CHAPTER 8 The hip and thigh
The hip joint
Whereas the glenohumeral joint functions mainly in an open kinetic chain position, the hip (coxofemoral) joint functions mainly in a closed chain position. For this reason, its structure is one of stability for weight bearing. In the standing position, however, the joint is not fully congruent, the anterosuperior portion of the cartilage of the head being exposed. It is only when the joint is taken into a position equivalent to that of the quadruped (90° flexion, 5° abduction, and 10° lateral rotation) that maximum articular contact of the head with the acetabulum occurs (Palastanga, Field and Soames, 1994).
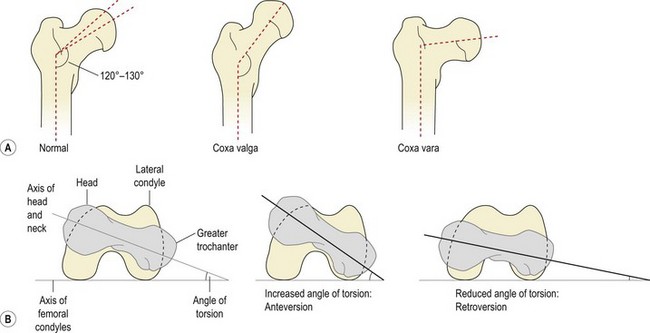
The femoral neck makes an angle (the angle of inclination) with the shaft of 120–130° in the adult, representing the adaptation of the femur to the parallel position of the legs in gait (Fig. 8.1A). This changes from 150° in the newborn to 142° by age 5, 133° by age 15, and 125° in the adult (Reid, 1992; Palastanga, Field and Soames, 1994). Greater angles than these are termed coxa valga, lesser angles as coxa vara.
Definition
In coxa vara the angle between the neck and shaft of the femur is reduced, and a knock-knee position results. In coxa valga the angle is increased and a bowleg position results.
Similarly, the axis of the femoral head and neck make an angle with the axis of the femoral condyles (Fig. 8.1B). This angle (angle of torsion, or angle of anteversion) is normally 10° in the adult, having reduced from 25° in the infant. Increased anteversion is linked to squinting or kissing patellae and this condition is twice as common in girls as in boys.
Craig’s test may be used to assess the angle of anteversion; it compares the angle of the femoral neck to that of the femoral condyles at the knee. The patient lies prone on a couch with the knee flexed to 90°. The therapist palpates the greater trochanter (posterior aspect), and the femur is medially and laterally rotated until the trochanter is parallel with the horizontal plane. The angle of anteversion is estimated from the angle of the lower leg to the vertical, and angles greater than 15° are considered abnormal (Sahrmann, 2002). Interestingly, this test has been found to be more reliable than radiological assessment (Ruwe et al., 1992).
Keypoint
Craig’s test estimates the angle of anteversion by palpation of the greater trochanter as the femur is rotated.
Weight bearing
In standing, each hip takes roughly 0.3 times bodyweight, increased to 2.4 times body weight when standing on one leg. Weight-bearing forces of up to 4.5 times bodyweight may be taken on the hip in running (Magee, 2002). In order to take weight most effectively, bony trabeculae line up in the direction of imposed stress. Two major systems exist within the femur (Fig. 8.2). The medial trabecular system travels from the medial cortex of the upper femoral shaft to the superior aspect of the head. This system takes vertically aligned forces created by weight bearing, and is aligned with the superior aspect of the acetabulum, the main weight-bearing region. The lateral trabecular system begins from the lateral cortex of the upper femoral shaft, crosses the medial system, and terminates in the cortical bone on the inferior aspect of the head. The lateral system is aligned to take oblique forces created by contraction of the hip abductors during gait.
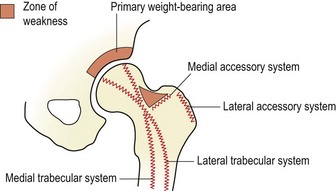
Figure 8.2 Bony trabeculae of the upper femur.
After Norkin, C.C. and Levangie, P.K. (1992) Joint Structure and Function, 2nd edn. FA Davis, Philadelphia. With permission of the publisher FA Davis.
In addition to the medial and lateral trabecular systems, the upper femur is reinforced by medial and lateral accessory systems which take forces created about the trochanters. A zone of weakness is left within the femoral neck which is susceptible to bending forces and is the site of femoral neck fracture (Norkin and Levangie, 1992).
Hip ligaments
The hip joint is strengthened by three capsular ligaments: the iliofemoral ligament and the pubofemoral ligament are on the anterior aspect of the joint, while the ischiofemoral ligament is on the posterior aspect (Fig. 8.3). As the hip is flexed, all three ligaments relax. However, in extension all three ligaments are tight, with the inferior band of the iliofemoral ligament being placed under greatest tension as it runs almost vertically. It is this ligamentous band which limits posterior tilt of the pelvis (Palastanga, Field and Soames, 1994).
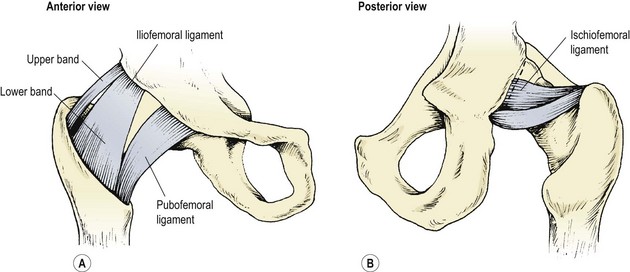
Figure 8.3 Capsular ligaments of the hip joint.
After Palastanga, Field and Soames (1994), with permission.
Keypoint
The inferior (lower) band of the iliofemoral ligament runs almost vertically. With hip extension it is under greatest tension and it limits posterior tilting of the pelvis.
During adduction, it is the turn of the superior band of the iliofemoral ligament to become tighter while the pubofemoral ligament and ischiofemoral ligament relax. In abduction the opposite occurs. In lateral rotation both the iliofemoral ligament and pubofemoral ligament are taut, while in medial rotation the ischiofemoral ligament tightens.
Screening examination
Hip conditions may refer pain anywhere within the L3 dermatome, over the front of the thigh and down to the knee. Initial observation includes resting position, muscle wasting, leg length and gait. Functional activities may also be revealing. Lying in bed with the affected side uppermost (hip adduction and medial rotation) places a stretch over the iliotibial band (ITB) and lengthens the posterior portion of the gluteus medius. This may be a consideration in ITB friction syndrome and for muscle imbalance over the hip. Pain on squatting (hip flexion), as when sitting on the toilet or sitting down into a low chair, warrants closer examination of flexion movements.
Examination for range of motion may be carried out in a supine position for flexion, abduction and adduction and both rotations. Medial and lateral rotation are best compared between the affected and unaffected hip in a prone position with the knees flexed to 90°. Resisted abduction is better tested in a side-lying position with the affected joint uppermost.
Compression of the joint through the flexed knee and circumduction with compression to ‘scour’ the femoral head into the acetabulum is an important assessment for arthritic changes. Both the lumbar spine and the sacroiliac joints must be examined, to eliminate them as a potential cause of pain referral. The straight leg raise and slump test should be used to eliminate the possible involvement of neural tissue. Cyriax (1982) warned that serious pathology may be present if the sign of the buttock is positive. Here, hip flexion with the knee bent is more painful and more limited than straight leg raising. A non-capsular limitation is present, and pain may make the end-feel empty. As hip flexion in straight leg raising is full range the sciatic nerve is unimpinged, and the non-capsular limitation precludes the hip joint. Possibilities include an inflammatory disease state, neoplasm and fracture.
Keypoint
With the sign of the buttock, hip flexion with the knee bent is more painful and more limited than straight leg raising. Serious hip pathology may be present and further investigation is required.
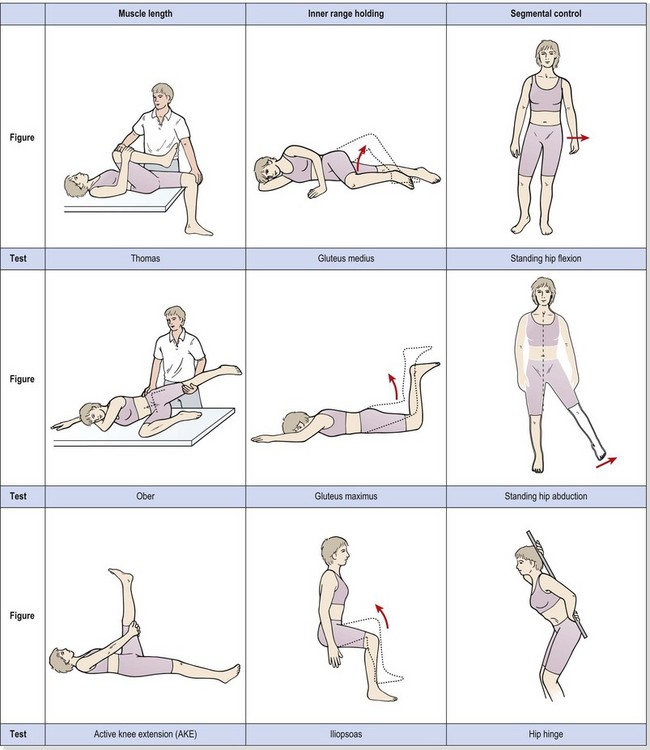
Muscle imbalance around the hip
The concept of muscle imbalance was covered in Chapter 5. In the hip region, the Thomas test and the Ober manoeuvre are used to assess for muscle tightness of the hip flexors (rectus femoris and iliopsoas) and hip abductors (tensor fascia lata and iliotibial band – TFL/ITB). Inner range holding ability of the gluteus medius is assessed with side-lying hip abduction and of the gluteus maximus with the prone-lying hip extension movement described below. Segmental control tests include standing hip flexion, standing hip abduction and the hip hinge (Table 8.1). All tests are described in Chapter 5.
Table 8.1 Muscle imbalance around the hip
Muscle injuries
Quadriceps
On the whole, strains occur mostly in two-joint muscles, due to the more complex coordination involved in controlling movement of two body segments simultaneously. Direct trauma, however, can be imposed on any muscle. In the hip region, this means that the rectus femoris, hamstrings and gracilis muscles tend to suffer strain. The more anterior position of the quadriceps, however, exposes these muscles to risk during contact sports, and to blunt trauma through collision with sports apparatus. A quadriceps contusion is often referred to colloquially as a ‘dead leg’ or ‘charley horse’.
Initially, there is local swelling over the front of the thigh, with some superficial bruising appearing later, often tracking down to the knee. The main danger with this injury is the development of myositis ossificans traumatica (MOT). Thigh contusions may be rated as grade 1 (mild), in which knee flexion beyond 90° is possible, grade 2 (moderate), in which motion is restricted to 45–90°, or grade 3 (severe), in which swelling and pain limit movement to less than 45°. This grading system can be an accurate predictor of the likelihood of MOT development. Jackson and Feagin (1973) assessed quadriceps contusions in 65 subjects, and found that none of the subjects with grade 1 injuries had developed MOT. However, 13 out of 18 subjects who had been graded 2 or 3 later went on to develop the condition, so the amount of movement present in the initial stages is an important indicator of the severity of the lesion, and the prognosis.
Keypoint
Following a quadriceps haematoma or ‘dead leg’, myositis (muscle calcification) is more likely to occur if an injured athlete is unable to flex the knee to 90°.
It is important to limit movement in grade 1 and 2 injuries and to discourage the use of massage, vigorous stretching or exercise and ultrasound, as these are contraindicated in the early post-injury stage. The RICE protocol is used to limit the tissue damage. Ice is applied with compression with the knee and hip flexed as far as is comfortable. Internal compression is therefore applied by fascial tightening (Reid, 1992), while external compression comes from the elastic bandage.
The athlete resuming contact sports should wear padding over the damaged area, to reduce the risk of secondary injury. It is important that full broadening of the muscle belly be obtained during rehabilitation. This will involve resisted quadriceps exercises, beginning with low intensity and building eventually to maximum voluntary contractions (MVC). This is equally important to endurance athletes as to power athletes. Often, distance runners, for example, do not use weight training, focusing instead on stretching. For this injury, however, longitudinal movement of the muscle is less important than lateral movement (broadening). This is because the rectus femoris, being a two-joint muscle, may limit movement, but the vasti, being single-joint muscles, do not. As the vasti form the bulk of the injured tissue, stretching, although important with this injury, is secondary to strength training.
In cases of MOT, calcification is slow, with fibroblasts beginning to differentiate into osteoblasts about 1 week after injury. Radiographic evidence of bone formation is usually visible after 3 weeks (Fig. 8.4). By 6–7 weeks after injury, the calcified mass generally stops growing. Total reabsorption may occur with minor lesions, but more major conditions may continue to show remnants of the mass. The mass rarely interferes with muscle contraction, so excision is not normally required (Estwanik and McAlister, 1990).
Rectus femoris
The rectus femoris is frequently injured by a mistimed kicking action. On examination, pain is usually apparent to resisted knee extension and hip flexion. Passive stretch into knee flexion coupled with hip extension and adduction is also painful. Injury is usually to either the upper insertion or the mid-belly. Upper insertion injuries are palpated with the patient half-lying to relax the muscle. The area of injury is usually the musculotendinous junction approximately four finger widths below the anterior superior iliac spine.
Keypoint
The most common point of injury to the rectus femoris is at the musculotendinous (MT) junction four fingerbreadths below the anterior superior iliac spine (ASIS).
Tenderness to the reflected head attaching to the anterior inferior iliac spine in a youth should raise the question of avulsion injury and may require x-ray confirmation.
Mid-belly tears are less common and are usually sited within the middle third of the thigh. Here, the muscle is subcutaneous and any swelling is immediately apparent. The athlete should flex the hip and knee to 45° against resistance, and as the muscle stands out any abnormality will become apparent.
The rectus femoris can be worked concentrically by flexing the hip against a resistance supplied by a weight bag attached to the knee. Two-joint action of the muscle can be worked with the athlete in supine with the injured leg over the couch side, flexed at both the knee and hip. Manual resistance is applied to the foot of the athlete as he or she extends the knee and flexes the hip simultaneously (Fig. 8.5A).
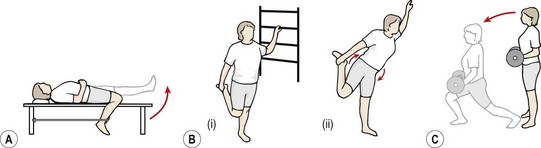
Figure 8.5 (A) Rectus femoris strengthening combining hip flexion and knee extension against elastic band resistance. (B) Rectus stretch. (i) Correct with pelvis fixed. (ii) Incorrect, anterior pelvic tilt throws stress on lumbar spine. (C) Alternate leg lunge. Front leg stresses quadriceps and gluteals, rear leg stresses hip flexors and knee extensors.
Stretching must involve both knee flexion and hip extension and can be carried out in a side-lying position by the athlete, or by the therapist. When performing a rectus femoris stretch in standing (Fig. 8.5B), the abdominal muscles must be tightened to stabilize the pelvis before the hip stretch is applied. Failure to do so will increase the apparent range of motion by anterior tilt of the pelvis with stress thrown on the lumbar spine. Lunging actions are also useful, for both general flexibility and eccentric control (Fig. 8.5C).
Keypoint
The rectus femoris muscle must be stretched and strengthened at both the knee and hip simultaneously.
Results are generally very good, even with complete tears (Fig. 8.6), where full function may be regained even though a marked muscle deformity is present.

Sartorius
Injury to the sartorius is usually an avulsion from the anterior superior iliac spine. There is usually immediate pain, often radiating into the anterior thigh. Swelling and bruising is seen over the iliac crest, often tracking down the thigh. Flexion/adduction of the hip with flexion of the knee causes pain. Displacement of the bone fragment may be from a few mm to 3 cm, but although surgical reattachment of the bone fragment has been described (Veselko and Smrkolj, 1994), conservative treatment normally suffices. The athlete should be non-weight bearing initially, followed by partial weight bearing ambulation for 3–6 weeks, depending on the intensity of pain. Full strength and flexibility must be regained before competitive sport is resumed.
The hamstrings
The hamstrings may be injured either at their attachment to the ischial tuberosity or within their mid-bellies and, less commonly, at the knee (see below). The hamstring pull is the classic sprinting injury, with the athlete spectacularly pulling up in mid-flight with obvious pain.
Pain is apparent on straight leg raising and resisted knee flexion. Resisted flexion and tibial rotation will determine whether the biceps femoris or semimembranosus and semitendinosus is affected.
To palpation, the structure of the muscles differentiates them. The semitendinosus and long head of biceps have a combined attachment on the lower medial facet of the ischial tuberosity, the two muscles travelling together for a short distance until they form fusiform muscle bellies. The semitendinosus almost instantly forms into a long slender tendon, and travels around the medial condyle of the tibia to attach to the medial surface of the tibia below gracilis. The biceps has two proximal attachments; the long head, as described, and the short head from the lower linea aspera. The muscle swings downwards and laterally across the posterior aspect of the thigh and around the lateral ligament to insert into the head of the fibula. The biceps has a dual innervation, and asynchronous stimulation of the two heads has been described as a factor in injury (Burkett, 1975). The semimembranosus comes from the lateral facet of the ischial tuberosity and travels down and medially, becoming flattened and broader as it does so. The semimembranosus is deep to both the semitendinosus and biceps, and divides into five components when it reaches the knee. The principal insertion is to the posterior aspect of the medial tibial tubercle.
Keypoint
The semimembranosus attaches from the lateral aspect of the ischial tuberosity, the semitendinosus and biceps from the medial. At the knee the biceps is lateral, the semitendinosus (medial) is cord-like and the semitendinosus (medial) is flat.
Biomechanics and hamstring injury
During the running cycle, the hamstrings contract eccentrically to decelerate the leg in late forward swing. This action also helps to stabilize the knee. During the support phase, the hamstrings act concentrically to extend the hip, and continue to stabilize the knee by preventing knee extension. During push-off, the hamstrings and gastrocnemius, both two-joint muscles, paradoxically extend the knee. This action is necessary because the mechanical efficiency of the quadriceps is reducing at this point (Sutton, 1984).
The ratio of the strength of the hamstrings to that of the quadriceps muscles (HQ ratio) is important. Normally, the quadriceps is the stronger of the two muscle groups (Table 8.2), as demonstrated by its greater volume. However, any disturbance to this natural balance may leave the weaker muscle group open to injury. The optimum value of the HQ ratio varies from 50% to 80% (Kannus, 1989), with average values in the region of 60%. After knee injury, quadriceps wasting may result in the two muscle groups producing the same power, giving an HQ ratio of 100% (Burnie and Brodie, 1986a).
Table 8.2 Percentage of strength relative to quadriceps at 100%
| Hamstrings | 50–60% |
| Adductors | 90% |
| Abductors | 60% |
| Hip flexors | 55% |
From Reid (1992).
Strength measures comparing quadriceps to hamstrings are traditionally carried out with an isometric dynamometer. However, the disadvantages of joint specificity and lack of movement make isokinetic testing more desirable. During isokinetic testing the speed of movement should match the speed of the sport as closely as possible. The speed must be quoted, as the absolute value of the HQ ratio increases as velocity of movement increases (Burnie and Brodie, 1986b). Slow speeds (45°/s) have been shown to give ratios of 60% and high speeds (300°/s) ratios of 80% (Sutton, 1984). Isokinetic testing in the standard sitting position does not allow hip motion, and movement of the limb does not occur in a closed kinetic chain, so testing is not ideal.
Aetiology of hamstring injury
Tears tend to occur when there is a breakdown in the reciprocal action of the quadriceps and hamstrings, and happen at one of two instances in the running cycle. First, during late forward swing as the hamstrings are decelerating the limb and the athlete feels the muscle ‘stretch’, and secondly, during the take off phase as the athlete ‘pushes’. Changes in muscle coordination as a result of an alteration in the sensitivity of muscle spindles have been cited as a contributory factor to injury. It has been suggested (Sutton, 1984) that an athlete who is fatigued unconsciously increases the sensitivity of the muscle spindles, which respond to stretch with an exaggerated contraction, and this in turn causes injury.
Lack of flexibility may predispose to hamstring injury, and may be assessed with the athlete lying supine with one hip flexed to 90°. Maintaining this position by gripping the leg with the hands, the athlete attempts to straighten the leg with quadriceps power only (AKE test). Adequate flexibility is indicated by an ability to lock the leg out while maintaining 90° hip flexion. Alterations in the normal 60% strength ratio between the quadriceps and hamstrings and a deficit greater than 10% between the two sets of hamstrings has also been cited as a predisposing factor (Burkett, 1970).
Many hamstring injuries tend to recur, and lack of full rehabilitation may be one cause. After injury, athletes are usually aware of lack of mobility in the hamstrings and are often conscientious about stretching exercises. However, muscle wasting is not so obvious in the hamstrings as it is in the quadriceps, and so many athletes forget to spend time regaining hamstring strength. In addition, using eccentric exercises as part of a general leg conditioning programme may strengthen the series of elastic components within the hamstrings (the non-contractile portion of the muscle, including the muscle tendon and the connective tissue framework of the muscle itself), making them better equipped to withstand loading at heel strike (Stanton and Purdam, 1989). The inclusion of plyometric training in late stage rehabilitation of hamstring injury is therefore essential.
A systematic review of the causation of hamstring injuries in sport (Foreman et al., 2006) was not able to reveal a single factor to be consistently associated with hamstring injury due to the wide variety of research methodologies used in studies. However six common themes were identified (Table 8.3).
Table 8.3 Factors associated with hamstring injury causation
| Factor | Implication |
|---|---|
| Muscle strength & imbalance | Reduced hamstring strength may not be able to counteract quadriceps force during knee extension in swing phase |
| Muscle control | Poor neuromuscular control may affect interaction of thigh muscles |
| Flexibility | Reflects on ability of muscle to absorb shock |
| Previous injury | Rehabilitation may have been inadequate or risk factors still present |
| Anthropometry | Age, race, number of type II fibres and anterior pelvic tilt all implicated |
| Muscle fatigue | Injuries more common while athletes fatigued, running gait change suggested |
From Foreman et al. (2006).
Exercise therapy following hamstring injury
Strength
Exercise therapy aims to progressively increase the function of all the fitness components relevant to hamstring function. Strength restoration begins with isometric contractions within the pain-free range to facilitate muscle broadening and reduce adhesion formation. Concentric strength is later introduced against limb resistance initially, followed by therapist resistance and later light-weight resistance. Knee flexion may be used in both lying and standing. Hip extension (from outer to inner range) is used in prone lying and also standing. The two may be worked in PNF patterns using hip extension, abduction and external rotation combined with knee extension, and the reverse using hip flexion, adduction and internal rotation combined with knee flexion. Both patterns are used initially against controlled therapist resistance but may be later usefully modified against elastic band or pulley resistance.
Where isokinetics are available, a variation of speeds is important. Slow speeds of 60° and 120°/s may be used to begin with, progressing to 240° and 300°/s as pain allows. Hamstring isolation exercises, such as leg curls in lying and standing (Fig. 8.7), have their place in initial rehabilitation to ensure maximal muscle broadening, but have distinct limitations which must be recognized. First, these exercises work only the knee flexion function of the hamstrings, with little activity over the hip. Second, the action is open chain only, when the predominant function of the hamstrings occurs in closed chain format. Third, the exercises are often performed with the emphasis placed on inner-range contraction, which may tend to shorten the muscle. The hamstrings are unlikely to be posturally lengthened so that they require shortening. It is more likely that the muscles will already lack flexibility, so full range resisted work is preferable.
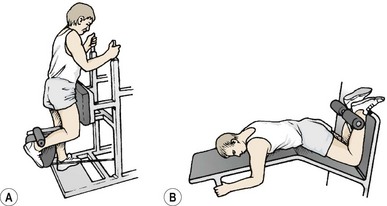
Figure 8.7 Hamstring isolation exercises. (A) Standing leg curl. (B) Lying leg curl. These are non-functional movements which must be used with caution.
Keypoint
Weight training machines often work the hamstrings only in open chain format. This type of action often shortens the hamstrings and works them at the knee only. Closed chain actions involving simultaneous knee and hip movement are more functional.
Eccentric training
Eccentric training of the hamstrings is an important component of rehabilitation. At the end of the swing phase of gait, the hamstrings decelerate the limb by eccentric action, and so preparing the athlete for this action is essential. Eccentric training has been shown to favourably affect the length−tension curve of the hamstrings measured on an isokinetic dynamometer (Clark et al., 2005). Subjects showed a 19.4% change in the position of peak force creation towards the extended knee which may protect against eccentric overload at the end of the swing phase. Eccentric hamstring training of this type has been shown to reduce the incidence of injury in elite soccer (Arnason et al., 2008), and to successfully rehabilitate Australian rules football players (Brughelli, Nosaka and Cronin, 2009). Eccentric exercises include box drops, negative lunges and eccentric leg extension from high kneeling (Nordic hamstring exercise) (Fig. 8.8).

Closed chain actions
Closed chain exercises may be performed by modifying many common exercises. Leg rowing (Fig. 8.9A) is a useful exercise. The athlete sits on a towel (on a wooden floor) or plastic tray (on a carpeted floor) with the feet fixed. The action is to pull the body forwards by hamstring action, mimicking a rowing position. Sitting astride a gym bench or ‘form’ (Fig. 8.9B), the athlete digs the heels into the ground and again pulls the body forwards using leg strength alone. Both of these actions may be performed unilaterally or bilaterally. The slide trainer may also be used for sagittal leg pumping actions with the knees straight or bent (Fig. 8.9C). The sitting leg press weight training apparatus may be used for the sprint kick exercise (Fig. 8.9D). Instead of sitting on the bench, the athlete turns around and places the shoulder against the chair back, and the ball of the foot on the machine pedal. The action is to press the machine pedal with a combined hip and knee extension action.
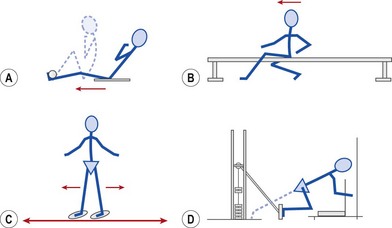
Figure 8.9 Hamstring exercises in closed kinetic chain. (A) Athlete sits on a towel on a wooden floor with feet fixed. Pull body forwards by flexing the knees and hips. (B) Sitting astride a gym bench, grip the feet against the floor and pull the body forwards. (C) Using a commercial slide trainer, straight leg hip flexion and extension is performed. (D) Kneeling on a seated leg press machine, hip and knee extension is performed.
Speed, power and flexibility
Speed and power are worked using plyometric activity. Stepping, jumping, lunging and hopping actions are all useful and are progressed for range and speed against body weight resistance and for power against weight resistance. For this later aspect, a weighted jacket is easier (and safer) than holding weights.
Flexibility exercises for the hamstrings must take account of pelvic action and the action of the two-joint muscle. In addition, relative flexibility may dictate that the majority of the stretching force is imposed on the lumbar spine in toe-touching type movements (Fig. 8.10A).
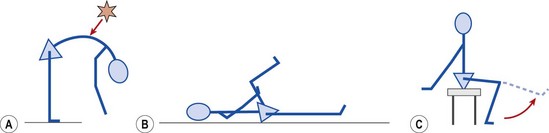
Figure 8.10 Hamstring flexibility exercises. (A) Tight hamstrings limit anterior pelvic tilt, throwing stress onto the less flexible thoracolumbar junction. (B) Active knee extension. (C) Tripod stretch.
Flexibility may begin with active knee extension (Fig. 8.10B). The advantage of this movement is the reciprocal innervation gained from quadriceps action, and the control that the athlete has over the movement. In addition, the back is supported throughout the action. The tripod stretch (Fig. 8.10C) is also a useful exercise which requires a combination of pelvic stability with hamstring flexibility.
Groin injuries
Groin injury has a general incidence of between 0.5% and 6.2%, with the incidence increasing to between 5% and 13% in soccer (Choi, McCartney and Best, 2008). Groin conditions fall broadly into two categories, those affecting the symphisis pubis (joint) and those affecting the adductors (muscle).
Adductor strain
Variously called groin strain and rider’s strain, a tear of the adductor muscles gives pain to resisted adduction, and abduction stretch. Damage is usually to the musculotendinous junction about 5 cm from the pubis, or more rarely the teno-osseous junction, giving pain directly over the pubic tubercle (adductor longus) or body of the pubis.
The condition is more common in sports requiring a rapid change of direction, and where the adductors are used for propulsion. Pain is often experienced with sprinting, lunging and twisting on the straight leg.
Ultrasound must be used with caution because of the proximity of this area to the genitalia. Isometric contractions may be carried out by gripping a foam pillow between the knees. During the subacute phase, transverse frictions may be applied with the athlete in a supine position, with the affected leg abducted and the knee flexed and supported on a pillow.
Strength and flexibility
The adductor muscles are often neglected with respect to strengthening and flexibility, particularly in the male athlete. Sagittal plane leg movements are common in weight training, and although frontal plane actions are possible, they are infrequently used.
Treatment for the condition must therefore involve stretching and strengthening the adductors. Initially, strength exercises such as side-lying (injured limb down), hip adduction with a weight bag over the knee (early) or ankle (more advanced) are useful. Later, adduction may be performed using a weight and pulley apparatus (Fig. 8.11). Power training may be carried out by flicking a medicine ball with the foot with an adduction action. Swimming exercises, such as breast stroke, and hip adduction with a paddle secured to the lower leg are also of benefit. Closed kinetic chain actions using running, side stepping, jumping and hopping are included during late stage rehabilitation.
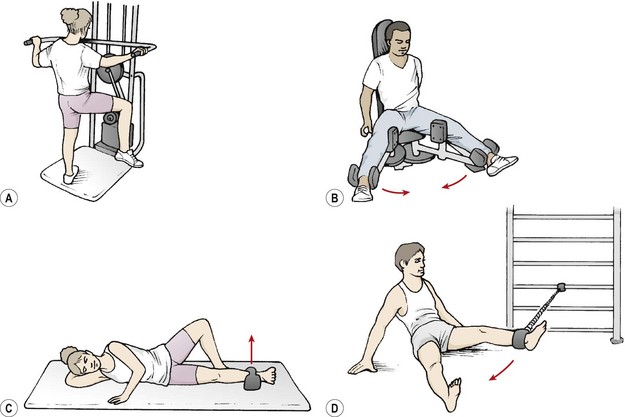
Figure 8.11 Hip adductor strengthening. (A) Unilateral weight-training. (B) Bilateral weight-training approach. (C) Weight bag. (D) Resistance tubing.
Adductor stretching may be used for both the short adductors with the knee bent, and gracilis with the knee straight. One common exercise is the ‘tailor position’ stretch (Fig. 8.12A), where the soles of the feet are together and the knees are pressed down with the hands or elbows. Although a useful movement, athletes often allow the pelvis to posteriorly tilt, flexing the lumbar spine (Fig. 8.12B). The posterior tilt of the pelvis pushes the pubic bone forwards, allowing a greater apparent range of motion and the knee to drop down further. A neutral pelvic position may be maintained by sitting on a wedge (Fig. 8.12C), or alternatively placing a rolled towel beneath the ischial tuberosities. As the knees are pressed down, the spine should be lengthened (’reach the top of your head to the ceiling’). The gracilis may be stretched in the stride sitting position with the leg straight, the same cautions concerning pelvic tilt applying. A more advanced gracilis stretch can be performed against a wall (Fig. 8.12D). The hips are flexed to 90° and the legs straight. Contract–relax (CR) stretching is performed by closing the legs (adduction resisted by limb weight) and then relaxing them into abduction.
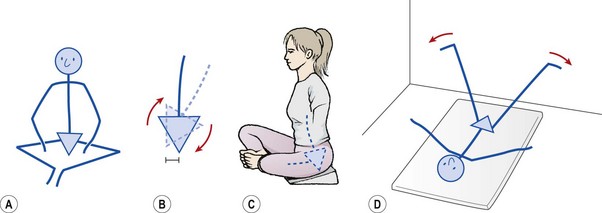
Figure 8.12 Adductor stretching. (A) Common adductor stretch. (B) Allowing the pelvis to posteriorly tilt pushes the pubis forwards. (C) Sitting on a wedge maintains the neutral lordosis. (D) Long adductor stretch.
Keypoint
When stretching the adductor muscles, take account of the degree of pelvic tilt. Posterior pelvic tilt will draw the pubic bone forwards and release tension from the adductor muscles in many stretches. Ensure that the athlete maintains lumbopelvic alignment throughout the stretch.
One complication of the disorder is the formation of myositis ossificans traumatica within the adductor origin. This is usually a consequence of inadequate rest during the acute stage of the condition. This condition is often described, somewhat inaccurately, under the general term ‘osteitis pubis’ (see below).
Osteitis pubis
True osteitis pubis is a condition affecting the pubic symphysis rather than the pubis itself, although the two conditions often coalesce. Diagnostically it is necessary to differentiate osteitis pubis from osteomyelitis pubis. The nature of osteitis pubis is inflammatory, while that of osteomyelitis pubis is infection. The most common infective agent is Staphylococcus aureus. This may come from infection during gynaecological or urological operations, or may be without an identifiable origin (Pauli et al., 2002).
Keypoint
Osteitis pubis is inflammatory in nature, while osteomyelitis pubis is an infection, most commonly of Staphylococcus aureus bacteria.
The clinical features of the two conditions are similar, except that osteomyelitis pubis is confirmed by biopsy and culture to identify the pathogen. Intravenous antibiotic treatment is usually effective.
With osteitis pubis, shearing stress is placed on the pubic symphysis during mid-stance as the non-weight bearing hip drops, tilting the pelvis. With distance runners, and particularly after pregnancy when the pubic symphysis is still mobile, this repetitive stress may inflame the pubic symphysis, a condition known as pubis stress symphysitis (Rold and Rold, 1986). Several etiological factors have been suggested including restriction of hip mobility, hip and abdominal muscle imbalance, and sports involving repetitive twisting and cutting actions (LeBland: Leblanc &, 2003).
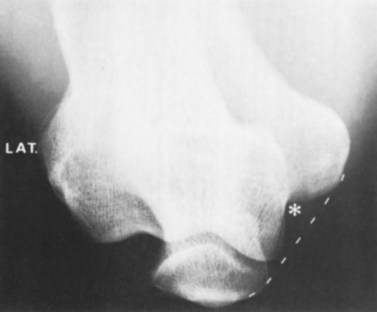
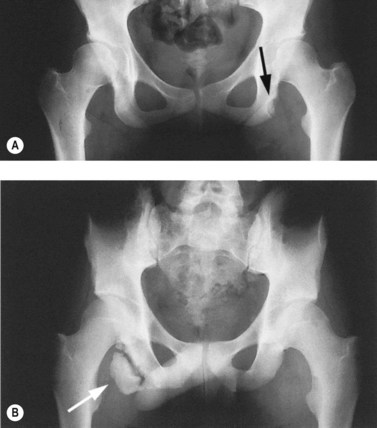
With osteitis pubis no instability of the pubic symphysis occurs, but there is tenderness over the area with rarefaction of the pubic bones and sometimes widening of the symphysis pubis apparent on x-ray. Erosion of the superior and inferior aspects of the symphysis may also occur (Fig. 8.13). The athlete often has a waddling gait, and may describe occasional crepitus. Severe (long-term) cases may progress to sclerosis and eventual narrowing of the symphysial joint space requiring wedge resection (Grace, Shives and Coventry, 1989). Bone marrow oedema may be visible on MRI scan.
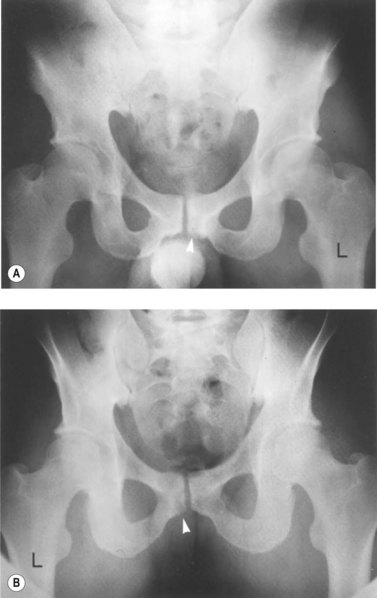
Figure 8.13 Osteitis pubis. (A) Anterior and (B) posterior view showing bone fragment.
From Magee (2002) with permission.
Palpation may be used to differentiate true osteitis pubis from tendinitis of the gracilis or avulsion injury to the gracilis attachment. The gracilis muscle attaches to the inferior aspect of the symphysis and local palpation may reveal spot tenderness (Fig. 8.14). Both of these conditions give pain to resisted adduction as well as to local palpation. Importantly, osteitis pubis often gives pain to pelvic springing tests to the iliac crest whilst gracilis conditions do not. The condition may be graded as illustrated in Table 8.4.
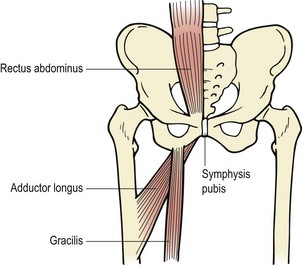
Table 8.4 Grading of osteitis pubis
| Grade | Symptoms |
|---|---|
| I | Unilateral symptoms involving dominant leg, pain in inguinal region and adductor muscles |
| II | Bilateral symptoms with inguinal and adductor muscle pain |
| III | Bilateral inguinal pain with adductor and abdominal symptoms |
| IV | Adductor and abdominal pain referred to pelvis and lumbar spine. Exacerbation when walking on uneven surfaces or cough/sneeze. Limitation of ADL |
ADL− activities of daily living.
After Wollin and Lovell (2006).
Keypoint
Palpation of the groin reveals the attachment of rectus abdominis at the top of the symphysis and adductor longus as a tight cord at the bottom. Gracilis attaches to the inferior portion of the symphysis away from the mid-line.
Patients diagnosed earlier experience fewer symptoms and return to play faster (Wollin and Lovell, 2006). Rehabilitation focuses on core stability and strength / endurance of the muscles attaching to the pelvis. Initially functional rest may be used, avoiding resisted exercise and ballistic stretching to the adductors and rectus abdominis. Isometric actions of the deep abdominals and pelvic floor are combined with isometric hip adduction. Fitness may be maintained with static cycling and aquajogging providing these actions are pain free. As pain subsides exercises progress, avoiding mid- to end-range abduction. Hip musculature may be retrained using resistance bands or pulleys. Hip stability training using single leg standing actions to retrain the gluteus medius and core stability work are essential. Stretching must target the gracilis, which, as it attaches below the knee, must involve abduction movements with the knee straight. Rehabilitation progresses to skating actions on a slide board (Fig. 8.15A,B) and full range adduction actions against resistance are used within pain tolerance (Fig. 8.16A,B). Progression of both range of motion and speed of motion on a slide board are used. A rehabilitation protocol has been described by Wollin and Lovell (2006) which gives exercise suggestions and criteria for progression. This programme (Table 8.5) has been used to successfully rehabilitate young soccer players, all of whom returned to competitive sport symptom free with no recurrence reported at 12 months follow up.



Table 8-5 Rehabilitation programme for osteitis pubis
| Module I | |
| Module II | |
| Module III | |
| Module IV |
ABD − abduction; ADD − adduction; EXT − extension; FLEX − flexion; PF − pelvic floor; RTUS − real time ultrasound; TrA − transversus abdominis.
From Wollin and Lovell (2006) with permission.
Where conservative management fails and symptoms are both severe and long lasting, invasive management is required. Injection with corticosteroid has shown a moderate success rate for return to sport (58.6% with return 8 weeks following injection) but a high number of athletes (20.7%) may not respond (Connell, Powell and McCaffrey: O’, 2002). Prolotherapy using dextrose and lidocaine has shown a better success rate (91.7% return to sport within 9 weeks of injection) suggesting that it may be superior to corticosteroid (Topol, Reeves and Hassanein, 2005). Surgery using curettage of the pubic symphysis or pubic symphysis stabilization with polypropylene mesh has also been used successfully where symptoms were long term (17 months). Complications included haemospermia and intermittent scrotal swelling (Choi et al., 2008).
Avulsion injuries around the hip
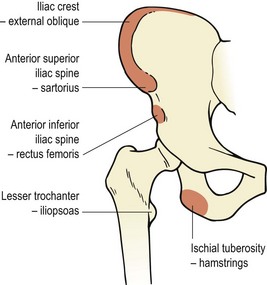
Avulsion injuries occur when a rapid muscle contraction pulls on the bony origin of the muscle. This may occur if the contracting muscle suddenly meets an unexpected resistance, such as kicking and catching the ground. Alternatively, avulsion may occur through uncontrolled stretching, particularly unsupervised full-range ballistic stretching (Fig. 8.17). This may occur to the sartorius at the anterior superior iliac spine, the rectus femoris at the anterior inferior iliac spine, the hamstrings at the ischial tuberosity or, less commonly, to the iliopsoas at the lesser trochanter (Fig. 8.18).
Avulsion usually occurs at the apophysis in a young (14–17 years) athlete. However, as the ischial apophysis unites later (20–25 years), avulsion of the hamstrings at the ischial tuberosity may be seen up until this age and has been described in judo exponents (Kurosawa et al., 1996). At this time the tenoperiosteal junction is generally stronger than the unfused growth centre. There is usually little displacement due to the thickness of the periosteum. Athletes usually complain of a sudden onset of pain with limitation of movement over the affected joint. Treatment involves RICE, and, importantly, protection from tension forces over the muscle. X-ray is used to confirm the injury and bone healing usually occurs within 3–6 weeks where displacement has not occurred. With displacement of the hamstring origin, suturing may be required (Oravo and Kujala, 1995).
Bursitis
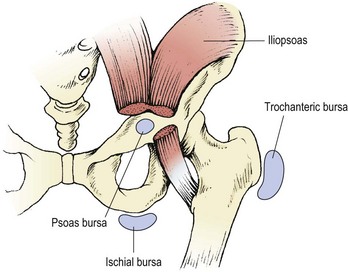
The main sites of bursitis around the hip are the trochanteric bursa, and, to a lesser extent, the ischial bursa and psoas bursa (Fig. 8.19).
Trochanteric bursitis
The trochanteric bursa lies between the gluteus maximus and the posterolateral surface of the greater trochanter. Bursitis may arise if flexibility of the iliotibial band (ITB) is reduced. Normally, the ITB moves forwards with flexion and backwards with extension of the hip. The bursa may be irritated if the movement of the ITB is limited, a cause of ‘snapping hip syndrome’ (see below). Biomechanical faults in running which tax the gluteus maximus or alter pelvic tilt in the frontal plane are also a causal factor. Running on a banked surface with one foot lower than the other, and excessive posterolateral heel wear, which increases supination at heel strike, will increase pressure on the bursa via the ITB. Muscle imbalance between the adductors and abductors, especially in an athlete with a wide pelvis, or in young athletes with a tendency to run with the feet crossing, may also be a contributory factor.
Pain often comes on gradually over the lateral aspect of the hip, in some cases radiating down to the knee. It may be aggravated by crossing the legs, climbing stairs and getting into and out of a car. Pain may be elicited by passively flexing, adducting and medially rotating the affected hip, and with resisted hip abduction allowing muscle tension to compress the bursa beneath the gluteus maximus. Palpation for tenderness is carried out in a side-lying position, with the injured limb uppermost and slightly flexed. The patient can often feel the injury while lying in this position because of the hip adduction involved. Pressure for palpation should be directed behind, rather than on top of, the trochanter. The Ober manoeuvre is often positive.
Keypoint
Trochanteric bursitis gives pain over the lateral aspect of the hip. Palpation is carried out in a side-lying position, with the injured limb uppermost and slightly flexed. Pressure for palpation should be directed behind, rather than on top of, the trochanter.
Treatment aimed at reducing pain and inflammation must be linked to a removal of the cause, be it training or biomechanically related. Phonophoresis with hydrocortisone gel may be useful as the bursa is fairly superficial. If the ITB is shortened (the Ober manoeuvre will confirm this), stretching is obviously called for.
In patients where pain is referred and point tenderness is not present, trochanteric bursitis may be differentiated from arthritis by the absence of a capsular pattern.
Ischial and psoas bursitis
Psoas bursitis usually occurs as a result of excessive activity. Pain is reproduced by passive hip flexion and adduction. In addition, slight pain can occur on contraction of the psoas in a position of maximal hip flexion. Palpation over the lesser trochanter is made easier by flexing the hip and knee to 45° and externally rotating the hip. The limb is supported on a pillow.
Ischial bursitis (weavers’ bottom) gives pain after prolonged sitting, and may be set off by direct trauma, such as a fall onto the backside when ice-skating. There is pain on palpation of the bursa between the ischial tuberosity and the gluteus maximus. This condition may be mistaken for a hamstring pull but is differentiated by the absence of pain to resisted knee flexion. The condition is aggravated by tight hamstrings, speed work and excessive hill running.
Treatment is by rest from the aggravating movement, and anti-inflammatory modalities. Where ischial bursitis has developed through overuse, hamstring stretching may be required.
Neural structures and posterior thigh pain
Discal involvement
The hip is an L3 structure and so can refer pain down the front of the thigh. However, posterior thigh pain frequently accompanies low back pain and may be a result of nerve entrapment in the absence of accompanying symptoms in the back. Distinguishing between sciatic impingement and hamstring injury is not always straightforward. A history of trauma is important, and if straight leg raising (SLR) causes pain but resisted knee flexion does not, the spine should be examined further. Weakness on resisted knee flexion could be through intramuscular trauma, pain inhibition or impaired neural conduction. Lasegue’s sign (straight leg raise) will cause pain from sciatic and hamstring stretch; however, adding neck flexion will not affect the hamstrings but will stretch the dural covering of the cord and nerve roots. Pain of discal origin will therefore be worse and that of hamstring origin unchanged.
The slump test is helpful both diagnostically and therapeutically, and is used to assess tension in the pain-sensitive structures around the vertebral canal and/or intervertebral foramen. During the slump test, a hamstring tear will give pain as the leg is straightened, but will not be made worse by slumping the spine, providing the pelvis does not tilt.
Kornberg and Lew (1989) assessed athletes with grade I hamstring tears using the slump test. Where positive, they used the slump therapeutically as a stretching exercise, and found that the addition of the slump procedure to standard physiotherapy management of the injuries (which had included stretching exercises) was significantly more effective in returning a player to full function. They argued that abnormal neural tension had produced symptoms which mimicked hamstring injury. In addition, they made the point that increased tension in the neural structures could elevate the resting tone of the hamstrings, predisposing them to intrinsic injury.
Piriformis syndrome
The piriformis muscle (Fig. 8.20) attaches from the front of the second to fourth sacral segments, the gluteal surface of the ileum and the sacrotuberous ligament. It then travels through the greater sciatic notch to attach to the upper medial side of the greater trochanter. Its position is such that the sciatic nerve rests directly on the muscle, and in 15% of the population (Cailliet, 1983) the muscle is divided into two with the sciatic nerve passing between the two bellies.
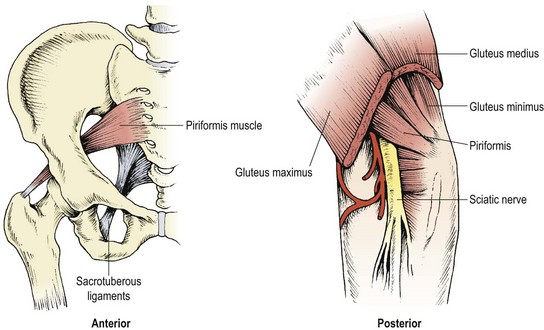
Piriformis syndrome occurs in women more frequently than men (ratio 6 : 1). If the muscle is inflamed, shortened or in spasm it will impinge on the sciatic nerve, giving pain and tingling in the posterior thigh and buttock. Pain is deep and localized and examination of the lumbar spine and sacroiliac joints is unrevealing. Palpation of the muscle may be carried out with the patient prone in the frog position (hip flexed and abducted bringing knee to chest), or rectally. Resisted lateral rotation of the affected hip gives pain, and passive stretch into internal rotation is painful and may be limited.
Management involves pain-relieving modalities and stretching the external rotators of the hip. A simple self-stretch can be taught to the patient. If the right hip is affected, the left hip is flexed to 90° and the right foot is placed on the left knee. The right hip is pushed gently into abduction and external rotation (Fig. 8.21).
Gluteus medius tendinitis
Pain over the insertion of the gluteus medius into the greater trochanter has been reported as a common cause of hip pain (Lloyd-Smith, Clement and McKenzie, 1985). Pain from the gluteus medius itself can be differentiated from trochanter bursitis by palpation (tendinitis gives pain proximal to the trochanter, bursitis directly over it) and resisted movements. Pain to resisted abduction will define tendinitis, while bursitis will generally not give pain to resistance. However, the two conditions may coexist.
Although the exact cause of this condition is unclear, lengthening of the posterior fibres of the gluteus medius (PGM) has been proposed as part of a hip adduction syndrome (Sahrmann, 2002). Here, the PGM and hip lateral rotator muscles are long and weak due to single leg standing in a swayback posture with the hip held adducted and medially rotated. The trunk may be laterally flexed over the stance leg.
The condition is more common in women than in men due to the width of the pelvis, and muscle overstretch also occurs at night with the affected leg on top (adduction and medial rotation). Pain and burning occur along the lateral aspect of the hip and thigh, and are worse in the morning after sleeping. Discomfort reduces with activity but increases with fatigue, particularly with prolonged standing.
Treatment note 8.1 Trigger point treatment of buttock structures
Pain from muscle origin may be treated by direct pressure and dry needling. Dry needling or trigger point acupuncture involves inserting a sterile acupuncture needle into the muscle which is normally overactive and may be in spasm. As the needle enters the muscle, it meets tissue resistance. The needle may gradually be pressed into the firmer tissue as the tissue gives way. Precise surface marking is required for this technique and knowledge of underlying structures is essential.
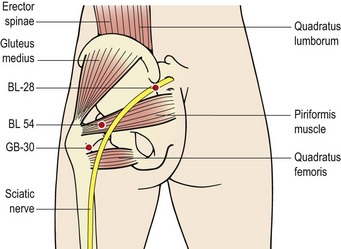
In the hip, the major hip muscles treated in this way are the piriformis, gluteus medius and quadratus femoris. The lumbar multifidus may be treated as it thickens between the sacrum and medial aspect of the ilium, an area called the multifidus triangle. In addition, the quadratus lumborum and erector spinae may be needled at their insertion onto the iliac crest (Gunn 1996, 2000).
Surface marking
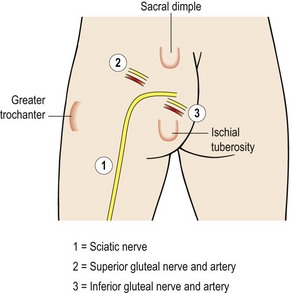
To visualize important structures in the buttocks, three lines may be drawn joining the sacral dimple (posterior superior iliac spine, PSIS), greater trochanter and ischial tuberosity (Borley, 1997). The sciatic nerve emerges from the pelvis midway along a line drawn from the sacral dimple and the ischial tuberosity. It then runs in a semicircle to a point halfway along a line joining the ischial tuberosity and the greater trochanter of the femur. The superior gluteal nerve and artery pass a point 1/3 along a line joining the sacral dimple to the greater trochanter. The inferior gluteal nerve and artery pass a point 1/3 along a line joining the ischial tuberosity and the sacral dimple (Fig. 8.22).
Trigger points
To facilitate palpation, the patient should be placed in side-lying with the painful side on top and the hip flexed. The gluteus medius may be treated about 5 cm along a line from the iliac crest to the greater trochanter. It is sometimes easier to palpate the greater trochanter and allow the palpating finger to move backwards and upwards until a painful point is located. The quadratus femoris can only be located with the gluteal muscle relaxed, and it may be palpated from the posterior aspect of the greater trochanter to the lateral edge of the ischial tuberosity. As it is a lateral rotator of the hip, medially rotating the femur will place the muscle on stretch and make palpation easier. The piriformis is located along a line from the greater trochanter to the 2nd, 3rd and 4th sacral segments. If deep manual pressure is used points within the muscles may be chosen. For dry needling, use of points close to the greater trochanter or ischial tuberosity avoids the risk of hitting the sciatic nerve.
The quadratus lumborum and erector spinae may be palpated along the iliac crest. To facilitate location the patient should be side flexed away from the painful side to place the muscle on stretch. The multifidus is large and thick in the lumbar spine and in the area between the PSIS and sacral spines down to a level of S4 (the multifidus triangle), and muscle may be treated for trigger points with either manual therapy or dry needling (Fig. 8.23).
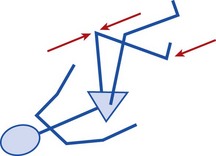
Definition
Hip adduction syndrome occurs when athletes stand favouring one leg in a swayback posture. The weight-bearing leg drifts into adduction and medial rotation, and the trunk side flexes over the stance leg. The posterior fibres of the gluteus medius muscle become long and weak as a result.
Restoration of muscle balance is the key to management. Exercises to shorten the PGM are used which combine hip abduction and lateral rotation in side-lying (Fig. 5.9C). Athletes with this condition should avoid crossing their legs when sitting. When standing they should make a conscious effort to carry their weight evenly over both legs. During prolonged standing they should perform gluteal bracing (20–30 second hold) every 30 minutes.
Hamstring syndrome
Puranen and Orava (1988) described athletes with gluteal pain radiating into the posterior thigh who had no history of trauma. Pain occurred most often in the sitting position, and when stretching the hamstrings. Local tenderness was evident to the ischial tuberosity, neurological examination was normal, and extensive physiotherapy, including electrical modalities stretching and strengthening (no specific details given), failed to remove the symptoms.
At operation, tight fibrotic bands were found from the semitendinosus and biceps femoris, with the thickest actually within the bulk of the biceps. These were located close to the sciatic nerve and in some cases actually adhered to it.
Release of the tight bands gave symptomatic relief to 52 of the 59 patients treated. The authors proposed that excessive stretching may have led to hypercompensation within the muscles, particularly in sprinters and hurdlers.
Hip joint pain
The hip (coxa-femoral) joint itself may be implicated in a number of sports injuries. Arthritic changes to the joint, labral involvement and joint displacement (anterior femoral glide) causing tissue impingement are the most important hip joint conditions encountered in sport.
Hip arthritis
Osteoarthrosis of the hip affects between 1% and 2% of the adult population with women making up 60−75% of this group. The condition often occurs secondary to other pathology, most typically osteonecrosis, Perthes’ disease, developmental dysplasia, slipper femoral epiphysis, hip fracture and congenital coxa vara or valga (Fagerson, 2009). X-ray shows narrowing of the joint on the weight-bearing portion with osteophyte formation. Manual therapy has been shown to be of value in the non-operative treatment of hip OA, with pain, stiffness, hip function and range of motion all changing significantly (Hoeksma et al., 2004). Acupuncture is also of value (Haslam, 2001), with six sessions of 25 minutes duration giving significant improvement of pain and function (WOMAC score) which is maintained for 8 weeks after stopping treatment. Change of lifestyle is also effective, and includes weight reduction, exercise modification, reduction in load carrying and use of walking aids. Clinically a combination of acupuncture and manual therapy may be used to target pain and enable a patient to embark on a progressive exercise programme to re-strengthen the supporting musculature of the hip. Patients often find joint mobility exercise including pool work of value, and exercise therapy has been shown to be of value at reducing both pain and disability (Van Baar et al., 1998).
Several hip arthroplasty (replacement) techniques are used broadly falling into total and partial replacement with and without cement. Three main incisions are used as shown in Table 8.6, and exercise prescription should take into account the muscles affected.
Table 8.6 Most common hip arthroplasty approaches
| Approach | Muscle region |
|---|---|
| Posterior | Piriformis and short femoral external rotator muscles removed and reconnected |
| Lateral | Greater trochanter removed (osteotomy) to lift up gluteus medius and gluteus minimus muscles. Reconnected using wires |
| Anterior | Cut between sartorius and TFL (anterior) or between TFL and gluteus medius (anterolateral) |
TFL − tensor fascia lata.
Labral tears
It is estimated that 55% of athletes who present with hip pain of unknown etiology may have a labral tear (McCarthy et al., 2001). The acetabular labrum is a rim of connective tissue attached to the acetabulum. Triangular in cross section, it is wide and thinner in its anterior region and largely avascular. The labrum attaches through a 2 mm thick zone of calcified cartilage and itself merges with the articular cartilage of the joint proper. Nerve fibres have been identified within the labral substance (Kim and Azuma, 1995) making it possible that this structure may be the source of pain. The labrum functions to deepen the hip socket by 20% increasing its surface area by nearly 30% and so reducing the force per unit area (Lewis and Sahrmann, 2006). By acting as a seal for the joint, the labrum keeps the synovial fluid within the articular cartilage, increasing fluid pressure and unloading the joint. Removal of the labrum has been found to increase contact stress by as much as 92% (Ferguson et al., 2000).
Labral tears are thought to occur in sport during end range forcible lateral rotation with hyperabduction or hyperextension. However, Santori and Villar (2000) found that nearly 75% of tears were not actually associated with a specific event. Hip dysplasia has been given as a risk factor for the development of labral tears. Dysplasia may result from a shallow acetabulum, change in anteversion or an alteration in the distance from the centre of the femoral head to the axis of the shaft (offset angle).
Keypoint
Hip dysplasia is a bony abnormality of the acetabulum or femoral head which results in malalignment of the joint. There is an inadequate containment of the femoral head in its socket.
The majority of patients report pain in the anterior hip or groin with clicking on certain movements. Locking and giving way are also common. There may be some limitation of movement, commonly rotation with hip flexion and adduction. The tear is most commonly anterior in the western hemisphere, and posterior in the East, and is thought to be associated with the preference for chair sitting or squatting in these geographical regions, respectively (Lewis and Sahrmann, 2006). End range flexion, adduction and medial rotation are commonly painful, with the FADDIR test (flexion−adduction−internal rotation) identifying possible anterior labral tear, anterior superior impingement or iliopsoas bursitis (Magee, 2008). The test is performed with the patient supine. The leg is flexed to 120°, abducted and inwardly (medial) rotated. From this position it is moved into adduction and outward (lateral) rotation as it is brought down towards the couch.
Non-surgical management focuses on the correction of hip movement dysfunction. Standing posture is assessed noting hip extension in a swayback alignment, and hip hyperextension during gait. Activities include tests for relative strength of iliopsoas, gluteus medius, gluteus maximus and deep hip lateral rotators. Hip lateral rotation with abduction is encouraged to activate the posterior gluteus medius and quadratus femoris muscles. These muscles act to glide the hip posteriorly and inferiorly. The quadratus femoris in rodents has been shown to have a higher (69.9%) distribution of slow twitch fibres than the known postural muscle soleus (35.1%), suggesting an important role in sustaining neutral alignment of the limb (Hitomi et al., 2004). Posterior and inferior glide is encouraged using the quadruped rocking action described below.
Hip impingement
Impingement of the femur onto the acetabulum (femoroacetabular impingement) has been identified as a factor in the development of OA of the hip (Ganz et al., 2003). Impingement may occur in the presence of an abnormally shaped femoral head (Cam impingement) where the head of the femur contacts the acetabulum during end range flexion. Alternatively a leverage effect may occur (pincer impingement) due to tissue approximation where the posterior aspect of the femoral head is forced against the acetabulum at end range flexion.
Keypoint
In cam impingement the anterior aspect of the acetabulum is forced against the femoral head. In pincer impingement the posterior acetabulum is affected.
Pain occurs with flexion activities and is generally worse with low sitting. Restoration of muscle balance around the hip is the non-operative treatment of choice. Where bony deformity is present, typically flattening of the femoral neck (pistol grip deformity) or a change to the normally spherical contour of the femoral head, surgery may be required. Arthroscopic debridement and contouring the femoral head have been described, but excessive remodeling may risk fracture (Mardones et al., 2005).
Symptoms of both impingement and anterior labral tear may respond to correction of movement impairment/dysfunction. Anterior femoral glide (Sahrmann, 2002) is the most common impairment and occurs because the posteriorly placed hip muscles fail to posteriorly glide the femoral head during flexion. Pain occurs in the groin during flexion movements and prolonged sitting. The condition is seen in those who use hip hyperextension during their sport (dancers, yoga) or those who have an inflexible flatback and compensate by extending the hip instead. The key test is monitoring the position of the greater trochanter during active hip flexion (Fig. 8.24). As the hip is actively flexed or extended, the greater trochanter should remain in a neutral position. Where anterior glide occurs, the trochanter moves forwards (glide) and inwards (medial rotation). The condition is associated with a swayback posture (hip extended when standing), hyperpronation of the feet and medial rotation of the femur. The TFL muscle tends to be dominant over the gluteus medius in single leg standing and hip abduction, and the hamstrings dominant over the gluteus maximus during hip extension. Underactivity of the iliopsoas during flexion and the gluteal muscles during hip extension has been shown to increase anterior hip joint force (Lewis, Sahrmann and Moran, 2007). Comparison of the iliopsoas to rectus femoris/tensor fascia lata/sartorius during hip flexion and the gluteal muscles to the hamstrings during hip extension has shown the iliopsoas and gluteal muscles to be the most important in reducing anterior hip force during flexion−extension, respectively (Lewis Sahrmann and Moran, 2009).

Keypoint
Preferential recruitment of the iliopsoas during hip flexion and the gluteal muscles during hip extension reduces excessive forces acting on the anterior hip.
Rehabilitation of anterior glide includes exercises to encourage posterior and inferior glide of the femoral head. Passive motion is four point kneeling (quadruped) and rocking back towards the heels is used together with the side-lying clamshell action and hip abduction with lateral femoral rotation. Resting positions should avoid exacerbation of the condition and so swayback posture is corrected, and crossing the legs (medial rotation) avoided. Where night pain occurs the athlete should place a pillow between their knees in lying on the side to avoid medial rotation of the hip. Key exercises during rehabilitation of anterior impingement are shown in Table 8.7.
Table 8.7 Key exercises used in the management of anterior hip impingement
Reproduced from Sahrmann (2002).
The young athlete
Pain and limitation of movement in the hip in children should always be treated with caution. The extreme forces placed on the hip by weight bearing, combined with osseous and vascular changes occurring about the joint during adolescence, can lead to a variety of serious orthopaedic conditions.
The blood supply to the femoral head may be compromised in the very young. From birth until the age of 4 years blood reaches the femoral head via the metaphysis. From the age of 8 years, vessels through the ligamentum teres supply the head. Between these two periods the lateral epiphyseal vessels are the only source of blood to the femoral head (Cyriax, 1982). In addition, the upper femoral epiphysis does not fuse with the shaft until about 20 years of age.
Perthes’ disease
Persistent hip or groin pain and/or a limp in young males (4–12 years) may be the result of Perthes’ disease, an avascular necrosis (osteochondrosis) of the femoral head. The bony nucleus of the epiphysis becomes necrosed. The upper surface of the femoral head flattens and the epiphyseal line widens, altering the biomechanical alignment of the joint. When the bone is revascularized it hardens again, leaving a permanent deformity. Objective examination often reveals slight limitation of all hip movements with protective spasm. The condition may be precipitated by joint effusion at the hip following trauma, or a non-specific synovitis (Apley and Solomon, 1989).
Slipped capital femoral epiphyses
Trauma, or more usually simply weight bearing, in the young athlete (10–20 years) may result in slipping of the upper (capital) femoral epiphysis. The condition is more common in tall adolescents who have shown a rapid increase in height, and in the obese individual. In these two cases hormone imbalance has been suggested, in the first case an excess of growth hormone and in the second an excess of sex hormone (Reid, 1992).
Pain is usually felt in the hip or knee, and may begin simply as a diffuse ache to the knee alone. The epiphyseal junction may soften and, with weight bearing or trauma, may cause the head of the femur to slip on the neck, usually downwards and backwards. Slippage may compromise the blood flow to the femoral head through the neck, causing osteonecrosis with sclerosis and femoral head collapse. If left, the slipped epiphyses will fuse to the femoral neck in the abnormal position.
Objective examination often reveals limitation of flexion, abduction and medial rotation (the athlete is unable to touch the abdomen with the thigh). The leg is often rested in lateral rotation, and the gait pattern is antalgic. The condition is classified as stable when the patient is able to walk and unstable when the patient is unable to walk even with crutches.
Leg shortening up to 2 cm is common, and radiographs reveal widening and a ‘woolly’ appearance of the epiphyseal plate. On the x-ray, a line traced along the superior aspect of the femoral neck will reveal a step deformity (Fig. 8.25). The line remains superior to the head rather than passing directly through it (Trethowan’s sign).

Treatment is through surgical pinning rather than reduction. In a study of 240 patients, 21 were found to have osteonecrosis following unstable slipped capital femoral epiphysis while none were found from the stable group (Tokmakova, Stanton and Mason, 2003). Osteonecrosis was found to be more likely in those treated with multiple pins rather than a single pin, and the risk of osteonecrosis increased where reduction of an unstable slippage was performed.
Capsular tightening
Inflammation within the hip joint leads to the characteristic capsular pattern of marked limitation of flexion and medial rotation with some limitation of abduction. Adduction and lateral rotation are generally full (Cyriax and Cyriax, 1983). Initially, the synovium becomes inflamed, giving synovitis. Pain is from chemical stimulation of sensory nerve endings within the synovium and is often dull and throbbing in nature, being worse at night and at rest. If the synovitis does not resolve, swelling causes capsular pain by mechanically stretching nerve endings between the collagen fibres of the capsule. Eventually, secondary capsular fibrosis occurs, leading to capsular tightening and deformity. When pain and inflammation abate, the capsular tightening and associated loss of muscle stretch and strength leave the patient with hip dysfunction.
Capsular tightening will respond to mobilization procedures and later to stretching exercises. Hip flexion may be stretched using the Thomas test as an exercise. The patient lies supine with the popliteal area of the knees over the couch end. The unaffected leg is straight and hangs below couch level, while the knee and hip of the affected side are flexed to chest level. Hip extension may be promoted with the modified lunge described above.
Treatment note 8.2 Manual therapy techniques to the hip
The hip is a joint which responds well to manual therapy, but as the largest joint in the body, treatment can be difficult. In sports especially it is common to have a very large sportsman such as a rugby player and a very small therapist. The answer is to use leverage and body position and a variety of seatbelt techniques to reduce the stress on the therapist.
Quadrant test
The flexion/adduction or quadrant test (Maitland, 1986) is a useful test to assess the surface of the hip joint. However, the test requires that the therapist take the weight of the whole leg which, in the case of a large athlete, may be considerable. To make this test more manageable, the therapist should link the fingers over the patient’s knee (Fig. 8.26) and rest the far forearm along the patient’s calf. The couch should be just below hip level to allow the therapist to lean over the hip as the flexion/adduction force is applied. In this position a longitudinal force (axial compression) may be applied as the therapist flexes the knee slightly, and the body and forearms may be twisted to medially rotate the joint to increase the contact area of the joint.

Lateral gliding
A lateral gliding (transverse) accessory movement is imposed on the joint by modifying the grip used in the quadrant test (Fig. 8.27). The interlinked hands now grip around the patient’s thigh (use a towel to protect the skin) and the side of the patient’s femur rests on the therapist’s chest. The action is to distract the joint using the therapist’s body sway rather than arm strength. The movement should come from a slight softening of the therapist’s knees together with trunk movement, rather than trunk movement alone.

Lateral glide using seatbelt
The lateral gliding motion may be increased by using a seatbelt or webbing strap. The patient is in crook (hook) lying and a belt is fastened around the thigh and around the therapist’s hip at the level of the ischial tuberosities (Fig. 8.28). The femur is stabilized by resting it against the therapist’s chest and gripping around the knee with the hand. The degree of lateral glide may be assessed by palpating with the right hand. The lateral glide force is produced by the therapist leaning back slightly and softening the knee.

Longitudinal distraction (hip traction)
Hip traction is one of the most relieving mobilizations for the hip joint, where capsular limitation is present. The patient is in supine and the couch positioned below the therapist (Fig. 8.29), and the therapist takes up a stride standing position. A seatbelt is wound around the patient’s ankle in a figure of eight – the patient’s sock may be left on to protect the skin from abrasion. The belt passes around the therapist’s lower waist and the tension is taken up (Fig. 8.30). The hip is positioned in its loose pack position (flexion, abduction, lateral rotation) and the distraction force is imposed by the therapist leaning back. Either an oscillation or continuous traction may be used.


Hip pointer
The relatively unprotected iliac crest is vulnerable to direct blows from any hard object, be it a hockey ball, boot or another player’s head. Contusion is often persistent, especially if the periosteum is affected, and the condition is described as a ‘hip pointer’. The pain from the injury is so severe that the trunk is flexed to the affected side. The athlete is often unable to take a breath and may panic.
Following reassurance, the iliac crest is examined and usually reveals dramatic pain but little bruising or swelling. The abdominal muscles are often rigid and the hips pulled into flexion. After 24–48 hours more extensive bruising appears and local tenderness may last for weeks. A raised area may persist for many months. Ice may be used initially to relieve pain, and the area padded when the athlete resumes sport.
Clicking hip syndrome
Clicking or snapping hip can occur to repeated flexion and extension movements. The condition is common in dancers and young athletes, and is usually painless. However, it is of obvious concern to the athlete as in some cases the sound is loud enough for others to hear.
There are two main types of clicking hip, internal and external (Reid, 1992). Although there have been many proposed causes of this condition, one of the most common causes of internal clicking hip is the suction phenomenon. This can occur during exercises such as sit-ups and requires reassurance rather than treatment. Alternative causes include tight ligaments and tendons passing over bony prominences.
Definition
The suction phenomenon is a result of pressure changes within the synovial fluid of a joint. As a joint moves, positive and negative pressures are created within the fluid. As negative pressure (suction) collapses rapidly, air bubbles are sucked into the fluid giving a soft click.
External clicking hip is usually a result of the gluteus maximus tendon clicking over the greater trochanter, or the iliotibial band clicking over the greater trochanter. Sometimes the click can be reproduced during examination by flexing and extending the hip in adduction, in which case tight abductors are a contributory factor. The Ober manoeuvre is often positive in these cases.
If the condition is painful, treatment designed to reduce local inflammation may be required. In painless instances, stretching of the ITB and hip abductors can help. The athlete begins in a side-lying position with the affected leg uppermost. The upper leg is abducted, and hip hitching is performed to shorten the leg (lateral tilt of the pelvis). The pelvic fixation is maintained as the upper leg is lowered into adduction.
Apley A.G., Solomon L. Concise System of Orthopaedics and Fractures. Oxford: Butterworth-Heinemann; 1989.
Arnason R., Andersen T., Holme I., et al. Prevention of hamstring strains in elite soccer: an intervention study. Scandinavian Journal of Medicine and Science in Sports. 2008;18:40-48.
Borley N.R. Clinical Surface Anatomy. London: Manson Publishing; 1997.
Brughelli M., Nosaka K., Cronin J. Application of eccentric exercise on an Australian rules football player with recurrent hamstring injuries. Physical Therapy in Sport. 2009. In press
Burkett L.N. Causative factors in hamstring strains. Medicine and Science in Sports and Exercise. 1970;2:39-42.
Burkett L.N. Investigation into hamstring strains: the case of the hybrid muscle. American Journal of Sports Medicine. 1975;3:228-231.
Burnie J., Brodie D.A. Isokinetic measurement in preadolescent males. International Journal of Sports Medicine. 1986;7:205-209.
Burnie J., Brodie D.A. Isokinetics in the assessment of rehabilitation: a case report. Clinical Biomechanics. 1986;1:140-146.
Cailliet R. Soft Tissue Pain and Disability. Philadelphia: F.A. Davis; 1983.
Choi H., McCartney M., Best T. Treatment of osteitis pubis and osteomyelitis of the pubic symphysis in athletes: A systematic review. British Journal of Sports Medicine. 2008.
Clark R., Bryant A., Culgan J., Hartley B. The effects of hamstring strength training on dynamic jumping performance and isokinetic strength parameters. Physical therapy in sport. 2005;6:67-73.
Cyriax J.. eighth ed Textbook of Orthopaedic Medicine vol. 1 London: Baillière Tindall, 1982.
Cyriax J.H., Cyriax P.J. Illustrated Manual of Orthopaedic Medicine. London: Butterworth-Heinemann; 1983.
Estwanik J.J., McAlister J.A. Contusions and the formation of myositis ossificans. Physician and Sports Medicine. 1990;18(4):52-64.
Fagerson T. Hip pathologies: diagnosis and intervention. In: Magee D.J., Zachazewshi J.E., Quillen W.S., editors. Pathology and Intervention in Musculoskeletal Rehabilitation. St Louis, MO: Saunders-Elsevier, 2009.
Ferguson S.J., Bryant J.T., Ganz R., Ito K. The influence of the acetabular labrum on hip joint cartilage consolidation. Journal of Biomechanics. 2000;33:953-960.
Foreman T.K., Addy T., Baker S., et al. Prospective studies into the causation of hamstring injuries in sport: A systematic review. Physical Therapy in Sport. 2006;7:101-109.
Ganz R., Parvizi J., Beck M., et al. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clinical Orthopaedics and Related Research. 2003;417:112-120.
Grace J.N., Shives T.C., Coventry M.B. Wedge resection of the symphysis pubis for the treatment of osteitis pubis. Journal of Bone and Joint Surgery. 1989;71A:358-364.
Gunn C.C. Treatment of Chronic Pain. Edinburgh: Churchill Livingstone; 1996.
Gunn C.C. The Gunn Approach to the Treatment of Chronic Pain. London: Course notes, Westminster Hospital; 2000.
Haslam R. A comparison of acupuncture with advice and exercises on the symptomatic treatment of osteoarthritis of the hip: a randomised controlled trial. Acupuncture in Medicine. 2001;19:19-26.
Hitomi Y., Sumiko T., George W., et al. Seven skeletal muscles rich in slow muscle fibers may function to sustain neutral position in the rodent hindlimb. Comparative Biochemisty and Physiology. 2004;140(1):45-50.
Hoeksma H.L., Dekker J., Ronday K., et al. Comparison of manual therapy and exercise therapy in osteoarthritis of the hip: a randomized clinical trial. Arthritis and Rheumatism. 2004;51:722-729.
Jackson D.W., Feagin J.A. Quadriceps contusions in young athletes: relation of severity of injury to treatment and prognosis. Journal of Bone and Joint Surgery. 1973;55A(1):95-105.
Kannus P. Hamstring/quadriceps strength ratios in knees with medial collateral ligament insufficiency. Journal of Sports Medicine and Physical Fitness. 1989;29(2):194-198.
Kim Y.T., Azuma H. The nerve endings of the acetabular labrum. Clinical Orthopaedics. 1995;320:176-181.
Kornberg C., Lew P. The effect of stretching neural structures on grade one hamstring injuries. Journal of Orthopaedic and Sports Physical Therapy. 1989;7(2):481-487.
Kurosawa H., Nakasita K., Saski S., Takeda S. Complete avulsion of the hamstring tendons from the ischeal tuberosity: a report of two cases sustained in judo. British Journal of Sports Medicine. 1996;30:72-74.
LeBlanc K., LeBland K.A. Groin pain in athletes. Hernia. 2003;7:68-71.
Lewis C.L., Sahrmann, S.A. Acetabular labral tears. Physical Therapy. 2006;86(1):110-120.
Lewis C., Sahrmann S.A., Moran D.W. Anterior hip joint force increases with hip extension, decreased gluteal force, or decreased iliopsoas force. Journal of Biomechanics. 2007;40(16):3725-3731.
Lewis C., Sahrmann S.A., Moran D.W. Effect of position and alteration in synergist muscle force contribution on hip forces when performing hip strengthening exercises. Clinical Biomechanics. 2009;24(1):35-42.
Lloyd-Smith T.D., Clement D.B., McKenzie D.C. A survey of overuse and traumatic hip and pelvic injuries in athletes. Physician and Sports Medicine. 1985;13:131.
Magee D.J. Orthopedic Physical Assessment. Philadelphia: W.B. Saunders; 2002.
Magee D.J. Orthopedic physical assessment, fifth ed. St Louis. USA: Saunders-Elsevier; 2008.
Maitland G.D. Vertebral Manipulation, third ed. Oxford: Butterworth-Heinemann; 1986.
Mardones R.M., Gonzalez C., Chen Q., et al. Surgical treatment of femoroacetabular impingement: evaluation of the effect of the size of the resection. Journal of Bone and Joint Surgery (America). 2005;87:273-279.
McCarthy J.C., Noble P.C., Schuck M.R., et al. The role of labral lesions in development of early degenerative hip disease. Clinical Orthopaedics. 2001;393:25-37.
Norkin C.C., Levangie P.K. Joint Structure and Function, second ed. Philadelphia: F.A. Davis; 1992.
O’Connell M., Powell T., McCaffrey N. Symphyseal cleft injection in the diagnosis and treatment of osteitis pubis in athletes. American Roentgen Ray Society. 2002;179:955-959.
Oravo S., Kujala U.M. Rupture of the ischeal origin of the hamstring muscles. American Journal of Sports Medicine. 1995;23:702-705.
Palastanga N., Field D., Soames R. Anatomy and Human Movement, second ed. Oxford: Butterworth-Heinemann; 1994.
Pauli S., Willemsen P., Declerck K., et al. Osteomyelitis pubis versus osteitis pubis: a case presentation and review of the literature. British Journal of Sports Medicine. 2002;36:71-73.
Puranen J., Orava S. The hamstring syndrome: a new diagnosis of gluteal sciatic pain. American Journal of Sports Medicine. 1988;16(5):517-521.
Read M.T. A Practical Guide to Sports Injuries. Oxford: Butterworth-Heinemann; 2000.
Reid D.C. Sports Injury Assessment and Rehabilitation. London: Churchill Livingstone; 1992.
Rold J.F., Rold B.A. Pubis stress symphysitis in a female distance runner. Physician and Sports Medicine. 1986;14(June):61-65.
Ruwe P.A., Gage J.R., Ozonoff M.B., Deluca P.A. Clinical determination of femoral anteversion: a comparison of established techniques. Journal of Bone and Joint Surgery (Am). 1992;74:820.
Sahrmann S.A. Diagnosis and Treatment of Movement Impairment Syndromes. St Louis: Mosby; 2002.
Santori N., Villar R.N. Acetabular labral tears: result of arthroscopic partial limbectomy. Arthroscopy. 2000;16:11-15.
Stanton P., Purdam C. Hamstring injuries in sprinting: the role of eccentric exercise. Journal of Orthopaedic and Sports Physical Therapy. 1989;10(9):343-349.
Sutton G. Hamstrung by hamstring strains: a review of the literature. Journal of Orthopaedic and Sports Physical Therapy. 1984;5(4):184-195.
Tokmakova K., Stanton R.P., Mason D. Factors influencing the development of osteonecrosis in patients treated for slipped capital femoral epiphysis. Journal of Bone and Joint Surgery (America). 2003;85:798-801.
Topol G., Reeves K., Hassanein K. Efficacy of dextrose prolotherapy in elite male kicking sport athletes with chronic groin pain. Arch Phys Med Rehab. 2005;86:697-702.
Van Baar M.E., Assendelft W.J., Dekker J., et al. The effectiveness of exercise therapy in patients with osteoarthritis of the hip or knee: a randomized controlled trial. Journal of Rheumatology. 1998;25:2432-2439.
Veselko M., Smrkolj V. Avulsion of the anterior superior iliac spine in athletes: case reports. Journal of Trauma. 1994;36:444-446.
Wollin M., Lovell G. Osteitis pubis in four young football players: A case series demonstrating successful rehabilitation. Physical Therapy in Sport. 2006:153-160.