CHAPTER 2 Sports massage
Massage is one of the original core skills of physiotherapy (Copestake, 1917), which unfortunately fell from popularity because of the belief that it was ‘unscientific’. Thankfully, massage is making a re-emergence in the more fashionable guise of ‘sports massage’, both within physiotherapy and through the development of specialist massage therapists. A variety of massage types are commonly used, and a taxonomy of massage terminology by Dixon et al. (2007) described four main categories (Table 2.1).
Relaxation massage aims to create a feeling of wellness by moving body fluids (especially blood and lymph). This massage category includes both classical Swedish massage and Sports massage and is applied on healthy subjects. Traditional techniques in this grouping are highlighted in Table 2.2. Clinical massage may use these same techniques, but is applied to a pathological region of the body. Additional procedures such as trigger point release are often used to target pain. In clinical massage there may be considerable overlap with manual therapy which may be applied either to soft tissues (clinical massage) or joints (mobilization and manipulation). Movement re-education involves both massage and non-massage techniques. Where techniques such as Pilates, Alexander technique and Feldenkrais are used these are hands off procedures categorized as exercise therapy. Movement re-education using hands on techniques include tablework where the clinician assists or resists movement using proprioceptive neuromuscular facilitation (PNF) or MET (MET). These procedures may be preceded by relaxation massage to normalize muscle tone. Energy work capitalizes on the interaction between therapist and patient which always occurs during treatment. Now however the emphasis is to move blocked energy or ‘life force’ which is thought to flow within the body. In Chinese medicine this energy is Qi, in Ayerveda it is Prana. Massage in this category includes contact techniques such as Acupressure and Shiatsu and non-contact techniques such as Reiki and Healing.
| Effleurage |
| Unidirectional stroking movement travelling proximally |
| Petrissage |
| Soft tissue compression including kneading, picking up, wringing, rolling and shaking |
| Frictions |
| Small, deep circular or transverse movements at specific anatomical sites |
| Tapotement |
| Percussive actions including clapping, hacking, beating, tapping, shaking and vibration |
Massage techniques
Effleurage
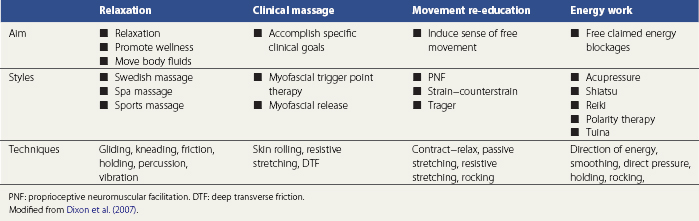
Two types of effleurage are used (Fig. 2.1). The first is a superficial stroking movement designed to produce a sensory reaction, either of relaxation (slow stroking) or stimulation (fast stroking). The second is a deep action aimed at assisting lymphatic and venous drainage. The tissue manipulation starts distally and proceeds proximally in the direction of the heart, for example, ‘knee to groin’ or ‘elbow to axilla’. The proximal portion of the limb is treated first to clear lymphatic and venous congestion. This will allow the tissue fluids mobilized by the distal massage to move against less restriction.
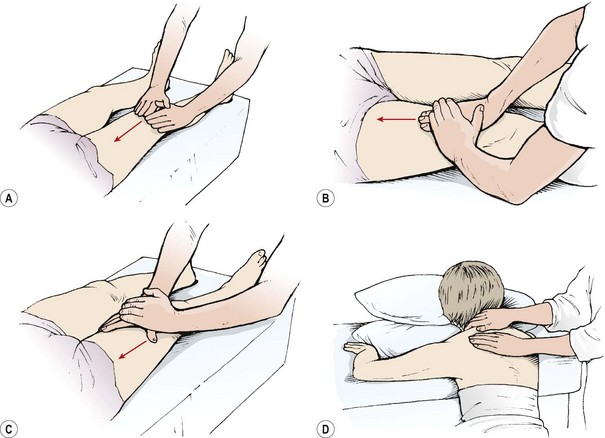
Figure 2.1 Effleurage. (A) Both hands cover the surface of the limb. (B) Reinforced hand for deeper pressure. (C) Thumb web used to contour limb. (D) Superficial stroking—the flat hands or fingertips are pulled towards the therapist.
Keypoint
Where deep stroking (effeurage) is used to assist lymphatic flow, the massage direction is from distal to proximal, towards the heart.
The therapist uses the hands either together or separately with one supporting the other to create more force. Skin contact is maintained throughout the action, and as they move, the hands change shape to contour the limb. Contouring the hand in this way helps to relax the hand muscles. The whole of the hand and not just the leading edge should apply the pressure, to avoid sticking or jerking. In addition the hand should remain relaxed and not grip hard.
The force for the movement should come from overall body motion and not simply arm strength. The therapist adopts a stance with one foot in front of the other (walk standing) and transfers his or her weight from the rear to the front foot. The arms and hands transmit, rather than create, the force. At the beginning of the action the elbows will be bent, and at the end, full reach is achieved by straightening the arms. At this end-point a slight overpressure is applied and the movement pauses before being repeated.
Keypoint
The hands are used to transmit force created by the legs and trunk. The hands should not create force themselves.
Some therapists prefer to maintain skin contact with a light stroking action as the hand is returned to the starting position. The advantage of this technique is that the movement is continuous, but the disadvantage is that sometimes the light pressure can be uncomfortable to a ticklish subject.
A light effleurage movement may be used to begin massage, to spread oil and acclimatize the athlete to massage and assist in relaxation. In addition, the lightness of the touch helps the practitioner to feel altered areas of tissue tension which may be focused on later. As effleurage proceeds, the depth of the movement can increase, developing the superficial stroking action into deep longitudinal pressure.
Petrissage
Various petrissage movements are used (Fig. 2.2). In each case the hands maintain contact with the skin and do not glide over the skin surface except when progressing from one area to another.
Frictional massage
With frictions, only the therapist’s fingers or thumbs are used to give an accurate, deep, soft tissue manipulation (Fig. 2.4). The fingers should be held locked but not hyperextended. With small areas, the first and second fingers are used overlapping as one unit. Larger areas may require the use of all of the fingertips of one hand reinforced by the other hand. The friction may either be circular or transverse.
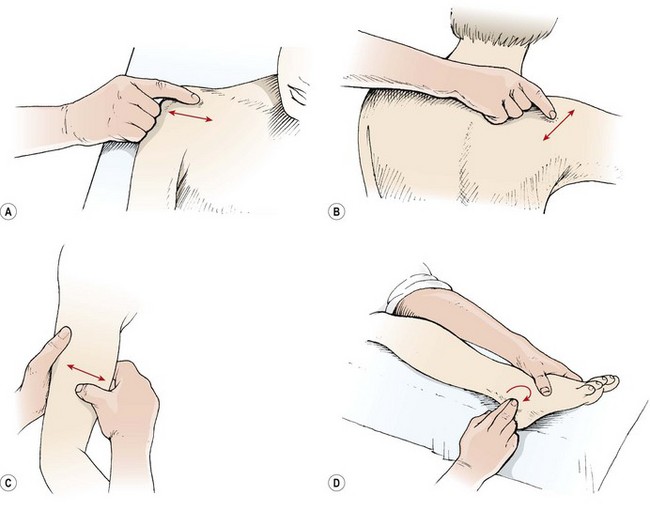
Figure 2.4 Frictional massage. (A) Deep transverse friction—single finger. (B) Reinforced finger. (C) Transverse friction of muscle belly. (D) Circular friction to break up oedema.
Circular frictions are normally used to break up thickened oedema, particularly around a joint. Three or four circular actions are used, gradually increasing in depth depending on patient tolerance. Pressure is released and the hand moved to another position before the friction is resumed.
Deep transverse frictions
Deep transverse frictional massage (DTF) is a specific manipulation technique pioneered by Cyriax (1941). The aim of the technique (Table 2.3) is to move the tissues with a view to improving function, and to induce hyperaemia and pain relief (Kesson and Atkins, 1998). DTF involves a transverse sweeping movement of the connective tissues which aims to discourage cross-link formation between collagen fibres. By applying shear and gliding movements in this way, tensile strength of the healing scar may be improved and adhesions reduced. Gentle DTF applied in the acute phase of healing could increase the rate of phagocytosis by inducing agitation of tissue fluid. In the chronic stage of healing, the therapeutic movement produced by DTF is said to soften and mobilize adhesions (Kesson and Atkins, 1998) in preparation for later tissue mobilization.
Table 2.3 Aims of deep transverse frictions (DTF)
Hyperaemia may be produced by DTF in the underlying tissues. Clinically, a red, raised area is seen on the skin as the technique is applied, and it is assumed that the same increase in regional blood flow occurs in the underlying tissues (Winter, 1968). The potential increase in the inflammatory response is required in chronic lesions but not in acute lesions. For this reason DTF, if used in the acute phase of injury, must be gentle and given over a shorter period to avoid hyperaemia production.
Treatment note 2.1 Saving your hands
Massage and manual therapy are powerful techniques; however, by their very nature they can cause considerable stress to the therapist’s hands. One study has shown that manual therapists are 3.5 times more likely to develop pain in the wrists and hands compared to non-manual therapists (Bork et al., 1996). Another study showed that therapists who used manual therapy were 7.7 times more likely to develop thumb pain and 4.0 times more likely to report wrist pain. Clearly this is an ‘at risk’ area and anything which can be done to reduce this risk is important.
Hyperextending finger joints
Many people have hyperextending finger joints (Fig. 2.5), meaning that, as they place pressure with the pad of their finger or thumb, the terminal digit is unstable and the joint extends further than normal, stressing both the ligaments and the muscles in the finger. In order to prevent this, both deep transverse frictional massage and joint mobilization techniques should be carried out with other parts of the hand.


Mobilization procedures can be carried out using the pisiform bone of the hand (Fig. 2.6). This small bone has approximately the same area as the thumb, and pressure can be placed through the straight wrist and carpal bones directly onto the pisiform itself. Where this area is too large, a plunger (Fig. 2.7) can be used. These come with a variety of different sized heads to correspond to different treatment areas.



For transverse frictional massage, the elbow may be used on large joints (Fig. 2.8). Because the elbow has a tendency to slip, it should be supported using the web of the finger and thumb of the opposite hand. Where direct digital pressure is needed over a period of time, for example deactivating trigger points deep within a muscle, a ‘knobber’ is useful (Fig. 2.9). This is a plastic device with a variety of different shaped balls on the end which can be used for greater or lesser pressure. These can be easily held in the hand to provide direct pressure to the trigger point. As an alternative, either a single knuckle or two knuckles may be used to provide greater or lesser pressure (Fig. 2.10).




Strain on the flexed wrist
Tendons around the wrist can become inflamed if the wrist is held in a flexed or adducted position for a long time. Where joint distraction movements are used (Fig. 2.11) it is important to pull through a straight angle of the wrist with the carpals and radius and ulna in line rather than flexed. This will ensure that the tendon sheath is not stretched and therefore compressed against the tendon itself. In addition, when using the thumb for manual therapy, again it is important that the wrist is in its neutral position and you avoid stretching the thumb tendons over the radial styloid.
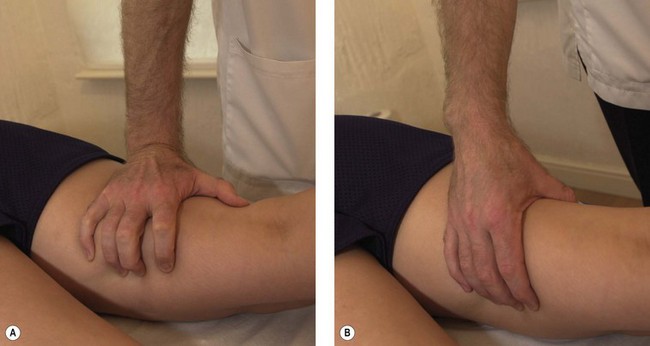
Figure 2.11 Avoiding stress on the wrist and hand. (A) Poor wrist and hand alignment. (B) Corrected.
As a general guide, the practitioner’s elbow should be kept tucked into the side of the body, the wrist should be in line with the radius and ulna, and the finger tendons should be as relaxed as possible. In addition, exercises to warm up the hands and fingers should be performed before starting clinic sessions, aiming to take the wrist and finger joints to their full range of motion in each direction, maintaining the stretch position for 20–30 seconds.
The pain reduction seen with DTF may result from the massage acting as a noxious stimulus (counter-irritant) through mechanoreceptor activity. This would explain why DTF used aggressively gives better pain reduction than DTF given lightly, as the more aggressive approach will cause greater mechanoreceptor stimulation, which has been shown to increase pain suppression (Bowsher, 1988). Pain relief seen clinically is often fairly long-lasting, and a study by de Bruijn (1984) showed pain relief for up to 48 hours following DTF of 5 minutes maximum.
Restoration of function is often the most striking effect of DTF. On reassessment, range of motion is usually significantly increased and muscle contraction more easily performed. Kelly (1997) confirmed this in a study looking at 46 subjects who showed an increase in force of muscle contraction and an increased range of dorsiflexion after DTF of the gastrocnemius muscle.
DTF technique
DTF is performed with the skin of the patient and the finger(s) of the therapist acting as a single unit. A number of hand positions may be used to maximize the force applied to the tissues but minimize the stress imposed on the practitioner’s hands (Fig. 2.12). The action demands great anatomical accuracy and must be of sufficient depth and sweep to affect the desired tissues. The point at which the DTF is applied corresponds to the lesion in the tissues rather than the painful point, as pain is often referred away from the original site of injury.
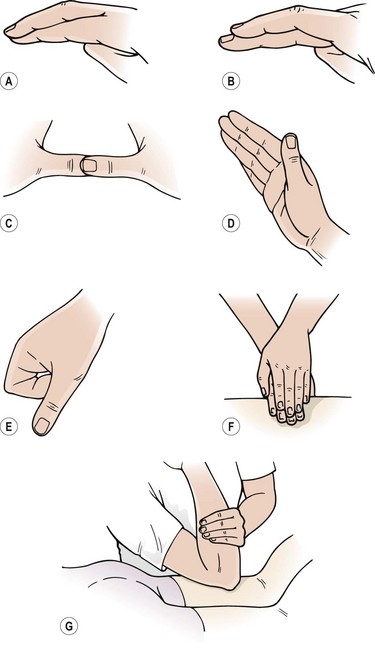
Figure 2.12 Hand positions for deep transverse frictions (DTF). Modified from Kesson and Atkins (1998). (A) Single finger. (B) Reinforced finger. (C) Reinforced thumb. (D) Knife edge of the hand. (E) Single knuckle. (F) Reinforced finger pads. (G) Elbow.
Keypoint
With DTF the practitioner’s fingers and the patient’s skin move as one unit. The fingers must not glide over the skin surface.
Tendons are generally frictioned in a stretched position, with the lesion often lying at the teno-osseous junction. Tendons in a sheath are again placed on stretch with the aim of rolling the sheath around the tendon as the DTF is given. Muscles are treated in relaxed inner range, to facilitate broadening and separation of the muscle fibres in an imitation of normal function. Ligaments are placed under slight stretch to allow the practitioner’s fingers access to the lesion.
Tapotement
The percussive movements may be used to stimulate, or for evacuation of a hollow cavity. Percussion for evacuation, such as that used in chest physiotherapy, is not within the context of this book.
For stimulating tapotement the hands are relaxed, and follow each other in a succession of alternating movements. With clapping, the wrists are flail and the cupped hand strikes the body creating a hollow (rather than slapping) sound. Hacking involves striking the skin with either the ulnar border of the hand (severe) or the back of the tips of the fingers by using a pronation/supination movement of the forearm (mild). Beating or pounding is performed with the ulnar border of the semi-closed fist and tapping with the fingertips. The percussion techniques are used over bulky muscle areas but must avoid bony areas (spine of the scapula, patella) as these will be painful if struck (Fig. 2.13).
Massage medium
Massage can require both slip (lubrication) and grip (friction), depending on the particular technique being performed. Grip media include talc or corn starch, while lubricants may be oils, creams or lotions. Where one technique progresses on to another, practitioners may often find themselves wanting one medium while using another. The functions of grip and slip media are shown in Table 2.4. It must be noted, when using oil, that patients may be allergic to nuts and suffer anaphylactic shock. Peanuts are the most common nut allergen with approximately 1 in 500 of the population affected (Demain, 1996). Traditionally used arachis oil is derived from peanuts, and oils such as almond are obviously nut based.
Table 2.4 Function of media used in massage
| Lubricant (slip) | Friction medium (grip) |
|---|---|
Sources Holey and Cook (1997) and Kesson and Atkins (1998) with permission.
Definition
Anaphylactic shock can present as respiratory distress, hypotension, oedema, rash, tachycardia, pale clammy skin and sometimes convulsions and cyanosis. It can be life-threatening if oedema affects the larynx as airflow is obstructed.
Vegetable oils are absorbed into the skin, whereas mineral oils remain on the skin surface to create a ‘sheen’ or skin gloss. Vegetable oils may therefore be used as carriers for essential oils and can have a nutrient effect on the skin. Mineral oils, because they remain on the skin surface, maintain their lubrication properties and last longer. Some vegetable oils may be thick and viscous, feeling tacky to the touch. In addition, vegetable oils have a shorter shelf-life and will go rancid (oxidize) when exposed to the air.
Practical application of techniques
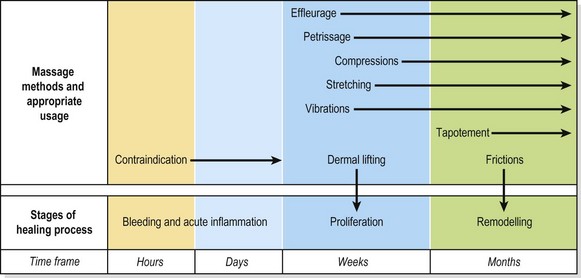
Sports massage is generally used on healthy (non-injured) subjects. Clinical massage is contraindicated during the bleeding phase and early proliferation phase of healing, between 48 and 72 hours after injury. During the proliferative stage of healing light superficial effleurage and petrissage may be used. As healing progresses these techniques may become deeper and firmer with the addition of compression and stretching procedures. In the remodelling phase soft tissue manipulations such as deep transverse frictions may be used, and where trigger points exist as part of muscle spasm these can be released by direct pressure. Where fluid stasis exists through chronic healing, more vigorous procedures such as tapotement may be used prior to exercise therapy or movement re-education. Figure 2.14 provides a summary of massage techniques at different stages of healing.
Prior to the commencement of treatment a full medical history is taken and physical assessment carried out. A skin inspection must be performed. Cuts are either protected by waterproof taping, or the practitioner must wear protective gloves. Where a skin lesion is large, massage should not proceed directly over the area.
The lower limb
Posterior thigh
Massage to the posterior aspect of the leg begins with the athlete lying prone with the knee slightly flexed to take the stretch off the popliteal structures. The shin is supported by a rolled towel. A towel is placed over both legs, and folded back to reveal the leg to be massaged. The towel covers the leg again to maintain body heat once leg massage has finished, and the other leg is uncovered and massaged in turn. Where swelling is the main concern, the massage procedures begin in the upper leg to clear the lymphatic vessels here before fluid is pushed into them by lower leg massage. Effleurage begins the movement. A small amount of gel or cream is placed on the practitioner’s hand and warmed, through friction, before application.
Where increased muscle tone is detected, muscle shaking is used to aid relaxation. The palm may be placed across the fibres of the muscle with the shaking movement perpendicular to the leg (transverse shaking). Alternatively, with a smaller limb, the hand may grip the muscle belly with the fingers parallel to the muscle fibres (longitudinal shaking). The palm contact for the shaking procedure causes the whole muscle to vibrate, and the effect is general. Where a more local effect is required, the fingertips are used, rather than the palm, in a ‘claw hand’ contact for local vibration. The action is now directed downwards into the depth of the muscle rather than along its length.
The effleurage stroke begins over the popliteal fossa and proceeds up the centre of the thigh to the buttock crease. The second stroke is medial, and the third stroke is lateral, both ending at the buttock crease.
Petrissage strokes begin with palmar kneading, one hand reinforcing the other, and is carried out over the bulky middle area of the hamstrings. Picking up is used over the length of the muscle, with wringing and rolling used over the muscle bellies. In each case, the tissue manipulation begins just above the popliteal fossa and proceeds centrally, medially and laterally, the number of ‘muscle strips’ depending on the size of the athlete’s leg.
Adductor region
Local massage to the adductors may be given with the athlete supine and the hip flexed, abducted and externally rotated. The knee then rests on a folded pillow or the therapist’s pelvic rim, with the far hand stabilizing the knee. Alternatively, half crook side lying may be chosen (Fig. 2.15). The near hand begins the massage with effleurage and shaking, moving from the medial epicondyle of the knee to the groin. Palmar kneading and picking up are used, followed by deep effleurage along the length of the adductor fibres using the thumb pad. Transverse frictions, if required, may be given by altering the hand so that the dominant hand lies perpendicular to the thigh. Flicking, using the ulnar borders of the hands in a rapid alternating action, is the most appropriate percussion technique. Hacking can be painful due to the fusiform nature of the muscle, while clapping tends to be better carried out with the athlete in side lying (see below). The massage finishes with effleurage, and the athlete’s position lends itself well to the use of passive stretching techniques, including contract–relax for the short adductors. An alternative starting position, which allows the application of more pressure, is half crook side lying with the affected leg extended on the couch. The unaffected leg lies forwards with the hip and knee flexed and the knee supported on a pillow to prevent pelvic and spinal rotation.

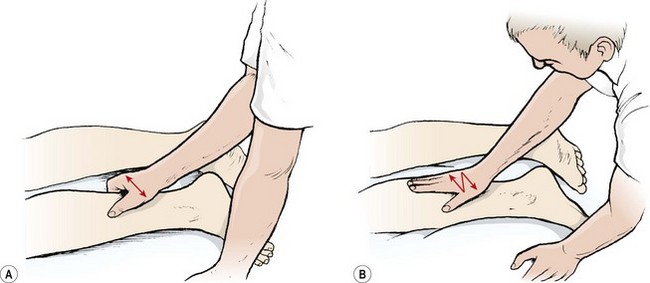
Calf and Achilles
The calf area is treated after the posterior thigh in cases of general massage where swelling is the major concern. The shin is supported on a folded towel, or the leg being treated may be hooked over the other leg. Effleurage and muscle shaking are used to begin the treatment. Superficial strokes are applied longitudinally from Achilles to knee with the hands working side by side or one hand resting over the other, depending on limb size. The stroking movement is localized by using the thumb pads placed side by side, with the movement directed along the muscle fibres (Fig. 2.16). Kneading is given to the muscle bellies only, with picking up and muscle rolling being especially useful in cases of consolidated oedema. Circular frictions are applied along each side of the Achilles tendon. This may be applied with one finger supporting the other or using a light pinch grip massaging both sides of the Achilles at once.

Figure 2.16 Calf treatment. (A) Localized stoking using thumb pads. (B) Effleurage using thumb web. (C) Massage of the peronei.
An alternative starting position is with the knee held flexed by the therapist’s hand while the other hand supplies the effleurage stroke, with the web of the hand. The calf is then massaged in two or three sections, depending on size. Where more pressure must be exerted, crook lying is the position of choice. The therapist sits on the couch and supports the athlete’s foot against his or her thigh. Effleurage is given with one cupped hand over the other. The therapist can lean back to exert more pressure. Local stroking is then applied with the fingertips rather than the thumbs. In the crook lying position, the edge of the tibialis posterior and the peronei may be massaged using either the fingertips or the thumb, with the rest of the fingers stabilizing the hand.
Anterior thigh
Massage to the anterior thigh proceeds in a similar order to that of the posterior thigh. Less direct pressure is used due to the reduced muscle bulk, and percussion movements are rarely used. Finger kneading may be used effectively around the patella especially over the suprapatellar pouch in the case of local pooling of oedema within this area. Kneading is probably the most useful procedure over the quadriceps because of the ease with which the muscle bellies are picked up.
Shin
Massage is only applied to the peronei over the lateral aspect of the shin due to the lack of muscle over the medial tibia. The size of the lateral compartment dictates that the whole hand cannot be used. Effleurage is applied with the thumbs held side by side or with the fingers, with the thumb stabilizing the hand. Alternatively, the hypothenar eminence may be used in larger subjects.
The back
Lower back
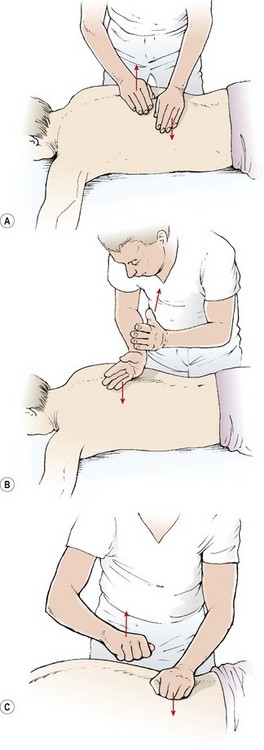
The subject is in the prone lying position with a rolled towel beneath the shins to flex the knees and take the stretch off the sciatic nerve. If the lordosis is very deep, some subjects find it more comfortable to have a folded towel placed beneath the abdomen. Massage to the back may be given in any direction, and the practitioner does not need to work ‘distal to proximal’, as with the limbs. The massage begins with effleurage from the posterior iliac crest to the scapula (Fig. 2.17). The fingers follow the line of the erector spinae muscle fibres and cover the back in two or three sections, depending on the athlete’s size. Lateral effleurage (lateralizing) then follows, from the spine around the trunk to the abdomen. Kneading with the palms and heels of the hands begins at the inferior angles of the scapulae and works down towards the sacrum with alternating pressure movements of the hands. The line follows the line of the erector spinae. Both kneading and picking up may be used over the quadratus lumborum. Transverse kneading may be used across the erector spinae with the fingertips pulling towards the therapist and the sides of the thumbs pushing away. Local finger stroking is used with the thumbs pressing together, and finger kneading is performed with the pads of the fingers along the length of the erector spinae, across the posterior rim of the pelvis, and along the posterior aspect of the lower ribs. Skin rolling is used from the ilium to the scapula and transversely around the circumference of the lower trunk.
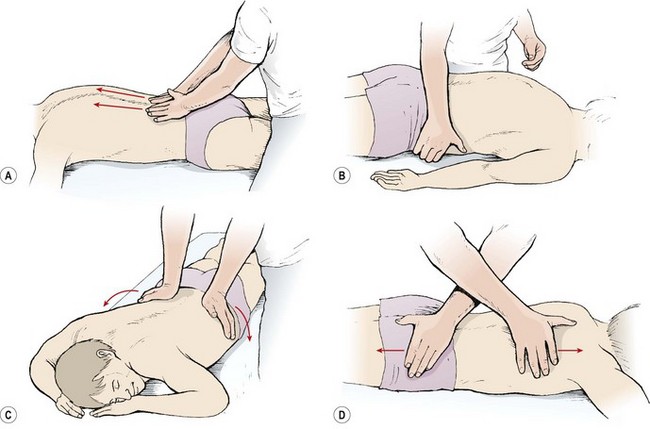
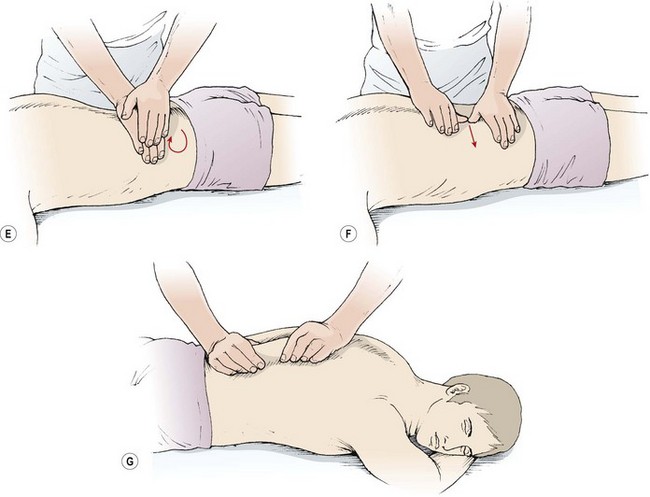
Figure 2.17 Lower back massage. (A) Effleurage following the line of the erector spinae. (B) Lateral effleurage. (C) Deep lateralizing. (D) Fascial stretch. (E) Kneading. (F) Transverse kneading. (G) Skin rolling.
Fascial stretching may be used to good effect in the lower spine. The forearms are crossed and the hands are placed flat over the back. The practitioner leans forwards and down exerting pressure and pressing the hands apart to impart and stretch on the lumbar fascia. The hand must not slide over the skin surface as this will cause painful friction: the skin and hand move as one unit.
The lower back massage finishes with effleurage and light finger stroking movements to aid relaxation.
Upper back
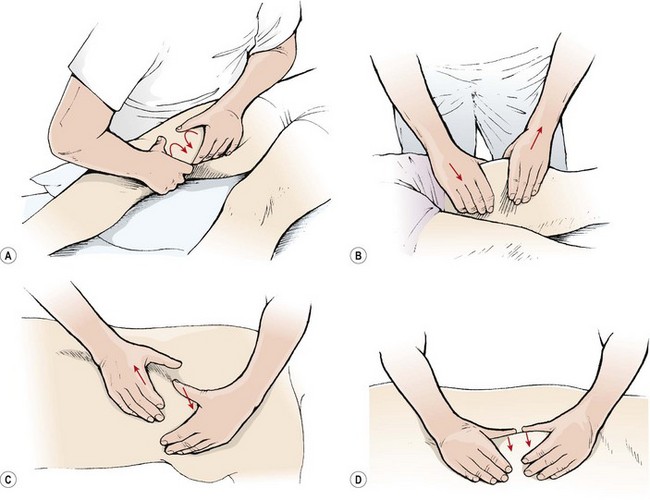
When applying upper back massage, the therapist stands at the couch side and later changes position to the head of the couch facing caudally (Fig. 2.18). Effleurage begins over the trapezius in a diamond shape, from the inferior angle of the scapula to the occiput, out to the acromion and down to the inferior angle once more. Kneading with the heel of the hand is used from the occiput to lower scapula. Petrissage is especially useful over the middle fibres of trapezius, with ringing and rolling both appropriate techniques. Kneading, using the pads of the fingers, is useful along the length of the cervical extensors and to the rhomboids and levator scapulae. If the shoulder is internally rotated (hand behind the back), the medial border of the scapula can be lifted from the ribcage and the side of the therapist’s hand can be used to massage beneath the undersurface of the scapula (serratus anterior and subscapularis muscles). Hacking, clapping and flicking actions are used over the middle trapezius fibres only, the superficial bony surfaces making these techniques inappropriate over the scapula and upper spines.
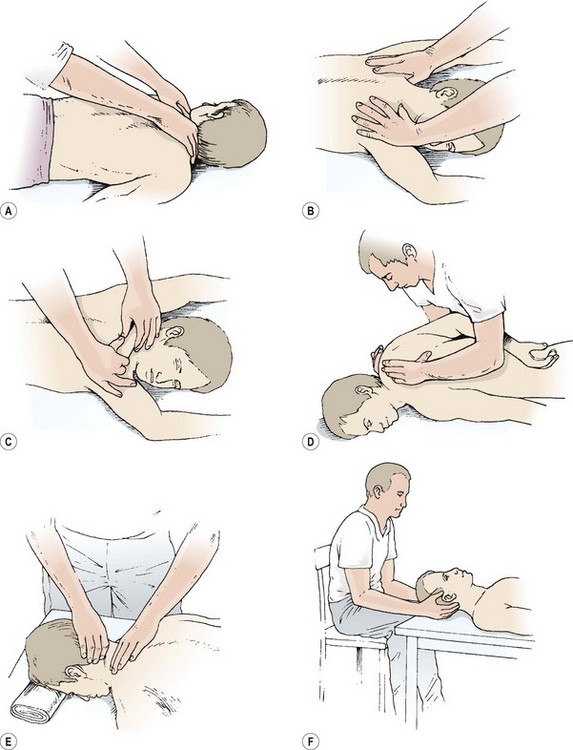
Figure 2.18 Upper back massage. (A,B) For upper back massage the therapist stands at the couch side and later changes to the head end. (C) Kneading the middle fibres of trapezius. (D) With the shoulder internally rotated the medial border of the scapula is lifted. (E) Massage to the upper trapezius. (F) Suboccipital techniques.
The therapist then transfers to the head of the couch. Kneading and pressure techniques to the middle fibres of trapezius are more effective from this position. In addition, finger kneading and friction may be carried out to the occiput. Where massage is required to the upper cervical and suboccipital regions only, the athlete may be positioned supine, lying with the head supported on a folded towel. The therapist sits at the head end of the couch and uses finger kneading and friction to the suboccipital tissues. From this position, passive stretching techniques for the upper trapezius and levator scapulae may then be carried out.
The upper limb
Shoulder and upper arm
Arm and shoulder massage may be carried out in either sitting or supine positions (Fig. 2.19). When sitting, the athlete’s arm is supported on a small table, or if lying, the arm is supported on a pillow or folded towel. Alternatively, the arm may be usefully supported across the therapist’s leg (covered by a folded towel) for certain upper arm and shoulder procedures. The treatment begins with effleurage, the therapist holding the athlete’s hand for limb stability. The therapist anchors the athlete’s near hand. The palm of the therapist’s far hand rests over the extensor aspect of the athlete’s hand to begin the effleurage stroke. The movement begins distally, with the therapist’s far hand moving from the athlete’s fifth finger along the ulnar aspect of the forearm, across the under edge of the upper arm to end at the axilla. For the second stroke, the athlete’s forearm is moved into mid-pronation. The action begins at the back of the athlete’s hand and covers the radial side of the forearm and side of the upper arm, to again end at the axilla. For the flexor aspect of the arm, the therapist changes hands so that the near hand carries out the massage stroke. The movement begins at the thumb, and glides along the radial side of the forearm and anterior aspect of the upper arm to the axilla. The next stroke begins over the athlete’s palm, and proceeds over the flexor aspect of the forearm and inner edge of the upper arm to the axilla. The last effleurage stroke begins on the flexor aspect of the fifth finger and moves across the inner edge of the forearm and upper arm to the inner axilla.
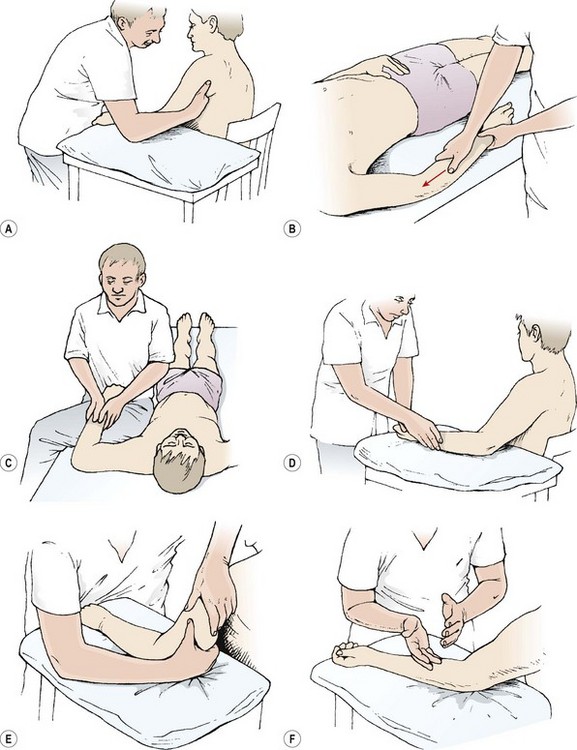
Figure 2.19 Massage of the shoulder and upper arm. (A) Arm supported on table in sitting. (B) Supine lying. (C) Using the therapist’s leg for support. (D) Effleurage using the thumb web. (E) Wringing the triceps. (F) Hacking the flexor aspect of the forearm.
Muscle shaking is performed using the same single-handed grip as effleurage. The deltoid and triceps are shaken using the outer hand, while the biceps is shaken using the inner hand. In each case the other hand holds the athlete’s hand to stabilize the arm.
Kneading begins with the hands placed on the anterior and posterior aspects of the deltoid. The hands press together, compressing the shoulder, and work alternately in circular motions. The alternate movement continues down the length of the upper arm with the hands gripping biceps and triceps, and moving around the arm slightly to cover the flexor and extensor aspects of the forearm. Each hand moves along the skin only as the compression pressure is released. Thumb kneading may be used for the forearm, with the thumbs lying side by side. The pressure is transmitted with the length of the distal phalanx rather than the tip (‘along’ rather than ‘in’).
Picking up and muscle rolling may be performed single-handed or with both hands alternately. The single-handed action maintains the grip on the athlete’s hand (or elbow in the case of shoulder treatment) for stability. The therapist’s outer hand is used for procedures on the posterior deltoid, triceps and forearm extensors, the inner hand for the anterior deltoid, biceps and forearm flexors. Double-handed actions are used for the middle fibres of the deltoid following on from kneading for the upper fibres of trapezius (see above). The thumb and finger grip must avoid placing pressure over the acromion.
Wringing is used over the bellies of the biceps and triceps. In the case of the biceps, the therapist stands in front of the athlete with the hands over the anterior position of the arm and the fingers placed medially. For the triceps, the hands cup the posterior portion of the arm, again with the fingers medially placed. The wringing action is carried out using the cupped hands in opposition. The forearm flexors are wrung using the thumb pads in opposition to the pads of the index and ring fingers.
Percussion techniques are performed first on the flexor aspect of the whole arm with the forearm supinated, and then on the extensor aspect with the forearm pronated. For the extensor aspect the therapist stands level with the athlete’s waist and faces the head. With the athlete’s forearm pronated, the action works from the posterior axilla and posterior deltoid across the triceps and then to the forearm extensors. For the flexor aspect, the therapist changes position to stand above the athlete’s arm facing the feet. The athlete’s forearm is supinated and the action begins at the medial axilla, and works down the front of the deltoid, over the biceps and across the forearm flexors. The therapist must take care to avoid contact with bony prominences and superficial tendons at the shoulder and elbow.
Foot massage
Foot massage (Fig. 2.20) may be used following an injury where swelling and scar tissue are present. In addition, foot massage is particularly beneficial as an aid to relaxation. Reflexology is a specialized form of foot massage not covered in this book.

Figure 2.20 Foot massage. (A) Finger kneading. (B) Plantar kneading using the knuckles. (C) Deep digital pressure of the sole.
Foot massage is often combined with passive joint movement (physiological and accessory), because the joints of the foot often become stiff through the use of constricting footwear. The reader is referred to Maitland (1991) and Kaltenborn (1989) for details of the techniques.
Effleurage is given by starting with the therapist’s hands cupping the athlete’s foot, with the fingers resting medially. Initially, both hands move from the toes to the ankle. As the action becomes firmer, one hand remains stationary to support the foot while the other carries out the massage stroke. General kneading is carried out with one hand holding the toes and the other imparting pressure through the hypothenar eminence. More specific finger kneading and circular frictions are used for the interossei. Firm digital pressure is used over the sole of the foot with the thumb pads or single knuckle. Light percussion techniques (finger tapping) are used only over the medial longitudinal arch with the foot supported in slight plantarflexion. A stretching action is used for the metatarsals. The hands surround the foot, with the thumbs on the plantar surface and the fingertips coming together on the dorsal surface. The action is to press the thumbs into the plantar surface of the metatarsal heads and pull the neighbouring metatarsal bones down with the fingers. Slow passive movements are then used to fully stretch the tissues. Each toe is tractioned in turn, and flexion, extension, abduction and adduction are used for each of the metatarsal phalangeal (MTP) joints. Circular frictions and finger kneading are used around the malleoli, and to each side of the Achilles tendon.
Effects of massage
Effects of massage are achieved through mechanical, physiological, neurological and psychological processes, and the interrelation between these. Several parameters have been studied, but it is likely that the compound effect of these parameters is more important clinically than isolated effects.
Treatment note 2.2 Trigger points
Trigger points (myofascial trigger points) are highly sensitive local areas which often lie within a tight band of the muscle fibres. In general, trigger points (TrP) can cause pain in a muscle at rest, or, particularly, when a muscle is placed on stretch. Because the TrP is painful when the muscle is placed on stretch, it prevents the muscle from lengthening and so can alter body alignment (see Muscle imbalance, Chapter 5).
TrPs are painful to palpation and often appear as nodules or tight bands within the muscle itself. Sudden pressure or flicking the fingers across the band can cause the muscle to jump, a reaction known as the ‘twitch response’ or ‘jump sign’. Some trigger points lie over traditional acupuncture points, while others are simply within the muscle.
A TrP may either be active or latent. A latent TrP does not cause pain at rest, but only when it is palpated. Although not painful, the muscle that the TrP is associated with can still be shortened and restrict movement. An active TrP causes both pain and tenderness at rest or when the muscle is stretched during daily activities. Palpation of an active TrP causes pain and referral of the pain in a pattern which mimics the patient’s main symptoms.
TrPs may be located within the belly of a muscle (central TrP) or at the muscle attachment (attachment TrP). In the case of the latter, a TrP may be found at both the teno-osseous and musculotendinous junctions where the muscle attaches to bone, tendon or aponeurosis (sheet of tendon).
A number of theories have been proposed for TrP activation, including damage to the muscle sarcolemma resulting in an alteration to the muscle contraction threshold, local muscle ischaemia, and an alteration in the release of acetylcholine from the motor end plate.
Massage treatment of trigger points (TrPs)
TrPs may be treated through a number of mechanisms (see Table 5.5), including several massage techniques, dry needling and stretching.
Ischaemic compression
In this technique, pressure is applied slowly and progressively to the TrP (sudden pressure can stimulate the TrP). The pressure is maintained until the tenderness to palpation has reduced and the end-feel of the tissue changes from a hard elastic recoil to a softer resistance. As this occurs, a slow continuous stretch may be placed on the muscle to lengthen it.
Ischaemic compression relies on heavy pressure from the practitioner and either the thumbs or supportive finger (see Treatment note 2.1) may be used, or several mechanical devices are available (Fig. 2.21).


Muscle stripping
This is a deep stroking massage applied with minimal lubrication to the skin to prevent friction only. Firm pressure is used along the length of the taut band at a rate of approximately 2–3 cm every 3 seconds. The direction should be distal to proximal, creating a ‘milking movement’ and causing a reflex hyperaemia that returns the muscle site to its normal condition.



Tissue fluids
Compression and squeezing will improve venous and lymphatic drainage, visible when superficial vessels are massaged (Hollis, 1987). Interstitial pressure is increased and fluid absorption aided. Fresh blood will enter the area. The superficial skin response to vigorous massage is an axon reflex. Redness results (flare) through dilatation of skin arterioles and slight swelling (wheal) occurs through increased permeability of the capillary wall, allowing tissue fluid to escape into the surrounding area. The deep response to vigorous massage, however, can be a reduction in blood flow, if muscle tone is increased and blood flow through the muscle reduces as a consequence.
Early research showed that deep stroking and kneading of the calf for a 10-minute period increased blood volume for 40 minutes (Bell, 1964), and blood pressure has been shown to reduce following back massage (Barr and Taslitz, 1970). Intradermal dye injections have been used to show lymph flow improvements with massage (McMaster, 1937), and massage has been shown to be significantly better at improving lymph flow compared to electrical stimulation and passive movements (Ladd, Kottke and Blanchard, 1952).
A decrease in the viscosity of both blood and plasma has been shown following a 20-minute whole body massage (Ernst et al., 1987). Stimulatory mechanical massage has been shown to be ineffective at increasing blood flow and aiding recovery (Carafelli et al., 1990). This type of massage can cause muscle contraction through the initiation of a tonic vibration reflex, and will therefore reduce blood perfusion through the muscle.
Pain relief and relaxation
Short-term pain relief, particularly through friction massage, is thought to be brought about by the closure of the pain gate and stimulation of endogenous opioids (Cyriax, 1980). In contrast, gentler techniques do not appear to give this response. No significant change has been shown in beta endorphin or beta lipotrophin levels on pain-free subjects using effleurage and petrissage of the back over a 30-minute period (Day, Mason and Chesrown, 1987).
Massage has been found to be superior to relaxation therapy in the treatment of fibromyalgia (Sunshine et al., 1996). Two 30-minute massage periods were given weekly over a 5-week period and the significant changes included an increased number of sleep hours and a reduction in substance P, pain rating and number of tender points.
One of the greatest benefits from massage seems to be psychological, with increased feelings of wellbeing and decreased arousal levels (Longworth, 1982; Hemmings, 2001). Massage has been shown to improve mood state in a group of amateur boxers during intensive training (Hemmings, 2000) and perceived recovery following athletic training and competitive performance (Hemmings et al., 2000). Pre-competition sports massage has been shown to produce a positive response, with athletes able to cope better with physical exertion (Harmer, 1991).
Tissue mobilization
Tissues are mobilized as they are moved over each other, and adhesions stretched with more forceful actions. Massage has been shown to aid recuperation from muscle fatigue (Balke, Anthony and Wyatt, 1989), and is commonly used both before and after exercise with this in view. Sports massage has been shown to be effective at reducing delayed onset muscle soreness (DOMS) when it is applied within 2 hours of eccentric exercise (Smith et al., 1994). Creatine kinase (CK) levels were reduced, and a slight increase in both neutrophil emigration and cortisol levels was noted. Stimulatory massage, however, may have the reverse effect. CK and lactate dehydrogenase (LDH) have been shown to increase significantly following vigorous whole body massage, possibly illustrating mechanical trauma to the muscles, with resultant increased cell membrane activity (Arkko, Pakarinen and Kari-Koskinen, 1983). Tissue damage of this type has been used to argue the case for rigorous training for therapists applying massage to athletes (Callaghan, 1993).
Investigation of the effect of leg massage on recovery from high intensity cycling has shown no significant difference in power output (Wingate test) following massage (Robertson et al 2004). However a significant change was shown in fatigue index, mean value for the massage group being 30.2 and that for the non-massage group 34.2.
Muscle tone and length
Studies of muscle tone using the Hoffman (H) reflex have shown a decrease in H reflex amplitude during, but not following, massage (Morelli, Seabourn and Sullivan, 1990; Sullivan et al., 1991).
Use of massage on hamstring flexibility in a sit and reach test has shown a greater effect with those who were less flexible (Barlow et al., 2004) although the results were non-significant in each case. In this study mean change was 6.0% for those receiving massage compared to 4.5% for the control group. Interestingly, however, these scores were considerably larger for less flexible individuals where the massage group changed by 18.2% and by 15.5% in the non-massage group.
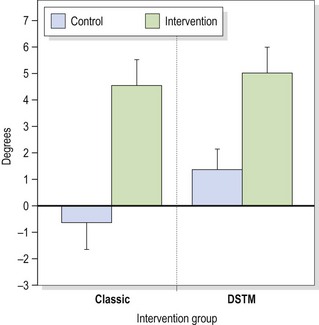
Massage has been shown to increase hamstring flexibility measured using a passive knee extension (PKE) test. Hopper et al. (2005) performed either classical massage or deep soft tissue massage (classical techniques followed by specific work over tighter tissue elements) for 8 minutes on the posterior thigh. Range of motion was increased (Figure 2.24) but this increase was not maintained for longer than 24 hours. This result is important, however, as the increased range of motion could be incorporated into a postural re-education programme where muscle tightness is an element in movement dysfunction, for example in forward bending.
Joint mechanics
Massage affects the soft tissues, but during treatment we often need to target the joints in tandem with soft tissue therapy. Individual joint (articular) techniques will be covered in the clinical chapters, but let’s firstly have a brief overview of some principles behind joint techniques.
Accessory movements
The movements of a joint are of two types, physiological and accessory. Physiological movements are those which the athlete can perform actively, for example flexion and extension of the knee. Accessory movements cannot be produced actively as individual movements, but occur automatically between articulating surfaces of a joint as it moves. Three accessory movements are of particular importance when treating sports injuries: these are roll, slide and spin.
Close and loose pack
The two opposing surfaces of a joint do not fit together exactly; they are said to be non-congruent. But, with the joint in one particular position its surfaces will come as close together as they are able, and this is known as ‘close pack’. In this position the joint capsule and ligaments twist and pull the joint surfaces together into approximation. The joint space is at a minimum and the concave surface of one bone fits tightly into the convex shape of the other. No further movement is possible in a joint which is close packed, and so this position is avoided when trying to mobilize the joint.
Loose pack position is exactly the opposite. As the joint surfaces are released from their close pack position, elastic recoil of the soft tissues surrounding the joint enables its surfaces to move apart, maximizing the joint space. The loose pack position is the resting position often taken up after injury because more joint fluid can accumulate. In loose pack positions joint play is possible. This consists of small accessory movements which give the joint its ‘spring’. These are essential to the normal functioning of the joint and play a part in joint nutrition and combined movements.
Definition
In close pack the joint surfaces are most congruent with each other. The joint capsule and ligaments are taut and the joint is relatively immobile. In loose pack the joint surfaces are non-congruent, the capsule and ligaments lax, and the joint is mobile.
Interestingly many fractures of the upper limb occur with a fall onto the outstretched arm, which is a close packed position, and many ligament sprains occur in loose packed position (Hertling and Kessler, 1990). Examples of close and loose pack positions are given in Table 2.5.
Table 2.5 Close packed and loose packed positions of selected joints
| Joint(s) | Close packed position | Loose packed (resting) position |
|---|---|---|
| Facet (spine) | Extension | Midway between flexion and extension |
| Temporomandibular | Clenched teeth | Mouth slightly open |
| Glenohumeral | Abduction and external rotation | 55° abduction, 30° horizontal abduction, rotated so that the forearm is in the transverse plane |
| Acromioclavicular | Arm abduction to 30° | Arm resting by side, shoulder girdle in the physiological position |
| Sternoclavicular | Maximum shoulder elevation | Arm resting by side, shoulder girdle in the physiological position |
| Ulnohumeral (elbow) | Extension | 70° elbow flexion, 10° forearm supination |
| Radiohumeral | Elbow flexed 90°, forearm supinated 5° | Full extension, full supination |
| Proximal radioulnar | 5° supination | 70° elbow flexion, 35° forearm supination |
| Distal radioulnar | 5° supination | 10° forearm supination |
| Radiocarpal (wrist) | Extension with ulnar deviation | Midway between flexion−extension (so that a straight line passes through the radius and third metacarpal) with slight ulnar deviation |
| First carpometacarpal | Full opposition | Midway between abduction-adduction and flexion-extension |
| Metacarpophalangeal (fingers) | Full flexion | Slight flexion |
| Metacarpophalangeal (thumb) | Full opposition | |
| Interphalangeal | Full extension | Slight flexion |
| Hip | Full extension, internal rotation and abduction | 30° flexion, 30° abduction, and slight external rotation |
| Knee | Full extension and external rotation of the tibia | 25° flexion |
| Talocrural (ankle) | Maximum dorsiflexion | 10° plantarflexion, midway between maximum inversion and eversion |
| Subtalar | Full supination | Midway between extremes of inversion and eversion |
| Midtarsal | Full supination | Midway between extremes of range of movement |
| Tarsometatarsal | Full supination | Midway between extremes of range of movement |
| Metatarsophalangeal | Full extension | Neutral |
| Interphalangeal | Full extension | Slight flexion |
From Clarkson, H.M. and Gilewich, G.B. (1989) Musculoskeletal Assessment. Williams and Wilkins, Baltimore MD. With permission.
Treatment note 2.3 Concept of mobilization and manipulation
Mobilization using accessory movements
Where pain and stiffness limit the normal (physiological) movement of a joint, rather than pressing further into this painful range, accessory movements may be used. By increasing the range available to accessory motion, the physiological range may also increase (Maitland, 1986, 1991).
If pain is the dominant factor, this is treated first. When stiffness overshadows pain the aim is to increase the patient’s range of motion even though some soreness may be produced during and following treatment. Most patients will present with a combination of pain and stiffness, and when there is doubt as to which is the predominant feature, pain is treated first.
When joint movement is limited, the point of limitation falls short of the anatomical range (that which is available to a joint because of its structure). As the joint is mobilized the point of limitation moves closer to the anatomical range. Within a range of movement four grades of mobilization techniques are used (Table 2.6).
Table 2.6 Grades of mobilization procedures
| Grade I | Small amplitude movement near the starting position of the range |
| Grade II | Large amplitude movement occupying any free part of the range |
| Grade III | Large amplitude movement moving into stiffness |
| Grade IV | Small amplitude movement at the end of range |
After Maitland (1986), with permission.
Represented diagrammatically (Fig. 2.25), grades I and II do not reach the end range, and are used when pain is the predominant feature. Grades III and IV are performed to end-range movement and are used when stiffness is the main problem.
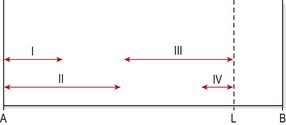
Figure 2.25 Grades of joint mobilization. A, starting point of movement range. B, anatomical limitation of range. L, limitation point due to pain.
A number of techniques may be used. In the knee, for example, lateral movements (Fig. 2.26) and anteroposterior (AP) movements (Fig. 2.27) are useful accessory movements for treatment, while normal bending and straightening (flexion and extension) represent the physiological movements which would be expected to increase as a result of joint mobilization.


Mobilization with movement
With this concept, it is proposed that injury results in not just a reduction in range of motion, but also an alteration in movement throughout the range, or maltracking. Three techniques are used. NAGS (natural apophyseal glides) are accessory movements performed in line with the facet plane orientation. SNAGS (sustained natural apophyseal glides) are gliding mobilizations performed as the patient moves.
Peripheral joints may also be treated in a similar way using mobilizations with movement (MWM) in an attempt to correct maltracking of the joint. In the case of a hinge joint such as the elbow (Fig. 2.28) the proximal segment is stabilized while the distal segment is subjected to a gliding (transverse) mobilization by the therapist. The unique feature of this type of mobilization, however, is that the patient then actively performs the previously symptomatic movement. If pain increases, it indicates that the direction of glide was incorrect and this is reversed and the movement attempted again. Pain reduction should occur; if pain again increases the technique is said to be unsuitable.

Joint manipulation
A manipulation is a high velocity thrust of small amplitude performed at the end-range of motion. The thrust is often accompanied by a pop or click from alteration of gaseous pressure within the synovial fluid when the joint surfaces are tractioned (the suction phenomenon), or a tearing sensation if adhesions are ruptured. Replacing a subluxed joint may also be audible.
Manipulation may be used to stretch out capsular contraction, to rupture joint adhesions, or to move an intra-articular displacement (Cyriax, 1982). Manipulative rupture of adhesions and manipulative reduction is achieved with a high velocity (fast), low amplitude (small) movement. This may be accompanied by traction using some methods. The aim is to perform the technique so quickly that muscle contraction is unable to limit the motion. However, joint manipulation is rarely used where a joint is protected by obvious spasm, as soft tissue techniques to relieve the spasm are normally used first.
Arkko P.J., Pakarinen A.J., Kari-Koskinen O. Effects of whole body massage on serum protein and hormone concentrations, enzyme activities and haematological parameters. International Journal of Sports Medicine. 1983;4:265-267.
Balke B., Anthony J., Wyatt F. The effects of massage treatment on exercise fatigue. Clinical Sports Medicine. 1989;1:189-196.
Barlow A., Clarke R., Johnson N., et al. Effect of massage of the hamstring muscle group on performance of the sit and reach test. British Journal of Sports Medicine. 2004;38:349-351.
Barr J.S., Taslitz N. Influence of back massage on autonomic functions. Physical Therapy. 1970;50:1679-1691.
Bell A.J. Massage and the physiotherapist. Physiotherapy. 1964;50:406-408.
Bork B., Cook T.M., Rosecrance J., Engelhardt K. Work related musculoskeletal disorders among physical therapists. Physical Therapy. 1996;76:827-835.
Bowsher D. Modulation of nociceptive input. In Wells P.E., Frampton V., Bowsher D., editors: Pain Management by Physiotherapy, second ed, Oxford: Butterworth-Heinemann, 1988.
Callaghan M.J. The role of massage in the management of the athlete: a review. British Journal of Sports Medicine. 1993;27(1):28-33.
Carafelli E., Sim J., Carolan B., Libesman J. Vibratory massage and short term recovery from muscular fatigue. International Journal of Sports Medicine. 1990;11:474-478.
Clarkson H.M., Gilewich G.B. Musculoskeletal Assessment. Baltimore, MD: Williams and Wilkins; 1989.
Copestake B.M.G. The Theory and Practice of Massage and Medical Gymnastics. London: H.K. Lewis; 1917.
Cyriax J. Massage, Manipulation and Local Anaesthesia. London: Hamilton; 1941.
Cyriax J. Textbook of Orthopaedic Medicine, tenth ed. London: Baillière Tindall; 1980.
Cyriax J. Textbook of Orthopaedic Medicine vol. 1, eighth ed. London: Baillière Tindall, 1982.
Day J.A., Mason R.R., Chesrown S.E. Effect of massage on serum level of β-endorphin and β-lipotrophin in healthy adults. Physical Therapy. 1987;67:926-930.
de Bruijn R. Deep transverse friction: its analgesic effect. International Journal of Sports Medicine. 1984;5:35-36.
Demain S. Departmental danger of death. Physiotherapy. 1996;82(1):71.
Dixon M.W., Herman K.J., Thompson D., Cherkin D.C. Massage terminology. Its all in the name. Sportex Dynamics. 2007;11:14-21.
Ernst E., Matrai A., Magyarosy I., et al. Massages cause changes in blood fluidity. Physiotherapy. 1987;73:43-45.
Harmer P.A. The effect of pre-performance massage on stride frequency in sprinters. Athletic Training. Journal of the National Athletic Training Association of America. 1991;26:55-59.
Hemmings B. Sports massage and psychological regeneration. British Journal of Therapy and Rehabilitation. 2000;7:425-429.
Hemmings B., Smith M., Graydon J., Dyson R. The effects of massage on physiological restoration, perceived recovery and repeated sports performance. British Journal of Sports Medicine. 2000;34:109-115.
Hemmings B.J. Physiological, psychological and performance effects of massage therapy in sport: a review of the literature. Physical Therapy in Sport. 2001;2(4):165-170.
Hertling D., Kessler R.M. Management of Common Musculoskeletal Disorders. Philadelphia: J.B. Lippincott; 1990.
Holey E.A., Cook E.M. Therapeutic Massage. Oxford: Butterworth-Heinemann; 1997.
Hollis M. Massage for Therapists. Oxford: Blackwell Scientific Publications; 1987.
Hopper D., Conneely M., Chromiak F., et al. Evaluation of the effect of two massage techniques on hamstring muscle length in competitive female hockey players. Physical Therapy in Sport. 2005;6:137-145.
Kaltenborn F.M. Manual Mobilization of the Extremity Joints. Norway: Olaf Norlis Bokhandel; 1989.
Kelly E. The effects of deep transverse frictional massage to the gastrocnemius muscle. Journal of Orthopaedic Medicine. 1997;19:3-9.
Kesson M., Atkins E. Orthopaedic Medicine. Oxford: Butterworth-Heinemann; 1998.
Ladd M.P., Kottke F.J., Blanchard R.S. Studies of the effect of massage on the flow of lymph from the foreleg of the dog. Archives of Physical Medicine and Rehabilitation. 1952;33(8):971-973.
Lancey V. An overview of sports massage. Sportex Health. 2002;7:26-27.
Longworth J. Psychophysiological effects of slow stroke back massage in normotensive females. Advances in Nursing Science. 1982;July:44-61.
Maitland G.D. Vertebral Manipulation, fifth edn. Oxford: Butterworth-Heinemann; 1986.
Maitland G.D. Peripheral Manipulation, third edn. Oxford: Butterworth-Heinemann; 1991.
McMaster P.D. Changes in the cutaneous lymphatics of human beings and in the lymph flow under normal and pathological conditions. Journal of Experimental Medicine. 1937;65:347.
Morelli M., Seabourn D.E., Sullivan J. Changes in H-reflex amplitude during massage of triceps surae in healthy subjects. Journal of Orthopaedics and Sports Physical Therapy. 1990;12:55-59.
Robertson A., Watt J.M., Galloway S. Effects of leg massage on recovery from high intensity cycling exercise. British Journal of Sports Medicine. 2004;38:173-176.
Smith L.L., Keating M.N., Holbert D., et al. The effects of athletic massage on delayed onset muscle soreness, creatine kinase, and neutrophil count: a preliminary report. Journal of Orthopaedics and Sports Physical Therapy. 1994;19:93-99.
Sullivan S.J., Williams L.R.T., Seabourne D.E., Morelli M. Effects of massage on alpha motoneuron excitability. Physical Therapy. 1991;71:555-560.
Sunshine W., Field T., Schanberg S., et al. Massage therapy and transcutaneous electrical stimulation effects on fibromyalgia. Journal of Clinical Rheumatology. 1996;2:18-22.
Winter B. Transverse frictions. South African Journal of Physiotherapy. 1968;24:5-7.