related to the client’s health and well-being (McBride, 2004)?
• As you close the session, ask, “Is there anything else I should know about your family and this experience?”
Planning
Wright and Leahey (2009) identify therapeutic questioning as a nursing intervention that nurses can use with their client families to identify family strengths; help family members sort out their personal fears, concerns, and challenges in health care situations; and provide a vehicle for exploring alternative options. Interventive questioning can be either linear or circular.
Circular questions focus on family interrelationships and the impact a serious health alteration has on individual family members and the equilibrium of the family system. Examples of therapeutic questions are found in Box 13-4. The nurse uses information the family provides as the basis for additional questions.
The following case example demonstrates its use when the nurse asks a family, “What has been your biggest challenge in caring for your mother at home?”
In this example, each family member’s concern is related but different. The therapeutic circular question opens a discussion about each person’s anxiety. As family members hear the concerns of other family members, and as they hear themselves respond, their perspective broadens. The resulting conversation forms the basis for developing strategies that are mutually acceptable to all family members.
Selekman (1997) identifies four elements to consider when designing therapeutic interventions within a family context:
• The family’s definition of the problem
• Key family characteristics (e.g., language, beliefs, and strengths)
Meaningful involvement in the client’s care not only differs from family to family, it differs among individual family members (Sydnor-Greenberg, Dokken, & Ahmann, 2000). Individual family members have different perspectives. Hearing each family member’s perspective helps the family and nurse develop a unified understanding of significant treatment goals and implications for family involvement.
Although treatment plans should be tailored around personal client goals, acknowledging family needs, values, and priorities enhances compliance, especially if they are different. Shared decision making and development of realistic achievable goals makes it easier for everyone concerned to accomplish them with a sense of ownership and self-efficacy about the process. Taking little achievable steps is preferred to attempting giant steps that misjudge what the family can realistically do.
Exercise 13-7 provides practice with developing a family nursing care plan.
Implementation
Nurses can only offer interventions; it is up to the family to accept them (Wright & Leahey, 2009). Suggested nursing actions to promote positive change in family functioning include
• Encouraging the telling of illness narratives
• Commending family and individual strengths
• Offering information and opinions
• Validating or normalizing emotional responses
Encouraging Family Narratives
Families need to tell their story about the experience of their loved one’s illness or injury; it may be quite different from how the client is experiencing it. The differences can lead to a more complete understanding.
Nurses play an important role in helping families understand, negotiate, and reconcile differences in perceptions without losing face.
Incorporating Family Strengths
Otto (1963) introduced the concept of family strengths as potential and actual resources families can use to make their life more satisfying and fulfilling to its members. When health care changes are required, and they usually are with clients suffering from serious illness or injury, working through family strengths rather than focusing on deficits is useful. Viewing the family as having strengths to cope with a problem rather than being a problem is a healing strategy, giving the family hope that a problem is not the end point but rather only a circumstance in need of a solution.
Feeley and Gottlieb (2000) identify four different types of strengths nurses can help the family use to achieve important health outcomes:
• Traits that reside within an individual or a family (e.g., optimism, resilience)
• Assets that reside within or are associated with an individual or a family (e.g., finances, social, spiritual, or work relationships)
• Capabilities, skills, or competencies that an individual or a family has developed (e.g., problem-solving skills)
• A quality that is more transient in nature than a trait or asset (e.g., motivation)
Questions nurses can use specifically to elicit family strengths include:
• What has the family been doing so far that has been helpful?
• What is going well for this family?
• How have they (family) been able to do as well as they have done?
• What beliefs or previous experiences or relationships are sustaining them and preventing the problem from being worse?
• What advice would they give to other people in the same situation? (Tapp & Moules, 1997)
Giving Commendations
Limacher and Wright (2003) define commendations as “the practice of noticing, drawing forth, and highlighting previously unobserved, forgotten, or unspoken family strengths, competencies or resources” (p. 132). Commendations are particularly effective when the family seems dispirited or confused about a tragic illness or accident. More than a simple compliment, commendations should reflect patterns of behavior existing in the family unit over time. Wright and Leahey (2009) differentiate between a commendation (“Your family is showing much courage in living with your wife’s cancer for 5 years.”) and a compliment (“Your son is so gentle despite feeling so ill.”) (p. 270). They suggest giving at least one commendation per interview.
Ryan and Steinmiller (2004) recommend naming family strengths in front of the family. For example, nurses can verbally reflect on the strength of the family in coping with multiple problems, the capacity to stay involved when client anger threatens the relationship, or the ability of the family to thoroughly research a health problem. Exercise 13-8 provides practice with giving commendations.
Informational Support
Helping a family become aware of information from the environment and how to access it empowers families. By showing interest in the coping strategies that have and have not worked, the nurse can help the family see progress in their ability to cope with a difficult situation.
You can offer family members informational support related to talking with extended family, children, and others about the client’s illness. You can help family members prepare questions for meeting with physicians. Finally, you can engage with families in discussions about the cultural, ethical, and physical implications of using or discontinuing life support systems. This is nursing’s special niche, as these conversations are rarely one-time events, and nurses can provide informal opportunities for discussing them during care provision.
Meeting the Needs of Families with Critically Ill Clients
Having a family member in an ICU represents a serious crisis for most families. Eggenberger and Nelms (2007) suggest, “Patients enter a critical care unit in physiological crisis, while their families enter the hospital in psychological crisis” (p. 1619). Box 13-5 identifies care needs of families of critically ill clients. Family-centered relationships are key dimensions of quality care in the ICU.
Proximity to the client
The need to remain near the client is a priority for many family members of clients in the ICU (Perrin, 2009; Verhaeghe et al., 2005). Although the family may appear to hover too closely, it is usually an attempt to rally around the client in critical trouble (Leon, 2008). Viewed in this way, nurses can be more empathetic. As the family develops more confidence in the genuine interest and competence of staff, the hovering tends to lessen. Liberal visitation policies can result in “increased family involvement with patient care, increased family communication with nurses, and greatly decreased number of complaints from families” (Van Horn & Kautz, 2007, p. 102).
Families can be a primary support to clients, but they usually need encouragement and concrete suggestions for maximum effect and satisfaction. Family members feel helpless to reverse the course of the client’s condition and appreciate opportunities to help their loved one. Suggesting actions that family members can take at the bedside include doing range-of-motion exercises, holding the client’s hand, positioning pillows, providing mouth care or ice chips. Talking with the client, even if the person is unresponsive, can be meaningful.
Helping families balance the need to be present with the client’s needs to conserve energy and have some alone time to rest or regroup is important. Family members also need time apart from their loved one for the same reasons. Tactfully explaining the need of critically ill clients to have family presence without feeling pressure to interact can be supportive. Encouraging families to take respites is equally important.
At the same time, nurses need to be sensitive to and respect a family member’s apprehension or emotional state about their critically ill family member. Individual family members may need the nurse’s support in talking about difficult feelings.
Nurses can role model communication with clients, using simple caring words and touch. Families are quick to discern the difference between nurses who are able to connect with a critically ill client in this way, as evidenced in a family member’s comment that “some seem to have a way with him and they talk to him like he is awake” (Eggenberger & Nelms, 2007, p. 1623).
Caring for Families in the Pediatric Intensive Care Unit
Parents of children in the pediatric intensive care unit (PICU) want to be with their children as often as possible, but particularly when the child is having a procedure or is uncomfortable (Aldridge, 2005). Parents of children in the PICU need frequent reassurance from the nurse about why things are being done for their child and about treatment-related tubes and equipment. They want to actively participate in their child’s care and have their questions honestly answered (Aldrich).
Families often act as the child’s advocate during hospitalization, either informally by insisting on high-quality care or formally as the legal surrogate decision maker designated to make health care decisions on behalf of the client. The nurse is a primary health care provider agent in working with families facing these issues. A critical intervention for the family as a whole and its individual members is to help them recognize their limitations and hidden strengths, and to maintain a balance of health for all members.
Providing information
Families with clients in the ICU have a fundamental need for information, particularly if the patient is unresponsive—“Not knowing is the worst part.” This cannot be stressed enough. Providing updated information as a clinical situation changes is critical. Even if there is no change in the client’s condition, most families will need to have information repeated because of anxiety that may limit processing of complex or emotionally difficult information (Van Horn & Kautz, 2007). They need to know exactly what is being done for their loved one in simple understandable terms, and to have their questions answered honestly (Miracle, 2006). This information is particularly critical when family members must act as decision makers for clients who cannot make them on their own (Perrin, 2009).
How health care providers deliver information is important. Even if the patient’s condition or prognosis leaves little room for optimism, the family needs to feel some hope and that the staff genuinely cares about what is happening with the client and family (Perrin, 2009; Verhaeghe, Defloor, Van Zuuren, et al., 2005).
Daily contact with the nurse assigned to the client in the ICU is a critical nursing action (Miracle, 2006) that the family needs. Identifying one family member to act as the primary contact helps ensure continuity between staff and family. A short daily phone call when family members cannot be present keeps the family connection and reduces family stress (Leon, 2008). Families need ongoing information on the client’s progress, modifications in care requirements, and any changes in expected outcomes, with opportunities to ask questions and clarify information. Nurses in the ICU often serve as mediators between client, family, and other health providers to ensure that data streams remain open, coordinated, and relevant.
Family-centered relationships in the community
The Centers for Disease Control and Prevention (CDC) estimates that approximately 70% of deaths in the United States are the result of chronic disease. Although many of these individuals are able to self-manage their disease, an increasing number will require family support with coping, self-management, and palliative care. Increasingly, nurses are called on to help families effectively manage the care of people with chronic illness who can no longer take care of themselves or who require additional support to maintain their independence (McKenry & Price, 2005).
The concept of the family caregiver as a key member of the health care team has become increasingly important as more people live with chronic illness on a daily basis in the community or subacute care facility. Medalie and Cole-Kelly (2002) define the functional family as the group coping with the everyday affairs of the client. Caregiving responsibilities can include providing personal care, performing medical procedures, managing a client’s affairs, and facilitating or coordinating medical care and social services for the client (Levine, 2004).
Healthy family members have concurrent demands on their time from their own nuclear families, work, church, and community responsibilities. This is particularly true when spouses have to become caregivers in younger families (Gordon & Perrone, 2004). A significant change in health status can cause previous unresolved relationship issues, which may need advanced intervention in addition to the specific health care issues. When individual family members are experiencing a transition, for example, ending or entering a relationship, or job change, they may not be as available as support and can experience unnecessary guilt about it. Nurses need to consider the broader family responsibilities people have as an important part of the context of health care in providing holistic care to a particular family.
Meeting family informational needs
Sharing information is a mutual process. Nurses need to welcome and respect family input and engage the family in mutual decision making (Levine, 2004). Helping client families anticipate what will happen as a chronic disease progresses and how the day-to-day needs will change helps eliminate the stress of the unknown. Nurses can offer suggestions about how to respond to these changes, and offer support to the family caregiver as they emerge. Helping family members access services, support groups, and natural support networks at each stage of their loved one’s illness empowers family members because they feel they are helping in a tangible way.
Supporting the caregiver
Providing emotional support is crucial to helping families cope. Remaining aware of one’s own values and staying calm and thoughtful can be very helpful to a family in crisis. Remember that your words can either strengthen or weaken a family’s confidence in their ability to care for an ill family member.
Focus initially on issues that are manageable within the context of home caregiving. This provides a sense of mastery and satisfaction. The nurse can encourage the family to develop new ways of coping or can list alternatives and allow the family to choose coping styles that might be useful to them. Focus on what goes well, and ask the family to share with you their ideas about how to best care for the client.
Many families will need information about additional home care services, community resources and options needed to meet the practical, and financial and emotional demands of caring for a chronically ill family member.
Encouraging families to use natural helping systems increases the network of emotional and economic support available to the family in time of crisis. Examples include contact with other relatives, neighbors, friends, and churches. Spiritual beliefs and support from extended family and friends enhance family resilience in times of trauma and loss (Greeff & Human, 2004).
Validating and normalizing emotions
Families can experience many conflicting emotions when placed in the position of providing protracted care for a loved one. Compassion, protectiveness, and caring can be intermingled with feelings of helplessness and being trapped. Major role reversals can stimulate anger and resentment for both client and family caregiver.
Sibling or family position or geographic proximity may put pressure on certain family members to provide a greater share of the care. Criticism or advice from less involved family members can be disconcerting and conflicts about care decisions can create rifts in family relationships. Some caregivers find themselves mourning for their loved one, even though the person is still alive, wishing it could all end and feeling guilty about having such thoughts.
These emotions are normal responses to abnormal circumstances. Listening to the family caregiver’s feelings and struggles without judgment can be the most healing intervention you can provide. Nurses can normalize negative feelings by offering insights about common feelings associated with chronic illness. Family members may need guidance and permission to get respite and recharge their commitment by attending to their own needs. Support groups can provide families with emotional and practical support, and a critical expressive outlet.
Psychosocial issues for parents with chronically ill children can cover many relationship issues, for example, how to respond and discipline children with chronic illness. Siblings sometimes get shortchanged emotionally, if not physically, when the focus necessarily is on the child with a serious illness or disability (Drench, Noonan, Sharby, & Ventura, 2007). Well siblings may experience feelings of resentment, worry that they might contract a similar illness, or have unrealistic expectations of their part in the treatment process. Siblings need clear information about the sick child’s diagnosis and care plan. They need to be treated as children with needs of their own and should not be expected to assume adult caretaker responsibility for younger siblings while parents focus on the ill child (Fleitas, 2000). Exercise 13-9 provides practice with using intervention skills with families.
Evaluation
Referrals, continuing the contact with another health professional, or family education about when to contact the health system may be needed (Wright & Leahey, 2004). The referral should include a summary of the information gained to date and should be communicated by the health team member most knowledgeable about the client’s condition. Discuss with the client what will be shared with the referral resource.
Summary
This chapter provides an overview of family communication and the complex dynamics inherent in family relationships. Families have a structure, defined as the way in which members are organized. Family function refers to the roles people take in their families, and family process describes the communication that takes place within the family. Theoretical frameworks, developed by Bowen, Minuchin, Duvall, and McCubbin, are particularly relevant for nurses in understanding family dynamics in health care settings.
Family-centered care is developed through a combination of strategies designed to gather information in a systematic, efficient manner starting with the genogram and ecomap. Therapeutic questions and giving family commendations are interventions nurses can use with families.
Families with critical illness need continuous updated information, and the freedom to be with their family member as often as possible. Involving the family in the care of the client is important. Parents want to participate in the care of their acutely ill client.
Nursing interventions are aimed at strengthening family functioning and supporting family coping during hospitalization and in the community.
References
Aldridge, M. Decreasing parental stress in the pediatric intensive care unit. Crit Care Nurse. 2005;25(6):40–51.
Barker, P. Different approaches to family therapy. Nurs Times. 1998;94(14):60–62.
Bell, J.M. Encouraging nurses and families to think interactionally: revisiting the usefulness of the circular pattern diagram. J Fam Nurs. 2000;6(3):203–209.
Bowen, M. Family therapy in clinical practice. Northvale, NJ: Jason Aronson, 1978.
Byng-Hall, J. Therapist reflections: diverse developmental pathways for the family. J Fam Ther. 2000;22:264–272.
Cicchetti, D., Blender, J.A. A multiple levels of analysis perspective on resilience: implications for the developing brain, neural plasticity, and preventive interventions. Ann N Y Acad Sci. 2006;1094:248–258.
Clark, S. The double ABCX model of family crisis as a representation of family functioning after rehabilitation from a stroke. Health Med. 1999;4(2):203–220.
Cole-Kelly, K., Seaburn, D. Five areas of questioning to promote a family oriented approach in primary care. Fam Syst Health. 1999;17(3):341–348.
Dalton, W., Kitzmann, K. Broadening parental involvement in family-based interventions for pediatric overweight: implications from family systems and child health. Fam Commun Health. 2008;31(4):259–268.
Drench, M., Noonan, A.C., Sharby, N., Ventura, S. Psychosocial aspects of health care, ed 2. Upper Saddle River, NJ: Pearson Prentice Hall, 2007.
Duvall, E. Marriage and family development. Philadelphia: JB Lippincott, 1958.
Eggenberger, S., Nelms, T. Being family: the family experience when an adult member is hospitalized with a critical illness. Issues Clin Nurs. 2007;16:1618–1628.
Feeley, N., Gottlieb, L. Nursing approaches for working with family strengths and resources. J Fam Nurs. 2000;6(1):9–24.
Fleitas, J. When Jack fell down, Jill came tumbling after: siblings in the web of illness and disability. Am J Matern Child Nurs. 2000;25(5):267–273.
Gerson, R., McGoldrick, M., Petry, S. Genograms: assessment and intervention, ed 3. New York, NY: WW Norton & Co, 2008.
Gilbert, R. The eight concepts of Bowen theory. Falls Church, VA: Leading Systems Press, 2006.
Glasscock, F., Hales, A. Bowen’s family systems theory: a useful approach for a nurse administrator’s practice. J Nurs Adm. 1998;28(6):37–42.
Goldenberg, H., Goldenberg, I. Family therapy: an overview. Belmont, CA: Thomson Brooks/Cole, 2008.
Gordon, P., Perrone, K. When spouses become caregivers: counseling implications for younger couples. J Rehabil. 2004;70(2):27–32.
Greeff, A., Human, B. Resilience in families in which a parent has died. Am J Fam Ther. 2004;32:27–42.
Kristjanson, L., Aoun, S. Palliative care for families: remembering the hidden patients. Can J Psychiatry. 2004;49(6):359–365.
Leahey, M., Harper-Jaques, S. Family-nurse relationships: core assumptions and clinical implications. J Fam Nurs. 1996;2(2):133–152.
Leahey, M., Svavarsdottir, E. Implementing family nursing: how do we translate knowledge into clinical practice. J Fam Nurs. 2009;15(4):445–460.
Leon, A. Involving family systems in critical care nursing: challenges and opportunities. Dimens Crit Care Nurs. 2008;27(6):255–262.
Leon, A., Knapp, S. Involving family systems in critical care nursing: challenges and opportunities. Dimens Crit Care Nurs. 2008;27(6):255–262.
Levine, C. Always on call: when illness turns families into caregivers. Nashville, TN: Vanderbilt University Press, 2004.
Limacher, L., Wright, L. Commendations: listening to the silent side of a family intervention. J Fam Nurs. 2003;9(2):130–150.
McBride, J.L. Managing family dynamics. Fam Pract Manag. 2004;11(7):70.
McCormick, M., Hardy, K. Re-visioning family therapy: race, culture and gender in clinical practice, ed 2. New York: The Guilford Press, 2008.
McCubbin, H.I., McCubbin, M.A., Thompson, A. Resiliency in families: the role of family schema and appraisal in family adaptation to crisis. In: Brubaker T.H., ed. Family relations: challenges for the future. Newbury Park, CA: Sage, 1993.
McCubbin, H.I., McCubbin, M.A., Thompson, A.I., et al. Resiliency in ethnic families: a conceptual model for predicting family adjustment and adaptation. In: McCubbin H.I., McCubbin M.A., Thompson A.I., et al, eds. Resiliency in Native American and immigrant families. Thousand Oaks, CA: Sage Publications, 1998.
McKenry, P., Price, S. Families and change: coping with stressful events and transitions. Thousand Oaks, CA: Sage, 2005.
Medalie, J., Cole-Kelly, K. The clinical importance of defining family. Am Fam Physician. 2002;65(7):1277–1279.
Minuchin, S. Families and family therapy. Boston: Harvard University Press, 1974.
Miracle, V. Strategies to meet the needs of families of critically ill patients. Dimens Crit Care Nurs. 2006;25(3):121–125.
Nichols, M., Schwartz, R. Family therapy: concepts & methods, ed 9. Prentice Hall: Upper Saddle River NJ, 2009.
Novilla, M., Barnes, N., De La Cruz, N., Williams, P. Public health perspectives on the family. Fam Commun Health. 2006;29(1):28–42.
Otto, H. Criteria for assessing family strength. Fam Process. 1963;2:329–338.
Perrin, K. Understanding the essentials of critical care nursing. Upper Saddle River, NJ: Pearson Prentice Hall, 2009.
Rempel, G., Neufeld, A., Kushner, K. Interactive use of genograms and ecomaps in family caregiving research. J Fam Nurs. 2007;13(4):403–419.
Rivera-Andino, J., Lopez, L. When culture complicates. RN. 2000;63(7):47–49.
Ryan, E., Steinmiller, E. Modeling family-centered pediatric nursing care: strategies for shift report. J Spec Pediatr Nurs. 2004;9(4):123–129.
Schor, E.L. Family pediatrics: report of the Task /force on the Family. Pediatrics. 2003;111(6 Pt2):154–171.
Selekman, M. Solution focused therapy with children: harnessing family strengths for systemic change. New York: Guilford Press, 1997.
Sydnor-Greenberg, N., Dokken, D., Ahmann, E. Coping and caring in different ways: understanding and meaningful involvement. Pediatr Nurs. 2000;26(2):185–190.
Tapp, D., Moules, N. Family skills labs: facilitating the development of family nursing skills in the undergraduate. J Fam Nurs. 1997;3(3):247–267.
The Bowen Center, Washington, DC. Bowen theory: societal emotional process, 2004. Available online, http://www.thebowencenter.org/pages/conceptsep.html. [Accessed May 25, 2009].
Toman, W. Family therapy and sibling position. New York: Jason Aronson Publishers, 1992.
Trotter, T., Martin, H. Family history in pediatric primary care. Pediatrics. 2007;120:S60–S65.
Vandall-Walker, V., Jensen, L., Oberle, K. Nursing support for family members of critically ill adults. Qual Health Res. 2007;17(9):1207–1218.
Van Horn, E., Kautz, D. Promotion of family integrity in the acute care setting: a review of the literature. Dimens Crit Care Nurs. 2007;26(3):101–107.
Verhaeghe, S., Defloor, T., Van Zuuren, F., et al. The needs and experiences of family members of adult patients in an intensive care unit: a review of the literature. J Adv Nurs. 2005;14:501–509.
von Bertalanffy, L. General systems theory. New York: George Braziller, 1968.
Walsh, F. The concept of family resilience: crisis and challenge. Fam Process. 1996;35(3):261–279.
Wigert, H., Berg, M., Hellstrom, A.L. Parental presence when their child is in neonatal intensive care. Scand J Caring Sci. 2010;23:139–146.
Wright, L., Leahey, M. How to conclude or terminate with families. J Fam Nurs. 2004;10(3):379–401.
Wright, L.M., Leahey, M. Nurses and families: a guide to family assessment and intervention, ed 5. Philadelphia: FA Davis, 2009.