CHAPTER 4 Physical training and injury
Principles of training
Supercompensation
In any form of training the body is exposed to a workload or physical stress of a frequency, intensity, time (duration) and type sufficient to cause physical change. Together, these variables make up the training volume representing the total amount of exercise/work performed.
To achieve a training effect, the body must be overloaded, that is, exposed to a physical stress which is greater than that encountered in everyday living. The response to this training stress is catabolism, the breakdown of metabolic fuels or tissues. Following the catabolic response, the tissues react by adapting and becoming better suited to coping with the imposed stress; this adaptation is known as anabolism, and involves tissue growth. With training, the anabolic effect is excessive, causing the tissues to grow stronger, a process called supercompensation.
The process of adaptation to an imposed demand (stress) is succinctly described by the general adaptation syndrome or GAS (Seyle, 1956). Initially there is an alarm reaction or ‘shock’. This may last for several weeks, and during this time an athlete’s performance will be impaired, leading to stiffness. Over time, the body adapts to the stress and the athlete enters the resistance phase which is the process of ‘supercompensation’, enabling the body to cope more effectively with stress at that imposed level.
If the stress imposed on the body is too great, or if an athlete fails to allow a sufficient recovery period for the body to adapt, the exhaustion phase may be reached. The body becomes stiff and sore again and the athlete quickly loses motivation. Boredom sets in—overreaching and eventually overtraining has occurred. Lack of adequate rest, poor diet and too little sleep to allow recovery can all lead to exhaustion.
Overtraining syndrome
Training involves stressing the body so that it overcompensates and gains a training effect. Some fatigue after exercise is therefore desirable and this type of acute fatigue leads to an increase in performance. However, if the training volume is too great, or the recovery period between training bouts too brief, athletes will overreach giving a temporary reduction in performance. Where overreaching (OR) is marked, stagnation will result in a brief performance reduction. This may occur for example after a hard training camp, and the effect would be positive providing recovery is adequate. Overreaching of this type is termed ‘functional OR’. Continuing the increase in training intensity without allowing recovery will lead to a reduction in performance called non-functional OR. A short-term decrement in performance occurs which allows the athlete to recover within a 2-week period (Lehmann et al., 1999). If recovery is not adequate and training continues, the progression is to overtraining. Recovery in this case may takes months or in some cases years (Meeusen et al., 2006).
Overtraining syndrome (OTS) occurs when the body is subjected to stresses beyond its capacity to adapt. Lack of adaptation to training leads in turn to a reduction in sports performance and a number of important potential health concerns. The symptoms of OTS are initially similar to those of hard training, such as muscle aching and fatigue. However, the experienced coach and athlete can detect when these changes are greater than normal. Several physiological effects are thought to underlie OTS, including autonomic nervous system changes, alteration in endocrine response, suppression of immune function and variation in brain neurotransmitters (Wilmore, Costill and Kenney, 2008). Alteration in sympathetic nervous system drive is seen in athletes who emphasize high intensity resistance training giving increased heart rate, blood pressure, and basal metabolic rate, loss of appetite and decreased body mass.
Symptoms of OTS
One of the adaptations to normal training is a change in the hypothalamic pituitary axis (HPA) characterized by an increase in the ACTH/cortisol ratio during the post workout recovery period. In OTS there is a change in the rise in ACTH following exercise and this has been used to identify non-functional OR and OTS. Using two exercise bout tests Meeusen et al. (2004) were able to demonstrate large increases in hormonal release following the first exercise bout but suppression following the second. Time to fatigue tests which are specific to an athlete’s sport have also been used to detect OTS (Halson and Jeukendrup, 2004). Typically athletes suffering from OTS are able to begin an exercise session performing normally but then suffer from an unexplained performance drop. Fatigue tests are therefore more predictive than incremental tests (Meeusen et al., 2006).
Mood state questionnaires are very useful in the identification of OTS as negative affective states characterize the condition. Questionnaires such as the recovery-stress questionnaire (RestQ-Sport) may be used but athletes should ideally be tracked throughout their training to identify a baseline to show deviation. This is a 76-item questionnaire which assesses the physical and mental impact of training (Kellman, 2001). Heart rate variability (HRV) has also been used as an assessment tool of OR. HRV increases with heightened parasympathetic tone and has been shown to be significantly elevated following chronic training (Meeusen et al., 2006).
Many athletes describe an increase in URT infections following hard training—the so called ‘open window’ effect. This effect seems to be more prevalent with OR and OTS. A 2-week period of intense training has been shown to reduce bacterial defense response (bacterially stimulated neutrophil degradation) by 20% (Robson et al., 1999) and a 1-week intense programme to lower T-cell count (Lancaster et al., 2004)
The initial management OTS is dependent on identifying OR. This is made easier by having the athlete keep a training log (Table 4.1) so that changes in response to their baseline measure may be recognized early and appropriate action taken. Where OR is suspected it is vital that training volume be reduced, and in more severe cases total rest may be called for over a period of many weeks. Prevention focuses on periodization of training to vary training variables including frequency, intensity, time and type (FITT). High quality diet and adequate sleep play a pivotal role in exercise recovery and the prevention of OTS.
FITT: frequency, intensity, time, type; RPE: rating of perceived exertion; UTI: upper respiratory tract infection; MSK: musculoskeletal.
Halson S., Jeukendrup A. Does overtraining exist? An analysis of overreaching and overtraining research. Sports Medicine. 2004;34:967-981.
Kellmann M., Kallus K.W. Recovery-Stress Questionnaire for athletes: User manual. Champaign, IL: Human Kinetics Publishers; 2001.
Lancaster G.I., Halson S.L., Khan Q., Drysdale P., Jeukendrup A. The effects of acute exhaustive exercise and intensified training on type 1/ type 2 T cell distribution and cytokine production. Exercise Immunology Review. 2004;10:91-106.
Lehmann M., Foster C., Gastmann U., et al. Overload, performance incompetence, and regeneration in sport. New York: Plenum; 1999.
Meeusen R., Duclos M., Gleeson M., Rietjens G. Prevention, diagnosis and treatment of the Overtraining Syndrome. ECSS position statement. European Journal of Sports Science. 2006;6(1):1-14.
Meeusen R., Piacentini M.F., Busschaert B., Buyse L. Hormonal responses in athletes: the use of a two bout exercise protocol to detect subtle differences in overtraining status. European Journal of Applied Physiology. 2004;91:140-146.
Robson P.J., Blannin A.K., Walsh N.P. The effect of an acute period of intense interval training on human neutrophil function and plasma glutamine in endurance trained male runners. Journal of Physiology. 1999;515:84-85P.
Wilmore J.H., Costill D.L., Kenney W.L. Physiology of sport and exercise, fifth ed. Champaign, IL: Human Kinetics Publishers; 2008.
Progressive exercise
As fitness improves, the intensity of the load which is required to produce a training effect will increase. Adaptation to the load occurs, and so further improvement will only occur if the training intensity is increased. Physical activity in itself is therefore not synonymous with physical training. A training effect will only occur if an activity is sufficiently demanding.
In addition to a minimum intensity, the training load must be continued for a certain time. High intensity training which is too brief may not allow time for the physical adaptations required by the body. The frequency of training—that is, how often it is carried out—is also important. Training is a stimulus which causes an anabolic adaptation. This adaptation will take time, and so adequate recovery must be allowed between training sessions for the body tissues to modify themselves. The type of training will dictate the type of tissue adaptation which occurs, a principle known as specificity (McCafferty and Horvath, 1977) (see below).
Training effects are not permanent. The motor system adapts to the level (overload) and type (specificity) of stress that is imposed on it. If the stress is removed, and training ceases, the motor system will again adapt to the new, now lower, level of stress, and detraining will occur. This transient nature of training adaptation is known as the reversibility principle (Thorstensson, 1977; Enoka, 1994).
Definition
The reversibility principle describes the gradual loss of training effects when the training overload is reduced, a process referred to as detraining.
When training for aerobic (cardiopulmonary) fitness or stamina, exercise intensity may be assessed by measuring heart rate or maximal oxygen uptake (VO2 max). The American College of Sports Medicine (1978) recommended the quantity and quality of exercise required to develop and maintain aerobic fitness and body composition. A training frequency of 3–5 days per week is required, at an intensity of 60–90% of the maximum heart rate reserve, or 50–85% VO2 max. This should be carried out for a duration of 15–60 minutes, and be continuous or rhythmical in nature. These recommendations were later updated to include the provision of resistance training, flexibility and weight loss (ACSM, 1990, 2002). For strength gains, one set of 8–12 repetitions was recommended, with 8–10 exercises for the major muscles groups, for 2 days per week. A balanced flexibility programme should include both static and dynamic range of motion exercise to work the major muscle/tendon groups. Each stretch should be held for at least 10–30 seconds, and four repetitions should be used for each group two to three times per week. To achieve significant weight loss,  hours of moderate exercise with an energy expenditure of at least 2000 calories per week is recommended. To achieve this, either continuous or accumulative exercise may be used at an exercise intensity of 55–69% maximal heart rate. Accumulated daily duration should be 30–40 minutes per day (Table 4.2).
hours of moderate exercise with an energy expenditure of at least 2000 calories per week is recommended. To achieve this, either continuous or accumulative exercise may be used at an exercise intensity of 55–69% maximal heart rate. Accumulated daily duration should be 30–40 minutes per day (Table 4.2).
Table 4.2 ACSM guidelines for maintaining fitness in apparently healthy individuals
| Cardiovascular | |
| Frequency | 3–5 times per week |
| Intensity | 55–90% HRmax |
| Time | 20–60 min |
| Type | Large muscle groups. Rhythmic and continuous activity |
| Muscular | |
| Frequency | 2–3 times per week |
| Intensity | 8–10 exercises 1 set of 8–12 repetitions to volitional fatigue 75% 1 RM resistance |
| Time | 20 minutes |
| Type | Resistance training for major muscle groups |
| Flexibility | |
| Frequency | 3 times per week |
| Intensity | 3−5 repetitions for each exercise Maintain at point of mild discomfort |
| Time | 10–30 second hold |
| Type | Static stretch for major muscle groups |
HR max: maximal heart rate; 1 RM: maximum resistance lifted for single repetition.Source ACSM (1978, 2002).
Importantly each of us is different, and will respond differently to training. This principle of Individuality underlies successful exercise prescription. Variation in tissue adaptation, neural, cardiopulmonary and endocrine changes, and psychology dictate that we will all respond slightly differently to exercise. Individuality explains why when two people begin a gym programme, for example, one may progress quite rapidly (high responder) while the other may struggle to make gains (low responder). The main reason for individuality is hereditary. A study of a 20-week endurance training programme using identical twins (Prud’homme et al., 1984) showed a similar training response for each twin pair, but a substantial variation across subjects of maximal aerobic power improvement (0−40%). Assessing the difference in training response (VO2 max) using family members (Bouchard and Rankinen, 2001) has shown that high or low responders tend to be clustered within families, again representing a genetic and/or familial tendency.
Fitness
Physical fitness has been defined as a set of attributes that relate to the ability of people to perform physical activity (McArdle et al., 1991), or the ability of a person to function efficiently and effectively to enjoy leisure, to be healthy, to resist hypokinetic disease and to cope with emergency situations (Kent, 1994).
Fitness can be thought of as a continuum from optimal fitness at one side through average fitness to complete lack of fitness and death (Fig. 4.1). The exact components of fitness required to make an individual optimally efficient and effective will be determined largely by the physical activity to be performed.

Fitness may be subdivided into two types: task (performance)-related fitness is that required for sport and within occupational activities; health-related fitness includes components which are associated with some aspect of health. Physical training will improve fitness, but may not always enhance health. Extreme development of any one of the fitness components, in isolation, will upset the delicate balance between the components, and may actually be detrimental to health. For example, excessive development of flexibility will lead to hyperflexibility and, when strength lags behind, instability. Excessive development of strength may reduce range of motion, leaving an athlete ‘muscle bound’. Favouring some muscles to the detriment of others will often lead to a change in the equilibrium point (resting position) of a joint.
The benefits of exercise are numerous (Table 4.3). However, as we have seen (Treatment Note 4.1) there is a balance between training sufficiently hard to gain the effects of overload, but not so hard that the athlete overreaches (OR) in the short term or eventually progresses to overtraining (OTS). Many athletes will be familiar with the symptom of staleness, and of an increased incidence of UTI.
Table 4.3 Benefits of regular exercise
Source US Department of Health and Human Sciences (1999) Physical Activity and Health. Report of the Surgeon General. http://www.cdc.gov.
Definition
Upper respiratory tract infection (UTI or URTI) is a condition affecting the nose, respiratory tract, sinuses, pharynx or larynx. Typical symptoms include nasal congestion, running nose, cough, sore throat and fever. Exposure to a virus or less commonly a bacterium gives symptoms between 1 and 3 days later which may last up to 10 days. Common names for the condition include colds, sinusitis and laryngitis.
Infection of this type occurs because although training in general has been shown to enhance immune function, following intense training the immune system is depressed. This temporary depression leaves the athlete susceptible to infection, and is called the ‘open window’. It is thought that intense exercise changes adrenocorticotropic hormone (ACTH) and cortisol concentrations and has a knock-on effect on blood glucose concentration, negatively affecting the immune system (Nieman and Pedersen, 1999). Moderate exercise does not have this effect, and the window remains closed giving the long term immune system the benefits of exercise without short term immunosuppression.
Fitness components
The fitness components may be conveniently defined as ‘S’ factors (Table 4.4). The term ‘stamina’ is used to encompass both cardiopulmonary and local muscle endurance. Cardiopulmonary endurance is associated with a reduced risk of coronary heart disease (Ashton and Davies, 1986), and local muscle endurance is a factor in any sustained activity, especially joint stability. Suppleness (flexibility) and strength (see below) are concerned with the health of the musculoskeletal system, to maintain both range of movement and joint integrity. Speed (rate of movement) and power (rate of doing work) are both needed in later stage rehabilitation as part of proprioceptive training. Skill training is important, not just for sports specific actions, but for the skill of individual movement such as scapulohumeral rhythm or gait re-education, for example.
Table 4.4 ‘S’ factors of fitness
| Factor | Concept |
|---|---|
| Stamina | Cardiopulmonary and local muscle endurance |
| Suppleness | Passive and active flexibility |
| Strength | Isometric, isotonic (concentric and eccentric) isokinetic strength |
| Speed | Speed (rate of movement) and power (rate of doing work) |
| Skill | Motor skill |
| Specificity | Overload must match tissue adaptation required |
| Spirit | Psychological aspects of injury, including illness behaviour |
The term ‘specificity’ refers to the SAID principle, that is ‘specific adaptation to imposed demands’. The change taking place in the body of an athlete (adaptation) as a result of training (the imposed demand) will be determined by the type of training which is used, and will be specific to it.
Specificity applies to strength and power development, but also to the energy systems used while exercising. A particular cardiopulmonary training programme will cause specific training adaptations. Aerobic fitness developed on a cycle ergometer, for example, will differ slightly from that obtained while running.
It is important, therefore, that training matches as accurately as possible the action which the athlete will use in a sport in terms of joint range, muscle work, energy system and skill.
The term ‘spirit’ covers the psychological effects of exercise as discussed below.
Psychological effects of exercise
Exercise and self-concept
Several psychological characteristics have also been shown to change as a result of participation in a regular exercise programme. Enhancement of self-confidence, self-esteem and body image are seen, and reductions in anxiety, depression, stress and tension have been demonstrated.
Enhanced well-being
Athletes often claim that exercise makes them ‘feel good’, and the ‘runners’ high’ is a widely reported phenomenon. Reductions in stress and anxiety have been reported, lasting for between 2 and 5 hours after the cessation of training (Morgan, 1985), and decreased depression has been demonstrated as a result of 6–20-week exercise programmes (Greist et al., 1979). In addition, altered states of consciousness have been described following distance running (Mandell, 1979). Weight training programmes have been shown to enhance self-concept in both male (Dishman and Gettman, 1981; Tucker, 1982) and female (Brown and Harrison, 1986) athletes. Three theories exist to explain these phenomena: the distraction hypothesis, and the production of monoamines and endorphins.
How exercise makes an athlete feel better
The distraction hypothesis proposes that participation in vigorous exercise distracts the athlete from stress. Comparisons between exercise, meditation and distraction show similar reductions in state anxiety, but the effect resulting from exercise appears to last longer (Morgan, 1985).
Depression is also affected by exercise. Reductions in the monoamine chemicals noradrenaline (norepinephrine) and serotonin (5-HT) are associated with depressed states in humans, and these same chemicals have been shown to increase in rats subjected to chronic exercise (Brown et al., 1979). Increases in the release of endorphins and enkephalins, or slowing of the dissociation rates of these chemicals has also been proposed (Pert and Bowie, 1979). By measuring plasma levels of these chemicals or using opiate antagonists to neutralize them, researchers have demonstrated some association between exercise and endorphins (Farrell et al., 1983).
Exercise addiction
Exercise addiction, or exercise dependence, is the physiological or psychological dependence on regular exercise, usually distance running, but other forms of exercise such as body-building may also show this trend. Athletes who are addicted to exercise show symptoms of withdrawal and show uncontrollable craving for a particular exercise type at the expense of other training.
Definition
Exercise addiction is physical or psychological dependence on regular exercise of a single type. Athletes show uncontrollable craving and symptoms of withdrawal when the exercise is not practised.
The experience of exercise for an athlete, and the way in which this fits into the rest of his or her life, is one factor which determines whether or not an exercise becomes addictive (Crossman, Jamieson and Henderson, 1987). An individual’s need for exercise can be either positive or negative. Positive addiction exists when an athlete receives some psychological or physical benefit from an activity, and is able to control the activity.
The negatively addicted athlete is controlled by the activity and will experience severe negative effects (withdrawal) with a missed exercise bout. Such athletes often engage in an activity at the expense of their health or at the expense of other factors, such as relationships and career prospects. The negatively addicted athlete may be failing to gain approval from significant others and may harbour feelings of inadequacy or unattractiveness. This type of athlete often exercises alone or in isolation from the group. They experience feelings of enhanced self-concept and even euphoria during exercise. Importantly, such individuals are more likely to ignore pain or injury and work through this to complete a workout. In the same vein, they tend to be anxious if a workout is missed and almost appear to suffer ‘withdrawal symptoms’ (Table 4.5).
Table 4.5 Characteristics of exercise addiction
| The athlete may: |
Adapted from Glasser, W. (1976) Positive Addiction. Reprinted by permission of HarperCollins Publishers Inc. and Anshel, M.H. (1991) A psycho-behavioral analysis of addicted versus non-addicted male and female exercisers. Journal of Sport Behavior, 14 (2), 145–154.
Warm-up
Many athletes conscientiously warm-up in the belief that they will protect themselves against injury, and enhance their sporting performance. While neither of these beliefs have been conclusively proven, there is mounting evidence in the literature to suggest that both may contain elements of truth. Two studies are of particular note. Wedderkopp, Kaltoft and Lundgaard (1999) found that warm-up significantly reduced both traumatic and overuse injury frequency. Players in the control group (non-warm-up) were found to be 4.9 times more likely to become injured than those who warmed up. Looking at knee and ankle injury incidence in hard ball players, Olsen, Myklebust and Engebretsen (2005) studied 1837 youth handball players in Norway and found a significantly lower incidence of injury in the warm-up group (0.5 injuries per 1000 player hours) compared to the control group (0.9 injuries per 1000 player hours). These same authors concluded that a warm-up programme reduced the incidence of injury by 50%.
Warm-up types
Warm-up may be either passive, involving an external heat source, or active, involving body heat. An active warm-up, in turn, may be general, using the whole body, or specific, working only those body parts to be used in competition, and studies have shown improvements from each (Table 4.6).
Table 4.6 Some historical studies on efficiency of warm-up
| Reference | Warm up type | Result |
|---|---|---|
| Carlile (1956) | Passive | Improvements in swimming times after hot showers (8 minutes at 40°C) |
| Davies and Young (1983) | Passive | Warmed the triceps surae muscles using hot water baths. Showed increases in peak power output with cycling and jumping tasks |
| Sargeant (1987) | Passive | Water baths. Showed increases in peak force and power of 11% after heating, and reductions of up to 21% after cooling |
| Richards (1968) | Active—general | Stool stepping before vertical jump task. 1- and 2-min warm-ups improved performance by 23%. 4 min had no effect. 6 min warm-up reduced performance by 27% |
| DeVries (1959) | Active—specific | Compared passive (hot showers and massage), active (calisthenics) and specific (swimming) warm-up prior to swimming task. Significant improvement only after specific warm-up |
Many external heat sources are suitable for a passive warm-up. Common types used by athletes include hot baths or showers and saunas. Clinically, physiotherapists use a number of modalities including hot packs, whirlpool baths and electrotherapy (short-wave diathermy in particular). Benefits are claimed to result from the increase in tissue temperature, and physical performance has been improved using this type of warm-up.
With a passive warm-up, no significant active body movement is used, and little energy is expended. Subsequent physical work will not therefore be impaired due to depletion of energy stores. This type of warm-up can be useful clinically, when active movement is either not desirable or not possible.
General warm-ups are the type most commonly used in sport. The overall body temperature is raised by active exercise, increasing the temperature of the deep muscles and body core. Specific warm-up involves movements which are to be used in actual competition, but at a reduced intensity. Rehearsal of body movement takes place, and the specific tissues directly involved in the activity are heated. This type of warm-up would seem especially appropriate for events requiring highly skilled and coordinated actions.
Effects of warm-up
A warm-up achieves its effect through physiological, psychological and biomechanical methods. Physiological effects are largely due to increases in tissue temperature, while psychological effects are mainly due to practice. Biomechanical effects are achieved by alterations in the tissue response to mechanical strain.
Cardiovascular changes
The change from a relaxed resting state to a higher training level should be gradual, to avoid suddenly stressing the cardiovascular system. Equally, to stop training quickly, and reduce cardiac output too rapidly, can compromise venous return.
A warm-up of sufficient intensity will cause an alteration in regional blood flow. When resting, only 15–20% of the total blood flow goes to the skeletal muscles, but after about 10 minutes of general exercise this figure is increased to 70–75% (Renstrom and Kannus, 1992). During a warm-up, blood flow is increased to active muscles and reduced to visceral tissues earlier than would occur without a warm-up. Increased blood flow causes the delivery of nutrients and removal of metabolic wastes to be enhanced.
Barnard et al. (1973) examined the effects of sudden strenuous exercise on men with no symptoms of cardiac problems. Each subject ran vigorously on a treadmill for 10–15 seconds without a warm-up. In 70% of these subjects, abnormal changes were seen on an ECG trace, indicative of subendocardial ischaemia. These changes were reduced, or even abolished, when a warm-up was performed before activity. Similarly, the effect of sudden onset exercise on blood pressure was improved. Average systolic blood pressures of 168 mmHg were seen without warm-up and these reduced to 140 mmHg when warm-up preceded exercise.
One of the reasons for these changes is that the adaptation of the coronary blood flow to strenuous exercise is not instantaneous. The cardiac output is unable to increase quickly enough to meet the demands of sudden high intensity work (Astrand and Rodahl, 1986), and a warm-up gives the cardiovascular system time to respond.
Tissue temperature
The ability to perform physical work is improved by elevated temperature (Bergh and Ekblom, 1979a). Warm-up prior to maximal exercise will enable the adaptations necessary for these changes to occur sooner.
Oxygen dissociation from haemoglobin is more rapid and complete, and oxygen release from myoglobin is greater at higher temperatures (Astrand and Rodahl, 1986). The critical level of various metabolic processes is lowered, causing an acceleration in metabolic rate and a more efficient usage of substrates. Muscle contraction is more rapid and forceful (Bergh, 1980). The sensitivity of nerve receptors and speed of transmission of nervous impulses are both increased as temperature rises (Astrand and Rodahl, 1986). This more rapid transmission of kinaesthetic signals is particularly important when complex highly skilled movements are used. These temperature-dependent changes are summarized in Table 4.7.
| Improvement | Mechanism |
|---|---|
| Muscle work | Faster muscle contraction and relaxation speeds |
| Economy of movement | Lowered viscous resistance within muscle |
| Oxygen delivery and usage | Haemaglobin releases oxygen more easily as tissue temperature rises |
| Nerve conduction | Increased temperature accelerates metabolic rate within nerve. Specific warm-up rehearses motor pattern |
| Blood perfusion | Local vascular bed dilated |
Source McArdle, W.D., Katch, F.I. and Katch, V.L. (2001) Exercise Physiology, Energy, Nutrition and Human Performance, 5th edn. Lea and Febiger, Philadelphia. With permission.
The increased tissue temperature created by a warm-up will alter the force−velocity curve of a muscle. The effect is to shift the curve to the right by 12% for each 1°C increase in temperature (Enoka, 1994). The change in contraction velocity (maximal velocity of shortening) results in an increase in peak power output of the muscle (Fig. 4.2).
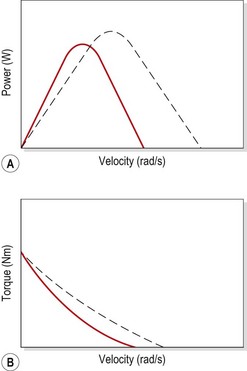
Figure 4.2 Effect of tissue temperature increase due to warm-up. (A) Peak power is increased demonstrated by increased height obtained on vertical jump test. (B) Maximum velocity of shortening increased and torque–velocity curve shifts to the right.
Adapted from Enoka, R.M. (1994) Neuromechanical Basis of Kinesiology, 2nd edn. Human Kinetics, Illinois. With permission.
Large temperature changes have been shown to affect maximal isometric force. Cooling the hand muscles to 15°C reduced maximum isometric force by 30% (Ranatunga, Sharpe and Turnbull, 1987), while warming the quadriceps changed maximal isometric torque from 262 Nm at 30.4°C to 312 Nm at 38.5°C, an increase of 2.4%/1°C (Bergh and Ekblom, 1979b).
Mobilization hypothesis
In the initial period of intense exercise, high amounts of energy are required immediately. The anaerobic reserves are quickly used up, and the aerobic system has not yet become fully functional. The difference between the energy needed and that which can be supplied is known as the oxygen deficit, and represents stored energy and the build up of metabolic wastes (Fig. 4.3). When exercise stops, the body continues to provide energy aerobically to replenish the energy stores and metabolize waste products which have accumulated. This, in turn, creates the oxygen debt.
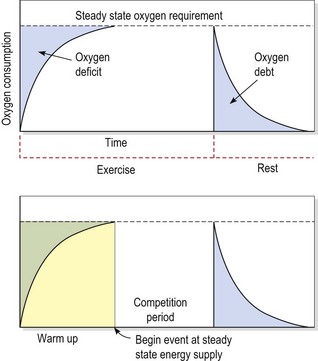
Gutin and Stewart (1971) argued that a function of warm-up was to mobilize the body’s cardiovascular system to reach a steady state. As warm-up was stopped, a brief rest period before competition allowed the oxygen debt to be repaid, without letting the cardiovascular system return to normal levels. When competition commenced, the oxygen deficit would be smaller, and some anaerobic energy would be available to the athlete at the end of exercise.
Gutin et al. (1976) asked subjects to pedal a cycle ergometer at an intensity sufficient to produce a heart rate of 140 b.p.m., a rate which they claimed equated with a 50–60% VO2 max. The subjects’ performance in a subsequent exercise task was significantly better than a control group who did not undertake a warm-up, a result possibly due to the mechanism described above.
A rest period is essential after the warm-up, to allow the oxygen debt to be repaid. But, following rest, the body must be kept warm to maintain the warm-up effects until the athlete competes. As an illustration, Andzel and Gutin (1976) used bench stepping both as a warm-up and exercise task. A 30- or 60-second rest after the warm-up resulted in improved performance, but when no rest period followed the warm-up, performance remained unchanged.
How long should a warm-up last, and what intensity of exercise should be used? A number of papers have addressed these questions. Andzel (1982) compared warm-up periods at an intensity sufficient to produce a heart rate of 120 and 140 b.p.m., followed by a 30-second rest period. Performance was significantly better with the 140 b.p.m. group. Richards (1968) argued that while some warm-ups would enhance performance, others could interfere with performance if fatigue set in. By varying the length of stool stepping, she concluded that a 1- or 2-minute warm-up was superior to a 4- or 6-minute period in her study. Bonner (1974) saw similar effects by altering warm-up periods with a static cycle task. Where performance was reduced in these examples, the workload was obviously too high. Sargeant and Dolan (1987) compared warm-up periods with changing intensity assessed by percentage of VO2 max, and concluded that a 39% VO2 max intensity was superior to a warm-up at 56% VO2 max.
Unfortunately there are no hard and fast rules to guide the athlete in terms of warm-up duration and intensity, but, generally, once the heart rate has reached about 140 b.p.m., this should be sustained for 2–3 minutes. This workload should be sufficient to induce light sweating, and is appropriate for the cardiopulmonary part of the warm-up. Obviously, the time taken to achieve this heart rate will depend on exercise intensity and fitness level, so the total warm-up period will be considerably longer.
Biomechanical effects
Safran et al. (1988) showed that a greater force and length of stretch was required to tear isometrically preconditioned muscles (Fig. 4.4). They claimed that the rise in temperature occurring during the warm-up period could alter the viscosity of the connective tissue within the muscle, and that isometric contractions caused a stretch at the musculotendinous junction. LaBan (1962) showed a 1.5% increase in the length of a stretched tendon following a temperature increase to 42.5°C. Warren, Lehmann and Koblanski (1971) demonstrated increases of 5.8% in length and 58% in force to failure for tendons heated to 45°C.
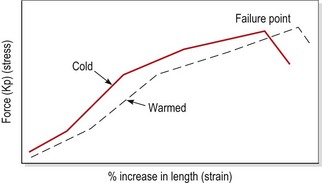
Figure 4.4 The effect of warm-up on tissue failure.
After Safran, M.R. et al. (1988) The role of warmup in muscular injury prevention. American Journal of Sports Medicine, 16 (2), 123–129. With permission.
Shellock and Prentice (1985) argued that muscle elasticity is dependent on blood saturation. They claimed that cold muscles with lower blood saturation levels were therefore more susceptible to injury. Fluids exhibit higher viscosity with lower temperatures, and so joint inertia will be greater when the synovial fluid of a joint is colder.
Changes have also been noted in structural stiffness of muscle following warm-up and exercise. Immediately following activity, muscle stiffness is increased, but can be significantly reduced by stretching. The increase in stiffness is thought to result from thixotropy (Enoka, 1994), the property exhibited by materials whereby they become more fluid when disturbed (shaken). Within muscle, stable bonds are formed between actin and myosin filaments. The bonds are increased following activity, but disengaged by stretching. This has important implications for both warm-up and cool-down. Warm-up will help minimize general muscle stiffness, while cool-down will reduce the actin and myosin bonding which remains following exercise (see also DOMS).
Proprioception has been shown to improve as a result of warm-up (Bartlett and Warren, 2002). Joint position appreciation is more sensitive in the knee after a warm-up, demonstrating that joints seem to accommodate to increased ligamentous laxity which results from a reduction in stiffness due to exercise. The method through which this occurs is thought to be an increase in the sensitivity of the proprioceptive mechanisms around the knee.
Psychological effects
Psychological aspects of warm-up fall broadly into two categories: first, there are psychological effects of a physical warm-up which will be dealt with below; second, aspects of sports psychology, such as visualization and imagery, which are dealt with in the section on sports psychology related to injury.
Two psychological factors are important in the context of warm-up; these are rehearsal and arousal.
Rehearsal
Rehearsal will only take place when an athlete performs a specific warm-up, with actions relevant to the sport to be performed in competition. During the warm-up, the athlete is re-familiarizing him- or herself with the skilled movements required by a sport. Confidence is improved, and the athlete may be more relaxed following this practice.
When an athlete is performing a skilled task, a period of rest followed by resumption of the same task may result in impaired performance. This phenomenon is called warm-up decrement (WUD), and is well documented (Adams, 1961; Schmidt, 1982).
Definition
Warm-up decrement is the gradual loss of the effects of the warm-up in the period between the warm-up and competition.
A number of explanations have been suggested to account for WUD. At a basic level it is seen as simply forgetting an aspect of the motor skill. Nacson and Schmidt (1971) suggested that WUD results from a loss of ‘activity set’. They claimed that a number of variables such as arousal level and attention had to be adjusted (tuned) to a specific task. With practice, the adjustments reach an optimal level, which is reduced with rest. They showed that WUD could be reduced if, during the rest period, a completely different movement was practised. This second movement could not contribute to the memory of the first task, but did require a similar activity set to the original skill.
So far, we have dealt with skills which were practised during the warm-up period to improve subsequent sporting performance. Where one type of training has a direct effect on another, a transfer effect is taking place.
Definition
A transfer effect is the interaction between two similar forms of training. An activity set is a group of variables which are adjusted or ‘tuned’ to a specific physical task.
When the practice of one task improves the performance of another, positive transfer is occurring. However, if during a warm-up skills are practised which are different to those needed for competition, they may interfere with the learning process and negative transfer can occur. Here, performance suffers because a slightly different skill, with a different activity set, is remembered. An example would be practising tennis strokes with a racquet of different weight and size to that of the one used in competition.
Arousal
The second psychological effect of warm-up is that of arousal. The relationship between level of arousal and performance is demonstrated by the inverted-U hypothesis (Fig. 4.5). In a plot of arousal level against performance, initially increased arousal correlates initially with improved performance. But, as arousal continues to increase, an optimal level is reached. Above this point, further arousal is detrimental to performance.
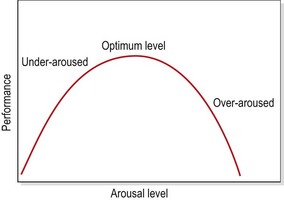
The point of optimum arousal is related to the psychological profile of the athlete and the complexity of the task to be performed. Activities which require fine muscular control (such as archery) or involve important decision-making (such as wicket-keeping) generally require lower arousal levels. Where actions involve gross muscular actions without fine control and without complex decision-making (power-lifting, for example) a higher level of arousal is generally required.
The function of warm-up, therefore, must be to psychologically prepare the athlete, and place him or her at the level of arousal appropriate to the task to be undertaken. A highly motivated (aroused) athlete may need to be relaxed prior to a complex activity. Conversely, a poorly motivated athlete due to compete in a strength event may need to be ‘psyched up’ to an increased arousal level.
Warm-up technique
The intensity and duration of the warm-up period will depend on both the type of activity to be undertaken and the athlete’s fitness. A fitter athlete competing at a high level will take longer to warm-up as the body’s thermoregulatory system will be more efficient.
During cold weather it will take longer for the body’s core temperature to increase, and so the warm-up should be longer or more vigorous. A warm-up should generally be of sufficient intensity and duration to raise the body’s core temperature by 1–2°C, recognized by the onset of mild sweating. The warm-up effects may persist for 45–80 minutes, the time variation being dependent on the rate of heat loss (DeVries, 1980).
Practically, the warm-up may be divided into three parts: pulse raising, mobility and rehearsal (Norris, 2002).
Pulse raising
The pulse raising (cardiovascular or ‘CV’) portion of a warm-up should induce mild sweating, and is best performed wearing a full track suit or other insulating clothing. This will retain body heat and maintains the benefits of the warm-up until competition. Gentle jogging, light aerobics or using CV machines in a gym are all pulse raising activities.
Mobility
Mobility exercises should be performed that are sufficient to take the joints through their full range of motion, the exact range being determined by the movements to be used during sport. The aim is to ensure that the movements used in sport will not overstretch the tissues. A distinction must be made here between maintenance stretching and developmental stretching. Maintenance stretches are used prior to a sport to take the tissues to their maximum comfortable range. For developmental stretching, exercises are used which aim to increase this range of motion, and so a thorough warm-up is performed first. Maintenance stretches therefore form part of a warm-up, while developmental stretches are practised in a separate stretching session.
Rehearsal
To rehearse complex actions in a warm-up, movements may either be performed at a lower intensity level, or split up into their subcomponents. For example, in weight training, the first set of an exercise can be carried out with a light resistance, or even an unweighted bar or stick. In hurdling, the leg action may be practised slowly and to lower levels, gradually increasing in both speed and height until the normal hurdling action has been achieved.
Only when the individual can perform the movement correctly has the rehearsal portion of the warm-up achieved its aim.
Warm-down
On cessation of exercise it is important to reverse the processes which occurred during the warm-up. The heart is no longer helped by the rhythmic contraction and relaxation of the leg muscles. Consequently, to stop intense exercise immediately will increase the demand on the cardiovascular system, causing the heart rate to rise. Metabolic waste products formed during exercise, such as lactic acid, will no longer be carried away from the working area with so much vigour. Instead they will remain in the area, causing pain. This is thought to be one possible cause of delayed onset muscle fatigue (Byrnes and Clarkson, 1985). Flushing the area with fresh blood by performing a gentle warm-down can reduce this effect.
Flexibility training
Flexibility is the range of motion possible at a specific joint or series of articulations, or the amount (amplitude) of joint movement and the general absence of stiffness.
Two types of flexibility are generally recognized, static and dynamic. Static (or extent) flexibility refers to the amount of movement obtained by passively moving a limb to a maximum degree. Dynamic flexibility is concerned with the amount of active movement possible as a result of muscle contraction. The concern here is not so much the degree of movement present as the ease with which it is obtained. This type of flexibility is more important in speed and power events in particular.
Definition
Static flexibility is the amount of movement obtained by passively moving a limb. Dynamic flexibility is the active movement possible as a result of muscle contraction.
Dynamic flexibility must not be confused with agility, which can be defined as the ability to rapidly change the direction of either the whole body or individual body parts without loss of balance (Borms, 1984).
Effects of flexibility training
Flexibility training is generally thought to achieve effects in two broad areas, those of performance enhancement and injury prevention, and these two areas will be addressed here.
Improved performance
To achieve maximal performance, a limb must be able to move through a non-restricted range of motion. In sprinting, for example, lack of adequate dynamic flexibility could result in a reduced stride length with possible reductions in sprinting speed. In addition, greater resistance to movement through increased joint inertia and muscle stiffness at the end of movement range is more energy consuming.
Good flexibility is associated with good sporting performance in all activities where a maximal amplitude of movement is required to achieve the best technical effects. Similarly, a limited range of movement can reduce work efficiency in these situations. In addition, if flexibility is increased, force may be applied over an increased distance, thus facilitating acceleration of an implement.
Injury prevention
A variety of authors have argued that flexibility may condition tissues to have greater tensile strength and elasticity, leading to injury prevention and a reduction in soft tissue pain. This has led some to suggest that the type of training programmes undertaken could affect the number of injuries suffered (Ekstrand et al., 1983). There is some evidence to support this stand. Netball players who had not warmed up were shown to have an increased risk of injury (Hopper, 1986), while warming up and stretching have been shown to be important factors in the prevention of hamstring injuries in Australian football (Seward and Patrick, 1992). In a study of army recruits, Hartig and Henderson (1999) showed the effect of hamstring stretching over a 13-week period on overuse injuries. Using 298 subjects, they showed an incidence rate of 29.1% for the control (non-stretching) group and 16.7% for the stretching group.
Muscle stiffness has been shown to reduce as a result of stretching (McNair and Stanley, 1996). Using five repetitions of a static stretch and holding each repetition for 30 seconds, stiffness was reduced to the same degree as with a warm-up for 10 minutes at 60% HR max. Static stretching has also been shown to improve muscle compliance and enhance muscle force development (Rosenbaum and Henning, 1995) as well as reduce the passive resistance offered by a muscle. This latter effect has been shown to return to pre-stretching levels within 1 hour (Magnusson, Simonsen and Kjaer, 1996). These biomechanical changes affecting muscle stiffness could lead to an injury prevention effect of stretching.
Although individual studies indicate the possibility of an injury prevention effect of stretching, taken as a whole the research does not support this. Herbert and Gabriel (2002) summarized the information gained from five studies and concluded that there was no evidence that stretching either before or after exercise protects against muscle soreness or risk of injury. In a later study Weldon and Hill (2003) conducted a review of seven papers and decided that no definitive conclusions could be made concerning the value of stretching, due to the poor quality of the available studies. Fradkin et al. (2006) conducted a systematic review of studies from 1966 to 2005 and concluded that although there was insufficient statistical evidence to endorse or discontinue routine warm-up ‘the weight of evidence is in favour of decreased risk of injury’.
Tightness occurs in muscle groups in set patterns, with the biarticular muscles (mobilizers) showing a greater tendency to shorten. For example, of the hip extensors, it is the hamstrings (biarticular) rather than the gluteals (uniarticular) which commonly show tightness and injury through tearing. Tightness of the muscle may pull a joint out of alignment, altering the equilibrium point of the joint and predisposing to joint injury.
Flexibility training and muscle power output
Muscle power depends not just on muscle contraction, but on a combination of active contraction, muscle reflex activity and elastic recoil of the non-contractile elements associated with a muscle. We have seen that one effect of flexibility training is to reduce muscle stiffness. This in turn could have a direct effect on power development by changing the elastic forces created by the rebounding muscle.
Kokkonen et al. (1998) tested subjects with a one repetition maximum (1 RM) lift, and found the subject’s lifting ability to be reduced by 7–8% following static stretching. Using a footplate to stretch and measure strength output from the soleus muscle Fowles et al. (2000) used 13 maximal passive stretches over a half-hour period, holding each stretch for over 2 minutes. Again they measured maximal muscle contraction and found that strength in the stretching group reduced by 28% immediately after stretching, reducing to 12% after 30 minutes and 9% after 60 minutes. Using a leg extension exercise Behm et al. (2001) used 20 minutes of static stretching, with each repetition held for 45 seconds. These authors found a 12% decline in maximal leg strength, confirming the results of the previous studies.
A number of mechanisms may be responsible for this stretch-induced decline in strength output. EMG measurement has revealed a 20% decline in quadriceps activity after stretching (Behm et al., 2001). Muscle activation (using interpolated twitch) has also been shown to decrease by 13% (Fowles et al., 2000).
In addition to alteration in muscle stiffness and electrical changes to the muscle, microscopic damage similar to that seen following eccentric activity also seems to occur. Creatine kinase (CK) levels have been shown to increase by over 60% following intense stretching (Smith et al., 1993), confirming this.
Muscle reflexes
A number of structures can limit joint range of motion (Table 4.8) and the ability of muscle to relax and allow a stretch to occur is one of the most important in sport. For this reason, three muscle reflexes are important when using flexibility training, the stretch reflex, autogenic inhibition, and reciprocal innervation (Table 4.9).
Table 4.8 Factors limiting range of motion at a joint
Table 4.9 Muscle reflexes and stretching
| Stretch reflex | |
| Responds to: | |
| —change in velocity (phasic) (e.g. knee jerk reflex) | Facilitatory (↑ tone) |
| —change in length (postural) (e.g. body sway) | |
| Autogenic inhibition | |
| (the reverse stretch reflex) | |
| —Golgi tendon organ (GTO) measures tension | Inhibitory (↓ tone) |
| Reciprocal innervation | |
| —Agonist contracts, antagonist relaxes to allow movement | Inhibitory (↓ tone) |
When a muscle is stretched, elongation is detected by the muscle spindle afferent nerve fibres. These receptors send impulses to the dorsal roots of the spinal cord, and a reflex is caused which contracts the extrafusal fibres of the same muscle, in opposition to the original stretching force. The reflex is therefore facilitatory. The stretch imposed may be either sudden (as in a knee jerk reflex), where the muscle responds to a change in velocity, or prolonged (as with postural sway), where the muscle measures the change in length.
In addition to the muscle spindle, the Golgi tendon organ (GTO) in the muscle tendon will also register stretch. Both these receptors are affected by changes in muscle length, but the GTO is also receptive to changes in muscle tension (Bray et al., 1986).
When a muscle is stretched, there is a corresponding stretch of the muscle spindle. But, if the stretch lasts for longer than 6 seconds, the GTO registers not only the change of length of the muscle, but also the alteration in tension in the muscle tendon. The GTO will then cause a reflex relaxation of the muscle, a process known as autogenic inhibition or the reverse stretch reflex. This has a protective function, causing the muscle to relax and allowing it to stretch before it is damaged. It is therefore inhibitory.
Stretching which involves short jerking movements will tighten the muscle through the stretch reflex, while movements lasting for longer than 6 seconds will allow the muscle to relax again through stimulation of the GTO, which will override the stretch reflex. If the tension of the muscle to be stretched is increased through isometric contraction, once relaxed the muscle tone will reduce below normal resting levels, enabling a greater stretch to be applied. The stretch reflex (H reflex) has been shown to be suppressed for 10 seconds following isometric contraction of this type (Moore and Kukulka, 1991), giving a 10-second period during which stretching may be applied.
Definition
The H reflex (Hoffman reflex) is an artificially induced equivalent of the stretch reflex produced in a laboratory by stimulating a muscle with a single electric shock.
When a muscle is tensed, a reflex relaxation of the antagonist will occur, a process known as reciprocal innervation. If, for example, the biceps muscle contracts to flex the elbow, its antagonist, the triceps, must relax to allow the movement to occur. This reflex is modified in co-contraction, where both the agonist and antagonist muscles contract simultaneously (Levine and Kabat, 1952). Co-contraction functions to increase joint stiffness and contributes to stability and accuracy of rapid movements (Enoka, 1994).
Most coaches, athletes and therapists would recognize that regular stretching can increase range of motion. One of the methods by which this occurs may be neural plasticity at spinal level (Alter, 1996). Experiments with monkeys (Wolpaw, Lee and Carp, 1991) have shown that the H reflex can be modified as a result of using EMG biofeedback. The magnitude of the H reflex can be increased, reduced or altered completely, and following surgical transection of the spinal cord these changes remain, indicating that the plasticity is occurring at spinal level rather than through brain influence. It may be possible that the threshold of the stretch reflex in man can be altered through a process of desensitization (habituation) so that the reflex threshold is higher (less likely to occur). This would modify the muscle’s resistance to stretching and thereby increase available range of motion. Neuronal activity has been shown to reduce with both static and ballistic stretching (Vujnovich and Dawson, 1994).
Techniques of flexibility
Five methods of stretching are generally recognized: static, ballistic, active and two proprioceptive neuromuscular facilitation (PNF) techniques (Table 4.10).
Table 4.10 Summary of stretching techniques
Static stretching
During static stretching, a muscle is stretched to the point of discomfort and held there for an extended period. As the muscle is held, the athlete will feel a reduction in the pain stimulus from sharp acute pain to a more dull diffuse sensation. If the static stretch is held by the therapist, the end-feel of the muscle resistance will change from a strong (firm) elastic feel to a more yielding feel. Static stretches should be held for a prolonged period. A 30-second hold has been shown to be more effective than a 15-second hold, with no greater benefit seen when the holding time is extended to 60 seconds (Bandy and Irion, 1994). Four or five repetitions should be performed, as no further benefit is seen when the number of repetitions is increased from this (Taylor et al., 1990).
Ballistic stretching
Ballistic stretching involves taking the limb to its end of movement range, and adding repetitive bouncing movements. There is a suggestion that injury may result from abrupt stretching of this type (Etnyre and Lee, 1987) and so the technique has become less popular. Although this may be true for vigorous ballistic stretches which are uncontrolled, adding small stretches to the end of range gained by static stretching (pulsing) has been shown to reduce neurone excitability further than static stretching alone (Vujnovich and Dawson, 1994). To perform ballistic stretching more safely, firstly it should be given after static stretching, and secondly it should be given progressively in terms of both velocity of stretch and range of motion. Such a stretching session would begin with a warm-up and then move to static stretching (5 reps, each held for 30 seconds), which would then progress to 3–5 reps of end range pulsing (high velocity, short range). This would then progress to longer range movements at slow velocity, and finally to long range movements at steadily increasing velocity.
Active stretching
Active stretching involves pulling a limb into full inner range so that the antagonist muscle is stretched passively while the agonist is strengthened. This type of stretch is important when correcting muscle imbalance. The inner range contraction is used to shorten a lengthened (lax) muscle, while the shortened muscle is stretched using a functionally relevant movement.
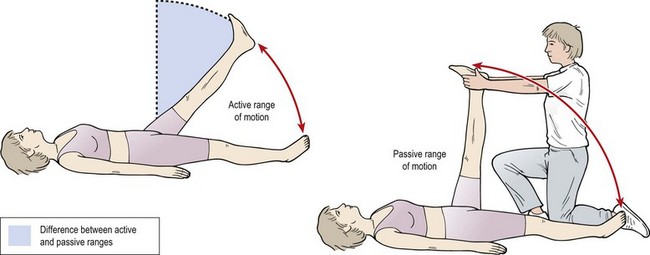
When stretching a biarticular muscle, full inner range contraction is not possible at both ends simultaneously and so the opposing muscle cannot be fully stretched. For example, the hamstrings cannot pull the hip to full inner range extension and the knee to full inner range flexion at the same time, as they are activity insufficient. This means that the rectus femoris muscle will in turn not be fully stretched. Passive range of motion will therefore be greater than active range of motion for a biarticular muscle. One of the aims of stretching, however, should be to reduce this difference to a minimum, giving the athlete active control over a greater range of motion (Fig. 4.6), as this may reduce the likelihood of injury (Lashville, 1983). In addition, although passive range of motion is greater than active, the active range normally more closely resembles the movements used in sport and so is more specific.
One of the main advantages of active stretching in the early period of rehabilitation is the control that the athlete has where pain is present. As one muscle is being tightened to stretch another, the athlete is in control of the movement throughout. This may give the athlete the confidence to stretch into ranges which they would not normally be prepared to enter in the presence of pain.
Treatment note 4.2 Passive stretching
There are several passive stretching techniques which are useful in the clinic situation. The therapist applies these on the patient initially without the patient taking an active part in the procedure. Once full passive range has been obtained through a hold−relax technique, contract−relax and CRAC procedures may be used with the same exercise.
Hamstrings
Straight leg raising may be performed with the patient’s leg resting on the therapist’s shoulder. The leg is held with one hand to stop it slipping and the other hand keeps the knee locked. The therapist takes up a walk standing position with the weight on the back leg to begin (Fig. 4.7); as the stretch is put on, the therapist shifts the weight onto the front leg by lunging forward. In this way the therapist protects his or her back and avoids moving into a flexed position of the trunk.

To emphasize the upper portion of the hamstrings (ischial origin), the patient’s knee is flexed by 20° by altering the hand position. The whole leg is pressed into hip flexion, maintaining the slightly flexed knee position (Fig. 4.8).

Rectus femoris
The rectus femoris is stretched in a side lying position (Fig. 4.9). The affected leg is uppermost and the patient bends the underneath knee and holds onto this, to guard against anterior pelvic tilt and hyperextension of the lumbar spine as the stretch is put on. The therapist flexes the knee and holds this flexed position using pressure of his/her abdomen. The femur is then pulled back into extension using hand pressure over the knee and pelvis. Where the upper portion of the rectus is to be targeted, knee flexion is released slightly to allow for a greater extension stretch at the hip. It should be remembered that only 15° of extension is available at the hip before anterior pelvic tilt begins. Further extension range will therefore affect the lumbar spine rather than impose a greater stretch on the rectus.

Upper trapezius
The upper trapezius is frequently overactive and may develop painful trigger points. The stretch is performed in supine lying to allow the therapist to use massage techniques over the muscle belly if required.
For the right trapezius (Fig. 4.10), begin by elevating the right shoulder to relax the trapezius. Laterally flex the neck to the left and maintain this position using pressure with the right hand. Impart the stretch by pressing down on the right shoulder with the left hand. An X grip of this type is easier for the therapist to apply, while pressing on the shoulder rather than the neck is more comfortable for the patient. The stretch may be varied by using neck flexion with the patient’s head on a block or rolled towel.

When using massage techniques with the muscle on stretch, the neck and shoulder position may be maintained by using the left forearm as a ‘strut’ between the two structures. The right hand is then free to apply the massage technique.
PNF stretching
PNF (proprioceptive neuromuscular facilitation) techniques have been adopted by the sporting world from neurological physiotherapy treatments. These techniques use alternating contractions and relaxations of muscles and capitalize on the various muscle reflexes to achieve a greater level of relaxation during the stretch.
Two PNF techniques are used in sport, contract-relax (CR) and contract-relax-agonist-contract (CRAC). The CR technique involves lengthening a muscle until a comfortable stretch is felt. From this position, the muscle is isometrically contracted, and held for a set period. The muscle is relaxed, and then taken to a new lengthened position until the full stretch is again felt by the subject. The rationale behind the CR method is that the contracted muscle will relax as a result of autogenic inhibition, as the GTO fires to inhibit tension. Some authors argue that a maximal isometric contraction is needed to initiate relaxation through the GTO mechanism (Janda, 1992). Others recommend the use of minimal isometric contractions (Lewit, 1991) which seem more appropriate in situations where pain is present.
With the CRAC method, the muscle is stretched as above, but in the final stages of the stretch, the opposing muscle groups are isometrically contracted as the stretch is applied, to make use of reciprocal inhibition of the agonist and reduce its tension. PNF stretches have been shown to be more effective than static or ballistic movements (Holt, Travis and Okita, 1970; Cornelius and Hinson, 1980; Holt and Smith, 1983; Etnyre and Abraham, 1986), with CRAC methods generally being better than CR.
There are two major disadvantages to PNF techniques. First, the extra tension developed in the muscle results in greater pain, and this in turn may reduce user compliance, an important consideration in early rehabilitation. Secondly, as PNF involves isometric contractions, the user must be discouraged from holding the breath and using a valsalva manoeuvre. The raised intra-abdominal and intra-thoracic pressure which occurs with this technique can lead initially to a reduction in venous blood flow to the heart and a decreased cardiac output. On expiration, increases in blood pressure in excess of 200 mmHg have been recorded (Alter, 1996).
Keypoint
When using PNF stretching athletes must not hold their breath during the isometric phase of the movement. They should breathe normally throughout the motion range.
An extensive description of stretching exercises with teaching points, measurement and uses may be found in Norris (2007). Video footage of exercise technique together with printable stretching exercise prescription sheets is shown in Norris (1996).
Factors affecting flexibility
The amount of movement present at a joint during a stretch (amplitude) is affected by internal (body) and external (environmental) factors (see Table 4.8). Internal factors include the bony contours of the joint. These will differ among individuals, and in certain pathologies such as arthritis, movement will decrease as bone formation changes. These factors cannot readily be affected by flexibility training but must be taken into consideration when prescribing stretching programmes, especially with the elderly and during rehabilitation.
Other internal factors include volume of surrounding tissue, an obese individual frequently being less flexible than a lean one. Muscle tissue, tendons and joint capsules are other internal factors which may result in movement limitation. Jones and Wright (1982) indicated that 47% of mid-range stiffness is due to the joint capsule, 41% due to muscle fascial sheaths, 10% due to the tendon and 2% due to the skin. Other factors include cartilage and viscosity of joint fluid (Holland, 1968). Muscle tension will limit range of motion, providing active resistance. When a muscle is relaxed, the connective tissue framework of the muscle rather than the myofibrillar elements will provide a passive resistance.
Temperature is one external factor which affects flexibility (see p. 95). An increase in tissue temperature can result in both a reduction in synovial fluid viscosity and increased soft tissue extensibility. At a temperature of approximately 40°C a thermal transition of collagen occurs, allowing a greater plastic deformation when stretched (Rigby, 1964). Elastic (recoverable) deformation of connective tissue is favoured by high force, short duration stretching with tissue at normal body temperature or slightly cooled, while plastic deformation (permanent lengthening) is greater with lower force, longer duration stretching at elevated temperatures. If the tissue is then allowed to cool in this stretched position, results may be better (Sapega et al., 1981).
Individual variations in body structure can have apparent effects on flexibility. Individuals with long slender limbs are likely to be more flexible than shorter individuals with thicker musculature. However, good flexibility in one joint does not guarantee similar attributes in other joints, because flexibility has been shown to be joint specific (Harris, 1969).
In general, flexibility decreases with age (Harris, 1969), although among individuals this trend is very much dependent on activity levels and other lifestyle factors (Borms, 1984). A general belief is that girls are more flexible than boys, but it is not clear whether this is due to body structure or social and environmental influences (Goldberg, Saranitia and Witman, 1980).
Therapeutic stretching
When stretching is used as a manual therapy to mobilize a joint after injury or surgery, the various techniques will be combined. If muscle spasm is the limiting factor, ice may be used to limit the pain and this may be combined with PNF stretching (cryostretch procedures). However, to stretch connective tissue effectively, higher than normal temperatures are required, so heat is the modality of choice, where muscle spasm does not limit movement.
The ability of the heat source to reach the tissue to be stretched must be considered, and this will largely depend on the tissue depth and vascularity. In superficial tissues and joints superficial heat (heat lamp, hot pack, hot water soak) will have a beneficial effect on tissue extensibility. The deeper tissues will not be heated directly. However, muscle spasm may reduce as a result of pain relief. Deeper heating (microwave, shortwave diathermy, ultrasound) may have a direct heating effect on deeper tissues, enabling some of the temperature dependent effects on tissue to be achieved (Sapega et al., 1981).
After heating, passive stretching may be applied by the therapist, or, where long term stretch is to be used, pulley systems and weights can apply the passive stretch. This is especially useful for an immobile joint where adhesions limit movement.
Strength training
Strength is the ability to overcome a resistance; it is the maximum tension which a muscle can produce (McArdle, Katch and Katch, 2001). Strength is usually measured as the torque exerted in a single maximal isometric contraction of unrestricted duration (Enoka, 1994). However, clinically it is important to define the type of strength by prefacing the term with the category of muscle contraction which was used. We should therefore talk of isometric or isotonic strength, rather than simply strength alone.
Adaptation to resistance training
Muscular contraction involves a combination of physiological and neurological processes, and consequently adaptations to resistance training are both myogenic (structural) and neurogenic (seen on EMG only) in nature (Table 4.11).
Table 4.11 Physiological adaptations to resistance training
| Variable | Response |
|---|---|
| Muscles fibres | |
 Number Number |
? |
| Size |
Increase |
| Type |
? |
| Strength |
Increase |
| Capillary density | |
| Bodybuilders |
No change |
| Powerlifters |
Decrease |
| Mitochondria | |
| Volume |
Decrease |
| Density |
Decrease |
| Twitch contraction time | Decrease |
| Enzymes | |
| Creatine phosphokinase |
Increase |
| Myokinase |
Increase |
| Phosphofructokinase |
Increase |
| Carbohydrate metabolism |
Increase |
| Basal metabolism | Increase |
| Intramuscular fuel stores | |
| ATP |
Increase |
| Phosphocreatine (PC) |
Increase |
| Glycogen |
Increase |
| Triglyceride |
? |
| VO2 max | |
| Circuit weight training |
Increase |
| Heavy resistance training |
No change |
| Connective tissue | |
| Ligament strength |
Increase |
| Tendon strength |
Increase |
| Body composition | |
| % fat |
Decrease |
| Lean body mass |
Increase |
| Bone | |
| Mineral content/density |
Increase |
| Cross-sectional area |
No change |
Source McArdle, W.D., Katch, F.I. and Katch, V.L. (2002) Exercise Physiology, 5th edn. Lippincott, Williams and Wilkins, Philadelphia. With permission.
Keypoint
Adaptations to resistance training are from both myogenic (structural) and neurogenic (functional) sources.
Myogenic changes
Hypertrophy
One of the most noticeable myogenic adaptations to resistance exercise is increased muscle size through muscle growth or hypertrophy. Increased cross-sectional area has been found to result from an increase in size of individual muscle fibres. Hypertrophied muscle fibres may have 30% greater diameter and 45% more nuclei (McArdle, Katch and Katch, 2001). The increase in size occurs in both type I (slow twitch) and type II (fast twitch) fibres. Selective hypertrophy can occur, causing just the type I or just the type II fibres to increase in size, the ratio between the two fibre types remaining the same. In normal adults the ratio is about 1 : 1 or 2 : 1, but in competitive bodybuilders ratios as high as 6 : 1 have been found, compared to 0 : 1 in sprinters (Astrand and Rodahl, 1986). In addition, heavy resistance training has been shown to increase the proportion of type IIA (fast oxidative glycolytic) fibres (Bandy, Lovelace-Chandler and McKitrick-Bandy, 1990).
In addition to the increase in fibre size, which occurs with hypertrophy, connective tissue proliferation is also seen (McArdle, Katch and Katch, 2001). Thickening of the muscle’s connective tissue support, and that of the musculotendinous junction, may reduce the risk of soft tissue trauma.
Keypoint
With resistance training connective tissue as well as muscle is enhanced, providing the possibility for injury reduction.
Endurance training has long been known to increase the number of mitochondria and the capillary density (number per square millimetre of tissue). However, resistance training is thought to lead to hypertrophy without a significant increase in the number of capillaries (Astrand and Rodahl, 1986). As the number of capillaries stays the same but the size of the muscle tissue increases, the capillary density is reduced. Each capillary must now supply a greater fibre area with oxygen and nutrients, a factor which may account for the relatively poor aerobic capacity of athletes who train solely for strength.
Alterations in muscle energy stores have been reported following resistance training programmes. Increased intramuscular stores of adenosine triphosphate (ATP) and creatine phosphate (CP) have been reported (MacDougall et al., 1977). Similarly, increases in two of the enzymes of anaerobic glycolysis (phosphofructokinase and lactate dehydrogenase) have been reported (Costill et al., 1979). Increases in phosphogen stores and the enzymes of anaerobic glycolysis could be expected to prolong the maintenance of a maximal muscle contraction (Bandy, Lovelace-Chandler and McKitrick-Bandy, 1990).
Hypertrophy in seniors
Weight training was once thought of as the preserve of the young. However, research now shows that muscle training effects are significant in seniors as well. Increases of muscle volume of 26%, peak torque of 46% and 28.6% in total work output have been reported following resistance training programmes for healthy men with an average age of 67 years (Roman, 1993; Yarasheski, 1993; Sipala and Suominen, 1995). In even older subjects, Fiatarone (1994) tested a 10-week resistance programme on 63 women and 37 men and showed average strength increases of 113% and increase in cross-sectional area of 2.7%. Perhaps of more importance were the improvements in functional ability which these physiological changes achieved, with significant improvements in gait velocity (11.8%) and stair climbing speed (28.4%).
Hyperplasia
The possibility of muscle fibre splitting (hyperplasia) in humans has always been a contentious subject. A greater number of muscle fibres is seen in competitive bodybuilders, but this is thought to be a congenital feature of the more successful athletes (Bandy, Lovelace-Chandler and McKitrick-Bandy, 1990). New muscle fibres may develop from satellite cells. These cells lie between the sarcolemma and the basal lamina of the muscle fibre at the end of the muscle. They are normally dormant, but become active in the case of muscle injury, and when stimulated they proliferate. With high intensity muscle training, satellite cell activation may occur to replace cells damaged by training. There may be no significant gain in fibre number therefore. Longitudinal splitting may occur where a large muscle fibre splits into two daughter cells (a process known as lateral budding) (Gonyea et al., 1986). In mammals, hyperplasia through satellite cell proliferation and longitudinal splitting does occur, but only where hypertrophy is not the main system of muscle growth (McArdle, Katch and Katch, 2001). In humans, most authors agree that the increase in cross-sectional area following resistance training is the result of hypertrophy rather than hyperplasia.
Neurogenic changes
Significant strength gains may be made at the beginning of a strength training programme without noticeable changes in muscle size. The increase in strength is thought to be the result of more efficient activation of the motor units (Astrand and Rodahl, 1986). As Sale (1988) stated, ‘strength has been said to be determined not only by the quantity and quality of the involved muscle mass, but also by the extent to which the muscle mass has been activated’.
Increased EMG activity occurs during maximal muscle contraction following a resistance training programme, indicating an increased recruitment of motor units and a greater firing rate (Bandy, Lovelace-Chandler and McKitrick-Bandy, 1990). For a muscle to produce its greatest force, all of the motor units it contains must be recruited. Normally, high threshold motor units are only recruited in periods of extreme need, with the smaller motor units being recruited first. The small diameter slow oxidative (SO) fibres are recruited at low force levels, while the larger fast glycolytic (FG) fibre may not be recruited until 90% of maximum force production is reached. Between these two extremes, lower threshold FG and fast oxidative glycolytic (FOG) fibres are recruited (Fig. 4.11A).
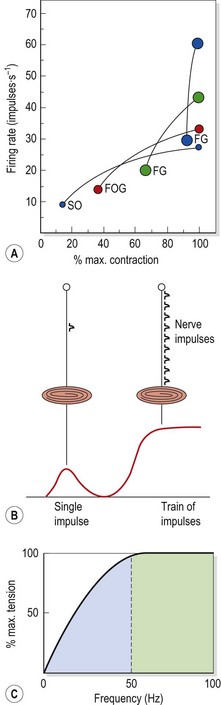
Figure 4.11 Neural adaptation to strength training. (A) The size of motor unit recruitment. The small slow twitch oxidative (SO) motor units are recruited at low force levels. The largest high threshold fast twitch glycolytic (FG) are not recruited until 90% maximal force is obtained. Between these two extremes are the lower threshold FG units and the fast twitch oxidative glycolytic (FOG). For each line, the low point shows the recruitment threshold and the high point shows the maximum firing rate obtained with maximum contraction force. (B) Effect of firing rate on muscle force. A single impulse from the axon to the muscle creates a twitch contraction giving a low force output. A high frequency train of impulses (high firing rate) creates a longer tetanic contraction, giving a force which is ten times greater. (C) Force–frequency curve. At low frequencies small increases in frequency give very large increases in force. At high frequencies the reverse is true, and doubling the frequency from 50 Hz to 100 Hz gives virtually no corresponding increase in force.
From Sale, D.G. (1992) Neural adaptation to strength training. In Strength and Power in Sport (ed. P.V. Komi). IOC Medical Publication, Blackwell Scientific, Oxford. With permission.
Keypoint
Small diameter motor units are recruited at lower resistances. The largest diameter fibres may not be recruited until 90% of maximum voluntary contraction (MVC) is reached.
In addition to enhanced recruitment, an increase in firing rate (frequency) of motor units is also seen. A single nerve impulse will cause an isolated twitch response, while a number of impulses are required to produce a sustained contraction (Fig. 4.11B). The greater the excitation of a motoneurone, the greater the firing rate of the motor unit in impulses per second (Hz). Motor units fire at rates of between 10 and 60 Hz, with large increases in force seen for small increases in frequency at the lower end of the spectrum. At the higher end (Fig. 4.11C), increasing the frequency of motor unit excitation has little effect on force production.
With strength training, a subject may gain the ability to recruit the large motor units more easily and so increase the muscle force production. In addition, the firing rate of the motor units utilized in a contraction may be enhanced with training.
Motor unit synchronization (groups of motor units being activated together) has been shown to be greater in strength athletes than control subjects, and is likely to increase as a result of a resistance training programme. This change is more likely to increase the rate of force development rather than peak force itself (Sale, 1988).
Evidence for neural adaptation following strength training comes from EMG studies which show increased activation of prime movers, as a result of improved skill and coordination. For example, during plyometric exercise the high stretch load can result in a period of inhibition at the start of the eccentric phase while the trained individual shows facilitation, possibly as an adaptation of reflex response (Sale, 1992).
Activation of the prime mover may be limited by insufficient motivation, or inhibition. During new strength tasks, excessive co-contraction may occur to stabilize and protect the moving joints. Simultaneous contraction of the antagonist will reduce the force output of the agonist through reciprocal inhibition. Training could reduce the co-contraction and allow greater activation of the agonist muscle group resulting in a greater force output (Sale, 1988). Such inhibition may explain the phenomenon of bilateral deficit (Sale, 1992). In a weight-training exercise which requires the simultaneous use of both limbs (for example, the squat, leg press or arm pressing movements), the total force which a subject can produce is often considerably less than the sum of the force of the individual limbs acting alone. In contrast to this inhibitory interlimb effect, cross-education represents an overflow of chronic changes from the working muscle to the non-working muscle. This is commonly seen in rehabilitation where an injured muscle may be enhanced by working its uninjured counterpart. Both bilateral deficit and cross-education represent neural adaptation as there are often no significant morphological changes.
Increases in load may occur in resistance training without substantial elevations in strength. Rutherford (1988) cited an example of subjects training on a leg extension exercise. Improvements of 200% in load lifted were accompanied by strength increases of only 11%. He argued that increased coordination of muscles used as ‘fixators’ in the leg extension movement could account for the improved weight training ability.
Whatever the exact mechanisms involved, it seems clear that neural adaptation is largely responsible for the initial strength gains following a resistance training programme. Gains made later on are more likely to result from muscle hypertrophy. In addition, neural adaptation is likely to be one of the factors leading to specificity of strength training.
Specificity of strength training
Maximum force production from a muscle is, then, the result of a blend of myogenic and neurogenic adaptations which are specific to a particular movement pattern. Improvements in contractile properties such as maximum force, velocity of shortening and rate of tension development can vary with the type of contraction used in training. Training a muscle to perform in a particular movement is not simply a question of overloading it against a resistance. For example, strengthening the leg muscles with a squatting exercise will not increase the performance on a leg extension movement to the same degree as training the same muscles on a leg extension bench. To strengthen a muscle for a specific movement, an exercise must mimic the movement as closely as possible. Similarly, strength gains resulting from isometric training will be specific to the joint angle at which the training was carried out.
Training a muscle at a specific velocity will result in strength gains at speeds close to, or less than, the training velocity (Rutherford, 1988), a phenomenon known as velocity specificity. One explanation of this principle is that before training, subjects are unable to produce maximal contractions at all velocities, and through practice they learn to fully activate their prime movers only at the velocities used during training.
Another possibility is preferential hypertrophy of one fibre type. There is little evidence for transformation of one fibre type to another, except following electrical stimulation. Preferential hypertrophy of type II fibres does occur, but at both fast and slow velocities, so the neural explanation seems more likely.
Muscle work
Muscle contractions may be categorized into two types, static (isometric) where the limb segments do not move, and dynamic (isotonic) where movement does occur. The term isotonic (same tension) is confusing, however, because as the limb segments move, leverage forces change and the muscle tension varies continually.
Dynamic contractions may be subdivided into either concentric (muscle shortening) or eccentric (muscle lengthening). Isokinetic contractions are dynamic (and may be concentric or eccentric), but the speed of contraction is held constant by continually varying the resistance. Isokinetic systems do not permit acceleration, the speed being held constant. Isoacceleration (Westing, Seger and Thorstensson, 1991) involves a subject working against a preset acceleration (concentric) or deceleration (eccentric).
The term ‘isotonic’ has come to be used to describe a concentric or eccentric contraction performed using free weights or a machine which offers a fixed resistance, and this convention is adhered to in this book for clarity.
During concentric contractions, alterations in leverage of the limb throughout the movement mean that the resistance imposed can be no greater than the weakest part of the muscle force curve. If the resistance exceeds the weakest point, the movement is not completed, and the subject reaches a ‘sticking point’. The force generated with concentric exercise cannot therefore be maximal throughout the range.
Eccentric training
During an eccentric contraction the muscle is lengthening under active tension. Eccentric contractions are frequently used to resist gravity, the muscles being used as a ‘brake’. Tensions developed during eccentric contractions are greater than those of concentric or isometric contractions, leading some authors to argue that the training effect is superior (Darden, 1975).
Greater strength increases have been demonstrated using eccentric training in comparison with concentric activity. Subjects working eccentrically for six repetitions at 120% of the concentric 1 RM have been shown to produce equivalent strength gains to those performing 10 repetitions at 80% of 1 RM (Johnson et al., 1976). However, the amount of muscle soreness (DOMS) encountered with pure eccentric work makes it more appropriate to start a training period with concentric contractions and progress to eccentric contractions in the final stages. In addition, training specificity and safety considerations make eccentric training in isolation less desirable.
Lengthening a muscle immediately before a concentric action will increase the force output of the muscle, a process known as pre-loading. Vertical height attained in a single leg and a two leg squat is significantly increased with pre-loading (Fig. 4.12) (Enoka, 1994). The pre-load effect occurs because it takes time for the chemical processes involved in muscle contraction to come on line. Actin and myosin coupling is not immediate but is ‘ramped up’ as the muscle is stimulated. By beginning a jump with the muscle partially contracted, this period is taken up (Jaric, Gavrilovic and Ivancevic, 1985).
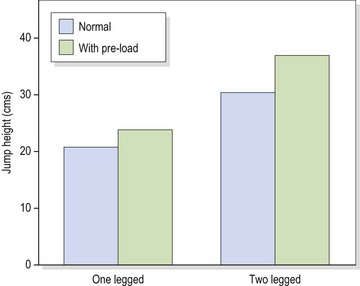
Figure 4.12 Effect of pre-loading on vertical jump height.
From Enoka, R.M. (1994) Neuromechanical Basis of Kinesiology, 2nd edn. Human Kinetics, Illinois.
Another method of producing power during eccentric action is the stretch–shorten cycle. Here, the muscle to be worked is first stretched, and the total power produced consists of contractile force and elastic recoil of the inert muscle structures.
Plyometrics
Rapid eccentric contraction used immediately before an explosive concentric action (stretch–shorten cycle) forms the basis of plyometric training. This type of training was first used in Eastern Bloc countries in the development of speed (Verhoshanski and Chornonson, 1967). The movements involve a pre-stretch of a muscle, followed by a rapid contraction, causing the athlete to move in the opposite direction. Effects are achieved in both the contractile and inert structures of the muscle.
The rapid stretch of the muscle stimulates a stretch reflex, which in turn generates greater tension within the lengthening muscle fibres. In addition to increased tension, the release of stored energy within the elastic components of the muscle makes the concentric contraction greater than it would be in isolation. Increased tension will in turn stimulate Golgi tendon organ (GTO) activity, inhibiting excitation of the contracting muscle. Desensitization of the GTO has been suggested as a possible mechanism by which plyometrics allows greater force production (Bosco and Komi, 1979).
The use of muscle contraction involving acceleration in the concentric phase and deceleration in the eccentric phase more closely matches the normal function seen in sport, and therefore has advantages in terms of training specificity. However, the rapid movements involved are not suitable in early stage training as they can be relatively uncontrolled.
Several neuromuscular adaptations have been proposed for the effect of plyometric exercise (Table 4.12), and exercise of this type has been shown to significantly increase peak power output (Potteiger, 1999). Comparing plyometric exercises with their non-power equivalents demonstrates the advantages of this training. A plyometric jump compared to a deep knee bend action used 22% less energy, produced 9% more work and was 40% more efficient (Lees and Graham-Smith, 1996), while a rebound bench press compared to a standard lift gives 30% more work, allowing the athlete to lift 5.4% greater weight.
Table 4.12 Proposed neuromuscular adaptations to plyometric training
Source Potteiger, J.A. (1999) Muscle power and fiber characteristics following 8 weeks of plyometric training. Journal of Strength and Conditioning Research, 13 (3), 275–279. With permission.
Practical considerations of plyometric training
Plyometric exercise is only effective when the concentric contraction occurs immediately following the pre-stretch cycle. If there is a pause in activity, some of the benefits are lost as elastic energy is wasted, and the effect of the stretch reflex is altered (Voight and Draovitch, 1991). The ability to recover the stored elastic energy within the tissues depends on the time period between concentric and eccentric activity, known as the coupling time. The stored elastic energy of the leg extensor muscles has a half life of 4 s (Lees and Graham-Smith, 1996), and the coupling time in plyometric exercise has been measured at average periods of 23 ms. Providing the coupling time remains at these levels, nearly all the stored elastic energy can be utilized.
Injury considerations in plyometrics
This type of training is intense, and should only be used after a thorough warm-up, and usually at the end of an exercise programme. To perform plyometrics, the athlete needs a good strength base, and his proprioceptive activity should be tested using single leg standing and single leg half squats (eyes closed, position maintained for 30 seconds) before training commences. Any loss in proprioception may cause the athlete to fall as fatigue sets in. Safety considerations, including proper clothing and footwear and a firm non-slip sports surface, are essential.
Compression forces present in plyometrics have the potential for injury. Spinal shrinkage has been measured at 1.75 mm after 25 repetitions of a drop jump from a height of 1.0 m so this type of exercise is not suitable for individuals with a history of low back pain of discal origin. In normal walking, deceleration forces have been measured at 3 g (three times earth’s normal gravity), while in a drop jump from a height of 0.4 m the deceleration has been measured at 23 g (Lees and Graham-Smith, 1996). This type of force acting on the lower limb makes plyometrics unsuitable for those with a history of arthritis in the joints of the lower limb or spine.
Keypoint
Plyometrics is an advanced, intense form of exercise, not suitable for the beginner. Safety considerations are essential throughout.
Three types of exercises are normally used: in-place, short response and long-response (Table 4.13). In-place activities include such things as standing jumps, drop jumps and hopping. Short-response actions are those such as the standing broad jump, the standing triple jump and box jumps. Long response movements include bounding, hopping and repeated hurdle jumps.
Table 4.13 Plyometric exercises
| Exercise type | Movement | Description |
|---|---|---|
| In-place | Standing jumps |
Jumping and landing on the same spot, to emphasize the vertical component of the jump |
| Drop jumps |
Use gravity and body weight to increase resistance and emphasize eccentric component of movement | |
| Hopping |
Straight, zig-zag, or rotatory hopping on the same spot | |
| Short response | Standing broad jump |
Emphasizes horizontal component of jump |
| Standing triple jump |
Combines several jumps and hops over a distance | |
| Box jumps |
Jump over an object to emphasize both vertical and horizontal component of jump | |
| Long response | Bounding |
Greater horizontal range than others. Single/double/alternate legs |
| Hopping |
Repeated combinations of straight/zig-zag/rotatory hopping | |
| Repeated hurdle jumps |
Horizontal and vertical jump component for endurance |
Although plyometric activity is primarily used for lower limb training, is does have an important place for the upper limb and trunk. Overhead throwing actions using a medicine ball, and throwing and catching from a bent-knee sit-up position are examples of this.
Resistance may be added to increase the overload on the working muscles as the plyometric activity is used. Vertical jumps may be performed using light dumb-bells, or a squat/leg press machine, and horizontal movements (lateral jumps, side hops) can be overloaded using an elastic cord.
Plyometrics has its use in late stage rehabilitation, and functional pre-competitive testing following injury. The adaptations produced by this type of activity within a previously injured muscle are likely to make it more capable of withstanding explosive effort, as encountered in sprinting and jumping activities, for example. This, in turn, may reduce the risk of re-injury. Using heavy resistance exercise in late stage rehabilitation of the injured athlete may allow the limb to regain lost strength, but without plyometric activity it is likely that the limb could still break down in the competitive situation, because the strength activity does not match the speed and power of the action to be used on the field of play.
Resistance training methods
Exercise progression
As with exercise in general, strength training requires a muscle to be ‘overloaded’ or worked at a resistance greater than that normally encountered. This may be achieved in a number of ways, the most common of which in the context of sports injuries is weight training.
To increase the overload placed on a muscle, and progress the exercise, a number of methods may be employed, as listed below:
Increasing the resistance, exercise duration and frequency will make the exercise harder, as will reducing the rest interval. Altering the effect of gravity, by inclining or declining a bench, will affect the point of maximal leverage. Changing the length of the lever arm will also alter the resistance, for example arm abduction performed in the standing position will be harder with a weight bag in the hand than with one fastened to the elbow.
The relationship between length–tension and force–velocity means that altering the starting length of a muscle or the speed of movement will change the overload. For example, when performing a sit-up exercise the hip flexors and abdominal flexors will work. By bending the hips, the work of the hip flexors will be reduced, increasing the overload of the abdominal flexors.
As the speed of movement increases, the force output from the muscle is reduced. In addition, more rapid actions have more momentum and are therefore harder to stop (a safety consideration) and are performed with ballistic muscle actions.
The type of muscle work (isometric or isotonic) and the function of the muscle (agonist/fixator, etc.) can be used to great effect, as can the range of movement. Initial rehabilitation exercises, where range of movement is limited, tend to be isometric in nature, progressing to isotonic and increasing the range of motion. The motor skill involved with group muscle action makes it vital that a muscle is not simply worked as a prime mover, but as a fixator and synergist as well.
The combination of repetitions (number of complete executions of an exercise) and sets (number of repetitions grouped together) in weight training is the subject of considerable debate. In general, low numbers of repetitions have been traditionally used to increase strength, while higher numbers have been favoured for endurance. Medium numbers of repetitions are usually referred to as ‘power’ training, although it is unlikely that this would be effective unless the speed of the movement were increased.
A number of combinations of sets and repetitions have been developed, one of the most widely used being that of DeLorme and Watkins (1948).
Weight training programmes
DeLorme and Watkins
This method requires the user to first discover the maximum weight which can be lifted for the 10 repetition maximum (10 RM). The programme then consists of three sets of 10 repetitions at percentages of this maximal value, as follows:
Strength gains were assessed using a 1 RM (single repetition maximum) each week, and gains in strength from 20 lb lifted before the programme to 60 lb lifted after 36 days were seen.
The DeLorme and Watkins programme enables the movement to be rehearsed before a maximal contraction is required, perhaps recognizing the importance of neurogenic factors in strength performance.
Practically there are a number of issues in determining 1 RM. Fatigue after each lift means than a rest period of 1–5 minutes has to be given after a single repetition before the test can be repeated to failure. Also, the relationship between the 1 RM and 10 RM changes with training: 7–10 RM has been shown to represent 68% of the 1 RM for untrained subjects but 79% of the 1 RM for trained subjects (McArdle, Katch and Katch, 2001).
Pyramid system
In this routine, the number of repetitions performed with each set is reduced as the weight increases, the subject working on a ‘light to heavy’ system. This results in the athlete performing a few repetitions to fatigue when the muscle is thoroughly warm. An example is given below:
Oxford technique (reverse pyramid)
This is the reverse of the pyramid system. Now the user adopts a ‘heavy to light’ system, starting by performing 10 repetitions at their 10 RM and reducing to 75% and 50% of this value:
The Oxford technique (Zinovieff, 1951) works on the principle that as the muscle fatigues, the weight should be reduced to take account of the reduction in force output.
DAPRE technique
Knight (1979) recommended that the resistance to be lifted should be based on previous performance. The technique of daily adjusted progressive resistance exercise (DAPRE) determines when, and by how much, to increase the weight, and allows for individual differences in the rate of strength development, as shown below:
Four sets are performed as indicated in Table 4.14, the first two sets being 10 and then six repetitions with one half and then three-quarters of the ‘working weight’. This is roughly a 6 RM, and is determined from previous performance. In the third set, the weight is adjusted depending on the number of repetitions which could be performed. For example, if in the third set the athlete is able to lift the weight only five times, the weight used in the fourth set will be the same. If he or she were able to perform 10 repetitions in the third set, the weight is increased by 2.5 to 5 kg. The number of repetitions performed during the fourth set with this adjusted weight determine the new working weight to be used in the next training session.
Table 4.14 Guidelines for adjusting weight in the DAPRE technique
| Number of repetitions performed in third set | Adjusted working weight (fourth set) | Next session |
|---|---|---|
| –2 | Deduct 2.5–5 kg | Deduct 2.5–5 kg |
| 3–4 | Deduct 0–2.5 kg | Same weight |
| 5–6 | Same weight | Add 2.5–5 kg |
| 7–10 | Add 2.5–5 kg | Add 2.5–7.5 kg |
| 10–11 | Add 5–7.5 kg | Add 5–10 kg |
High intensity strength training
For a muscle to work maximally, during the final set an athlete should not stop training simply because a certain number of repetitions have been performed, but only when no more can be performed. In this way volitional fatigue rather than number of repetitions determines the extent of the set.
If maximal work can be performed in a single set, multiple sets may not be necessary. Hurley et al. (1984) showed strength increases of 33% for lower body and 50% for upper body, when using a single set of 8–12 repetitions performed to volitional fatigue. Silvester et al. (1982) found that one set of arm curls performed to volitional fatigue was as effective at increasing biceps strength as three sets at maximal weights.
Messier and Dill (1985) also showed a single set performed to volitional fatigue produced greater mean values of amount of weight lifted than three sets at sub-maximal weight. The duration of training in this study was 20 minutes, compared to 50 minutes required for a multiple set programme. Single set programmes have been compared to two set and four set programmes and found to be equally effective when compared for improvement of muscle size, strength and upper body power over a 10-week period (Ostrowski et al., 1997).
Hass et al. (2000) found a single set programme to be as effective as a three set programme (8–12 reps to volitional fatigue) over a 13-week programme. Importantly, they also reported that the single set programme took less time to perform (25 min) than the three set programme (60 min), improving compliance. They encountered a 25% dropout rate for the three set programme. High intensity strength training, although effective, may not be appropriate for early rehabilitation when pain will limit the intensity of training which an athlete is capable of. In addition, single set programmes are probably better suited to beginners, or as a brief intense period of strength training within a more broadly based programme. Single set programmes do not offer the same training volume as multiple set programmes and have been shown to be less effective for long term training, especially when multiple set programmes are used with periodization (Bryant: Kraemer, Stone and O’, 1997).
Circuit training
Circuit training consists of a series of exercises performed in a continuous sequence, and a number of formats are available. Three variables are important in the construction of a circuit (Lawrence and Hope, 2002), timing (controlling movement from one station to another), layout (shape of circuit) and exercise choice (free exercise, resistance, functional).
Timing is used to control movement of subjects from one exercise station to another. A specific time may be performed at each station and this may vary between exercises, for example longer periods on a static cycle and shorter on resistance machines. Alternatively, the instructor may dictate the pace using a stopwatch, and vary this, depending on feedback from participants. Lighting systems (traffic light) and music may also be used to dictate time. The number of repetitions may also be used to set the time, dictated either by the instructor or by the user (Table 4.15).
Table 4.15 Timing in circuit training
| Method of controlling timing | Description |
|---|---|
| Stopwatch | Time dictated by instructor and may vary depending on feedback from participants |
| Exercise station specific | Time set specific to exercise station type |
| Music | Change station as music changes |
| Lighting system | Use traffic light system built into gym |
| Repetitions (user) | User decides number of reps and records this |
| Repetition (instructor) | Instructor determines number of reps |
Source Lawrence, D. and Hope, B. (2002) Complete Guide to Circuit Training. A C Black, London. With permission.
Circuit layout will be dictated by both safety and effectiveness. Typical examples include the line, corners, stations and half split (Fig. 4.13). A variety of free exercises or apparatus may be chosen, incorporating different fitness components. Exercises for strength (push-ups, chins) may be interspersed with flexibility (straight leg raise), stamina (jogging), speed (throwing a medicine ball) and skill (flamingo balance). Specificity of training may be enhanced by mimicking the actions involved in a particular sport. For example, a circuit may be set up on a football pitch involving short sprints, zig-zag running, dribbling skills and shooting skills, in addition to upper body and trunk work. An example of a typical circuit is given in Fig. 4.14.
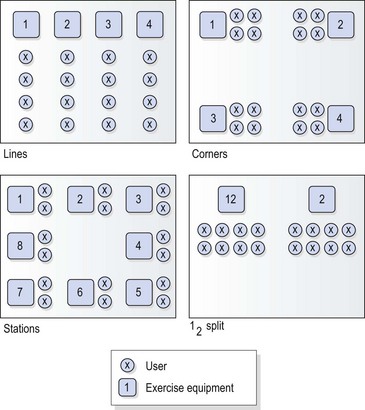
Figure 4.13 Examples of circuit layout.
Adapted from Lawrence, D. and Hope, B. (2002) Complete Guide to Circuit Training. With permission from A&C Black Publishers, an imprint of Bloomsbury Publishers Ltd.
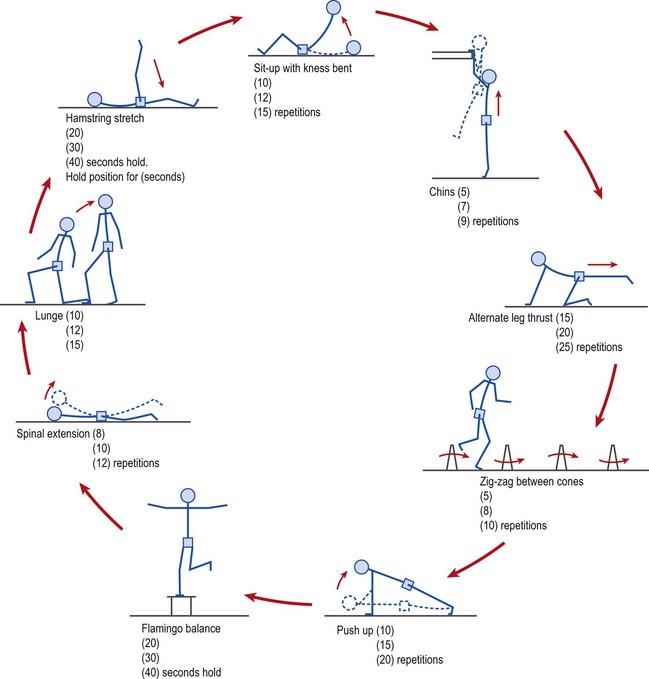
Figure 4.14 Circuit training. Example of general circuit, with values for beginners (top), intermediate (middle) and advanced (bottom) athletes.
Circuit weight training (CWT)
Circuits may be designed using only one specific type of exercise. An example of this more specialized circuit is circuit weight training or circuit resistance training (CWT/CRT) using only resistance training apparatus. Less emphasis is placed on heavy overload or a single muscle group, and instead a more general fitness programme is obtained. CWT involves alternating the body part worked (arms/legs/trunk) to prevent fatigue of one muscle group. Various types of work–rest ratio may be used. Typical combinations would be eight or more exercises, with a weight of 40–55% 1 RM. A maximum number of repetitions may be performed for 30 seconds, with a rest of 15 seconds, to gain a more general body conditioning programme.
Increase in cardiopulmonary (CP) fitness has been shown with CWT, but it is dependent on rest period, exercise intensity, exercise type and total work. Allen, Byrd and Smith (1976) failed to show significant changes in VO2 max using 30-second work and 60-second rest periods, the long rest period allowing too much recovery. A programme using a shorter rest period (15 seconds) showed an increase of 11% VO2 max in women but no significant change in men (Wilmore, Parr and Girandola, 1978). Here, the rest period was short enough, but the exercise intensity for the men was not adequate. The women worked at 87.6% of their VO2 max, but the men at only 78.2% of theirs. Longer training programmes have been shown to produce better results in terms of VO2 max improvement (Pollock, Cureton and Greniger, 1969), and Gettman, Ayres and Pollock, (1978) showed a 3.5% increase in VO2 max after a 20-week CWT programme. Subjects performed at 50% of their maximum strength in a 30-minute programme, which progressed from 10 to 20 repetitions with a rest period which was reduced from 30 to 20 seconds.
Slow speed (60°/s) isokinetic CWT has been shown to be better than high speed (120°/s) training at increasing cardiopulmonary fitness (Gettman and Ayres, 1978). This reflects the importance of the total work performed during the circuit. Athletes using slow speed training worked for a longer period than those using the high speed programme.
Improvements in VO2 max are not as great with CWT as with running. Average values after a 20-week programme being 3.5% for CWT compared with 35% for running (Gettman and Pollock, 1981). However, the real value of CWT is to maintain cardiopulmonary fitness when an athlete is unable to run or perform other cardiopulmonary fitness activities due to lower limb injury. In a study comparing CWT with running, Gettman, Ayres and Pollock (1979) examined subjects who worked for 8-week periods, first at CWT, then on a running programme, and finally on either running or CWT. Improvements in VO2 max obtained by running were preserved with CWT, and both groups maintained cardiopulmonary fitness to the same levels. Increases in lean body mass, reductions in body fat and strength improvements have all been shown with CWT (Gettman and Pollock, 1981).
One criticism of many of the studies into the cardiopulmonary effects of CWT is that the testing usually uses only treadmill assessment, whereas CWT uses upper body work as well (McArdle, Katch and Katch, 2001). One study which assessed CWT on both a treadmill and an arm crank dynamometer gave improvement in aerobic capacity after CWT of 7.8% with treadmill testing and 21.1% with arm crank dynamometry (Harris and Holly, 1987), illustrating the greater all-body conditioning (cross training) benefits of CWT.
Kinetic chain exercise
Movement of the limbs occurs as a kinetic chain. Several joints arranged in sequence move together to produce a complex motor action. If the terminal joint in the kinetic chain can move freely, the chain is open. If this same joint is unable to move independently because it faces a significant resistance, the action constitutes a closed kinetic chain.
Definition
In a closed chain action, both the proximal and distal ends of the chain of movement are fixed, and motion occurs between the two. In an open chain action the proximal segment is fixed but the distal segment moves freely.
Most functional activities involving the lower limb in sport are performed using a closed kinetic chain. Walking, running, jumping and rising from a sitting position are all examples of closed kinetic chain activities. One of the only open kinetic chain activities of the lower limb normally used in sport is kicking.
We have seen the importance of exercise specificity in terms of muscle work and energy system, but the exercise must also be specific to the type of kinetic chain action used. To exercise the quadriceps on a leg extension bench (open chain) does not accurately reflect the demands placed on the lower limb with running and jumping (closed chain). As many of the adaptations produced during resistance training, particularly in the first 4 weeks of training, are neurogenic in nature, the mismatch in movement patterns could detrimentally affect the athlete’s performance (Palmitier et al., 1991).
A common open chain movement used in knee training is the seated leg extension exercise. The muscles primarily responsible for this action are the quadriceps. Contrast this to the closed chain movement of the squat. When the leg extends to raise the body from the squatting position, the hamstrings extend the hip and assist in knee extension as the foot is stabilized. This co-contraction (co-activation) greatly reduces the anterior shear forces acting on the knee, and is of particular importance in the rehabilitation of anterior cruciate ligament (ACL) repairs.
Several additional differences exist between open (single joint or ‘isolation’) and closed chain (multi-joint or ‘general’) exercises in resistance training. In an open chain action, movement occurs mainly distal to the joint axis, whereas, with a closed chain action, motion is both proximal and distal to the joint. An open chain action primarily emphasizes concentric work, but a closed chain movement brings a more balanced action of concentric, eccentric and isometric contractions into play.
Implications for rehabilitation
The evidence on mixtures of sets, repetitions and types of muscle work indicates that no single combination yields optimal gains for everyone. In early rehabilitation, where range of motion is severely limited, isometric exercise is useful. Performing this type of exercise in inner range will contribute to joint stability, and it is important that this be obtained before resisted movement is begun.
Because isometric gains are joint angle specific, resistance training should progress rapidly to involve all types of muscle work. At the beginning of a weight-training programme we have seen that neurogenic changes predominate. Practising the skilled movement involved in the exercise is therefore important at this stage, so multiset regimes are likely to be more successful. As rehabilitation progresses, all the fitness components must be worked. Power and speed are important and should be combined with rapid eccentric contractions in plyometric routines. Cardiopulmonary fitness may be maintained using circuit weight training, where lower limb injury prevents activities such as running, cycling or swimming.
For pure strength gains, high intensity programmes are more suitable for well-motivated individuals. Those who are poorly motivated may not be able to perform maximally in one set and so would be better to stay on more traditional multiset programmes.
For a weight training exercise to be maximal throughout the range of motion, the resistance offered to the muscle must change. Some form of accommodating resistance provided by an asymmetric cam or electronic braking system may be useful. Alternatively, free weights using bodybuilding techniques such as ‘forced repetitions’ and ‘cheating repetitions’ can be used. Here, a training partner or body swing, respectively, is used to take the weight through the point of maximal leverage traditionally called the ‘sticking point’.
Specificity of training makes it of paramount importance that exercise mimics as closely as possible the function which will be required of the athlete. At this stage, sports specific skills should be practised in preference to pure strength work.
Muscle pain
Muscle pain occurs under normal circumstances with exercise, and does not necessarily indicate injury. Two types of pain are generally recognized. First, pain which occurs during exercise but disappears when the activity stops (ischaemic pain). Secondly, with unaccustomed exercise, discomfort may not occur immediately afterwards, but pain comes on a number of days later (delayed onset muscle soreness).
Keypoint
Ischaemic muscle pain occurs during exercise but disappears when activity stops. Delayed onset muscle soreness (DOMS) does not occur immediately, but comes on a number of days later.
Ischaemic muscle pain
Pain of this type begins in the working muscle and increases in intensity as exercise continues. It disappears when exercise stops and generally leaves no after-effects. The rise in intramuscular pressure during exercise can compress the blood vessels running through a muscle, producing ischaemic pain.
The accumulation of metabolites is generally accepted to be the cause of the pain. Lactic acid is often cited as the culprit, but patients who are unable to produce lactic acid (McArdle’s syndrome) still suffer ischaemic pain. Histamine, acetylcholine, serotonin (5-HT), potassium and bradykinin are the most likely agents to cause the pain of ischaemia (Newham, 1991).
Delayed onset muscle soreness
Delayed onset muscle soreness (DOMS) is residual muscle pain which occurs 24–48 hours following unaccustomed bouts of intense exercise. Eccentric muscle work and exercise with a long muscle length have been shown to increase the intensity of the delayed onset soreness (Clarkson and Byrnes, 1986; Jones, Newham and Torgan, 1989). A number of possibilities exist for the cause of this pain, and it is probable that it is the result of a combination of factors, the contribution of each being related to activity type and individual differences (Table 4.16).
Table 4.16 Factors associated with delayed onset muscle soreness (DOMS)
Mechanical trauma can develop as a result of the high tensions developed during eccentric contractions (Newman et al., 1983). More trauma is likely with eccentric work than with other muscle actions because the tensions created during eccentric contraction are usually greater. In a study of downhill running, increases in creatine kinase and myoglobin were seen, suggesting that structural damage was occurring within the muscle (Byrnes and Clarkson, 1985).
Disruption seems to be to the connective tissue elements, rather than the contractile tissue within the active muscles. Hydroxyproline, a product of connective tissue breakdown has been detected in the urine of subjects suffering from DOMS (McArdle, Katch and Katch, 1986), suggesting connective tissue damage. The cytoskeleton of the muscle, when damaged, becomes more permeable, allowing excess leakage of muscle enzymes and an increased uptake of injected radioisotopes (Newham, 1991). Further, changes in the sarcoplasmic reticulum of the muscle cell have been shown to depress calcium muscle metabolism, altering muscle contraction and causing pain (McBride, 1998).
Unaccustomed exercise can also produce a build-up of metabolites within the working muscle. This in turn will give rise to osmotic changes in the cellular environment of the muscle, resulting in fluid retention and subsequent pressure on sensory nerves. Similarly, ischaemia of the working muscle can occur, leading to an accumulation of pain (p) substance, bringing on reflex muscle spasm (DeVries, 1961; Abraham, 1977).
A number of methods have been suggested to relieve DOMS. Stretching has been shown to reduce pain in the anterior tibial muscles (DeVries, 1961), and would certainly seem to be able to reduce muscle spasm. Increasing the blood flow to the muscle during the warm-down period is also helpful. This can be achieved by gentle exercise, hot showers or massage. In each case, a possible mechanism of relief is that of flushing fresh blood through the muscle to remove metabolic wastes, and pumping the lymphatic vessels to remove local oedema and reduce interstitial pressure.
Muscle fatigue
Muscle fatigue can present as a loss of force or power output, slowing of relaxation, changes in contractile characteristics and alterations in electrical properties. Two basic mechanisms of fatigue have been described, central and peripheral. Central fatigue refers to changes occurring proximal to the motor neurone, and involves neural and psychological changes such as motivation and recruitment. Peripheral fatigue involves the motor unit itself, and occurs chiefly through exhaustion of the muscle energy supplies. The type and intensity of activity being performed will decide whether central and peripheral fatigue occur separately or in combination.
If a subject is told to push as hard as possible for as long as possible, without feedback, force output will fall due to fatigue. If central fatigue occurs, more force can only be generated when the muscle is stimulated electrically.
Traditionally, fatigue types have been studied by comparing forces generated by maximum stimulated contraction (MStC), with those of maximal voluntary contractions (MVC). In unfatigued muscle, the MVC is the same as the MStC. With central fatigue, the force produced during MVC is less than that from an MStC, while in peripheral fatigue there is no difference between force of MVC and MStC (Bigland-Ritchie, 1981).
Peripheral fatigue can be further categorized into high and low frequency types. The natural firing frequencies of normal voluntary contractions are approximately 5–30 Hz. High frequency fatigue occurs when a muscle is stimulated at high frequencies between 50 and 100 Hz, while low frequency fatigue is the loss of force at low stimulation frequencies between 10 and 40 Hz.
Abraham W.M. Factors in delayed onset muscle soreness. Medicine and Science in Sports. 1977;9(1):11-20.
Adams J.A. The second facet of forgetting: a review of warm-up decrement. Psychological Bulletin. 1961;58:257-273.
Allen T.E., Byrd R.J., Smith D.P. Hemodynamic consequences of circuit weight training. Research Quarterly. 1976;47:299-306.
Alter M.J. Science of Flexibility, second ed. Champaign, Illinois, USA: Human Kinetics; 1996.
American College of Sports Medicine (ACSM). The recommended quantity and quality of exercise for developing and maintaining fitness in healthy adults. Medicine and Science in Sports and Exercise. 1978;10:VII-X.
American College of Sports Medicine (ACSM). The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness in healthy adults. Medicine and Science in Sports and Exercise. 1990;22:265-274.
American College of Sports Medicine. Progression models in resistance training for healthy adults. Medicine and Science in Sports and Exercise. 2002;34:364-380.
Andzel W.D. One mile run performance as a function of prior exercise. Journal of Sports Medicine. 1982;22:80-84.
Andzel W.D., Gutin B. Prior exercise and endurance performance: a test of the mobilisation hypothesis. Research Quarterly. 1976;47(3):269-276.
Anshel M.H. A psycho-behavioral analysis of addicted versus non-addicted male and female exercisers. Journal of Sport Behaviour. 1991;14(2):145-154.
Ashton D., Davies B. Why Exercise?. London: Basil Blackwell; 1986.
Astrand P-O., Rodahl K. Textbook of Work Physiology. Maidenhead: McGraw-Hill; 1986.
Bandy W.D., Irion J.M. The effect of time on static stretch of the flexibility of the hamstring muscles. Physical Therapy. 1994;74(9):845-852.
Bandy W.D., Lovelace-Chandler V., McKitrick-Bandy B. Adaptation of skeletal muscle to resistance training. Journal of Orthopaedic and Sports Physical Therapy. 1990;12(6):248-255.
Barnard R.J., Gardner G.W., Diaco N.V., MacAlpin R.N., Kattus A.A. Cardiovascular responses to sudden strenuous exercise: heart rate, blood pressure, and ECG. Journal of Applied Physiology. 1973;34:883.
Bartlett M.J., Warren P.J. Effect of warming up on knee proprioception before sporting activity. British Journal of Sports Medicine. 2002;36:132-134.
Behm D.G., Button D.C., Butt J.C. Factors affecting force loss with prolonged stretching. Canadian Journal of Applied Physiology. 2001;26:261-272.
Bergh U. Human power at subnormal body temperatures. Acta Physiologica Scandinavica. 1980;478(Suppl.):1-39.
Bergh U., Ekblom B. Physical performance and peak aerobic power at different body temperatures. Journal of Applied Physiology. 1979;46:885-889.
Bergh U., Ekblom B. Influence of muscle temperature on maximal muscle strength and power output in human skeletal muscles. Acta Physiologica Scandinavica. 1979;107:33-37.
Bigland-Ritchie B. EMG and fatigue of human voluntary and stimulated contractions. In: Porter R., Whelan J., editors. Human Muscle Fatigue: Physiological Mechanisms. Pitman Medical, London: Ciba Foundation Symposium, 1981. 82
Bonner H.W. Preliminary exercise: a two-factor theory. Research Quarterly. 1974;45:138-147.
Borms J. Importance of flexibility in overall physical fitness. International Journal of Physical Education. 1984;11:2.
Bosco C., Komi P.V. Potentiation of the mechanical behaviour of the human skeletal muscle through pre-stretching. Acta Physiologica Scandinavica. 1979;106:467.
Bouchard C., Rankinen T. Individual differences in response to regular physical activity. Medicine and Science in Sports and Exercise. 2001;33(6 Suppl):S446-51.
Bray J.J., Cragg P.A., Macknight A.D.C., Mills R.G., Taylor D.W. Lecture Notes on Human Physiology. Oxford: Blackwell Scientific; 1986.
Brown B.S., Payne T., Kim C., Moore G., Krebs P., Martin W. Chronic response of rat brain norepinephrine and serotonin levels to endurance training. Journal of Applied Physiology. 1979;46:19-23.
Brown R.D., Harrison J.M. The effects of a strength training program on the strength and self-concept of two female age groups. Research Quarterly for Exercise and Sport. 1986;57(4):315-320.
Byrnes W.C., Clarkson M.C. Delayed onset muscle soreness following repeated bouts of downhill running. Journal of Applied Physiology. 1985;59:283.
Carlile F. Effect of preliminary passive warming on swimming performance. Research Quarterly. 1956;27(2):143-151.
Clarkson P.M., Byrnes K.M. Muscle soreness and serum creatine kinase activity following isometric, eccentric, and concentric exercise. International Journal of Sports Medicine. 1986;7:152-155.
Cornelius W.L., Hinson M.M. The relationship between isometric contraction of hip extensors and subsequent flexibility in males. Journal of Sports Medicine and Physical Fitness. 1980;20:75-80.
Costill D.L., Fink W.J., Getchell L.H., Ivy J.L., Witzmann F.A. Lipid metabolism in muscle of endurance trained males and females. Journal of Applied Physiology: Respiratory, Environmental and Exercise Physiology. 1979;47:787.
Crossman J., Jamieson J., Henderson L. Responses of competitive athletes to lay-offs in training: exercise addiction or psychological relief? Journal of Sport Behaviour. 1987;10(1):28-38.
Darden E. Positive and negative work. Scholastic Coach. 1975;45:6-12. and 85–86
Davies C.T.M., Young K. Effect of temperature on contractile properties and muscle power of triceps surae in humans. Journal of Applied Physiology. 1983;55:191-195.
DeLorme T., Watkins A. Techniques of progressive resistance exercise. Archives of Physical Medicine and Rehabilitation. 1948;29:263-273.
DeVries H.A. Effects of various warm-up procedures on 100 yard times of competitive swimmers. Research Quarterly. 1959;30:11-20.
DeVries H.A. Prevention of muscular distress after exercise. Research Quarterly. 1961;32:177.
DeVries H.A. Physiology of Exercise for Physical Education and Athletics. Dubuque: Willium C. Brown; 1980.
Dishman R.K., Gettman L.R. Psychological vigour and self-perceptions of increased strength. Medicine and Science in Sports and Exercise. 1981;13:73-74.
Ekstrand J., Gillquist J., Moller M., et al. Incidence of soccer injuries and their relation to training and team success. American Journal of Sports Medicine. 1983;11(March–April):63-67.
Enoka R.M. Neuromechanical Basis of Kinesiology, second ed. Champaign, Illinois: Human Kinetics; 1994.
Etnyre B.R., Abraham L.D. H-reflex changes during static stretching and two variations of proprioceptive neuromuscular facilitation techniques. Electroencephalography and Clinical Neurophysiology. 1986;63:174-179.
Etnyre B.R., Lee E.J. Comments on proprioceptive neuromuscular facilitation stretching. Research Quarterly for Exercise and Sport. 1987;58(2):184-188.
Farrell P.A., Gates W.K., Morgan W.P., Pert C.B. Plasma leucine enkephalin-like radioreceptor activity and tension-anxiety before and after competitive running. In: Knuttgen H.G., Vogel J.A., Poortmans J., editors. Biochemistry of Exercise. Champaign, Illinois: Human Kinetics, 1983.
Fiatarone M.A. Exercise training and nutritional supplementation for physical frailty in very elderly people. New England Journal of Medicine. 1994;330:1769.
Fowles J.R., Sale D.G., Macdougall J.D. Reduced strength after passive stretch of the human plantarflexors. Journal of Applied Physiology. 2000;89:1179-1188.
Fradkin A.J., Gabbe B.J., Cameron P.A. Does warming up prevent injury in sport? The evidence from randomized controlled trials. Journal of Science and Medicine in Sport. 2006;9:214-220.
Gettman L.R., Ayres J.J. Aerobic changes through 10 weeks of slow and fast speed isokinetic training (abstract). Medicine and Science in Sports and Exercise. 1978;10:47.
Gettman L.R., Pollock M.L. Circuit weight training: a critical review of its physiological benefits. Physician and Sports Medicine. 1981;9(1):44-60.
Gettman L.R., Ayres J.J., Pollock M.L. The effect of circuit weight training on strength, cardio-respiratory function, and body composition of adult men. Medicine and Science in Sports and Exercise. 1978;10:171-176.
Gettman L.R., Ayres J.J., Pollock M.L. Physiological effects on adult men of circuit strength training and jogging. Archives of Physical Medicine and Rehabilitation. 1979;60:115-120.
Glasser W. Positive Addiction. New York: Harper and Row; 1976.
Goldberg B., Saranitia A., Witman P. Preparticipation sports assessment: an objective evaluation. Pediatrics. 1980;66:736-745.
Gonyea W.J., Sale D.G., Gonyea F.B., Mikesky A. Exercise induced increases in muscle fiber number. European Journal of Applied Physiology and Occupational Physiology. 1986;55:137-141.
Greist J.H., Klein M.H., Eischens R.R., Faris J., Gurman A.S., Morgan W.P. Running as treatment for depression. Comprehensive Psychiatry. 1979;20:41-53.
Gutin, B., Stewart, K., 1971. Prior exercise and endurance. Physiology meeting. Springfield, Mass. Cited in Gutin et al. (1976).
Gutin B., Stewart K., Lewis S., Kruper J. Oxygen consumption in the first stages of strenuous work as a function of prior exercise. Journal of Sports Medicine. 1976;9:60-65.
Harris K.A., Holly R.G. Physiological response to circuit weight training in borderline hypertensive subjects. Medicine and Science in Sports and Exercise. 1987;19:246.
Harris M.L. Flexibility: a review of the literature. Physical Therapy. 1969;49(6):591-601.
Hartig D.E., Henderson J.M. Increasing hamstring flexibility decreases lower extremity overuse injuries in military basic trainees. American Journal of Sports Medicine. 1999;27:173-176.
Hass C.J., Garzarella L., Hoyos D., Pollock M.L. Single versus multiple sets in long-term recreational weightlifters. Medicine and Science in Sports and Exercise. 2000;32(1):235-242.
Herbert R.D., Gabriel M. Effects of stretching before and after exercising on muscle soreness and risk of injury: systematic review. British Medical Journal. 2002;325:468-470.
Holland G.L. The physiology of flexibility: a review of the literature. Kinesiology Review 1968;49-62.
Holt L.E., Smith R. The Effect of Selected Stretching Programs on Active and Passive Flexibility. Del Mar, CA, USA: Research Center for Sport; 1983.
Holt L.E., Travis T.T., Okita T. Comparative study of three stretching techniques. Perceptual and Motor Skills. 1970;31:611-616.
Hopper D. A survey of netball injuries and conditions related to these injuries. Australian Journal of Physiotherapy. 1986;32(4):231-239.
Hurley B.F., Hagberg J.M., Allen W.K., Seals D.R., Young J.C., Cuddihee R.T., Holloszy J.O. Effect of training on blood lactate levels during submaximal exercise. Journal of Applied Physiology: Respiratory Environment, and Exercise Physiology. 1984;56:1260.
Janda, V., 1992. Muscle and Back Pain: Assessment and Treatment of Impaired Movement Patterns and Motor Recruitment, associated course to the 5th International Symposium of the Physical Medicine Research Foundation, Oxford.
Jaric S., Gavrilovic P., Ivancevic V. Effects of previous muscle contractions on cyclic movement dynamics. European Journal of Applied Physiology. 1985;54:216-221.
Johnson B.L., Adamezyk J.W., Tenmore K.O., Stromme S.B. A comparison of concentric and eccentric muscle training. Medicine and Science in Sports and Exercise. 1976;8:35-38.
Jones D.A., Newham D.J., Torgan C. Mechanical influences on long standing human muscle fatigue and delayed onset muscle pain. Journal of Physiology. 1989;224:173-186.
Jones R.J., Wright V. Relative importance of various tissues in joint stiffness. Journal of Applied Physiology. 1982;17(5):824-828.
Kent M. Oxford Dictionary of Sports Science and Medicine. Oxford: Oxford University Press; 1994.
Knight K.L. Knee rehabilitation by the daily adjustable progressive resistance exercise technique. American Journal of Sports Medicine. 1979;7:336.
Kokkonen J., Nelson A.G., Cornwall A. Acute muscle stretching inhibits maximal strength performance. Research Quarterly for Exercise and Sport. 1998;69:411-415.
Kraemer W.J., Stone M., O’Bryant H. Effects of single vs. multiple sets of weight training; impact of volume, intensity and variation. Journal of Strength and Conditioning Research. 1997;11:143-147.
LaBan M.M. Collagen tissue: implications of its response to stress in vitro. Archives of Physical Medicine and Rehabilitation. 1962;43:461-466.
Lashville A.V. Active and passive flexibility in athletes specialising in different sports. Soviet Sports Review. 1983;18(1):30-32.
Lawrence D., Hope B. Complete Guide to Circuit Training. London: A&C Black; 2002.
Lees A., Graham-Smith P. Plyometric training: a review of principles and practice. Sport Exercise and Injury. 1996;2:24-30.
Levine M.G., Kabat H. Co-contraction and reciprocal innervation in voluntary movement in man. Science. 1952;116:115-118.
Lewit K. Manipulative Therapy in Rehabilitation of the Locomotor System, second ed. Oxford: Butterworth-Heinemann; 1991.
MacDougall J.D., Ward G.R., Sale D.G., Sutton J.R. Biochemical adaptation of human skeletal muscle in heavy resistance training and immobilization. Journal of Applied Physiology. 1977;43:700-703.
Magnusson S.P., Simonsen E.B., Kjaer M. Biomechanical responses to repeated stretches in human hamstring muscle in vitro. American Journal of Sports Medicine. 1996;24(5):622-628.
Mandell A.J. The second wind. Psychiatric Annals. 1979;9:57-69.
McArdle W.D., Katch F.I., Katch V.L. Exercise Physiology: Energy, Nutrition, and Human Performance, third ed. Philadelphia: Lea and Febiger; 1986.
McArdle W.D., Katch F.I., Katch V.L. Exercise Physiology, fourth ed. Philadelphia: Lippincott, Williams and Wilkins; 1991.
McArdle W.D., Katch F.I., Katch V.L. Exercise Physiology, Energy, Nutrition, and Human Performance, fifth ed. Philadelphia: Lea and Febiger; 2001.
McArdle W.D., Katch F.I., Katch V.L. Exercise Physiology, fifth ed. Philadelphia: Lippincott, Williams and Wilkins; 2002.
McBride J.M. Effects of resistance exercise on free radical production. Medicine and Science in Sports and Exercise. 1998;30:67.
McCafferty W.B., Horvath S.M. Specificity of exercise and specificity of training: a subcellular review. Research Quarterly. 1977;48:358-371.
McNair P.J., Stanley S.N. Effect of passive stretching and jogging on the series elastic muscle stiffness and range of motion of the ankle joint. British Journal of Sports Medicine. 1996;30:313-318.
Messier S.P., Dill M.E. Alteration in strength and maximal oxygen uptake consequent to Nautilus circuit weight training. Research Quarterly. 1985;56(4):345-351.
Moore M.A., Kukulka C.G. Depression of Hoffman reflexes following voluntary contraction and implications for proprioceptive neuromuscular facilitation therapy. Physical Therapy. 1991;71:321-333.
Morgan W.P. Affective beneficence of vigorous physical activity. Medicine and Science in Sports and Exercise. 1985;17(1):94-100.
Nacson J., Schmidt R.A. The activity-set hypothesis for warmup decrement. Journal of Motor Behavior. 1971;3:1-15.
Newham D.J. Skeletal muscle pain and exercise. Physiotherapy. 1991;77(1):66-70.
Newman D.J., Mills K.R., Quigley B.M., Edwards R.H.T. Pain and fatigue after concentric and eccentric muscle contractions. Clinical Science. 1983;64:55-62.
Nieman D., Pedersen B. Exercise and immune function. Sports Medicine. 1999;27(2):73-80.
Norris C.M. Stretching Physiotools compatable CD ROM programme. Helsinki, Finland: Physiotools, 1996.
Norris C.M. Bodytoning. London: A&C Black; 2002.
Norris C.M. The complete guide to stretching, third ed. London: A&C Black; 2007.
Olsen O.E., Myklebust G., Engebretsen L. Exercises to prevent lower limb injuries in your sports: cluster randomized controlled trial. BMJ. 2005;330:449-452.
Ostrowski K.J., Wilson G., Weatherby P., Lyttle A. The effect of weight training volume on hormonal output and muscular size and function. Journal of Strength and Conditioning Research. 1997;11:148-154.
Palmitier R.A., An K., Scott S.G., Chao E.Y.S. Kinetic chain exercise in knee rehabilitation. Sports Medicine. 1991;11(6):402-413.
Pert C.B., Bowie D.L. Behavioral manipulation of rats causes alterations in opiate receptor occupancy. In: Usdin E., Bunney W.E., Kline N.S., editors. Endorphins in Mental Health. Oxford: Oxford University Press, 1979.
Pollock M.L., Cureton T.K., Greniger L. Effects of frequency of training on working capacity, cardiovascular function and body composition of adult men. Medicine and Science in Sports. 1969;1:70-74.
Potteiger J.A. Muscle power and fiber characteristics following 8 weeks of plyometric training. Journal of Strength and Conditioning Research. 1999;13(3):275-279.
Prud’homme D., Bouchard C., Leblanc C., Landry F., Fontaine E. Sensitivity of maximal aerobic power to training is genotype-dependent. Medicine and Science in Sports and Exercise. 1984;16(5):489-493.
Ranatunga K.W., Sharpe B., Turnbull B. Contractions of a human skeletal muscle at different temperatures. Journal of Physiology. 1987;390:383-395.
Renstrom P., Kannus P. Prevention of injuries in endurance athletes. In: Shephard R.J., Astrand P.O., editors. Endurance in Sport. Oxford: IOC Medical Commission Publication, Blackwell Scientific; 1992:325-350.
Richards D.K. A two factor theory of the warm-up in jumping performance. Research Quarterly. 1968;39:668-673.
Rigby B. The effect of mechanical extension under the thermal stability of collagen. Biochimica et Biophysica Acta. 1964;79:634-636.
Roman W.J. Adaptations in the elbow flexors of elderly males after heavy resistance training. Journal of Applied Physiology. 1993;74:750.
Rosenbaum D., Henning E.M. The influence of stretching and warm up exercises on Achilles tendon reflex activity. Journal of Sports Science. 1995;15:481-484.
Rutherford O.M. Muscular coordination and strength training: implications for injury rehabilitation. Sports Medicine. 1988;5:196-202.
Safran M.R., Garrett W.E., Seaber A.V., Glisson R.R., Ribbecsk B.M. The role of warmup in muscular injury prevention. American Journal of Sports Medicine. 1988;16(2):123-129.
Sale D.G. Neural adaptation to resistance training. Medicine and Science in Sports and Exercise. 1988;20(5):135-145.
Sale D.G. Neural adaptation to strength training. In: Komi P.V., editor. Strength and Power in Sport. Oxford: IOC Medical Publication, Blackwell Scientific, 1992.
Sapega A.A., Quedenfel T.C., Moyer R.A., Butler R.A. Biophysical factors in range of motion exercise. Physician and Sports Medicine. 1981;9(12):57-65.
Sargeant A.J. Effect of muscle temperature on leg extension force and short term power output in humans. European Journal of Applied Physiology. 1987;56:693-698.
Sargeant A.J., Dolan P. Effect of prior exercise on maximal short term power output in humans. Journal of Applied Physiology. 1987;63:1475-1480.
Schmidt R.A. Motor Control and Learning. Champaign, Illinois: Human Kinetics; 1982.
Seward H.G., Patrick J. A three year survey of Victorian football league injuries. Australian Journal of Medicine and Science in Sport. 1992;24(2):51-54.
Seyle H. The Stress of Life. New York: McGraw-Hill; 1956.
Shellock F.G., Prentice W.E. Warming up and stretching for improved physical performance and prevention of sports related injuries. Sports Medicine. 1985;2:267-278.
Silvester L.J., Stiggins C., McGown C., Bryce G. The effect of variable resistance and free-weight training programs on strength. National Strength and Conditioning Association Journal. 1982;3:30-33.
Sipala S., Suominen H. Effects of strength and endurance training on thigh and leg muscle mass and composition in elderly women. Journal of Applied Physiology. 1995;78:334.
Smith L.L., Brunetz M.H., Chenier T.C. The effects of static and ballistic stretching on delayed muscle soreness and creatine kinase. Research Quarterly for Exercise and Sport. 1993;64:1438-1446.
Taylor D.C., Dalton J., Seaber A.V., Garrett W.E. The viscoelastic properties of muscle-tendon units. American Journal of Sports Medicine. 1990;18:300-309.
Thorstensson A. Observations on strength training and detraining. Acta Physiologica Scandinavica. 1977;100:491-493.
Tucker L.A. Effect of a weight training program on the self concept of college males. Perceptual and Motor Skills. 1982;54:1055-1061.
Verhoshanski Y., Chornonson G. Jump exercises in sprint training. Track and Field Quarterly. 1967;9:1909.
Voight M.L., Draovitch P. Plyometrics. In: Albert M., editor. Eccentric Muscle Training in Sports and Orthopaedics. London: Churchill Livingstone, 1991.
Vujnovich A.L., Dawson N.J. The effect of therapeutic muscle stretch on neural processing. Journal of Orthopedic and Sports Physical Therapy. 1994;20(3):145-153.
Warren C.G., Lehmann J.F., Koblanski J.N. Elongation of rat tail tendon: effect of load and temperature. Archives of Physical Medicine and Rehabilitation. 1971;51:465-474.
Wedderkopp N., Kaltoft M., Lundgaard B. Prevention of injuries in young female players in European team handball. A prospective intervention study. Scandinavian Journal of Medicine and Science in Sports. 1999;9:41-47.
Weldon S.M., Hill R.H. The efficacy of stretching for prevention of exercise-related injury: a systematic review of the literature. Manual Therapy. 2003;8(3):141-150.
Westing S.H., Seger J.Y., Thorstensson A. Isoacceleration: a new concept of resistive exercise. Medicine and Science in Sports and Exercise. 1991;23(5):631-635.
Wilmore J.H., Parr R.B., Girandola R.N. Physiological alterations consequent to circuit weight training. Medicine and Science in Sports and Exercise. 1978;10:79-84.
Wolpaw J.R., Lee C.L., Carp J.S. Operantly conditioned plasticity in spinal cord. Annals of the New York Academy of Sciences. 1991;627:338-348.
Yarasheski K.E. Acute effects of resistance exercise on muscle synthesis in young and elderly adults. American Journal of Physiology. 1993;265:210.
Zinovieff A.N. Heavy resistance exercise, the Oxford technique. British Journal of Physical Medicine. 1951;14:129.