Communicating with Older Adults
At the end of the chapter, the reader will be able to:
1 Discuss concepts of normal aging.
2 Identify the use of theoretical frameworks used in the care of older adult clients.
3 Describe assessment strategies with older adults.
4 Describe supportive nursing care strategies with older adults.
5 Discuss assessment and support interventions for cognitively impaired older adults.
This chapter focuses on assessment and communication strategies related to client-centered relationships with older adults. The chapter presents basic concepts about aging as part of the life process and explores age-related changes that can affect communication. Developmental frameworks and the nursing process form a structural foundation for providing care to older adults. Communication strategies to support successful aging and to use with clients demonstrating cognitive impairment are included. Effective communication is critical to the health and well-being of older adults.
Basic concepts
Effective communication with older adult adults requires a thorough understanding of the normal health-related changes associated with aging. Aging is a term used to describe “advancing through the life cycle, beginning at birth and ending at death” (Pankow & Solotoroff, 2007, p. 19). Although aging is a lifelong process, the most common interpretation refers to physiologic decline, and associated mental and social changes occurring in late adulthood.
Aging is a normal physiologic process, accompanied to a greater or lesser degree by changes in appearance and energy levels, degenerative changes in organs and tissues, a weaker immune system, sensory losses, and decreased functional capacity related to mobility. Aging affects physical strength, stamina, and flexibility, and ultimately, an individual’s ability to negotiate the physical environment. Cotter and Gonzalez (2009) define “successful aging as the ability to adapt flexibly to age-related changes without relinquishing the central components of self-definition” (p. 335).
Older adults are often treated as if they represent a single cohort, when, in fact, there are huge differences in their life experiences, opportunities, capabilities, interests, and relationships. As people live longer, the term older adult or senior is broken down into three age cohorts: young old (65–74 years), old-old (75–84 years), and oldest-old (85 years and older) (Moody, 2010). A lot of older adults are frail and can have reduced function because of age-related disease, but many will retain a high level of physical and intellectual function until close to their death.
Each person’s experience of the aging process is unique, reflecting his or her genetic makeup, personality, life experiences, as well as environmental and cultural factors. Aging is a life process influenced by many factors, some of which are preventable or reversible. Although genetic and physiologic factors are not totally within an older person’s control, learning adaptive self-management strategies can make a major difference in an older adult’s overall health and quality of life.
Aging need not be a negative experience. Healthy older adults generally have more time and less responsibilities. There is time to travel, engage in activities one didn’t have time for previously, develop new interests, take a course, take an active role in community activities, share their talents with others, and enjoy family and grandchildren. Our attitude toward aging can become a self-fulfilling prophecy. Bortz (1990) states:
If we dread growing old, thinking of it as a time of forgetfulness and physical deterioration, then it is likely to be just that. On the other hand, if we expect it to be full of energy and anticipate that our lives will be rich with new adventures and insight; then that is the likely reality. We prescribe who we are. We prescribe what we are to become. (p. 55)
Biggs (2001) notes that positive stories of aging need to be told and incorporated into contemporary social policy. Older adults often lack the developmental supports provided earlier in life. People take pride in teaching and supporting children and young adults to achieve the life building skills they need as their developmental needs change. Articles detail the signs and symptoms of degenerative changes, with less attention paid to what older adults need to enhance quality of health and well-being.
Aging has direct and indirect effects on communication and interpersonal relationships. Nurses working with older clients need to have a thorough understanding of the aging process and positive respect for their struggles. Exercise 19-1 provides you with an opportunity to explore your personal ideas about aging.
Aging and health
Sowers and Rowe (2007) note, “By 2050, the number of persons aged 60 and over is projected to increase from 600 million to almost 2 billion (p. 11). Four- and five-generation families are becoming common as life span increases. Family-based assistance as the primary source of long-term care for the frail elderly will continue to increase (Gavan, 2003).
Older adults are not a homogenous population with similar health needs. Individual differences in the aging process allow many to experience relatively few health problems even into their eighties. But it is true that after the age of 60, people are more vulnerable to a variety of age-related diseases, such as cancer, cardiac and circulatory problems, stroke, and degenerative bone loss. Older people may gradually lose control over some of their bodily functions and movements, which interferes with their sense of dignity and self-image (Franklin, Ternestedt, & Nordenfelt, 2006). Older adults disproportionately experience a larger number of chronic conditions and diseases. As a cohort, they are the largest users of health services (Scholder, Kagan, & Schumann, 2004).
Older adults can experience subtle discrimination in accessing health care, level of screening and choice of treatment options. Physicians are less likely to use extensive diagnostic testing or aggressive treatment with older adults and they are underrepresented in clinical trials in part because of co-existing medical conditions. Medicare does not pay for experimental drugs. Other obstacles include navigating the complexity of the medical system, and limitations and gaps in services for chronic health care conditions. The decreasing number of physicians and other health care providers accepting elderly clients and/or suboptimal Medicare reimbursement for chronic care conditions is another factor.
Contemporary older adults
Our view of the elderly is changing as people live longer and experience less disability for shorter periods before death. Our perception of quality of life for older adults is changing and is likely to continue to evolve.
Contemporary “older adults” are not the same as they were even a few decades ago. They have been exposed to different opportunities than their parents had, related to economics, health, information technology, gender roles, and so on (Curtis & Dixon, 2005). As baby boomers “come of age,” they represent a highly educated cohort who is more health conscious and better informed about health matters than in previous generations. By 2030, the baby boomers will have all reached the age of 65, double the number of older adults at the beginning of the 21st century (Mellor & Rehr, 2005). To date, this cohort represents the future for health care needs of older adults. Very shortly, it will become the present. Exercise 19-2 offers an opportunity to think about the implications of planning health care for contemporary older adults (baby boomers).
Older adults are generally healthier in terms of less severe functional problems and chronic disability. They are living longer with a more robust quality of life (Maples & Abney, 2006). With current recessionary trends and Social Security changes, people are retiring later, and many remain actively engaged in the community. With many more people living into their 90’s, living adult children in their fifties and sixties are likely to become primary caregivers for very old relatives. Health care reform, long-term care, the future of Medicare, and new images of health and well-being in older adults are important issues that health care professionals will need to consider.
The literature, anchored by Rowe and Kahn (1998), identifies three fundamental characteristics associated with successful aging:
Theoretical frameworks used in the care of older adult clients
Erik erikson’s ego development model
Erikson’s (1982) model of psychosocial development is one of the only developmental models that specifically addresses later adulthood (>60 years) as a stage of ego development. Erikson portrays the maturational crisis of old age as that of ego integrity versus ego despair. Awareness of one’s personal mortality leads to the psychosocial crisis identified with this last stage of ego development.
Ego integrity relates to the capacity of older adults to look back on their lives with satisfaction and few regrets, coupled with a willingness to let the next generation carry on their legacy. Integrity involves acceptance of “one’s one and only life cycle as something that had to be and that by necessity permitted of no substitution” (Erikson, 1950, p. 268). Acceptance develops through self-reflection and dialogue with others about the meaning of one’s life. Nursing strategies encourage life review, and reminiscence groups facilitate the process. Ego despair describes the failure of a person to accept one’s life as appropriate and meaningful. Left unresolved, despair leads to feelings of emotional desolation and bitterness.
Wisdom, the virtue associated with Erikson’s eighth and final stage of ego development, represents an integrated system of “knowing” about the meaning and conduct of life. It involves a general knowledge about human nature and specific knowledge about its variations. (Kunzmann & Baltes, 2003). Sharing one’s wisdom with others enhances the experience of ego integrity. Wisdom includes deep understanding of self and others, good judgment, and the insights that people have about living a life filled with courage, purpose, and meaning.
Le (2008) discusses two forms of wisdom: practical wisdom and transcendent wisdom. Practical wisdom emphasizes good judgment and the capacity to resolve complex human problems in the real world. Transcendent wisdom focuses on existential concerns and development of the self-knowledge that allows a person to transcend subjectivity, bias, and self-centeredness. Wisdom encourages older adults to share their understanding of life with those who will follow. Erikson (Erikson, Erikson, & Kivnick, 1986) believed that wisdom develops from confronting and successfully resolving life’s psychosocial crises. Sharing wisdom in the form of personal stories creates a strong legacy for those in the next generation. Exercise 19-3 explores the relationship of life experiences with wisdom.
Abraham maslow’s basic needs model
Maslow’s (1954) hierarchy of needs (see Chapter 1) helps nurses prioritize nursing actions, beginning with basic survival needs. Physiologic integrity, followed by safety and security, emerge as the most basic critical issues for aging adults and need to be addressed first. Love and belonging needs are challenged by increased losses associated with death of important people. Esteem needs, especially those associated with meaningful purpose, and independence remain important issues in later life. Abraham Maslow believed that self-actualization occurs more often in middle-aged and older adults (Moody, 2010).
Applications
Assessment strategies with older adult clients
New situations can cause transitory confusion for older adults, apart from cognitive impairment. Many clients are aware of the stereotypes associated with aging and are reluctant to expose themselves as inadequate in any way. Knowing what to expect helps decrease anxiety and build trust. Continuity of care with one primary caregiver, when possible, helps foster the development of a comfortable nurse-client relationship.
Older adults are likely to be more responsive when time is taken to establish a supportive environment before conducting a formal assessment. Otherwise, it can be difficult for clients to discuss emotional issues associated with the aging process or their physical ailments. Sensitive issues such as loneliness, abuse and neglect, caregiver burden, fears about death or frailty, memory loss, incontinence, alcohol abuse, and sexual dysfunction will only be discussed within a trustworthy relationship (Adelman, Greene, & Ory, 2000).
Older adults appreciate having the nurse provide structure to the history-taking interview by explaining the reasons for it and what it will involve (Cochran, 2005). Asking clients to share something about themselves and their life history, apart from the reasons for the health visit or admission, helps to establish rapport and increases the client’s comfort level.
By relating their life stories and exploring options relevant to their current health situation, older adults are able to step back and look at their situation in the present from a broader perspective. Nurses get to know the client as a person, rather than categorically as an “older adult.” Box 19-1 identifies communication guidelines for assessment interviews.
Moody (2010) maintains that old age “is shaped by a life time of experience” (p. 2). Assessment of older adult clients begins with their story. As they relate their story, look for value-laden psychosocial issues (e.g., independence, fears about being a burden, role changes, and vulnerability) and client preferences. These are significant issues for older adults clients that may not be directly expressed.
Helping clients identify sources of social support, personal resources, and coping strategies helps soften the impact of physical and emotional stressors associated with age-related transitions (Gilmer & Aldwin, 2003). Exercise 19-4 provides a glimpse into the life stories of older adults.
Assessing age-related sensory changes
Sensory changes occur with normal aging. In particular, hearing and vision changes can have a direct and significant impact on communication and cognitive processing (Gonsalves & Pichora-Fuller, 2008). Vision and hearing enhancements are essential to ensuring client safety and staying connected with people in their environment. Anderson (2005) notes that addressing common causes of sensory impairment and providing sensory cues can help reduce confusion.
Hearing: According to the National Institute on Deafness and Other Communication Disorders (NIDCD, 2010), one in three people older than 60 and half of those older than 85 will experience hearing loss. Hearing loss associated with normal aging begins after age 50 years and is due to loss of hair cells (which are not replaced) in the organ of Corti in the inner ear. This change leads initially to a loss in the ability to hear high-frequency sounds (e.g., f, s, th, sh, ch) and is called presbycusis (Gallo, 2000). Lower frequency sounds of vowels are preserved longer. Older adults have special difficulty in distinguishing sounds against background noises and in understanding fast-paced speech. Hearing problems can diminish an older person’s ability to interact with others, attend concerts and other social functions, and understand medical directions.
Adaptive Strategies for Hearing Loss: With a little planning in modifying communication with the hearing-impaired older adult, the relationship should not be any different from one with a client who does not have this disability. Ideally, you should position yourself at the same level as the client. It is important to speak with a normal or slightly louder than normal voice tone. You do not need to shout. Other strategies include the following:
• Address the person by name before beginning to speak. It focuses attention.
• If the person has a “better” ear, sit or stand on the side with the more functional ear.
• Speak slowly and distinctly.
• If your voice is high-pitched, lower it.
• If older adults doesn’t understand certain words, rephrase rather than repeat the words.
• Face older adults so they can see your facial expression and/or read your lips to enhance comprehension. Keep the client’s view of your mouth unobstructed.
• Help older adults adjust hearing aids. Lacking fine-motor dexterity, older adults may not be able to insert aids correctly to amplify hearing. Make sure hearing aids are turned on. If difficulties persist, check the batteries.
• Keep background noise to a minimum (e.g., radio or television).
• Solicit feedback to monitor how much and what the person has heard.
Vision: Vision normally declines as a person ages (Whiteside, Wallhagen, & Pettengill, 2006). Colors become dimmer, and images are less distinct. Even with corrective lenses, blurring occurs, and words are harder to read in soft lighting. Brighter lighting and larger print help immensely. More serious age-related vision problems such as cataracts, glaucoma, and age-related macular degeneration can cause blindness.
Vision has implications for effective communication and functional ability. Older adults with progressive vision loss may not see you shaking your head or nodding. They may see changes in emotional facial expressions. Loss of vision can affect a person’s ability to perform everyday activities (e.g., dressing, preparing meals, taking medication, driving, handling the checkbook, and seeing phone numbers). Vision affects functional ability to engage in hobbies or leisure activities (e.g., reading, doing handwork, and watching television). Poor vision is a major safety issue related to falls.
Adaptive Strategies for Vision Loss: Nurses can play a vital role in supporting the independence of the visually impaired client with a few simple strategies.
• If eyeglasses are worn, make sure they are clean, and in place.
• Stand in front of the client.
• Verbally explain all written information, allowing time for the client to ask questions.
• Provide bright lighting with no glare.
• When using written materials, consider font and letter size for readability. Use upper and lowercase letters rather than all capitals. Use solid paper, with sharp contrasting writing, and a lot of white space.
Assessment of cognitive changes
Age-related changes in cognition for healthy adults are minimal and should not require major modifications in communication, although mental processing and reaction times may be slower (Moody, 2010). Without the ravages of disease, older adults show little loss of intelligence but may require more time in completing verbal tasks or in retrieving information from long-term memory (Wilson, Bennet, & Swartzendruber, 1997). Older adults are less likely to make guesses when they are presented with ambiguous testing items in mental status examinations. They may hesitate or not respond as well if they are under time pressure to perform. Otherwise, there should be no difference in functioning.
Approximately 6% to 8% of the population older than 65 years and more than 30% of those who reach the age of 85 will experience profound progressive cognitive changes associated with dementia (Yuhas et al., 2006). Dementia is characterized by memory loss, personality changes, and a deterioration in intellectual functioning that affects every aspect of the person’s life. A small percentage of abnormal cognitive changes are caused by other organic problems (e.g., drug toxicity, metabolic disorders, and depression) and may be reversed with treatment.
Appraisal of serious cognitive changes is critical to assessment of older adults, because it has the most impact on a person’s ability to perform activities of daily living (Moody, 2010). When the nurse has concern about a client’s cognitive capability, it is prudent to perform a mental status assessment early in the interview to avoid obtaining questionable data. The Mini-Mental State Examination (Folstein, Folstein, & McHugh, 1975) measures several dimensions of cognition (e.g., orientation, memory, abstraction, and language). Guidelines for mental status testing with older adults are presented in Box 19-2.
Another useful assessment tool is the clock drawing test (CDT). The client is asked to draw a clock with numbers and a selected time; for example, 20 minutes after 8. A normal score is given if the numbers are presented in the correct sequence and position, and the clock displays the requested time. An abnormal score suggests dementia, and further evaluation is recommended.
Assessment of functional status
More than any other factor, impaired functional status is associated with an older adult’s inability to live independently. Functional status refers to a broad range of purposeful abilities related to physical health maintenance, role performance, cognitive or intellectual abilities, social activities, and level of emotional functioning. Stress, acute and chronic illness, and age-related physiologic changes influence a person’s ability to function (Zisberg, Zysberg, Young, & Schepp, 2009).
Functional status rather than chronologic age should be the stronger indicator of disability-related needs in older adults. Chronologic age is somewhat of a misnomer, in that functional impairment is not associated solely with age. Burke and Laramie (2004) note that a chronically ill 50-year-old with no support system may have more disabling symptoms of aging than a healthy, active 75-year-old with a strong social support system in place.
Although age typically robs some of life’s vigor from older adults, most healthy cognitively intact older adults are able to perform activities of daily living (ADLs) independently, or with a little assistance. Instrumental activities of daily living (IADLs) are more complex than basic ADLs. IADLs refer to tasks older adults have to cope with on a daily basis, include cooking, cleaning, shopping, managing medications, getting to places beyond walking, using a telephone, and paying bills (Kleinpell, 2007).
From a basic health perspective, function relates to a person’s ability to perform essential ADLs. Essential ADLs refer to six areas of essential function: “toileting, feeding, dressing, grooming, bathing, and ambulation” (Miller, 2009, p. 96).
Evaluation of functional abilities helps determine the type and level of care an older adult requires. Functional abilities in older adults can range from vigorous, active, and independent, to frail and highly dependent, with serious physical, cognitive, psychological, and sensory deficits (Bonder & Bello-Haas, 2009).
Assessment of pain
Persistent pain is a common concern of older adults, related to chronic conditions such as osteoarthritis, diabetic peripheral neuropathy, constipation, among others (Jansen, 2008). Both client and health care professionals can assume that moderate or episodic pain associated with chronic disorders of aging is a natural part of growing old. Pain limits an older adult’s functional ability and compromises well-being; it should not be considered a normal consequence of aging. There is no more reason for an older adult client to suffer with chronic pain than there is for the younger client.
Chronic coexisting disorders such as depression or dementia can limit an older adult’s ability to report or to correctly interpret underlying causes of pain. For example, undiagnosed depression may present as neck or shoulder pain, severe enough to interfere with sleep or activity. Liberal dispensing of analgesics to older adults for pain relief without full assessment of the nature of the pain and considering compliance issues can lead to undesired outcomes. Rowan and Faul (2007) label prescription drug abuse as one of the fastest growing public health problems among older adults in the United States.
Older adults, even those who are cognitively intact, can have trouble interpreting the level of their pain with the commonly used Faces Pain Scale. Although they can report whether their pain interferes with daily functioning, identifying pain levels on a linear scale is more of a challenge (Gloth, 2004).
A comprehensive pain assessment for older adults should ask the client to
• Describe the quality and nature of the pain, for example, aching, burning, pressure, acute, or stabbing. (Some older adults will use the word discomfort instead of pain.)
• Identify when the pain occurs and under what circumstances.
• Identify specific pain patterns and/or changes in pain intensity.
• Describe how the pain affects the client’s physical, psychological, and social functioning (Feldt, 2008).
• Define the area of the body where the pain occurs, whether it is deep or superficial, localized or radiating.
Assessment of pain in cognitively impaired clients and in those who cannot communicate verbally, for example, a stroke victim with receptive aphasia, is accomplished through behavioral observation. Behaviors suggestive of pain include grimacing, tightened muscles, groaning, crying, agitation, lethargy, and unwillingness to move.
Psychosocial assessment
Windsor and Anstey (2008) cite several studies indicating that older adults experience higher psychosocial well-being compared with younger counterparts. Older adults are more likely to seek emotionally meaningful activities in the moment and are less concerned with future achievements.
Loss is a reoccurring issue for older adults. Most will suffer more meaningful losses of people, activities, and functions that were important to them than earlier in life.
Although most people weather the necessary losses of life, late-life depression is an often untreated problem in older adults. Unlike symptoms of depression in younger people, somatization with vague physical complaints may be its first presenting sign (Arnold, 2005). Whenever the nurse senses a loss of emotional energy in life and feelings of desolation about their situation, it is important to seek additional data from the client. Statements warranting further exploration include:
“Life doesn’t hold much for me anymore.”
“I’d never do anything to myself, but sometimes I wish I wasn’t here.”
Age is a strong risk factor for suicide, among older white men (Groh & Whall, 2001). Statements reflecting helplessness and hopelessness should never be taken lightly.
Supportive planning and intervention strategies in nurse-client relationships
Personal strengths form the basis for planning and interventions. Although older adults face many negative situational stressors, they also possess a lifetime of strengths that can be temporarily forgotten. Many older adults can live independently with social, spiritual, and environmental supports, with a good quality of life.
General nursing care for cognitively intact older adult clients, with the exception of acute care, centers around providing supports related to self-management of chronic illness and promoting healthy lifestyles. The level of support people need depends on personal, financial, and social resources that the older adult has at his or her disposal, and is willing and able to use. Asking questions such as “Can you tell me who visits you, or whom you have visited in the last month?” “If you needed immediate help, whom are you able to call?” and “Do you have enough sources of income to meet your basic needs?” gives nurses important data needed for planning and intervention.
Psychosocial communication supports
Older adults who are institutionalized in nursing homes appreciate short, frequent conversations. Like everyone else, the need to be acknowledged is paramount to older adults’ sense of self-esteem. Heliker (2009) describes a story sharing intervention identified as “a reciprocal give-and-take process of respectful telling and listening that focuses on what matters to the individual and minimizes the power of one over another” (p. 44). Conducted in long-term care facilities, this strategy emphasizes simple one-on-one human conversations with older adults about topics of interest to them.
Everyone has a story to tell. The use of short stories to frame conversation as a shared experience reminds clients that they have a valued social identity that goes beyond descriptions of their health. Each time an older adult tells their story, they remember when they saw themselves as a valued, productive member of society and that someone cares to listen. Nurses can teach and model this communication strategy with nursing assistants.
The conversational world for older adults can narrow for many reasons, for example, mobility, death of friends, and transportation. Spontaneous current events to draw from as a means of starting a conversation are not as available. A limited conversation repertoire happens with cognitively intact older adults, and they may repeat stories.
Repetitive stories can be frustrating for nurses. Rather than thinking, “Oh my, here he goes again with that old ‘Model T’ car story,” it is better to respond to the story and enter the conversation as fully as possible. Each conversation is an opportunity to gain insight into the person who he or she was, what aspirations and dreams were fulfilled or unfulfilled, what contributions are valued, and what goals are yet to be attained.
Life Review
Life review is a useful intervention with older adult clients. Gentle prompts and relevant questions for clarification are required. Sharing recollections from youth or early adulthood days with a compassionate listener helps older adults review their life, establish its meaning, and confront their conflicts, as well as pleasures. Sometimes it provides opportunities for older adults to reconcile long-standing conflicts (Bohlmeijer et al., 2009).
Reminiscence Groups
The interpersonal contact in groups can be therapeutic for lonely, isolated older adults (Henderson & Gladding, 2004). Guidelines for group communication with older adult clients in long-term care settings are presented in Box 19-3.
A specialized therapeutic form of group for older adults in long-term settings is the reminiscence group. Minardi and Hayes (2003) differentiate between life review, which explores life events in depth, and reminiscence groups, which focus on sharing life experiences from a socializing and a therapeutic perspective. They are powerful sources of self-esteem for older adult clients.
Reminiscence groups follow a structured format, with themes decided beforehand. Examples include special times in childhood or adolescence, child-rearing or work experience, and handling of a crisis. The leader guides the group in telling their stories, asking questions, and points out common themes to stimulate further reflections. Members create for themselves a shared reality by revealing to one another what life has meant and can be for them. In the process of remembering critical incidents, people can reconnect with sometimes forgotten parts of their life that held meaning for them. Jonsdottir, Jonsdottir, Steingrimsdottir and Tryggvadottir, 2001) note, “Recalling the past helps people to adjust to life’s changes and thus provides a sense of continuity, integrity and purpose within the person’s current life context” (p. 80).
Social and spiritual supports
Social isolation compromises the health and well-being of older adults (Strine, Chapman, Balluz, & Mokdad, 2008). Staying engaged with life to whatever extent is possible and stimulating the mind are two critical strategies healthy older adults can use on a daily basis to promote health and well-being as they grow older.
Quality friendship is an incomparable resource for older adults. Social support for older adults may need to be more proactive and wide-ranging than for younger people, because the older adults’ physical or intellectual vulnerability. They may require instrumental support with self-management of IADLs from family and friends. Helping family members and friends balance necessary assistance with the client’s need for autonomy is a delicate art.
Bishop (2008) notes, “Social and spiritual ties share an interdependent link to positive psychological well-being in late adulthood (p. 2). For people who have lost a “people” support system, connection with a personal God or faith can be a very important source of support. Older adults express their spirituality through prayer, reading their bible, and engaging in religious or spiritual practices.
Awareness of a shortened life span promotes thinking about existential issues, death, and for some, the need to work through unresolved life issues. Spiritual interventions relevant to the care of older adults include instilling hope, prayer, and talking about the client’s spiritual concerns. Helping clients cope with unfinished business and find forgiveness for self and others is identified as an important nursing intervention (Delgado, 2007). Clients with advanced dementia will often respond positively to spiritual hymns remembered from the past and to Bible readings.
Environmental supports
Maintaining independence for as long as possible with a good quality of life should be a goal for older adults. Independence is something most people take for granted as a younger adult, but it becomes a significant issue for older adults and their caregivers. Corey and Corey (2006) note, “As we age, we have to adjust to an increasingly external locus of control when confronted with losses over which we have little control” (p. 403).
The nurse plays a critical role in helping older adults maintain their autonomy. For older clients, being independent means that they are still in charge of their lives. As nurses assist clients to clarify values, make choices, and take action, a stronger understanding of their unique needs and strengths emerges. Older adults need to take as much responsibility for their choices and goal setting in health care as is possible.
Dialogues linking successful past coping experiences with present situations make it easier for the client to imagine possible individualized coping skills in the present. At the end of the dialogue, the nurse might summarize what the client has expressed and follow up with, “I enjoyed talking with you. You’ve had a fascinating life. What do you think is next for you?”
Nurses need to be sensitive to the unexpressed fears of older adults around surrendering their independence. Formal support services in the community, home health aides, and informal family supports can be critical factors in enabling frail older adults to remain independent.
You may need to directly observe environmental supports, bearing in mind a potential association in the older adults’ mind between accepting help and relinquishing independent living. For example, an older adult in cardiac rehabilitation told his nurse that he had a bedside commode and no stairs in his home. When the nurse visited the home, there was no commode, and the client’s home had a significant number of stairs. He told the nurse that he was afraid she would take steps to make him move if these facts were known.
Safety supports
Although there will always be a delicate balance between the client’s needs and restrictions or supports needed for safety, usually at least some areas can be negotiated. Simple interventions to promote independence include the following:
• Allowing elders personal choices about their bedtime, within reason
• Respecting choices in food selection
• Providing chair risers that help elders raise themselves from sitting to standing position
• Safety modifications in the home (e.g., bathtub rails, scatter rug removal, night lights)
• Including elder clients in decision making about health care and giving them the information they need to make responsible choices
Modern technology presents new possibilities to support the independence of older adults. Telehealth assistive services encompass virtual health visits, reminder systems, home security, social and health alarm monitors, and compensatory supports for failing functional abilities (Magnusson, Hanson, & Borg, 2004). Although telehealth is currently unavailable in many areas, innovative technology is likely to become an increasingly important component of support care for independent older adults.
Medication Supports
Polypharmacy is a fact of life for older adults. As people age, many need multiple medications to maintain a healthy lifestyle. Polypharmacy places older adults at risk for side effects and drug interactions because of age-related changes in metabolism (Cochran, 2005). Medications in general have a stronger effect on the older population and take longer to eliminate from the body.

Keeping track of medications can be challenging for older adults. Usually there is more than one provider. Prescriptions from different providers can create adverse reactions. When a provider lacks access to the complete client profile of medications, or does not have knowledge that the client is taking over-the-counter medications, the client suffers. Encouraging clients or a family to keep a written list of all medications to be shared with each provider helps prevent adverse drug interactions.
Healthy People 2010 objectives (Department of Health and Human Services [USDHHS], 2000) identify polypharmacy among older adults with chronic illness as a key safety issue. Medication mismanagement is associated not only with adverse drug reactions, but with hospital and nursing home admission. It is a major contributor to falls and hip fractures. Factors associated with poor self-management of medications include complexity of taking multiple medications, using incorrect techniques, improper medication storage, level of health literacy, cost of medications factors, and poor eyesight. Nurses should use every opportunity, informal as well as formal, to help clients establish and maintain appropriate self-management of medications (Curry, Walker, Hogstel, & Burns, 2005). The adage “start low, and go slow” (Miller, 2009, p. 129), which is a basic principle of geriatric drug prescription and regular communication with prescribers, is essential. Simplifying the older adult’s medication regimen and regular checking of expiration dates enhance medication management and lessen the possibility of adverse reactions.
During an assessment interview, and on each subsequent home or primary care visit, you should ask specifically about medication and treatment implementation. Ownby (2006) recommends using an open-ended question, such as “Tell me how you take your medications,” rather than asking, “Are you taking your medication as prescribed?” (p. 33). Box 19-4 covers key areas for medication assessment. Visually checking medications with the client and talking about how the medication is working with the client and/or primary caretaker is useful in home care.
Careful instruction as to the purpose, dosage, anticipated outcomes, and side effects can increase medication compliance. Establish a system with the client or family for medication administration, for example, prefilled medication dispensers or a medication calendar. Use a teach-back strategy to ensure that instructions are understood, and the client or family feels comfortable with their knowledge and capacity to implement administration.
Elder Abuse
Elder abuse represents a major threat to the safety and well-being of older adults. The term refers to the mistreatment of vulnerable older adults, usually at the hands of caregivers, including professional personnel. The most common form of elder abuse is neglect, both passive and active. Active neglect is deliberate. Passive neglect occurs when clients, most notably those with dementia, do not receive properly supervised care.
Elder abuse is a difficult problem to identify and treat. Diminished mental capacity compromises an older adult’s ability to even understand what is happening, let alone take constructive actions to stop the abuse, or to use any community services available to them (Nerenberg, 2008). Alternative options for older adults are not readily available, and older adults are reluctant to consider a nursing home as an option. Pride, embarrassment, and a desire to protect family members prevent vulnerable older adults from wanting to prosecute a family member for abuse or neglect. If the nurse identifies abuse or neglect, it must be reported to appropriate social and legal protective services.
Advocacy support
Fundamental rights of older adults in health care settings are identified in Box 19-5. Nurses play an important service in explaining treatment to clients and families, and helping them frame questions for physicians and hospitalists. Nurses assume advocate roles with older adults around the following issues:
• Right to refuse medication or treatment
• End-of-life decisions about care and life support issues
• Liaison between an older adult client and other health professionals
• Mediator with family and client concern around treatment, level of care, and placement issues
• Suspected cases of elder abuse
• Balancing an older adult’s need for freedom with necessary protections
Role modeling is an indirect form of advocacy, affecting the interpersonal relationships older adults have with their caregivers. Nursing assistants or professional caregivers provide the majority of care for older adult clients. Role-modeling excellent care and respect for the dignity of the older client, regardless of medical condition, is important. It is noted by family and nonprofessional staff, and has a ripple effect on the care that they provide.
Nurses can refer client family members to local Alzheimer’s disease and related dementia support groups. Support groups provide a place to talk about the challenges of caring for their family member. The 36-Hour Day (Mace & Rabins, 2006), developed from the insights of family members coping with dementia in a loved one, is an excellent resource.
Advocating for Legal Protections
Frail older adults and particularly clients with dementia usually need legal protection to safeguard their personal and financial affairs, and to allow others by proxy to make health care decisions when they are unable to do so. Nurses can be invaluable resources and advocates for clients and families in discussing health-related personal legal matters. Advance directives and a durable power of attorney for health care (proxy) provide direction for the client’s health care wishes should the person become incapacitated. For financial and property manners, the client needs to have a durable power of attorney, a living trust, and/or a will. Power of attorney documents are subject to state laws and are only in effect when people are unable to manage their own affairs. Under broad federal guidelines, state laws determine qualifications for Medicaid and property distribution if a person dies with no will or trust. Guidelines vary from state to state. Medicaid qualifications may be important for families requiring long-term care for a family member.
The time to execute legal documents to client rights is before clients become unable to cognitively assign decision-making authority to someone they trust. Clients in the early stages of dementia usually have sufficient mental competence to participate in legal decisions regarding their health care and finances. Later, they may not be able to execute the documents. Consultation with a lawyer regarding wills, durable and health powers of attorney, and living wills should be initiated at this time (Arnold, 2005).
Once cognitive capacity is lost, a court procedure is necessary to establish a conservatorship or guardianship. This action is more costly and emotionally painful for most families, as it requires legally certifying the person as incompetent. Mental incompetence is a medicolegal determination that identifies a person’s inability to manage his or her personal affairs because of injury, disease, or disability.
Clinical incompetence refers to a person’s inability to make appropriate health care decisions or to carry them out, as determined by a physician or qualified health care practitioner. Nurses can help clients make their wishes known and feel more comfortable about allowing trusted people in their lives to act on their behalf.
Health promotion for older adults
The CDC maintains that health-damaging behaviors such as poor nutrition, inactivity, and alcohol and tobacco abuse contribute heavily to the onset of disability in the elderly. They recommend an integrated health promotion approach to address common risk factors and comorbidities in older adults (Lang et al., 2005).
Older adults are much more health conscious today. They benefit from health promotion activities tailored to their stage of life. It is never too late to practice good nutrition; engage in healthful exercise such as strength training, walking, and yoga; connect with social relationships on a regular basis; and improve safety factors.
At the same time, healthy older adults are not young people. Their nutrition, exercise, and other health needs are different. Health promotion strategies need to be modified to meet the unique requirements of this population (Nakasato & Carnes, 2006). Box 19-6 identifies areas of relevant health promotion activities for older adults.
Through regularly scheduled health promotion activities, nurses can assist clients in learning about a healthier lifestyle. Nurses can engage older adults in health promotion activities by appealing to their interests and by incorporating cultural values in the presentation. Examples of relevant activities can include:
• Preparing examples of healthy ethnic food (e.g., “soul cooking the healthy way”)
• Assigning blocks of time for preventive screening, specifically for older adults
• Combining multiple prevention services into one clinical visit
• Providing free flu and pneumonia immunizations at convenient times in traditional and nontraditional settings (Lang et al., 2005; Penprase, 2006)
Health Teaching
Moody (2010) notes that health teaching for the elderly is critical if they are to master the tasks of old age and maintain their health. Healthy older adult clients are similar to other adult learners, except that they may need more time to think about how they want to handle a situation. The sensitive nurse observes the client before implementing teaching and gears teaching strategies to meet the individual learning needs of each client.
Assuming that older adult clients lack the capacity to understand instructions is a common error. Health care providers often direct instruction to the older adult client’s younger companion, even when the client has no cognitive impairment. This action invalidates the client and diminishes self-worth. Mauk (2006) identifies simple modifications to reduce age-related barriers to learning when teaching older adults. Suggestions include:
• Explain why the information is important to the client.
• Use familiar words and examples in providing information.
• Draw on the client’s experiences and interests in planning your teaching.
• Make teaching sessions short enough to avoid tiring the client and frequent enough for continuous learning support.
Assessment and support interventions for cognitively impaired older adults
Assessment of cognitive function should occur early in the client relationship. Dementia is a neurologic syndrome characterized by a progressive decline in intellectual and behavioral functioning that ends in death. Alzheimer’s disease is the most common form, followed by vascular dementia and rare forms of dementia.
Symptoms of cognitive impairment and communication difficulties in older adults can be similar in clients suffering from depression, delirium, and dementia. Diagnosis has important implications for treatment. Communicating with a client suffering from dementia requires a different set of strategies than for the client with depression. Clients with depression can still communicate normally. Table 19-1 identifies important differences between these three common disorders in late adulthood. Secondary clinical depression and/or delirium can be superimposed on dementia, making a difficult situation even more challenging. Exercise 19-5 provides an opportunity to distinguish between dementia, delirium, and depression, using a case study.
TABLE 19-1
Sorting Out the Three D’s: Delirium, Dementia, Depression
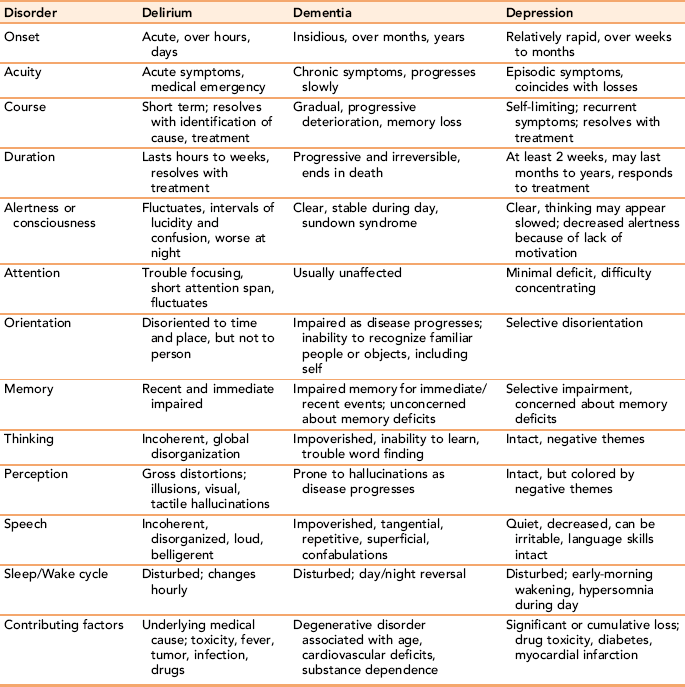
Adapted from Arnold E: Sorting out the three D’s: delirium, depression, dementia, Holist Nurs Pract 19(3):99–104, 2005.
Supporting adaptation to daily life
Box 19-7 outlines early cognitive changes seen with dementia. Memory loss is a consistent finding. Structure and consistency in the environment are important themes to consider. In the early stages, nurses can help clients develop reminder strategies such as making notes to themselves and using colored labels, alarms, or calendars. Focusing on what the client can do, rather than on deficits, does not change the course of the dementia. This strategy taps into the functions still available to the client and decreases feelings of hopelessness (Cotter, 2009).
Apraxia, defined as the loss of the ability to take purposeful action even when the muscles, senses, and vocabulary seem intact is a common feature of dementia. The person appears to register on a command but acts in ways that suggest he or she has little understanding of what transpired verbally. In the following case example, the caregiver observes the client’s difficulty. Notice how her response supports his ability to function. The client in the example had been the president of his company before being diagnosed with dementia.
Supporting communication
Difficulty with communication is a hallmark of dementia. The dementia client’s loss of communication is a gradual process initially and most clients can maintain superficial conversation, with empathetic support. Miller (2008) notes that dementia affects basic receptive (decoding and understanding) and expressive (conveying information) forms of communication. These deficits impact the person’s capacity to think abstractly and solve problems. Clients may have more difficulty with communication when stressed or tired. Identify yourself and address the client by name before beginning each conversation. Clients benefit from frequent orientations, word sharing, and redundancy. Box 19-8 summarizes communication guidelines.
The use of cues in communication is helpful to the older adult with short-term memory impairment. Word retrieval to express ideas diminishes (aphasia) over time. The dementia client, unable to continue, stops in mid-sentence or continues with phrases that have little to do with the intended meaning (Mace & Rabins, 2006). Allow extra time for clients to decode the material.
Anything to help reduce the client’s anxiety about groping for thoughts that do not come easily is useful. Helping clients put words or thoughts together allow the conversation to continue. Nurses can support clients by filling in missing words, or supplying a logical meaning, and then asking the client if this is what he or she meant. Another strategy is to almost finish a sentence and have the client supply the last word. If there are terms the client typically substitutes for common words or phrases, for example, the word “clock” for asking about time, use the client’s term. You also can ask the client to point to an object or describe something similar if you don’t understand what the client is referencing (Miller, 2008). As dementia progresses, clients become increasingly unable to understand and express complete thoughts. Eventually the client with dementia cannot carry on even simple conversations. Use questions that can be answered with a yes or no for clients with less verbal skill. Note whether the client’s behavior is consistent with the yes or no answer, and follow up if the behavior is incongruent with the words.
Restate ideas using the same words and sequence, and validate the meaning of a client’s response. Instead of using abstract prompts (like a specific time), use words directly applicable to the client’s daily routine, such as “before lunch” to anchor the client’s recognition of time frames. If a client rambles, you can refocus attention by selecting a single relevant thought from the stream of loosely connected ideas.
Cognitively impaired clients often are unable to follow instructions that consist of multiple steps. Breaking instructions down into single smaller steps helps mildly impaired clients master tasks that otherwise are beyond their comprehension.
Asking mild to early moderate cognitively impaired older adults about their past life experiences serves as a way to connect verbally with those who might have difficulty telling you what they had for breakfast 2 hours ago. Nurses should appreciate that when cognitively impaired adults share memories they are giving a gift to the nurse by sharing part of themselves when they may have very little else to give.
Remote memory (recall of past events) is retained longer than memory for recent events. Family members can be encouraged to reminisce with dementia clients. This can be a meaningful experience for the family member even when the client cannot actively engage in the discussion, as it is a means of connecting. It is not uncommon for a dementia client to show through facial expression or garbled words that he or she too experiences the connection, even if only for a fleeting moment. Or it may come later.
Touch
Touch is something clients with dementia can no longer ask for, create for themselves, or tell another of its meaning. Touch is a form of communication, used to reinforce simple verbal instructions with cognitively impaired adults, and as a primary form of communication. It is experienced “not only physically as sensation, but also affectively as emotion and behavior” (Kim & Buschmann, 2004, p. 35). As dementia progresses, gentle touch can anchor an anxious or disoriented person in present time, space, and humanity. When used to gain a client’s attention, or to guide a person toward an activity, touch can acknowledge a client’s stress, calm an agitated client, or provide a sense of security. In general, clients with dementia appreciate the use of touch. But to some, it can be frightening if the client perceives the caregiver as threatening. You can usually tell when a client thinks you are entering his or her personal space by looking at facial expression. Before using touch, make sure that the client is open to it.
Putting lotion on dry skin, giving back rubs, and warming cold hands or feet can be meaningful to the dementia client, as is something as simple as holding the client’s hand. When a person is no longer able to recognize familiar caregivers by name, nurturing touch provides a touchstone with the physical reality of someone who cares about the client. It may be his or her only remaining opportunity for human interaction.
Reality orientation groups
Reality orientation groups are used with older adults experiencing moderate-to-severe cognitive impairment. Focusing on their personal environment, these groups keep people in touch with time, place, and person. Topics can include landmarks in the dining room, routes to the dining room or bathroom, the date, time and weather, what people would like to wear, and so on. Reality orientation groups may be conducted daily or weekly with three to four clients (Minardi & Hayes, 2003).
Validation therapy
Validation describes a therapeutic communication process used in later stages of dementia. Developed by Naomi Feil, validation recognizes that a client is responding to a different reality related to time, place, or person (Minardi & Hayes, 2003). Rather than confronting dementia clients with “facts”—that people they knew or places they have lived are no longer available to them—the nurse focuses on the personal meaning events and people hold for the client. For example, you might say, “Tell me about Mary,” or “What was it like living on M street?”
Defusing catastrophic reactions
Older adults with memory loss lack the cognitive ability to develop alternatives. They emotionally overreact to situations, and can have what look like temper tantrums in response to real or perceived frustration. Older adult tantrums are called catastrophic reactions, and they represent a completely disorganized set of responses. Usually there is something in the immediate environment that precipitates the reaction. Fatigue, multiple demands, overstimulation, misinterpretations, or an inability to meet expectations are contributing factors (Mace & Rabins, 2006).
The emotion may be appropriate, even if its behavioral manifestation is not. Warning signs of an impending catastrophic reaction include restlessness, body stiffening, verbal or nonverbal refusals, and general uncooperativeness.
Instead of focusing on the behavior, try to identify and eliminate the cause(s) (Hilgers, 2003). Use distraction to move older adults away from the offending stimuli in the environment; use postponement. For example, you could say, “We will do that later; right now, let’s go out on the porch,” while gently leading the person away. Direct confrontation and an appeal for more civilized behavior usually serve to escalate rather than diminish the episode.
Sundowning is the term used to describe episodic agitated behavior occurring in the late afternoon or early evening with clients in the middle stages of dementia. Common childlike behaviors of whining, agitation, and temper tantrums characterize the syndrome. Small doses of medication are used to alleviate symptoms. Caution is needed to avoid over-sedating the client.
Caring for clients with advanced dementia
As the dementia progresses, people lose control over most of their body functions and will experience one or more psychopsychiatric symptoms. They will require total care, which, in many cases, will include formal and informal caregiving strategies. Table 19-2 identifies common neuropsychiatric symptoms associated with advanced dementia, with suggested behavioral communication interventions.
TABLE 19-2
Neuropsychiatric Symptoms with Suggested Behavioral Communication Interventions
| Neuropsychiatric Symptom Pattern | Suggested Intervention |
| Agitation | Identify and remove cause Assess for physical problems Reduce stimuli, suggest a walk Use simple repetitive activities: folding towels, rolling socks Use soothing music, Bible verses Look for patterns that trigger agitation |
| Aggression: grabbing, hitting | Recognize that the client is frightened Decrease stimuli, move client to a quiet place Don’t take the client’s behavior personally Respect and enlarge the client’s personal space Identify and minimize cause Make eye contact; speak in a calm voice Acknowledge frustration; don’t reprimand Check medications |
| Withdrawal: decreased socialization, apathy, social isolation | Use simple activities Find simple socialization opportunities, and support client involvement |
| Refusal/resistance to suggestions | Drop the topic/activity and reintroduce later |
| Disturbed motor activity: wandering, pacing, raiding waste cans, shadowing caregiver | Keep the environment safe Remove trash Use medical alert bracelets Label drawers, room (photos help) Use locks on doors at home |
| Sleep disturbances: Day/night sleep reversal, calling out/moaning in sleep | Keep active during the day Toilet client as needed during night without conversation Control wandering at night; lead back to bed; avoid use of restraints |
| Hallucinations, delusions, illusions | Respond to the emotion, not content Reduce stimuli Use good nonglare lighting Use distraction, e.g., walk, simple activity Use touch, reassurance, postponement |
| Disinhibition: inappropriate speech, touching, improper body exposure, entering other people’s space | Don’t reprimand Respond to the emotion Redirect client |
| Incontinence: urine, feces, eliminating in wrong places | Check for bladder infection, fecal impaction Note elimination pattern; establish corresponding toileting timetable Schedule toileting at frequent intervals Toilet before bedtime Take client to bathroom, verbally cue Use washable clothing, Velcro closings |
| Swallowing difficulty: choking, stuffing mouth, not swallowing | Cut food into small pieces, offer small quantities of liquid at one time Check medications for size, modify as needed Sit with client while eating Verbally cue to chew and swallow |
| Agnosia: difficulty recognizing faces, including one’s own | Remove or cover mirrors if client is frightened by self-image Verbally identify familiar people and their relationship to the client |
Treatment goals for clients with advanced dementia should emphasize dignity, quality of life, and supportive comfort strategies, rather than focusing on prolonging life (Rabins, Lyketsos, & Steele, 2006).
Summary
This chapter discusses concepts of aging and presents supportive communication strategies nurses can use in client-centered relationships with older adults. Aging is associated with a decline in sensory and motor functions for most people, but contemporary older adults can expect to live longer and enjoy a better quality of life than in previous generations.
Erikson’s theory of psychosocial development identifies wisdom as the virtue associated with his last stage of ego development, integrity versus despair. Supportive strategies to assist clients maximize their health and well-being during this important stage of life focus on communication, social and spiritual structure, the environment, safety, and medication management.
Assessment of depression, delirium, and dementia is important, as some symptoms are hard to differentiate. Guidelines for communicating with clients with dementia emphasize touch, as well as verbal supports. Strategies such as reminiscing, promoting client autonomy, using a proactive approach, acting as a client advocate, and treating older adults with dignity are proposed. Health promotion activities that take into account the unique needs and cultural values of older adults are more likely to be successful. As a primary provider in long-term care and in the community, the nurse is in a unique role to support and meet the communication needs of older adult clients.
References
Adelman, R.D., Greene, M., Ory, M., et al. Communication between older patients and their physicians. Clin Geriatr Med. 2000;16(1):1–24.
Anderson, D. Preventing delirium in older people. Br Med J. 2005;73(74):25–34.
Arnold, E. Sorting out the 3 D’s: delirium, dementia, depression. Holist Nurs Pract. 2005;19(3):99–104.
Biggs, S. Toward critical narrativity: stories of aging in contemporary social policy. J Aging Stud. 2001;15(4):301–316.
Bishop, A. Stress and depression among older residents in religious monasteries: do friends and God matter? Int J Aging Hum Dev. 2008;67(1):1–23.
Bohlmeijer, E., Kramer, J., Smit, F., et al. The effects of integrative reminiscence on depressive symptomatology and mastery of older adults. Community Ment Health J. 2009;45:476–484.
Bonder B.R., Bello-Haas V., eds. Functional performance in older adults, ed 3, Philadelphia: FA Davis, 2009.
Bortz, W. Use it or lose it. Runner’s World. 1990;25:55–58.
Burke, M., Laramie, J. Primary care of the older adult: a multidisciplinary approach, ed 2. St. Louis: Mosby, 2004.
Cochran, P. Acute care for elders prevents functional decline. Nursing. 2005;35(10):70–71.
Corey, M., Corey, G., Groups for the elderly. Groups: process and practice, ed 7, Belmont, CA, Thompson Brooks, 2006.
Cotter, V. Hope in early-stage dementia: a concept analysis. Holist Nurs Pract. 2009;23(5):297–301.
Cotter, V., Gonzalez, E. Self-concept in older adults: an integrative review of empirical literature. Holist Nurs Pract. 2009;23(6):335–348.
Curry, L., Walker, C., Hogstel, M., et al. Teaching older adults to self-manage medications: preventing adverse drug reactions. J Gerontol Nurs. 2005;31(4):32–42.
Curtis, E., Dixon, M. Family therapy and systemic practice with older people: where are we now? J Fam Ther. 2005;27(1):43–64.
Delgado, C. Meeting clients’ spiritual needs. Nurs Clin North Am. 2007;42(2):279–293.
Department of Health and Human Services (USDHHS). Healthy people 2010. Washington, DC: U.S. Government Printing Office, 2000.
Erikson, E.H. Children and Society. New York: Norton, 1950.
Erikson, E. The life cycle completed. New York: Norton, 1982.
Erikson, E., Erikson, J., Kivnick, H., et al. Vital involvement in old age: the experience of old age in our time. New York: WW Norton & Company, 1986.
Feldt, K. Pain assessment in older adults. In: Jansen M., ed. Managing pain in older adults. New York: Springer; 2008:35–54.
Folstein, M.F., Folstein, S., McHugh, P.R., et al. Mini-mental state: a practical method for grading cognition state of patients for the clinician. J Psychiatr Res. 1975;12:189–198.
Franklin, L., Ternestedt, B., Nordenfelt, L., et al. Views on dignity of elderly nursing home residents. Nurs Ethics. 2006;13(2):130–146.
Gallo, J.J. Handbook of geriatric assessment, ed 3. Gaithersburg, MD: Aspen, 2000.
Gavan, C.S. Successful aging families—a challenge for nurses. Holistic Nurs Pract. 2003;17(1):11–18.
Gilmer, D., Aldwin, C. Health, illness, and optimal ageing: biological and psychosocial perspectives. Thousand Oaks, CA: Sage Publications, 2003.
Gloth, F.M. Handbook of pain relief in older adults. Totowa, NJ: Humana Press, 2004.
Gonsalves, C., Pichora-Fuller, M. The effect of hearing loss and hearing aides on the use of information and communication technologies by community-living older adults. Can J Aging. 2008;27(2):145–157.
Groh, C.J., Whall, A.L. Self-esteem disturbances. In: Maas M.L., Buckwalter K.C., Hardy M.D., et al, eds. Nursing care of older adults: diagnoses, outcomes, & interventions. St. Louis: Mosby, 2001.
Heliker, D. Enhancing relationships in long-term care: through story sharing. J Gerontol Nurs. 2009;35(6):43–49.
Henderson, D.A., Gladding, S.T. Group counseling with older adults. In: DeLucia-Waack J.L., Gerrity D.A., Kalodner C.R., et al, eds. Handbook of group counseling and psychotherapy. Thousand Oaks, CA: Sage, 2004.
Hilgers, J. Comforting a confused patient. Nursing. 2003;33(1):48–50.
Ito, M., Takahashi, R., Liehr, P., et al. Heeding the behavioral message of elders with dementia in day care. Holist Nurs Pract. 2007;21(1):12–18.
Jansen, M. Common pain syndromes in older adults. In: Jansen M., ed. Managing pain in older adults. New York: Springer; 2008:17–34.
Jonsdottir, H., Jonsdottir, G., Steingrimsdottir, E., et al. Group reminiscence among people with end-stage chronic lung diseases. J Adv Nurs. 2001;35(1):79–87.
Kim, E., Buschmann, M. Touch—stress model and Alzheimer’s disease. J Gerontol Nurs. 2004;30(12):33–39.
Kleinpell, R. Supporting independence in hospitalized elders in acute care. Crit Care Nurs Clin North AM. 2007;19(3):247–252.
Kunzmann, P., Baltes, B. Wisdom-related knowledge: affective, motivational, and interpersonal correlates. Pers Soc Psychol Bull. 2003;29:1104–1119.
Lang, J., Moore, M., Harris, A., et al. Healthy aging: priorities and programs of the Centers for Disease Control and Prevention. Generations. 2005;29(2):24–29.
Le, T. Cultural values, life experiences, and wisdom. Int J Aging Hum Dev. 2008;66(4):259–281.
Mace, N.L., Rabins, P.V. The 36-hour day: a family guide to caring for people with Alzheimer’s disease, other dementias, and memory loss in later life, ed 4. Baltimore, MD: The Johns Hopkins University, 2006.
Magnusson, L., Hanson, Borg, M., et al. A literature review study of information and communication technology as a support for frail older people living at home and their family carers. Technol Disabil. 2004;16:223–235.
Maples, M.F., Abney, P. Baby boomers mature and gerontological counseling comes of age. J Couns Dev. 2006;84:3–9.
Maslow, A. Motivation and personality. New York: Harper & Row, 1954.
Mauk, K.L. Healthier aging: reaching and teaching older adults. Holist Nurs Pract. 2006;20(3):158.
Mellor, M.J., Rehr, H. Baby boomers: Can my eighties be like my fifties? New York, NY: Springer Publishing Co, Inc, 2005.
Miller, C. Communication difficulties in hospitalized older adults with dementia. Am J Nurs. 2008;108(3):58–66.
Miller, C. Nursing for wellness in older adults, ed 5. Philadelphia: Lippincott Williams & Wilkins, 2009.
Minardi, H., Hayes, N. Nursing older adults with mental health problems: therapeutic interventions—part 2. Nurs Older People. 2003;15(7):20–24.
Moody, H. Aging: concepts and controversies. Thousand Oaks, CA: Pine Forge Press, 2010.
Nakasato, Y., Carnes, B. Health promotion in older adults: promoting successful aging in primary care settings. Geriatrics. 2006;61(4):27–31.
Nerenberg, L. Elder abuse prevention: emerging trends and promising strategies. New York: Springer Publishing Co, 2008.
National Institute on Deafness and Other Communication Disorders (NIDCD). Hearing loss and older adults. Available at: www.nidcd.nih.gov/health/hearing/older.asp. [Accessed, August 16, 2010].
Ownby, R. Medication adherence and cognition: medical, personal and economic factors influence level of adherence in older adults. Geriatrics. 2006;61(2):30–35.
Pankow, L., Solotoroff, J. Biological aspects and theories of aging. In: Handbook of gerontology: evidence-based approaches to theory, practice, and policy. Hoboken NJ: John Wiley & Sons, Inc; 2007:19–56.
Penprase, B. Developing comprehensive health care for an underserved population. Geriatr Nurs. 2006;27(1):45–50.
Rabins, P.V., Lyketsos, C.G., Steele, C.D., et al. Practical dementia care, ed 2. New York: Oxford University Press, 2006.
Rowan, N., Faul, A. Substance abuse. In: Blackburn J., Dulmus C., eds. Handbook of gerontology: evidence-based approaches to theory, practice, and policy. Hoboken, NJ: John Wiley & Sons, Inc; 2007:309–332.
Rowe, J., Kahn, R. Successful aging. New York: Dell Publishing, 1998.
Scholder, J., Kagan, S., Schumann, M.J., et al. Nursing competence in aging overview. Nurs Clin North Am. 2004;39:429–442.
Sowers, K., Rowe, W. Global aging. In: Blackburn J., Dulmus C., eds. Handbook of gerontology: evidence-based approaches to theory, practice, and policy. Hoboken, NJ: John Wiley & Sons, Inc; 2007:3–15.
Strine, T.W., Chapman, D.P., Balluz, L., et al. Health-related quality of life and health behaviors by social and emotional support: their relevance to psychiatry and medicine. Soc Psychiatry Psychiatr Epidemiol. 2008;43:151–159.
Wilson, R.S., Bennet, D.A., Swartzendruber, A., et al. Age-related change in cognitive function. In: Nussbaum P.D., ed. Handbook of neuropsychology and aging. New York: Plenum Press, 1997.
Whiteside, M., Wallhagen, M., Pettengill, E., et al. Sensory impairment in older adults: part 2: vision loss. Am J Nurs. 2006;106(11):52–61.
Windsor, T., Anstey, K. Volunteering and psychological well-being among young-old adults: how much is too much. Gerontologist. 2008;48(1):59–70.
Yuhas, N., McGowan, B., Fontaine, T., et al. Interventions for disruptive symptoms of dementia. J Psychosoc Nurs. 2006;44(11):34–42.
Zisberg, A., Zysberg, L., Young, H., et al. Trait routinization, functional and cognitive status in older adults. Int J Aging Hum Dev. 2009;69(1):17–29.