Theoretical Perspectives and Contemporary Dynamics
At the end of the chapter, the reader will be able to:
1 Describe the role of nursing theory in clinical practice, education, and research.
2 Discuss the historical development of nursing theory.
3 Describe the different types and levels of nursing theory.
4 Identify relevant nursing theory frameworks used in the nurse-client relationship.
5 Identify applications of psychodynamic, developmental, and behavior concepts in nurse-client relationships.
6 Describe the use of communication theory in nursing practice.
7 Discuss contemporary social perspectives and dynamics that influence nurse-client relationships in clinical practice.
Every nurse, regardless of specialty, uses the nurse-client relationship as a fundamental means for providing safe, effective, patient-centered nursing care. The nurse-client relationship is based on an integration of scientific evidence-based practice (EBP) guidelines and values-based application of nursing principles in health care.
This chapter introduces selected theory frameworks and contemporary perspectives related to communication and the nurse-client relationship. Included in this chapter are concepts related to nursing, developmental, psychological, and communication theories. A brief introduction to changes in the health care system and contemporary issues influencing nursing practice and the nurse-client relationship is included.
Basic concepts
Monti and Tingen (2006) define discipline as “a community of interest that is organized around the accumulated knowledge of an academic or professional group” (p. 28). Nurses globally represent the largest group of health care providers and are in a unique position to have a major impact on present and future nursing practice. They can be expected to take a key role in mapping a quality health care system in which nurses will increasingly support individuals and communities in self-managing their own health. As part of a collaborative team of health care professionals, nurses are able to seamlessly and appropriately link clients with health services and health professionals at the right time, across health care settings. Electronic records and communication technologies provide nurses with capabilities and clinical supports that were not possible even a decade ago, to assist clients at entry points to an increasingly complex health care system. According to Donaldson and Crowley (1978), the discipline of nursing is concerned with the following factors:
• “Principles and laws that govern the life processes, well-being, and optimum functioning of human beings, sick or well;
• Patterning of human behavior in interaction with the environment in critical life situations; and
• Processes by which positive changes in health status are affected.” (p. 113)

Nursing theory
The fundamental knowledge base required of nurses includes human growth and development, pathophysiology, pharmacology, epidemiology, genetics, immunology, microbiology, health assessment and chronic disease management, psychology, and sociology. The theoretical foundations of nursing are drawn from philosophy, theory, research, and the practice wisdom of the profession (Smith & Liehr, 2008).
A theory represents a theorist’s thoughtful examination of a phenomenon, defined as a concrete situation, event, circumstance, or condition of interest. Theory defines the relationships among its concepts, assumptions, and propositions in a formal, systematic manner, and provides a conceptual foundation for nursing research studies (Polit & Beck, 2007).
Types of theory
Four types of theory are used in nursing practice, education, and research:
• Descriptive theory describes the properties and components of nursing as a professional discipline and explains what is important about the phenomenon.
• Explanatory theory identifies the functions of nursing and describes how the properties and components relate to each other.
• Predictive theory forecasts the relationships between the components of the model, how they occur, and what happens if an intervention is applied.
• Prescriptive theory identifies the conditions under which relationships occur and focuses on nursing therapeutics (Polit & Beck, 2007).
Historical development
Theory development is essential to maintaining the truth of any discipline (Reed & Shearer, 2007). The first nursing theorist was Florence Nightingale. She wrote the first published work on nursing theory, in which she differentiated the practice of nursing from other disciplines. She linked health with the environmental factors and offered guidelines for influencing the client’s environment to help clients heal. In her classic work Notes on Nursing, Nightingale demonstrated through medical statistics that environmental cleanliness and hand washing were major factors in preventing infection in clinical situations. An early advocate for high-quality care, Nightingale’s use of statistical data marks her as one of the first nurse researchers (Dossey et al., 2005; Kudzma, 2006).
Nursing theory development was relatively dormant until the middle of the 20th century, when nursing leaders in major universities began to describe a theoretical body of knowledge unique to professional nursing. Their graduate students provided ideas, struggled to understand the language and meaning of concepts, critiqued ideas, and developed important research studies to test the validity of nursing concepts (Fawcett, 2005).
Because nursing practice is embedded in a sociocultural context, nursing theory as a framework for practice has evolved as new information developed. Early nursing theorists, such as Virginia Henderson (1966) and Dorothy Johnson, supported the medical model, which focused primarily on identifying and modifying illness and disability. Modern nursing theorists, such as Rosemarie Parse and Betty Newman, incorporate a stronger emphasis on health promotion, client strengths, and preventive nursing strategies to facilitate health and well-being in line with today’s conceptualization of health and well-being.
Nursing’s metaparadigm
Nursing’s metaparadigm, or worldview, distinguishes the nursing profession from other disciplines and emphasizes its unique functional characteristics. Four key concepts—person, environment, health, and nursing—form the foundation for all nursing theories. Although each theorist’s theoretical interpretation differs, person, environment, health, and nursing are reflected as central constructs in all nursing theories (Marrs & Lowry, 2006). Despite major transformational changes in the health care system from a medical model to a public health model, the conceptual strength of person, environment, health, and nursing as the cornerstone of nursing theory persists.
Concept of Person: Person, defined as the recipient of nursing care, is considered from a holistic perspective as having unique biopsychosocial and spiritual dimensions. The term person is applied to individuals, family units, the community, and target populations such as the elderly or mentally ill. Personal factors “comprise features of the individual that are not part of a health condition or health states” (World Health Organization [WHO], 2001, p. 17). For example, gender, lifestyle, coping styles, habits, among others, are a part of person, to be considered in conjunction with health and environment factors. The complexity of “person” as a key concept in nursing is evidenced in the increasingly robust explanations provided by current nursing theorists (Greene, 2009). Knowledge of the client as a person—his or her preferences, perceptions, beliefs, and values—is combined with the nurse’s self-awareness as a basic understanding needed in all professional nursing relationships. This knowledge is an essential characteristic of “patient-centered care” currently identified as a central goal for the nation’s health care system (Institute of Medicine [IOM], 2001; Shaller, 2007). Preserving and protecting a client’s basic integrity and health rights as a unique individual is a unique ethical responsibility of nurse to client, whether the person is a contributing member of society, a critically ill newborn, a comatose client, or a seriously mentally ill individual. The concept of “person” supersedes health diagnosis, apart from and before a specific health care problem is considered (American Holistic Nurses Association, 2004).
Concept of Environment: Environment refers to the internal and external context of the client, as it shapes and is affected by a client’s health care situation. The WHO (2001) states, “Contextual Factors include both personal and environmental factors” (p. 8). Person and environment are so intertwined that to consider person as an isolated variable in a health care situation is impracticable. The concept of environment includes the cultural, developmental, and biopsychosocial conditions that influence a client’s perceptions or behavior. For example, poverty, education, religious or spiritual beliefs, type of community (rural or urban), family strengths and challenges, and access to resources are part of a client’s environmental context. Even climate, space, pollution, and food choices are important dimensions of environment that nurses may need to consider in choosing the most appropriate nursing interventions. Hegyvary (2007) urges nurses to “take the lead in health ecology” (p. 103). The concept of environment and health ecology becomes increasingly important as health care becomes a global enterprise and nursing responsibility.
Concept of Health: Nursing actions emphasize health and well-being. The word health derives from the word whole.Weil (2004) defines health as “a dynamic and harmonious equilibrium of all elements and forces making up and surrounding a human being” (p. 51). The concept of health exists on a continuum, and encompasses the entire life span, beginning with birth, and including palliative care and a peaceful death. Health involves individuals, families, and communities as a multidimensional concept having physical, psychological, sociocultural, developmental, and spiritual elements. Health includes disease prevention and promoting healthy lifestyle behaviors, regardless of clinical diagnosis (Morgan & Marsh, 1998).
Healthy People 2010, the health agenda for the United States for the next decade, considers quality of life as a desired outcome of health and health promotion activities. Quality of life is defined as a personal experience of subjective well-being and general satisfaction with life that includes, but is not limited to, physical health. Health is a social concern, particularly for people who do not have personal control over their health or the necessary resources to enhance their health status (Meleis, 1990). Exercise 1-1 provides an opportunity to explore the multidimensional meaning of health. Health is a cultural concern because people explain health, wellness, pathology, and treatment from the perspective of their cultural beliefs. For example, depression is explained as sadness in the Asian culture. Nurses play a major role in assessing health behaviors, and in recommending and working with individuals and families to achieve and maintain a healthy lifestyle.
Concept of Nursing: In 1956, Margaret Mead noted that nurses are invariably found wherever there is human pain and suffering. This statement has been expanded in modern times to include health promotion and disease prevention strategies designed to offset the occurrence of pain and suffering, and to minimize its effects once it has occurred. The International Council of Nursing (ICN) defines nursing as “encompassing autonomous and collaborative care of individuals of all ages, families, groups and communities, sick or well and in all settings” (ICN, 2006).
The overarching goal of all nursing activities is to empower clients by providing them with the support they need to achieve optimal health and well-being. Nursing services are designed to build on and strengthen the natural capacities of individuals, families, and communities through a continuum of services ranging from health promotion and health education, to direct care, rehabilitation, and research evaluation.
Contemporary roles associated with nursing include advanced practice, community advocacy in shaping public health policies, and leadership in nursing management and education. Health behavior changes are strongly influenced by person-centered interventions promoted through normal nurse-client relationships. Exercise 1-2 looks at professional nursing.
Levels of nursing theory
The levels of nursing theory are categorized according to their level of abstraction: grand theory, mid-range theory, and practice theory (Marrs & Lowry, 2006).
• Grand theories address the key concepts and principles of the discipline as a whole. Examples include Martha Rogers’s theory of unitary beings, Margaret Neuman’s theory of expanding consciousness, Parse’s theory of human becoming, and Dorothea Orem’s self-care deficit theory of nursing.
• Mid-range theories cover more discrete aspects of a phenomenon specific to professional nursing, exploring them in depth rather than exploring the full phenomena of nursing (Marrs & Lowry, 2006). To be classified as a mid-range theory, the concepts must be applicable to many nursing situations, easily recognized, operationalized in nursing practice, and capable of being tested (Whall, 2004). A mid-range theory can derive from a grand theory, or from inductive research methodologies such as concept analysis or grounded theory (Meleis, 2006). Examples include Peplau’s theory of interpersonal relationships and Pender’s theory of health promotion.
• Practice theories are the most limited form of nursing theory. Walker and Avant (2005) believe that practice theories should receive greater attention in guiding the direction of modern nursing. The value of practice theory lies in the development of situation-producing guidelines for EBP, based on the day-to-day experiences of professional nurses. Marrs and Lowry (2006) note that “practice theories may be as simple as a single concept that is operationalized, and may be linked to a special population or situation” (p. 47). Exercise 1-3 provides an opportunity to critique an article using nursing theory in clinical practice.
Theory as a guide to practice
Donaldson and Crowley (1978) characterize a discipline as having “a unique perspective, a distinct way of viewing all phenomena, which ultimately defines and limits the nature of its inquiry” (p. 113). Nursing theory informs nursing practice by furnishing a distinct body of nursing knowledge that nurses universally recognize as being unique to their discipline. They offer a systematic, organized way to view and interpret nursing care. In addition, concepts, drawn from multiple interdisciplinary perspectives and sources, serve as a guide for curriculum development and clinical practice.
Nursing theories provide a basis for research and a framework for understanding study results. Theoretical frameworks guide nursing research by generating hypotheses that can be supported or refuted from a theoretical perspective. When the researcher completes a study, the discussion will contain an interpretation of the findings in relation to the identified theoretical framework.
The art of nursing
Theoretical understandings do not describe variations in a client’s individual needs, perceptual or educational skills, or socioeconomic and cultural differences that require accommodations in therapeutic approach. This comes from the art of nursing, which includes caring and presence in combination with scientific applications to define nursing from a different, yet integrated perspective (Fingeld-Connett, 2008).
Integration occurs as a seamless interactive process in which nurses combine knowledge, skills, and scientific medical understandings with an individualized knowledge of the humanity of each client as a unique individual with physical, cognitive, emotional, and spiritual needs. Gramling (2004) describes the art of nursing as the “nurse’s mode of being knowing, and responding” and suggests that it represents “an attunement rather than an activity” (p. 394). It is the element of care that nurses and clients tend to remember best.
Patterns of Knowing: In her classic work, Carper (1978) describes four patterns of knowing embedded in nursing practice: empirical, personal, aesthetic, and ethical. Although the patterns of knowing are described as individual prototypes, in practice, they inform care as an integrated focus of knowledge. Together they lay the epistemological and ontological foundation of nursing practice (Zander, 2007). Holtslander (2008) notes that “this integrated, inclusive, and eclectic approach is reflective of the goals of nursing, which are to provide effective, efficient, and compassionate care while considering individuality, context, and complexity” (p. 25). The four patterns of knowing include:
• Empirical ways of knowing, which are grounded in the science of nursing. Nurses incorporate empirical ways of knowing as the basis for scientific rationales when choosing appropriate nursing interventions.
• Personal ways of knowing, which help nurses connect with and acknowledge the humanness of another. Personal knowing occurs when a nurse is able to intuitively understand and treat individual clients as unique human beings because of the nurse’s own personal experience and awareness of his or her own humanness.
• Carper equates esthetics with the art of nursing. Aesthetic ways of knowing are intangible, but they allow for creative applications in the relationship through meaningful connections with the larger environment and life experience. Esthetic ways of knowing link the art of nursing with its scientific application. An example of aesthetic ways of knowing is found in storytelling, in which the nurse seeks to understand the experience of the client’s journey through illness (Leight, 2002). Nurses can use stories to clarify or enhance a variety of themes and supplement instructions.
• Ethical ways of knowing refer to the moral aspects of nursing. Ethical ways of knowing encompass knowledge of what is right and wrong, attention to standards and codes in making moral choices, responsibility for one’s actions, and protection of the client’s autonomy and rights (Altmann, 2007). Exercise 1-4 provides an application of patterns of knowing in clinical practice.
Applications
Using nursing theory frameworks in clinical practice
Nursing theory and practice represent reciprocal interactive processes. Theory frameworks are used to guide critical thinking and actions in nursing practice; practice informs nursing theory. Different theories and nursing models provide a variety of lenses from which to approach the nursing process. This section addresses a short list of selected nursing theories with particular relevance for use with nurse-client relationships. Alligood (2010) notes a shift in the 21st century from theory development to a new era of theory applicability and utilization. Contemporary nurses will play an important role in this process.
Nursing theory and the therapeutic relationship
Hildegard Peplau’s (1952; 1997) mid-range theory of interpersonal relationships is considered an essential nursing theory framework for the study of interpersonal relationships. The model describes how the nurse-client relationship can facilitate the identification and accomplishment of therapeutic goals to enhance client and family well-being (see Chapter 5). In today’s health care environment, nurse-client relationships are of short duration, and nursing interventions have to be brief, concise, and effective. Despite the brevity of the relationship, Peplau’s basic principles of building rapport, developing a working partnership, and terminating a relationship remain relevant. Originally conceptualized as a central phenomenon in psychiatric nursing, Peplau’s framework for interpersonal relationships is applicable to all areas of nursing (McCarthy and Aquino-Russell (2009).
Holistic nursing theories focus on the meaning of a health experience and are used as guides in nurse-client relationships to help clients create a productive way of understanding and responding to difficult health situations. Exemplars include Rosemarie Parse’s (1998) theory of human becoming and Margaret Newman’s (1986) theory of expanding consciousness. Parse’s theory, which focuses on valuing a person’s health situation and quality of life from the client’s perspective, is an important consideration in developing patient-centered approaches. Newman patterned her theory of health based on Martha Rogers’s earlier theory of unitary human beings and interconnectedness with the environment. Her theory emphasizes mutual interaction between nurse and client unique to each client situation. Each therapeutic interaction is designed to move the human system toward making health choices that transcend physical limitations. Her theory is useful in helping clients with chronic illness find meaning in their situation through expanding consciousness about new possibilities for living with illness and maximizing patterns needed for health and well-being.
Caring: Caring is recognized as a hallmark of quality nursing practice and an essential concept in effective nurse-client relationships. Crowe (2000) suggests, “Caring does not involve specific tasks, instead it involves the creation of a sustained relationship with the other” (p. 966). Characteristics of professional caring, as identified by graduate nurses, include: (a) giving of self, (b) involved presence, (c) intuitive knowing and empathy, (d) supporting the patient’s integrity, and (e) professional competence (Arnold, 1997). Caring is a relationship attitude and a commitment to the well-being of clients and families, demonstrated through actions for and on behalf of them.
Caring is a primary construct in nursing theories developed by Jean Watson (1988), and Madeleine Leininger (1985; 2002). Both theorists believe caring is central to the practice of nursing. Watson’s theory promotes caring as a primary transpersonal value, and moral imperative concerned with protecting and preserving the dignity and humanity of the client. Her model describes the empathetic features of caring (Jasmine, 2009). Watson identified 10 carative factors, which are applicable to nurse client relationships (Box 1-1). These factors have, over time, evolved into a broader concept of “clinical caritas” and “caritas processes,” terms that Watson considers to be a more fluid and mature framework for nursing in the 21st century. This expanded version is identified on Jean Watson’s website: http://www.nursing.ucdenver.edu/faculty/jw_evolution.htm.
Leiniger’s theory of cultural care expands on the concept of caring within a broader cultural context. Transcultural nursing theory incorporates cultural perspectives in applying relationship and nursing process concepts to culturally diverse clients. Leininger’s sunrise diagram outlines the dimensions of cultural assessment).
Theoretical perspectives from other disciplines
Professional nursing includes concepts and theoretical perspectives from other disciplines as a foundation for practice, related to the nurse-client relationship (Villarruel, Bishop, Simpson, Jemmott, & Fawcett, 2001). Exemplar concepts from models are identified in this chapter and reintroduced in later chapters. They are not meant to be inclusive but were selected because of their relevance in implementing nurse-client relationships.
Psychodynamic models
Sigmund Freud (1937), acknowledged as the Father of Psychiatry, recognized the therapeutic value of talking about stressful life experiences as a way of reducing their impact, and problem-solving difficult life problems. Freud’s ideas about transference, defined as projecting irrational attitudes and feelings from the past onto people in the present, are useful in understanding the origin of difficult behaviors in nurse-client relationships. For example, the client who says to the young nurse, “Get me a real nurse! You’re young enough to be my daughter, and I don’t want to talk with you about my personal life,” may be having a transference reaction having little to do with the nurse’s competence. Recognizing this statement as a transference reaction helps the nurse depersonalize the client’s comment, allowing for a more appropriate response.
Transference feelings can also occur within the nurse. Unless these feelings are recognized and resolved, they can compromise the effectiveness of the therapeutic relationship. Referred to as countertransference, these feelings represent unconscious attitudes or exaggerated feelings a nurse may develop toward a client. Not all transference feelings are negative. Positive countertransferences of strong attraction, oversolicitousness, or special treatment can represent transference feelings that lead to boundary crossings or violations.
Freud was the first clinician to identify age-related sequential stages of personality development. His theory of linear psychosexual development focused on children from birth through adolescence. Failure to resolve stages of development result in immature behavioral response patterns such that the person remains “fixated” at an earlier stage of development. For example, a person experiencing little parental support in early childhood may find it difficult to trust that health providers will help.
Freud believed that people protect themselves against anxiety through the use of unconscious ego defense mechanisms (see Chapter 20). Defensive behaviors that compromise the development of a therapeutic relationship can reflect a person’s use of ego defense mechanisms.
Carl Jung: Carl Jung’s (1971) theoretical perspectives provide nurses with a basis for examining the complex dimensions of gender roles and our universal heritage as human beings. He referred to a person’s universal heritage as the collective unconscious and suggested that forces from the past continue to influence behaviors in the present. Jung characterized the first half of life as a search for self, and the second half as a search for soul. Jung’s personality theory for mid-life and beyond is relevant in helping nurses to understand and support the older adult’s shifting needs to find new inner meaning and direction in the second half of life.
Interpersonal Relationship Approaches: Harry Stack Sullivan
Harry Stack Sullivan (1953) introduced the idea of the therapeutic relationship as a human connection that heals. Hildegard Peplau (1997) credits Sullivan’s model of therapeutic relationship as a foundation for her mid range theory of interpersonal relationships in nursing practice. A corrective interpersonal experience with a helping professional can help individuals discover their strength and value through relationship.
Sullivan introduced the concept that people cannot always relate easily to a helping person and may need ongoing, compassionate, supportive encouragement to make use of the therapeutic relationship even when the helper is extremely empathetic. This is especially true for individuals experiencing shock, panic, serious mental illness, or brain damage. Further explanation of Sullivan’s theory as it relates to therapeutic relationships is presented in Chapter 5.
Psychosocial development theories
Two developmental theories, adapted from psychology, guide the study of interpersonal relationships in health care. Nurses use Erik Erikson’s (1950) theory of psychosocial development to assess developmental client needs, and to design developmentally age-appropriate nursing interventions (see Chapter 4). Erikson modified Freud’s age-related developmental stages to focus on progressive stages of psychosocial, rather than psychosexual, maturation. Erikson believed that people continue to mature throughout life. Exercise 1-5 offers an opportunity to review a person’s perception of different developmental life stages.
Different life experiences and culture—for example, the death or divorce of a parent, frequent moves, family abuse, and ethnic norms—can affect the actual timetable and expression of psychosocial development of individuals. When life crises coincide with normal developmental crises, the developmental crisis can be more difficult to resolve, for example, a diagnosis of breast cancer occurring at menopause. Table 1-1 presents the key stage development theories. Exercise 1-6 provides an opportunity to look at the influence of life circumstances on psychosocial development.
TABLE 1-1
Distinguishing Freud’s Psychosexual and Erikson’s Psychosocial Stages of Personality Development
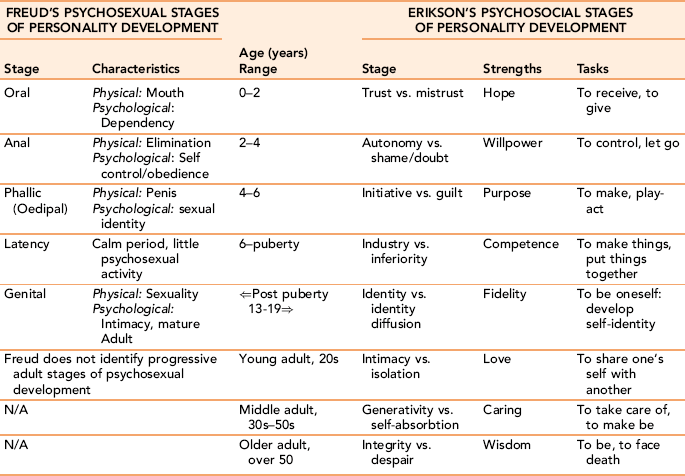
Data Source: Erikson E: Childhood and society, New York, 1950, WW Norton.Sigelma C, Rider E. Life-Span Human Development, 6th edition. Belvont CA: 2009, Wadsorth Cengage Learning.
Abraham Maslow: Nurses use Abraham Maslow’s needs theory (1970) as a framework to prioritize client needs and develop related nursing approaches. Maslow’s hierarchy of needs theory proposes that people are motivated to meet their needs in an ascending order beginning with meeting basic survival needs, moving into psychological and social spheres as essential needs are satisfied, and ending with self-actualization. Figure 1-1 illustrates Maslow’s model with associated nursing diagnoses.
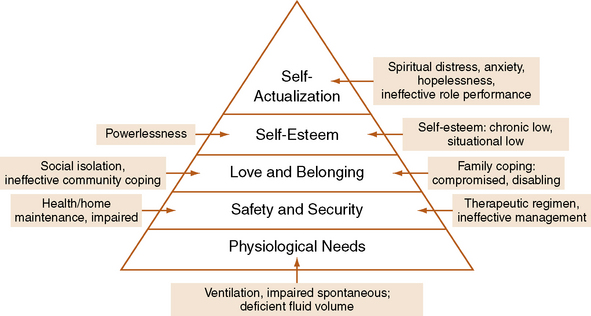
Physiologic needs required for survival are the most fundamental. Maslow referred to basic needs as “deficiency” needs, meaning that if they cannot be met, the person is at risk for survival. Basic needs include satisfying hunger, thirst, and sexual appetites, and sensory stimulation. Maslow’s second level, safety and security needs, includes physical safety and emotional security, for example, housing and freedom from abuse. Once a person meets safety and security needs, love and belonging needs, related to being a part of a family or community, become the focus. Basic need satisfaction allows for the attention to growth needs for self-esteem and self-actualization. A sense of dignity, respect, and approval by others for the self within is the hallmark of successfully meeting self-esteem needs.
Maslow’s highest level of need satisfaction, self-actualization, represents humanity at its best. Self-actualized individuals are not superhuman; they are subject to the same feelings of insecurity that all individuals experience, but they recognize and accept their vulnerability as part of the human condition. Box 1-2 presents characteristics of self-actualization. Not everyone reaches Maslow’s self-actualization stage.
Although nurses routinely use Maslow’s theory to prioritize nursing interventions, how the client and/or family prioritize health care needs is an important assessment. This consideration will enhance client cooperation, and family support will affect compliance. Exercises 1-7 and 1-8 provide practice with using Maslow’s model in clinical practice.
Person-centered models
Carl Rogers: Carl Rogers’s person-centered model forms a solid theoretical foundation for examining the current concepts of “client-centered care” as a key dimension of quality nurse-client relationships, as described in later chapters. Rogers emphasized an equal partnership between client and health care provider. He pointed to the primacy of client as the agent of healing. According to Rogers (1961), “If I can provide a certain type of relationship, the other person will discover within himself the capacity to use that relationship for growth and change, and personal development will occur” (p. 33).
Rogers identified three “helper” characteristics essential to the development of client-centered relationships: unconditional positive regard, empathetic understanding, and genuineness. He later added a fourth characteristic: a spiritual or transcendental presence as an intuitive way of being with a client (Anderson, 2001).
Rogers’s concepts of a person-centered relationship also are applicable for nurse-client health teaching formats (see Chapter 16). They have found merit as a foundation for the patient-centered health care approaches advocated by the IOM.
Aaron Beck: Concepts from Aaron Beck’s (1991) cognitive behavioral therapy (CBT) model uses a person-centered approach aimed at helping individuals troubled by faulty thinking reframe the meaning of difficult situations. Beck believed that there is a relationship between a person’s thoughts, feelings, and behaviors. By helping people become aware of and modify negative or dysfunctional thoughts, beliefs, and perceptions (cognitive distortions), it is possible for individuals to change behavior patterns, resulting in a more constructive approach to a problem situation. The focus of treatment is not on the behavior itself, but rather on the internal perceptions and thoughts that create and perpetuate self-defeating behaviors. Table 1-2 identifies irrational beliefs and common triggers.
TABLE 1-2
Irrational Beliefs and Common Triggers
| Orientation | Example | Common Triggers |
| Self | “I must do everything perfectly, and put 110% into everything I do. Otherwise, I will never be a good nurse.” | Failing a test, being criticized by a client or instructor |
| Others | “Everyone must like and respect me. No one should be angry with me. I should always be able to get what I want, when I want it. Otherwise, I am not worth much.” | Having someone cut in front of me, reject or challenge my opinions, waiting in line for services |
| World | “The world and everything in it should be predictable, and things should happen as I believe they should. Otherwise, there is no point to my doing anything.” | Elections, allocation and availability of resources, taxes, lack of equal opportunities, prejudice |
Faulty or negative thinking causes a person to interpret neutral situations in an unrealistic, exaggerated, or negative way. These automatic negative thoughts are classified as cognitive distortions. Examples include magnifying or minimizing the impact of a single behavior as being a commentary on the whole person, selective attention, mind reading, rigid rules about what a person “should” do, and so forth. Related to the concept of distortions is the concept of schema or schemata. This a term used to describe a person’s learned rules and understandings of the stimulus world, and his/her relationship to it. A core schema becomes a template for understanding the meaning of incoming information and appraising its value to the self. It is more pervasive and harder to dislodge. Although distortions seem to be legitimate assessments, they are not valid. Cognitive distortions and schemata are related to behaviors of self, others, and the world (Hale-Evans, 2006).
Nurses can teach people to challenge distortions through Socratic questioning. By gathering and weighing evidence to support a position, people are able to distinguish between a distorted perception and a realistic appraisal of its validity. Ridding oneself of unrealistic expectations and negative self-thoughts allows cognitive space for thinking about possible options and broader choices. Once a problem is appropriately categorized, the solutions become more apparent.
Communication theories
Communication theories are concerned with the transmission of information. Communication is an essential characteristic of human functioning. Through communication, we construct meaning and share it with others. Most of us take communication for granted until it is no longer a part of our lives. Communication can take place intrapersonally (within the self) or interpersonally (with others).
Intrapersonal communication takes place within the self in the form of inner thoughts and beliefs that are colored by feelings and influence behavior. Interpersonal communication is defined as a cyclic, reciprocal, interactive, and dynamic process, with value, cultural, and cognitive variables that influence its transmission and reception. Interpersonal communication has a content and a relationship dimension. The content dimension (verbal component) refers to the data. The relationship dimension (nonverbal metacommunication) helps the receiver interpret the message. People tend to pay more attention to nonverbal communication than to words when they are noncongruent with each other.
Human communication is unique. Only human beings have large vocabularies and are capable of learning new languages as a means of sharing their ideas and feelings. Communication includes language, gestures, and symbols to convey intended meaning, exchange ideas and feelings, and share significant life experiences. Basic assumptions serving as the foundation for the concept of communication are presented in Box 1-3.
Linear model
Linear models consist of three components:
• The sender is the source or initiator of the message. The sender encodes the message (i.e., puts the message into verbal or nonverbal symbols that the receiver can understand). Encoding a message appropriately requires a clear understanding of the receiver’s mental frame of reference (e.g., feelings, personal agendas, past experiences) and knowledge of its purpose or intent.
• The message consists of the transmitted verbal or nonverbal expression of thoughts and feelings. Effective messages are relevant, authentic, and expressed in understandable language.
• The receiver is the recipient of the message. Once received, the receiver decodes it (i.e., translates the message into word symbols and internally interprets its meaning to make sense of the message). An open listening attitude and suspension of judgment strengthens the possibility of accurately decoding the sender’s message. The channels of communication through which a person receives messages are the five senses: sight, hearing, taste, touch, and smell.
Circular transactional models
A circular model is a transactional model that expands linear models to include the context of the communication, feedback loops, and validation (Figure 1-2). With this model, the sender and receiver construct a mental picture of the other, which influences the message and includes perceptions of the other person’s attitude and potential reaction to the message. In this sense, transactional models reflect system theory with feedback and context added to the linear model. Communication is conceptualized as a continuous, interactive activity in which sender and receiver continuously influence each other as they converse. The human system (client) receives information from the environment (input), internally processes the information and reacts to it based on its own internal functions (throughput), and produces new information or behavior (output) as a result of the process. Feedback (from the receiver or the environment) allows the system to correct or maintain its original information.
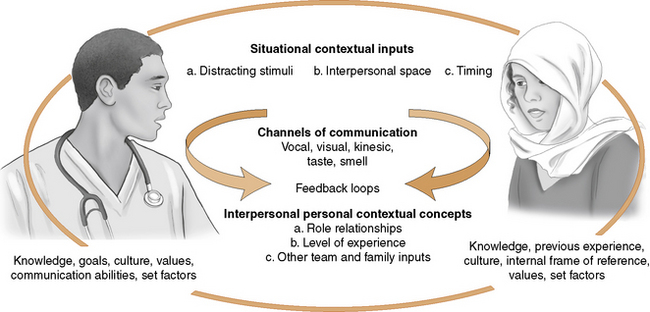
Circular models take into account the role relationships between communicators. People take either symmetric or complementary roles in communicating. Symmetric role relationships are equal, whereas complementary role relationships typically operate with one person holding a higher position than the other in the communication process. Nurses assume a complementary role of clinical expert when helping the client to achieve mutually determined health goals, and a symmetric role in working with the client as partner on developing mutually defined goals and the means to achieve them. Exercise 1-9 provides an opportunity to contrast linear versus circular models of communication.
Therapeutic communication
Therapeutic communication is a term originally coined by Ruesch (1961) to describe a goal-directed form of communication used in health care to achieve goals that promote client health and well-being. Doheny et al. (2007) observed that “when certain skills are used to facilitate communication between nurse and client in a goal directed manner, the therapeutic communication process occurs” (p. 5). Nurses use therapeutic communication skills to provide new information, correct misinformation, promote understanding of client responses to health problems, explore options for care, assist in decision making, and facilitate client well-being.
Contemporary social issues and dynamics
Theoretical frameworks sensitize nurses to perceive, think about, and act on relevant client information in a systematic way. In today’s practice environment, theory is insufficient as a guide to practice. Recognition that nursing practice is deeply embedded in the political factors, and the cultural context in which nursing is practiced is critical. Engebretson (2003) notes that cultural constructions of health and illness determine the nature of helpful provider-client interactions and influence the ways in which people make decisions and use health care services. Many factors (e.g., economics, unprecedented changes in demographics, multidisciplinary approaches to health care delivery, and advances in technology) are changing nursing’s professional landscape (Booth et al., 1997). Nurses must be knowledgeable about the contemporary societal issues and political dynamics that currently influence the conduct of the nurse-client relationship in fundamental ways. The clinical skill sets for nurses in the past need to be replaced with expanded competencies that reflect the changing health care delivery system.
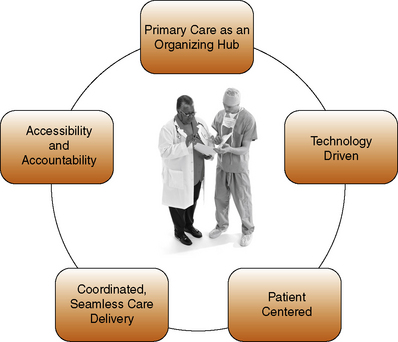
Changes in health care delivery
A key change is a shift from health care delivery provided mainly in hospitals to care delivered in primary care settings in the community. Figure 1-3 displays fundamental characteristics of contemporary health care delivery systems. Science and technology are keeping people living longer with a better quality of life than could have been imagined even a few decades ago. Clients are discharged quicker and sicker than in previous decades, partly because of capitated management of health care. Most will require additional education and support to self-manage chronic health conditions. The emphasis in health care has changed from a focus solely on service delivery to an expanded population focus on health promotion for health and well-being. People are expected to take responsibility for their own health and well-being. These changes provide the impetus for exploring nursing practice from a broader perspective.
As a result of these changes, the scope of practice and nature of work for contemporary nurses is multidimensional, multirelational, and highly complex. Managed care, the emergence of integrated interdisciplinary professional roles as the preferred model of provider service delivery, public reporting of clinical outcomes, and inclusion of client quality of life and satisfaction with care as expected clinical outcomes have revolutionized previous thinking about what needs to be included in nurse-client relationships. The length of the relationship is brief, with a focus on the client as the central person on the health care team.
Nurses practice across a wider range of clinical settings. They are expected to be multiskilled and able to function competently in a variety of health care environments. Health care relationships between clients and providers, and among interdisciplinary professional colleagues are collaborative and complementary.
Health care consumers expect more. They are better informed about their health conditions and are expected to take an active role in self-management of chronic diseases. The level of knowledge about health information on the Internet, medications, drug interactions, and health promotion/disease prevention strategies has increased exponentially.
New Professional and Consumer Roles: Nurses need to appreciate the larger number of stakeholders, including clients and families involved in health care relationships. Incorporating multiple perspectives in health care management across a continuum of care that extends into the community is the norm. Nurses are expected to have knowledge about and apply a variety of paradigms to real-life situations in clinical practice. Client roles have evolved from being passive recipients of health care into active autonomous partners, with providers involving shared authority over decision making in their treatment.
The context of the nurse-client relationship includes a broader connection with other clinicians, health care decision makers, and even occasionally policy makers. New interprofessional relationships are influencing the need for and provision of nursing services. Nurses have professional accountability, not only as a member of their profession but as members of a professional team. Instruction about interdisciplinary roles is evolving as a national curriculum thread in medical, nursing, social work, and pharmacy with combined student courses (see Chapter 7).
Demographic changes and health disparities
Health care in the United States is not equally accessible. There are glaring gaps in access to care, with many segments of a growing minority population receiving inadequate or no health care. Regulation and surveillance of quality in health care with reliance on performance measures to describe the nation’s progress has made the quality of health care more transparent and has highlighted the plight of major segments of the nation’s population (Institute of Medicine (IOM, 2003)).
Health disparities disproportionately impact the elderly, children, and minority populations. Demographic changes with a marked increase in the percentage of older adults and ethnically diverse consumers needing ongoing health care raise important ethical and medical issues.
Healthy People 2010 (U.S. Department of Health and Human Services, 2000) identifies “reducing health disparities” as a primary goal for health care. Appreciation for the rapidly increasing diversity of our society is compelling in health care, not only because of differences in health-related characteristics, but because of language, economic, and social barriers to seeking health care.
On March 23, 2010, President Obama signed an historic health care reform bill, passed by Congress. The Patient Protection and Affordable Care Act is designed to provide better health care insurance coverage for consumers of health care services. Included in the bill is health insurance for children with preexisting conditions, and access to affordable insurance for previously uninsured adults. Funding to increase the number of nurses, physicians, and other health professionals is included. Like all sweeping changes imposed by law, health care reform will take time to implement and will undergo modification as it is put into practice.
Health care reform is necessary to provide access to care and the level of health care services needed to reduce health disparities. Nurses can and should be in the forefront of helping the nation provide affordable, culturally congruent health care as an essential means of reducing health disparities.
Evidence-based practice
The IOM (2001) calls for an innovative health care system that is evidence based, patient centered, and systems oriented. Porter-O’Grady (2010) suggests that EBP represents an integration of client concerns and individual clinical applications with external evidence from clinical data and research, and best practices. The strength of the connection requires the blending of extensive clinical experience with sound clinical research and professional judgment in real-time situations with clients.
Quality nursing practice, implemented through the nurse-client relationship, is theory guided and evidence based. EBP is dynamically related to nursing theory through empirical ways of knowing. Nursing theory provides a reference framework for understanding the complex features of human responses in health care. This is a necessary, but insufficient condition for excellence. Since the late 1990s, EBP has emerged as a primary means to advance professional standards in nursing practice and to enhance the quality of care for clients (Van Achterberg, Holleman, & Van de Ven, 2006).
Sackett, Rosenberg, and Gray (1996) define EBP as “the conscientious explicit and judicious use of current best evidence in making decisions about the care of individual patients” (p. 71). Systematic review of all randomized, controlled, clinical trials and EBP guidelines based on findings and opinions of expert committees provide the strongest evidence. EBP consists of four elements:
• Best practices, derived from consensus statements developed by expert clinicians and researchers
• Evidence from scientific findings in research-based studies found in published journals
• Clinical nursing expertise of professional nurses, including knowledge of pathophysiology, pharmacology, and psychology
• Preferences and values of clients and family members (Sigma Theta Tau International, 2003)
All health care disciplines are being called on to deliver quality health care according to standardized, evidence-based guidelines that in the future will be used “to define best practices rather than to support existing practices” (Youngblut & Brooten, 2001, p. 468).
Person-centered care
Scientific guidelines need to be balanced by values-based nursing knowledge. Person-centered care is mandated as an essential characteristic of contemporary health care. Ironically, it is a value that nursing has always championed. Gottlieb and Gottlieb (1998) identify nursing values important to health care in the 21st century as caring, holism, health promotion, continuity of care, family-based care, and working in partnership with individual and community agendas (see Chapters 15 and 24).
Patterns of knowing help nurses individualize care tailored to the particular needs of each client (Mead, 2000; Fawcett, Watson, & Neuman, 2001). Issues related to making “the health care system patient centered and performance focused” include:
• “Continuous healing relationships,
• Customization as the source of control
• Shared knowledge and the free flow of information
• Safety as a system priority,
• Anticipation of patient needs rather than reacting to events” (Harris, 2001, p. 86)
In contemporary clinical practice, the client is recognized as a central person on the health care team. There is a clear assumption that clients and family will assume greater responsibility for maintaining health and well-being, as well as for primary self-management of chronic illness. Access to care, client safety, and continuity of care, health promotion, and maintenance of health represent an evolving emphasis in health care delivery. A person centered nursing framework developed by McCormack and McCance (2006) identifies environmental characteristics, pre-requisites and person centered outcomes associated with providing patient centered care.
Frist (2005) asserts that the focus of the 21st century health care system must be on the “patient, such that health care system will ensure that patients have access to the safest and highest-quality care, regardless of how much they earn, where they live, how sick they are, or the color of their skin” (p. 468). The concept of mutuality in treatment planning has been strengthened to include active involvement in shared decision making about treatment (Mead and Bower, 2000). New models of client-centered care can include shift reports in client rooms, reviewing care plans for the day early in the shift with clients, asking about their priorities, and working closely with other health team members to deliver quality care (Jasovsky, Morrow, Clementi, & Hindle, 2010).
System oriented continuity of care
Continuity of care delivered through a networked health care delivery system rather than an individualized clinical approach to health care is quickly becoming the norm in service delivery (see Chapter 24). The Pew Commission (Bellack & O’Neil, 2000) set forth 21 competencies that nurses will need to incorporate into their nursing care to be successful practitioners in the 21st century (Box 1-4). Communication skills and the development of team-based professional interpersonal relationships with clients, other professionals, and families will be key to achieving and integrating these competencies in health care delivery.
Advances in technology
Advances in technology have revolutionized health care delivery, documentation, and availability of medical information. With technology, communication is possible to any location at any time. Malloch (2010) notes, “What has not changed is the need for effective personal relationships in the evaluation and selection of new technologies; human to human sensitivity, acknowledgment, and respect for the patient care experience” (p. 1).
Nurses increasingly face the challenge of being present in relationships to clients and other health professionals in a digital age dominated by technology. Technologic advances such as the electronic house call, Internet support groups, and the virtual health examination are still in their infancy but may well take the place of office visits and become a major health care resource in the future, particularly in remote areas (Kinsella, 2003). Telehealth is fast becoming an integral part of the health care system, used both as a live interactive mechanism (particularly in remote areas, where there is a scarcity of health care providers) and as a way to track clinical data. Two important outcomes are reduction of health costs and access to care (Peck, 2005).

Telehealth technologies allow nurses a new level of interaction with clients and other health providers.
The Internet serves as a vital source of health information for consumers and health care providers, instantly linking them with current scientific and medical breakthroughs in diagnosis and treatment. Sophisticated technology allows health experts in geographically distant areas throughout the world to share information and to draw important conclusions about health care issues in real time. New technologies have the capacity to bring highly trained specialists into the home through the Internet and teleconferencing. Clark (2000) describes a “virtual” application of technology from the perspective of a Canadian nurse caring for a client in a remote area as it might occur in the year 2020.
Positioning Nurses as Key Players: Nursing has had a long and honorable commitment to providing care for poor, marginalized, and vulnerable populations, consistent with the goal of reducing health disparities. Table 1-3 identifies seven conditions and their evolutionary correlates needed to secure a key player role for nurses in the new health care delivery system.
TABLE 1-3
Criteria for Survival of the Nursing Profession Based on Evolutionary Principles
| Criteria or Condition | Evolutionary Principle |
| Nursing needs to be relevant. | In nature, an organism will survive only if it occupies a niche, that is, performs a specific role that is needed in its environment. |
| Nursing must be accountable. | In every environment there is a limited amount of resources. Organisms that are more efficient and use the available resources more effectively are much more likely to be selected by the environment. |
| Nursing needs to retain its uniqueness while functioning in a multidisciplinary setting. | In nature, an organism will survive only if it is unique. If it ceases to be so, it is in danger of losing its niche or role in the environment. In other words, it might lose out if the new species is slightly better adapted to the role, or if physically similar enough, it might even breed with that species and thus completely lose its identity. Successful organisms must also learn to coexist with many different species so that their role complements that of the other organisms. |
| Nursing needs to be visible. | In nature, organisms often are required to defend their niche and their territory usually by an outward display that allows other similar species to be aware of their presence. By being “visible,” similar species can avoid direct conflict. In addition, visibility is also important for recognition by members of their own species, to allow for the formation of family and social units, based on cooperation and respect. |
| Nursing needs to have a global impact. | In nature, if a species is to survive, it must make its presence felt not just to its immediate neighbors but to all the members of its environment. Often, this results in a species adapting a unique presence, whether it is a color pattern, smell, or sound. |
| Nurses need to be innovators. | In evolution, the organisms that survive are, more often than not, innovators that have the flexibility to come up with new and different solutions to rapid changes in environmental conditions. |
| Nurses need to be both exceptionally competent and strive for excellence. | During evolution, when new niches open up, it is never possible for more than one species to occupy one niche. Only the best adapted and most competent among the competing organisms will survive; all others, even if only slightly less competent, will die. |
From Bell (1997) as cited in Gottlieb L, Gottlieb B: Evolutionary principles can guide nursing’s future development, Journal of Advanced Nursing 28(5):1099, 1998.
Summary
This chapter presents theoretical concepts important to the understanding of the nurse-client relationship. These models bring order to nursing practice, and provide a cognitive structure for developing a body of knowledge for professional nursing and a theoretical basis for nursing research. Four theoretical concepts found in all nursing theories are person, health, nursing, and environment. The art of nursing helps nurses integrate scientific understandings with a personalized approach to individual clients.
Hildegard Peplau’s theory of interpersonal relationships form the theoretical basis for understanding the nurse’s role in the nurse-client relationship. Concepts from other developmental and psychological theories broaden the nurse’s perspective and understanding of client behaviors. Nurses use Erikson’s model of psychosocial development to provide nursing care in line with developmental needs of their clients and Maslow’s need theory to prioritize care activities. Carl Rogers offered basic concepts concerning the characteristics the nurse needs for developing effective interpersonal relationships with clients. Therapeutic communication is used in the nurse-client relationship as a primary means of achieving treatment goals.
Changes in the health care delivery system require nurses to embrace new skill sets consistent with contemporary health care changes. What nurses bring to the table, the essential values of professional nursing practice—caring relationships with clients, a holistic view of persons, a wide range of scientific and value-based knowledge combined with critical thinking and clinical reasoning skills—remain unchanged. Nurses have an unprecedented opportunity to make a difference and shape the future of nursing practice through communication at every level in health care delivery.
References
Alligood, M. Nursing Theory: Utilization and Application, ed 4. Maryland Heights, MO: Mosby Elsevier, 2010.
Altmann, T. An evaluation of the seminal work of Patricia Benner: theory or philosophy? Contemp Nurs. 2007;25:114–123.
American Holistic Nurses Association What is holistic nursing?, 2004. Available online:, http://www.ahna.org/about/whatis.html.
Anderson, H. Postmodern collaborative and person-centered therapies: what would Carl Rogers say? Journal of Family Therapy. 2001;23:339–360.
Arnold, E. Caring from the graduate student perspective. International Journal of Human Caring. 1997;1(3):32–42.
Awa, M., Yamashita, M. Persons’ experience of HIV/AIDS in Japan: application of Margaret Newman’s theory. Int Nurs Rev. 2008;55:454–461.
Bateson, G. Mind and nature. New York: Dutton, 1979.
Beck, A.T. Cognitive therapy and the emotional disorders. London: Penguin Books, 1991.
Bell, G. Selection: The Mechanism of Evolution. New York: Chapman & Hall, 1997.
Bellack, J., O’Neil, E. Recreating nursing practice for a new century: recommendations and implications of the Pew Health Professions Commission’s final report. Nurs Health Care Perspect. 2000;21(1):14–21.
Booth, K., Kenrick, M., Woods, S. Nursing knowledge, theory and method revisited. J Adv Nurs. 1997;26(4):804–811.
Carper, B. Fundamental patterns of knowing in nursing. ANS Adv Nurs Sci. 1978;1:13–23.
Clark, D.J. Old wine in new bottles: delivering nursing in the 21st century. J Nurs Scholarsh. 2000;32(1):11–15.
Crowe, M. The nurse-patient relationship: a consideration of its discursive content. J Adv Nurs. 2000;31(4):962–967.
Doheny, M., Cook, C., Stopper, M. The discipline of nursing. Stamford, CT: Appleton & Lange, 2007.
Donaldson, S.K., Crowley, D.M. The discipline of nursing. Nurs Outlook. 1978;26:113–120.
Dossey, B., Selander, L., Beck, D., et al. Florence Nightingale today: healing, leadership, global action. Silver Spring, MD: American Nurses Association, 2005.
Engebretson, J. Cultural constructions of health and illness: recent cultural changes toward a holistic approach. J Holist Nurs. 2003;21(3):203–227.
Erikson, E. Childhood and society. New York: WW Norton, 1950.
Fawcett, J. Contemporary nursing knowledge: Analysis and evaluation of nursing models and theories, ed 2. Philadelphia: Davis, 2005.
Fawcett, J., Watson, J., Neuman, B., et al. On nursing theory and evidence. J Nurs Scholarsh. 2001;33(2):115–119.
Fingeld-Connett, D. Qualitative convergence of three nursing concepts: art of nursing, presence and caring. J Adv Nurs. 2008;63(5):527–534.
Freud, S. The basic writings of Sigmund Freud. New York: Modern Library; 1937. [(Brill AA, translator)].
Frist, W. Health care in the 21st century. N Engl J Med. 2005;352:267–272.
Gottlieb, L., Gottlieb, B. Evolutionary principles can guide nursing’s future development. J Adv Nurs. 1998;28(5):1099–1105.
Gramling, K. A narrative study of nursing art in critical care. J Holist Nurs. 2004;22(4):379–398.
Greene, C. A comprehensive theory of the human person from philosophy and nursing. Nurs Philos. 2009;10(4):263–274.
Hale-Evans, R. Mind performance hacks. Seastopol, CA: O’Reilly Media, Inc, 2006.
Harris, J. Shaping the system and culture of health care. Dermatol Nurs. 2001;13(2):86.
Hegyvary, S. An agenda for nursing as a means to improve health. J Nurs Scholarsh. 2007;39(2):103–104.
Henderson, V. The nature of nursing. New York: Macmillan, 1966.
Holtslander, L. Patterns of knowing hope: Carper’s fundamental patterns as a guide for hope research with bereaved palliative care givers. Nurs Outlook. 2008;56(4):25–30.
Institute of Medicine (IOM). Unequal treatment: confronting racial and ethnic disparities in health care. Washington, D.C.: National Academies Press, 2003.
Institute of Medicine (IOM). Crossing the quality chasm: a new health system for the 21st century. Washington, D.C.: National Academies Press, 2001.
International Council of Nurses The ICN definition of nursing, 2006. [International Council of Nurses website]. 2006. Available online:, http://www.icn.ch/definition.htm.
Jasmine, T. Art, science or both? Keeping the care in nursing. Nurs Clin North Am. 2009;44(4):415–421.
Jasovsky, D., Morrow, M., Clementi, P., et al. Theories in action and how nursing practice changed. Nurs Sci Q. 2010;23(1):29–38.
Jung, C.G. The stages of life. In: Campbell J., ed. The portable Jung. New York: Viking, 1971.
Kinsella, A., Telemedicine connection. Advance for Providers of Post-Acute Care, 2003;May-June:24–26.
Kudzma, E. Florence Nightingale and health care reform. Nurs Sci Q. 2006;19(1):61–64.
Leininger, M. Transcultural care diversity and university: a theory of nursing. Thorofare, NJ: Charles B. Slack, 1985.
Leininger, M. Transcultural Nursing: Concepts, Theories, Research, and Practice, ed 3. New York: McGraw Hill, 2002.
Leight, S. Starry night: using story to inform aesthetic knowing in women’s health nursing. J Adv Nurs. 2002;37(1):108–114.
Malloch, K. Innovation leadership: new perspectives for new work. Nurs Clin North Am. 2010;45(1):1–9.
Marrs, J., Lowry, L. Nursing theory and practice: connecting the dots. Nurs Sci Q. 2006;19(1):44–50.
Maslow, A. Motivation and personality, ed 2. New York: Harper & Row, 1970.
McCarthy, C., Aquino-Russell, C. A comparison of two nursing theories in practice: Peplau and Parse. Nurs Sci Q. 2009;22(1):34–40.
McCormack, B., McCance, T. Development of a framework for person centred nursing. J Adv Nurs. 2006;56(5):472–479.
Mead, N., Bower, P. Patient centredness: a conceptual framework and review of the empirical literature. Soc Sci Med. 2000;51:1087–1110.
Mead, P. Clinical guidelines: Promoting clinical effectiveness or a professional minefield? J Adv Nurs. 2000;31(1):110–116.
Meleis, A. Being and becoming healthy: the core of nursing knowledge. Nurs Sci Q. 1990;3(3):107–114.
Meleis, A. Theoretical nursing: development and progress, ed 4. Philadelphia: Lippincott, 2006.
Monti, E., Tingen, M. Multiple paradigms of nursing science. In Cody W., ed.: Philosophical and theoretical perspectives for advanced practice nursing, ed 4, Sudbury, MA: Jones and Bartlett Publishers, 2006.
Morgan, I., Marsh, G. Historic and future health promotion contexts for nursing. Image J Nurs Sch. 1998;30(4):379–383.
Newman, M. Health as expanding consciousness. St. Louis MO: Mosby, 1986.
Parse, R.R. The human becoming school of thought. Thousand Oaks, CA: Sage Publications, 1998.
Peck, A. Changing the face of standard nursing practice through telehealth and telenursing. Nurs Adm Q. 2005;29(4):339–343.
Peplau, H. Interpersonal relations in nursing. New York: Putnam, 1952.
Peplau, H. Peplau’s theory of interpersonal relations. Nurs Sci Q. 1997;10(4):162–167.
Polit, D., Beck, C. Nursing research: generating and assessing evidence for nursing practice, ed 8. Philadelphia: Lippincott Williams & Wilkins, 2007.
Porter-O’Grady, T. A new age for practice: creating the framework for evidence. In: Malloch K., Porter-O’Grady T., eds. Introduction to evidence-based practice in nursing and health care. ed 2. Sudbury, MA: Jones and Bartlett Publishers; 2010:1–29.
Reed, P., Shearer, N. Perspectives on nursing theory. Philadelphia: Lippincott, 2007.
Rogers, C. On becoming a person. Boston: Houghton Mifflin, 1961.
Ruesch, J. Therapeutic communication. New York: Norton, 1961.
Sackett, D., Rosenberg, W., Gray, J., et al. Evidence based medicine: what it is and what it isn’t. Br Med J. 1996;312(7023):71–72.
Shaller, D., October. Patient-centered care: what does it take? The Commonwealth Fund, 2007. Available online:, http://www.commonwealthfund.org/Content/Publications/Fund-Reports/2007/Oct/Patient-Centered-Care--What-Does-It-Take.aspx. [Accessed December 18, 2009].
Sibbald, B. 2020 vision. Can Nurse. 1995;91(3):3.
Sigelma, C., Rider, E. Life-Span Human Development, ed 6, Belvont CA: Wadsorth Cengage Learning, 2009.
Sigma Theta Tau International Sigma Theta Tau International’s position statement on evidence-based nursing, 2003. [Sigma Theta Tau International’s website]. 2003. Available online:, http://www.nursingsociety.org.
Smith, M.J., Liehr, P. Theory-guided translation: emphasizing human connection. Arch Psychiatr Nurs. 2008;22(3):175–176.
Sullivan, H.S. The interpersonal theory of psychiatry. New York: Norton, 1953.
United States Department of Health and Human Services. Healthy people 2010. McLean, VA: International Medical Publishing, 2000.
Van Achterberg, T., Holleman, G., Van de Ven, M., et al. Promoting evidence-based practice: the roles and activities of professional nurses’ associations. J Adv Nurs. 2006;53(5):605–612.
Villarruel, A.M., Bishop, T.L., Simpson, E.M., et al. Borrowed theories, shared theories, and the advancement of nursing knowledge. Nurs Sci Q. 2001;14(2):158–163.
Walker, L., Avant, K. Strategies for theory construction in nursing, ed 4. Upper Saddle River, NJ: Pearson Prentice Hall, 2005.
Watzlawick, P., Beavin-Bavelas, J., Jackson, D. Some tentative axioms of communication. In: Pragmatics of Human Communication—A Study of Interactional Patterns, Pathologies and Paradoxes. New York: W. W. Norton; 1967.
Watson, J. Nursing: human science and human care: a theory of nursing. New York: National League for Nursing, 1988.
Weil, A. Health and healing. New York: Houghton Mifflin, 2004.
Whall, A. The structure of nursing knowledge: analysis and evaluation of practice, middle-range and grand theory. In Fitzpatrick J., Whall A., eds.: Conceptual models of nursing: analysis and application, ed 4, Stamford, CT: Appleton & Lange, 2004.
World Health Organization (WHO). International classification of functioning, disability and health. Geneva: WHO, 2001.
Youngblut, J., Brooten, D. Evidence-based nursing practice: why is it important? AACN Clin Issues. 2001;12(4):468–476.
Zander, P. Ways of knowing in nursing: the historical evolution of a concept. Journal of Theory Construction & Testing. 2007;11(1):7–11.