CHAPTER 13 The lumbar spine
Spinal problems are among the most common conditions encountered in physical medicine. More working days are lost because of back pain than any other single condition, and sport does not escape this epidemic. Table 13.1 lays out the cost to the individual and to society as a whole.
Table 13.1 Low back pain: the scope of the problem
GP—general practitioner; LBP—low back pain; NHS—National Health Service.Compiled from Fryomoyer and Cats-Baril (1991) Clinical Standards Advisory Group (1994), CSP (2004), Airaksinen et al. (2005).
In sport, the frequency of back pain suffering presents a similar challenge. Exercise itself has a positive effect on the low back both in terms of injury prevention and rehabilitation. Those with an activity level of at least 3 hours per week have a generally lower lifetime risk of low back pain (Harreby et al., 1997). After an injury has occurred, exercise therapy has been shown to be effective at returning patients to their daily activities and to work (Van Tulder et al., 2000; Mercer et al., 2006), and has been recommended as the mainstay of treatment for this region (Waddell, Feder and Lewis, 1997).
Although exercise is beneficial to the low back, the varied activities within sport subject the spine to significant stress which often results in injury. In terms of percentage, 10–20% of all sports injuries involve the spine (Thompson, 2002), but this percentage differs between sports (Table 13.2).
Table 13.2 Back pain in specific sports
| Sport | Effect |
|---|---|
| Canoeing | 22.5% suffer from lumbago |
| Cross-country skiing | 64% suffer from back pain |
| Cycling | Incidence of back pain as high at 73.2% |
| Golf | Lifetime incidence as high at 63% |
| Gymnastics | 86% of rhythmic gymnasts report low back pain. 63% of Olympic female gymnasts have MRI abnormalities |
| Rowing | Mechanical back pain most common type |
| Squash | 51.8% of competitive players report back injury |
| Swimming | 37% suffer back pain especially with breaststroke and butterfly |
| Triathlon | 32% suffer low back pain |
| Windsurfing | Low back pain most common ailment |
| Yachting | Lumbosacral sprain most common injury (29%) |
From Thompson, B. (2002) How should athletes with chronic low back pain be managed in primary care? In Evidence Based Sports Medicine (eds D. MacAuley and T. Best). BMJ Books, London. With permission.
A detailed study of back pain is outside the scope of this book, but it is necessary to look at a number of features of spinal injury which are important within the context of sport. Much of the material for the initial parts of this section is modified from Norris (1995), and the reader is referred to that article series and Norris (2008) for a more in-depth review.
Structure
The spinal disc
There are 24 intervertebral discs lying between successive vertebrae, making the spine an alternately rigid then elastic column. The amount of flexibility present in a particular spinal segment will be determined by the size and shape of the disc, and the resistance to motion of the soft tissue support to the spinal joints. The discs increase in size as they descend the column, the lumbar discs having an average thickness of 10 mm, twice that of the cervical discs. The disc shapes are accommodated to the curvatures of the spine, and the shapes of the vertebrae. The greater anterior widths of the discs in the cervical and lumbar regions reflect the curvatures of these areas. Each disc is made up of three closely related components: the annulus fibrosis, nucleus pulposus and cartilage end plates.
Keypoint
Discs increase in size going down the spine, with the lumbar (low back) discs having a thickness of about 1 cm, twice that of the cervical discs. In the cervical and lumbar areas discs are wider anteriorly, creating the spinal curves.
The annulus is composed of layers of fibrous tissue arranged in concentric bands (Fig. 13.1). Each band has fibres arranged in parallel, and the various bands are in turn angled at 45° to each other. The bands are more closely packed anteriorly and posteriorly than they are laterally, and those innermost are the thinnest. Each disc has about 20 bands in all, and fibre orientation, although partially determined at birth, is influenced by torsional stresses in the adult (Palastanga, Field and Soames, 1989). The posterolateral regions have a more irregular make-up, and this may be one reason why they become weaker with age, predisposing them to injury.
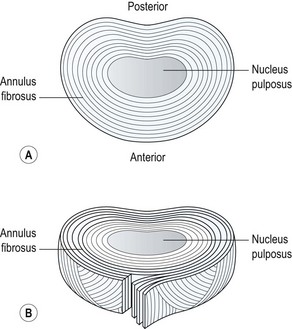
Figure 13.1 (A) Concentric band of annular fibres. (B) Horizontal section through a disc.
From Oliver and Middleditch (1991) with permission.
The annular fibres pass over the edge of the cartilage end plate of the disc, and are anchored to the bony rim of the vertebra and to its periosteum and body. The attaching fibres are actually interwoven with the fibres of the bony trabeculae of the vertebral body. The outer layer of fibres blend with the posterior longitudinal ligament, but the anterior longitudinal ligament has no such attachment (Vernon-Roberts, 1987).
The hyaline cartilage end plate rests on the surface of the vertebra. This is approximately 1 mm thick at its outer edge and becomes thinner towards its centre. The central portion of the end plate acts as a semi-permeable membrane to facilitate fluid exchange between the vertebral body and disc. In addition, it protects the body from excessive pressure. In early life the end plate is penetrated by canals from the vertebral body, but these disappear after the age of 20–30 years. After this period the end plate starts to ossify and become more brittle, the central portion thinning and in some cases being completely destroyed.
The nucleus pulposus is a soft hydrophilic (water attracting) substance taking up about 25% of the total disc area. It is continuous with the annulus, but the nuclear fibres are far less dense. The spaces between the collagen fibres are filled with proteoglycan, giving the nucleus its water-retaining capacity, and making it a mechanically plastic material. The area between the nucleus and annulus is metabolically very active and sensitive to physical force and chemical and hormonal influence (Palastanga, Field and Soames, 1989). The proteoglycan content of the nucleus decreases with age, but the collagen volume remains unchanged. As a consequence, the water content of the nucleus reduces. In early life the water content may be as high as 80–90%, but this decreases to about 70% by middle age.
Keypoint
With age: (i) the back wall of the disc becomes weaker, (ii) the end plate at the top and bottom of the disc becomes brittle, and (iii) the disc dries up, reducing its water content from 90% (child) to 70% (middle age).
The lumbar discs are the largest avascular structures in the body. The nucleus itself is dependent upon fluid exchange by passive diffusion from the margins of the vertebral body and across the cartilage end plate. Diffusion takes place particularly across the centre of the cartilage end plate which is more permeable than the periphery. There is intense anaerobic activity within the nucleus (Holm et al., 1981), which could lead to lactate build up and a low oxygen tension, placing the nuclear cells at risk. Inadequate adenosine triphosphate (ATP) supplies could lead to cell death.
The facet joint
The facet (zygapophyseal) joints are synovial joints formed between the inferior articular process of one vertebra and the superior articular process of its neighbour. As with all typical synovial joints, they have articular cartilage, a synovial membrane and a joint capsule. However, the zygapophyseal joints do have a number of unique features (Bogduk and Twomey, 1991).
The capsule is a lax structure which enables the joint to hold about 2 ml of fluid. It is replaced anteriorly by the ligamentum flavum, and posteriorly it is reinforced by the deep fibres of multifidus. The joint leaves a small gap at its superior and inferior poles creating the subscapular pockets (Fig. 13.2). These are filled with fat, contained within the synovial membrane. Within the subscapular pocket lies a small foramen for passage of the fat in and out of the joint as the spine moves.
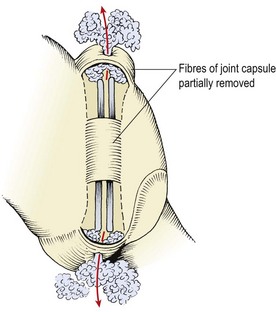
Figure 13.2 Lumbar zygapophyseal joint viewed from behind. Fat in the subscapular pockets moves through foramina in the superior and inferior capsules.
From Bogduk and Twomey (1991), with permission.
Keypoint
The facet joint has a loose capsule reinforced by the ligamentum flavum at the front and the multifidus muscle at the back. The capsule has small pockets at its top and bottom which contain fat globules which travel in and out of the joint as it moves.
Intracapsularly there are three structures of interest (Fig. 13.3). The first is the connective tissue rim, a thickened wedge-shaped area which makes up for the curved shape of the articular cartilage in much the same way as the menisci of the knee do. The second structure is an adipose tissue pad, a 2 mm fold of synovium filled with fat and blood vessels. The third structure is the fibroadipose meniscoid, a 5 mm leaf-like fold which projects from the inner surfaces of the superior and inferior capsules. These latter two structures have a protective function. During flexion, the movement of the articular facets leaves some of their cartilage exposed. Both the adipose tissue pad and the fibroadipose meniscoid are able to cover these exposed regions (Bogduk and Engel, 1984).
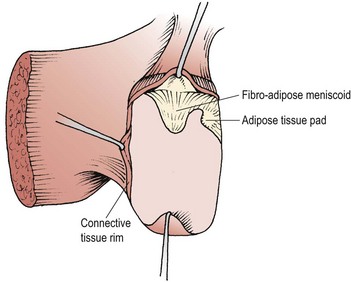
Figure 13.3 Intra-articular structures of the lumbar zygapophyseal joints.
From Bogduk and Twomey (1991), with permission.
With ageing, the cartilage of the zygapophyseal joint can split parallel to the joint surface, pulling a portion of joint capsule with it. The split of cartilage with its attached piece of capsule forms a false intra-articular meniscoid (Taylor and Twomey, 1986). Normally, the fibroadipose meniscus itself is drawn out from the joint on flexion, and should move back in with extension. However, if the meniscoid fails to move back, it will buckle and remain under the capsule, causing pain and acute locking (Bogduk and Jull, 1985). A mobilization or manipulation which combines flexion and rotation may allow the meniscoid to reduce and so relieve pain.
The facet has an overlapping neural supply, with ascending, local and descending facet branches coming from the posterior primary ramus. The nerve endings in the facet joint capsules are similar to those in the annulus of the disc, and although the disc is more sensitive, the facet joints can be a source of referred pain to the lower limb (Hirsch, Ingelmark and Miller, 1963), but not neurological deficit (Mooney and Robertson, 1976).
Spinal loading
Vertebral body
Within the vertebra itself, compressive force is transmitted by both the cancellous bone of the vertebral body and the cortical bone shell. Up to the age of 40, the cancellous bone contributes between 25% and 55% of the strength of the vertebra. After this age the cortical bone shell carries a greater proportion of load as the strength and stiffness of the cancellous bone reduces with decreasing bone density due to ageing (Rockoff, Sweet and Bleustein, 1969). As the vertebral body is compressed, blood flows from it into the subchondral post-capillary venous network (Crock and Yoshizawa, 1976). This process reduces the bone volume and dissipates energy (Roaf, 1960). The blood returns slowly as the force is reduced, leaving a latent period after the initial compression, during which the shock-absorbing properties of the bone will be less effective. Exercises which involve prolonged periods of repeated shock to the spine, such as jumping on a hard surface, are therefore more likely to damage the vertebrae than those which load the spine for short periods and allow recovery of the vertebral blood-flow before repeating a movement.
Keypoint
As the spine is compressed ‘spring’ is provided by blood flowing out of the spinal bone. As the compression is released, the blood flows back in again. If the spine is not allowed to recover from a single compression force before another is imposed, the spinal bone will be excessively stressed.
Intervertebral disc
Weight is transmitted between adjacent vertebrae by the lumbar intervertebral disc. The annulus fibrosis of a disc, when healthy, has a certain bulk and will resist buckling. When loads are applied briefly to the spine, even if the nucleus pulposus of a disc has been removed, the annulus alone exhibits a similar load-bearing capacity to that of the fully intact disc (Markolf and Morris, 1974). When exposed to prolonged loading, however, the collagen lamellae of the annulus will eventually buckle.
The application of an axial load will compress the fluid nucleus of the disc causing it to expand laterally. This lateral expansion stretches the annular fibres, preventing them from buckling. A 100 kg axial load has been shown to compress the disc by 1.4 mm and cause a lateral expansion of 0.75 mm (Hirsch and Nachemson, 1954). The stretch in the annular fibres will store energy which is released when the compression stress is removed. The stored energy gives the disc a certain springiness which helps to offset any deformation which occurred in the nucleus. A force applied rapidly will not be lessened by this mechanism, but its rate of application will be slowed, giving the spinal tissues time to adapt.
Deformation of the disc occurs more rapidly at the onset of axial load application. Within 10 minutes of applying an axial load the disc may deform by 1.5 mm. Following this, deformation slows to a rate of 1 mm per hour (Markolf and Morris, 1974), accounting for a subject’s loss of height throughout the day. Reduction in disc height slackens the collagen fibres in both the annulus and the spinal ligaments. A 2-hour compressive force which reduces the disc height by 1.1 mm has been shown to reduce resistance to flexion by 41% and increase flexion range by 12% (Adams et al., 2002). The range of flexion increases gradually throughout the day as tissues slacken and resistance is reduced. The greatest increase is seen in the first hours of rising.
Under constant loading the discs exhibit creep, meaning that they continue to deform even though the load they are exposed to is not increasing. Compression causes a pressure rise, leading to fluid loss from both the nucleus and annulus. About 10% of the water within the disc can be squeezed out by this method (Kraemer, Kolditz and Gowin, 1985), the exact amount being dependent on the size of the applied force and the duration of its application. The fluid is absorbed back through pores in the cartilage end plates of the vertebra when the compressive force is reduced.
Keypoint
The disc will compress and deform most within the first 10 minutes of a force being applied. Deformation may be as much as 1.5 mm loss in height initially, and then slows until 10% of the total water content of the disc has been lost.
Exercises which axially load the spine have been shown to result in a reduction in subject height through discal compression. Compression loads of 6–10 times bodyweight have been shown to occur in the L3–L4 segment during a squat exercise in weight training for example (Cappozzo et al., 1985). Average height losses of 5.4 mm over a 25-minute period of general weight training, and 3.25 mm after a 6 km run have also been shown (Leatt, Reilly and Troup, 1986). Static axial loading of the spine with a 40 kg barbell over a 20-minute period can reduce subject height by as much as 11.2 mm (Tyrrell, Reilly and Troup, 1985). Clearly, exercises which involve this degree of spinal loading are unsuitable for individuals with discal pathology (Table 13.3).
Table 13.3 Effect of exercise on the spinal disc
The vertebral end plates of the discs are compressed centrally, and are able to undergo less deformation than either the annulus or the cancellous bone. The end plates are, therefore, likely to fail (fracture) under high compression (Norkin and Levangie, 1992). Discs subjected to very high compressive loads show permanent deformation but not herniation (Farfan et al., 1970; Markolf and Morris, 1974). However, such compression forces may lead to herniation of nuclear material through the disc endplate known as a Schmorl’s node (Bernhardt et al., 1992) (Fig. 13.4 Adams et al., 2002).

Figure 13.4 Schmorl’s node: herniation of nuclear material through the disc endplate.
Reproduced from Adams et al. (2002).
Keypoint
A Schmorl’s node is the herniation of discal material through the disc endplate and into the vertebral body.
Bending and torsional stresses on the spine, when combined with compression, are more damaging than compression alone, and degenerated discs are particularly at risk. Average failure torques for normal discs are 25% higher than for degenerative discs (Farfan et al., 1970). Degenerative discs also demonstrate poorer viscoelastic properties and therefore a reduced ability to attenuate shock.
Age related changes
We have seen that with age the back wall of the disc weakens, the end plates become brittle and the disk reduces its water content from 90% in childhood to 70% in middle age. In addition, the disc’s reaction to a compressive stress changes with age, because the ability of the nucleus to transmit load relies on its high water content. The hydrophilic nature of the nucleus is the result of the proteoglycan it contains, and as this changes from about 65% in early life to 30% by middle age (Bogduk and Twomey, 1987), the nuclear load-bearing capacity of the disc reduces. When the proteoglycan content of the disc is high, up to the age of 30 years in most subjects, the nucleus pulposus acts as a gelatinous mass, producing a uniform fluid pressure. After this age, the lower water content of the disc means that the nucleus is unable to build as much fluid pressure. As a result, less central pressure is produced and the load is distributed more peripherally, eventually causing the annular fibres to become fibrillated and to crack (Hirsch and Schajowicz, 1952).
Brown pigmentation is seen which is an indication of change in the collagenous tissue (Adams et al., 2002), and the nucleus becomes dry and fibrous. As the disc drys, the annulus takes more of the compressive strain of weight bearing. However, the annulus itself weakens through the accumulation of defects and fissures over time (Fig. 13.5).
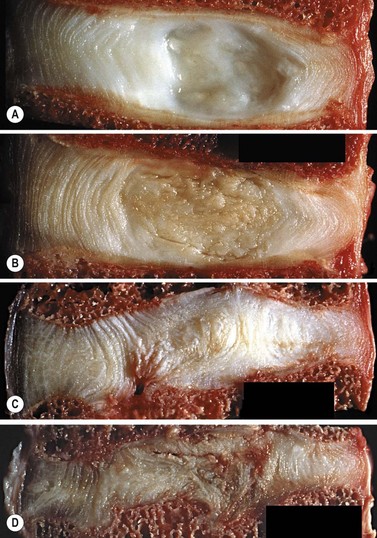
Figure 13.5 Discal degeneration. (A) healthy disc (B) early shrinkage (C) Disc thinning with smorls node formation (D) Gross discal thinning and loss of disc height.
Reproduced from Adams et al. (2002).
As a result of these age-related changes the disc is more susceptible to injury later in life. This, combined with the reduction in general fitness of an individual and changes in movement patterns of the trunk related to the activities of daily living, greatly increases the risk of injury to this population. Individuals over the age of 40, if previously inactive, should therefore be encouraged to exercise the trunk under the supervision of a physiotherapist before attending fitness classes run for the general public.
Movements of the spine
Flexion
During flexion movements the anterior annulus of the lumbar discs will be compressed while the posterior fibres are stretched. Similarly, the nucleus pulposus of the disc will be compressed anteriorly while pressure is relieved over its posterior surface. As the total volume of the disc remains unchanged, its pressure should not increase. The increases in pressure seen with alteration of posture are therefore due not to the bending motion of the bones within the vertebral joint itself but to the soft tissue tension created to control the bending.
Discal pressure changes
If the pressure at the L3 disc for a 70 kg standing subject is said to be 100%, supine lying reduces this pressure to 25%. The pressure variations increase dramatically as soon as the lumbar spine is flexed and tissue tension increases (Fig. 13.6). The sitting posture increases intradiscal pressure to 140%, while sitting and leaning forward with a 10 kg weight in each hand increases pressure to 275% (Nachemson, 1987). The selection of an appropriate starting position for trunk exercise is therefore of great importance. Superimposing spinal movements from a slumped sitting posture, for example, would place considerably more stress on the spinal discs than the same movement beginning from crook lying.
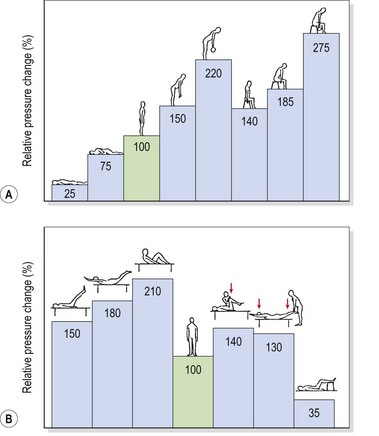
Figure 13.6 Relative pressure changes in the third lumbar disc. (A) In various positions. (B) In various muscle strengthening exercises.
From Nachemson (1976).
Keypoint
The highest discal pressures are seen in loaded slumped sitting, that is sitting with the lumbar lordosis reversed (flexed) while holding a weighted object. This type of posture must be avoided in sport, especially during weight training exercises such as seated shoulder press.
During flexion, the posterior annulus is stretched and the nucleus is compressed onto the posterior wall. The posterior portion of the annulus is the thinnest part, and the combination of stretch and pressure to this area may result in discal bulging or herniation.
As the lumbar spine flexes, the lordosis flattens and then reverses at its upper levels. Reversal of lordosis does not occur at L5–S1 (Pearcy, Portek and Shepherd, 1984). Flexion of the lumbar spine involves a combination of anterior sagittal rotation and anterior translation. As sagittal rotation occurs, the articular facets move apart, permitting the translation movement to occur. Translation is limited by impaction of the inferior facet of one vertebra on the superior facet of the vertebra below (Fig. 13.7). As flexion increases, or if the spine is angled forward on the hip, the surface of the vertebral body will face more vertically increasing the shearing force due to gravity. The forces involved in facet impaction will therefore increase to limit translation of the vertebra and stabilize the lumbar spine. Because the zygapophyseal joint has a curved articular facet, the load will not be concentrated evenly across the whole surface, but will be focused on the anteromedial portion of the facets.
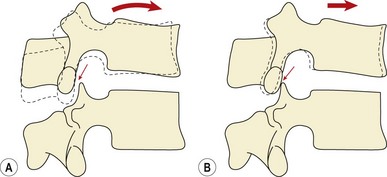
Figure 13.7 Vertebral movement during flexion. Flexion of the lumbar spine involves a combination of anterior sagittal rotation and anterior translation. As sagittal rotation occurs, the articular facets move apart (A), permitting the translation movement to occur (B). Translation is limited by impaction of the inferior facet of one vertebra on the superior facet of the vertebra below.
From Bogduk and Twomey (1987), with permission.
The sagittal rotation movement of the zygapophyseal joint causes the joint to open and is therefore limited by the stretch of the joint capsule. Additionally, the posteriorly placed spinal ligaments will also be tightened. Analysis of the contribution to limitation of sagittal rotation within the lumbar spine, through mathematical modelling, has shown that the disc limits movement by 29%, the supraspinous and interspinous ligaments by 19% and the zygapophyseal joint capsules by 39% (Adams, Hutton and Stott, 1980).
Extension
During extension the anterior structures are under tension while the posterior structures are first unloaded and then compressed, depending on the range of motion. With extension movements the vertebral bodies will be subjected to posterior sagittal rotation. The inferior articular processes move downwards causing them to impact against the lamina of the vertebra below. Once the bony block has occurred, if further load is applied the upper vertebra will axially rotate by pivoting on the impacted inferior articular process. The inferior articular process will move backwards, overstretching, and possibly damaging, the joint capsule (Yang and King, 1984). With repeated movements of this type, eventual erosion of the laminal periosteum may occur (Oliver and Middleditch, 1991). At the site of impaction, the joint capsule may catch between the opposing bones giving another cause of pain (Adams and Hutton, 1983). Structural abnormalities can alter the axis or rotation of the vertebra, so considerable variation between subjects exists (Klein and Hukins, 1983).
Rotation
During rotation, torsional stiffness is provided by the outer layers of the annulus, by the orientation of the zygapophyseal joints, and by the cortical bone shell of the vertebral bodies themselves. In rotation movements, the annular fibres of the disc will be stretched according to their direction. As the two alternating sets of fibres are angled obliquely to each other, some of the fibres will be stretched while others relax. A maximum range of 3° of rotation can occur before the annular fibres will be microscopically damaged, and a maximum of 12° before tissue failure (Bogduk and Twomey, 1987). As rotation occurs, the spinous processes separate, stretching the supraspinous and interspinous ligaments. Impaction occurs between the opposing articular facets on one side causing the articular cartilage to compress by 0.5 mm for each 1° of rotation, providing a substantial buffer mechanism (Bogduk and Twomey, 1987). If rotation continues beyond this point, the vertebra pivots around the impacted zygapophyseal joint causing posterior and lateral movement (Fig. 13.8). The combination of movements and forces which occur will stress the impacted zygapophyseal joint by compression, the spinal disc by torsion and shear, and the capsule of the opposite zygapophyseal joint by traction. The disc provides only 35% of the total resistance (Farfan et al., 1970).
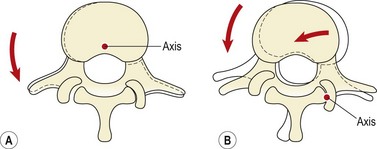
Figure 13.8 Vertebral movement during rotation. (A) Initially rotation occurs around an axis within the vertebral body. (B) The zygapophyseal joints impact and further rotation causes the vertebra to pivot around a new axis at the point of impaction.
From Bogduk and Twomey (1987), with permission.
Lateral flexion
When the lumbar spine is laterally flexed, the annular fibres towards the concavity of the curve are compressed and will bulge, while those on the convexity of the curve will be stretched. The contralateral fibres of the outer annulus and the contralateral intertransverse ligaments help to resist extremes of motion (Norkin and Levangie, 1992). Lateral flexion and rotation occur as coupled movements. Rotation of the upper four lumbar segments is accompanied by lateral flexion to the opposite site. Rotation of the L5–S1 joint occurs with lateral flexion to the same side.
Movement of the zygapophyseal joints on the concavity of lateral flexion is by the inferior facet of the upper vertebra sliding downwards on the superior facet of the vertebra below. The area of the intervertebral foramen on this side is therefore reduced. On the convexity of the laterally flexed spine the inferior facet slides upwards on the superior facet of the vertebra below, increasing the diameter of the intervertebral foramen.
End-range spinal stress in sport
If the trunk is moving slowly, tissue tension will be felt at end-range and a subject is able to stop a movement short of full end-range and protect the spinal tissues from overstretch. However, rapid movements of the trunk will build up large amounts of momentum. When the subject reaches near end-range and tissue tension builds up, the momentum of the rapidly moving trunk will push the spine to full end-range, stressing the spinal tissues. In many popular sports, exercises often used in a warm-up are rapid and ballistic in nature and performed for a high number of repetitions. These can lead to excessive flexibility and a reduction in passive stability of the spine.
In addition, end-range stress can be experienced with postural changes and an alteration in the control of movement within the lumbar spine. Clinically, a number of directional patterns have been described (Sullivan: O’, 2000). Flexion of the lumbar spine is seen with a gross reduction in the depth of the lumbar lordosis (Fig. 13.9). The athlete suffers pain when semi-flexed postures are maintained, and with prolonged sitting activities. When put in a four point kneeling position, the lumbar spine remains flexed. Extension of the lumbar spine is seen in the lordotic posture with the pelvis anteriorly tilted. In standing, and especially during extension movements of the whole spine or hip, the lumbar spine appears to ‘hinge’ as a single level rather than extend through its whole length. Lateral flexion movements are seen with tightness to the lateral flexors (quadratus lumborum and lateral external oblique). This is brought to the fore with single leg standing activities. Here, the patient, instead of transferring bodyweight with the pelvis, laterally flexes the spine and a noticeable scoliosis is apparent.
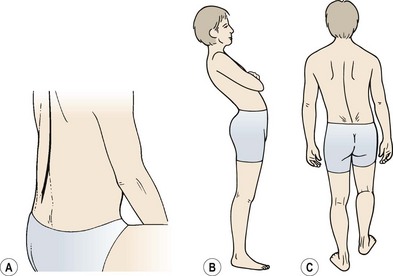
Figure 13.9 Directional patterns of end-range stress in the lumbar spine. (A) Flexion. (B) Extension. (C) Lateral shifting.
After O’Sullivan (2000), with permission.
Discal injury
During flexion, extension and lateral flexion, one side of the disc is compressed and the other stretched. In flexion, the axis of motion passes through the nucleus, but with extension the axis moves forwards (Klein and Hukins, 1981). This fact, coupled with the increased range of motion during flexion, makes it the more dangerous movement. Combinations of torsion and flexion place the disc at particular risk from plastic deformation, which stretches the annular fibres irreversibly, and may cause fibre damage.
A single movement of flexion will stretch and thin the posterior annulus, but it is repeated flexion, especially under load, which is likely to give the most serious pathological consequences. Discal injury occurs frequently through repeated flexion movements, and when a flexion/rotation strain is placed on the spine during lifting.
When hyperflexion takes place, the supraspinous and interspinous ligaments will overstretch, reducing the support to the lumbar spine. Circumferential tearing will occur to the disc annulus posterolaterally, usually at the junction between the disc lamina and end plate (Oliver and Middleditch, 1991). The outer annular fibres are innervated, a possible cause of the ‘dull ache’ in the lumbar spine which often precedes disc prolapse. Rotation strain will increase the likelihood of these injuries. Although rotation is limited in the lumbar spine, it is increased significantly as a result of facet joint degeneration and during flexion as the facets are separated.
Posterolateral radial fissuring occurs later, and connects the disc nucleus to the circumferential tear, allowing the passage of nuclear material towards the outer edge of the disc. This type of injury has been produced experimentally during discal compression in a combined flexed and laterally flexed posture (Adams and Hutton, 1982). An annular protrusion can occur when the pressure of the displaced nuclear material causes the annulus to bulge. Eventually, nuclear material is extruded (herniated) through the ruptured annular wall (Fig. 13.10).
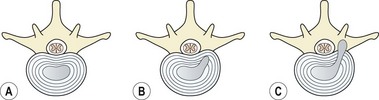
Figure 13.10 Stages of disc herniation. (A) Normal disc. (B) Nuclear bulge with annulus intact. (C) Ruptured annulus, nuclear protrusion onto nerve root.
The discal injury may occur gradually as a result of repeated bending, giving symptoms of gradually worsening pain. Pain occurs initially in the lower back, and with time the symptoms are peripheralized into the buttock and lower limbs.
Keypoint
Repeated bending may give gradually worsening low back pain. With time the symptoms peripheralize (travel outwards) into the buttocks and legs.
Sudden pain may occur from a seemingly trivial injury which acts as the ‘last straw’ to cause the disc herniation. Loads of sufficient intensity may give rise to an abrupt massive disc herniation. The stress is usually one of weight combined with leverage during a lifting action. Hyperflexion of the spine occurs, due in part to overstretching of the posterior lumbar ligaments.
Radiographic investigations of discal movement have been made by inserting metal pins into the lumbar nucleus pulposus and asymmetrically loading the disc (reported in McKenzie, 1990). These have shown that the disc migrates towards the area of least load. When the asymmetrical load was removed, the nucleus remained displaced, but its relocation was accelerated by compression in the opposite direction or by traction.
A number of studies have investigated the phenomenon of discal nuclear movement within the lumbar discs. Beattie, Brooks and Rothstein (1994) showed movement during extension with healthy discs but not with degenerative discs, and Edmondston, Song and Bricknell (2000) demonstrated 6.7% anterior displacement between flexion and extension in L1/2, L2/3 and L5/S1. Fennell, Jones and Hukins (1996) used MRI scanning to demonstrate anterior movement during extension.
Spinal ligaments
A number of spinal ligaments are of concern to the biomechanics of the lumbar spinal segment: the anterior and posterior longitudinal ligaments, the intertransverse ligament, the ligamentum flavum, the interspinous and supraspinous ligaments and the capsular ligaments of the facet joint (Fig. 13.11). A general reduction in energy absorption of all the ligaments has been found with age (Tkaczuk, 1968). The stiffest is the posterior longitudinal ligament and the most flexible the supraspinous (Panjabi, Jorneus and Greenstein, 1984). The ligamentum flavum in the lumbar spine is pre-tensioned (resting tension) when the spine is in its neutral position, a situation which compresses the disc. This ligament has the highest percentage of elastic fibres of any tissue in the body (Nachemson and Evans, 1968), and contains nearly twice as much elastin as collagen. With age and degeneration there is a reduction of the elastin content of the the ligamentum flavum, and calcification is sometimes apparent (Adams et al., 2002). The anterior longitudinal ligament and joint capsules have been found to be the strongest, while the interspinous and posterior longitudinal ligaments are the weakest (Panjabi, Hult and White, 1987).
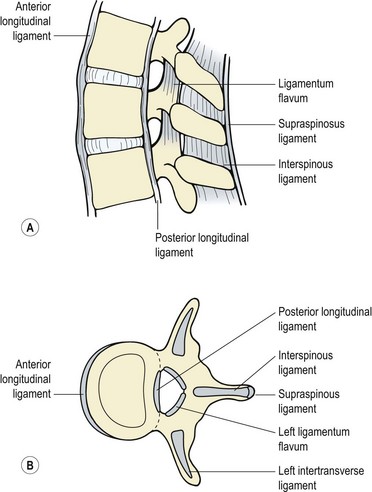
Figure 13.11 Ligaments of the spinal segment. (A) Side view. (B) Superior view.
Reprinted by permission from Norris, C.M. (2000) Back Stability. Human Kinetics, Champaign, Illinois.
The ligaments act rather like rubber bands, resisting tensile forces but buckling under compressive loads (Fig. 13.12). They must allow adequate motion and fixed postures between vertebrae, enabling a minimum amount of muscle energy to be used. In addition, they protect the spine by restricting motion and in particular protect the spinal cord in traumatic situations, where high loads are applied at rapid speeds. In this situation, the ligaments absorb large amounts of energy.
The longitudinal ligaments are viscoelastic, being stiffer when loaded rapidly, and they exhibit hysteresis as they do not store the energy used to stretch them.
Definition
Viscoelasticity is the ability of a material to store and dissipate energy during mechanical deformation. The deformation is dependent on the rate of loading. Hysteresis occurs when a material is stressed and does not immediately return to its previous shape when the stress is released.
When loaded repeatedly, they become stiffer, and the hysteresis is less marked, making the longitudinal ligaments more prone to fatigue failure (Hukins, 1987). The supraspinous and interspinous ligaments are further from the flexion axis, and therefore need to stretch more than the posterior longitudinal ligament when they resist flexion.
Low back pain
The exact structure which is affected in low back pain is open to discussion, and often it is virtually impossible to identify precisely which tissue is causing a patient’s symptoms (Spitzer, LeBlanc and Dupuis, 1987). Diagnostic labels may often be misleading, with pathology identified which does not necessarily relate to the patient’s symptoms. Identification of the movement dysfunction or movement impairment (Sahrmann, 2002) may be a better guide to effective rehabilitation.
To this end, the approach taken by McKenzie (1981) is extremely useful. Back pain may be classified as mechanical or chemical (non-mechanical) in origin. Mechanical pain is produced by deformation of structures containing nociceptive nerve endings, and there is a clear correlation between certain body positions and the patient’s symptoms.
Non-mechanical pain, on the other hand, is of a constant nature. This may be exacerbated by movement or position, but importantly, no position will be found which completely relieves the symptoms. This category encompasses both inflammatory and infective processes.
Keypoint
Mechanical pain is produced by deformation of sensitive structures. There is a definite correlation between body positions and the patient’s symptoms. Non-mechanical pain is constant, and no position can be found which completely relieves the symptoms.
Inflammation will occur following trauma, and the accumulation of chemical irritant substances will affect the nociceptive fibres and give pain. This type of pain will continue for as long as the nociceptor irritation continues. With rest, irritation will settle and healing progress. Part of this healing process is scar formation, so the type of pain will change from a constant chemical pain to a mechanical pain developed through adaptive shortening of the affected tissues. Non-mechanical conditions also include those which refer pain to the spine, such as vascular or visceral damage and carcinoma. Clearly, it is essential to differentiate between mechanical and non-mechanical pain in the lower back. When no movement can be found which reduces the patient’s symptoms and if a period of rest does not allow the symptoms to subside, the patient requires medical investigation.
Examination of the back
Screening examination
Examination of the lumbar spine can be either very complex or relatively simple, depending on the approach taken. The reliability and reproducibility of tests for the spine increases when the information to be gained from the tests is kept to a minimum (Nelson et al., 1979). For this reason, the work of Cyriax (1982) and McKenzie (1981) is valuable as it provides enough information to treat the majority of patients. In addition, the tests tell the practitioner when further investigation is necessary.
Observation deals initially with posture while standing and sitting, and the appearance of the spine at rest. Assessment of the patient’s movements provides essential information to guide rehabilitation. Scoliosis and loss of normal lordosis are of particular note, as is the level of the iliac crests. Flexion, extension and lateral flexion are tested initially as single movements to obtain information about range of motion, end feel and presence of a painful arc. Flexion and extension are then repeated to see if these movements change the intensity or site of pain, bearing in mind the centralization phenomenon and dysfunction stretch. Side-gliding movements are also tested to repetition. Flexion and extension may be further assessed in a lying position to obtain information about nerve root adhesion (flexion) and greater range of extension. This initial examination then indicates whether neurological testing of sensation, power, reflexes and further nerve stretch is required. In addition, the history, signs and symptoms will indicate whether the pelvis and sacroiliac joints warrant further attention, or if resisted tests should be included.
Diagnostic triage
Diagnostic triage extends the screening examination by categorizing low back pain into three types: simple backache, nerve root pain and serious pathology (Table 13.4).
|
Nerve root pain: specialist referral not generally required within first 4 weeks, if the pain is resolving
|
After Waddell, G., Feder, G. and Lewis, M. (1997) Systematic reviews of bed rest and advice to stay active for acute low back pain. British Journal of General Practice, 47, 647–652, and Norris (2000).
With simple backache the patient is generally young to middle age (20–55 years), and the pain is restricted to the low back and buttocks or thighs. The pain is mechanical in nature because it changes with movement, being eased or aggravated by specific actions which are repeatable. The patient is generally in good health and there is no history of weight loss, nausea or fever. Often there is a history of injury or overuse.
Nerve root pain is normally unilateral and the leg pain may be worse than the pain in the low back. Pain may radiate into the foot, and numbness or paraesthesia (altered sensation) may be present. This type of pain may require further investigation if it does not show signs of significant improvement within 4 weeks of onset.
Where examination reveals non-mechanical pain in a young (under 20) or older (over 55) athlete, specialist investigation is required. This is especially the case where there is a previous history of an associated medical condition, or if the patient has been unwell, shows an obvious structural deformity of the spine or demonstrates gait disturbance. Where altered sensation is present in the ‘saddle’ area (perineum and genitals) further investigation is required as this indicates possible disc protrusion of the lower sacral nerve roots. Where this is present with difficulty in passing urine, an inability to retain urine and/or a lack of sensation when the bowels are opened, there is a possibility of compression of the cauda equina and immediate emergency referral is required (Kesson and Atkins, 1998; Magee, 2002).
The straight leg raise
The straight leg raise (SLR) or Lasegue’s sign is a widely used test to assess the sciatic nerve in cases of back pain. Although widely used, the test has limited diagnostic accuracy when diagnosing herniated discs. In a systematic review of 11 studies assessing the accuracy of SLR against surgery as a reference standard, Deville et al. (2000) found a low specificity of 0.26 and a sensitivity of 0.91.
Keypoint
Specificity (true negative) of a test indicates its ability to detect those who do not have a condition, while sensitivity (true positive) indicates how good a test is at detecting patients who have a condition. Both are measures of diagnostic accuracy which is the measure of agreement between a clinical test and a reference standard.
In addition to its effect on the sciatic nerve, the SLR test also places stretch on the hamstrings, buttock tissues, sacroiliac joint, posterior lumbar ligaments and facet joints in addition to lengthening the spinal canal (Urban, 1986). Confirmation that the nerve root is the source of pain may be improved by raising the leg to the point of pain and then lowering it a few degrees. The neuromeningeal structures are then further stretched either from below by dorsiflexing the foot, or applying firm pressure to the popliteal fossa over the posterior tibial nerve. Pressure from above is produced by flexing the cervical spine. When performing the SLR, as the leg is raised the knee should not be allowed to bend and the pelvis should stay on the couch.
The dura within the spinal canal is firmly attached to the foramen magnum above and the filum terminale below. Trunk flexion causes the spinal canal to lengthen and therefore stretches the dura, whereas extension, by shortening the canal, induces dural relaxation allowing the sheath to fold. The neuromeningeal pathway is elastic, so tension imparted at one point will spread throughout the whole length of the spine. As the SLR is performed, the initial motion is of the nerve at the greater sciatic notch. As hip flexion goes through 35°, movement occurs proximal to the ala of the sacrum, and during the next 35° the movement is at the intervertebral foramen itself. The last degrees of the SLR do not produce further nerve movement, but simply increase the tension over the whole course of the nerve (Grieve, 1970) (Fig. 13.13).
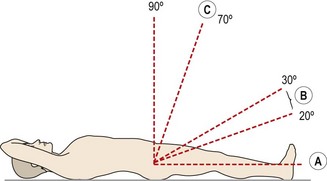
Figure 13.13 Effects of straight leg raising. A. Movement of sciatic nerve begins at the greater sciatic notch. B. Movement of roots begins at the intervertebral foramen. C. Minimal movement only, but increase in tension.
From Oliver and Middleditch (1991), with permission.
Testing the unaffected leg (crossed SLR or ‘well leg’ test) may also give symptoms. This manoeuvre pulls the nerve root and dura distally and medially, but increases the pressure on the nerve complex by less than half that of the standard SLR test. When the ipsilateral SLR causes pain, it simply means that one of the tissues connected to the nerve pathway is sensitized. Because the crossed SLR stretches the neural structures less, the resting tension of these tissues must be higher to cause pain. The crossed SLR may therefore be a more reliable predictor of large disc protrusions than the ipsilateral SLR (Urban, 1986).
Slump test
The slump test is used to assess tension in the pain-sensitive structures around the vertebral canal or intervertebral foramen, and to ensure that these structures are able to stretch properly (Maitland, 1986; Butler, 1991). To perform the manoeuvre the patient sits unsupported over the couch side with the knees together and flexed to 90°. The posterior thigh is in contact with the couch. The patient is then instructed to relax the spine completely and ‘slump’ forward, keeping the cervical spine in its neutral position (‘look forwards, not down’). The therapist (standing at the side of the patient) places overpressure onto the patient’s shoulders to increase the movement, attempting to bow the spine rather than increase hip flexion (Fig. 13.14A).
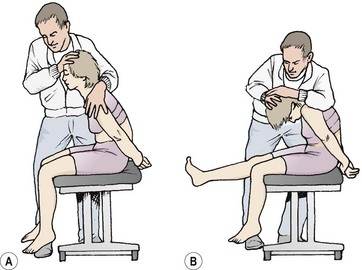
From this position the patient is asked to flex the neck (‘chin to chest’) and then straighten the leg on the unaffected side first (Fig. 13.14B). In each case the examiner places overpressure on the area and assesses the result. The athlete is then asked to dorsiflex the ankle (‘pull your toes up’). Neck flexion is slowly released, and the response monitored. The opposite leg is then tested. A normal test result is one where there is a pain-free lack of knee extension by about 30° and slight central pain over T9/10 (Maitland, 1986).
Mechanical therapy
Three mechanical conditions are recognized in the lower back: the postural syndrome, dysfunction and derangement (McKenzie, 1981).
Postural syndrome
The postural syndrome occurs when certain postures or body positions place pain sensitive soft tissues around the lumbar spine under prolonged stress. Pain is intermittent, and only occurs when the particular posture is taken up, and ceases when the offending posture is changed. This can be frustrating for the patient because they can find nothing wrong. There is no deformity, vigorous activity is frequently painless as the stresses it imposes on the tissues are continually changing. The fault usually lies with poor sitting posture which places the lumbar spine in flexion. After sport, the patient is warm and relaxed and so sits in a slumped position, perhaps in the bar after a game of squash. Discomfort occurs after some time and this gradually changes to pain. The patient often has the idea that sport makes the pain worse, but this is not the case. The poor sitting posture used when relaxing after sport is the true problem.
Keypoint
With the postural syndrome, pain occurs through tension on pain-sensitive soft tissues in the back. Particular body positions cause pain, and when these are released the pain subsides.
Pain may also occur in sport from extreme positions. Hyperflexion when lifting a weight from the ground or performing stretching exercises, hyperextension when pressing a weight overhead, or performing a back walkover in gymnastics are common examples.
The most important part of management with the postural syndrome is patient education. To this end, the slouch-overcorrect procedure for correcting sitting posture is useful (McKenzie, 1981). The patient sits on a stool, and is allowed to slouch into an incorrect sitting posture for some time until back pain ensues. He or she is then taught a position of maximum lordosis, and learns how to change rapidly and at will, from the incorrect slouch to this overcorrect maximum lordosis. Once the patient has seen the relationship between poor sitting posture and pain, he or she is taught a correct sitting posture mid-way between the two extreme movement ranges. The use of a lumbar pad or roll is helpful to maintain the lordosis in sitting.
Where hyperflexion or hyperextension is the cause of postural pain, video is particularly useful in enabling athletes to appreciate the strain they are placing on the lumbar spine. Re-education of movement and skill training, with emphasis on the position of the spine and hips, are helped by video playback. Body landmarks over the pelvis and spine are marked first using white adhesive dots. Biofeedback is also useful, especially when trying to correct hyperflexion. In its simplest form, strips of prestretched elastic tape are placed at either side of the lumbar spine. When the athlete flexes, the tape ‘drags’ on the skin and acts as a reminder to avoid the flexed position.
Dysfunction
Dysfunction pain is caused by overstretching adaptively shortened structures within the lumbar spine. The previously damaged structures have shortened due to prolonged disuse, or scar tissue formation. When the normal range of motion is attempted at the affected segment, the shortened soft tissues are stretched prematurely. The essential feature with dysfunction is pain at the end of movement range which disappears as soon as the end-range stretch is released. The position is self-perpetuating because the pain which occurs with stretching causes the patient to avoid the full range motion and so the adaptive shortening is compounded.
Dysfunction may occur secondary to trauma, or as a result of the postural syndrome. Typically, the patient is stiff first thing in the morning and the back ‘works loose’ through the day, so the patient is generally better with activity. Loss of extension leads to a reduced lordosis, and loss of flexion becomes apparent when the patient tries to touch the toes. Frequently, the patient will deviate to the side of the dysfunction. Once dysfunction has been detected, (static) stretching is required and/or joint mobilization procedures. Although mobilizations at grades III and IV are useful to help restore range of movement, this passive treatment must be coupled with active stretching procedures which the patient can practise at home to help regain lost physiological range.
Accessory movements cannot usually be practised by the patient, and are perhaps a more appropriate form of manual therapy where physiological stretching causes excessive pain. It is important that stretching be practised little and often, to allow the patient to recover from the soreness which follows the lengthening of contracted tissues. The patient must be instructed to press gently into the painful end-range point in an attempt to increase the range of motion. There is always a tendency to try and avoid the painful position with back pain, but with dysfunction this is precisely the position we want to work in.
Keypoint
Dysfunction pain is caused by overstretching adaptively shortened structures within the lumbar spine. The most common form is an extension dysfunction where the lumbar curve (lordosis) appears flat and lumbar extension range is limited.
The most common dysfunction following low back pain is loss of extension (McKenzie, 1981). The extension loss may be regained by a combination of mobilization, manipulation and mechanical therapy. The classic mechanical therapy procedure is extension in lying (EIL), either with or without belt fixation. The patient lies prone on the treatment table, with the lumbar spine held by a webbing fixation belt. This is placed around both the lower spine and treatment table at a point just below the spinal segment which is blocked to extension. From this position, the patient performs a modified press-up exercise, trying to fully extend the arms while keeping the hips in contact with the couch surface (Fig. 13.15). At home the patient should continue the exercise at regular intervals throughout the day. Various modifications may be used to apply the pressure—EIL with the patient lying on a ironing board using a thick belt, or positioning the spine under a low piece of furniture, or manual pressure from a spouse or the weight of a small child.

Loss of flexion may be similarly regained, but this time the mechanical therapy technique is flexion in lying (FIL), or flexion in standing (FIS). Initially the patient uses FIL. The movement begins in a crook-lying position. From this position the patient pulls the knees to the chest. As maximum hip flexion is reached, further movement occurs initially by flexion of the lower lumbar and lumbosacral segments, and then the upper lumbar area (Fig. 13.16). FIS is simply a toe-touching exercise performed very slowly. Gravitation effects place greater stress on the lumbar discs, so the exercise must proceed with caution. The differences between FIS and FIL are two-fold. First, with FIS the legs are straight, and so the nerve roots are stretched, a particularly useful effect when dealing with nerve root adhesion. Secondly, the sequence of flexion is reversed, with the upper lumbar areas moving before the lower lumbar and lumbosacral areas. Where there was a deviation in flexion at the initial examination, flexion in step standing may be used (Fig. 13.17). Here, one leg is placed on a stool and the patient pulls the chest downwards onto the flexed knee. In so doing, flexion is combined with slight lateral bending. Other dysfunctions such as loss of lateral flexion, side-gliding, or rotation may occur but they are less common. In addition, it must be remembered when assessing symmetry of bilateral movements that most people are slightly asymmetrical anyway. We must be certain that any asymmetry that exists is relevant to the patient’s present symptoms before we spend time correcting it.


Derangement
Derangement occurs when the nucleus or annulus of the disc is distorted or damaged, altering the normal resting position of two adjacent vertebrae. Pain is usually constant and movement loss is apparent, so much so in some cases that the condition is completely disabling. Derangement of the lumbar disc is a common cause of low back pain, and Cyriax (1982) claimed there are eight ways in which a damaged disc can move, and classified these according to discal position (Table 13.5). McKenzie (1981) described seven types, classified according to symptoms, as derangements 1 to 7. The McKenzie classifications were later simplified (McKenzie and May, 2003), derangements now being classified as either central (symmetrical) or unilateral (asymmetrical), with or without pain to the knee (Table 13.6).
Table 13.5 Cyriax classification of disc lesions
| Gradual small posterior displacement |
| Pain brought on by stooping or lifting and relieved by standing or resting. Articular signs only, sometimes with painful arc, SLR is full |
| Swift large posterior displacement |
| Severe low back pain of traumatic origin, or from overuse following prolonged stooping. Constant ache with intermittent twinges. Articular signs of flexion deformity, dural signs of limited SLR and lumbar pain in full neck flexion |
| Massive posterior protrusion |
| Posterior longitudinal ligaments may rupture, compression sciatic nerve roots and giving sympathetic signs. Perineal pain and bilateral symptoms, limited SLR with root palsy. Saddle analgesia with bladder weakness |
| Posterolateral protrusion |
| Previous history of general backache, changing to unilateral pain, pins and needles or numbness, aggravated by coughing. Limitation of trunk flexion and SLR. Pain often increased by neck flexion |
| Anterior protrusion in the elderly |
| Backache and/or unilateral pain with pins and needles in the feet, often mimicking claudication. Symptoms are present only when the patient has been upright for some time and relieved by sitting or lying. Flexion reduces symptoms. SLR full, no neurological deficit |
| Anterior protrusion in adolescents |
| Osteochondrosis giving pressure erosion of the vertebral body, and kyphotic posture. Associated with excessive weight bearing |
| Vertical protrusion |
| Schmorl’s node formation. No pain, but radiographic appearance confirms abnormality. T10 most commonly affected. Alternatively, biconcave disc phenomenon with osteoporosis |
| Circular protrusion |
| Compression causes uniform discal bulging, with traction to the periosteum and subsequent osteophyte formation. Limited spinal mobility |
Adapted from Cyriax (1982).
Table 13.6 McKenzie symptom patterns
| Pattern | Previous derangement classification |
|---|---|
| Central (symmetrical) | 1, 2, 7 |
| Unilateral (asymmetrical) ± pain to knee | 3, 4, 7 |
| Unilateral (asymmetrical), pain below knee | 5, 6 |
After McKenzie and May (2003).
Deformities of scoliosis and kyphosis are common, with local or referred pain over the lumbar and sacral dermatomes depending on the severity of injury. Again, management may be by manual or mechanical therapy or a combination of the two. Mechanical therapy aims at centralizing the pain and reversing the sequence of pain development which occurred as the disc lesion progressed. The aim is to transfer pain which is felt laterally in the spine or in the leg to a more central position. It is perfectly acceptable for the intensity of the pain to increase providing its position is altered to a more central one.
Keypoint
Derangement occurs when a spinal disc is distorted, altering the resting position of the vertebrae. Pain is usually constant and movement loss is seen. The aim is to centralize the pain, taking it from the leg or buttock back into the spine, and finally reducing it altogether.
The movements used are those which reduced the patient’s symptoms in the initial examination. Where a scoliosis exists, initially the most effective movement is usually side-gliding in standing (SGIS). The therapist stands at the side of the patient holding the patient’s hips. The therapist then gently presses the patient’s shoulders towards the convexity of the scoliosis aiming to obtain a sliding rather than laterally flexing movement. The patient may continue this by placing the hand on a wall (arm abducted to 90°) and shifting the hips towards the wall (Fig. 13.18). Once the pain moves into a more central position, the EIL exercise begins with the aim of centralizing the pain further. Although these movements are frequently very effective for posterolateral protrusions, it must be emphasized that it is the movement which reduces the symptoms which is practised, and this may vary tremendously between patients.

Manual therapy of the lumbar spine
Manual therapy is a general term which describes hands-on procedures used to treat the joints and soft tissues. The most common subdivisions are mobilization and manipulation. Mobilization is a graded form of passive movement used repeatedly (oscillation), while manipulation is a term usually confined to single high-velocity low-amplitude techniques (thrust). However, the terms are frequently profession specific and may be used to define scope of practice. Procedures such as fascial manipulation, specific soft tissue mobilization and neural mobilization describe a hands-on technique specific to a target tissue. Bone and soft tissue techniques are commonly used by physiotherapists, osteopaths and chiropractors and other practitioners in orthopaedic medicine. Soft tissue techniques are also used by massage therapists of all types.
The point at which manual therapy is used in sport will vary depending on both the condition and the practitioner using the therapy. Some practitioners rarely use manual therapy, claiming that to do so could make a patient dependent upon this type of care, while others use only mobilization and manipulation, claiming that it gives a more rapid response. The true picture probably lies somewhere between the two extremes. There are certainly patients for whom mechanical therapy is too painful initially. These patients usually respond to mobilization to relieve pain and then to increase mobility, and this treatment may be followed by mechanical therapy and exercise therapy at a later date. Equally, there are patients who look upon manual treatment as a panacea which will always cure them, and so they feel they have no need to care for their own spine. For these patients, clearly mechanical therapy must be emphasized.
Mobilization and manipulation techniques for the lumbar spine
For the lumbar spine, there are two techniques (of literally thousands) which are especially valuable and will be briefly described. The first is the rotation movement (Fig. 13.19A). This is performed in the side-lying starting position, with the painful side uppermost, so that the pelvis is rotated away from the painful side. Both knees and hips and bent (crook-side lying) with the upper leg bending slightly more than the lower. The therapist stands behind the patient and imparts a grade I or II mobilization by rhythmically pushing on the patient’s pelvis, allowing the thorax to rock freely. With grades III and IV, the patient’s underneath arm is pulled through to rotate the thorax so that the chest faces more towards the ceiling. The upper leg bends slightly further so that the knee clears the couch side, and the lower leg is straighter to act as a pivot (increasing the flexion of the lower leg will flex the lumbar spine further). Therapist pressure is now over the pelvis and humeral head. This movement may be taken further to apply a manipulation. A lower couch position is used, and the end-range point of spinal rotation is maintained by the therapist pushing down on the patient’s pelvis and shoulder through straight arms, and in so doing applying slight traction. As the patient exhales, a high velocity, low amplitude thrust is applied. A tremendous number of variations exist to allow for alterations in range of motion, direction of rotation, and combined movements. These procedures are described in detail by Maitland (1986) and Cyriax and Cyriax (1983).
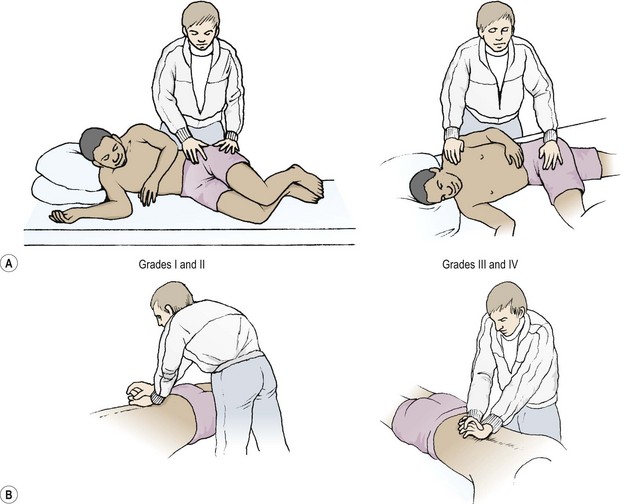
Extension movements in their simplest form may be produced by using posteroanterior pressures and derivatives of this technique (Fig. 13.19B). Posteroanterior central vertebral pressure (Maitland, 1986) may be performed with the patient prone. The pressure may be imparted with the pads of the thumbs, or the ulnar border of the hand (pisiform/hamate) pressing over the spinous processes. Movement is gradually taken up as the therapist moves his or her weight directly over the patient’s spine and an oscillation is begun. Variations include combined movements, unilateral pressures, bilateral pressure over the transverse processes, and the addition of hip extension among others.
Where the mobilization is taken to a grade V, joint manipulation occurs. Mobilization can be differentiated from manipulation in that the former is an oscillatory technique (typically at around 2 Hz) while the latter is a thrust. Usually an audible click or pop is heard (cavitation) with manipulation whatever velocity is used, and the cavitation effect has been said to be the only characteristic to distinguish manipulation from other spinal techniques (Evans and Breen, 2006).
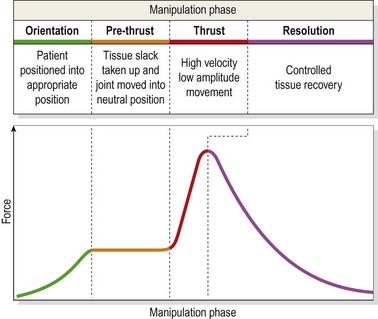
Typically manipulation is carried out in three or four phases (Herzog and Symons, 2001; Evans and Breen, 2006)—pre-thrust, thrust and resolution (Fig. 13.20). During the orientation phase the patient is positioned for comfort, safety and joint specificity of the manipulation force. The pre-thrust phase takes up tissue slack prior to the thrust procedure itself. Once cavitation has occurred, the tissues are released in a controlled fashion to prevent painful recoil of elastic soft tissue.
Manipulation effects
Manipulation is thought to have effects in four areas (Evans, 2002). The first is the release of trapped intra-articular material such as meniscoids in the spine or synovial folds in peripheral joints. These synovial folds have been shown to contain nociceptive nerve fibres (Giles and Taylor, 1987) and can therefore be a source of pain. Thrust manipulation gaps the facet joint (Cramer et al., 2000) reducing impaction and synovial trapping. The second effect is the relaxation of hypertonic muscle through sudden stretching. Thrust manipulation involving a sudden stretch has been shown to excite the motor pool (Herzog, Scheele and Conway, 1999). However, clinically reduction in spasm is seen and it has been suggested that this is a reduction of hypoalgesia of the dorsal horn in the spinal segment targetted by the manipulation (Vernon, 2000). Thirdly it is claimed that articular or peri-articular adhesions may be ruptured. It has been shown that the increased range of motion seen following thrust manipulation is independent of muscle tone. Using anaesthesia and muscle relaxants during surgery, Lewit (1985) demonstrated that cervical range of motion remained unchanged as muscle tone reduced, and suggested that this demonstrated an articular phenomenon in motion change following manipulative thrust. Following capsular tearing through trauma in sport, intra-articular haemorrhage followed by fibrosis is possible. However, targetting this type of motion reduction is more likely to respond to slower rate stretch (Evans, 2002).
The fourth area of manipulation effect is perhaps the most traditional, and that is an alteration or relocation of a displaced or subluxed joint. Biomechanical studies of vertebral motion following thrust manipulation demonstrate transient positional changes only (Gal et al., 1997) combined with a cavitation effect which gives the familiar click or pop heard following manipulation. Cavitation occurs in any synovial joint (Unsworth, Dowson and Wright, 1971), and is due to suction acting upon the synovial fluid. As the joint surfaces (in this case the facet joints of the lumbar spine) are separated, the contact area of the fluid changes forming a bubble which breaks as suction is continued. As the bubble collapses it forms a cloud of smaller bubbles and eventually vaporizes causing the familiar crack. Gas remains in solution for approximately 20 minutes following cavitation and during this time a second crack cannot be obtained from the same joint. This phase is known as the refractory period.
Nags and snags
Many patients who have disc lesions seem to respond well to techniques aimed at the facet joints. The connection between these seemingly dissociated conditions is a biomechanical one. As the disc bulges posteriorly, it causes the vertebrae to flex with a loss of lordosis. For this to happen, the facet joints must be mobile enough to open fully. However, in many cases, these joints are far from mobile, and the soft tissue surrounding them is placed on stretch, giving pain, which can be reduced using mobilization procedures.
Keypoint
A bulging disc will cause the vertebrae to flex and the facet joints to open. This will stress the soft tissues surrounding the joint giving pain which will respond to facet based mobilization techniques.
Mulligan (1989) described a number of procedures which combine manual and mechanical therapy, taking into account the planes of movement at the facet joints. In the lumbar spine, movement may be assisted using a sustained natural apophyseal glide (SNAG procedure) by applying therapist pressure over the spinous processes or articular pillars of the lumbar spine as the patient moves. SNAGs are weight-bearing mobilizations which are applied at end of range. They are applied simultaneously with movement, in line with the treatment plane (orientation of the articular surfaces) of the facet joint.
Flexion, extension or lateral flexion may be used either in sitting or standing. Either pisiform or thumb contact is used, and the direction of pressure is vertical in an attempt to separate, or at least assist separation of, the facets.
The starting position is with the patient sitting over the couch side (or standing) with the therapist behind. A belt is placed around the patient’s waist over the anterior superior iliac spines (this area may be padded with a towel if necessary). The patient is asked to flex forwards to the point of pain. They then back off slightly and the therapist applies the SNAG as the patient flexes again (Fig. 13.21A). If the correct level has been identified, the movement should be pain-free and of greater range. If pain persists, the level to be treated is changed, or a unilateral SNAG is performed over the articular pillar of the more painful side.

Keypoint
The movement should be less painful and of greater range when the SNAG is applied. If no change in pain or movement range occurs, change the vertebral level of application.
For extension, the patient is in the same starting position, but the couch is raised to afford the therapist a better mechanical advantage. The therapist stands slightly to one side in order to be clear of the patient as he or she extends back. The action must be lumbar extension, with the patient extending over the therapist’s hand, rather than extension of the whole spine on the hip with the patient pressing the whole bodyweight against the therapist’s hand (Fig. 13.21B). Rotation is performed with the patient stride sitting over the couch to fix the pelvis. The therapist grips around the patient’s trunk just above the painful level. Again, the overpressure is given with the ulnar border of the hand in the treatment plane (Fig. 13.21C).
The direction of motion and level of pressure application is decided both by the movement which is limited and the action which relieves the patient’s symptoms. As the patient moves, the vertical pressure is applied until end-range is obtained. Pressure is continued until the patient resumes the neutral position once more.
The sacroiliac joint
Structure
The three bones of the pelvis, the two innominates and the sacrum, form a closed ring. Anteriorly, the innominates join together at the pubic symphysis and posteriorly they join the sacrum via the sacroiliac joints (SIJ). Disorders of the pubic symphysis will often have repercussions on the SIJ, so examination should take place in both joints.
The sacral articular surface is shaped like a letter ‘L’ lying on its side, and is covered by hyaline cartilage, while the corresponding surface on the ilium is covered by fibrocartilage. The SIJ is a synovial joint, but its posterior surface is firmly secured by the interosseous ligament and so the joint may be considered as fibrous. There is great variation between individuals, in terms of the size, shape and number of articular surfaces, with 30% of subjects having accessory articulations between the sacrum and ilium (Grieve, 1976). With increasing age the joint becomes fibrosed and may eventually show partial bony fusion.
Movement
The normal SIJ does move. As the trunk is flexed, the sacral base moves forwards between the ilia and, with trunk extension in standing, the sacrum moves back again. The movement is usually only about 5 mm, but ranges up to 26 mm have been recorded (Frigerio, Stowe and Howe, 1974). Roentgen stereophotogrammetric analysis (RSA) has been used to assess SIJ motion. In this technique small metal (tantalum) balls less than 1 mm in diameter are implanted into the pelvic bones. Two synchronized x-ray tubes are then used to track free movement (Sturesson, Selvik and Uden, 1989; Sturesson, 2007). The accuracy of this technique is such that this technique is now considered the gold standard for orthopaedic research investigating small movements around joints. The SIJ research has shown that bone motion is not related to symptoms and that manipulation does not change bone motion, leading researchers to conclude that pain is inflammatory in nature. SIJ mobility in women is generally 30−40% greater than in men, but hypo- and hypermobility was not found. As the SIJ is loaded, motion is reduced and single leg standing coupled with spine extension maximally loads the joint through bodyweight and muscle action, perhaps making this a useful screening test during examination of back pain in sport.
Sacral motion is described as nutation and counter-nutation (Table 13.7). Nutation of the SIJ is an anterior tilting of the sacrum on the fixed pelvic (innominate or iliac) bones. The sacral base (top, flat area) moves down and forwards and the apex (point) moves up increasing the pelvic outlet. Nutation occurs as the lumbar lordosis increases and the iliac bones are pulled together impacting the SIJ. With counter-nutation the opposite movement occurs. It is a posterior tilting of the sacrum, with the base moving back and the apex (normally facing backwards) moving forwards and down. The pelvic outlet reduces and the pelvic bones move apart, distracting the SIJ. Counter-nutation occurs in non-weight bearing position and as the lumbar lordosis flattens.
Table 13.7 Movement of the sacroiliac joint (SIJ)
| Nutation | Counternutation |
|---|---|
 Anterior tilting of sacrum Anterior tilting of sacrum |
Posterior tilting of sacrum |
| Sacral base moves down and forward, apex moves up |
Sacral base moves up and back, apex moves down |
| Size of pelvic outlet increased, pelvic inlet decreased |
Pelvic inlet increased, outlet reduced |
| Occurs in standing |
Occurs in non-weight bearing position such as lying |
| Increased as lumbar lordosis increased |
Increased as lumbar lordosis decreased (flatback posture) |
| Iliac bones pulled together, SIJ impacted |
Iliac bones move apart, SIJ distracted |
| Superior aspect of pubis compressed |
Inferior aspect of pubis compressed |
From Norris (2000), with permission.
Definition
As the sacrum is a triangle pointed downwards, the sacral base is the large flat upper surface and the sacral apex the pointed lower portion. The sacrum and pelvic bones are joined together in a circle. The pelvic inlet is the space between the upper part of the bones and the pelvic outlet the space between the lower parts.
Postural asymmetry of the pelvis is common, and is evident when there is torsion of one ilium in relation to the other. On examination, one anterior superior iliac spine may be higher and one posterior superior iliac spine may be lower, for example. Unequal leg lengths, although normally asymptomatic, may cause the SIJ to become ‘blocked’, with a consequent alteration in gluteal muscle tone (Grieve, 1976). When shortening is more than 1–2 cm, torsion of the pelvis occurs with the ilium and sacral base on the side of the longer leg moving backwards and the pubis moving upwards. The degree of postural compensation between individuals will differ and so the pelvic position in reaction to altered leg length is variable.
Hormonal changes in pregnancy and, to a lesser extent, menstruation and menopause will also influence the SIJ. The general softening and relaxation of the pelvis leads to an increased range of motion which may remain for up to 12 weeks following childbirth. Local irritation of the SIJ leads to pain on gapping tests and limited hip abduction on the painful side. In addition, the lower PSIS is usually on the painful side.
Stability
The sacrum is inserted like the keystone of an arch, but seemingly the wrong way round, tending to be displaced rather than forced inwards with pressure. However, as the bodyweight is taken, the tension developed in the interosseous sacroiliac ligaments pulls the two halves of the pelvic ring together producing form closure (Fig. 13.22). In the sagittal plane the body weight falls ventral to the axis of rotation of the SIJ. This alignment would tend to rotate the sacrum forwards into a nutated position. During nutation the sacrotuberous ligament and the large interosseous ligament of the SIJ are tensioned, drawing the posterior part of the innominate bones together in a mechanism called self-locking. Counter-nutation disengages self-locking and so may lead to SIJ instability. Interestingly, because self-locking is disengaged during forward flexion of the trunk without a pelvic tilt (Lee, 1994), a stoop lift may dislodge the joint and is often a mechanism in SIJ pathology.
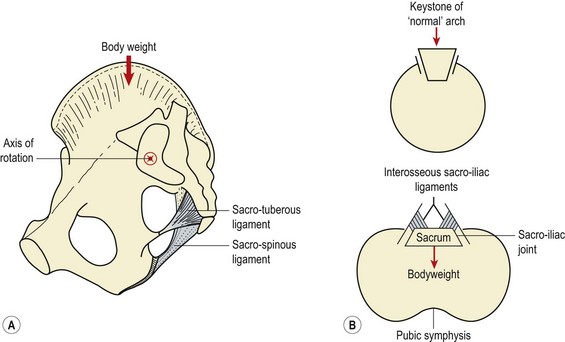
Figure 13.22 The sacroiliac joint. (A) Position. (B) Action in pelvic arch.
After Taylor and Twomey (1994), with permission.
Although no strong muscles cross the SIJ, the joint may be actively stabilized by a combination of forces acting over the joint, a process called force closure. The sacrotuberous ligament (sacrum to ischial tuberosity) and the long dorsal sacroiliac ligament (sacral segments 4/5 to posterior inferior iliac spine) blend to form an expansion measuring 20 mm wide by 60 mm long. This expansion attaches to the posterior layer of the thoracolumbar fascia (TLF) and to the aponeurosis of the erector spinae, and a number of other muscles have important tensioning effects in this area (Vleeming et al., 1995; Vleeming et al., 1997). Five stabilizing systems are described involving trunk and lower limb muscles coupling with lumbosacral fascia and ligaments (Fig. 13.23). These muscle–fascial couplings give the therapist the opportunity to use muscle re-education to stabilize the SIJ during rehabilitation (Treatment note 13.1).
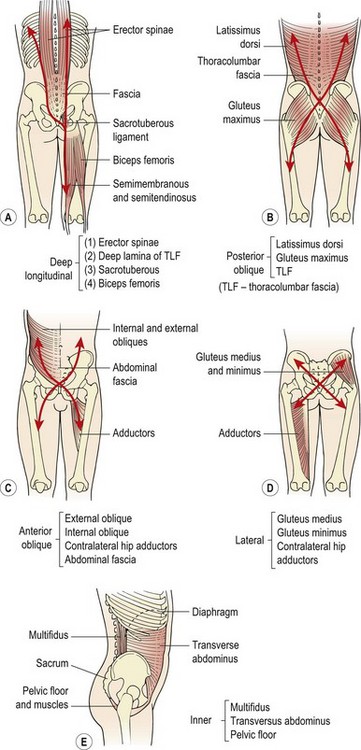
Figure 13.23 Sacroiliac joint stabilization—muscle/fascia coupling. (A) Deep longitudinal muscle system, (B) posterior oblique, (C) anterior oblique, (D) lateral, (E) inner.
From Magee (2002), with permission.
Treatment note 13.1 Lumbar stabilization starting positions
Muscle isolation
The lumbar stability programme begins with muscle isolation. The aim is to teach the correct abdominal hollowing (AH) action, avoiding substitution strategies such as breath holding, rectus abdominis and external oblique dominance, and obvious ribcage movement. Four starting positions may be used, and the one which is most suitable for the patient forms the basis of the programme progression (see Table 13.10).
Table 13.10 Starting positions for abdominal hollowing
From Norris CM (2000) Back Stability Human Kinetics Champaign Illinois with permission.
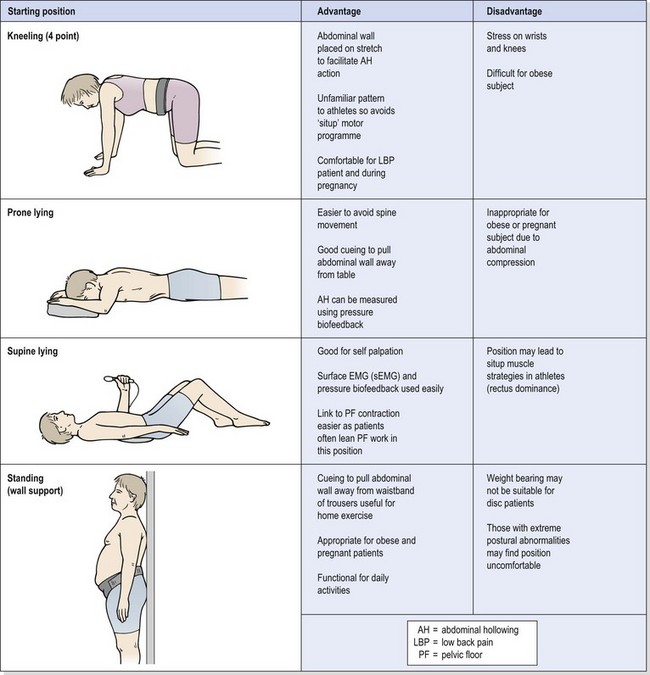
The four point (prone) kneeling position has the advantage that it is comfortable on the spine and is particularly suitable after low back pain or following/during childbirth. In addition, as it is an unfamiliar position for abdominal exercises, the position will not encourage a ‘sit-up motor programme’—that is, dominance of the rectus abdominis. This makes the position suitable for use with athletes where the aim is to reduce the reliance on the rectus. As abdominal hollowing is performed the abdominal wall is pulled upwards and a belt may be used to cue this movement, enabling the patient to pull away from the belt. This action is likely to be difficult for obese individuals simply because they have a greater tissue mass to lift, so another starting position may be more appropriate.
Prone lying (lying on the front) supports the back completely and avoids the ‘rocking’ action which some patients find it difficult to control in kneeling. In addition, as the abdominal wall is pulled away from the floor, cueing is provided, and a pressure biofeedback unit may be used to monitor the effect. Again the starting position may not be suitable for an obese subject as tissue mass makes movement initiation difficult.
Supine lying (lying on the back) enables the subject to self-palpate and the use of sEMG also adds to self-measurement. In addition, supine lying is the position often used for retraining pelvic floor (PF) muscle action and linking abdominal hollowing to PF muscle work is a useful method of initiating deep abdominal action. In athletes, however, close supervision will be required as there is a tendency to recruit the rectus abdominis and even to lift the head in this position.
Standing against a wall is most suitable for obese subjects as they can pull the abdominal wall away from a belt (or waistband of the trousers) with minimal muscle work which becomes very motivating. In addition, for those unfamiliar with exercise, standing activities are often better tolerated. Because the position is weight bearing, however, those with acute low back pain may not be able to tolerate prolonged standing and a lying starting position may be more suitable for them.
Examination
Subjective examination usually reveals a unilateral distribution of symptoms, perhaps spreading to the buttock, lower abdomen, groin or thigh, although pain may be referred to the foot. The traumatic history is frequently one of a fall, landing on the ischial tuberosity, with patients unable to walk distances without marked pain. The footballer in a mistimed sliding tackle or the youngster who falls while ice-skating are prime examples. In any sport where the range of motion required at the hip is great or repetitive unilateral leg movements are performed, SIJ irritation may be encountered. Tensile forces are increased with jumping activities onto both legs, while shear forces are raised with single leg activities, such as running and hopping. Dancers, gymnasts and high-jumpers are particularly prone to SIJ involvement, but any athlete may suffer trauma to the joint leading to local inflammation or mechanical disturbance.
Objective examination of the pelvis and SIJ is made initially with the patient standing. The general bony alignment and muscle contour is noted. The patient may be reluctant to take weight through the affected leg, and may walk with a limp. Loss of gluteal and abdominal muscle bulk has also been reported (Wells, 1986). The level of the gluteal folds and gluteal cleft is noted, as is that of the iliac crests and iliac spines.
Motion (kinetic) tests
Motion tests of the SIJ are used to assess the side of the body with the predominant dysfunction, and therefore the side to treat (Turner, 2002). They assess the contribution of the SIJ to general pelvic motion and are used before and after a treatment technique to determine effectiveness. Importantly, motion tests cannot accurately by themselves be used to determine the nature of a dysfunction or to imply that an altered motion test is a cause of pain. In addition, they cannot indicate whether a joint is ‘stiff’ or ‘locked’.
Two motion tests for the SIJ are typically used in sport, hip flexion in standing and forward flexion in standing (Fig. 13.24).
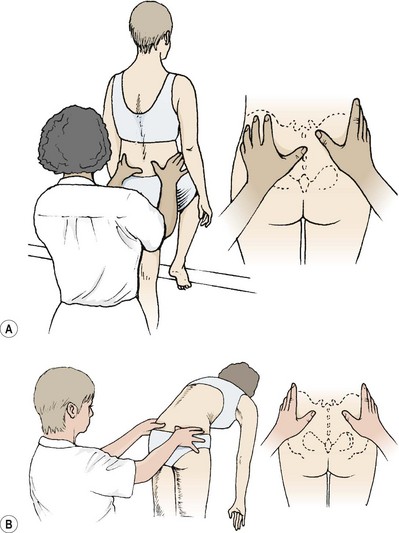
Figure 13.24 Motion tests of the sacroiliac joints. (A) The right PSIS should move caudally as the leg is lowered back to the ground. (B) Joint asymmetry. If one joint is lower, as the patient flexes it will move cephalically (Piedallu’s sign).
These tests may be used to guide manual therapy techniques but should not be used in isolation diagnostically (see below).
Palpation
Motion tests of the SIJ which rely on palpation have been shown to be unreliable (Laslett, 1997) and are only of real clinical use when used in parallel with other forms of objective examination. In a study of 45 patients using experienced manual therapists to assess six commonly used palpation tests, the maximum reliability was only fair, and in some tests the reliability was worse than that obtained through chance (van Duersen et al., 1990). Dreyfuss et al. (1992) found that as many as 20% of asymptomatic individuals gave a false positive on the standing or seated flexion tests, and Potter and Rothstein (1985) used experienced manual therapists to test 13 palpatory tests and found that simple agreement on the tests was less than 70% on most of the procedures.
Pain provocation tests are, however, more reliable. Laslett and Williams (1994) assessed 51 patients with six SIJ tests and found that interexaminer agreement was over 94% for the femoral thrust, and 88% for pelvic torsion (Gaenslen’s test), distraction and compression tests. These four tests are shown in Fig. 13.25.
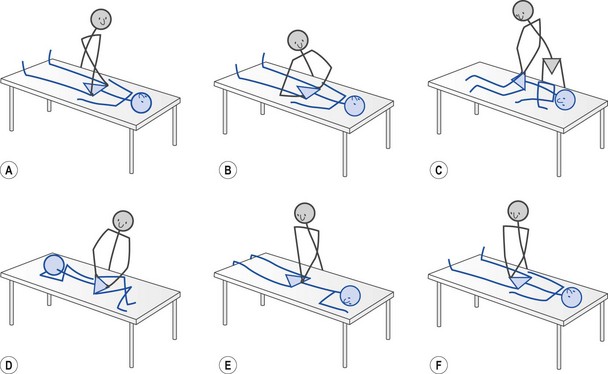
With persistent bilateral SIJ pain, the possibility of ankylosing spondylitis should be considered. The range of motion, especially lateral flexion, of the lumbar spine is limited, and muscle spasm may be evident. Where costovertebral involvement is present, chest expansion will be affected—often an early sign. The use of radiographs, erythrocyte sedimentation rate (ESR), and the presence of the antigen HLA B27 aid the diagnosis.
Change in leg length as SIJ assessment
A change in leg length may be used as an assessment of SIJ dysfunction (Don Tigny, 1985). The leg length change occurs because altered position of the innominate bones will also change the resting position of the acetabulum, placing it more proximal or distal and consequently altering leg length. The tests are used to identify a reduction in self-locking of the SIJ through nutation (anterior rotation) of the sacrum on the innominates.
Initially patients are positioned in crook lying and they are instructed to form a bridge and to place the hips back onto the couch. The therapist then passively extends the legs and compares leg length by palpating the undersurface the malleoli with the edge of the thumbs. The patient then performs a straight leg sit-up action (they may assist themselves by pulling on the couch with their hands) and the leg length is again assessed. If the leg gets longer (lying to sitting) it indicates a posterior innominate on the side of the longer leg, and if the leg gets shorter the indication is of an anterior innominate (Fig. 13.26).
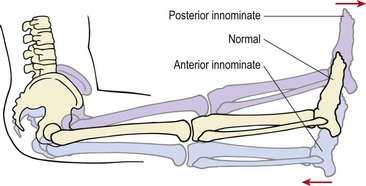
Treatment is aimed at the more painful side. Where anterior rotation occurs (leg shorter) the treatment is to posteriorly rotate the innominate (see below). Where anterior rotation has occurred (leg longer) it is thought that an upslip has occurred and this should be treated using leg traction (Turner, 2002).
Positional faults of the innominates
Three main positional faults occur in the SIJ, anterior innominate (common), upslip (common) and posterior innominate (less common) (Fig. 13.27). A variety of other appearances occur but they are not as frequently seen in day-to-day clinical practice. The reader is referred to Lee (1994) for further information.
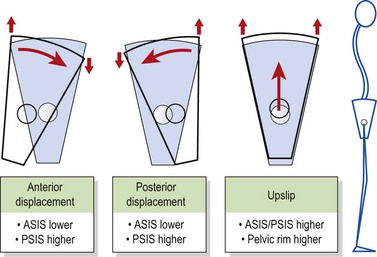

Assessment of SIJ stability
The SIJ is stabilized both passively (form closure) and actively (force closure). Failure of the stabilizing mechanisms may be assessed using the active straight leg raise (ASLR) test (Mens et al., 1997). The test first identifies SIJ stability, but, importantly, can also be used to highlight the most appropriate way to stabilize the joint and provides a valuable tool for the reassessment of the treatment intervention. It is therefore the assessment of choice for functional rehabilitation of SIJ dysfunction.
Keypoint
The active straight leg raise (ASLR) test is the assessment of choice for functional rehabilitation of SIJ dysfunction.
The patient is asked to actively lift the leg by 5 cm, keeping it straight, by engaging the hip flexor muscles. Weakness and/or pain on this movement on one side of the body indicates poor dynamic stability of the SIJ (force closure). The test is then performed again while the therapist assists form closure by: (i) compressing the pelvic rims, and (ii) using minimal posterior pelvic tilt (innominate rotation) on the ipsilateral side. Where these techniques reduce pain and increase strength, a SIJ belt should be used initially until force closure has been enhanced. To assess force closure the ASLR test is repeated while engaging the muscle–fascial systems shown in Fig. 13.24. For the inner system the transversus abdominis is contracted (abdominal hollowing), for the posterior oblique system the latissimus dorsi is engaged (resisted shoulder adduction).
The ASLR test has been demonstrated radiographically to alter alignment of the pelvic ring using pubic malalignment as a measure. ASLR of the normal limb shows no step deformity across the pubic ramus, but with the symptomatic limb, step deformity of 5 mm together with anterior innominate rotation has been recorded (Mens et al., 1997). In addition, the same study demonstrated that over 70% of symptomatic patients showed less strength in the ASLR and 80% of these showed strength improvement with a SIJ belt. In addition, in all but one patient the ASLR was more powerful with posterior rotation pressure over the ipsilateral ASIS.
Management of sacroiliac pain
In sport three treatment techniques for SIJ pain are particularly useful: manual therapy, exercise therapy and dry needling. As we have seen, manipulation does not cause movement at the SIJ, but both manipulation and mobilization are effective techniques for SIJ and pelvic pain. Lumbar rotator mobilization may be modified to affect the SIJ into the classic ‘gapping’ technique (Fig. 13.29A). The patient is positioned with the painful side uppermost, and the trunk rotated so that the shoulders rest close to the couch. The upper knee is drawn over the couch edge and fixed into position using the therapist’s body. The therapist uses their forearms as contact points, pressing the cephalic arm onto the lower ribs to fix body position and the caudal arm onto the iliac crest to apply the oscillatory mobilization or manipulative thrust. The direction of pressure is downwards and slightly forwards, aiming the line of force to the near couch edge.
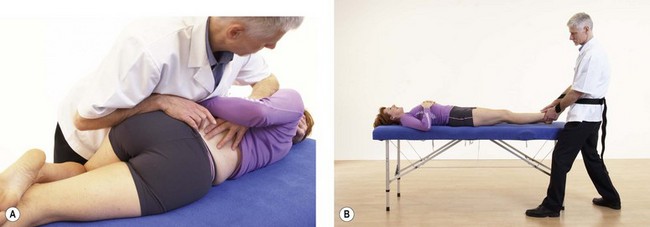
Distraction of the pelvic region is achieved using leg traction applied through a belt (Fig. 13.29B), in the ‘leg tug’ or longitudinal mobilization procedure. The patient lies supine with their feet at the end of the couch. The therapist fixes the patient’s foot of the unaffected side with their knee to stop the patient sliding down the couch. The ankle of the affected side is grasped using a figure-of-eight belt grip. Traction is applied as the therapist leans back which may be sustained, oscillatory or converted into a thrust.
Dry needling into the interosseous ligament, periosteal needling (pecking) over the posterior superior iliac spine and prolotherapy are all used successfully for SIJ treatment. Cusi et al., (2008) reported positive clinical outcomes in 76% of patients using three injections of hypertonic dextrose into the dorsal interosseous ligament assessing outcomes using standard questionnaires, ASLR, single leg standing and the posterior pelvic pain provocation test.
Stability exercise is used extensively in management of the SIJ and the muscle-fascia slings may be worked using variations of the hip hinge action with the legs straight (good morning exercise) or bent (dead lift exercise) shown in Fig. 13.30A&B.
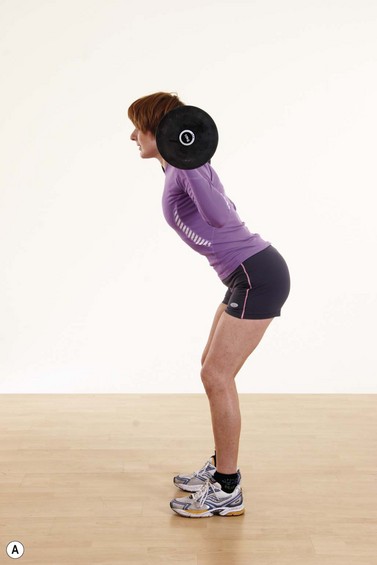

Spondylolysis
Spondylolysis is a defect in the neural arch (pars interarticularis), in 90% of cases between the lamina and pedicle of the fifth lumbar vertebra (Fig. 13.31). It is a fracture of the pars without slippage, and by the age of 7 years is present in 5% of the population (Reid, 1992). In athletes, however, the incidence may be as high as 20%, and it is often associated with other lumbar anomalies (Hoshina, 1980). Diagnosis is by bone scintigraphy often combined with MRI. In the clinic the single leg extension test may be used to recreate symptoms, but is not sensitive or specific for the detection of the active condition (Masci et al., 2006).
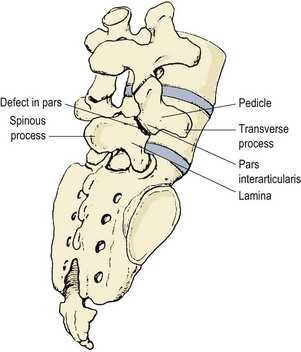
Keypoint
Bone scintigraphy is a method of assessing blood flow and metabolism of bone. A radioactive tracer is given to the patients and taken up by the bone. The rate and distribution of the tracer indicates affected bone areas.
The single leg extension test (stork extension) is performed by having the patient stand on one leg (affected side) and extend the spine to arch backwards. Compression and extension is imparted to the lumbar region. This may be combined with a quadrant test combining extension, lateral flexion and rotation of the lumbar spine to the painful side to maximally stress the region to reproduce the patient symptoms.
Where symptoms are present but no deformity is detectable on x-ray or bone scan, a pars interarticularis stress reaction has occurred without cortical interruption (Weber and Woodall, 1991). At one stage a congenital defect was thought to be present. However, the condition is not present from birth and increases in incidence with age. Furthermore, the ossification centres of the vertebra do not correspond to the position of the defect. Familial tendencies do exist, and racial differences have been described (Colcher and Hursh, 1952).
The most important consideration from the point of view of sport is that of trauma. Direct trauma may result in a non-union of the area or, more likely, a stress fracture forms over a prolonged period, especially as a result of repeated flexion overload, hyperextension or shearing stress to the lumbar spine. Athletes with hypolordosis in the lumbar spine are at risk from flexion overload whereas those demonstrating hyperlordosis may suffer the condition as a result of forced rotation causing torsion overload (Farfan, Osteria and Lamy, 1976). The pars interarticularis is positioned as a pivot between the disc and facet joints, and so is subjected to considerable stress. The condition has been described in weight-lifters and oarsmen (Kotanis et al., 1971), hockey players (Letts et al., 1985), gymnasts (Weber and Woodall, 1991) and fast bowlers (Williams and Sperryn, 1976; Becker, 2006).
Keypoint
Spondylolysis can form over a prolonged period, usually as a result of repeated flexion, hyperextension or shearing stresses imposed on the lumbar spine.
Repeated stress can lead to microfractures, especially if overtraining has occurred. As these heal they produce an elongated appearance of the bone. Lumbar pain is apparent; this may be unilateral or bilateral but is rarely associated with nerve root compression. Pain is experienced first with hyperextension, such as walk-over movements in gymnastics, and increases in intensity. Pain is aggravated by hyperextension or rotation, and may present with paraspinal muscle spasm. Unilateral pain may be reproduced using the single leg extension test and quadrant test described above, as these movements compress the pars interarticularis (Weber and Woodall, 1991). Flexion is normally painless although pain may occur as the athlete returns to standing. Oblique x-rays give the classic ‘terrier dog’ appearance (Fig. 13.32) with the dog’s collar represented by the pars interarticularis defect, which is bridged by fibrous tissue rather than bone. A negative x-ray does not rule out spondylogenic conditions, and a bone scan may be required (Ciullo and Jackson, 1985).
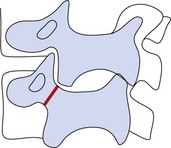
Figure 13.32 An oblique x-ray of the lumbar spine, which has the appearance of a terrier dog. In the lower segment a spondylolysis through the pars interarticularis appears as a collar around the dog’s neck.
From Corrigan and Maitland (1983), with permission.
Spondylolisthesis
Spondylolisthesis is an anterior shift of one vertebra on the other, usually L5 on S1. In sport, the condition is usually a progression from spondylolysis, but it may also occur in the elderly as a result of degeneration, or congenitally in association with spina bifida. The first degree injury involves slippage to a distance of one quarter the vertebral diameter, but further movement may occur up to a fourth degree injury which involves a full diameter displacement (Corrigan and Maitland, 1983). The major symptom is of back pain referred to the buttocks which is aggravated by exercise. Sciatica may be present as the condition is associated with disc protrusion in 5% of cases (Williams and Sperryn, 1976). The alteration in spinal alignment causes dimpling of the skin and extra skin folds above the level of injury. A step deformity to the spinous process at the lower level is normally apparent to palpation. The lordosis is usually increased, and severe spasm of the erector spinae may be present. Lumbar extension is often severely limited, and passive intervertebral pressure over the spinous process at the affected level is painful.
Figure 13.33 shows x-rays of spondylolisthesis. Figure 13.33A shows a grade 1 defect with mild forward slippage of L5 on S1. Figure 13.33B shows a grade 3 lesion with greater slippage, gapping of the neural arch and osteophyte formation on the vertebral body. To palpation a step deformity may be apparent with changes to skin folds in the area.
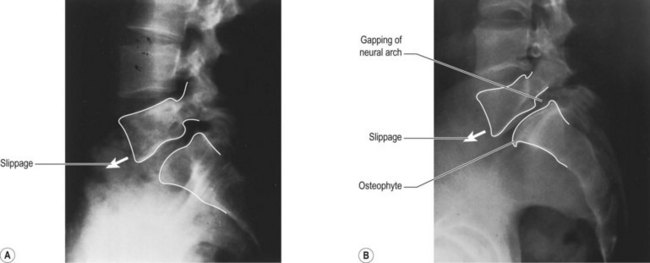
Figure 13.33 Spondylolisthesis of L5 and S1. (A) Grade 1 defect with mild forward slippage of L5 on S1. (B) Grade 3 defect showing greater slippage, gapping of the neural arch and osteophyte formation.
Reproduced from Magee, D.J. (2002) Orthopedic Physical Assessment, 4th edn, Saunders, Philadelphia.
Management of spondylogenic disorders
Treatment aims mainly to eliminate the symptoms of the condition rather than to obtain bony union. Initially, rest is required. This varies from ‘active rest’ by avoiding painful movements with mild conditions to total bed rest with very severe lesions. Occasionally, braces and casts are used to protect the spine until the acute pain subsides, but the most important component of management is closely supervised exercise therapy. Thorough functional assessment is carried out to investigate strength and flexibility. In addition to absolute values in comparison to norms for a particular athlete population, muscle imbalance is important. Transmission of ground forces to the spine is governed to a large extent by hip and spine musculature, and weakness or asymmetry here must be corrected. Anterior shear forces are compensated by an extension moment created by the abdominal muscles (especially the internal obliques and transversus) and the latissimus dorsi pulling on the thoracolumbar fascia. In addition, the paraspinals counteract shear forces in the lumbar spine (Farfan, Osteria and Lamy, 1976).
Correction of muscle imbalance which results from asymmetry in sport is important in the management of this condition. For example in cricket, fast bowlers have a high incidence of lumbar spondylolysis (1.65/1000 balls bowled) (Gregory, Batt and Wallace, 2002). Forces through the front leg may be up to nine times bodyweight vertically and two times bodyweight horizontally (Foster et al., 1989) and this may be repeated for up to 10 overs each of 6 balls (Becker, 2006). Asymmetry of the quadratus lumborum (QL), an important stabilizing muscle, has been shown in bowlers with the QL being larger on the ipsilateral side to the bowling arm. This correlates with injury where 80% of unilateral spondylolyses have been shown to occur on the contralateral side to the bowling arm, perhaps reflecting poor stability due to a weaker QL (Becker, 2006).
The use of a stability programme based on motor control has been shown to be effective in the management of this disorder (Sullivan et al.: O’, 1997). A 10-week specific stability programme was shown to be more effective than conventional exercise programmes involving gym work, sit-ups and swimming using measures of pain intensity, pain description and functional ability. In addition, the benefits of specific stabilization training was maintained at a 30-month follow-up.
Spinal stability
Evaluation
When the lumbar spine demonstrates instability, there is an alteration of both the quality and quantity of movement available within a vertebral segment. The unstable segment shows decreased stiffness (resistance to bending) and as a consequence movement is increased even under minor loads. Clinical assessment may reveal a number of classical physical signs as outlined in Table 13.8.
Table 13.8 Evaluating lumbar instability
| Classical physical signs | Evaluation based on movement dysfunction |
|---|---|
ASLR—active straight leg raise; PBU—pressure biofeedback unit; P4 − posterior pelvic pain provocation.
Paris (1985), Maitland (1986), Fritz et al (2007), Norris (2008).
Table 13.9 Integrated back stability model
| Phase | Content |
|---|---|
| Correction of movement dysfunction | |
| Development of back fitness | |
| Functional restoration |
Further examination is required to determine the level of loss of motion control, and tests focus on the reduction of symptoms when the spine is actively stabilized, and the subject’s ability to maintain a neutral lumbar posture. The former may be assessed using the prone instability test, the latter using pressure biofeedback. Where the patient has recently had a child (post-partum) the posterior pelvic pain provocation (P4) test and active straight leg raise (ASLR) may also be used to assess instability of the lumbopelvic region in general.
For the prone instability test (Fig. 13-34A,B) the patient lies prone with their chest supported on a treatment couch and legs resting on the floor. The patient’s pain is provoked using a posteroanterior (PA) pressure upon the spinous processes of the lumbar spine. They are then asked to lift the legs clear of the ground, and the test is positive if the muscle work of this action (hip extensors and spinal extensors) reduces their lumbar pain. The pressure biofeedback test is described below.


General principles
To maintain spinal stability, three inter-related systems have been proposed (Fig. 13.35). Passive support is provided by inert (non-contractile) tissues, while active support is from the contractile tissues. Sensory feedback from both systems provides coordination via the neural control centres (Panjabi, 1992). Importantly, where the stability provided by one system reduces, the other systems may compensate. Thus the proportion of load taken by the active system may increase to minimize stress on the passive system through load-sharing (Tropp, Alaranta and Renstrom, 1993). When this happens, we can view stability as a continuously varying process (Bergmark, 1989). This process is dynamic and quite different to the traditional view of clinical stability being a static mechanical state (stable or unstable).
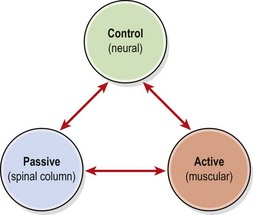
Figure 13.35 The spinal stabilizing system consists of three interrelating subsystems.
From Panjabi, M.M. (1992) The stabilizing system of the spine. Part 1. Function, dysfunction, adaptation and enhancement. Journal of Spinal Disorders, 5(4), 383–389. With permission.
Keypoint
Instability of the lumbar spine occurs when there is a decreased stiffness (resistance to bending) of a spinal segment. As a result, excessive movement occurs, even under minor loads.
The concept of a dynamic interrelating system gives the physiotherapist the opportunity to reduce pain and improve function by rehabilitating active or functional lumbar stabilization. Such improvement may be accomplished by augmenting both the active and neural control systems. Simply developing muscle strength is insufficient. Moreover, many popular strength exercises for the trunk actually increase mobility in this region to dangerously high levels (Norris, 1993; 1994a). Rather than improving stability, exercises of this type may reduce it and could therefore increase symptoms, especially those associated with inflammation.
Developing active lumbar stability
The original approach to lumbar stabilization was to focus on muscle isolation. However, this approach has been shown in many cases not to be effective (Koumantakis et al., 2005) leading to the development of an integrated approach (Norris, 2008; Norris and Mathews, 2008) which draws on evidence from several sources. The integrated back stability (IBS) approach is used in three overlapping phases (Fig. 13.36). During phase one movement dysfunction is addressed, prior to building back fitness in stage two. The final phase is functional restoration.
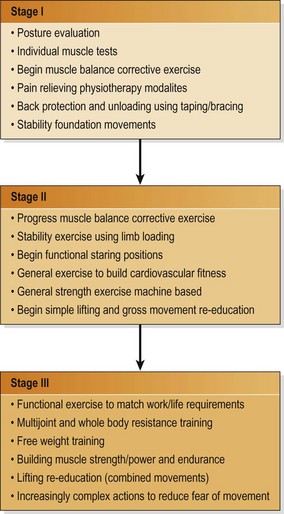
Norris, C.M and Matthew, M. (2008) The role of an integrated back stability program in patients with chronic low back pain. Complementary Therapies in Clinical Practice, 14, 255−263.
Phase I
Phase one initially focuses on pain relief, using physiotherapy modalities. This is because patients will find it difficult to perform exercise in the presence of pain inhibition. Posture evaluation and muscle balance tests are used to determine exercises which target postural changes relative to the patient’s symptoms. For example, where a patient has a flat back posture lumbar extension is used and for a patient with a lordotic posture lumbar flexion is the exercise of choice. At this stage correction of muscle imbalance forms a major part of the programme only if it is relevant to symptoms. In the lordotic posture, for example, the iliopsoas muscle may be found to be tight. Where this limits the patient’s ability to correct their lordotic posture and facet joint impaction is considered a potential source of pain, the iliopsoas will be stretched to enable the patient to posteriorly tilt their pelvis and disengage the lumbar facets.
Stability foundation movements are begun using isolation of the lumbar stabilizing muscles, with the aim of gaining voluntary control over these muscles. The muscles we are interested in are the deep abdominals, the gluteals and the intersegmental muscles of the spine, especially multifidus. These muscles often function poorly after injury, and may be incorrectly recruited as a result of intense training activities, which leads to muscle imbalance. When this happens the mobilizer muscles of the lumbopelvic region (rectus abdominis, hip flexors and hamstrings) often dominate movements with the stabilizers being poorly recruited. The focus of the back stability programme, therefore, is to reduce the dominance of the mobilizer muscles and enhance the function of the stabilizers.
The process starts with abdominal hollowing taught traditionally in a prone kneeling position with the spine in its neutral (mid-range) position (slight lordosis). As the transversus abdominis has horizontally aligned fibres, this action allows the abdominal muscles to sag, giving stretch facilitation. The patient focuses attention on the umbilicus and is instructed to pull the umbilicus ‘in and up’ while breathing normally. This action has been shown to dissociate activity in the internal obliques and transversus from that of rectus abdominis (Richardson, 1992), making the exercise especially useful for re-educating the stability where rectus abdominis has become dominant.
To facilitate learning, multisensory cueing is used (Miller and Medeiros, 1987) to increase the sensory input to the patient. Auditory cues can be provided by the therapist speaking to the subject and giving feedback about performance. Visual cues are given by encouraging the subject to look at the muscles as they function, and by using a mirror. Kinaesthetic cueing is accomplished by encouraging the subject to ‘feel’ the particular action, for example, to ‘feel the stomach being pulled in’. Tactile cues are provided by the therapist touching the subject’s abdomen as muscle contraction begins.
The action is held for 2 seconds initially, building to 5, 10 and eventually 30 seconds, breathing normally. Although initially the action may demand high levels of muscle work to facilitate learning, the eventual aim is to use minimal muscle activity. A useful teaching point is to contract the abdominal muscles as hard as possible and then to relax by half (50% MVC) and then half again (25% MVC). The therapist should monitor the ribcage to ensure that is does not move substantially, and the feeling should be one of the umbilicus drawing inwards and slightly upwards rather than of bulging (doming) or spinal flexion.
Once this has been achieved, the holding capacity of these muscles is built up until the patient can maintain the contraction for 10 repetitions, each held for 10 seconds (Richardson, 1992). Several other starting positions may be used (see Treatment note 13.1) and the most suitable position is chosen for the particular patient being treated.
Several errors can occur when a patient practises abdominal hollowing. Essentially, the rib cage, shoulders and pelvis should remain still throughout the action. The contour of the abdomen will flatten if a deep breath is taken and held, but the therapist should see the chest expansion involved. Where this occurs, the patient is instructed to exhale and hold this chest position as the exercise is performed. Placing a belt around the lower chest is useful to give feedback about chest movement (Richardson and Hodges, 1996).
Another substitution action is to use the external oblique to brace the abdomen. However, these muscles will pull on the lower ribs and depress them at the same time, slightly flexing the thoracic spine. A horizontal skin crease is often visible across the upper abdomen. Where this occurs, the patient is encouraged to perform pelvic floor contraction at the same time as abdominal hollowing. Simultaneous contraction of the gluteus maximus must be avoided with this action, as this will teach an inappropriate motor pattern for trunk stability during dynamic sports activity.
Keypoint
When performing the abdominal hollowing action, monitor the patient’s lower ribs. As the action is performed the ribs should stay still and neither raise nor lower.
Use of pressure biofeedback
Restoration of the abdominal hollowing mechanism can also be enhanced by the use of pressure biofeedback (Chattanooga Group Limited, Bicester, England). The biofeedback unit consists of a rubber bladder and pressure gauge similar to a sphygmomanometer.
Prone lying
In prone lying, the pressure biofeedback unit is placed beneath the abdomen with the lower edge of the bladder level with the anterior superior iliac spine, and the centre of the bladder over the umbilicus. The unit is inflated to 70 mmHg, and abdominal hollowing is performed. The aim is to reduce the pressure reading on the biofeedback unit by 6–10 mmHg, and to be able to maintain this contraction to repetition (10 repetitions of 10-second hold) to ensure that endurance of the target muscles is adequate (Richardson and Hodges, 1996).
Crook lying
As a further test, a crook lying position is used. The bladder of the unit is placed beneath the subject’s lumbar spine and inflated to show a constant figure of 40 mmHg. The subject is instructed to contract the abdominal muscles without performing a posterior pelvic tilt. If the lordosis is unchanged, a constant pressure is shown on the pressure unit. Increasing pressure shows flattening of the lordosis (lumbar flexion), while reducing pressure shows increased lordosis (lumbar extension). Excessive motion in either direction represents loss of lumbar stability. Alteration of starting position and the addition of simultaneous limb movement encourages body awareness and movement control.
Heel slide
The ability of the deep abdominals to maintain spinal stability may be accurately assessed using the heel slide manoeuvre. The subject starts in crook lying with the spine in a neutral position and the pressure biofeedback unit positioned beneath the lower spine. One leg is then gradually straightened, sliding the heel along the ground to take the weight of the leg. During this action, the hip flexors are working eccentrically and pulling on the pelvis and lumbar spine. If the strong pull of these muscles is sufficient to displace the pelvis, the pelvic tilt is noticeable by palpation of the anterior superior iliac spine (ASIS) and by an alteration of the pressure biofeedback unit. The action must be completed without using the substitution actions described above.
Multifidus muscle retraining (see also Chapter 5)
Measurement and enhancement of multifidus function is begun in prone lying. The fibres of multifidus are palpated medial to the longissimus at L4 and L5 levels. The spinous processes are identified and the fingers then slide laterally into the hollow between the spinous process and the longissimus bulk. The difference in muscle consistency is assessed, and then the patient’s ability to isometrically contract the multifidus in a ‘setting’ action is determined. The patient is encouraged to use multifidus setting in a sitting position with a neutral lumbar spine. Palpation is with the therapist’s thumb and knuckle of the first finger placed on either side of the lumbar spinous process at any one level. The instruction to the patient is to ‘feel the muscle swelling’ without actively flexing the lumbar spine. The patient’s own thumbs may be used to give feedback for home practice. Surface electromyography (sEMG) can also be used as the multifidus is superficial at this level. Multifidus function may also be enhanced using manual therapy techniques such as rhythmic stabilization.
Spasm of the multifidus has been proposed as a factor in many instances of chronic low back pain (Gunn, 1996). In addition to manual therapy techniques and dry needling (see Norris, 2001), muscle re-education may be used to restore normal function of the muscle. Contraction and relaxation of muscle is a familiar treatment protocol for pain reduction in muscles such as the upper trapezius for example. The same method would seem to apply to the multifidus.
Phase II
The second phase of the IBS programme is to build back fitness. Once the stable base has been established in phase I movements of the arms and legs are superimposed. For example, following abdominal hollowing in crook lying, the next exercise progression would be the heel slide (Fig. 13.37A). The patient performs the hollowing action, and while maintaining the neutral lumbar position, one leg is straightened, sliding the heel along the ground. The action of the hip flexors in this case tries to tilt the pelvis forwards (iliacus) and increase the lordosis (psoas). The abdominal muscles must work hard to stabilize the pelvis and lumbar spine against this pull. A number of other movements may be used including the bent knee fallout (Fig. 13. 37B), which works for rotary stability, and bridging actions (Fig. 13. 37C, D and E), which combine abdominal work with gluteal actions.
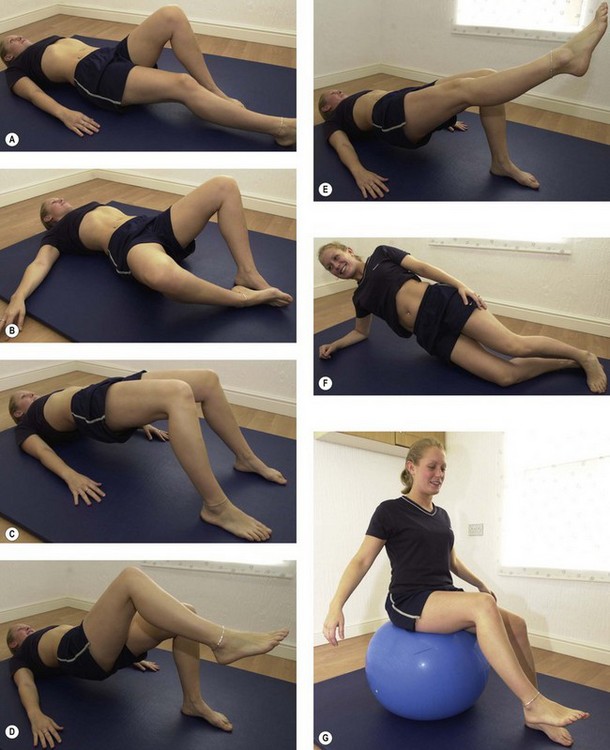
Figure 13.37 Lumbar stabilization exercises. (A) Abdominal hollowing with heel slide. (B) Bent knee fallout. (C) Bridging. (D) Single leg bridge. (E) Single leg bridge with leg straightening. (F) Side support. (G) Gym ball.
During phase II, dynamic movements of the spine are also used. Now the aim is to maintain both static (neutral position) and dynamic (lumbopelvic rhythm) alignment. Actions such as the trunk curl and hip hinge are useful, as are more traditional lumbar exercises involving rotation. A variety of additional movements may be used with the aim in each case of maintaining correct alignment of the spine through range and building holding capacity.
Side support movements (Fig. 13. 37F) work the quadratus lumborum and trunk side flexors which are important stabilizers in single handed carrying tasks especially.
In this phase general cardiovascular (CV) fitness is also built up and general strength exercises for the upper and lower limbs used. Strength in the limb muscles is vital for spinal health as the power of lifting should come from the legs rather than the spine. Upper limb strength is used for object positioning during manual handling and to bring the object close to the body to reduce leverage effects imposed upon the spine.
Phase III
When movement dysfunction has been corrected and back fitness enhanced, the athlete is required to maintain or adopt the stable position only when it is required, relaxing at times when the spine is not under stress. For this to occur, muscle reaction time must be reduced through proprioceptive training in functional positions. The aim here is to move the spine out of alignment and impose stress upon it so that the stabilizing muscles react quickly to realign the spine and protect it from excessive stress, in a similar approach to that used for the ankle and knee.
More complex activities can now be used which draw the subject’s attention away from the spine and into the environment. The aim now is to use proprioception to monitor the position and stability of the spine so that stability becomes more automatic and less attention demanding.
More complex resistance training appropriate to individual sporting requirements may also be used (Fig. 13.38). The correct relationship between lumbar alignment and pelvic alignment must be rigorously maintained. A convex contour of the abdominal wall (doming or bow-stringing) indicates that the deep abdominals are failing to maintain stability against the pull of rectus abdominis. A maximally flexed or extended lumbar spine indicates that mid-range (active) stability has been lost and joint approximation and inert tissue stretch are providing passive stability only.
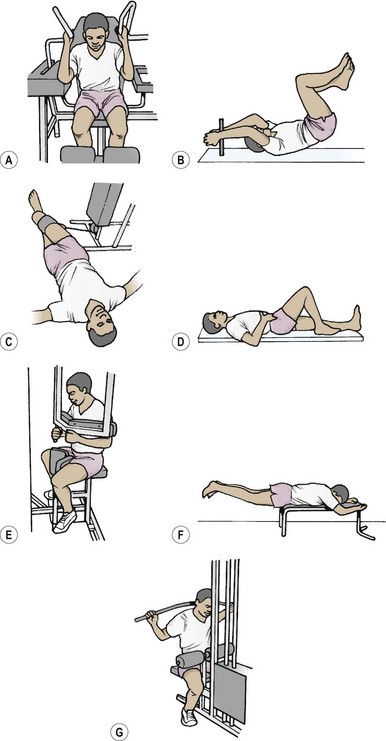
Figure 13.38 Examples of resistance exercises. Stage II (A) sitting abdominal curl, (B) reverse crunch, (C) lying cable trunk rotation, (D) heel slide, (E) sitting trunk rotation, (F) prone leg extension, (G) lateral pull-down.
From Norris, C.M. (2000) Back Stability. Human Kinetics, Champaign, Illinois. With permission.
The speed and complexity of movements is increased so that the athlete is forced to maintain stability automatically. The athlete’s attention is fully taken up by focusing on the complexity of the exercise task (see information processing bottleneck). Spinal alignment must be maintained in sports-related actions such as cycling, jogging, throwing and plyometric actions. Use of a balance board or balance shoes and Swiss gym ball (Fig. 13.37G) is useful (Irion, 1992; Lester, 1992; Lester and Posner-Mayer, 1993).
Mid-section training in sports
Training the abdominal region is fraught with danger for the lumbar spine, so close analysis of exercises for this region is useful. Application of core stability principles can reduce stress imposed on the spine during this type of training.
Function of the abdominal muscles
The rectus abdominis and lateral fibres of external oblique may be considered as the prime movers of trunk flexion, while the internal oblique and transversus abdominis are the major stabilizers (see Chapter 5). The rectus and external oblique are superficial muscles which often dominate trunk actions, while the transversus and internal oblique are more deeply placed and patients often show an inability to contract them voluntarily.
The rectus abdominis will flex the trunk by approximating the pelvis and rib cage. EMG investigation has shown the supra-umbilical portion to be emphasized by trunk flexion, while activity in the infra-umbilical portion is greater in positions where a posterior pelvic tilt is held (Lipetz and Gutin, 1970; Guimaraes et al., 1991). Some authors however, have questioned these findings, claiming that the differences between the two portions of rectus represent measurement errors rather than muscle function (Lehman and McGill, 2001). Internal oblique and transversus are activated by abdominal hollowing actions (Richardson et al., 1990), and the transversus acts at the initiation of movement to stabilize the trunk in overhead and lower limb actions (Hodges, Richardson and Jull, 1996).
In sport, the abdominal muscles essentially function to stabilize the trunk and provide a firm base of support for the arms and legs to work against. If stability is poor (in relation to total power of the athlete), limb actions will cause unwanted displacement of the pelvis and trunk. If we take an overhead pressing movement as an example (Fig. 13.39), where core stability is poor, the neutral position of the spine is lost and the spine is forced into potentially dangerous hyperextension.
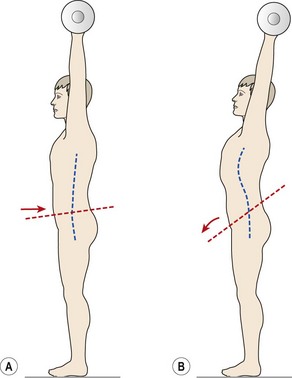
Analysis of conventional exercises
Two exercises underlie most abdominal training, the sit-up and the leg-raise, and we will look at these movements to determine their usefulness.
The sit-up
The sit-up is essentially an action where an athlete comes from a supine lying to a long sitting position by performing hip flexion, usually with trunk flexion. There are several modifications of this action which will be dealt with below.
In a classic sit-up, as soon as the head lifts, activity is seen in the rectus abdominis, and as a consequence the rib cage is depressed anteriorly. This initial period of flexion emphasizes the supra-umbilical portion of the rectus, the infra-umbilical portion and the internal oblique contracting later (Kendall, McCreary and Provance, 1993). As the internal oblique contracts, it pulls on the lower ribs, causing the ribs to flare out and so increase the infra-sternal angle. Laboratory analysis of the sit-up measuring horizontal and vertical forces, segmental kinematics and EMG (Cordo et al., 2003; Cordo et al., 2006) has shown the action to be divided into five interlinking phases. During phase I the cervical spine and upper trunk is flexed followed by lumbar flexion in phase II at which point peak muscle contraction is seen. This phase is the critical point of the exercise where maximum load is lifted, the legs may lift from the ground and the exercise is likely to fail. Phase III begins with anterior rotation of the pelvis and during phase IV the legs lower back to the ground to rest in phase V. During phase III the tilt of the pelvis may reverse from posterior tilt in the earlier phases due to abdominal muscle action to anterior tilt during the later phases due to hip flexor activity.
Abdominal ‘doming’ and pelvic fixation
One of the problems that poorly toned individuals face is bow-stringing or ‘doming’ of the abdominals, which is often seen at the initiation of the sit-up action. For the superficial abdominals (rectus abdominus and external oblique) to pull flat, the deep abdominals (transversus abdominus and internal oblique) must be strong enough to perform an abdominal hollowing action and act as stabilizers, holding the rectus sheath down. Where the deep abdominals are weak and the superficial abdominals are lengthened, the abdominal wall will be seen to dome and the athlete may lift the trunk with the lumbar spine extended or flat rather than flexed (Fig. 13.40).
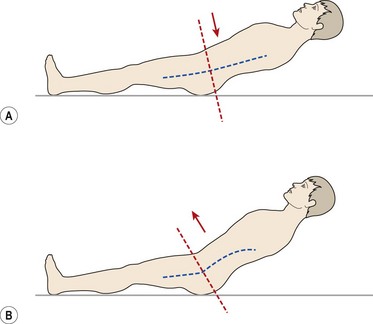
Figure 13.40 Trunk alignment during a sit-up exercise. (A) Deep abdominals pull abdominal wall flat. (B) Deep abdominals allow abdominal wall to ‘dome’, lengthened superficial abdominals allow anterior pelvic tilt, and hollow back.
Definition
Abdominal doming is said to occur when the abdominal wall bulges rather than flattens during a trunk exercise.
Fixation of the pelvis is provided by the hip flexors, especially iliacus through its attachment to the pelvic rim. The strong pull of the hip flexors is partially counteracted by the pull of the lateral fibres of external oblique and the infra-umbilical portion of the rectus abdominis, which tend to tilt the pelvis posteriorly. Action of the external oblique, if powerful enough, will compress the ribs and reduce the infra-sternal angle once more (Kendall, McCreary and Provance, 1993).
Effects of foot fixation
If the sit-up action is attempted from the supine lying position without allowing trunk flexion, there is a tendency for the legs to lift up from the supporting surface. This occurs because the legs constitute roughly one-third of the body weight and the trunk two-thirds.
As the abdominal muscles flex the spine, the centre of gravity of the upper body is moved caudally. Movement of the centre of gravity in this fashion reduces the lever arm of the trunk enabling the subject to sit up without the legs lifting (Fig. 13.41).
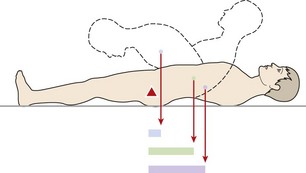
Figure 13.41 Changing leverage of the trunk. As the trunk flexes, the centre of gravity of the upper body moves closer to the hip, reducing the leverage effect.
From Norris (1994a), with permission.
In cases where the abdominal muscles are weak, maximum spinal flexion will not occur and so the lever arm of the trunk remains long. Now, the greater weight and lever arm of the trunk causes it to remain on the floor and the legs are seen to lift.
If the feet are fixed, the hip flexors can now pull powerfully without causing the legs to lift. In addition, the act of foot fixation itself may facilitate the iliopsoas (Janda and Schmid, 1980). Foot fixation requires the subject to pull against the fixation point by active dorsiflexion. This process stimulates the gait pattern at heel contact, increasing activity in the tibialis anterior, quadriceps and iliopsoas (flexor synergy).
Modifications of the sit-up
The bent knee sit-up and trunk curl
The bent knee sit-up is performed from the crook-lying starting position, with the knees flexed to 90° and hips flexed to 45°. The action is one of trunk flexion followed by, or performed with, hip flexion. The trunk curl is performed from the same starting position, but no hip flexion occurs, the lumbar spine remaining in contact with the supporting surface. The bench-curl is performed from a starting position of 90° hip flexion, the shin being supported on a bench or chair.
Bending the knees and hips to alter the starting position of the sit-up will affect both the passive and active actions of the hip flexors, and the biomechanics of the lumbar spine. In supine lying, the iliopsoas is on stretch, and aligned with the horizontal (Fig. 13.42). In this position, vertebral compression is at its greatest as the muscle contracts, and trunk lifting is at a mechanical disadvantage. The ratio of lifting to compression is therefore approximately 1 : 10 (Watson, 1983). As the knees are flexed, the iliopsoas is pulled more vertically and so the ratio of trunk lifting to vertebral compression is reduced to 2 : 5 in crook lying and 1 : 1 in bench lying.
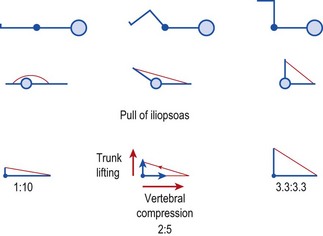
Figure 13.42 Mechanical advantage of iliopsoas during the sit-up. As the hip is flexed, the moment arm of the iliopsoas is lengthened. The muscle can therefore complete the sit-up action by using less force, and so vertebral compression is reduced.
From Norris (1994a), with permission.
With 45° hip flexion, tension development in the iliopsoas has been shown to be 70–80% of its maximum, while with the hips and knees flexed to 90° this figure reduces to between 40 and 50% (Johnson and Reid, 1991).
However, passive tension developed by the iliopsoas due to elastic recoil must also be considered. If the hips are flexed, the iliopsoas will not be fully stretched, and will not be able to passively limit the posterior tilt of the pelvis. Instead, to fix the pelvis and provide a stable base for the abdominals to pull on, the hip flexors will contract earlier in the sit-up action. This contraction, although occurring earlier, is of reduced intensity (Walters and Partridge, 1957) due to the length–tension relationship of the muscle.
With the legs straight in the traditional sit-up position, the iliopsoas is stretched, and can passively limit posterior tilting of the pelvis. However, in this stretched position, the iliopsoas is capable of exerting greater force during hip flexion. If the abdominal muscles are too weak to maintain the position of the pelvis, the stronger hip flexors will hyperextend the lumbar spine and cause the pelvis to tilt forwards, lengthening the abdominals, and hyperextending the lumbar spine. This type of action is, therefore, unsuitable for postural re-education if the aim is to shorten posturally lengthened abdominal muscles.
Correction of posturally lengthened abdominals
If the subject has lengthened abdominals, these are shortened by performing an inner range holding movement. This action is a modification of the trunk curl to combine three actions (Norris, 1994a, 1994b). The subject posteriorly tilts the pelvis, performs abdominal hollowing, and depresses the rib cage while exhaling (Fig. 13.43). Maximum trunk flexion is attempted, providing this is not contraindicated by lumbar pathology. If abdominal lengthening has occurred, the subject will show a greater passive range of motion than active range of motion to lumbar flexion.
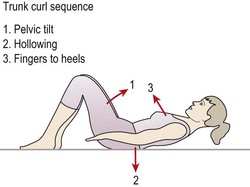
Keypoint
If abdominal lengthening has occurred, athletes will show a greater passive than active range of motion to lumbar flexion. This is corrected using inner range training and eccentric muscle work.
To correct this, an eccentric action is used. The subject uses his or her finger tips on the outside of the knees to pull the body into full passive lumbar flexion. They set the abdominal muscles and attempt to hold this position as they let the hand grip relax. Initially, they will only be able to decelerate the lowering action using an eccentric contraction of the target muscles. As muscle adaptation occurs, the movement will become more controlled and slower. Eventually an isometric hold will become possible and finally a concentric action. Once this is achieved, full range exercise is begun, using slow movements building up to a total repetition time of 10–30 seconds.
Straight-leg raising
The bilateral straight leg raise (SLR) has been shown to create only slight activity in the upper rectus, although the lower rectus contributes a greater proportion of the total abdominal work than with the sit-up (Lipetz and Gutin, 1970). The rectus works isometrically to fix the pelvis against the strong pull of iliopsoas (Silvermetz, 1990). The force of contraction of the iliopsoas is at its maximum when the lever arm of the leg is greatest, near the horizontal, and reduces as the leg is lifted towards the vertical. EMG recordings of straight leg raising (Juker et al., 1998) confirm the contraction difference in the iliopsoas in relation to the rectus abdominis. Compared to maximum intensity (100%) the SLR gives an iliopsoas intensity of 35% and a rectus abdominis intensity of 37%. The trunk curl exercise is more efficient in terms of abdominal training, giving an iliopsoas intensity of 7% and a rectus intensity of 62%.
Keypoint
The straight leg raise places almost the same work intensity on the iliopsoas as it does on the rectus abdominis muscle.
In subjects with weaker abdominals, the pelvis will tilt and the lumbar spine will hyperextend. This forced hyperextension will dramatically increase stress on the facet joints particularly in the lumbar spine. The movement is likely to be limited by impaction of the inferior articular processes on the laminae of the vertebrae below, or in some cases by contact between the spinous processes (Twomey and Taylor, 1987). Where this action occurs rapidly, damage may result to the facet joint structures. Once contact has occurred between the facet and lamina, further loading will cause axial rotation of the superior vertebra (Yang and King, 1984). The superior vertebra pivots, causing the inferior articular process to move backwards overstretching the joint capsule.
Laboratory analysis of the straight leg raise action (Sheilds and Heiss, 1997) has demonstrated two muscle synergies. The first shows high levels of rectus abdominis and external oblique activity coupled with low levels from the internal oblique. The second synergy shows low rectus activity with high external and high internal oblique activity. The low level internal oblique usage in the first synergy is likely to result in doming of the abdominals.
Modification of straight-leg raising
As none of the abdominal muscles actually cross the hip, they are not prime movers of the straight-leg raising movement. However, the action is an important one as it emphasizes the pelvic stabilizing function of the infra-umbilical portion of the rectus abdominis, and lateral external oblique.
A number of exercises serve as modifications of the bilateral straight leg raise to reduce the stress on the lumbar spine. The first action is the heel slide (Fig. 13.44A). From a crook-lying starting position an abdominal hollowing action is performed to stabilize the spine. From this position, one leg is straightened while keeping the heel on the ground and sliding the leg into extension.
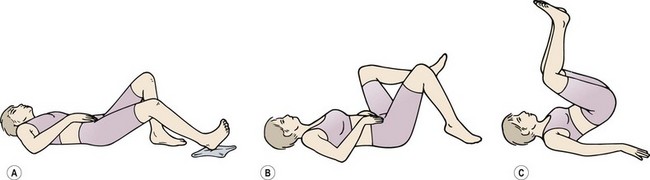
Figure 13.44 Modifications of the straight-leg raise. (A) Heelslide. (B) Leg lowering. (C) Pelvic raise.
From Norris (2001), with permission.
The second movement is leg lowering (Fig. 13.44B). For this exercise the subject lies supine with the knees and hips bent to 90°. From this position, the lumbar spine is gently flattened into the mat and one leg is lowered by eccentric action of the hip flexors while maintaining the flat contour of the abdomen (avoiding doming) and not allowing any pelvic tilt.
The third exercise uses leg and pelvic motion on a fixed trunk to increase the emphasis on the lower abdominals. The subject begins the action in crook lying and draws the knees right up onto the chest (Fig. 13.44C). The action is then a posterior pelvic tilt combined with abdominal hollowing to flex the lower lumbar spine and raise the sacrum off the supporting surface. Again the repetition time is gradually increased to 10–30 seconds. Because both of these exercises flex the lumbar spine, a passive extension action, such as extension in lying and anterior pelvic tilting, should be performed at the end of the exercise bout to compensate for flexion stresses.
Adams M.A., Hutton W.C. Prolapsed intervertebral disc: a hyperflexion injury. Spine. 1982;8(3):327.
Adams M.A., Hutton W.C. The mechanical function of the lumbar apophyseal joints. Spine. 1983;8:327-330.
Adams M.A., Hutton W.C., Stott J.R.R. The resistance to flexion of the lumbar intervertebral joint. Spine. 1980;5:245-253.
Adams M., Bogduk N., Burton K., Dolan P. The Biomechanics of Back Pain. Edinburgh: Churchill Livingstone; 2002.
Airaksinen O., Brox J.I., Cedraschi. European Guidelines for the Management of Chronic Non-specific Low Back Pain. Brussels: European Commission Publications; 2005.
Beattie P.F., Brooks W.M., Rothstein J.M. Effect of lordosis on the position of the nucleus pulposus in supine subjects: a study using MRI. Spine. 1994;19(18):2096-2102.
Becker C. Lumbar spondylolysis. Sportex Medicine. 2006;Jan:6-9.
Bergmark A. Stability of the lumbar spine. Acta Orthopaedica Scandinavica Supplementum. 1989;230(60):3-54.
Bernhardt M., White A.A., Panjabi M.M., McGowan D.P. Lumbar spine instability. In Jayson M.I.V., editor: The Lumbar Spine and Back Pain, fourth ed, Edinburgh: Churchill Livingstone, 1992.
Bogduk N., Engel R. The menisci of the lumbar zygapophyseal joints: a review of their anatomy and clinical significance. Spine. 1984;9:454-460.
Bogduk N., Jull G. The theoretical pathology of acute locked back: a basis for manipulative therapy. Manual Medicine. 1985;1:78-82.
Bogduk N., Twomey L.T. Clinical Anatomy of the Lumbar Spine. Edinburgh: Churchill Livingstone; 1987.
Bogduk N., Twomey L.T. Clinical Anatomy of the Lumbar Spine, second ed. Edinburgh: Churchill Livingstone; 1991.
Butler D.S. Mobilisation of the Nervous System. Edinburgh: Churchill Livingstone; 1991.
Cappozzo A., Felici F., Figura F., Gazzani F. Lumbar spine loading during half-squat exercises. Medicine and Science in Sports and Exercise. 1985;17(5):613-620.
Ciullo J.V., Jackson D.W. Pars interarticularis stress reaction, spondylolysis, and spondylolisthesis in gymnasts. Clinics in Sports Medicine. 1985;4:95-110.
Clinical Standards Advisory Group (CSAG). Reports on Back Pain. London: HMSO; 1994.
Colcher A.E., Hursh A.M.W. Pre-employment low back X-ray survey: a review of 1500 cases. Industrial Medicine and Surgery. 1952;21:319.
Cordo P.J., Garfinkel V., Smith T., et al. The sit-up: complex kinematics and muscle activity in voluntary axial movement. Journal of Electromyography and Kinesiology. 2003;13:239-252.
Cordo P.J., Hodges P., Smith T., et al. Scaling and non-scaling of muscle activity kinematics and dynamics in sit-ups with different degrees of difficulty. Journal of Electromyography and Kinesiology. 2006;16:506-521.
Corrigan B., Maitland G.D. Practical Orthopaedic Medicine. London: Butterworth; 1983.
Cramer G.D., Tuck N., Knudsen J., et al. Effects of side posture positioning and side posture adjusting on the lumbar zygapophyseal joints as evaluated by magnetic resonance imaging. Journal of Manipulative and Physiological Therapeutics. 2000;23:380-394.
Crock H.V., Yoshizawa H. The blood supply of the lumbar vertebral column. Clinical Orthopaedics. 1976;115:6-21.
CSP. New statistics on the incidence of back pain. The YouGov poll. http://www.csp.org.uk, 2004.
Cusi M., Sauners J., Hungerford B., et al. The use of prolotherapy in the sacro-iliac joint. British Journal of Sports Medicine. 2008. (in press)
Cyriax J.. eighth ed Textbook of Orthopaedic Medicine vol. 1 London: Baillière Tindall, 1982.
Cyriax J.H., Cyriax P.J. Illustrated Manual of Orthopaedic Medicine. London: Butterworth; 1983.
Deville W.L., van der Windt D.A., Dzaferagic A., et al. The test of Lasegue: systematic review of the accuracy in diagnosing herniated discs. Spine. 2000;25(9):1140-1147.
Don Tigny R.L. Function and pathomechanics of the sacroiliac joint. Physical Therapy. 1985;65:35-44.
Dreyfuss Dreyfuss, P., Dreyer, S., Griffin, J., Hoffman, J., Walsh, N., 1992. Positive sacroiliac screening tests in asymptomatic adults. Proceedings of the First Interdisciplinary World Congress on Low Back Pain and its Relation to the Sacroiliac Joint. San Diego, CA.
Edmondston S.J., Song S, Bricknell R.V. MRI evaluation of lumbar spine flexion and extension in asymptomatic individuals. Manual Therapy. 2000;5(3):158-164.
Evans D.W. Mechanisms and effects of spinal high velocity low amplitude thrust manipulation: Previous theories. Journal of Manipulative and Physiological Therapeutics. 2002;25:251-262.
Evans D.W., Breen A.C. A biomechanical model for mechanically efficient cavitation production during spinal manipulation: prethrust position and the neutral zone. Journal of Manipulative and Physiological Therapeutics. 2006;29(1):72-82.
Farfan H.F., Cossette J.W., Robertson G.H., Wells R.V., Kraus H. The effects of torsion on the lumbar intervertebral joints: the role of torsion in the production of disc degeneration. Journal of Bone and Joint Surgery. 1970;52A:468.
Farfan H.F., Osteria V., Lamy C. The mechanical etiology of spondylolysis and spondylolisthesis. Clinical Orthopaedics and Related Research. 1976;117:40-55.
Fennell A.J., Jones A.P., Hukins D.W.L. Migration of the nucleus pulposus within the intervertebral disc during flexion and extension of the spine. Spine. 1996;21(23):2753-2757.
Foster D., John D., Elliott B., et al. Back injuries to fast bowlers in cricket: A prospective study. British Journal of Sports Medicine. 1989;23:150-154.
Frigerio N.A., Stowe R.R., Howe J.W. Movement of the sacro-iliac joint. Clinical Orthopaedic and Related Research. 1974;100:370.
Fryomoyer J.W., Cats-Baril W.L. An overview of the incidences and costs of low back pain. Orthopaedic Clinics of North America. 1991;22:263.
Gal J.M., Herzog W., Kawchuk G.N., et al. Movements of vertebrae during manipulative thrusts to un-embalmed human cadavers. Journal of Manipulative and Physiological Therapeutics. 1997;20:30-40.
Giles L., Taylor J. Human zygapophyseal joint capsule and synovial fold innervation. British Journal of Rheumatology. 1987;26:93-98.
Gould. Orthopedic and Sports Physical Therapy. St. Louis: C.V. Mosby; 1990.
Gregory P., Batt M., Wallace W. Comparing injuries of spin bowling with fast bowling in young cricketers. Clinical Journal of Sports Medicine. 2002;12(2):107-112.
Grieve G.P. Sciatica and the straight leg raising test in manipulative treatment. Physiotherapy. 1970;56:337.
Grieve G.P. The sacro-iliac joint. Physiotherapy. 1976;62(12):384-400.
Guimaraes A.C.S., Vaz M.A., De Campos M.I.A., Marantes R. The contribution of the rectus abdominus and rectus femoris in 12 selected abdominal exercises. Journal of Sports Medicine and Physical Fitness. 1991;31:222-230.
Gunn C.C. Treatment of chronic pain, second edition. Edinburgh: Churchill Livingstone; 1996.
Harreby M., Hesseloe G., Kier J., Neergaard K. Low back pain and physical exercise in leisure time in 38 year old men and women. European Spinal Journal. 1997;6:181-186.
Herzog W., Symons B. The biomechanics of spinal manipulation. Critical Reviews in Physical and Rehabilitation Medicine. 2001;13:191-216.
Herzog W., Scheele D., Conway P. Electromyographic responses of back and limb muscles associated with spinal manipulative therapy. Spine. 1999;24:146-153.
Hirsch C., Nachemson A. New observations on mechanical behaviour of lumbar discs. Acta Orthopaedica Scandinavica. 1954;22:184-189.
Hirsch C., Schajowicz F. Studies on structural changes in the lumbar annulus fibrosis. Acta Orthopaedica Scandinavica. 1952;22:184-189.
Hirsch C., Ingelmark V.E., Miller N. The anatomic basis for low back pain: studies on the presence of sensory endings in ligamentous capsular and intervertebral disc structures in the human lumbar spine. Acta Orthopaedica Scandinavica. 1963;33:1-17.
Hodges P., Richardson C., Jull G. Evaluation of the relationship between laboratory and clinical tests of transverses abdominus function. Physiotherapy Research International. 1996;1:30-40.
Holm S., Maroudas A., Urban J.P.G., Selstam G., Nachemson A. Nutrition of the intervertebral disc: solute transport and metabolism. Connective Tissue Research. 1981;8:101-119.
Hoshina H. Spondylolysis in young athletes. Physician and Sports Medicine. 1980;8:75-79.
Hukins D.W.L. Properties of spinal materials. In: Jayson M.I.V., editor. The Lumbar Spine and Back Pain. London: Churchill Livingstone, 1987.
Irion J.M. Use of the gym ball in rehabilitation of spinal dysfunction. Orthopaedic Physical Therapy Clinics of North America. 1992;23:375-398.
Janda Janda, V., Schmid, H.J.A., 1980. Muscles as a pathogenic factor in back pain. Proceedings of the International Federation of Orthopaedic Manipulative Therapists, 4th Conference, 17–18, New Zealand.
Johnson C., Reid J.G. Lumbar compressive and shear forces during various curl up exercises. Clinical Biomechanics. 1991;6:97-104.
Juker D., McGill S., Kropf S., Steffen T. Quantitative intramuscular myoelectric activity of lumbar portions of psoas and the abdominal wall during a wide variety of tasks. Medicine and Science in Sports and Exercise. 1998;30:301-310.
Kapandji I. The Physiology of Joints vol. 3 London: Churchill Livingstone, 1974 The Spine
Kendall F.P., McCreary E.K., Provance P.G. Muscles: Testing and Function, fourth ed. Baltimore: Williams and Wilkins; 1993.
Kesson M., Atkins E. Orthopaedic Medicine. Oxford: Butterworth-Heinemann; 1998.
Klein J.A., Hukins D.W.L. Functional differentiation in the spinal column. Engineering in Medicine. 1981;12(2):83.
Klein J.A., Hukins D.W.L. Relocation of the bending axis during flexion–extension of the lumbar intervertebral discs and its implications for prolapse. Spine. 1983;8:659-664.
Kotanis P.T., Ichikawa N., Wakabayashi W., Yoshii T., Koshimune M. Studies of spondylolysis found among weight lifters. British Journal of Sports Medicine. 1971;6:4.
Koumantakis G.A., Watson P.J., Oldham J.A. Supplementation of general endurance exercise with stabilization training, versus general exercise only. Clinical Biomechanics. 2005;20:474-482.
Kraemer J., Kolditz D., Gowin R. Water and electrolyte content of human intervertebral discs under variable load. Spine. 1985;10:69-71.
Laslett M. Pain provocation sacroiliac joint tests. In: Vleeming A., Mooney V., Dorman T., Snijders C., Stoeckart R., editors. Movement Stability and Low Back Pain. Edinburgh: Churchill Livingstone, 1997.
Laslett M., Williams M. The reliability of selected pain provocation tests for sacroiliac pathology. Spine. 1994;19:1243-1249.
Leatt P., Reilly T., Troup J.G.D. Spinal loading during circuit weight-training and running. British Journal of Sports Medicine. 1986;20(3):119-124.
Lee D.G. Clinical manifestations of pelvic girdle dysfunction. In Boyling J.D., Palastanga N., editors: Grieve’s Modern Manual Therapy, second ed, Edinburgh: Churchill Livingstone, 1994.
Lehman G.J., McGill S.M. Quantification of the differences in electromyographic activity magnitude between the upper and lower portions of the rectus abdominis muscle during selected trunk exercises. Physical Therapy. 2001;81(5):1096-1101.
Lester Lester, M.N., 1992. Spinal stabilization and compliance utilizing the therapeutic ball. Proceeding of the International Federation of Orthopaedic Manipulative Therapists, Vail, Colorado.
Lester M.N., Posner-Mayer J. Spinal Stabilization: Utilizing the Swiss Ball (video). Denver: Ball Dynamics; 1993.
Letts M., Smallman T., Afanasiev R., Gouw G. Fracture of the pars interarticularis in adolescent athletes: a clinical-biomechanical analysis. Journal of Paediatric Orthopaedics. 1985;6:40-46.
Lewit K. The muscular and articular factor in movement restriction. Man Medicine. 1985;1:83-85.
Lipetz S., Gutin B. An electromyographic study of four abdominal exercises. Medicine and Science in Sports and Exercise. 1970;2:35-38.
Magee D.J. Orthopedic Physical Assessment, forth ed. Philadelphia: Saunders; 2002.
Maitland G.D. Vertebral Manipulation, fifth ed. London: Butterworth; 1986.
Markolf K.L., Morris J.M. The structural components of the intervertebral disc. Journal of Bone and Joint Surgery. 1974;56A:675.
Masci L., Pike J., Malara F., Phillips B., et al. Use of the one legged hyperextension test and magnetic resonance imaging in the diagnosis of active spondylolysis. British Journal of Sports Medicine. 2006;40:940-946.
McKenzie R., May S. The Lumbar Spine: Mechanical Diagnosis and Therapy. Waikanae: Spinal Publications New Zealand; 2003.
McKenzie R.A. The Lumbar Spine: Mechanical Diagnosis and Therapy. Waikanae: Spinal Publications New Zealand; 1981.
McKenzie R.A. The Cervical and Thoracic Spine: Mechanical Diagnosis and Therapy. Waikanae: Spinal Publications New Zealand; 1990.
Mens J.M.A., Vleeming A., Snijders C.J., Stam H.J. Active straight leg raising test: a clinical approach to the load transfer function of the pelvic girdle. In: Vleeming A., Mooney V., Dorman T., editors. Movement Stability and Low Back Pain. Edinburgh: Churchill Livingstone, 1997.
Mercer C., Jackson A., Hettinga D., Barlos P. Clinical guidelines for the physiotherapy management of persistent low back pain part 1: exercise. London: Chartered Society of Physiotherapy; 2006.
Miller M.I., Madeiros J.M. Recruitment of internal oblique and transversus abdominis muscles during the eccentric phase of the curl-up exercise. Physical Therapy. 1987;67:1213-1217.
Mooney V., Robertson J. The facet syndrome. Clinical Orthopaedics. 1976;115:149-156.
Mulligan B.R. Manual Therapy—Nags, Snags, and PRPs etc. New Zealand: Plane View Services Wellington; 1989.
Nachemson A. The lumbar spine: an orthopaedic challenge. Spine. 1976;1:59-71.
Nachemson A. Lumbar intradiscal pressure. In: Jayson M.I.V., editor. The Lumbar Spine and Back Pain. London: Churchill Livingstone, 1987.
Nachemson A., Evans J. Some mechanical properties of the third lumbar inter-laminar ligament (ligamentum flavum). Journal of Biomechanics. 1968;1:211.
Nelson M.A., Allen P., Clamp S.E., De Dombal F.T. Reliability and reproducibility of clinical findings in low back pain. Spine. 1979;4:97-101.
Norkin C.C., Levangie P.K. Joint Structure and Function: A Comprehensive Analysis, second ed. Philadelphia: F.A. Davis; 1992.
Norris. Acupuncture: Treatment of Musculoskeletal Conditions. Oxford: Butterworth-Heinemann; 2001.
Norris C.M. Abdominal muscle training in sport. British Journal of Sports Medicine. 1993;27(1):19-27.
Norris C.M. Abdominal training: dangers and exercise modifications. Physiotherapy in Sport. 1994;14(5):10-14.
Norris Norris, C.M., 1994b. A flat stomach—the right way. Exercise Magazine November.
Norris C.M. Spinal stabilisation 2. Limiting factors to end-range motion in the lumbar spine. Physiotherapy. 1995;81(2):4-12.
Norris C.M. Back Stability. Champaign, Illinois, USA: Human Kinetics; 2000.
Norris C.M. Back Stability (second edition). Champaign, Illinois: Human Kinetics; 2008.
Norris C.M., Matthews M. The role of an integrated back stability program in patients with chronic low back pain. Complementary Therapies in Clinical Practice. 2008;14:255-263.
O’Sullivan P.B. Lumbar segmental instability. Manual Therapy. 2000;5(1):2-12.
O’Sullivan P.B., Twomey L.T., Allison G.T. Evaluation of specific stabilizing exercise in the treatment of chronic low back pain with radiologic diagnosis of spondylolysis or spondylolisthesis. Spine. 1997;22:2959-2967.
Oliver J., Middleditch A. Functional Anatomy of the Spine. Oxford: Butterworth-Heinemann; 1991.
Palastanga N., Field D., Soames R. Anatomy and Human Movement. Oxford: Butterworth-Heinemann; 1989.
Panjabi M.M. The stabilizing system of the spine. Part 1. Function, dysfunction, adaptation, and enhancement. Journal of Spinal Disorders. 1992;5(4):383-389.
Panjabi M.M., Hult J.E., White A.A. Biomechanical studies in cadaveric spines. In: Jayson M.I.V., editor. The Lumbar Spine and Back Pain. London: Churchill Livingstone, 1987.
Panjabi Panjabi, M.M., Jorneus, L., Greenstein, G., 1984. Lumbar Spine Ligaments: An In Vitro Biomechanical Study, ORS Transactions.
Paris S.V. Physical signs of instability. Spine. 1985;10(3):277-279.
Pearcy P., Portek I., Shepherd J. Three dimensional X-ray analysis of normal movement in the lumbar spine. Spine. 1984;9:294-297.
Potter N.A., Rothstein J.M. Intertester reliability for selected clinical tests of the sacroiliac joint. Physical Therapy. 1985;65:1671-1675.
Reid D.C. Sports Injury Assessment and Rehabilitation. London: Churchill Livingstone; 1992.
Richardson C., Toppenberg R., Jull G. An initial evaluation of eight abdominal exercises for their ability to provide stabilization for the lumbar spine. Australian Journal of Physiotherapy. 1990;36:6-11.
Richardson Richardson, C.A., 1992. Muscle imbalance: principles of treatment and assessment. Proceedings of the New Zealand Society of Physiotherapists Challenges Conference, Christchurch, New Zealand.
Richardon C.A., Hodges P. New Advances in Exercise to Rehabilitation Spinal Stabilization. Edinburgh: Course notes; 1996.
Roaf R. A study of the mechanics of spinal injuries. Journal of Bone and Joint Surgery (Br). 1960;42B:810-823.
Rockoff S.F., Sweet E., Bleustein J. The relative contribution of trabecular and cortical bone to the strength of human lumbar vertebrae. Calcified Tissue Research. 1969;3:163-175.
Sahrmann S.A. Diagnosis and treatment of movement impairment syndromes. St.Louis: Mosby; 2002.
Sheilds R.K., Heiss D.G. An electromyographic comparison of abdominal muscle synergies during curl and double straight leg lowering exercises with control of pelvic position. Spine. 1997;22(16):1873-1879.
Silvermetz M.A. Pathokinesiology of supine double leg lifts as an abdominal strengthener and suggested alternative exercises. Athletic Training. 1990;25:17-22.
Spitzer W.O., LeBlanc F.E., Dupuis M. Scientific approach to the assessment and management of activity related spinal disorders: a monograph for clinicians. Report of the Quebec Task Force on Spinal Disorders. Spine. 1987;12:7s.
Sturesson B. Movement of the sacroiliac joint with special reference to the effect of load. In: Vleeming A., Mooney V., Stoeckar R., editors. Movement, stability and lumbopelvic pain. Oxford: Churchill Livingstone, 2007.
Sturesson B., Selvik G., Uden A. Movements of the sacroiliac joints. A roentgen stereophotogrammetric analysis. Spine. 1989;14:162-165.
Taylor J.R., Twomey L.T. Age changes in lumbar zygapophyseal joints. Spine. 1986;11:739-745.
Taylor J.R., Twomey L.T. The lumbar spine from infancy to old age. In Twomey L.T., Taylor J.R., editors: Physical Therapy of the Low Back, second ed, Edinburgh: Churchill Livingstone, 1994.
Thompson B. How should athletes with chronic low back pain be managed in primary care? In: MacAuley D., Best T., editors. Evidence Based Sports Medicine. London: BMJ Books, 2002.
Tkaczuk H. Tensile properties of human lumbar longitudinal ligaments. Acta Orthopaedica Scandinavica. 115(Suppl.), 1968.
Tropp H., Alaranta H., Renstrom P.A.F.H. Proprioception and coordination training in injury prevention IOC Medical Commission Publication. Renstrom P.A.F.H., editor. Sports Injuries: Basic Principles of Prevention and Care. London: Blackwell Scientific, 1993.
Turner H. The Sacro Iliac Joint. Manchester, UK: Course notes; 2002.
Twomey L.T., Taylor J.R. Lumbar posture, movement and mechanics. In: Twomey L.T., editor. Physical Therapy of the Low Back. New York: Churchill Livingstone, 1987.
Tyrrell A.R., Reilly T., Troup J.D.G. Circadian variation in stature and the effects of spinal loading. Spine. 1985;10:161-164.
Unsworth A., Dowson D., Wright V. A bioengineering study of cavitation in the metacarpophalangeal joint. Annals of the Rheumatic Diseases. 1971;30:348-358.
Urban L.M. The straight-leg raising test: a review. In: Grieve G.P., editor. Modern Manual Therapy of the Vertebral Column. London: Churchill Livingstone, 1986.
Van Duersen L.L., Patijn J., Ockhuysen A.L., Vortman B.J. The value of some clinical tests of the sacroiliac joint. Manual Medicine. 1990;5:96-99.
Van Tulder M., Malmivaara A., Esmail R., Koes B. Exercise therapy for low back pain: a systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine. 2000;25:2784-2796.
Vernon H.T. Qualitative review of studies of manipulation induced hypoalgesia. Journal of Manipulative and Physiological Therapeutics. 2000;23:134-138.
Vernon-Roberts B. Pathology of intervertebral discs and apophyseal joints. In: Jayson M.I.V., editor. The Lumbar Spine and Back Pain. London: Churchill Livingstone, 1987.
Vleeming A., Mooney V., Dorman T., Snijders C. Movement Stability and Low Back Pain. Edinburgh: Churchill Livingstone; 1997.
Vleeming A., Pool-Goudzwaard A.L., Stoeckart R., Wingerden J.P., Snijders C.J. The posterior layer of the thoracolumbar fascia: its function in load transfer from spine to legs. Spine. 1995;20:753-758.
Waddell G., Feder G., Lewis M. Systematic reviews of bed rest and advice to stay active for acute low back pain. British Journal of General Practice. 1997;47:647-652.
Walters C., Partridge M. Electromyographic study of the differential abdominal muscles during exercise. American Journal of Physical Medicine. 1957;36:259-268.
Watson J. An Introduction for Mechanics of Human Movement. Lancaster, UK: MTP Press; 1983.
Weber M.D., Woodall W.R. Spondylogenic disorders in gymnasts. Journal of Orthopaedic and Sports Physical Therapy. 1991;14(1):6-13.
Wells P. The examination of the pelvic joints. In: Grieve G.P., editor. Modern Manual Therapy of the Vertebral Column. London: Churchill Livingstone, 1986.
Williams J.G.P., Sperryn P.N. Sports Medicine. London: Edward Arnold; 1976.
Yang K.H., King A.I. Mechanism of facet load transmission as a hypothesis for low-back pain. Spine. 1984;9:557-565.