CHAPTER 14 The thorax and thoracic spine
Thoracic spine
The unique feature of the vertebrae in the thoracic region is the presence of facets, both on the sides of the vertebral bodies and the transverse processes. These are for articulation with the ribs, forming the costovertebral and costotransverse joints (Fig. 14.1). Most of the ribs articulate with two adjacent vertebral bodies and one transverse process. The facets on the head of the ribs articulate in turn with demi-facets on the upper and lower borders of the vertebrae, and the crest on the rib head butts onto the intervertebral disc. The joint capsule is loose and strengthened anteriorly to form the three portions of the radiate ligament. The costovertebral joint cavity is divided into two by the intra-articular ligament, except for ribs one, ten, eleven and twelve which articulate with a single vertebra and have a single joint cavity.
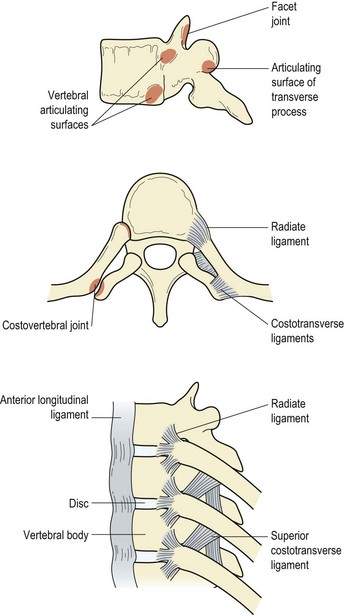
The costotransverse joints are formed only with the upper ten ribs. The joint is made between the articular facet of the transverse process and the oval facet on the rib tubercle. The thin joint capsule is strengthened by the costotransverse ligaments.
Sternal articulations
The sternocostal joints are formed between the medial end of the costal cartilages of ribs one to seven. The joint between the first rib and the sternum is cartilaginous, but all the others are synovial. Each is surrounded by a capsule and supported by radiate ligaments. The fibres of these ligaments fan out and intertwine with those of the ligaments above and below, and also with those of the opposite sternocostal joints. In addition, the radiate ligament fibres fuse with the tendinous fibres of the pectoralis major. The eighth, ninth, and tenth ribs form interchondral joints between their costal cartilages.
The costochondral joints are formed between the end of the rib and the lateral edge of the costal cartilage. The joint formed is cartilaginous, its perichondrium being continuous with the periosteum of the rib itself. Only slight bending and twisting actions are possible at this joint. The manubriosternal articulation is that between the upper part of the sternum and the manubrium. The joint is cartilaginous, with a hollow disc in its centre, and is strengthened by the sternocostal ligaments and longitudinal fibrous bands. About 7° of movement occurs at the joint in association with breathing.
Rib movements
Movement of the diaphragm, ribs and sternum increases the volume within the thorax with inspiration. Each rib acts as a lever, with one axis travelling through the costovertebral and sternocostal joints, and another through the costovertebral and costotransverse joints. The two axes permit two types of motion, known as ‘pump handle’ and ‘bucket handle’. In the pump handle action the upper ribs and sternum are raised, increasing the anteroposterior diameter of the thorax. With bucket handle motion the lower ribs move both up and out, widening the infrasternal angle and increasing the transverse diameter of the thorax. In the lower ribs (8−12) a third motion called ‘caliper action’ may also occur where the lateral diameter of the chest is increased, without significant joint motion.
The variation in movement between the upper and lower ribs is due, in part, to the differing structure of their respective costotransverse joints. The upper joints are cup-shaped permitting mainly rotation (pump handle), while those lower down are flat permitting both rotation and gliding movements (bucket handle).
Keypoint
The ribs can move forwards and upwards, increasing the anteroposterior diameter of the thorax (pump handle), and outwards, increasing the lateral diameter of the thorax (bucket handle).
In addition to respiratory motion, the ribs also move in association with the thoracic spine. With flexion of the spine the ribs move closer together and with extension they are pulled further apart, flattening the ribcage. This latter action in the upper ribs is important for the correct movement of the scapulothoracic joint. Lateral flexion causes the ribs on the concave side to move together and those on the convex side to move apart. Rotation gives horizontal gliding of one rib relative to another.
Ribcage shape at rest
The general shape of the ribcage will change as a result of thoracic mobility, with an increased thoracic kyphosis causing a general flattening of the ribcage. In addition, congenital abnormalities occur, including pigeon chest, funnel chest and barrel chest.
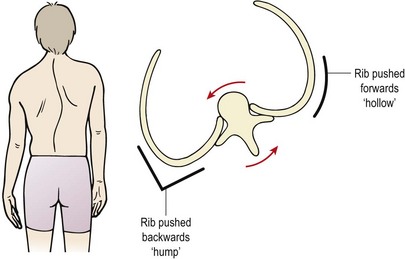
The ribcage will also alter shape in cases of scoliosis. The vertebral bodies rotate towards the convexity of the curve, dragging the ribs with them. The ribs on the convex side of the curve are pushed backwards creating a ‘hump’ and those on the concave side of the curve move anteriorly causing a ‘hollow’ (Fig. 14.2). Rotation of the vertebral body causes the spinous processes to move away from the mid-line, in the opposite direction to the scoliosis. Right rotation of the vertebra therefore sees the spinous process deviating to the left.
Movement of the thoracic spine
The relative thinness of the discs in the thoracic region, coupled with the presence of the ribs, makes movement here more limited than in other spinal areas. Extension is limited to about 30° with slightly more flexion being possible – roughly 40°. Flexion is freer in the lower thoracic region but still restricted by the ribs. Extension is limited by approximation of the facets and spinous processes as well as tissue tension, and causes the thoracic cage to become flatter. Lateral flexion is limited to roughly 25° to each side, a greater range being available in the lower region. Lateral flexion is accompanied by the same amount of rotation, which occurs contralaterally. For example, right lateral flexion is accompanied by right axial rotation, causing the tip of the spinous process to rest to the left of the mid-line. Rib movements accompany lateral flexion, with the ribs on the concave side compressing and those on the side of the convexity being pulled apart.
The range of rotation is larger than other movements, with 35° being possible to either side. However, when the spine is extended, both lateral flexion and rotation are dramatically reduced. As rotation occurs, the inferior facets of the upper vertebra slide laterally with respect to the lower vertebra, towards the direction of the rotation. Movement of the vertebra is accompanied by distortion of the ribs. The ribcage becomes more rounded on the side to which the rotation is occurring, and flattens on the opposite side.
Rotation of the thoracic spine is an important constituent of locomotion. In walking, when the right leg swings forward, the lower trunk and the pelvis rotate to the left about the fixed left leg. To keep the head facing forwards the upper spine must rotate to the right, pulling the shoulders back into a forward facing direction. As the upper and lower parts of the spine are rotating in opposite directions, there is a point at which the two movements cancel each other out. This point is the intervertebral disc between T7 and T8 which is not subjected to any rotation, while those vertebra immediately above and below rotate maximally, but in opposite directions.
Examination
The screening examination is essentially similar to that of the lumbar spine, except that rotation is the movement most likely to be revealing as this normally has the greatest range. Rotation is performed in a sitting position, with overpressure being given through the shoulders. Resisted flexion and extension may be performed in a lying or a sitting position. Resisted lateral flexion is tested in a standing position with the therapist initially at the patient’s side. The patient’s near wrist of the straight arm is gripped, as is the far shoulder. Stability is improved if the therapist widens his or her base of support by placing the near foot between those of the patient.
As rotation and lateral flexion accompany each other in the thoracic spine, it is often revealing to combine these movements at examination. Thoracic rotation is performed, and is followed by lateral flexion, first in one direction and then the other.
Palpation takes in the vertebrae, rib joints and ribs themselves, and is carried out with the patient in a prone position with the arms over the couch side to move the scapulae apart. Alternatively, posteroanterior (PA) pressures may be used with the thoracic spine extended using the elbow support prone-lying starting position. In a prone-lying position the spinous processes of the thoracic vertebrae are angled downwards like the scales of a fish. The thoracic vertebrae may be considered in threes, with the transverse processes being found relative to the spinous processes as shown in Table 14.1.
Table 14.1 Palpation of the thoracic vertebrae
| T1, 2, 3 | At the same level as spinous process |
| T4, 5, 6 | Between two successive levels |
| T7, 8, 9 | Level with spinous process of vertebra below |
| T10 | Level with vertebra below |
| T11 | Between two successive levels |
| T12 | At same level |
As an approximate guide to levels, the AC joint is normally aligned with the C7–T1 interspace, the spine of the scapula at T3 and the inferior scapular angle at T7.
The rib angles gradually spread out from the spine with the eighth rib being furthest (about 6 cm) from the mid-line. The rib angles can be palpated at the same levels as the transverse processes down to the T8/T9, by pushing the soft tissue to one side. The facet joints lie in the paravertebral sulci, and the transverse processes, which overlie the costotransverse joints, are found 3–4 cm from the mid-line. Guidelines for rib palpation are shown in Table 14.2.
| Rib structure | Region of palpation |
|---|---|
| 1st rib | Above clavicle, within supraclavicular fossa |
| 2nd | End level with manubriosternal joint (angle of Louis) |
| 4th | Lies on nipple line |
| 7th | End level with xiphisternal joint |
| 11th | Tip lies in mid-axillary line |
| 12th | Tip level with L1 |
| Rib angle | 3–4 cm lateral to end of transverse process |
| Costochondral (CC) joint | 3 cm lateral to parasternal line at 2nd rib, 12 cm lateral at 7th rib, 18 cm lateral at 10th rib |
| Costotransverse (CT) joint | Depression between transverse process and rib |
Modifications to the slump test for the thoracic spine
A variation of this test for the cervical and thoracic spine is to perform it in the long sitting position (Fig. 14.3A). From this position thoracic and lumbar flexion are added followed by cervical flexion (Fig. 14.3B). Altering the order of movement will change the neurodynamic demands (Butler and Slater, 1994), enabling the practitioner to refine the test. For example, performing cervical flexion before lumbar and thoracic flexion will challenge the cervical neural tissues more. The test can be further refined to place emphasis on the sympathetic trunk (Slater, Butler and Shacklock, 1994). This is especially relevant in the presence of sympathetic signs in conditions such as T4 syndrome, thoracic outlet syndrome and Raynaud’s syndrome, and in cases where cervicothoracic conditions mimic cardiac disease. Sympathetic testing is achieved by adding components of lateral flexion and rotation of the thoracic spine and lateral flexion of the cervical spine. Additional stress may be imposed by adding a minimal straight leg raise (SLR).

Figure 14.3 The slump test (long sitting). (A) Start. (B) Finish.
From Butler (1991) with permission.
Keypoint
Where sympathetic signs (skin changes, sweating, swelling) are present in conditions such as thoracic outlet syndrome (TOS) and Raynaud’s syndrome, modify the slump test to emphasize the sympathetic trunk. Add thoracic lateral flexion and rotation, and cervical lateral flexion to the standard slump test.
Injury to the ribcage
Direct trauma to the ribcage can result in damage to the ribs, intercostal muscles or, indirectly, to the rib joints. Deep breathing will usually reproduce the pain of rib or intercostal injury, and palpation can be used to reveal the exact site of injury as these structures are superficial. Trunk extension will open the ribcage and cause pain, and intercostal muscle tearing will generally give pain to resisted trunk flexion. Rib springing at a distance from the point of injury usually produces pain from a rib fracture.
Rib fracture
With rib fracture it is the tearing of the intercostal muscles which gives the pain rather than the fracture itself (Cyriax, 1982). The acute pain may be relieved by local strapping. Pre-stretched elastic adhesive strapping is applied across the area to restrict ribcage expansion and give the athlete a feeling of support. In the subacute phase active mobilization is required. If scar tissue formation is excessive and the source of pain, transverse frictions to the intercostal muscles along the line of the ribs are helpful. In addition, holding the rib down with the fingertips and practising deep inspiration will help to stretch the injured area. Exercises to expand the ribcage, such as deep inspiration and overhead reaching, or trunk lateral flexion to the contralateral side with or without rotation is also helpful to stretch the area.
Keypoint
Following rib injury, intercostal muscle stretching is useful. Deep breathing exercises coupled with manual therapy to isolate the movement to a single pair of ribs may also be used.
Where rib trauma is severe, there is a danger of pneumothorax. Here, air enters the pleural cavity changing the pressure within the thorax. The mediastinum is pressed away from the injured lung (mediastinal shift) with the potential to compress vital structures.
Definition
The mediastinum is the central compartment of the thoracic cavity, lying between the lungs. It contains the heart, major blood vessels, trachea, oesophagus, thymus and lymph nodes of the chest.
The athlete experiences severe chest or back pain and becomes breathless. They may begin to cyanose (lips going blue) and panic. First aid treatment is to cover the injured chest region with an airtight seal such as a sterile plastic film or watertight dressing. Examination with a stethoscope (auscultation) reveals an absence of lung sounds on the injured side indicating that air is not entering the lungs. Hospitalization is required, where a chest x-ray may reveal a deep sulcus sign showing that the costophrenic angle (junction of diaphragm and ribs) is abnormally deep. Treatment is by inserting a chest drain into the area outside the affected lung. The drain tube has a one-way valve allowing excess air to escape and the lung to re-expand.
Rib joints
The sternocostal joints may be sprained giving local swelling and tenderness, as may the costochondral joints (Tietze’s syndrome). True Tietze’s syndrome is a swelling of the costrochondral joints which contrasts to costrochondritis which is inflammation alone. Clinically however the two names are interchangeable.
Pressure on the sternum, or applied to the lateral aspect of the thorax, reproduces the pain, and palpation localizes the lesion. The injury can occur when performing exercises which force the arms into extension and abduction. Weight-training movements such as bench pressing and gymnastic exercises such as dips on parallel bars may both cause problems. Both the costovertebral and costotransverse joints may be subject to sprain, with pain occurring to rib movements and local palpation.
Costochondral pain must be differentiated from pain referral into the area from myocardial infarction, and from pathologies such as psoriatic arthritis or ankylosing spondylitis. In chest pain from myocardial infarction there is no history of sports trauma, and pain is vice-like and often described as a ‘clenched fist’ feeling which may refer up into the jaw. Pain of rib origin will be affected by rib movement and posture and is generally well localized. Medical pathologies affecting the ribs will generally have been present for some time and are differentiated by blood tests. Tests include the HLA-B27 genetic marker and erythrocyte sedimentation rate (ESR) which tests for non-specific inflammation throughout the body.
First rib injury
The first is the shortest and roundest of the ribs. It slopes downwards and forwards from its attachment to the first thoracic vertebra. It forms attachment for the scalene muscles, serratus anterior, and subclavius. Its superior surface bears a deep groove for the subclavian artery (posterior) and the subclavian vein (anterior). The arterial groove is the weakest part of the rib (Gurtler, Pavlov and Torg, 1985).
Fractures of the first rib may either be traumatic or the result of overuse. Overuse injuries have been reported as a result of repeated arm movements, such as heavy lifting and pitching (Bailey, 1985; Lankenner and Micheli, 1985; Gurtler, Pavlov and Torg, 1985). Symptoms are of pain associated with deep breathing, tenderness in the root of the neck, posterior aspect of the shoulder or axilla. Often the patient hears or feels a snap in the shoulder as when performing a sudden violent movement. Range of shoulder movement will usually be full but painful, especially to extension. Accurate diagnosis by radiographs in traumatic lesions is essential because of the proximity of the major vessels, nerves and lung. Bailey (1985) recommended serial radiographs for up to 6 months after stress fracture.
Keypoint
1st rib injury gives pain on deep breathing. Tenderness is common at the root of the neck, posterior aspect of the shoulder or axilla. Shoulder extension may also cause pain.
Management is by rest from the causal action, with shoulder support in a sling if pain is limiting. Gentle isometric shoulder exercises are used, and the condition usually resolves within 4–6 weeks.
Rib displacement
Respiratory movements of the ribs may be used to assess anteroposterior position, by comparing one side of the body to the other. If a rib on one side stops moving before the rib on the other side during inhalation, the rib is said to be depressed. Inhalation involves an upward movement of the rib, so if the rib stops moving, it has been held down. Similarly, if the rib stops moving during exhalation (downward movement) it is said to be elevated, because it is being held in an upward position.
Movement may also be forward or backward. An anterior displacement may occur with a subluxation of the costovertebral joint, and the rib is sheared forwards. The rib will appear more prominent than its neighbour. This can occur in sport due to a blow to the back, typically when a knee hits the player on the back of the chest in rugby. A posterior displacement is more common and presents as a prominence of the rib angle. This is normally due to a blow to the chest, again from a tackle or through seatbelt or steering-wheel trauma in a road traffic accident (RTA). Management of rib displacement is by the use of muscle energy techniques (MET) and rib joint mobilization (see Treatment note 14.1).
Treatment note 14.1 Manual therapy techniques for rib displacement
Manual therapy techniques encourage correct rib movement during respiration. Essentially they force the rib into the opposite direction to the one in which they are being held. The rib may be bound down by scar tissue, requiring continuous stretching, or through muscle tightness/shortness, requiring PNF stretching. The intercostal muscles (forced expiration), oblique abdominals (trunk rotation), serratus anterior (scapular protraction), latissimus dorsi (arm adduction), scalenes (1st rib, neck side flexion) and quadratus lumborum (12th rib, trunk side flexion) should all be considered.
Elevation
An elevated rib does not move down far enough during expiration. The aim is to encourage this movement and draw the rib down as the patient breathes out. For the 1st rib pressure is placed over the rib with the knuckle (key grip) (Fig. 14.4). The head is side flexed to relax the anterior scalene and the rib is pressed downwards with expiration. The 2nd rib is gripped within the axilla and pulled downwards as the patient exhales powerfully (Fig. 14.5). The remaining ribs may be gripped with the fingertips or pushed downwards using the knife edge of the hand (Fig. 14.6).



Depresssion
The depressed rib is bound down and stops moving upwards during inspiration. The aim is therefore to encourage further upward movement as the patient breathes in. For the 1st rib, stretch of the anterior scalenes is used (side flex the neck to the opposite side) to pull the rib upwards (Fig. 14.7). For the 2nd rib the finger or thumb pads press on the rib within the axilla (Fig. 14.8), and for the remaining ribs the thumb pad or pisiform presses on the rib undersurface within the intercostal space (Fig. 14.9).



Anterior displacement
Where the rib lies further forward than the rib on the other side of the body, the aim is to open the ribcage and pull the rib backwards. For an anterior rib on the right, the patient sits at the end of the couch with the therapist to the left. The patient folds the arms across the chest. The therapist hooks his or her fingers over the anterior rib and sidebends the patient to the left to open the ribcage, and rotates to the right to encourage the rib to move back (Fig. 14.10).

Posterior displacement
For a posterior rib, the contact area is with the heel of the hand over the rib angle. For a right posterior displacement the action is to sidebend to the left to open the ribcage and rotate to the left to draw the rib forwards (Fig. 14.11). An alternative approach is to perform a posteroanterior mobilization on the rib angle while the patient is prone. The pisiform of one hand performs the action while the pisiform of the other presses over the transverse process of the vertebra on the opposite side to prevent the vertebra from rotating as the rib is mobilized (Fig. 14.12).


Manual therapy
Joint mobilization
A variety of procedures may be used for the thoracic spine (Fig. 14.13).




Figure 14.13 Thoracic mobilisation (A) Using thumbs, (B) Using pisiform pressure, (C) rotatory mobilisaiton using heel of hand, (D) extension using leverage.
As a general note, the close proximity of structures in the thoracic region makes it difficult to assess precisely whether a patient’s symptoms are coming from the intervertebral joint, the costotransverse joint, the costovertebral joints or a combination of all three. For this reason many of the mobilizations affect all of these joints.
Trunk muscles
The trunk muscles are open to injury in the same way as any other muscle in the body, but muscle conditions are often overlooked in the search for signs of more complex injuries involving the intervertebral joints. Injury to the intercostal muscles has already been mentioned, but the abdominal muscles and erector spinae may also give pain from injury or muscle soreness.
Injury to the rectus abdominis has been described in tennis players especially. During the cocking phase of serving the arm is reached overhead and the spine hyperextended stretching the rectus and imposing high leverage forces upon the muscle (Maquirriain et al., 2002). This action requires highly coordinated sequential muscle activity which may break down in the presence of fatigue. Injury to the internal oblique can occur as part of a side strain syndrome during activities such as cricket, hurdling and javelin throwing, for example. Injury to the lateral abdominals is shown as a positive resisted side flexion test. MRI scan has shown separate involvement of the internal oblique, external oblique and transversus abdominis (Humphries and Jamison, 2004), and in each case the non-dominant side was affected. Isolated injury to the internal oblique has also been described in tennis (Maquirriain and Ghisi, 2006) although it is less common. Differential diagnosis must be made from rib fracture and iliac crest avulsion injury, both of which are revealed radiographically.
Keypoint
In side strain syndrome the side (lateral) flexor muscles are affected. The condition must be differentiated from rib fracture and iliac crest avulsion injury.
The abdominal muscles are tested isometrically to eliminate involvement of the spine. A crook-lying position is preferred, as this partially relaxes the iliopsoas. Straight flexion taxes the rectus abdominis while flexion–rotation works the oblique abdominals. Pure rotation is tested in a sitting position, while lateral flexion is tested either in a sitting or standing position.
The upper (supra-umbilical) portion of the rectus abdominis is assessed from a sit-up position, while the lower (infra-umbilical) portion is assessed by lowering the straight legs from 90° hip flexion to work the muscle in a reverse origin to insertion fashion. Comparison is made between the right and left sides of the rectus by palpation, and watching the displacement of the umbilicus which will be pulled to the side of the stronger muscle (Lacote et al., 1987).
Keypoint
During abdominal muscle contraction, movement of the umbilicus may be used to identify muscle imbalance. The umbilicus will deviate towards a stronger muscle, rather than moving inwards (abdominal hollowing), or straight upwards (upper rectus) or downwards (lower rectus).
The oblique abdominals are worked by performing rotation and lateral flexion, Rotation may be gauged using a twisting trunk curl action, for example reaching the right arm towards the left knee or isometric trunk rotation in sitting. Rotation to the left works the right external oblique and left internal oblique and vice versa. Resisted side flexion is performed grasping the patient’s hand and asking them to reach the other hand down to the side of their knee. The transversus abdominis acts to support the viscera and is active in forced expiration. It may be tested with the patient in a prone-kneeling position. From this position the subject breathes out against a resistance (balloon or spirometer) and pulls the abdominal wall in.
The erector spinae are tested in a prone-lying position, the subject being asked to extend the trunk and lift the chest from the couch. Isometric contraction is assessed by having the patient (in a prone-lying position) maintain a horizontal position of the trunk with only the legs supported. Alternatively, the patient should rest the chest over the couch end and attempt to straighten the legs to a horizontal position. The quadratus lumborum is tested with the subject prone, leg extended and slightly abducted, to elevate the pelvis laterally. Traction is placed through the elevated leg to oppose the pull of the quadratus lumborum (Kendall and McCreary, 1983).
Hernia
A hernia is a protrusion of the contents of a cavity through the cavity wall. Most usually an organ or peritoneum is forced through the muscular layer of the abdominal wall at sites of natural weakness where nerves and blood vessels leave the abdomen. The most common types are femoral, inguinal and incisional. Less common types include umbilical, epigastric and hiatus herniae.
Initial management of hernias is conservative, and involves instruction on actions to avoid increasing intra-abdominal pressure. When symptoms persist, surgery is required.
Surgical management and rehabilitation
Open repair is performed under a full anaesthetic and usually results in an 8 cm incision. The hernial sac is either pushed back inside the body or removed, and a plastic mesh placed over the back of the weakened area to create a tension free repair. The skin covering the mesh is closed using dissolving sutures. Using keyhole surgery, three cuts (0.5–1.5 cm) are made into the lower abdomen. Again a plastic mesh is secured over the hernia area and the skin repaired using dissolving sutures. As the keyholes are much smaller than the incision of an open repair, skin healing is faster.
Following surgery it is essential that abdominal muscle contraction is redeveloped, as pain inhibition will often prevent spontaneous recovery. During the immediate post-operative period there are two main concerns, the effect of the anaesthetic and the activities of daily living activities. Fluid intake should be increased to avoid dehydration which will result in a dry stool. Advise the patient to support their scar with the flat of their hand or a large soft pillow. Standard checking of the dressing should be made to ensure no leakage is occurring. Scar site infection should be suspected where body temperature rises, requiring urgent medical referral. Deep breathing exercises are used to avoid air stagnation within the lungs.
By 2−5 days post surgery, walking should be normal with the patient encouraged not to stoop to try to protect the repair area. Ice may be used over the scar area to ease swelling but temperature should be monitored closely as local skin sensation will be impaired. Pelvic floor exercise and abdominal hollowing should be begun as pain allows. Muscle retraining should use tactile cueing (touch and skin brushing), visualization and visual cueing, and repeated contractions. For this latter technique, the deep abdominal muscles are tightened (hollowing), relaxed partially and then tightened again, this time to a greater intensity. From 7−10 days exercise intensity and functionality should be increased progressively.
Sportsman’s hernia
Sportsman’s hernia or groin disruption is a condition which may mimic inguinal hernia in many ways (Gilmore, 1995). To understand the condition we need to look at the structure of the region.
The inguinal canal (Fig. 14.14) is approximately 4 cm long, and transports the spermatic cord in the male, the round ligament in the female, and in both sexes the ilioinguinal nerve. Its anterior wall is formed from the aponeurosis (tendon sheet) of the external oblique supported by the internal oblique muscle at its lateral third. The posterior wall is from the transversalis fascia reinforced by the conjoint tendon at its medial third. The roof of the canal is formed by the internal oblique and transversus abdominis as they merge to form the conjoint tendon running from the pubic crest to the pectineal line of the pelvis. The deep inguinal ring is about 1.5 cm above the mid-point of the inguinal ligament and is an opening in the transversalis fascia. The superficial inguinal ring is a hole in the external oblique aponeurosis and lies at the medial end of the tendon above the pubic tubercle.
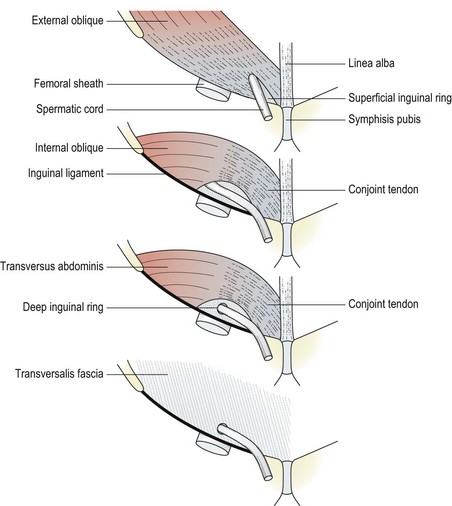
Figure 14.14 Formation of the inguinal canal.
From Palastanga, Field and Soames (1994), with permission.
Definition
The transversalis fascia is part of a membranous bag lining the abdomen; (i) it lies on the deep surface of the transversus abdominis muscle, (ii) its thick lower portion is attached to the inguinal ligament, (iii) the femoral vessels drag the fascia with them as they travel into the leg forming the femoral sheath.
Sportsman’s hernia (athletic pubalgia) is an injury of the muscular and fascial attachments to the anterior pubis (Kachingwe and Grech, 2008). Several structures may be involved (Table 14.3). The condition can include a tearing of the external oblique aponeurosis and the conjoint tendon, causing the superficial inguinal ring to dilate (Fig. 14.15). There may be a dehiscence (separation) between the conjoint tendon and the inguinal ligament but no hernial sac (Gilmore, 1995). The transversalis fascia may weaken and separate from the conjoint tendon (Hackney, 1993) and the external oblique has been said to tear at the site of emergence of the anterior ramus of the iliohypogastric nerve (Williams and Foster, 1995).
Table 14.3 Sportsman’s hernia: tissue pathology and history
| Tissues affected | Typical signs and symptoms | Differential diagnosis |
|---|---|---|
Unverzagt, Schuemann and Mathisen (2008); Kachingwe and Grech (2008).
The condition was originally described in soccer players but may occur in other sports. As many as 28% of soccer players may experience the condition (Kemp and Batt, 1998), and 50% of male athletes presenting with groin pain lasting longer than 8 weeks have been found during surgery to have sports herniae (Lovell, 1995).
There is a gradual onset of pain with one-third of the patients reporting a specific injury which may have resulted in tearing. Pain (in the inguinal, adductor or perineal region) is exacerbated by sports specific kicking actions and sudden changes in movement direction. The superficial inguinal ring is often dilated to palpation. Tenderness to palpation over the conjoint tendon and inguinal canal is increased by a resisted sit-up action. It is usual for several pathologies to coexist, with sportsman’s hernia occurring alongside adductor tendinitis. In a study of athletes with groin pain for more than 3 months, 19 out of 21 were found to have two or more separate pathologies (Ekberg, Persson and Abrahamson, 1988), and in general 25–30% of athletes with this condition can be expected to have a secondary diagnosis (Lovell, 1995).
Keypoint
A sportsman’s hernia is a separation of the external oblique aponeurosis from the inguinal ligament. It is a muscle attachment injury rather than a true hernia and no protrusion (hernial sac) is present.
Imaging may not identify the tissue affected, but is important to rule out alternative diagnoses (Kachingwe and Grech, 2008). Endoscopic examination may be used and followed by immediate repair where a defect is found. Ultrasonography may be used to identify the tissue changes at the exact point of tenderness. Coupled with a Valsalva manoeuvre ultrasound can differentiate true herniation from simple tissue overstretch. The use of colour Doppler permits the visualization of the epigastric vessels, and can assist in the differentiation of sports hernia from inguinal hernia. Direct inguinal hernia is said to lie medial to the inferior epigastric vessels, while the indirect hernia lies laterally to this vessel (Hagan et al., 2007).
Treatment is surgical (open or laparoscopic) where conservative management has failed. Repair of the torn conjoint tendon may be performed using polypropylene mesh and the tendon is approximated to the inguinal ligament. The external oblique is repaired and the inguinal ring reconstituted. Surgical success rates have been reported between 63 and 93% (Kemp and Batt, 1998), possibly reflecting the presence of additional pathologies.
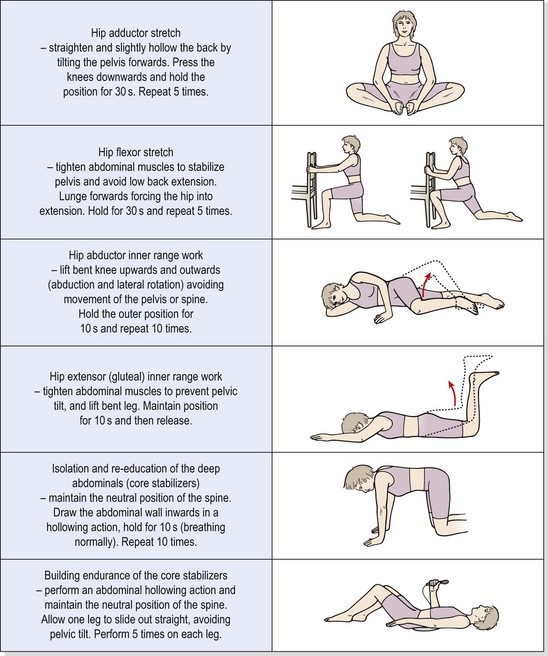
Both prevention (Gilmore, 1995; Norris, 1995) and successful rehabilitation of this condition rely heavily on correct abdominal training. One of the factors in the development of this condition may be a muscle imbalance which is created in the athlete by sit-up exercises. Tightness in the hip flexors, combined with preferential recruitment of the rectus abdominis and poor recruitment of the deep abdominals, leaves the lower abdominal area open to injury. Increasing the training emphasis on abdominal hollowing actions and reducing the emphasis on lumbar flexion actions is a key factor which should be combined with stretching of the tight hip flexors.
In addition, dominance of the adductor muscles in certain sports such as soccer should be considered. Stretching the tight adductors and working the abductors proportionally should be considered. It has been suggested that repeated adductor actions create a shearing force across the pubic symphysis that places stress on the posterior inguinal wall (Simonet, Saylor and Sim, 1995). In support of this hypothesis, it is common clinically to find athletes who have coexisting osteitis pubis and/or adductor tendinitis. Muscle balance exercises relevant to the prevention and rehabilitation of this condition are shown in Table 14.4.
Table 14.4 Muscle balance exercises for sports hernia
Thoracic outlet syndrome
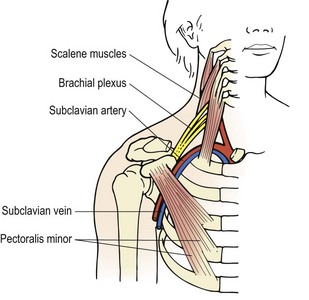
Thoracic outlet syndrome (TOS) affects the superior thoracic aperture, a region bordered by the T1 vertebra posteriorly, the medial edge of the 1st rib and the manubrium of the sternum. TOS is a compression of the neurovascular structures travelling to the axilla from the cervical region and typically involves the brachial plexus rather than the nerve roots (Fig. 14.16). Symptoms appear in the arm rather than the neck, with the lower cervical and upper thoracic area (C8/T1) most commonly affected. Bilateral tingling appears over the median or ulnar nerve distributions into the forearm and hand. The anatomy of the region favours compression. The nervous structures travel through the costoclavicular space, formed by the inner clavicle, first rib and insertions of the scalene muscles. The lower trunk of the brachial plexus and the subclavian artery travel through the outlet formed between the scalenus anterior and scalenus medius to rest on the first rib. Symptoms from vascular compression are less common than those from neurological involvement, but alteration in blood flow may be used as a test for the condition (see below).
Predisposing factors
The more oblique slope of the first rib in the female changes the costoscalene angle (Grieve, 1986) and may account for the increased incidence of the condition in females. Lower down, the neurovascular structures pass into the axilla beneath the coracoid process and the tendon of pectoralis minor.
In the non-athlete, middle-aged women are most commonly affected, with the typical clinical picture consisting of a round shouldered posture displaying a ‘dowager’s hump’ between C7 and T1. The thoracic kyphosis is usually stiff, showing tight pectoral tissues and limited shoulder movements. The thoracic segments and rib angles are often exquisitely tender. The pectoral girdle muscles may have weakened through prolonged disuse, and a ‘poking chin’ head position is common. This postural complex is summarized in Table 14.5.
Table 14.5 Postural presentation in thoracic outlet syndrome
Adapted from Grieve (1986).
In the athletic population, postural changes due to the nature of a sport will make the condition more likely, especially in overhead sporting actions. Excessive shoulder depression or overdevelopment of the trapezius and neck musculature in sports such as American football, rugby and throwing sports will put the athlete at risk. Tightness in the pectoralis minor may occur in swimmers. In tennis players, asymmetrical development with excessive scapular depression has been described (Zachazewski, Magee and Quillen, 1996). Athletes complain of pain and difficulty in gripping.
Carrying heavy objects or wearing a heavy coat exacerbates the problem, and simply allowing the arm to hang freely by the side can cause aching. The condition is seen commonly as an occupational injury, with the subject often noticing increased pain when reaching overhead. Typically, this pattern also occurs when a middle-aged woman takes up exercise in a keep-fit class. When severe, vascular signs such as coldness, blueing or whiteness of the skin may occur if the subclavian artery is affected. Equally, the patient may be woken at night with pain, or can experience numbness first thing in the morning.
Provocative tests for TOS
Various provocative tests are available which aim to reproduce the patient’s symptoms. Sustained scapular elevation, or simply holding the arms overhead may increase the signs. The Adson test examines the radial pulse while the patient breathes in deeply and holds the breath, at the same time extending the neck and rotating it either towards or away from the affected side. Abduction of the shoulder to 90° with full external rotation, combined with vigorous hand movements, may give rise to symptoms if compression is significant. This is sometimes called the elevated arm stress test (EAST) or abduction−external rotation (AER) position test (Fig. 14.17). In addition, exaggerating the military posture and at the same time placing longitudinal traction through the arms may limit the costoclavicular space and reproduce symptoms (Grieve, 1986).
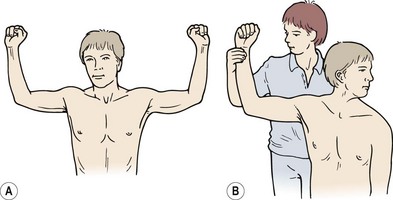
Figure 14.17 Provocative tests for thoracic outlet syndrome. (A) EAST test. (B) Modified Adson’s test.
Examination of the thoracic spine should also be made to differentiate the condition from T4 syndrome (see below), and the long-sitting slump test and upper limb tension tests should be performed.
Treatment
Conservative management is to elevate the scapulae in the first instance. Simply strengthening the trapezius may have little effect, first because the trapezius, as an anti-gravity muscle, is usually very strong, and secondly because the stronger muscle may still not be used correctly. Postural re-education is more successful, teaching a less depressed shoulder girdle resting position. Enhancement of scapular stability with scapular repositioning exercises, and modification of sport technique will also be required.
Tightness of the scalenes and pectoral muscles demands gentle PNF stretching techniques, and trigger point deactivation. Mobilization procedures of the thoracic spine are also helpful. Where neural tension tests are positive, mobilization of the neural tissues is required.
Vascular involvement
Vascular conditions which affect the upper limb in sport, although rare, are important, and are described in this chapter rather than Chapter 18. If missed, these conditions can lead to vascular insufficiency with serious long term effects. Early retirement from sport may be one result, but the worst case scenario is death as a result of a thromboembolus (Taylor and Kerry, 2003). Five more common vascular conditions are described below.
Definition
A thrombosis is a blood clot which forms within a blood vessel, occluding its flow. An embolism occurs when part of the thrombosis clot breaks loose and blocks a vessel further down.
Assessment of vascular involvement
The presentation of vascular injury can closely mimic other musculoskeletal conditions, but closer observation of the patient is often revealing. Skin changes including temperature and colour alterations may be noticed, with distal symptoms increasing on exertion. Symptoms will most commonly be provoked by placing the athlete’s limb into positions with a history of pain and increasing effort. Examination of the nail bed will often show capillary refill time to be prolonged. Here, the athlete’s nail is compressed until it goes white and then released. Normal pink skin colour should return immediately on pressure release; failure to do so suggests vascular insufficiency.
Keypoint
Capillary refill time is assessed by compressing the nail beds on the affected limb and comparing to the unaffected side. The nail goes white on compression and should return to normal skin colour upon release. Slowing of colour restoration indicates vascular involvement.
Distal pulses should be examined during positional changes and after exertion. Pulses on both sides of the body should be taken and compared. Following exertion the pulse strength should increase. Where vascular insufficiency results from compression by muscle, pulse strength can reduce in the distal limb following exertion. Assessment of the pulse is refined by using Doppler ultrasound. This measures the velocity of blood flowing towards and away from the machine probe to give an audible signal. The Allen test is also commonly used for upper limb vascular conditions. The test measures the collateral circulation in the hand which is supplied by the radial and ulnar arteries. To perform the test the athlete lifts their hand overhead and opens and closes their fist for 30 seconds. The therapist applies pressure over both the radial and ulnar arteries to cut off the blood flow to the hand. Keeping the hand elevated, the hand is opened and it appears whitened. Pressure is released from the ulnar artery and colour should return in 7−10 seconds, showing that the artery is normal. The test is repeated releasing the radial artery. The arm to arm blood pressure index (AABI) may also be used, which measures the systolic pressure of the symptomatic arm and compares this to the unaffected arm both before and after effort. A difference greater than 30−50 mmHg in systolic pressure is said to indicate reduced subclavian blood flow (Alan and Kerry, 2003).
T4 syndrome
The T4 syndrome (Maitland, 1986; McGuckin, 1986) produces vague widespread symptoms of pain and paraesthesia in the upper limbs and head, possibly with autonomic involvement. Any region between T2 and T7 may be affected, but the focus is normally around T4. The distribution of symptoms in the hand is glove-like in contrast to that of thoracic outlet syndrome, but many subjects have sensations extending from the wrist and forearm. Head symptoms appear in a ‘skull cap’ distribution, and the patient is commonly woken with pain. Onset may be due to unaccustomed activities or trauma (road traffic accident), but in many cases there is no specific history of injury. As with thoracic outlet syndrome, a predisposing factor is postural. Head protraction, shoulder girdle protraction and accentuated thoracic kyphosis are common, and place a stretch on the thoracic tissues.
Keypoint
Thoracic outlet syndrome gives bilateral tingling over the median or ulnar nerve distributions into the forearm and hand, but generally no head symptoms. T4 syndrome gives glove-like symptoms affecting the whole hand, and altered sensation in a skull cap distribution over the head.
On examination, movements can be localized by performing rotations and flexion/extension from a slumped sitting starting position. Palpation is carried out with the patient prone, head in mid-position, with the therapist standing at the patient’s head. The patient’s forearms hang over the couch side and the upper arms are abducted to 90° to widen the interscapular space. Signs of joint localization include pain, resistance to passive movement and guarding muscle spasm. Common findings include alteration of the alignment of one spinous process in comparison with its neighbours, with local pain to palpation. Examination must take in the cervical spine and first rib. The first rib is palpated above the centre of the clavicle, with the direction of pressure aimed towards the patient’s lower scapula.
Mobilization is used for any joints which exhibited signs at examination, and may be carried out with the patient in a supine position, arms folded across the chest and hands placed over the anterior aspect of the shoulders. The therapist places one hand beneath the patient’s thoracic spine with the side of his or her thumb or hand in contact with the area to be mobilized. Downward pressure is exerted through the patient’s arms onto the therapist’s hand. Postural correction may be carried out as with thoracic outlet syndrome.
Scheuermann’s disease
Scheuermann’s disease (juvenile osteochondrosis of the spine) is a condition predominantly affecting the thoracic spine around T9, although the lumbar levels may be involved (Greene, Hensinger and Hunter, 1985). The condition is more common in males, and occurs in about 6% of the adolescent population in the 12–18 age group (Corrigan and Maitland, 1983). There is a disturbance of the normal ossification of the vertebrae. The vertebrae ossify from three centres, one at the centre of the vertebral body and two secondary centres (the ring epiphyses) in the cartilage end plates. In Scheuermanns’s disease there is an alteration of the normal development of the ring epiphyses, but avascular necrosis does not occur (Gartland, 1987) in contrast to true osteochondrosis. Penetration of discal material is often seen through the cartilage end plate of the disc and into the vertebral body (Schmorl’s nodes). The changes are largely developmental, but trauma may play a part in exacerbating the condition. In contrast, when the central bony nucleus is affected Calve’s vertebral osteochondritis is present, a much less common condition affecting a single vertebra.
The changes in Scheuermann’s disease are primarily to the anterior margins of the thoracic vertebra as these bear greater weight. The disc narrows anteriorly, and deficient growth of the vertebral body occurs as a result of epiphyseal malformation. The vertebra gradually takes on a wedged formation. Normally, several vertebrae are affected in the thoracic spine. The athlete is usually a skeletally immature adolescent, with a ‘rounded back’ posture. In the active stage of the condition there may be localized pain, often provoked by repeated thoracic flexion as occurs in certain swimming strokes (butterflier’s back) and aerobic dance classes. Deep notches are visible over the anterior corners of the vertebrae on x-ray, and these appear sclerotic rather than rarefied (Fig. 14.18). The ring epiphyses are irregular, but the erythrocyte sedimentation rate (ESR) is normal.

Keypoint
In Scheuermann’s disease several thoracic vertebrae take on a wedged formation giving a rounded back posture. Pain is exacerbated by repeated thoracic flexion.
The condition is self-limiting, with pain generally ceasing at the end of skeletal growth. In the active stage rest is required, and thoracic taping may reduce pain through deload. In more severe cases, especially those affecting a number of thoracic segments where kyphosis exceeds 30°, a spinal brace (Milwaukee brace) may be required to prevent gross deformity. An exercise programme to prevent further deformity is essential. This normally involves strengthening in extension and patient education to avoid repeated flexion during activities and prolonged flexion in sitting and lying. In addition, increasing the lumbar lordosis and stretching the hamstrings has been recommended (Corrigan and Maitland, 1983).
A 4−6 week rehabilitation programme consisting of postural re-education, physiotherapy pain modalities (including acupuncture) and psychological support has been shown to reduce pain by 16−32% in a study of 351 patients with Scheuermann’s disease (Weiss, Dieckmann and Gerner, 2002). The maximum kyphotic angle was reduced from an average of 60.7° prior to treatment to 54.9° following physiotherapy treatment (Weiss, Dieckmann and Gerner, 2003).
Exercise therapy for the thoracic spine
As well as restoring fitness components to this body area (such as mobility and strength) following injury, posture is a prime consideration. One of the common postural faults in this region is an increase in kyphosis. The increased thoracic curve often begins with scapular abduction which moves the centre of gravity of the upper body forwards. In time, the thoracic spine flexes further as a result of the change in equilibrium. The increased curvature has a direct effect on scapulohumeral rhythm by limiting scapulothoracic motion and preventing the final degrees of abduction and extension of the glenohumeral joint. Reversing this trend requires a reduction in thoracic curvature to move the centre of gravity posteriorly, shortening of the shoulder retractors, and often restoration of correct shoulder depressor action. In the following section, examples are given of exercises to correct thoracic curvature by increasing extension. General examples of mobility exercises are also given for use in the restoration phase of injury.
Thoracic extension can be performed in a lying position. The pelvis is posteriorly tilted to flatten and block the lumbar spine, and the arms are lifted to the side and eventually overhead (Fig. 14.19A). Lifting the sternum to extend the thoracic spine without expanding the ribcage (Fig. 14.19B) is also a useful exercise and may be practised in a sitting, high kneeling or standing position. In elbow support prone kneeling (Fig. 14.19C) thoracic extension is performed by pressing (thrusting) the chest towards the floor. Passive extension may be performed by lying over a rolled towel, with the towel positioned at the apex of the thoracic curve (Fig. 14.19D). If the head does not rest on the mat, a thin pillow is used to prevent a protracted head position.



Figure 14.19 Exercise therapy for thoracic extension. (A) Thoracic extension, (B) Thoracic extension using towel as pivot, (C) Sternal lift.
Thoracic mobility to rotation and lateral flexion may be localized to various segmental levels (Fig. 14.20). Mobility to rotation is performed in a sitting position, and may be localized by changing the position of the arms. Leaving the arms at the sides and leading the movement with the head (looking around to the direction of movement) will focus movement to the upper thoracic spine. Holding the elbows horizontally stresses the mid-thoracic spine, which when reaching overhead pulls through the thoracolumbar fascia to stress the lower thoracic spine. Side (lateral) flexion may be mobilized by side-bending against a wall to prevent flexion/extension. With the hands by the sides (reach for the side of the knee) the lower thoracic region is stressed. Placing the hands behind the head and reaching up with the elbow transfers the centre of rotation higher up. Side-lying over a cushion or roll with the upper arm reaching overhead will stretch the muscles of side flexion as well as mobilizing the thoracic spine.
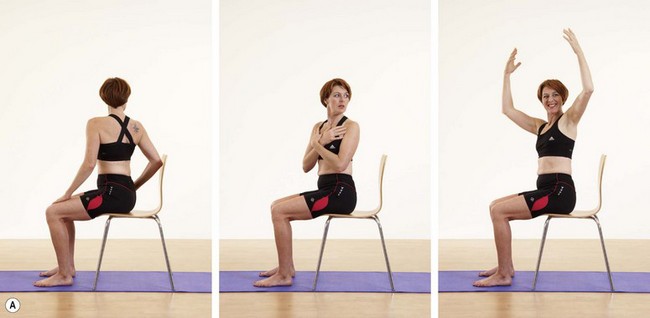

Figure 14.20 (A) Thoracic mobility exercises: (i) upper, (ii) mid, (iii) lower. (B) Thoracic side flexion: (i) lower region, (ii) upper region, (iii) side flexor stretch.
Examples of strength exercises for the thoracic spine musculature include single- or double-handed rowing actions, pull-downs and modified dips (Fig. 14.21).

Alan P., Kerry R. Vascular issues in sports. Part 1: the lower limb. Sportex Medicine. 2003;14:32-37.
Bailey P. Surfer’s rib: isolated first rib fracture secondary to indirect trauma. Annals of Emergency Medicine. 1985;14:346-349.
Bourdillon J.F. Spinal Manipulation. Oxford: Butterworth-Heinemann; 1982.
Butler D.S. Mobilization of the Nervous System. Edinburgh: Churchill Livingstone; 1991.
Butler D.S., Slater H. Neural injury in the thoracic spine: a conceptual basis for manual therapy. In Grant R., editor: Physical Therapy of the Cervical and Thoracic Spine, second ed, Edinburgh: Churchill Livingstone, 1994.
Corrigan B., Maitland G.D. Practical Orthopaedic Medicine. London: Butterworth; 1983.
Cyriax J. eighth ed Textbook of Orthopaedic Medicine vol. 1 London: Baillière Tindall, 1982.
Ekberg O., Persson N.H., Abrahamson P. Longstanding groin pain in athletes: a multidisciplinary approach. Sports Medicine. 1988;6(1):56-61.
Gartland J.J. Fundamentals of Orthopaedics, fourth ed. Philadelphia: W.B. Saunders; 1987.
Gilmore Gilmore, O.J.A., 1995. Personnal communication.
Greene T.L., Hensinger R.N., Hunter L.Y. Back pain and vertebral changes simulating Scheuermann’s disease. Journal of Pediatric Orthopaedics. 1985;5:1-7.
Grieve G.P. Modern Manual Therapy of the Vertebral Column. London: Churchill Livingstone; 1986.
Gurtler R., Pavlov H., Torg J.S. Stress fracture of the ipsilateral first rib in a pitcher. American Journal of Sports Medicine. 1985;13:277-279.
Hackney R.G. The sports hernia: a cause of groin pain. British Journal of Sports Medicine. 1993;27(1):58-62.
Hagan I., Burney K., Williams M., Bradley M. Sonography reveals casues of acute or chronic groin pain. Diagnostic Imaging. 2007;29:33-40.
Humphries D., Jamison M. Clinical and magnetic resonance imaging features of cricket bowler’s side strain. British Journal of Sports Medicine. 2004;38:e21.
Kachingwe A., Grech S. Proposed algorithm for the management of athletes with athletic pubalgia (sports hernia): a case series. Journal of Orthopaedic and Sports Physical Therapy. 2008;38(12):768-781.
Kemp S., Batt M.E. The sports hernia: a common cause of groin pain. Physician and Sportsmedicine. 1998;26(1):1-6.
Kendall F.P., McCreary E.K. Muscles Testing and Function, third ed. Baltimore: Williams and Wilkins; 1983.
Lacote M., Chevalier A.M., Miranda A., Bleton J.P., Stevenin P. Clinical Evaluation of Muscle Function. Edinburgh: Churchill Livingstone; 1987.
Lankenner P.A., Micheli L.J. Stress fracture of the first rib: a case report. Journal of Bone and Joint Surgery. 1985;67A:159-160.
Lovell G. The diagnosis of chronic groin pain in athletes. Australian Journal of Science and Medicine in Sport. 1995;27(3):76-79.
Magee D.J. Orthopedic Physical Assessment, fourth ed. Philadelphia: Saunders; 2002.
Maitland G.D. Vertebral Manipulation, fifth ed. London: Butterworth; 1986.
Maquirriain J., Ghisi J. Uncommon abdominal muscle injury in a tennis player: internal oblique strain. British Journal of Sports Medicine. 2006;40:462-463.
Maquirriain J., Ghisi J., Mazzucco J., Kokali A. Abdominal muscle strain injuries in the tennis player. Medicine and Science in Tennis. 2002;3:14-15.
McGuckin N. The T4 syndrome. In: Grieve G.P., editor. Modern Manual Therapy of the Vertebral Column. Edinburgh: Churchill Livingstone, 1986.
McKenzie R.A. The Cervical and Thoracic Spine: Mechanical Diagnosis and Therapy. New Zealand: Spinal Publications; 1990.
Norris C.M. Postural Considerations in Training, Presentation to the Football Association Medical Committee. England: Lilleshall; 1995.
Palastanga N., Field D., Soames R. Anatomy and Human Movement, second ed. Oxford: Butterworth-Heinemann; 1994.
Read M.T. A Practical Guide to Sports Injuries. Oxford: Butterworth-Heinemann; 2000.
Simonet W.T., Saylor H.L., Sim L. Abdominal wall muscle tears in hockey players. International Journal of Sports Medicine. 1995;16(2):126-128.
Slater H., Butler D.S., Shacklock M.O. The dynamic central nervous system: examination and assessment using tension tests. In Boyling J.D., Palastanga N., editors: Grieve’s Modern Manual Therapy, second ed, Edinburgh: Churchill Livingstone, 1994.
Taylor A., Kerry R. Vascular issues in sports. Part 2: the upper limb. Sportex Medicine. 2003;15:9-13.
Unverzagt C., Schuemann T., Mathisen J. Differential diagnosis of a sports hernia in a high school athlete. Journal of Orthopaedic and Sports Physical Therapy. 2008;38:63-70.
Weiss H.R., Dieckmann J., Gerner H.J. Effect of intensive rehabilitation on pain in patients with Scheuermann’s disease. Studies in Health Technology and Informatics. 2002;88:254-257.
Weiss H.R., Dieckmann J., Gerner H.J. The practical use of surface topography: following up patients with Scheuermann’s disease. Pediatric Rehabilitation. 2003;6(1):39-45.
Williams P., Foster M.E. Gilmores groin—or is it? British Journal of Sports Medicine. 1995;29(3):206-208.
Zachazewski J.E., Magee D.J., Quillen W.S. Athletic Injuries and Rehabilitation. Philadelphia: Saunders; 1996.