CHAPTER 5 Exercise therapy
Structure vs function
Often, student physiotherapists new to soft tissue injury management will focus attention purely on structure. Equipped with a wide knowledge of anatomy, they try to find which single structure has been injured, and to define that as their diagnosis. If it is a muscle tear, for example, they may note the muscle’s origin and insertion and treat the muscle in isolation. When it comes to exercise, they consider the muscle’s action and give this action as an exercise of some type. For example, if the hamstring muscles are torn, exercises are often given which simply involve flexing the knee against resistance and performing a toe-touching movement to stretch the muscle.
As experience is gained, the clinical physiotherapist realizes the error of this reductionist approach. If the body is reduced to a number of simple components, rehabilitation of a sporting injury is largely ineffective. The muscle may strengthen or increase in flexibility, for example, but the ability of the patient to perform the adaptations of daily living (ADL), and the athlete to participate in sport, often remains poor. The athlete with a hamstring tear treated in this way will very often find pain relieved mainly through the passage of time, but on return to sport the injury simply recurs.
Rather than reducing the body to simple structural components, if movement quality is the starting point for rehabilitation, the athlete’s ability is rapidly enhanced. Instead of considering the textbook anatomy of an area, if the therapist asks the simple question ‘how does this injury affect the whole athlete?’ the answer will often guide the rehabilitation programme perfectly. This whole person approach makes treatment holistic.
Definition
A reductionist approach seeks to understand complex items (in this case the body) in terms of their more simple component parts. A Holistic approach addresses the whole person.
The functional decrement which the patient is suffering becomes the central focus, rather than the structural damage, and as a consequence, rehabilitation is considerably more successful. The athlete with the hamstring injury described above may well lack strength and flexibility, and in the early stages of rehabilitation, simple single plane motions may suffice. But if the therapist considers the function of the hamstrings in the closed kinetic chain position, the action of the muscle in ballistic movements, the interaction of the hamstrings with bending and lifting, and the stresses imposed on a two-joint muscle, a whole series of exercises become available.
Through this approach the therapist can break away from the limitation of standard lists of exercises which fail to take account of the needs of the individual. Instead of the athlete grinding away in boredom at endless repetitions of a movement, exercise therapy can become vibrant and challenging. The end result is a more rewarding period of rehabilitation for both athlete and therapist.
The aim of this chapter is therefore to develop the theme of ‘functional exercise therapy’, and we will begin by looking at muscle imbalance. Further details of these concepts may be found in Norris (2008).
Muscle imbalance
Basic concepts
Changes in muscle length or strength occur throughout the body in set patterns rather than purely at random. The relationship between the tone and length of muscles around a joint is known as muscle imbalance and has been described by a number of authors (Janda and Schmid, 1980; Sahrmann, 1987; Richardson, 1992; Kendall, McCreary and Provance, 1993; Comerford, 1995; Norris, 1995a). Muscles may be broadly classified into two types for convenience. Those whose actions are mainly to stabilize a joint and approximate the joint surfaces, and those responsible more for movement, which more effectively develop angular rotation. The main differences between the two types of muscles are shown in Table 5.1. As we will see this categorization helps to clarify exercise prescription but is not an exact science. Some muscles or portions of muscles fall into both camps.
Table 5.1 Muscle types (basic classification)
| Stability | Movement |
|---|---|
| Deep | Superficial |
| Slow twitch | Fast twitch |
| One joint | Two joint |
| Weaken and lengthen | Tighten and shorten |
| Inhibited | Preferential recruitment |
Keypoint
Stability muscles hold a joint or body part firm and immobile. Movement muscles create body motion.
The stability muscles (stabilizers) tend to be more deeply placed, while the movement muscles (mobilizers) are superficial. In addition, mobilizers are often biarticular (two joint) muscles. For example, in the leg the rectus femoris is classified as a mobilizer, while the quadriceps are stabilizers. Stabilizer function is more slow twitch (type I) or tonic in nature, while that of the mobilizers tends towards fast twitch (type II) phasic action. This physiology suits the functional requirements of the muscles, enabling mobilizers to contract and build maximal tension rapidly, but at the cost of fatiguing quickly. The stabilizers build tension slowly and perform well at lower tensions over longer periods, being more fatigue resistant.
Classification of a muscle as a stabilizer with predominantly tonic functions refers to its most consistent response. Many muscles are able to exhibit both tonic and phasic contraction depending on requirement at the time. For example transversus abdominis shows tonic activity during gait when it contributes to spinal stability, but phasic activity associated with expiration during rapid breathing (Saunders, Rath and Hodges, 2004). Both the diaphragm (Hodges and Gandevia, 2000) and the pelvic floor muscles (Hodges, Pengel and Sapsford, 2007) exhibit tonic activity during an active arm lifting task and phasic activity during challenged breathing.
In general stabilizer muscles are better activated in closed kinetic chain actions, where movement occurs proximally on a distally stabilized segment. Mobilizer function is more effective in an open chain situation, where free movement occurs without distal fixation. The structure and functional characteristics of the two muscle categories make the stabilizers better equipped for postural holding and anti-gravity function. The mobilizers are better set up for rapid ballistic movements.
Keypoint
Movement muscles (mobilizers) are better activated in open chain actions. Stability muscles (stabilizers) are better activated in closed chain actions.
Two of the fundamental changes seen in the muscle imbalance process include tightening of the mobilizer (two-joint) muscles and laxity/loss of endurance within the inner range for the stabilizer (single-joint) muscles. These two changes are used as tests for the degree of muscle imbalance. The combination of length and tension changes alter muscle pull around a joint and so pull the joint out of alignment. Changes in body segment alignment and the ability to perform movements which dissociate one body segment from another form the bases of the third type of test used when assessing muscle imbalance (Fig. 5.1).
Keypoint
Through misuse or injury, stabilizing muscles tend to become lax (sagging) while movement muscles tend to tighten.
The mixture of tightness and weakness seen in the muscle imbalance process alters body segment alignment and changes the equilibrium point of a joint. In addition, imbalance leads to lack of accurate segmental control. The combination of stiffness (hypoflexibility) in one body segment and laxity (hyperflexibility) in an adjacent body segment leads to the establishment of relative flexibility (White and Sahrmann, 1994). In a chain of movement the body seems to take the path of least resistance, with the more flexible segment moving first and furthest. If we take as an illustration two pieces of rubber tubing (Fig. 5.2) of unequal strengths. When the movement begins at C and A is fixed, the more flexible area B–C moves more. This will still be the case if C is held still and A moves.
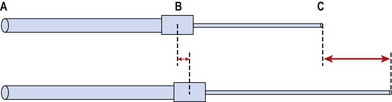
Figure 5.2 Relative stiffness. When the cord is stretched, the tighter segment (A–B) moves less than the looser segment (B–C).
Taking this example into the body, Figure 5.3 shows a toe-touching exercise. The two areas of interest with relation to relative stiffness are the hamstrings and lumbar spine tissues. As we flex forwards, movement should occur through a combination of anterior pelvic tilt and lumbar spine flexion. Subjects often have tight hamstrings and looser lumbar spine tissues due to excessive bending during everyday activities. During this flexion action, greater movement, and therefore greater tissue strain, will always occur at the lumbar spine. Excessive motion at this point can lead initially to pain simply through overstretch of pain sensitive structures. In the short to mid term the tissue insult creates an inflammatory response which both maintains the pain response and causes swelling. Longer term the combination of altered movement and tissue stress may lead to overuse injury. It become apparent in the toe-touching example that relative stiffness makes the toe-touching exercise ineffective as a hamstring stretch unless the trunk muscles are tightened to stabilize the lumbar spine.
Muscle adaptation
Muscle adaptation to reduced usage has been extensively studied using immobilized limbs (Appell, 1990). The greatest tissue changes occur within the first days of disuse. Strength loss has been shown to be as much as 6% per day for the first 8 days with little further loss after this period (Muller, 1970). Greater reduction in size and loss of numbers is seen in type I fibres, with a parallel increase in type II fibres, demonstrating selective atrophy of type I fibres (Templeton et al., 1984). However, not all muscles show an equal amount of type I fibre atrophy. Atrophy is largely related to change in use relative to normal function, with the initial percentage of type I fibres that a muscle contains being a good indicator of likely atrophy pattern. Those muscles with a predominantly anti-gravity function, which cross one joint and have a large proportion of type I fibres, show greatest selective atrophy (e.g. soleus and vastus medialis). Selective wasting in the calf muscles illustrates this well, with the soleus wasting by 60% and the plantaris by only 17% (Thomason et al., 1987). Those predominantly slow anti-gravity muscles, which cross multiple joints, are next in order of atrophy (e.g. erector spinae); last are phasic, predominantly fast type II muscles which can be immobilized with less loss of strength (e.g. biceps) (Lieber, 1992).
Keypoint
Following immobilization, muscles with a large number of type I (slow) fibres will show more marked atrophy. Muscles with predominantly type II (fast) fibres show less loss of cross-sectional area (CSA) and strength.
These three categories of muscles have led to stabilizers being subdivided into primary and secondary types (Jull, 1994) as shown in Figure 5.4. Examples of the three types include multifidus, transversus abdominis and vastus medialis oblique as primary stabilizers. The gluteals and oblique abdominals are classified as secondary stabilizers, while rectus femoris and the hamstrings are mobilizers, only acting as stabilizers in conditions of extreme need.
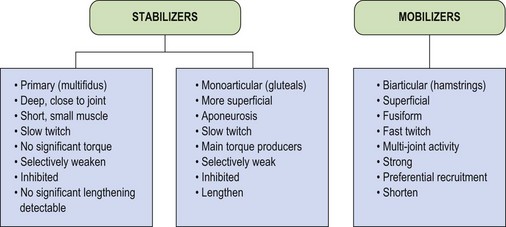
The primary stabilizers have very deep attachments, lying close to the axis of rotation of the joint. In this position they are unable to contribute any significant torque, but will approximate the joint. In addition, many of these smaller muscles have important proprioceptive functions (Bastide, Zadeh and Lefebvre, 1989). The secondary stabilizers are the main torque producers, being large monoarticular muscles attaching via extensive aponeuroses. Their multipennate fibre arrangement makes them powerful and able to absorb large amounts of force through eccentric action. The mobilizers are fusiform in shape, with a less powerful fibre arrangement, but one which is designed for producing large ranges of motion. In addition, the mobilizers are biarticular muscles, which have their own unique biomechanical characteristics.
Selective changes in muscle may also occur as a result of training (Richardson and Bullock, 1986). In the knee, rapid flexion–extension actions have been shown to selectively increase activity in the rectus femoris and hamstrings (biarticular) but not in the vasti (monoarticular). In this study, comparing speeds of 75°/s and 195°/s, mean muscle activity for the rectus femoris increased from 23.0 uV to 69.9 uV. In contrast, muscle activity for the vastus medialis increased from 35.5 uV to only 42.3 uV (Fig. 5.5). The pattern of muscle activity was also noticeably different in this study after training. At the fastest speeds the rectus femoris and hamstrings displayed phasic (on and off) activity while the vastus medialis showed a tonic (continuous) pattern (Fig. 5.6).
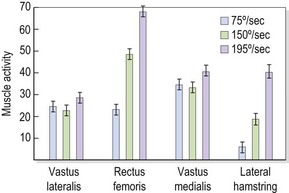
Figure 5.5 Changes in muscle activity with increases in speed.
From Richardson, C.A. and Bullock, M.I. (1986) Changes in muscle activity during fast, alternating flexion–extension movements of the knee. Scandinavian Journal of Rehabilitation Medicine, 18, 51–58. With permission.
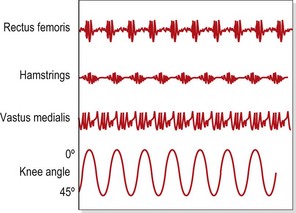
Figure 5.6 Patterns of muscle activity during rapid alternating knee flexion–extension. Biarticular muscles are phasic, monoarticular muscles are tonic.
Redrawn from Richardson, C.A. and Bullock, M.I. (1986) Changes in muscle activity during fast, alternating flexion-extension movements of the knee. Scandinavian Journal of Rehabilitation Medicine, 18, 51–58. With permission.
Even in the more functional closed kinetic chain position, similar changes have been found (Ng and Richardson, 1990). A 4-week training period of rapid plantarflexion in standing gave significant increases in jump height (gastrocnemius, biarticular) but also significant losses of static function of the soleus (monoarticular).
Changes in muscle length
Chronic muscle lengthening
Stabilizer muscles tend to ‘weaken’ (sag) whereas mobilizers tend to ‘shorten’ (tighten). Taking these responses further, primary stabilizers will react quickly to pain and swelling, by inhibition. Swelling has been shown to cause a reflex inhibition of muscles in the knee (de Andrade, Grant and Dixon, 1965; Stokes and Young, 1984). In addition, marked asymmetry of the multifidus has been shown using real-time ultrasound imaging.
Adaptation of primary stabilizers of the spine
Multifidus
The cross-sectional area (CSA) of the multifidus has been shown to be substantially reduced at the level of lumbar lesion (Hides et al., 1994). The authors suggested that the mechanism for the CSA reduction was inhibition through perceived pain via a long loop reflex.
In addition to changes in muscle bulk, alteration in fibre type has been shown in the multifidus in patients with low back pain (LBP) (Biedermann et al., 1991). A reduced ratio of slow twitch to fast twitch muscle fibres was shown, possibly as an adaptive response by the muscle to changes in functional demand placed upon it. Furthermore, injury may have caused a shift in the recruitment patterns of the motor units of the paraspinal muscles, with the fast twitch motor units being recruited before the slow twitch units.
Posture has also been shown to affect the multifidus. In a study of 20 healthy subjects, O’Sullivan et al. (2002) showed a reduction in activity of the multifidus (together with internal oblique and the thoracic erector spinae) in a sway-standing posture, indicating the importance for postural retraining when facilitating the muscle for rehabilitation. Prolonged flexion activities initially result in a reflex spasm of the multifidus, which reduces substantially if the posture is maintained. Williams et al. (2000) used a cat model to investigate sustained moderate flexion stress on seven preparations. They showed a reduction to 5% of this initial value within 3 minutes of taking up the posture, leading to tissue laxity and a loss of reflex protective muscle activity. Prolonged flexion (20 minutes, using cat preparation) has also been shown to result in multifidus spasm (Jackson et al., 2001), with full recovery not seen for 7 hours after initiation of rest.
Injection of hypertonic saline (a chemical irritant that has an effect similar to swelling) into the multifidus has shown that the muscle can be a source of both local and referred pain (Cornwall, John-Harris and Mercer, 2006), and some authors recommend dry needling the muscle in cases of acute low back pain (Gunn, 1996). Retraining of the muscle may be through isolated contraction initially, but successful rehabilitation involves use of the muscle during gross movement (Danneels, Vanderstraeten and Cambier, 2003).
Transversus abdominis
The transversus abdominis shows a similar response in the chronic LBP patient. Normally, this muscle acts as a primary stabilizer of the lumbar spine (Jull, 1994). It is active in both flexion and extension of the lumbar spine (Cresswell, Grundstrom and Thorstensson, 1992) and during action of the upper limb and lower limb in multiple directions (Hodges, Richardson and Jull, 1996). In addition, contraction of transversus abdominis precedes that of the other abdominal and lumbar extensor muscles (Cresswell, Oddsson and Thorstensson, 1994; Hodges and Richardson, 1996). Its primary function would seem to be to contract in response to forces applied to the trunk. In this way it is anticipating the requirement of stability and providing it.
Following LBP, transversus abdominis function changes considerably (Hodges and Richardson, 1995; Hodges, Richardson and Jull, 1996). Timing of onset of transversus contraction is delayed by a mean of 129 ms, while the action of the other abdominals is largely unchanged. When assessed in a hollowing action the transversus muscle shows a smaller increase in thickness measured by real-time ultrasound (between rest and contraction) in patients with low back pain than in normal subjects. Normal subjects showed a mean thickness increase of 49.7% while low back patients showed mean values of 19.15% (Critchley and Coutts, 2002). Re-education of transversus contraction is one important component in low back pain rehabilitation, but reliance on muscle isolation has been shown to be ineffective when compared to more general back stability programmes (see Chapter 14). Even authors who once advocated muscle isolation alone (Hodges and Richardson, 1996) now acknowledge that using this type of action as a primary exercise and then discharging the patient is erroneous (Hodges, 2009).
Quadratus lumborum
The quadratus lumborum (QL) is a muscle which has been described both as a movement muscle tending towards tightness (Janda, 1993) and as an important stabilizer in functional lifting tasks (McGill, Juker and Kropf, 1996). The medial fibres of the muscle connect directly to the lumbar transverse processes, therefore having the potential to stabilize the spine. The lateral fibres run between the ilium and iliolumbar ligament and the 12th rib, spanning the spine and acting as a movement muscle. The muscle is therefore separated into two functional components (Bergmark, 1989). The medial fibres can contribute directly to segmental support of the spine (Richardson et al., 1999), while the lateral portion may tend towards tightness and developing trigger points (Janda, 1993; Gunn, 2000).
The QL has been shown to be an important stabilizer of the spine in side carrying tasks especially (McGill, Juker and Kropf, 1996; McGill, 2000). It is important to note that when the spine fails (buckles) due to compressive loads, it does so laterally in the first instance, so a muscle which resists lateral forces is likely to be an important stabilizer when carrying loads. In addition, the QL functions differently to the erector spinae in forward bending, as it does not demonstrate a flexion relaxation response (Andersson et al., 1996). Whether the muscle reacts to injury and underusage in the same way as the transversus or multifidus is as yet uncertain. Categorization of the medial portion of the muscle as a stabilizer is certain, but sub-categorization into a primary or secondary stabilizer will require more evidence (Bullock-Saxton et al., 2000).
Adaptation of secondary stabilizers
The secondary stabilizer muscles show a tendency to lengthen and weaken. As postural muscles they almost seem to give way to the pull of gravity and ‘sag’. This reaction has been termed stretch weakness (Kendall, McCreary and Provance, 1993). The muscle has remained in an elongated position, beyond its normal resting position, but within its normal range. This is differentiated from overstretch where the muscle is simply elongated or stretched beyond its normal range.
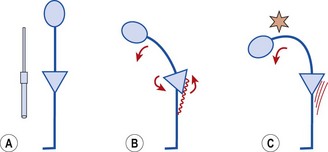
The length–tension relationship of a muscle dictates that a stretched muscle, where the actin and myosin filaments are pulled apart, can exert less force than a muscle at normal resting length. Where the stretch is maintained, however, this short-term response (reduced force output) changes to a long-term adaptation. The muscle tries to move its actin and myosin filaments closer together, and to do this, it must add more sarcomeres to the ends of the muscle (Fig. 5.7). This adaptation, known as an increase in serial sarcomere number (SSN), changes the nature of the length–tension curve.
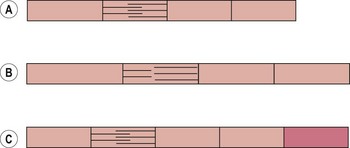
Figure 5.7 Muscle length adaptation. (A) Normal muscle length. (B) Stretched muscle—filaments move apart and muscle loses tension. (C) Adaptation by increase in serial sarcomere number (SSN), normal filament alignment restored, muscle length permanently increased.
Definition
Serial sarcomere number (SSN) is the number of sarcomere units along an individual muscle fibre. Muscles held in a lengthened position for a prolonged period will adapt by increasing their SSN.
Long-term elongation of this type causes a muscle to lengthen by the addition of up to 20% more sarcomeres (Gossman, Sahrmann and Rose, 1982). The length–tension curve of an adaptively lengthened muscle moves to the right (Fig. 5.8). The peak tension that such a muscle can produce in the laboratory situation is up to 35% greater than that of a normal length muscle (Williams and Goldspink, 1978). However, this peak tension occurs at approximately the position where the muscle has been immobilized (point A, Fig. 5.8). If the strength of the lengthened muscle is tested with the joint in mid-range or inner-range (point B, Fig. 5.8), as is common clinical practice, the muscle cannot produce its peak tension, and so the muscle appears ‘weak’. For this reason, manual muscle tests have been described as being more accurate indicators of positional (rather than total) strength (Sahrmann, 1987).
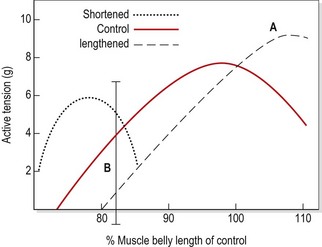
Figure 5.8 Effects of immobilizing a muscle in shortened and lengthened positions. The normal length–tension curve (control) moves to the right for a lengthened muscle, giving it a peak tension some 35% greater than the control (point A). When tested in an inner-range position (point B), however, the muscle tests weaker than normal.
Reprinted from Gossman, M.R., Sahrmann, S.A. and Rose, S.J. (1982) Review of length associated changes in muscle. Physical Therapy, 62 (12), 1799–1808. With permission.
In the laboratory situation the lengthened muscle will return to its optimal length within approximately 1 week if once more placed in a shortened position (Goldspink, 1992). Clinically, restoration of optimal length may be achieved by either immobilizing the muscle in its physiological rest position (Kendall, McCreary and Provance, 1993) and/or exercising it in its shortened (inner-range) position (Sahrmann, 1990). Enhancement of strength is not the priority in this situation; indeed, the load on the muscle may need to be reduced to ensure correct alignment of the various body segments and correct performance of the relevant movement pattern.
Immobilization of cat hind limb in a lengthened position (4 weeks) showed a 19% increase in SSN of the soleus muscle but no change in individual sarcomere length. Immobilizing in a shortened position gave a 40% decrease in SSN, again with no change in sarcomere length (Tabary, 1972). It has been argued that this type of adaptation enables the muscle to develop maximum tension when movement of the muscle is limited (Jaspers, Fagan and Tischler, 1985).
SSN may be partly responsible for changes in muscle strength without parallel changes in hypertrophy (Koh, 1995). SSN exhibits marked plasticity and may be influenced by a number of factors. For example, immobilization of rabbit plantarflexors in a lengthened position showed an 8% increase in SSN in only 4 days, while applying electrical stimulation to increase muscle force showed an even greater increase (Williams et al., 1986). Stretching a muscle appears to have a greater effect on SSN than does immobilization in a shortened position. Following immobilization in a shortened position for 2 weeks, the mouse soleus has been shown to decrease SSN by almost 20% (Williams, 1990). However, stretching for just 1 hour per day in this study not only eliminated the SSN reduction but actually produced nearly a 10% increase in SSN.
An eccentric stimulus may cause a greater adaptation of SSN than a concentric stimulus. Morgan and Lynn (1994) subjected rats to uphill or downhill running, and showed SSN in the vastus intermedius to be 12% greater in the eccentric trained rats after 1 week. In contrast to this, however, Koh and Herzog (1998) used the dorsiflexor muscles of the rabbit to assess the effect of eccentric training on SSN. Using a 2-week training session over a total of 12 weeks, they found little effect on SSN or fibre length, but the variation between the studies may well be related to species or training protocol differences.
Keypoint
Exercising at short muscle lengths reduces serial sarcomere number (SSN), while exercising at long muscle lengths increases SSN.
It has been suggested that if SSN adaptation occurs in humans, strength training might produce this type of change if it is performed at a joint angle different from that at which the maximal force is produced during normal activity (Koh, 1995).
Rather than being weak, the lengthened muscle lacks the ability to maintain a full contraction within inner range. This shows up clinically as a difference between the active and passive inner ranges. If the joint is passively placed in full anatomical inner range, the subject is unable to hold the position. Sometimes the position cannot be held at all, but more usually the contraction cannot be sustained, indicating a lack in slow twitch endurance capacity.
Shortening posturally lengthened muscle
Clinically, reduction of muscle length is seen as the enhanced ability to hold this inner-range contraction. As the muscle is already strong, the focus is not on resistance but on joint position (alignment) and holding time. The muscle is passively positioned within its inner range and the patient is instructed to hold this position. Initially this will not be possible and the limb will fall away from the inner-range joint position. The patient should be encouraged to slow the rate of limb fall to initiate an eccentric contraction. Once this is achieved, the eccentric action is emphasized, with the therapist placing the joint within its inner range and the patient using an eccentric action to guide the limb descent. Over time (sometimes within one treatment session, more normally 2–3 sessions), the patient will be able to hold the inner-range position for a short period of time (seconds only). The next phase in the restoration of muscle balance is to emphasize the inner-range holding ability, building to 10–30 seconds holding. Finally, the patient uses a concentric action to pull the limb into its inner range position, holds using an isometric action, and lowers under control (eccentric). At this point, muscle control through full range has been achieved.
Keypoint
Shortening a posturally lengthened muscle is achieved by working within inner range only. The initial muscle work is eccentric followed by isometric contractions with minimal loading.
Inner-range holding may or may not represent a reduction in SSN, but is a required functional improvement in postural control. Muscle shortening may certainly be achieved through splinting. Muscles immobilized in a shortened position in this way show loss of sarcomeres in series within 14–28 days (Tabary, 1972; Williams and Goldspink, 1978). With training, there is less evidence for reduction in SSN in humans. Muscle shortening has been shown in the dorsiflexors of horse riders. Clearly, this position is not held permanently as with splinting, but rather shows a training response. Following pregnancy, SSN increases in the rectus abdominis in combination with diastasis. Again, the length of the muscle gradually reduces in the months following birth. It is generally thought that inner-range training is likely to shorten a lengthened muscle, although the precise method through which this adaptation is achieved in humans is not certain (Goldspink, 1996). The treatment aim for a posturally lengthened muscle must ultimately be to change its resting length and therefore correct segmental alignment. In so doing the joints within a body region will be able once more to move through an optimal movement range (Sahrmann, 2002).
Inner-range holding ability
The ability of a stabilizer muscle to maintain an isometric contraction at low load over a period of time is vital to its anti-gravity function (Richardson, 1992). This may be assessed by using the classic muscle test position (see Appendix) and asking the subject to maintain a contraction in full inner range (Richardson and Sims, 1991). The important factor in the assessment is the length of time a static hold can be maintained without jerky (phasic) movements occurring. In each case the limb is placed passively into full inner range. When released, if the limb drops, the passive range of motion differs from the active range, which is an important indicator of poor stabilizer function. Full stabilizing function is achieved when a subject can maintain the inner-range position for 10 repetitions, each of 10 seconds duration (Jull, 1994). Often the first two or three repetitions are performed normally, and it is only with further repetition that the deficit becomes apparent.
Tests for the major stabilizing muscles
Tests for the major stabilizing muscles of the trunk, pelvic and shoulder girdle areas, including transversus abdominis, gluteus medius, gluteus maximus, the deep neck flexors and the lower trapezius are described below
Lower limb
Iliopsoas
The iliopsoas (IP) is assessed in the sitting position. The patient flexes the hip while maintaining a 90° knee flexion so that the foot is lifted clear of the ground (Fig. 5.9A). Where the IP is lengthened the thigh may drop down from the inner range position, or more commonly the pelvis is tilted backwards while the knee position is maintained. Backward tilting of the pelvis accompanied by flattening of the lumbar lordosis moves the origin of the muscle away from its insertion and lengthens the IP.
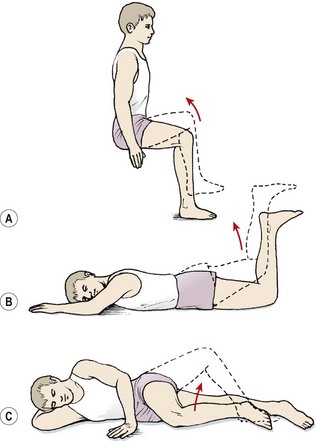
Figure 5.9 Inner-range holding of the lower limb. (A) Iliopsoas. (B) Gluteus maximus. (C) Gluteus medius.
The stabilizing function of psoas major (Gibbons, 2007) may be rehabilitated using a leg shortening action, asking the patient to imagine ‘sucking the hip back into its socket’ (see Chapter 14).
Gluteus maximus
The gluteus maximus is assessed in prone lying with the knee flexed to 90°. Flexing the knee shortens the hamstring muscles, placing them at a physiological disadvantage and making hamstring substitution less likely. The hip is lifted to inner-range extension and held (Fig. 5.9B). In this position, the gluteus maximus may be palpated; often, with a chronic low back pain patient, little activity is noted. Where the muscle is working, it may still not be able to maintain the inner range position over time. Here, the inner range position is held for 1–2 seconds and the limb slowly sinks to a lower position and is held at this mid-range angle. As endurance of the muscle fails, muscle shaking is evident as the large diameter fast twitch fibres of the muscle are used.
Gluteus medius
The gluteus medius is tested in side lying with the knee flexed. The action is combined with hip abduction, with slight lateral rotation to emphasize the posterior fibres of the muscle (Fig. 5.9C). Two starting positions may be used, both with the foot supported to work the limb in closed chain format. In the first the feet are placed together; in the second the foot of the upper leg is placed on the couch at mid-shin level. The action is to keep the foot still and lift the knee while keeping the trunk still. Rotation of the trunk at the pelvis must be avoided. The therapist should monitor the position of the greater trochanter of the upper leg and ensure that it points to the ceiling and does not move forwards or backwards.
Cervical spine
For the cervical spine the essential stabilizers are the deep neck flexors. These are retrained in the supine position using pressure biofeedback, with the cuff placed behind the head or upper cervical spine (Jull, 1994). The aim is to achieve suboccipital rather than lower cervical flexion. The action is a minimal flexion or ‘nodding’ action of the head alone, avoiding forceful actions or lifting the head from the couch.
Overactivity of the superficial muscles with trigger point development is common. The sternomastoid and anterior scalene especially may be shortened in a head held forward (HHF) posture. In addition, tightness and thickening are seen in the splenius capitis and splenius cervicis, as well as the semispinalis capitis and levator scapuli (Gunn, 1996).
Upper trunk
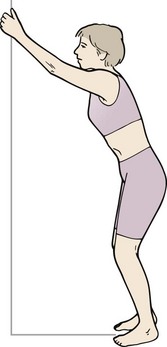
A blanket assessment of scapular stability may be usefully made in prone falling (Fig. 5.10). Slowly lowering (eccentric push-up) will often reveal inappropriate movement of the scapulae in the first phase of the action. The scapulae should remain apart, and firmly fixed to the thoracic wall throughout the movement. Scapular movement outward and upward indicates lack of stability (Janda, 1994). If the scapulae fall together, the rhomboids and levator scapulae are dominant (Kendall, McCreary and Provance, 1993). True winging, apparent through lifting of the medial edge of the scapula, represents serratus anterior inactivity. Retraining scapular stability is covered in Chapter 17 Treatment note 17.1.
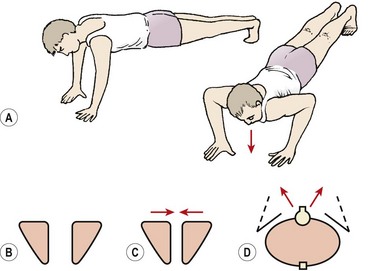
Figure 5.10 Eccentric push-up as a global assessment of scapulothoracic stability. (A) Athlete slowly lowers from a push-up position—note position of scapula. (B) Scapulae should remain apart and fixed to the ribcage as the body is lowered. (C) Scapulae fall together if rhomboids and levator scapulae are dominant. (D) True winging. The medial edges of the scapulae lift.
Lower trunk
Inner range holding of the lower trunk forms the basis of stabilization training and is covered in Chapter 13. A blanket assessment may be made (i) by using an isolation action such as the heel slide, or (ii) by assessing lumbopelvic alignment during whole body tasks. An inability to maintain the optimal alignment of the lumbar spine during whole body movements suggests instability and warrants closer examination. Spinal stabilization is covered in Chapter 13.
Muscle shortening
Mobilizer muscles have long fusiform shapes and, as such, show a tendency to tighten. Tightness in the hamstrings, for example (mobilizers, biarticular), is often seen, while tightness in the gluteals (stabilizers, monoarticular) is rare. As well as reducing range of motion, the tightened muscle is more likely to develop painful trigger points (Travell and Simons, 1983) These are small hypersensitive regions within a muscle which stimulate afferent nerve fibres, causing pain. The sensation created is a deep tenderness with an overlying increase in tone creating a palpably tender band of muscle. When palpated deeply, the trigger point creates a local muscle spasm, giving the ‘jump sign’ (Janda, 1993). The irritability threshold of a tight muscle is lowered, causing it to be activated earlier than normal in a movement sequence. One of the reasons for this is that, being tight, there is less ‘slack’ to take up in the muscle before contraction begins. In addition, the muscle shows an increased afferent input via the stretch receptors (Sahrmann, 1990).
Increased tone within the mobilizer muscle can close down the local capillary bed disrupting blood flow into and out of the working muscle tissue. The result is ischaemic pain which is dull, aching and diffuse in nature, often seen at rest. This is overlaid by the acute trigger point pain which is highly localized and may occur at the initiation of movement and may show a referral pattern (see Fig. 5.35).
Keypoint
Tight mobilizer muscles may develop both ischaemic pain which is dull and diffuse and trigger point pain which is acute, local and may demonstrate a referral pattern.
Tightness of mobilizer muscles is an important factor in muscle balance assessment. Rather than simply range of motion, however, we are interested in a subject’s ability to maintain body segment alignment while the stretch is put on. Using the straight leg raise (SLR) as an example of range measurement for the hamstrings, the point which indicates full range from a muscle imbalance perspective is not necessarily the end of available motion for the leg, but the point at which hamstring tension is sufficiently high to cause the pelvis to tilt (see below).
The lower limb
The tests used to assess muscle length may also be used to stretch a muscle if it is found to be tight. The three key movements to assess restriction of pelvic motion are the modified Thomas test, the SLR and the Ober test. If any movement reproduces the patient’s pain it is relevant, and if the range is significantly less than the optimal value given, the muscle will require specific stretching.
Thomas test
The Thomas test used here is modified from the original test first described by Jones and Lovett (1929). With the modified Thomas test (Fig. 5.11), the patient begins in crook lying at the end of the couch. The knees are brought to the chest and the back flattened to a point where the sacrum just begins to lift away from the couch surface but no further. One leg is held close to the chest to maintain the pelvic position and the other leg is straightened over the couch end. An optimal alignment exists when the femur lies horizontally, and aligned to the sagittal plane (no abduction). The tibia should lie vertically (90° knee flexion) and be aligned with the sagittal plane (no hip rotation), as shown in Fig. 5.11. If the femur rests above the horizontal and the knee is flexed less than 90°, tightness may be present in either the iliopsoas or rectus femoris. If the rectus is tight, straightening the knee will take the stretch off the muscle and the leg will drop down. If the knee is straightened and the leg stays in place, it indicates tightness in the iliopsoas. Deviation of the knee laterally (the ‘J’ sign) indicates a possible tightness in the iliotibial band (ITB), indicating that the Ober test should be performed to confirm the tightness. The Thomas test has been shown to be a repeatable measure using 11 subjects over a sequence of 10 trials (Bullock-Saxton and Bullock, 1994).
Ober test
The modified Ober test (Ober, 1936) begins in side lying (Fig. 5.12). The test assesses the length of the tensor fascia lata (TFL), providing the pelvis remains in a neutral position. In side lying, the lower leg is bent to improve stability and the therapist stabilizes the pelvis to avoid lateral pelvic dipping. The couch should be low enough to allow pressure to be placed through the iliac crest in the direction of the lower shoulder. Maintaining the neutral pelvic position, the hip is abducted and extended to 15°. It is then adducted while maintaining extension. An optimal length for an athlete would be seen when the upper leg is able to lower to couch level. This differs from the original test which was described with the knee flexed. Testing with the knee straight, however, places a greater stretch on the femoral nerve and the rectus femoris, which makes the test less precise. In addition the ITB has a greater stretch placed on it with the knee extended providing the hip remains in extension, as in this position the ITB is stretched over the greater trochanter (Magee, 2002).
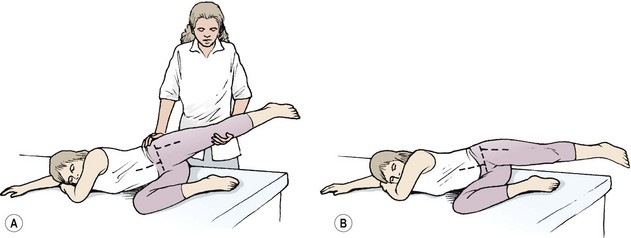
Figure 5.12 Ober test. (A) With pelvis neutral, upper leg should stay in extension and adduct past the horizontal. (B) A false reading is obtained if the pelvis is allowed to tip and the lumbar spine to laterally flex.
Where the TFL may be tight, causing friction syndromes, knee flexion may be added to localize the stretch towards or away from the knee. To differentiate pain in this case from that of neural origin from femoral nerve impingement, the prone knee bend test (PKB) may be used.
Definition
For the prone knee bend (PKB) test, the patient lies on their front, and the examiner flexes the knee maximally on the painful side to provoke pain in the low back, buttock or leg. This indicates an L2 or L3 nerve lesion, or involvement of the femoral nerve itself. Pain must be distinguished from quadriceps tightness.
Where hip extension is limited, the test can still be carried out, but the hip tightness must be assessed further to determine if it is muscular, capsular or osteological in nature.
Hamstring length tests
The hamstrings are assessed by three actions: the straight leg raise (SLR), active knee extension (AKE) and the tripod test.
The SLR test (Fig. 5.13A) is used to assess flexibility of the hamstrings but also as a clinical test for sciatic nerve entrapment. Although useful clinically to determine associated symptoms from neural involvement, the accuracy of the test as a muscle length measure may be questioned (Urban, 1981; Bohannon, 1982). To use the SLR as a muscle imbalance test, the anterior rim of the pelvis is palpated to note the point at which the pelvis begins to posteriorly tilt due to hamstring tightness. This is the point at which a stable base is no longer being provided for the hamstrings to stretch against, and is perhaps more relevant than full passive range pressing against a fully posteriorly tilted pelvis.
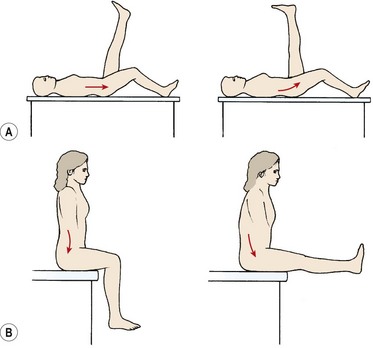
Figure 5.13 Assessing the effect of hamstring tightness on pelvic tilt. (A) Straight leg raise—the beginning of posterior pelvic tilt marks the loss of alignment. (B) Tripod test—as the leg is straightened the pelvis posteriorly tilts.
The AKE test (Fig. 5.14) is performed with the subject lying supine on a couch. The knee and hip are flexed to 90° and held in this position by the subject or therapist. The subject then straightens the leg using quadriceps action and holds the maximum knee extension for 3–5 seconds while the knee angle is measured. This test has been shown to be reliable in both the laboratory (Gajdosik and Lusin, 1983) and in a clinical setting (Norris and Mathews, 2005).
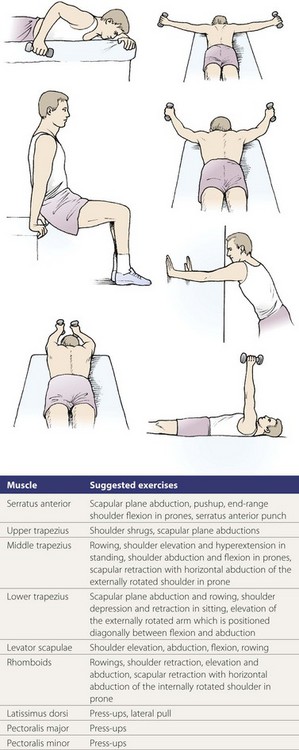
Figure 5.14 Active knee extension (AKE) test of hamstring muscles.
From Norris, C.M. (1999) The Complete Guide to Stretching. With permission from A&C Black Publishers, an imprint of Bloomsbury Publishers Ltd.
The tripod test (Fig. 5.13B) again assesses the interplay between hamstring flexibility and lumbar stability. In the sitting position (feet off the floor), one leg is straightened. Two measures are noted: first, the point at which posterior pelvic tilting occurs, and second, the total range of combined motion at both hip and knee. For optimal performance, the lumbar spine should remain neutral and allow the knee to straighten to within 10° of full extension while the femur remains horizontal.
Stretching tight muscles
Where muscle tightness is found, the test exercises may be used as starting positions for stretching. Before stretching tight muscles, we must ensure that excessive strain will not be placed on adjacent body parts through relative stiffness. This often requires some stability work before beginning the stretch. Passive static stretching is used initially, followed by contract–relax. Finally, the opposing muscles are shortened to full inner range to stretch the antagonist actively.
From the Thomas test position, the hip is flexed slightly and the knee extended against the resistance of limb weight alone. The position is held for 20–30 seconds and the leg is then lowered to a new stretched position. The opposing knee must remain tightly gripped to the chest to ensure the posterior pelvic tilt is maintained throughout the exercise. An alternative exercise to stretch the hip flexors while re-educating spinal stability is the half lunge (Fig. 5.15A). The half-kneeling position is taken up, with one hand placed on a chair to aid balance, the other pressing into the lumbar spine on the side of the dependent leg. The abdominal hollowing procedure is performed and is held throughout the exercise to maintain a neutral position of the lumbar spine. To impart the stretch, the body lunges forwards, forcing the dependent hip into extension while avoiding increasing the lordosis.
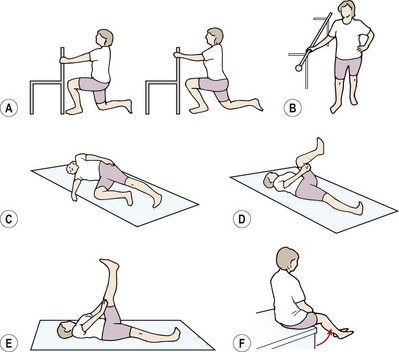
Figure 5.15 Hip flexibility exercises. (A) Half lunge. (B) Hip hitching in standing. (C) Hip hitching is maintained (pull pelvis up against hand) as upper leg is lowered into adduction. (D) Active knee extension (holding thigh). (E) Active knee extension (press thigh against hand). (F) Active knee extension in sitting—the tripod test.
In the Ober test position, the iliotibial band (ITB) is stretched. However, this exercise is only effective if the subject is able to stabilize the pelvis against frontal movement by maintaining a contraction of the quadratus lumborum and ipsilateral obliques. To re-educate this action, the subject is first taught a hip-hitching action in standing (Fig. 5.15B) to be repeated in lying. Finally, hip-hitching is performed and the subject maintains the contraction of the trunk side flexors on the side of the upper leg, as this leg is lowered into adduction and slight extension (Fig. 5.15C).
The hamstrings are initially stretched in the SLR test position. Exercise one (Fig. 5.15D) is the active knee extension (AKE) manoeuvre, where the upper leg is held in 90° hip flexion and the leg is straightened. An alternative is to straighten the leg in 160° hip flexion and then actively pull the straight leg up to 90° hip flexion without allowing the knee to bend (Fig. 5.15E). This combines inner-range shortening of the hip flexors with lengthening of the hip extensors.
Finally, the tripod test position combines lumbar stability with mobilizer lengthening in a functional starting position (Fig. 5.15F). The subject begins sitting on the edge of a couch with the feet off the floor. An upright sitting posture is taken with the lumbar spine in its neutral position. This position is maintained throughout the exercise by performing abdominal hollowing. The leg is now straightened to stretch the hamstrings against the stable base of the unmoving pelvis.
Longer periods of stretching are generally recommended, with holding times of 30 seconds being optimal. Some authors, however, recommend even longer holding times for combining stretch of the shortened muscle with shortening of the lengthened muscle. Using the tripod stretch position above, the patient would be instructed to sit with the back slightly lordosed (hollow) using minimal contraction of the erector spinae to anteriorly tilt the pelvis. They would then extend the knee to the point where tightness is felt and support the heel on a low stool. This low level stretch would be maintained for 20–30 minutes and repeated six times throughout the day (Sahrmann, 2002). Obviously, patient compliance is a large factor with this type of intervention, so the method of functional stretching must be built into a patient’s daily living. The stretch above, for example, may be given as an adaptation of the normal sitting position for an office worker.
The upper limb
Neck side flexion combined with other movements is a key movement for the trapezius, sternomastoid and anterior scalenes (Fig. 5.16).
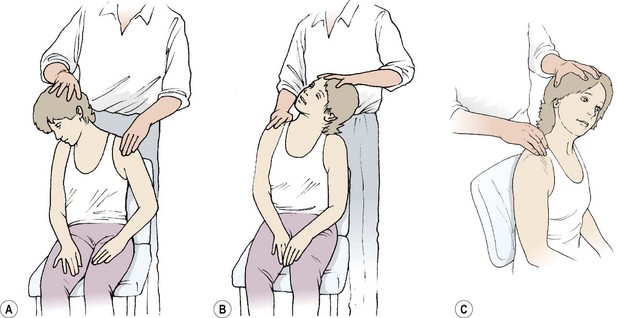
Figure 5.16 Neck side flexion tests. (A) Trapezius and levator scapulae (see text). (B) Sternomastoid. (C) Anterior scalene.
Upper trapezius and levator scapulae
The upper trapezius may be tight if the scapula is held in a downwardly rotated position. However, more normally the upper trapezius is hypertonic, its overactivity trying to compensate for underactivity of the lower trapezius and serratus anterior. Stretching consists of side flexion away from the tight muscle, combined with neck flexion. For this to be effective the scapula must be fixed. Clinically, many patients with an overactive upper trapezius also present with neck pain. For this reason scapular fixation is normally used as overpressure, rather than neck movements which would throw stress onto the painful cervical spine. To stretch the right muscle, the patient sits on a chair and elevates the right scapula. The patient then flexes the cervical spine and laterally flexes it to the left. This neck position is held by reaching over the head with the left arm and hand. Maintaining the cervical position, the right scapula is depressed and retracted to place the stretch on the muscle. Painful trigger points are often found within the upper trapezius muscle at the highest point of the muscle belly.
The levator scapulae is stretched using a similar movement, but this time adding rotation away from the muscle being stretched (in this case rotate to the left). A trigger point is often present in the levator scapulae, and this can be found by palpating the superior angle of the scapula and tracing the muscle distally from this point towards the upper cervical spine.
Sternomastoid
The sternomastoid is stretched by combining side flexion away, and rotation towards, the muscle being tested. Where the right sternomastoid is stretched, the head is turned to the left and side flexed to the right. Painful trigger points may be found in the centre of the muscle, level with the Adam’s apple (laryngeal prominence).
Anterior scalene and rhomboids
The anterior scalene is stretched initially by manual pressure on the first rib combined with side flexion away from the muscle. Further stretch is placed on the muscle by rotating towards the muscle and extending the lower cervical spine by performing a full chin-tuck action. The rhomboids are stretched by actively stabilizing the scapula and flexing the arms to 90° and protracting. The arms are then crossed to the elbows. Trigger points for the anterior scalene muscles lie over the anterior aspect of the neck, close to the clavicle, and for the rhomboid muscles along the medial edge of the scapula.
Pectoralis major and minor
In supine lying, the pectoralis major and minor and latissimus dorsi may be tested (Fig. 5.17). When lying supine, the posterior border of the acromion should rest no more than 2–3 finger breadths above the surface of the couch. A greater gap, combined with resistance to posterior shoulder girdle glide and painful direct palpation, represents tightness in the pectoralis minor. Trigger points may be located by palpating the corocoid process and tracing the muscle distally towards the upper ribs.
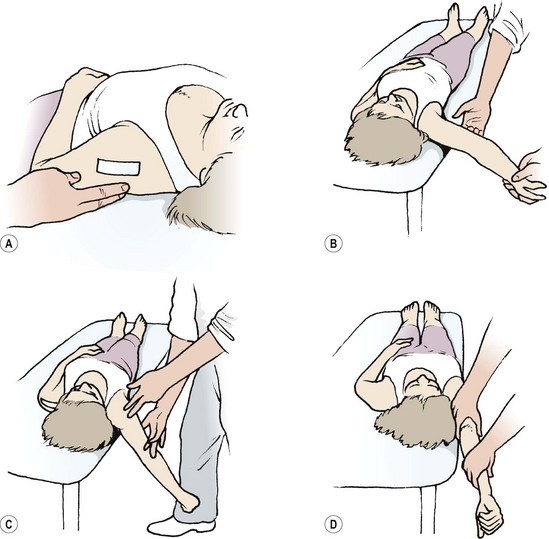
Figure 5.17 Supine lying tests. (A) Pectoralis minor. (B) Pectoralis major (sternal portion). (C) Pectoralis major (clavicular portion). (D) Latissimus dorsi.
The pectoralis major is assessed by arm abduction. The sternal portion of the muscle is assessed with the arm at 120° abduction. When released, it should rest level with the couch. The clavicular portion is evaluated by lowering the arm over the couch side into extension/abduction: 80–90° extension is the norm. Painful trigger points are often found along the lateral edge of the muscle with the arm placed in an abducted position.
Latissimus dorsi
Latissimus dorsi is stretched by taking the arm overhead into flexion/abduction to couch level. In addition, latissimus dorsi may be stretched in standing. The back is flattened against the wall and the shoulder flexed, adducted and externally rotated (Koala stretch). In sport, a more useful stretch is to hold onto a piece of apparatus above shoulder level and flex the knees and hips to stretch the latissimus and traction it simultaneously (Fig. 5.18). Trigger points may be found within the muscle but more commonly they are located at the insertion of the muscle into the iliac crest.
Posture
Why posture is important
The combination of altered muscle length and function will be noticeable as a change in body alignment to both static (posture) and dynamic (segmental control) assessment. When standing the body exists in elastic equilibrium (Scannell and McGill, 2003) the pull of soft tissues on either side of the body cancelling each other out. Passive tissue tension on either side of a joint will amount to a zero moment; that is, no combined leverage effect. This is the position of least strain, with minimal joint loading, and minimal muscle work required to maintain it. Deviation from this optimal alignment moves the body away from equilibrium and so joints are subjected to greater force, and to off-load this force additional muscle work is required. Sustained stress of this type leads to strain accumulation which may exceed the strain tolerance of tissue leading ultimately to tissue failure. All tissues are able to tolerate a certain amount of strain before they fail. Healthy tissue being more elastic is able to tolerate greater imposed loads than pathological tissue. Sub-optimal posture is therefore an important component of both injury prevention and injury management.
Postural assessment
Standing posture is assessed in comparison to a standard reference line or plumb-line (Kendall, McCreary and Provance, 1993). The plumbline acts as a guide for the clinician’s eye, making deviation from optimal alignment more obvious. The clinical usefulness of the vertical line may be enhanced by using a posture grid. The subject is positioned with a plumb-line passing just in front of the lateral malleolus. In an ideal posture, this line should pass just anterior to the mid-line of the knee, and then through the greater trochanter, bodies of the lumbar vertebrae, shoulder joint, bodies of the cervical vertebrae, and the lobe of the ear (Fig. 5.19).
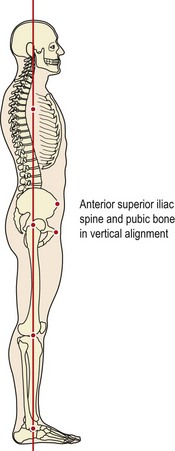
Figure 5.19 The standard reference line for posture.
After Kendall, F.P., McCreary, E.K. and Provance, P.G. (1993) Muscles. Testing and Function, 4th edn. Williams and Wilkins, Baltimore. With permission.
When viewed from the front, with the feet 3 inches apart, the line should bisect the body into two equal halves. The anterior superior iliac spines (ASIS) should be approximately in the same horizontal plane, and the pubis and ASIS should be in the same vertical plane (Kendall, McCreary and Provance, 1993). This alignment defines the neutral lumbopelvic alignment as one of 5° to the horizontal.
Anatomical landmarks are compared for horizontal level on the right and left sides of the body, and include the knee creases, buttock creases, pelvic rim, inferior angle of the scapulae, acromion processes, ears and the external occipital protuberances. In addition, the alignment of the spinous processes and rib angles are observed, with minor scoliosis becoming more evident when assessed in Adam’s position. The distance between the arms and the trunk (keyhole), skin creases and unequal muscle bulk are indicators of asymmetry requiring closer examination. Foot and ankle alignment are also assessed.
When compared to this standard line, four major posture types are commonly seen (Fig. 5.20): lordotic, sway back, kyphotic and flat back. Subjects often exhibit a combination of these types (for example kypho-lordotic) and sub-groups exist (for example flexible or rigid kyphotic). However, clinically it is the major deviations from optimal which are important, more minor changes being better tolerated. These deviations may exist through changes in muscle length and tone, habitual carriage (posture holding) or pathology and once described may require further investigation.
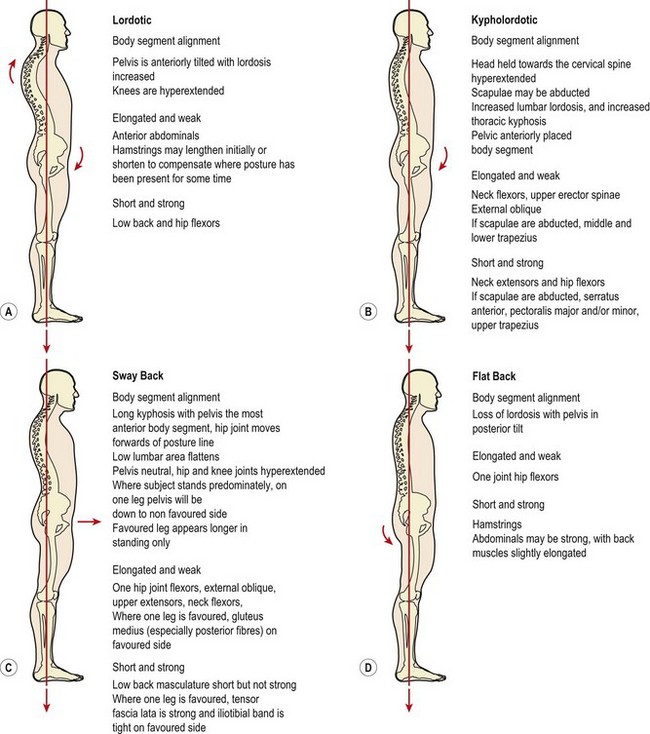
Figure 5.20 Posture types and muscle imbalance. When a subject is viewed from the side and compared to a standard posture line, four main posture types may be found. These are associated with shortened and lengthened muscles as shown.
After Kendall, McCreary and Provance (1993). Muscles. Testing and Function, 4th edn., Williams and Wilkins, Baltimore. With permission.
Lordotic posture
In the lordotic posture, anterior pelvic tilt is excessive. The abdominal muscles and gluteals are typically lengthened and of poor tone. The hip flexors may shorten if the posture has existed for some time. End range pelvic tilt is limited (unloaded) by overactivity and eventually tightness in the hamstring muscles. In an extreme lordotic posture, seen in chronic obesity, the lumbar spine rests in extension with the lumbar facet joints impacted and the elastic recoil of the hamstrings allowing the pelvis to hang. This posture equates with the pelvic crossed syndrome described by Janda and Schmid (1980). With obesity, the deep abdominal muscles become stretched and the viscera move forwards and downwards (visceral ptosis). In so doing they move anterior of the posture line (the gravity line), increasing the leverage acting upon them and effectively making them ‘heavier’. The combination of weight and leverage forces acting on the viscera makes the act of visceral compression by the deep abdominal muscles harder.
The lordotic posture is commonly seen in sport in young gymnasts and dancers where it is flexible. In addition, it is the posture most noticeable after childbirth due to muscle lengthening and habitual carriage and during obesity where it may be more rigid.
Keypoint
The lordotic posture may vary depending on the conditions which formed it. In sport (dance/gymnastics) muscle tightness may predominate. Following childbirth the habitual carriage combines with abdominal muscle lengthening. In morbid obesity muscle laxity exists combined with chronic joint loading.
Sway back posture
In the sway back posture the pelvis remains level, but the hip joint is pushed forward of the posture line. The hip is effectively extended, lengthening the hip flexors, and the body ‘hangs’ on the hip ligaments. The lordosis is now longer and more shallow than in the lordotic posture, and may extend up to the mid-thoracic spine. In addition, there is typically a noticeable crease where the direction of movement changes at a single spinal level, rather than through several, as is the case with the lordotic posture. A patient with this posture will often be able to point to the exact point of pain which normally occurs after prolonged standing.
The sway back posture may be combined with dominance of one leg in standing (‘hanging on the hip’), especially in the adolescent. Now, weakness in the gluteus medius allows the pelvis to tip laterally, a situation partially compensated by increased tone in the tensor fascia lata. Shortening is seen in the iliotibial band (ITB), with a prominent groove apparent on the lateral aspect of the thigh.
Flat back posture
With the flat back posture, the main problem is lack of mobility in the lumbar spine and a flattening of the lordosis. This posture reflects the extension dysfunction described by McKenzie (1981). The pelvis may be posteriorly tilted in comparison to the reference line, and the lumbar tissues are often thickened and immobile.
Flattening associated with repeated flexion movements of the trunk (manual handling) will show more mobility to flexion in the upper lumbar spine. Flattening associated with prolonged sitting will show greater flexion mobility in the lower lumbar spine.
Kyphotic posture
In the kyphotic posture, the shoulder joint moves anteriorly to the posture line and the thoracic kyphosis is increased. A number of pathological conditions may give rise to this condition (Table 5.2), and these should be differentiated from simple soft tissue imbalance.
Table 5.2 Pathological conditions giving rise to kyphotic posture
| Congenital abnormalities |
Source Magee (2002).
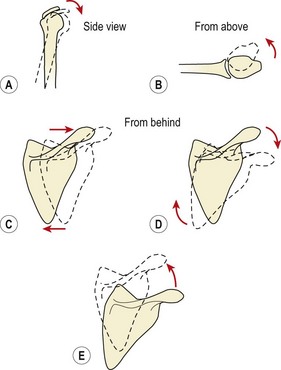
In an optimal upper body alignment (Table 5.3), the scapulae should be approximately three finger breadths from the spine and the medial borders of the scapulae should be vertical. Optimal positioning of the shoulder is assessed by comparing the head of the humerus in relation to the acromion process. In optimal positioning, no more than one-third of the humeral head should be anterior to the point of the acromion. The humerus should be held with the cubital fossa at 45° to the sagittal plane in relaxed standing. A greater angle than this indicates excessive medial rotation, indicative of tightness in the medial rotators (especially the pectoralis major) and lengthening of the lateral rotators.
Table 5.3 Alignment of the shoulder girdle
| From behind | From the side |
|---|---|
| Medial border of scapula vertical | Line from ear canal to centre of shoulder joint |
| Medial border of scapula no more than three finger breadths from the spinous processes | No more than one third of head of humerus anterior to acromion |
| Spine of scapula T3/T4 level, inferior angle at T7 | Humerus held with cubital fossa 45° to sagittal plane |
| Scapula flat against chest wall |
Deviation from this ideal is often described as a ‘round shouldered’ posture, a blanket term which covers a number of scenarios. Tightness in the anterior structures will pull the shoulder forwards, away from the posture line. The weight of the arm moves further from the centre of gravity of the upper body, dramatically increasing the leverage forces transmitted to the thorax. Eventually, the thoracic kyphosis will increase as a result. Tightness in the pectoralis minor pulls on the coracoid process tilting the scapula forwards superiorly (Fig. 5.21A). Tightness in the pectoralis major causes a combination of excessive medial rotation at the glenohumeral joint with anterior displacement of the humeral head (Fig. 5.21B). Excessive abduction of the scapula (Fig. 5.21C) and downward rotation (Fig. 5.21D) may result from lengthening of the lower trapezius and serratus anterior. Excessive elevation and upward rotation (Fig. 5.21E) may result from tightness in the upper fibres of trapezius.
Segmental control
Segmental control is the ability to dissociate the movement of one body segment from that of a neighbouring segment. It is dependent on stabilization ability and adequate mobilizer length. Where imbalance exists, lengthened muscle will fail to act sufficiently and will be dominated by shortened overactive movement muscles. This imbalance leads to an alteration in the movement pattern controlled by the muscles, giving subtle changes seen on examination. The quality of the patient’s movement changes making movement less efficient. Subjectively we can say that movement is sub-optimal or incorrectly executed. The patient’s action may be described as a movement dysfunction.
Definition
Segmental control is the ability to dissociate the movement of one body segment from another. It is dependent on stabilization ability and adequate mobilizer length.
The central features of segmental control require the pelvis to tilt independently of the lumbar spine in both frontal and sagittal planes, the shoulder girdle and thoracic spine to move in relation to each other, and the upper and lower portions of the cervical spine to move in a controlled fashion.
Treatment note 5.1 Therapist posture during treatment
Posture is normally seen from the perspective of the patient, either being part of their condition or their treatment. However, posture has another important aspect, that of the therapist’s health. Treatments carried out in a suboptimal posture over a period of time can result in musculoskeletal pain in the therapist.
In a study of physical therapists (PTs), over 62% had complained of back pain in the last year and of those, nearly 8% had been prevented from working by this (Cromie, Robertson and Best, 2000). In addition, 36% of PTs with musculoskeletal pain reported that maintaining a position for a prolonged time (for example massage) made their pain worse (Holder et al., 1999). Optimizing therapist posture is therefore a primary consideration before treatment begins.
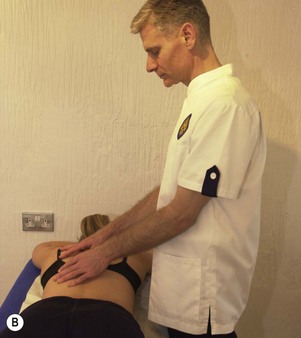
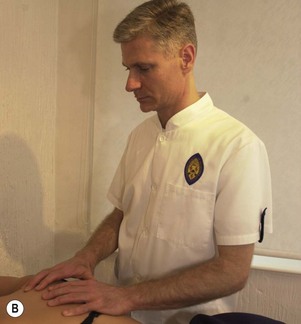
Low back
Maintaining lumbopelvic alignment is the key to safer treatment from the point of view of the therapist’s low back. The lumbar lordosis should be preserved and prolonged flexion avoided. The first factor in achieving this is to adjust the couch height to the correct level for the height of the therapist and to adjust it as the treatment techniques vary. For example, cervical techniques may require a high couch level (Fig. 5.22A) and lumbar techniques (Fig. 5.22B) a low level. Forgetting to adjust the couch between treatments may place considerable stress on the spine.


When the therapist has to lean over the couch, placing the knee on the couch surface will serve to support the spine and reduce leverage effects (Fig. 5.23). In addition, standing close to the couch rather than at a distance will reduce leverage and allow some of the weight to be supported by the couch itself (Fig. 5.24).



Thoracic spine
The major factor in the thoracic spine is scapular abduction and thoracic flexion. This occurs particularly with mobilization techniques on a low couch (Fig. 5.25) where upper body alignment is lost. The aim should always be to ‘think tall’ and extend the thoracic spine while drawing the scapulae down and in (depression and retraction).

Another factor in the upper body is overactivity in the upper portion of the trapezius muscle. This can occur when holding the arms away from the sides of the body and allowing the point of the shoulder (acromion process) to creep upwards towards the ear (Fig. 5.26). The aim should be to maintain the distance between the shoulder and ear and to keep the upper trapezius more relaxed.


Cervical spine
In the cervical spine, the chin should be drawn in slightly to avoid a forward head posture (Fig. 5.27). This posture commonly occurs when the therapist is focusing closely on a small object. Intense concentration leads to loss of cervical alignment which may ultimately cause tension headaches.

Lumbopelvic rhythm
The combination of movements of the hip on the pelvis and the lumbar spine on the pelvis increases the range of motion of this body area. In forward flexion in standing, for example, when the legs are straight, movement of the pelvis on the hip is limited to about 90° hip flexion. Any further movement, allowing the subject to touch the ground, must occur at the lumbar spine. In this example the body is acting as an open kinetic chain and the pelvis and lumbar spine are rotating in the same direction. Anterior tilt of the pelvis is accompanied by lumbar flexion (Fig. 5.28A). In the upright posture, the foot and shoulders are static and so spinal movement acts in a closed kinetic chain. In this situation, movements of the pelvis and lumbar spine (lumbopelvic rhythm) occur in opposite directions (Fig. 5.28B). Now, an anteriorly tilted pelvis is compensated by lumbar extension to maintain the head and shoulders in an upright orientation. The relationship between various pelvic movements and the corresponding hip joint action is shown in Table 5.4.
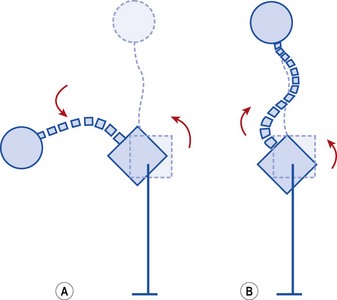
Figure 5.28 Lumbopelvic rhythm. (A) Lumbopelvic rhythm in open chain formation occurs in the same direction. Anterior pelvic tilt accompanies lumbar flexion. (B) Lumbopelvic rhythm in closed kinetic chain formation occurs in opposite directions. Anterior pelvic tilt is compensated by lumbar extension.
From Norris, C.M. (1995b) Spinal stabilisation, 2. Limiting factors to end range motion in the lumbar spine. Physiotherapy, 81, 4–12. Chartered Society of Physiotherapy. With permission.
Table 5.4 Relationship of pelvis, hip joint, and lumbar spine during right lower-extremity weight-bearing and upright posture
| Pelvic motion | Accompanying hip joint motion | Compensatory lumbar motion |
|---|---|---|
| Anterior pelvic tilt | Hip flexion | Lumbar extension |
| Posterior pelvic tilt | Hip extension | Lumbar flexion |
| Lateral pelvic tilt (pelvic drop) | Right hip adduction | Right lateral flexion |
| Lateral pelvic tilt (hip hitch) | Right hip abduction | Left lateral flexion |
| Forward rotation | Right hip MR | Rotation to the left |
| Backward rotation | Right hip LR | Rotation to the right |
MR − medial rotation, LR − lateral rotation. From Norkin, C.C. and Levangie, P.K. (1992) Joint Structure and Function, 2nd edn. FA Davis, Philadelphia. With permission.
For lumbopelvic rhythm to function correctly, hip flexion total movement range should be greater than lumbar flexion total range. In addition it should occur first during functional activities. In subjects where there is a history of back pain, however, the reverse situation often occurs, leading to stress through repeated flexion of the lumbar spine. In low back pain (LBP) patients’ muscle action during pelvic tilting has been shown to change, with the duration of gluteus maximus contraction significantly reduced (Leinonen et al., 2000). The ratio of lumbar spine movement on the pelvis (L) to pelvic movement on the hip (H) has also been shown to change with LBP. This ratio (L/H ratio) should be 2 : 1 at initiation of flexion changing to 1 : 1 at mid range bending and reversing to 1 : 2 at full end range (Esola et al., 1996). The movement range is similar with LBP patients, but the pattern of muscle work is altered showing greater electrical activity in the hamstrings and lower activity in the gluteal muscles (Mooney and Robertson, 1976; Leinonen et al., 2000).
In the lower trunk, the ability to dissociate lumbar movement from pelvic movement is clinically important, and is often lost in the chronic LBP patient. Three exercises are used to assess lumbopelvic rhythm: standing hip flexion, kneeling sit-back and the hip hinge.
Keypoint
During forward bending two motions occur, anterior pelvic tilt and spinal flexion. In patients with LBP, tightness in the hamstrings may delay the onset of pelvic tilt, altering the timing of this action rather than the total motion range.
Standing hip flexion
In the first (Fig. 5.29), the subject stands side on to a wall-bar for support. Hip flexion is then performed to beyond 90°. The movement should ideally occur in three phases. Initially, there should be no pelvic movement, with phase I consisting of hip flexion alone. During phase II the pelvis should begin to posteriorly tilt but the lumbar spine movement should not be excessive. In phase III no further hip or pelvic movement is available and the final position is obtained by lumbar flexion alone. Where control of lumbopelvic rhythm is poor, lumbar flexion often occurs early in phase I, with thoracic movement noticeable as the subject dips the chest downwards towards the knee. Once detected, this same movement is used to re-educate pelvic control, with the subject actively stabilizing the pelvis and initially performing hip flexion to only 10–20°.
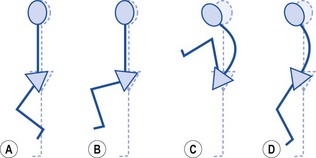
Figure 5.29 Lumbopelvic rhythm: standing. (A) Hip flexes, no pelvic or lumbar movement. (B) Posterior rotation of pelvis begins as hip approaches 90°. Lordosis flattens. (C) Maximum hip and pelvic motion. Lumbar flexion completes movement. (D) Incorrect: pelvic rotation and lumbar flexion occur immediately.
Kneeling sit back
Lumbopelvic rhythm is further assessed in prone kneeling (Fig. 5.30). From this position the subject sits back onto the ankles. Again, the action should occur in three phases. In phase I no lumbar or pelvic movement should occur. In phase II hip, pelvis and lumbar spine should all move, and in phase III lumbar flexion and some thoracic flexion finishes the action. Faulty lumbopelvic rhythm often shows up as lumbar flexion occurring immediately.
Hip hinge
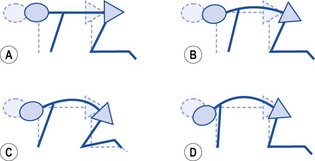
The hip hinge movement is the final action (Fig. 5.31), and the most important in terms of function as it mimics the bending action used in daily living activities. The L/H ratios for early (0–30°), middle (30–60°) and late (60–90°) forward bending should remain at 2 : 1, 1 : 1 and 1 : 2, respectively. There is therefore an increase in the contribution of pelvic tilt (pelvis moving on the hip) to forward bending as the action proceeds. A reduction in the contribution of pelvic tilt to the total range of forward bending leads to earlier lumbar motion in the activities of daily living (ADL). This in turn may increase the repetitive stress imposed on the low back tissues and could be an important factor in the re-occurrence of low back pain.
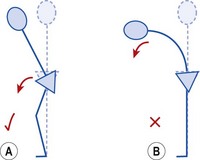
Figure 5.31 Hip hinge movement. (A) Correct: knees unlock, pelvis rotates anteriorly. Neutral lumbar position maintained. (B) Incorrect: pelvis fixed, flexion occurs to spine only.
The hip hinge test measures the subject’s ability to isolate pelvic motion from that of the lumbar spine. Initially, forward flexion is assessed, and the relative contribution of anterior pelvic tilt to this movement is important. With normal lumbopelvic rhythm, anterior pelvic tilt reduces the amount of lumbar flexion required to reach downwards to waist height. Where pelvic tilt is limited, greater lumbar flexion is required, and throughout the day the number of lumbar flexion movements is greatly increased, leading to accumulated stress on the body tissues in this area. The subject is retrained to maintain the neutral lumbar position and flex the hip on the fixed foot. To release tension from the hamstrings, the knees should be slightly unlocked as the movement begins.
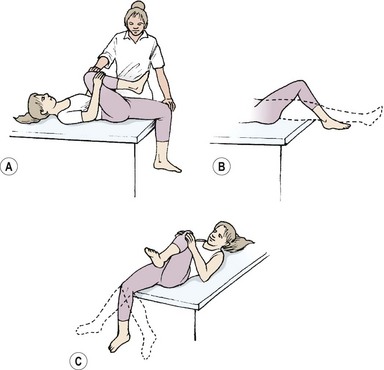
Pelvic motion in the frontal plane
Pelvic motion control in the frontal plane represents the Trendelenburg sign (see Fig. 7.10). When the bodyweight is supported on one leg, the hip abductors (mainly gluteus medius) of the supporting leg work to prevent the pelvis dipping. Their action, combined with that of quadratus lumborum of the contralateral leg, can dip the pelvis upwards on the free leg side, effectively adducting the hip on the supporting side. Where these muscles are unable to hold an inner-range contraction, the pelvis is seen to dip downwards towards the lifted (non-weight-bearing) leg, effectively adducting the weight-bearing limb.
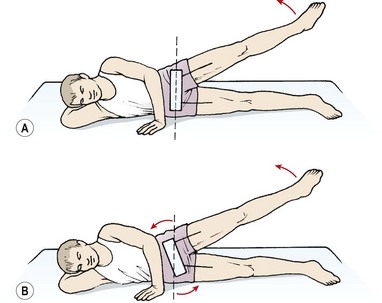
In the non-weight-bearing situation, inactivity of the gluteus medius shows as a false hip abduction movement. Normally, when the upper leg is lifted from side lying, the pelvis remains level and the hip moves on this stable base (Fig. 5.32). When the hip abductors are weak following hip pathology for example, the subject is unable to abduct the leg correctly. Instead, the pelvis is laterally tilted through the action of the trunk side flexors. Although the leg lifts, the relationship between the femur and pelvis remains unchanged, with close inspection showing the movement isolated to the lower spine.
The cervical and thoracic spines
Observation of segmental control of the cervical spine is used to differentiate the region into two functional areas: suboccipital and lower cervical (Fig. 5.33).
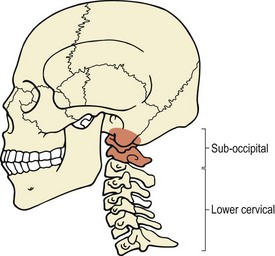
Definition
The suboccipital region consists of the occiput of the skull with the first and second cervical vertebrae (C1 and C2). The lower cervical region is made up of the remaining cervical and first thoracic vertebrae (C2 to T1).
Cervical spine
Protraction (chin poking forwards) and retraction (chin tucked in) of the head will change the orientation of the cervical spine. In protraction the suboccipital region is extended, and the lower cervical region flexed. The opposite occurs in retraction, with the suboccipital region flexed and the lower cervical region extended. A posture in which the head is held protracted or retracted rather than in a neutral position will govern cervical motion during other movement ranges.
As flexion is initiated, movement should occur in the upper cervical spine first. Where a protracted head posture is present, the lower cervical spine will often move first, with the upper region remaining extended in a lordosis (Fig. 5.34). As extension is performed, the head should move back over the shoulders before the upper cervical spine extends, indicating that both the upper and lower regions of the cervical spine are moving. If the head pivots to initiate the movement, extension may be limited to the upper region alone. If this occurs, a further test is to assess the degree of head retraction, which should show the ability of the lower cervical spine to extend.
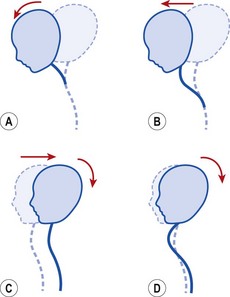
Figure 5.34 Movement of the cervical spine. (A) Upper cervical flexion—axial rotation. (B) Lower cervical flexion, upper extension with translation of joints. (C) Extension occurs in upper and lower cervical region. (D) Extension in upper cervical region only.
During rotation, the movement should be pure and accompanied by only slight lateral flexion. Excessive lateral flexion indicates a possible tightness in the levator scapulae and/or the scalenes. If these muscles are tight and are limiting rotation, shrugging the shoulders (and so relaxing the muscles) will increase the available range of rotation.
Thoracic spine
The thoracic spine is assessed with the subject sitting over the couch end. The subject should be able to reverse (flatten) the thoracic kyphosis as extension is attempted. Where movement is limited, differentiation should be made between a fixed kyphosis and a flexible kyphosis. Fixed kyphosis is osteological with osteoporosis and osteoarthritis being common causes. A flexible kyphosis occurs through muscle changes where the scapulae are protracted and the arms drawn forwards.
Rotation movements should be symmetrical. Emphasis is placed on the upper thoracic region when thoracic rotation is combined with cervical rotation. The mid-thoracic region is tested with the arms folded, while the lower thoracic region is emphasized by placing the patient’s arms overhead and pulling through the thoracolumbar fascia.
Restoration of muscle balance
Three elements combine to restore muscle balance: correction of muscle length, increasing core stability and correction of segmental control. The order in which these are used will depend on the patient’s symptoms, and will often be governed by pain rather than alignment. For example where a tight muscles is causing pain, this will be targetted first. If excess motion at the lumbar spine is causing overuse injury, stability may be chosen first to limit stress on inflamed tissue.
Muscle length
Tight muscles may inhibit their antagonists (Jull and Janda, 1987) and often develop painful trigger points. This is especially the case in the upper limb (Fig. 5.35). A trigger point (myofascial trigger point) is often located within a tight band of muscle. The point is painful to palpation and the muscle will often go into spasm if the trigger point is palpated briskly or flicked (the jump sign). For more information on trigger point pathology and treatment see Norris (2001).
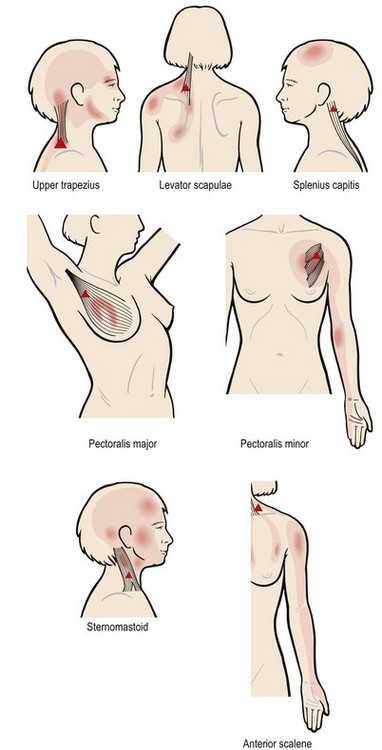
Figure 5.35 Trigger points within hyperactive upper limb muscles.
From Petty and Moore (2001) with permission.
Definition
A trigger point (TrP) is a highly sensitive local area within a taut band of muscle fibres. TrPs are thought to result from: (i) muscle ischaemia, (ii) a hyperactive muscle spindle, (iii) excessive release of acetylcholine at the muscle motor end plate.
Furthermore, through relative flexibility, a tight muscle will throw stress onto a hyperflexible body segment causing tissue stress and pain. Elimination of tightness and redevelopment of stability, coupled with correction of segmental movement, is therefore a key aim of treatment.
Where pain is a prominent factor, the elimination of this pain may be the primary aim of treatment. Pain which occurs through muscle spasm, or through trigger points in tight muscle, may be relieved by treatment aimed at reducing muscle tone. This can be achieved by modalities or manual therapy, and will often involve the use of stretching (Table 5.5).
Table 5.5 Methods of treating trigger points
| Electrotherapy |
Stability
Where pain is the result of persistent over stress on a hypermobile segment, the initial treatment should be aimed at segmental control and stability. Stability may have to be applied passively at first (through taping or splinting) until sufficient control of the muscular stabilizing system has been gained. Core stability itself is divided into three overlapping phases: muscle isolation, restoration of back fitness and functional actions. For full details of back stability rehabilitation programmes see Norris (2008).
Segmental control
Finally, where the tissues themselves are normal, but poor alignment has become habitual (particularly in adolescent athletes), coordination and alignment training may be all that is required. This will necessitate close inspection and regular feedback, and the use of a video in these cases is of great value.
Proprioceptive training
Background to proprioceptive training
Proprioception has been defined as a specialized variation of touch encompassing the sensations of both joint movement and joint position (Lephart and Fu, 1995). Practically, it is the ability of the body to use position sense and respond (consciously or unconsciously) to stresses imposed on the body by altering posture and movement (Houglum, 2001).
Definition
Proprioception is the awareness of the body in space. It is the use of joint position sense and joint motion sense to respond to stresses placed upon the body by alteration of posture and movement.
Proprioception encompasses three aspects, known as the ‘ABC of proprioception’. These are: agility, balance and coordination. Agility is the capacity to control the direction of the body or body part during rapid movements, while balance is the ability to maintain equilibrium by keeping the line of gravity of the body within the body’s base of support. Coordination is the smoothness of an activity. This is produced by a combination of muscles acting together with appropriate intensity and timing (Houglum, 2001).
Proprioceptive exercise is progressed in terms of skill and complexity rather than pure overload. The aim is to perform gradually more challenging actions while maintaining movement accuracy. The emphasis therefore is on quality of motion rather than quantity (volume) of muscle work.
Proprioception and injury
During acute injury, proprioception may play a protective role by reflex muscular splinting. The reflex, initiated by displacement of mechanoreceptors and muscle spindles, occurs far more rapidly than that brought about by pain (nociception) (Barrack and Skinner, 1984). Joint effusion contributes to a reduction in mechanoreceptor discharge, resulting in inhibition of muscular contraction. This is especially seen in the vastus medialis (VMO) of the knee, for example, where just 60 ml of intra-articular effusion may result in 30–50% inhibition of quadriceps contraction (Kennedy, Alexander and Hayes, 1982). Proprioceptive deficits have also been shown to parallel joint degeneration (Barrett, Cobb and Bentley, 1991), but it is unclear whether this occurs as a result of degeneration, or is in fact part of its aetiology (Lephart and Fu, 1995).
Keypoint
Following injury, an athlete’s proprioceptive ability will be impaired. Training to restore this is an essential part of sport rehabilitation.
From a clinical standpoint, proprioception may be seen to consist of three interrelating components (Beard et al., 1994) (Fig. 5.36), representing activity at spinal, brainstem and higher centre levels. Each component is assessed by a variety of different tests (Lephart and Fu, 1995).
Static joint position sense
First, static joint position sense is used to maintain posture and balance at brainstem level. Input for these actions is from joint proprioception, the vestibular centres in the ears, and from the eyes. Balance and postural exercise with the eyes open and/or closed may be used to enhance static joint position sense. This component is commonly measured by tests which address reproduction of passive positioning (RPP) and reproduction of active positioning (RAP). The subject is required to return the joint to its start position after either an active or passive movement.
Movement sense
Second, kinaesthetic awareness or ‘movement awareness’ is a result of higher centre activity. This component encompasses the detection of both joint displacement and velocity change. It is commonly assessed by measuring the threshold to detection of passive motion (TTDPM), the subject simply stating when he or she feels movement has begun. Once movement has been detected through kinaesthetic awareness, motor programmes may be performed automatically in many cases. Consciously performed joint positioning activities, especially at end-range, will enhance the development of automatic control and cognitive awareness (Lephart and Fu, 1995).
Regulation of muscle stiffness
Finally, closed loop efferent activity is required for reflex (spinal) activity and regulation of muscle stiffness, leading to dynamic joint stability. This type of activity underlies all movements by supplying reflex splinting when a joint is stressed. Damage to joint receptors has been shown to affect co-contraction of muscles and reduce joint stability. This, in turn, can lead to an increase in the likelihood of injury (Tyldesley and Grieve, 1989).
Proprioception is enhanced at this level through the initiation of reflex joint stabilization, using activities which involve sudden alterations in joint position. Reflex stabilization is therefore assessed through measurement of the onset of muscle contraction in relation to joint displacement. The aim is to see if the muscles are able to limit joint displacement and effectively stabilize the joint.
Proprioceptive research
Using TTDPM and RPP, Barrack and Skinner (1984) found decreased kinaesthesia with increasing age. In general, our highly mechanized Western society may fail to impose the variety of movements which an individual requires for optimal musculoskeletal health. This reduced movement ‘vocabulary’ decreases the proprioceptive stimulation needed for skilled motor action (Jull and Janda, 1987). After injury, proprioceptive input is further reduced due to prolonged inactivity and damage to proprioceptive nerve endings within the injured tissues. A number of authors have stressed the importance of proprioceptive training in rehabilitation following injury to the knee (Barrack and Skinner, 1984; Beard et al., 1994), ankle (Freeman, Dean and Hanham, 1965; Lentell, Katzman and Walters, 1990; Konradsen and Ravn, 1990) and shoulder (Smith and Brunolli, 1990; Lephart et al., 1994). The functional importance of proprioceptive training has also been emphasized during rehabilitation of the spine (Lewit, 1991; Irion, 1992; Norris, 1995a), although its use in spinal rehabilitation is less common than for other areas of the body.
Proprioception may be enhanced with training. Barrack and Skinner (1984) found enhanced kinaesthesia in trained dancers, and Lephart and Fu (1995) demonstrated the same in intercollegiate gymnasts. Both of these types of athletes practice free exercise using bodyweight as resistance, and use complex multijoint activities. This type of training would seem appropriate for proprioceptive rehabilitation.
Training techniques
Proprioceptive training involves highly skilled actions, often performed at speed, with the aim of making the movement less attention-demanding (automatic). Proprioceptive exercises are progressed in terms of speed and complexity aiming at quality of movement execution rather than simple overload. Multiple sensory inputs are used to improve the sense of both static position and movement. Once this has been achieved, dynamic stability exercises may be used.
Proprioceptive training may be performed by following the general stages by which an athlete actually learns any skilled action (Table 5.6).
Table 5.6 Learning motor skills
| Stage of learning | ||
|---|---|---|
| Stage (I)—understanding | Stage (II)—effective movement | Stage (III)—automatic action |
| Understand what is required from action | Refine action | Less attention required |
| Environmental cues important | Able to recognize own mistakes | Movement seems to ‘run by itself’ |
| Movements poorly coordinated | Movements more consistent and efficient | Speed of movement increased |
| Demonstration and movement cueing important | Energy expenditure lower | |
| Practical implication | ||
| Split complex movement sequences into simple components | Correct movement pattern when/if it erodes | Distract athlete to ensure less attention is used |
| Increase movement awareness by cueing | Stop if athlete becomes fatigued | Progress speed of movement while maintaining accuracy |
| Use palpation and passive movement to facilitate learning | Link simple actions together into sequences | Increase repetitions |
| Slow precise actions | Reduce environmental cues | Alter environmental cues |
| Progress only when athlete can perform action independently of therapist | Increase repetitions as endurance improves | Perform multiple actions |
| Require athlete to recognize their own mistakes (self-monitoring) | ||
How athletes learn skilled movements
Proprioceptive exercises are highly skilled, and in order to effectively prescribe this type of training we need to understand the way that an athlete actually learns a skilled movement. There are three overlapping stages to motor skill (movement) learning (Fitts and Posner, 1967; Schmidt, 1991).
Stage I (cognitive)
The first stage is the stage of understanding, where the athlete attempts to form an idea of the whole skill. The process is cognitive (thinking) rather than motor (doing) in nature, and hence the title of this learning stage. The athlete is learning what to do (and importantly, what not to do), and how to do it.
Environmental cues which later will go unnoticed are important to this early stage of learning. They provide an important frame of reference for building the new skill. For example, when learning a new dance step, a person will often focus attention on the foot position, which they later take for granted.
In this stage movements will be poorly coordinated. The athlete must concentrate intensely and will therefore tire easily. The therapist can assist by providing clear instructions and feedback. Complex actions should be split up into more simple components. For example, a single leg hop and twist would be learned as a single leg balance first in stage I. This would be followed by straight line hopping, and, eventually, hopping and twisting on the spot and finally hopping and twisting over a distance, in stages II and III.
Demonstration of the movement is important, and the athlete will need constant coaching and correction of the skill to prevent them practising mistakes.
One of the ways we can help learning in this stage is to use cueing, to paint a mental picture of an action in terms which an athlete can easily understand. For example, an abdominal hollowing action may be cued by asking the athlete to pull the tummy button in (visual), or use the fingers to feel the abdomen tightening (tactile). The instructor may use the voice intonation (auditory) to indicate the intensity of the movement.
Stage II (motor)
This is the stage of effective movement, when the athlete will try to make the motor programme more precise and refine the action. It is as though the original clumsy action is ‘whittled down’ to a smoother defined movement. Through practice, the athlete is now able to recognize mistakes, and so self-practice (unsupervised) can now be allowed.
The dependence on visual and verbal cues (stage I) now gradually gives way to the reliance on proprioceptive information. Movements become more consistent and the athlete is able to work on the finer details of an action. As the action becomes more efficient, energy expenditure is reduced because the athlete does not have to work as hard to produce the action. Environmental cues are used for timing and as anticipation develops, movements become smoother and less rushed.
Keypoint
As a motor skill becomes more efficient, energy expenditure is reduced and movements become smoother.
The individual movement sequences used in stage I are now linked together to give a longer skill sequence. The actions must still be slow and precise, with progression made only when the movement sequence is correct.
Stage III (automatic)
In this stage the action ‘runs by itself’ or becomes automatic (grooved). Movements in this stage demand less attention to perform and so the athlete can now perform other actions at the same time. The speed of the movement may be increased, and functions such as muscle reaction time become important. Here, the body is challenged (for example, knocking it off balance) and the athlete must react quickly with appropriate changes in posture and movements. This type of final training is used with balance balls and gym balls, for example.
Practical aspects of proprioceptive training
Training begins by splitting complex movements into a number of simple component sequences (Table 5.7), with the choice of exercise being determined by the functional requirements of the patient. Splitting the movement in this way enables the athlete to focus their attention selectively on a single action, making learning far easier. Initially actions must be slow and precise with the emphasis on control of the correct body position. The rate of movement is progressed, while maintaining accuracy, and the simple movement components are linked together to form the total activity sequence (Tropp, Alaranta and Renstrom, 1993). The athlete must stop when they become fatigued; failure to do so will often lead to practise of incorrect exercise technique and negative transfer effects.
Table 5.7 Proprioceptive training
| Increase awareness of correct pattern |
| Gain voluntary control of movement pattern |
| Gain automatic control of movement |
From Norris, C.M. (1995b) Spinal stabilisation, 2. Limiting factors to end range motion in the lumbar spine. Physiotherapy, 81, 4–12. Chartered Society of Physiotherapy. With permission.
Definition
A negative transfer effect occurs when an activity in training is learned to such a degree that it actually interferes with a skilled movement in sport performance.
Movement of other body parts draws the athlete’s attention away from the conscious control of the core action, and assists in the development of automatic actions. To gain true automaticity of a movement sequence, thousands of repetitions are needed. Rather than practising isolated exercises to repetition, functional activities should be built into an athlete’s activities of daily living (ADL).
Using proprioceptive training of the ankle as an example, single leg standing may begin, followed by single leg standing with 1/4 squat activities, and finally, the same base activity with throwing and catching. This could be built into an athlete’s daily activities (ADL) by performing simple home exercises such as cleaning the teeth while standing on one leg!
Once an action can be performed correctly on a stable surface, the subject may be positioned on a moving base of support. The subject must now use not just joint position and movement sense, but anticipation of body displacement, requiring reflex stabilization. Initially, the labile surface should involve uniaxial movements, for example a rocker board. Placing the pivot of this type of board in the frontal plane will work the flexion and extension reaction, while placing the pivot in the sagittal plane will work abduction and adduction. If the pivot is then placed diagonally, movements will be biaxial in nature. Progression is made to the wobble board where the pivot point is dome-shaped to allow triaxial motion. Other apparatus useful for balance work and muscle reaction includes the large diameter (65 cm) gymnastic ball, the mini-trampette, the ‘Fitter’ ski-training device (Fitter International Inc., Calgary, Alberta, Canada) and the ‘slide trainer’ (Forsa Fitness Equipment, London, England). In each case, as the athlete is pushed off balance, the aim is to maintain stabilization and enhance both movement detection and closed-loop reflex muscular stabilization. These actions must be built into an athlete’s normal training programme rather than isolated from it.
Examples of proprioceptive training for the ankle, knee, shoulder and spine are given in the relevant clinic chapters for these body parts.
Andersson E.A., Oddsson L., Grundstrom O., et al. EMG activities of the quadratus lumborum and erector spinae muscles during flexion-relaxation and other motor tasks. Clinical Biomechanics. 1996;11:392-400.
Appell H.J. Muscular atrophy following immobilisation: a review. Sports Medicine. 1990;10:42.
Barrack R.L., Skinner B.L. Joint kinesthesia in the highly trained knee. Journal of Sports Medicine and Physical Fitness. 1984;24:18-20.
Barrett D.S., Cobb A.G., Bentley G. Joint proprioception in normal, osteoarthritic, and replaced knees. Journal of Bone and Joint Surgery. 1991;73B:53-56.
Bastide G., Zadeh J., Lefebvre D. Are the ‘little muscles’ what we think they are? Surgical and Radiological Anatomy. 1989;11:255-256.
Beard D.J., Kyberd P.J., O’Connor J.J., Fergusson C.M., Dodd C.A.F. Reflex hamstring contraction latency in anterior cruciate ligament deficiency. Journal of Orthopaedic Research. 1994;12(2):219-228.
Bergmark A. Stability of the lumbar spine: a study in mechanical engineering. Acta Orthopaedica Scandinavica. 1989;230:20-24.
Biedermann H.J., Shanks G.L., Forrest W.J., Inglis J. Power spectrum analyses of electromyographic activity. Spine. 1991;16(10):1179-1184.
Bohannon R.W. Cinematographic analysis of the passive straight leg raising test for hamstring muscle length. Physical Therapy. 1982;62(5):1269-1274.
Bullock-Saxton J., Murphy D., Norris C., et al. The muscle designation debate: the experts respond. Journal of Bodywork and Movement Therapies. 2000;4(4):225-227.
Bullock-Saxton J.E., Bullock M.I. Repeatability of muscle length measures around the hip. Physiotherapy Canada. 1994;46(2):105-109.
Comerford, M., 1995. Muscle Imbalance, course notes, Nottingham School of Physiotherapy, Nottingham.
Cornwall J., John-Harris A., Mercer S.R. The lumbar multifidus muscle and patterns of pain. Manual Therapy. 2006;11:40-45.
Cresswell A.G., Grundstrom H., Thorstensson A. Observations on intra-abdominal pressure and patterns of abdominal intra-muscular activity in man. Acta Physiologica Scandinavica. 1992;144(4):409-418.
Cresswell A.G., Oddsson L., Thorstensson A. The influence of sudden perturbations on trunk muscle activity and intra abdominal pressure while standing. Experimental Brain Research. 1994;98:336-341.
Critchley D.J., Coutts F.J. Abdominal muscle function in chronic low back pain patients. Physiotherapy. 2002;88(6):322-332.
Cromie J., Robertson V., Best M. Work related musculoskeletal disorders in physical therapists. Physical Therapy. 2000;80(4):336-351.
Danneels L., Vanderstraeten G., Cambier D. Effects of three different training modalities on the cross sectional area of the lumbar multifidus in patients with chronic low back pain. British Journal of Sports Medicine. 2003;37(1):91.
de Andrade J.R., Grant C., Dixon A. Joint distension and reflex muscle inhibition in the knee. Journal of Bone and Joint Surgery. 1965;47(A):313-322.
Esola M.A., McClure P.W., Fitzgerald G.K., Siegler S. Analysis of lumbar spine and hip motion during forward bending in subjects with and without a history of low back pain. Spine. 1996;21(1):71-78.
Fitts P.M., Posner M.I. Human Performance. Westport, Connecticut: Greenwood Press; 1967.
Freeman M.A.R., Dean M.R.E., Hanham I.W.F. The etiology and prevention of functional instability of the foot. Journal of Bone and Joint Surgery. 1965;47B:678-685.
Gajdosik R., Lusin G. Hamstring muscle tightness: reliability of the active knee extension test. Physical Therapy. 1983;63(7):1085-1090.
Gibbons S.G.T. Clinical anatomy and function of psoas major and deep sacral gluteus maximus. In: Vleeming A., Mooney V., Stoeckart R., editors. Movement, Stability & Lumbopelvic Pain: Integration of Research and Therapy. Vancouver: Elsevier, 2007. Part 1, Section 1, Chapter 6
Goldspink G. Cellular and molecular aspects of adaptation in skeletal muscle. In: Komi P.V., editor. Strength and Power in Sport. Oxford: Blackwell, 1992.
Goldspink, G., 1996. Personal communication
Gossman M.R., Sahrmann S.A., Rose S.J. Review of length associated changes in muscle. Physical Therapy. 1982;62(12):1799-1808.
Gunn C. Treatment of Chronic Pain: Intramuscular Stimulation for Myofascial Pain of Radiculopathic Origin. Edinburgh: Churchill Livingstone; 1996.
Gunn, C.C., 2000. The Gunn Approach to the Treatment of Chronic Pain, course notes, Westminster Hospital, London.
Hides J.A., Stokes M.J., Saide M., et al. Evidence of lumbar multifidus muscle wasting ipsilateral to symptoms in patients with acute/subacute low back pain. Spine. 1994;19(2):165-172.
Hodges P.W. Transversus abdominis: a different view of the elephant. British Journal of Sports Medicine. 2009;42(12):941-944.
Hodges P., Gandevia S. Activation of the human diaphragm during a repetitive postural task. Journal of Physiology. 2000;522:165-175.
Hodges P.W., Richardson C.A. Neuromotor dysfunction of the trunk musculature in low back pain patients Washington Proceedings of the World Confederation of Physical Therapists Congress 1995
Hodges P., Richardson C., Jull G. Evaluation of the relationship between laboratory and clinical tests of transversus abdominis function. Physio-therapy Research International. 1996;1(1):30-40.
Hodges P.W., Pengel H.M., Sapsford R. Postural and respiratory function of the pelvic floor muscles. Neurourology and Urodynamics. 2007;26(3):362-371.
Holder N., Clark H., DiBlasio J., et al. Causes, prevalence and response to occupational musculoskeletal injuries reported by physical therapists. Physical Therapy. 1999;79(7):642-652.
Houglum P.A. Therapeutic Exercise for Athletic Injuries. Champaign, Illinois: Human Kinetics; 2001.
Irion, J.M., 1992. Use of the gym ball in rehabilitation of spinal dysfunction. Orthopaedic Physical Therapy Clinics of North America, Oxford, pp. 375–398.
Jackson M., Solomonow M., Zhou B., et al. Multifidus EMG and tension-relaxation recovery after prolonged static lumbar flexion. Spine. 2001;26(7):715-723.
Janda V. Muscle strength in relation to muscle length, pain and muscle imbalance. In Harms-Ringdahl K., editor: Muscle Strength: International Perspectives in Physical Therapy, eighth ed, Edinburgh: Churchill Livingstone, 1993.
Janda V. Muscles and motor control in cervicogenic disorders: assessment and management. In Grant R., editor: Physical Therapy of the Cervical and Thoracic Spine, second ed, Edinburgh: Churchill Livingstone, 1994.
Janda, V., Schmid, H.J.A., 1980. Muscles as a pathogenic factor in backpain. Proceedings of the International Federation of Orthopaedic Manipulative Therapists, 4th conference, New Zealand, pp. 17–18.
Jaspers S.R., Fagan J.M., Tischler M.E. Biomechanical response to chronic shortening in unloaded soleus muscles. Journal of Applied Physiology. 1985;59:1159-1163.
Jones R., Lovett R.W. Orthopedic Surgery. New York: William Wood and Co.; 1929.
Jull G.A. Headaches of cervical origin. In: Grant R., editor. Physical Therapy of the Cervical and Thoracic Spine. New York: Churchill Livingstone, 1994.
Jull G.A., Janda V. Muscles and motor control in low back pain: assessment and management. In: Twomey L.T., editor. Physical Therapy of the Low Back. New York: Churchill Livingstone, 1987.
Kendall F.P., McCreary E.K., Provance P.G. Muscles. Testing and Function, fourth ed. Baltimore: Williams and Wilkins; 1993.
Kennedy J.C., Alexander I.J., Hayes K.C. Nerve supply of the human knee and its functional importance. American Journal of Sports Medicine. 1982;10:329.
Koh T.J. Do adaptations in serial sarcomere number occur with strength training? Human Movement Science. 1995;14:61-77.
Koh T.J., Herzog W. Eccentric training does not increase sarcomere number in rabbit dorsiflexor muscles. Journal of Biomechanics. 1998;31:499-501.
Konradsen L., Ravn J.B. Ankle instability caused by prolonged peroneal reaction time. Acta Orthopedica Scandinavica. 1990;61(5):388-390.
Leinonen V., Kankaanpaa M., Airaksinen O., Hannine O. Back and hip extensor activities during trunk flexion/extension: effects of low back pain and rehabilitation. Archives of Physical Medicine and Rehabilitation. 2000;81(1):32-37.
Lentell G.L., Katzman L.L., Walters M.R. The relationship between muscle function and ankle stability. Journal of Orthopaedic and Sports Physical Therapy. 1990;11:605-611.
Lephart S.M., Fu F.H. The role of proprioception in the treatment of sports injuries. Sports Exercise and Injury. 1995;1(2):96-102.
Lephart S.M., Warner J.P., Borsa P.A., Fu F.H. Proprioception of the shoulder in normal, unstable, and surgical individuals. Journal of Shoulder and Elbow Surgery. 1994;3(4):371-381.
Lewit K. Manipulative Therapy in Rehabilitation of the Locomotor System, second ed. Oxford: Butterworth-Heinemann; 1991.
Lieber R.L. Skeletal Muscle Structure and Function. Baltimore: Williams and Wilkins; 1992.
Magee D.J. Orthopedic Physical Assessment, fourth ed. Philadelphia: W.B. Saunders; 2002.
McGill S. Biomechanics of the thoracolumbar spine. In: Dvir Z., editor. Clinical Biomechanics. Edinburgh: Churchill Livingstone, 2000.
McGill S.M., Juker D., Kropf P. Quantitative intramuscular myoelectric activity of quadratus lumborum during a wide variety of tasks. Clinical Biomechanics. 1996;11:170-172.
McKenzie R.A. The Lumbar Spine: Mechanical Diagnosis and Therapy. Lower Hutt, New Zealand: Spinal Publications; 1981.
Mooney V., Robertson J. The facet syndrome. Clinical Orthopaedics and Related Research. 1976;115:149-156.
Morgan D.L., Lynn R. Decline running produces more sarcomeres in rat vastus intermedius muscle fibers than does incline running. Journal of Applied Physiology. 1994;77:1439-1444.
Muller E.A. Influence of training and of inactivity on muscle strength. Archives of Physical Medicine and Rehabilitation. 1970;51:449-462.
Ng G., Richardson C.A. The effects of training triceps surae using progressive speed loading. Physiotherapy Practice. 1990;6:77-84.
Norkin C.C., Levangie P.K. Joint Structure and Function, second ed. Philadelphia: F.A. Davis; 1992.
Norris C.M. Spinal stabilisation. Physiotherapy. 1995;81(2):1-4.
Norris C.M. Spinal stabilisation, 2. Limiting factors to end range motion in the lumbar spine. Physiotherapy. 1995;81:4-12.
Norris C.M. The Complete Guide to Stretching. London: A&C Black; 1999.
Norris C.M. Acupuncture: Treatment of Musculoskeletal Conditions. Oxford: Butterworth-Heinemann; 2001.
Norris C.M., Mathews M. Intertester reliability of a self monitored active knee extension test. Journal of Bodywork and Movement therapies. 2005;9:256-259.
Norris C.M., Mathews M. The role of an integrated back stability program in patients with chronic low back pain. Complementary Therapies in Clinical Practice. 2008;14:255-263.
O’Sullivan P.B., Grahamslaw K.M., Kendell M., et al. The effect of different standing and sitting postures on trunk muscle activity in a pain free population. Spine. 2002;27(11):1238-1244.
Ober F.B. The role of the iliotibial and fascia lata as a factor in the causation of low back disabilities and sciatica. Journal of Bone and Joint Surgery. 1936;18:105-110.
Petty N.J., Moore A.P. Neuromusculoskeletal Examination and Assessment. Edinburgh: Churchill Livingstone; 2001.
Richardson C.A. Muscle imbalance: principles of treatment and assessment Proceedings of the New Zealand Society of Physiotherapists Challenges Conference. New Zealand: Christchurch, 1992.
Richardson C.A., Bullock M.I. Changes in muscle activity during fast, alternating flexion–extension movements of the knee. Scandinavian Journal of Rehabilitation Medicine. 1986;18:51-58.
Richardson C.A., Sims K. An inner range holding contraction: an objective measure of stabilizing function of an antigravity muscle Proceedings of the World Confederation for Physical Therapy, 11th International Congress, London. 1.
Richardson C., Jull G., Hodges P., Hides J. Therapeutic Exercise for Spinal Segmental Stabilisation in Low Back Pain. Edinburgh: Churchill Livingstone; 1999.
Sahrmann S.A. Posture and muscle imbalance: faulty lumbar-pelvic alignment and associated musculoskeletal pain syndromes Postgraduate Advances in Physical Therapy. Berryville, Virginia: Forum Medicum, 1987.
Sahrmanyn, S.A., 1990. Diagnosis and treatment of movement-related pain syndromes associated with muscle and movement imbalances, course notes, Washington University.
Sahrmann S.A. Diagnosis and Treatment of Movement Impairment Syndromes. St Louis: Mosby; 2002.
Saunders S.W., Rath D., Hodges P.W. Postural and respiratory activation of the trunk muscles changes with mode and speed of locomotion. Gait Posture. 2004;20:280-290.
Scannell J.P., McGill S.M. Lumbar posture—should it, and can it be modified? A study of passive tissue stiffness and lumbar position during activities of daily living. Physical Therapy. 2003;83(10):907-917.
Schmidt R.A. Motor Learning and Performance. Champaign, Illionis: Human Kinetics; 1991.
Smith R.L., Brunolli J. Shoulder kinaesthesia after anterior glenohumeral joint dislocation. Physical Therapy. 1990;69:106-112.
Stokes M., Young A. The contribution of reflex inhibition to arthrogenous muscle weakness. Clinical Science. 1984;67:7-14.
Tabary J.C. Physiological and structural changes in the cat’s soleus muscle due to immobilisation at different lengths by plaster casts. Journal of Physiology. 1972;224:231-244.
Templeton G.H., Padalino M., Manton J., et al. Influence of suspension hypokinesia on rat soleus muscle. Journal of Applied Physiology. 1984;56:278-286.
Thomason D.B., Herrick R.E., Surdyka D., Baldwin K. Time course of soleus muscle myosin expression during hind limb suspension and recovery. Journal of Applied Physiology. 1987;63:130-137.
Travell J.G., Simons D.G. Myofascial Pain and Dysfunction. Baltimore: Williams and Wilkins; 1983.
Tropp H., Alaranta H., Renstrom P.A.F.H. Proprioception and coordination training in injury prevention. In: Renstrom P.A.F.H., editor. Sports Injuries. Basic Principles of Prevention and Care. London: IOC Medical Commission, Blackwell Scientific, 1993.
Tyldesley B., Grieve J.I. Muscles, Nerves and Movement: Kinesiology in Daily Living. Oxford: Blackwell Scientific; 1989.
Urban L.M. The straight leg raising test: a review. Journal of Orthopaedics and Sports Physical Therapy. 1981;2(3):117-133.
White S.G., Sahrmann S.A. A movement system balance approach to management of musculoskeletal pain. In: Grant R., editor. Physical Therapy of the Cervical and Thoracic Spine. New York: Churchill Livingstone, 1994.
Williams M., Solomonow M., Zhou B.H., Baratta R.V., Harris M. Multifidus spasms elicited by prolonged lumbar flexion. Spine. 2000;25(22):2916-2924.
Williams P.E. Use of intermittent stretch in the prevention of serial sarcomere loss in immobilised muscle. Annals of the Rheumatic Diseases. 1990;49:316-317.
Williams P.E., Goldspink G. Changes in sarcomere length and physiological properties in immobilized muscle. Journal of Anatomy. 1978;127:459-468.
Williams P., Watt P., Bicik V., Goldspink G. Effect of stretch combined with electrical stimulation on the type of sarcomeres produced at the ends of muscle fibers. Experimental Neurology. 1986;93:500-509.