CHAPTER 11 The ankle
Approximately 14% of all sports injuries are sprains to the ankle, representing one ankle injury each season for every 17 participants. In high risk sports, such as jumping and running, this percentage is even higher, at 25% of all lost-time injuries (Reid, 1992). Ankle sprain has been shown to be 2.4 times more common in the dominant leg, and to have a high (73.5%) prevalence of recurrence (Yeung et al., 1994).
The joint mechanics of the ankle and foot have been described in Chapter 7. The ankle joint is the articulation between the trochlear surface of the talus and the distal ends of the tibia and fibula. The fibula may support 15–20% of the body weight (Lambert, 1971), with the fibula moving downwards and laterally during the stance phase of running to deepen the ankle mortice and enhance stability. This fibular motion creates tension in the interosseous membrane and tibiofibular ligament to provide some shock attenuation. Loss of this mechanism through tibiofibular disruption greatly affects the ankle joint, with a 1–2 mm lateral shift of the fibula increasing joint forces by as much as 40% (Reid, 1992).
Keypoint
The fibula can support up to 1/5 of the bodyweight and moves during the stance phase of running to deepen the ankle mortice and enhance ankle stability.
The ankle is subjected to considerable compression forces during sport (Fig. 11.1). Compression forces as high as five times body weight have been calculated during walking and up to 13 times body weight during running (Burdett, 1982).
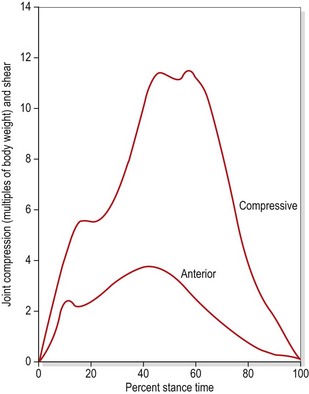
Figure 11.1 Compression forces on the talus during running.
From Burdett, R.G. (1982) Forces predicted at the ankle during running. Medicine and Science in Sports and Exercise, 14, 308. With permission.
Collateral ligaments
The joint is strengthened by a variety of ligaments, the collaterals being the most important from the point of view of injury. Both medial and lateral collateral ligaments travel from the malleoli, and have bands attaching to the calcaneus and talus.
The medial (deltoid) ligament (Fig. 11.2A) is triangular in shape. Its deep portion may be divided into anterior and posterior tibiotalar bands. The more superficial part is split into tibionavicular and tibiocalcaneal portions, which attach in turn to the spring ligament. The lateral ligament (Fig. 11.2B) is composed of three separate components, and is somewhat weaker than its medial counterpart. The anterior talofibular (ATF) ligament is a flat band 2–5 mm thick and 10–12 mm long which travels from the anterior tip of the lateral malleolus to the neck of the talus, and may be considered the primary stabilizer of the ankle joint (Palastanga, Field and Soames, 1989). The posterior talofibular (PTF) ligament travels almost horizontally from the fossa on the bottom of the lateral malleolus to the posterior surface of the talus. Lying between the ATF and PTF ligaments is the calcaneofibular ligament, arising from the front of the lateral malleolus to pass down and back to attach onto the lateral surface of the calcaneum. The role of the collateral ligaments in maintaining talocrural stability is summarized in Table 11.1.
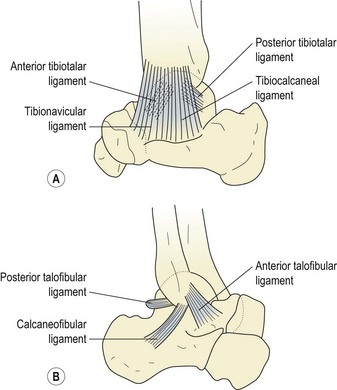
Table 11.1 Role of the collateral ligaments in ankle stability
| Movement | Controlled by |
|---|---|
| Abduction of talus | Tibiocalcaneal and tibionavicular bands |
| Adduction of talus | Calcaneofibular ligament |
| Plantarflexion | ATF ligament and anterior tibiotalar band |
| Dorsiflexion | Posterior tibiotalar band and PTF ligament |
| External rotation of talus | Anterior tibiotalar and tibionavicular bands |
| Internal rotation of talus | As above with ATF ligament |
Adapted from Palastanga, Field and Soames (1989).
Injury
The most common injury to the ankle is damage to the ATF ligament with or without involvement of the peroneus brevis. The subtaloid and mid-tarsal joints may be involved, but will be dealt with separately for clarity. The typical history of ankle injury is one of inversion, sometimes coupled with plantarflexion. The athlete ‘goes over’ on the ankle, usually on an uneven surface. One of three grades of ligament injury may occur.
Keypoint
The anterior talofibular (ATF) ligament is 2–5 mm thick and 10–12 mm long, approximately the width of the index finger. Its fibres run roughly parallel to the sole of the foot. Injury to the ATF is the most common sports injury affecting the ankle.
Swelling
There is usually an egg-shaped swelling in front of, and around, the lateral malleolus. When viewed from behind, the definition of the Achilles tendon is a good indicator of severity of injury (Reid, 1992). With more severe injuries (grade III) the definition of the Achilles tendon is lost due to excessive bleeding into the joint (Fig. 11.3).
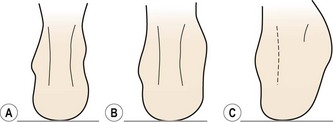
Figure 11.3 Assessing severity of ankle injury from swelling. (A) Normal joint. Contour of Achilles tendon well defined. (B) Grade I/II injury. Clear swelling but Achilles tendon outline still visible. (C) Grade III injury. Profuse swelling obscures outline of Achilles tendon.
Objective measurement of swelling is made using the figure-of-eight measure, a valid and reliable measure (Mawdsley, Hoy and Eerwin, 2000; Rohner-Spengler, Mannion and Babst, 2007). For this test the end of a tape measure is placed on the anterolateral aspect of the ankle midway between the tibialis anterior tendon and the lateral malleolus. The tape is passed medially over the dorsum of the foot to the tuberosity of navicular and then beneath the plantar aspect proximal to the tubercle of the 5th metatarsal. The tape passes medially once more to rest distal to the medial malleous and is pulled across the Achilles back to the starting point.
Manual evaluation
The lateral malleolus should be gently palpated to assess if bone pain is present; if it is, an x-ray may be required (see below). If palpation reveals tenderness below, rather than over, the lateral malleolus and the athlete is able to bear weight, there is a 97% probability of soft tissue injury alone (Vargish and Clarke, 1983). Any fracture that is missed by this type of close palpation is likely to be an avulsion or non-displaced hairline type that will respond favourably to management as a sprain (Garrick and Webb, 1990).
Stress tests to the ankle are useful to assess the degree of instability in the subacute phase, and to give a differential diagnosis. Acute injuries may be exacerbated by full range motion with overpressure. The capsule of the ankle joint itself is assessed by passive dorsiflexion and plantarflexion only, the capsular pattern presenting as a greater limitation of plantarflexion. However, as the ankle ligaments span the subtaloid and mid-tarsal joints, inversion/eversion and adduction/abduction are also included in ankle joint examination.
The ATF ligament is placed on maximum stretch by passive inversion, plantarflexion, and adduction. The heel is held with the cupped hand and the subtaloid joint inverted. The opposite hand grasps the forefoot from above and swings it into plantarflexion and adduction. In addition, anterior glide of the talus on the tibia should be assessed with the foot in a neutral position. The heel is again held in the cupped hand, but this time the palm of the opposite hand is over the anterior aspect of the lower tibia. The calcaneus and talus are pulled forward as the tibia is pushed back. Movements are compared with that of the uninjured side for range and quality.
Keypoint
The ATF ligament is tested by passive inversion, plantarflexion and adduction. The athlete’s heel is held with the cupped hand and the heel is twisted inwards. The opposite hand grasps the forefoot from above and draws down and in.
The calcaneocuboid ligament is stressed by combined supination/adduction and the calcaneofibular ligament by inversion in a neutral position. The medial collateral ligament is stressed by combined plantarflexion/eversion/abduction (anterior fibres) or eversion alone (middle fibres). Resisted eversion will not be painful unless the peronei are affected (see below).
Ligamentous laxity may be assessed using the anterior draw test when acute inflammation has subsided. The patient’s foot is placed in slight (10−15°) plantarflexion and the heel is gripped with the therapist’s cupped hand, while the other hand stabilizes the lower tibia and fibula. The heel is drawn forwards against an opposite force pressing the tibia backwards and the amount of anterior movement is noted if the talus moves out of the ankle mortice. The test determines the integrity of both the anterior talofibular ligament and the calcaneofibular ligament and has been shown to be valid when compared to surgical observation (van Dijk et al., 1996).
Keypoint
The anterior draw test assesses ligamentous laxity, and is most useful when acute inflammation and muscle spasm have subsided.
Following severe ankle sprain or fracture, a bony link may form between the tibia and fibula (tibiofibular synostosis). Typically, pain occurs after an injury, and increases during vigorous activity, mimicking stress fracture. Pain is most severe during the push-off action of running and jumping, and dorsiflexion is often limited to 90°, mimicking impingement pain (see below). The synostosis is revealed by x-ray and removed surgically (Flandry and Sanders, 1987).
X-ray
Accurate physical examination will usually give sufficient information to preclude fracture, making x-ray unnecessary in most cases. Only 15% of patients suffering an acute ankle injury may have a fracture, and the Ottawa Ankle Rules provide a highly accurate clinical decision guide in this respect (Stiell et al., 1994). The rules state:
A poster describing the rules is free to download at www.ohri.ca/emerg/cdr/docs/cdr_ankle_poster.pdf.
In a systematic review of 27 studies (15 581 patients) Bachmann et al. (2003) found the sensitivity of the Ottawa Ankle Rules to be almost 100% and claimed that their application would reduce the number of unnecessary radiographs by 30−40%.
Fractures associated with ankle injuries
Several fractures may occur at the time of injury, and can go unnoticed unless a thorough examination is carried out. Often these fractures only become apparent during rehabilitation when swelling begins to subside. It falls on the astute therapist to question why rehabilitation is not progressing normally and to refer for further investigation, which may include x ray, MRI or CT scan.
Pott’s fracture
This is a fracture affecting either the lateral or medial malleolus. To palpation pain is located close to the malleolus itself rather than in the ligament tissue. The subject usually finds it difficult to bear weight in the clinic, and will not have been able to bear weight immediately after injury. Where the ankle mortice has been compromised, internal fixation is usually required. Hairline fractures, stable fractures and those affecting the posterior aspect of the malleolus and/or involving less than 25% of the articular surface are normally managed conservatively.
Maisonneuve fracture
This is a spiral fracture of the fibula together with a tear of the distal tibiofibular syndesmosis and the interosseous membrane. The medial malleolus normally fractures and the deltoid ligament ruptures. The injury occurs only in high-impact activities and requires urgent surgical referral.
Osteochondral lesion of talar dome
This fracture is more common in cases where ankle sprain has occurred in the presence of a compression force such as landing from a single leg jump. The talar dome is compressed within the ankle mortise and may fracture at the superomedial corner particularly. The condition is normally not recognized at the time of injury, but presents as a dull persistent ache during rehabilitation. There will be persistent swelling with stiffness. The site can be palpated by plantar flexing the ankle to draw the talar dome forwards of the ankle mortise. Injury may be graded from (I) focal compression of the subchondral bone through to (IV) fully detached bone fragment. Treatment is by reduced weight bearing while maintaining motion to stimulate cartilage healing (Karlsson, 2007). Occasionally arthroscopic removal of the bone fragment may be required.
Avulsion fracture of 5th metatarsal base
The force which causes an acute lateral ligament injury is sometimes severe enough to pull (avulse) the peroneus brevis tendon away from its attachment to the 5th metatarsal. The avulsion fracture is usually treated conservatively.
Fracture of talar process
The lateral aspect of the talus, which normally articulates with the fibula and calcaneus, may fracture. Pain occurs over the bone area which is palpated anterior and inferior to the tip of the lateral malleolus. If the fracture is not displaced, simple immobilization is required. Where displacement is greater than 2 mm excision or internal fixation is generally required (Karlsson, 2007).
Fracture of calcaneus process
The anterior calcaneal process is palpated anterior to the sinus tarsi. This area is normally not tender in cases of lateral ligament injury, but where fracture has occurred tenderness is exquisite. The fracture may not be revealed by x-ray and can require MRI or CT scan. Again immobilization is required unless the fragment is displaced in which case excision may be called for.
Management of an ankle sprain
Immediate management consists of the PRICE protocol, with electrotherapy modalities as appropriate. Intermittent pneumatic compression (IPC) used in conjunction with cooling is effective. In the subacute phase, massage, especially finger kneading around the malleolus, is of value in preventing the development of pitting oedema. Transverse frictions may be used to encourage the development of a mobile scar, and may be used as a prelude to manipulation for scar tissue rupture in a chronic injury. Grade II and III injuries present with marked swelling and are protected non-weight bearing (severe injury) or preferably partial weight bearing with a compression bandage. Where minimal swelling indicates a grade I injury, an eversion strapping may be applied to protect the ligament from inversion stresses and to shorten it. A felt wedge is used beneath the heel to evert the subtaloid joint, and a U-shaped pad is placed over the submalleolar depressions to prevent pockets of oedema forming and to apply even compression when the ankle is strapped. Adhesive strapping is applied after skin preparation or underwrap, initially to lock the subtaloid joint and then to passively evert the foot. The athlete can then walk partial weight bearing in a well-supporting shoe.
Early mobility is essential to increase ligament strength and restore function. For grade I and II injuries, early mobilization has been shown to be more effective than immobilization. In a group of 82 patients with these grades of injury, 87% who were immobilized with a plastercast for 10 days still had pain after 3 weeks. This compared to 57% of those who received early mobilization in the form of an elastic strap for 2 days followed by a functional brace for 8 days (Eiff, Smith and Smith, 1994). Even grade III injuries (rupture) respond better to conservative treatment than surgery. Studies have shown 87% good and excellent results with conservative management compared to 60% for surgery of grade III injuries. In addition at 6 weeks post injury the surgical group had limited range of motion not seen in the conservative group (Kaikkonen, Kannus and Jarninen, 1996).
Non-weight bearing ankle exercise is instigated within the pain-free range, and fitness is maintained by general exercise. Strapping is replaced by a tubular elastic bandage as pain subsides.
Rehabilitation of the injured ankle
As with any joint, rehabilitation of the ankle aims at restoring mobility, strength and function (Table 11.2). With the ankle, however, of particular concern is the restoration of normal proprioception.
Table 11.2 Guidelines for rehabilitation of ankle sprain
| Immediate post-injury management |
| Initial rehabilitation (2–5 days after injury) |
| Intermediate rehabilitation (6–14 days) |
| Final rehabilitation (2–6 weeks) |
Resisted exercise using rubber powerbands is used for inversion, eversion, dorsiflexion and plantarflexion, together with combinations of these movements. Maximum repetitions are used to restore muscle endurance, while strength is developed using maximal resistance. Eversion movements are performed with the band placed over both forefeet. For other movements, one end of the band is placed around a table leg, and the other over the foot. Various thicknesses of band are used as the exercises are progressed.
Static stretching exercises include calf and Achilles tendon stretching (see above), and inversion/eversion movements applied manually by the athlete. The starting position for these latter movements is sitting with the injured leg crossed over the contralateral limb. The exercise mimics the stability test for the ligaments outlined above.
Partial, and then full weight-bearing exercises are used to develop strength in a closed kinetic chain position and to restore proprioception. In single leg standing (wall-bar support) trunk movements are performed to throw stress onto the ankle; in addition, exercises such as heel raising, toe lifts and inversion/eversion are performed. A balance beam (flamingo balance) is used, and again trunk and hip movements of the contralateral limb throw stress onto the injured ankle. The foot may be placed along the beam, or with the beam travelling transversely and only the toes supported. Intense muscle activity is seen around the ankle as the athlete attempts to maintain his or her balance. By varying the athlete’s footwear and performing the exercises in bare feet, the stresses imposed are altered.
A balance board with a single transverse rib is used for sagittal movements, and a longitudinal rib for frontal plane actions. A board with a domed central raise (wobble board or ankle disc) is used to combine movements for circumduction. In addition to trunk movements, actions such as throwing and catching while standing on the balance board are helpful as these take the athlete’s attention away from the ankle, and so are a progression in terms of skill. Performing balance board exercises blindfolded, and therefore eliminating visual input, has been shown to be effective at improving proprioception in the ankle (De Carlo and Talbot, 1986).
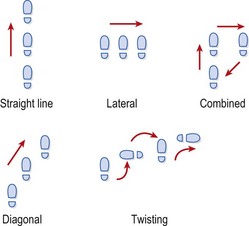
Running, hopping and jumping activities are all used, on varying surfaces including sand, grass and a mini-trampoline. Hopping direction is varied to alter the stress on the joint. Straight line hopping places an anteroposterior stress on the joint while lateral hopping imposes a mediolateral stress. Combined directions, diagonal hopping and twisting when hopping are all used to impose multiple stresses on the joint (Fig. 11.4). Running in a circle, figure-of-eight and on hills/cambers all change the stress on the ankle, and hopping and jumping develop power rather than strength.
Proprioception in the unstable ankle
The importance of proprioceptive training to prevent the development of chronic instability (giving way in normal usage) is of great importance. Freeman, Dean and Hanham (1965) compared ligament injuries to the foot and ankle treated by immobilization, ‘conventional’ physiotherapy, and proprioceptive training, which consisted of balance board exercises. After treatment, 7% of the proprioceptive group showed instability compared to 46% of those treated by other means. Balance ability was measured using a modified Rhomberg test, which assesses the ability to maintain single leg standing while the eyes are closed. Lentell, Katzman and Walters (1990) assessed the strength of the ankle musculature in 33 subjects with instability and found that there was no significant difference between the injured and uninjured sides. However, when balance ability was measured, the majority of subjects exhibited a deficit between the two extremities. Konradsen and Ravn (1990) measured the time taken for peroneal contraction to occur in response to a sudden inversion stress in chronically unstable ankles. Their results showed the peroneal reaction time to be prolonged with injured ankles (82 ms) compared to the uninjured side (65 ms), indicating a proprioceptive deficit. Karlsson and Andersson (1992) found similar results, quoting 84.5 ms and 81.6 ms for peroneus longus and peroneus brevis, respectively, for involved limbs compared to 68.8 and 69.2 for uninvolved.
Glencross and Thornton (1981) assessed joint position sense to plantarflexion and found significantly greater errors in the replication of the test position for injured ankles compared to uninjured controls. Lentell et al. (1995) measured the threshold of the detection of passive motion and found a significant difference (greater amount of inversion) between injured and uninjured sides.
Definition
Peroneal reaction time is the difference between the onset of a rapid inversion force acting on the ankle (mechanical joint displacement) and the initiation of peroneal muscle contraction to try to resist this force (physiological muscle splinting).
Although reflex control of the ankle through peroneal reaction time may be important, central nervous system (CNS) factors have also been shown to act. Konradsen, Voight and Hojsgaard (1997) showed that inversion stress sufficient to cause ligament damage occurred within 100 ms. Although the peroneal muscles may begin their contraction rapidly in response to such a stress (within 50–60 ms), it takes time for sufficient tension to build up to overcome the force of bodyweight. Such a force has been shown to require 170–180 ms to build to sufficient intensity, showing that the ankle musculature cannot react fast enough to protect the ankle from injury due to sudden inversion stress (Caulfield, 2000).
In the trunk, it has been shown that patients with chronic low back pain have lost the ability to anticipate the need for stability (Hodges and Richardson, 1996) and it seems that this anticipatory function may also be important in ankle stability. Dyhre-Poulsen, Simonsen and Voight (1991) measured EMG activity in the soleus and tibialis anterior in jumping activities and found that these muscles contracted before landing, and similar results have been found with the peroneal muscles in jumping tasks (Caulfield, 2000).
As the ankle ligaments and capsule are torn, articular nerve fibres are also likely to be damaged, leading to a partial deafferentiation of the joint. This, in turn, will decrease the athlete’s motor control and inhibit reflex stabilization of the foot and ankle. In addition, joint swelling has been shown to affect muscle control in the knee (Stokes and Young, 1984) and ankle (Petrik et al., 1996), and alteration in the motor programme provided by the CNS may occur (Caulfield, 2000).
Proprioceptive training should be incorporated into general rehabilitation training. Where chronic instability is seen, the modified Rhomberg Test or Star Excursion Balance Test (SEBT) (Table 11.3) may be used to monitor the degree of proprioceptive deficit. The modified Rhomberg test, although simpler to apply in the clinic, measures unidirectional stability, whereas the SEBT measures multidirectional stability. Progressive stability training has been shown to improve ankle stability measured on the SEBT (Rasool and George, 2007), the programme progressing from solid floor to soft mat with eyes open and then closed. A review of the effect of proprioceptive training on the ankle (Hughes and Rochester, 2008) concluded that muscle reaction time, kinaesthetic deficits and postural sway all improve with proprioceptive exercise. A sample ankle stability training protocol is shown in Box 11.1.
Table 11.3 Measurement of ankle stability
| Modified Rhomberg Test | Star Excursion Balance Test (SEBT) |
|---|---|
| The subject stands on their injured leg with their eyes open and hands by their sides. If they are able to maintain their balance for 5−10 seconds they are instructed to close their eyes. Body sway and loss of balance are noted. | The subject stands on their injured leg in the centre of a grid (star) marked with tape on the floor. Each arm of the grid extends at 45° increments from the centre. The subject reaches along each line as far as they can with their contralateral leg while maintaining balance. The distance of the reach is recorded for each limb of the grid and any asymmetry noted. |
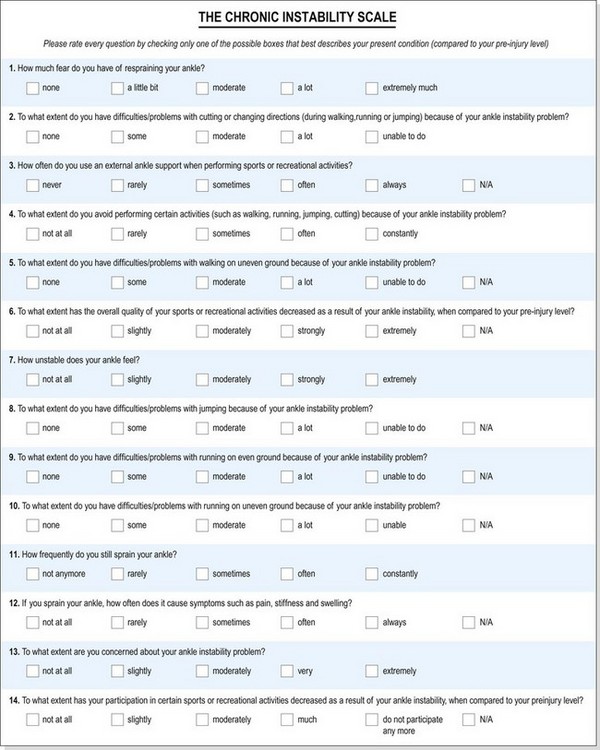
The multidimensional profile of patients suffering from chronic ankle stability may be assessed using the Chronic Ankle Instability Scale (CAIS), a valid and reliable questionnaire (Eechaute et al., 2008). The questionaire consists of 14 questions concerning daily activities, function and psychosocial factors (Fig. 11.5).
Ankle taping
Ankle taping may be used to reduce excessive inversion–eversion stress in the previously injured athlete, or as a preventive measure. Taping itself has traditionally been used, but semi-rigid orthoses are becoming increasingly popular. These allow dorsiflexion–plantarflexion but limit inversion–eversion and so should have a less detrimental effect on overall lower limb mechanics.
Orthoses have been shown to be as effective as taping at reducing inversion–eversion movement, but have the advantage that this support is more effectively maintained throughout training. Greene and Hillman (1990) compared several ankle orthotics with taping and found that after 20 minutes of exercise the taping revealed maximal losses of restriction while the orthoses demonstrated no mechanical failure. Rovere et al. (1988) showed ankle stabilizers to be more effective than taping at reducing ankle injuries. Surve et al. (1994) showed a lower incidence of ankle sprain and a reduced severity of injury in soccer players with a previous history of ankle injury who wore a semi-rigid ankle orthosis. No change in incidence of injury was seen in those without a previous history of injury.
In addition to support characteristics, the effect on lower limb mechanics is important. Taping has been shown to throw stress onto the forefoot as the foot compensates for the reduction of dorsiflexion in mid-stance in walking subjects (Carmines, Nunley and McElhaney, 1988). Where an ankle orthosis allows normal dorsiflexion, the forefoot is likely to receive less compensatory stress.
The combination of forefoot stress and loss of restriction capabilities may make the use of ankle orthoses preferable to taping in certain circumstances. The contribution of taping to proprioception, providing an increased skin stimulation to movement, may also be of importance. Restoration of full ankle function with a combination of strength and balance activities must always be the main consideration, with ankle supports used as an interim measure wherever possible.
Impingement syndromes
Repeated forced dorsiflexion, such as occurs with dismounts in gymnastics, jumps in ballet and especially soccer may cause anterior impingement of the talus on the tibia (anterior tibiotalar impingement), a condition described colloquially as ‘footballer’s ankle’. The synovium may be repeatedly trapped, becoming chronically swollen and hypertrophied. The condition may also occur secondary to a severe lateral ligament sprain if the distal aspect of the ATF ligament impinges on the talus. Pain occurs over the front of the ankle, and is exacerbated by dorsiflexion with overpressure. Radiographs may reveal talar osteophytes, but these may not actually contribute to the impingement.
Forced plantarflexion, for example repeated bag work in kick boxing, may cause posterior impingement giving pain over the back of the ankle without tenderness to the Achilles tendon. The area of impingement this time is the posterior talus and the tibia.
Both conditions show slight swelling and represent a repeated impaction of the joint surfaces leading to compression of the articular cartilage and subchondral bone. These structures do not show great sensitivity, and will not be the primary source of pain. Instead, pain must come from the periosteum, the joint capsule or, more likely, from chemical irritation and mechanical stress caused by the inflammatory response itself. Impingement syndromes respond to rest, anti-inflammatory modalities and training modification.
If the impingement force persists, an exostosis may form on the back or front of the lower tibia, depending on the type of stress involved.
Definition
An exostosis is a benign (non-harmful) growth of bone which occurs at the edge of a joint. It may occur through mechanical stimulation of the bone membrane (periosteum) through repeated microtrauma.
The exostosis may be up to 1 cm long in some cases (Donoghue: O’, 1976), and should this break off, it will float in the joint as a loose body. In cases where the exostosis causes symptoms, it should be surgically removed.
Rapid, forceful dorsiflexion, such as may occur in a fall onto the feet, can force the talus up with enough force to stress the distal tibiofibular ligament. The joint is tender to palpation within the sulcus between the tibia and fibula, and pain is elicited to passive dorsiflexion but not inversion or eversion. Treatment involves strapping the foot to limit dorsiflexion, and using a heel raise.
On the posterior aspect of the talus, the flexor hallucis longus travels in a small groove. If the bone lateral to this point is extended, it is called Stieda’s process. When this piece occurs as a separate bone (ossicle) attached to the talus by fibrous tissue, it is known as the os trigonum. Between 8 and 13% of the population have one of these bony configurations (Brodsky and Khalil, 1987) (Fig. 11.6). Three mechanisms have been proposed for the development of the os trigonum (Reid, 1992). The secondary ossification centre in the region may fail to fuse, or repeated trauma (impingement) may cause a stress fracture. An acute fracture may also ensue following forced plantarflexion with or without avulsion of the posterior band of the lateral ligament (Cedell, 1974).
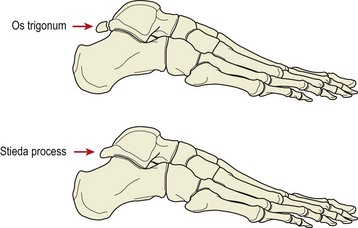
Figure 11.6 Lateral view of the ankle, showing the os trigonum and Stieda’s process.
From Brodsky, A.E. and Khalil, M.A. (1987) Talar compression syndrome. Foot and Ankle, 7, 338–344. With permission.
Repeated plantarflexion may compress the os trigonum and give impingement pain, palpable over the posterolateral talus between the Achilles tendon and the peroneal tendons. If symptoms fail to settle with conservative management, surgical removal of the ossicle may be called for. This is often performed with release of the adjacent tendon sheath of flexor hallucis longus.
Tendinopathy in association with the malleoli
Peroneal muscles
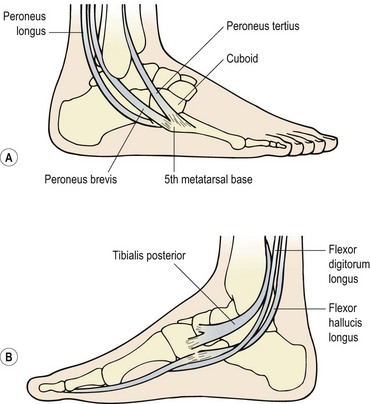
The tendons of peroneus longus and brevis pass around the lateral malleolus, while those of tibialis posterior, flexor digitorum longus and flexor hallucis longus pass around the medial malleolus (Fig. 11.7). Any of the tendons, their sheaths or their retaining retinacula may be inflamed or injured.
One complication of ankle sprain is a strain or avulsion of the peroneus brevis as it attaches to the base of the fifth metatarsal (see above). There may be local bruising, and pain is reproduced by resisted eversion. Point tenderness, proximal to the base of the fifth metatarsal, indicates the tendon, while bone pain may indicate avulsion. Radiographs are required to differentiate avulsion from a fracture to the fifth metatarsal itself (Jones fracture). Treatment of peroneus brevis strain is similar to that of an ankle injury, with frictions performed to the tendon while the foot is inverted and exercises to restore strength and flexibility of the peroneus brevis. Where swelling has occurred over the peroneus brevis insertion, it may spread to the joints formed by the cuboid bone, and mobilization of this bone may be required. Complete avulsion of the tendon may require immobilization for 1 or 2 weeks (Karlsson, 2007).
Keypoint
Following ankle sprain, the peroneus brevis muscle and its attachment to the base of the 5th metatarsal should be examined. In addition, the mobility of the cuboid bone should be checked, to exclude involvement of either of these structures.
Peroneal tendon dislocation may occur if the tip of the lateral malleolus is fractured with forced dorsiflexion (skiing) or a direct blow (soccer). Occasionally, severe inversion injury may rupture the peroneal retinaculum and allow the tendons to sublux or dislocate forwards over the fibula with resisted dorsiflexion and eversion. Local pain is present, and a ‘snapping’ sensation is felt as the tendons move over the bone. Surgical management is required, with several procedures being performed to re-establish the anatomy of the region. Re-attachment of the retinaculum, deepening of the peroneal groove, and placing the peroneal tendons under the calcaneofibular ligament have been variously described (Martens, Noyez and Mulier, 1986; Apley and Solomon, 1993).
Flexor hallucis longus
The flexor hallucis longus (FHL) passes behind the medial malleolus in a separate tendon sheath, which runs along the anterior aspect of the talus. The sheath passes between the medial and lateral tubercles of the talus, under the sustentaculum tali, and beneath the flexor retinaculum. The fibro-osseous tunnel so formed predisposes the tendon to mechanical irritation.
Pain may occur to resisted hallux flexion, with tenderness lying medial to the Achilles tendon. Pain is usually noticeable during the push-off phase of walking and running. A fusiform swelling and thickening of the tendon may occur in dancers with repeated point work. Eventually, the thickening may interfere with the movement of the tendon within its sheath giving rise to ‘trigger toe’ (Sammarco and Miller, 1979).
Tibialis posterior
The tibialis posterior tendon passes in a groove around and beneath the medial malleolus, the latter structure acting as a pulley. During pronation, the tendon is pressed onto the underlying bone of the groove, and in athletes who hyperpronate during the stance phase, tendon or tendon sheath pathology may occur. Tenderness, swelling and/or crepitus is noted in the local area along the tendon sheath. Resisted plantarflexion and inversion may cause pain and will cause the tendon to stand out making palpation easier.
Tarsal tunnel syndrome
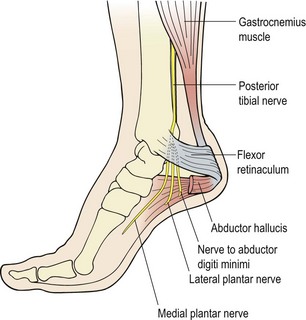
The tarsal tunnel is formed by the medial malleolus, calcaneus and talus on one side and the flexor retinaculum and medial collateral (deltoid) ligament on the other (Fig. 11.8). It begins approximately 2–3 cm proximal to the medial malleolus, and through it travels the posterior tibial nerve. The tunnel ends where the medial and lateral plantar nerves enter the abductor hallucis.
The tunnel may be restricted anatomically by tightness in the fascia and retinacula which normally result from trauma or overuse and the buildup of scar tissue. Increased pronation and a valgus (outwardly tilted) heel will tighten the flexor retinaculum and make the condition more likely. Following fracture of the calcaneum, tarsal tunnel syndrome may occur in as many as 10% of cases, as a result of either bony impingement or tightness of the cast (Reid, 1992). On occasion, irritation of training shoes may also give a similar clinical picture.
The most common symptom is burning and loss of sensation in the plantar aspect of the foot which is worse with activity and better for rest. The big toe is the most common area of complaint. Nerve conduction tests to the abductor hallucis (and abductor digiti minimi) confirm the diagnosis (Fu, Delisa and Kraft, 1980).
Treatment is by correction of excessive pronation and rearfoot valgus together with modification of footwear. Soft tissue mobilization and stretching may also be needed. Resistant cases may require surgical decompression.
Subtaloid joint
The subtaloid joint (STJ) (Fig. 11.9) has a thin capsule strengthened by the medial, posterior and lateral talocalcaneal ligaments. The joint cavity is isolated from that of the ankle and mid-tarsal joints, and its stability is largely maintained by the interosseous talocalcanean ligament running from the sinus tarsi to the talus.
Subtaloid mobility is often reduced following ankle sprain or fracture of the calcaneus from a fall onto the heel. Movement may also be reduced by impaction when jumping on a hard surface in inadequate footwear. The lack of mobility sometimes goes unnoticed, unless the patient is assessed by a physiotherapist.
Manual assessment and mobilization of accessory movements may be performed with the patient in a supine-lying position, with the heel over the couch end. Initially, the therapist grips around the distal part of the patient’s leg with one hand pressing the leg onto the couch. The therapist’s forefingers grip the talus and the calcaneum is cupped in the opposite hand (Fig. 11.10A). The calcaneum is then moved on the fixed talus. Releasing the talus, both talus and calcaneum are moved together on the fixed lower leg. Gross subtaloid joint movement may be performed by cupping the heel in both hands and performing forceful inversion/eversion actions (Fig. 11.10B).

Figure 11.10 Manual therapy of the subtaloid joint. (A) Stabilize lower leg and move talus. (B) Gross subtalar movement. (C, D) Distraction and gliding.
Some distraction may be given to the STJ in supine with one hand cupping the calcaneum laterally and applying a caudal force while the other hand stabilizes the dorsomedial aspect of the mid-foot (Fig. 11.10C). In the prone position, with the patient’s foot slightly plantarflexed, and the toes over the couch end, a distraction force may be imparted by pushing caudally with the heel of the hand onto the posterior aspect of the calcaneus near the Achilles tendon insertion (Fig. 11.10D). Following injury, rearfoot position should be assessed as posting may be required.
Mid-tarsal joint
The mid-tarsal joint (see Fig. 11.9) is composed of the calcaneal cuboid joint (lateral), and the talocalcaneonavicular joint (medial). Four ligaments are important from the perspective of sports injuries. The plantar calcaneonavicular (spring) ligament is a dense fibroelastic structure running from the sustentaculum tali to the navicular behind its tuberosity. The plantar calcaneocuboid ligament passes from the anterior inferior aspect of the calcaneus to the plantar surface of cuboid behind the peroneal groove. The long plantar ligament stretches the whole length of the lateral aspect of the foot. It arises from between the tubercles of the calcaneus and passes forwards, giving off a short attachment to the cuboid, and so forming a roof over the tendon of peroneus longus. The ligament then attaches to the bases of the lateral four metatarsal bones. The bifurcate ligament is in two parts, and travels from a deep hollow on the upper surface of the calcaneus to the cuboid and navicular.
The calcaneocuboid joint takes the full bodyweight as it forms part of the lateral longitudinal arch of the foot. Stability is provided by the plantar calcaneocuboid and long plantar ligaments, reinforced by the tendon of peroneus longus. The talocalcaneonavicular joint is stabilized by the plantar calcaneonavicular and bifurcate ligaments together with the tendon of tibialis posterior.
The calcaneocuboid ligament may be injured at the same time as the ATF. Pain is reproduced by fixing the rearfoot in dorsiflexion and eversion, and inverting and adducting the forefoot. Often the condition goes unnoticed at the time of injury as the AFT sprain is the dominant pain. Chronic pain results, and transverse frictions and scar tissue rupture may be required, with temporary forefoot posting.
Apley A.G., Solomon L. Apley’s System of Orthopaedics and Fractures, seventh ed. Oxford: Butterworth-Heinemann; 1993.
Bachmann L., Kold E., Koller M., et al. Accuracy of Ottawa ankle rules to exclude fractures of the ankle and mid-foot: systematic review. BMJ. 2003;326:1-7.
Brodsky A.E., Khalil M.A. Talar compression syndrome. Foot and Ankle. 1987;7:338-344.
Burdett R.G. Forces predicted at the ankle during running. Medicine and Science in Sports and Exercise. 1982;14:308.
Carmines D.V., Nunley J.A., McElhaney J.H. Effects of ankle taping on the motion and loading pattern of the foot for walking subjects. Journal of Orthopaedic Research. 1988;6:223-229.
Caulfield B. Functional instability of the ankle joint. Physiotherapy. 2000;86(8):401-411.
Cedell C.A. Rupture of the posterior talotibial ligament with avulsion of a bone fragment from the talus. Acta Orthopaedica Scandinavica. 1974;45:454.
De Carlo M.S., Talbot R.W. Evaluation of ankle joint proprioception following injection of the anterior talofibular ligament. Journal of Orthopaedic and Sports Physical Therapy. 1986;8(2):70-76.
Dyhre-Poulsen P., Simonsen E., Voight M. Dynamic control of muscle stiffness and H-reflex modulation during hopping and jumping in man. Journal of Physiology. 1991;437:287-304.
Eechaute C., Vaes P., Duquet W. The chronic ankle instability scale: Clinimetric properties of a multidimensional, patient-assessed instrument. Physical Therapy in Sport. 2008;9:57-66.
Eiff M.P., Smith A.T., Smith G.E. Early mobilisation versus immobilisation in the treatment of lateral ankle sprains. American Journal of Sports Medicine. 1994;22:83-88.
Flandry F., Sanders R.A. Tibiofibular synostosis: an unusual cause of shin splint-like pain. American Journal of Sports Medicine. 1987;15:280-284.
Freeman M.A.R., Dean M.R.E., Hanham I.W.F. The etiology and prevention of functional instability of the foot. Journal of Bone and Joint Surgery 4 1965 678-685 47B
Fu R., Delisa J.A., Kraft G.H. Motor nerve latencies through the tarsal tunnel in normal adults. Archives of Physical Medicine and Rehabilitation. 1980;61:243.
Garrick J.G., Webb D.R. Sports Injuries: Diagnosis and Management. London: W.B. Saunders; 1990.
Glencross D., Thornton E. Position sense following joint injury. Journal of Sports Medicine. 1981;5:241-242.
Greene T.A., Hillman S.K. Comparison of support provided by a semirigid orthosis and adhesive ankle taping before, during, and after exercise. American Journal of Sports Medicine. 1990;18(5):498-506.
Hodges P.W., Richardson C.A. Contraction of transversus abdominis invariably precedes movement of the upper and lower limb. In: Proceedings of the 6th International Conference of the International Federation of Orthopaedic Manipulative Therapists. Norway: Lillehammer; 1996.
Hughes T., Rochester P. The effects of proprioceptive exercise and taping on proprioception in subjects with functional ankle instability: A review of the literature. Physical Therapy in Sport. 2008;9:136-147.
Kaikkonen A., Kannus P., Jarninen M. Surgery versus functional treatment in ankle ligament tears. Clinical Orthopaedics. 1996;326:194-202.
Karlsson J. Acute ankle injuries. In: Brukner P., Khan K., editors. Clinical Sports Medicine. third ed. Sydney: McGraw Hill; 2007:612-631.
Karlsson J., Andersson G. The effect of external ankle support in chronic lateral ankle joint instability. American Journal of Sports Medicine. 1992;20:257-261.
Konradsen L., Ravn J.B. Ankle instability caused by prolonged peroneal reaction time. Acta Orthopaedica Scaninavica. 1990;61(5):388-390.
Konradsen L., Voight M., Hojsgaard C. Ankle inversion injuries: the role of the dynamic defence mechanism. American Journal of Sports Medicine. 1997;25:54-58.
Lambert K. The weight bearing function of the fibula. Journal of Bone and Joint Surgery. 1971;53A:507.
Lentell G., Bass B., Lopez D., et al. The contributions of proprioceptive deficits, muscle function, and anatomic laxity to functional instability of the ankle joint. Journal of Orthopedic and Sports Physical Therapy. 1995;21:206-215.
Lentell G.L., Katzman L.L., Walters M.R. The relationship between muscle function and ankle stability. Journal of Orthopaedic and Sports Physical Therapy. 1990;11(12):605-611.
Magee D.J. Orthopedic Physical Assessment, fourth ed. Philadelphia: Saunders; 2002.
Martens M.A., Noyez J.F., Mulier J.C. Recurrent dislocation of the peroneal tendons: results of rerouting the tendons under the calcaneofibular ligament. American Journal of Sports Medicine. 1986;14:148-150.
Mawdsley R., Hoy D., Eerwin P. Criterion-related validity of the figure-of-eight method of measuring ankle edema. Journal of Orthopaedic and Sports Physical Therapy. 2000;30:149-152.
O’Donoghue D.H. Treatment of Injuries to Athletes. Philadelphia: W.B. Saunders; 1976.
Palastanga N., Field D., Soames R. Anatomy and Human Movement. Oxford: Heinemann Medical; 1989.
Petrik J., Mabey M.A., Rampersaud R.J., Amendola A. The effects of isolated ankle effusion on H reflex amplitude, viscoelasticity, and postural control of the ankle. Proceedings of the American Academy of Orthopedic Surgeons. 1996;12(2):81-86.
Rasool J., George K. The impact of single leg dynamic balance training on dynamic stability. Physical Therapy in Sport. 2007;8:177-184.
Reid D.C. Sports Injury Assessment and Rehabilitation. London: Churchill Livingstone; 1992.
Rohner-Spengler M., Mannion A., Babst R. Reliability and minimal detectable change for the figure-of-eight-20 method of measurement of ankle edema. Journal of Orthopaedic and Sports Physical Therapy. 2007;37:199-205.
Rovere G.D., Clarke T.J., Yates C.S., Burley K. Retrospective comparison of taping and ankle stabilizers in preventing ankle injuries. American Journal of Sports Medicine. 1988;16:228-233.
Sammarco G.J., Miller E.H. Partial rupture of the flexor hallucis longus in classical ballet dancers. Journal of Bone and Joint Surgery. 1979;61A:440.
Stiell I.G., McKnight R., Greenberg G., et al. Implementation of the Ottawa Ankle Rules. JAMA. 1994;271:827-832.
Stokes M., Young A. The contribution of reflex inhibition to arthrogenous muscle weakness. Clinical Science. 1984;67:7-14.
Surve I., Schwellnus M.P., Noakes T., Lombard C. A fivefold reduction in the incidence of recurrent ankle sprains in soccer players using the sport-stirrup orthosis. American Journal of Sports Medicine. 1994;22:601-606.
Van Dijk C.N., Mol B., Lim L.S., et al. Diagnosis of a ligament rupture of the ankle joint. Physical examination, arthrography, stress radiography and sonography compared in 160 patients after inversion trauma. Acta Orthopaedica Scandinavica. 1996;67:566-570.
Vargish T., Clarke W.R. The ankle injury: indications for the selective use of X-rays. Injury. 1983;14:507-512.
Yeung M.S., Chan K-M., MPhil C.H.S., Yuan W.Y. An epidemiological survey on ankle sprain. British Journal of Sports Medicine. 1994;28:112-116.