CHAPTER 18 The elbow
Structure and function
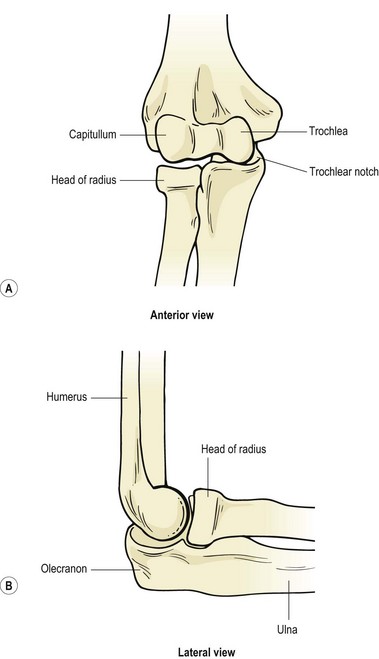
The primary purpose of the shoulder is often described as positioning the arm to facilitate hand action. The elbow, in turn, functions to shorten or lengthen the arm, largely to allow the hand to be brought to the mouth. The elbow complex consists of the humeroulnar and humeroradial articulations and the superior radioulnar joint, all of which share the same capsule (Fig. 18.1).
Definition
Joints within the elbow are: humeroulnar between the trochlea of the humerus and the trochlea notch of the ulnar; humeroradial between the capitulum of the humerus and the superior surface of the head of the radius; superior radioulnar between the circumference of the head of the radius and the fibro-osseous ring formed by the radial notch of the ulna and the annular ligament.
When viewed from the side, the distal end of the humerus is larger anteriorly and inferiorly, and sits at an angle of 45° to the longitudinal axis of the bone. Similarly, the trochlear notch of the ulna bulges, making a comparable angle to its axis. This structure postpones contact between the humerus and ulna on flexion, and allows more space between the bones to accommodate soft tissues. The ‘nutcracker effect’ is therefore reduced as the bones come together.
Bony alignment and joint contact areas
Viewed from the front, the radius and ulna are slanted laterally to the shaft of the humerus, the angulation forming the carrying angle (Fig. 18.2A). This is approximately 10–15° for men, increasing to 20–25° for women. This bony alignment means that normally, as the arm is flexed the hand moves towards the shoulder, and the radius and ulna end up in line with the humerus (Fig. 18.2C). Variations in carrying angle between individuals, mainly due to altered configuration of the trochlear groove, may occur and will alter the resting position of the radius and ulnar at full flexion (Fig. 18.2B,D). Changes in bony alignment may also occur after injury – an important factor in rehabilitation following elbow fractures.
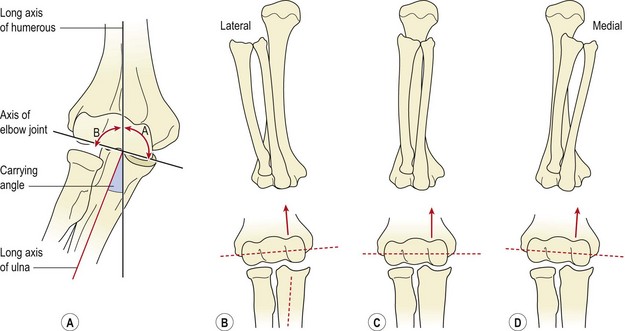
Figure 18.2 (A) Carrying angle. (B) Lateral orientation. (C) Most common configuration of the trochlear groove. (D) Medial orientation.
After Norkin, C.C. and Levangie, P.K. (1992) Joint Structure and Function, 2nd edn. Davis, Philadelphia. With permission.
The contact area between the joint surfaces of the elbow complex increases throughout flexion. In full extension the lower medial part of the trochlear notch of the ulna is used, with no contact occurring between the radius and ulna. At 90° the contact area is a diagonal (lower medial to upper lateral) across the trochlear surface, with only slight pressure between the humerus and radial head. In full flexion definite contact occurs between the radius and ulna, and the trochlear contact areas increase (Fig. 18.3). Full flexion is thus required to ensure adequate nutrition of the whole articular cartilage, a situation sometimes not possible in obese or heavily muscled individuals due to the approximation of the flexor soft tissues.
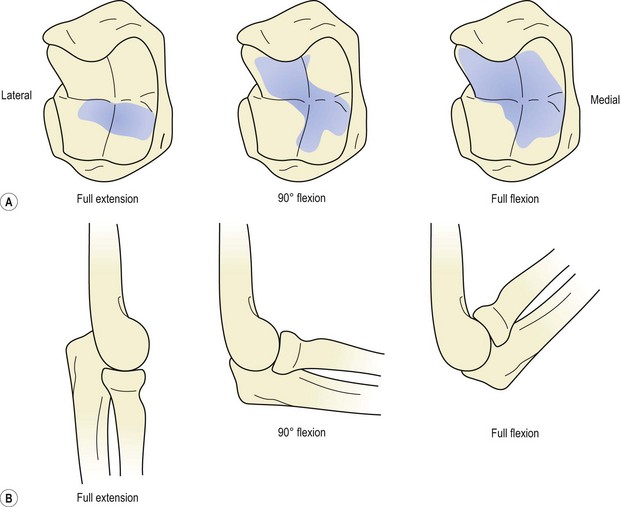
Figure 18.3 Contact areas at different elbow positions. (A) The trochlear notch. (B) The head of the radius.
From Palastanga, Field and Soames (1989), with permission.
Collateral ligaments
The elbow collateral ligaments are positioned on the ulnar (inner) and radial (outer) aspects of the joint. The ulnar or medial collateral ligament (MCL) spreads out from the medial epicondyle to form two thick anterior and posterior bands, joined by a thinner intermediate (oblique) portion. The radial or lateral collateral ligament (LCL) is a single triangular structure attaching just below the lateral epicondyle and blending with the annular ligament of the radius.
As occurs in the knee, the collateral ligaments of the elbow become taut at different degrees of flexion. The anterior fibres of both the medial and lateral collateral ligaments are taut in extension, whereas the posterior fibres are taut in flexion. Protection is provided against valgus and varus strains throughout the whole range of joint movement as a result.
Flexion is limited by muscle contact and impingement of the radial head on to the radial fossa. In addition, tension occurs in the triceps and posterior joint capsule, and finally, in lean individuals, the shafts of the radius and humerus themselves come into contact (Fig. 18.4A).
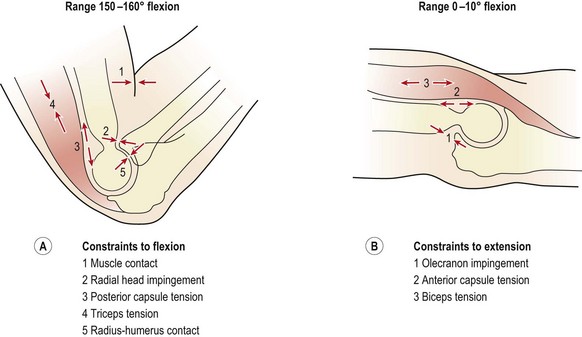
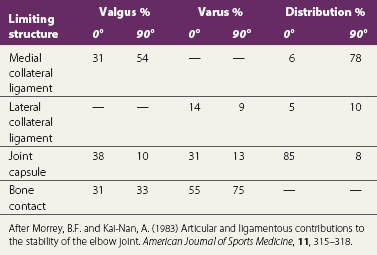
In extension, when the muscles are relaxed, valgus stability is provided by the medial collateral ligament, anterior capsule and bony configuration. As the elbow flexes, the anterior capsule relaxes, and its role is taken on by the medial collateral ligament, which provides 31% of joint stability in extension and 54% at 90° flexion (Table 18.1). In contrast, varus stress is resisted in the main by bone contact supplemented by the anterior capsule. The lateral collateral ligament only contributes 14% of the total stability of the joint with the elbow in full extension, and 9% with it flexed to 90° (Morrey and Kai-Nan, 1983). With joint distraction, the main limiting factor in extension is the joint capsule, and with the joint flexed to 90°, the medial collateral ligament. End-range is limited by a combination of the olecranon impinging into the olecranon fossa, and tension in the anterior capsule and biceps (Fig. 18.4B).
Pronation and supination of the forearm involve not just the superior and inferior radioulnar joints, but also the ulnohumeral, radiohumeral and radiocarpal joints. With pronation, the head of the radius twists on the capitulum and swings on the radial notch of the ulna, tightening the quadrate ligament. The radial head tilts, and is pulled into the capitulotrochlear groove, and the ulna moves into slight extension and abduction at the ulnohumeral joint (Lee, 1986). Consequent to this, at the inferior radioulnar joint the ulnar notch of the radius swings medially over the ulnar head. A traumatic injury to the elbow is therefore likely to affect the wrist, and, to be complete, clinical examination should include both joints.
Screening examination
Following inspection, objective examination begins with flexion and extension, each performed to full range, noting the joint end-feel. The normal end-feel to extension is hard while that to flexion is soft. Pronation and supination are performed with the elbow held to the side of the body and arm flexed to 90°. The end-feel should be springy. Further differentiation may be obtained by combining flexion and extension with abduction and adduction (valgus/varus) stresses, and by assessing gliding motions of the individual component joints of the elbow complex (Fig. 18.5). The capsular pattern is of flexion more limited than extension, and rotations relatively free.


Figure 18.5 (A) Abduction; (B) adduction; (C) flexion−abduction; (D) flexion−adduction; (E) pronation; (F) supination; (G) compression; (H) distraction.
The inferior radioulnar joint is stressed by pronation and supination, and may require further examination if pain is produced. Screening examinations of the neck and shoulder are performed if referred pain is suspected, and full neurological examination may be required. The front of the elbow lies within the C5 and C6 dermatomes, while the back of the elbow is in the C7 dermatome. Pain may therefore be referred to the elbow from the cervical nerve roots or the shoulder region.
The contractile structures are examined by resisted movements, performed firstly with the elbow flexed to 90°. One of the therapist’s hands supports the elbow to restrict shoulder movement and the other applies resistance to flexion and extension. For pronation and supination, the lower forearm (not the hand) is gripped. The grip must be tight and positioned over the radial styloid to avoid a friction burn to the patient’s skin. Resisted wrist flexion and extension are performed with the elbow locked.
Ligamentous instability may be assessed by combining movement of the forearm and upper arm. The MCL is assessed by applying an abduction force to the forearm with the elbow unlocked. At the same time the humerus is laterally rotated. For the LCL the technique is reversed, an adduction force being imposed on the forearm and the humerus pulled into medial rotation. In each case both excessive movement and reproduction of the patient’s symptoms indicate a positive test result.
Lateral pain
The term ‘tennis elbow’ is often used colloquially as a blanket description for any soft tissue pain between the shoulder and wrist, and there has been little agreement in the past as to the exact site of the lesion. The condition was first documented in the late 1800s when it was described as ‘lawn tennis arm’. Cyriax (1936) described 26 different lesions to which the condition had been attributed, while Lee (1986) cited 12 more general causes, as shown in Table 18.2. The terms ‘lateral’ and ‘medial tennis elbow’ have been used (Nirschl, 1986), but in this book the name tennis elbow is used to describe lateral epicondylitis while ‘golfer’s elbow’ refers to medial epicondylitis. The ratio of lateral to medial epicondylitis encountered clinically has been shown to be 7 : 1 (Leach and Miller, 1987).
Table 18.2 General causes of tennis elbow
From Lee, D.G. (1986) Tennis elbow: a manual therapist’s perspective. Journal of Orthopaedic and Sports Physical Therapy, 12(2), 81–87. With permission.
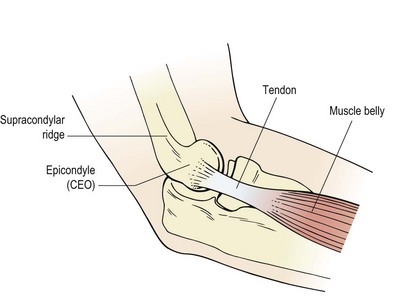
Tennis elbow (lateral epicondylalgia) is a lesion to the common extensor origin (CEO), with the primary site being the tendon of extensor carpi radialis brevis (ECRB) and/or the extensor carpi radialis longus (ECRL). ECRL attaches to the lateral supracondylar ridge (lower third) and travels to the base of the 2nd metacarpal, while ECRB attaches more distally to the lateral epicondyle itself via the common extensor tendon where it spreads onto the lateral ligament of the elbow. From here the muscle inserts into the base of the 3rd metacarpal. When testing for tennis elbow (see below) the muscles may be differentiated by placing resistance over the 2nd and 3rd metacarpals. Pain with rested middle finger extension (3rd metacarpal) suggests ECRB. Most commonly, the injury is at the tenoperiosteal junction of the tendons, but scar tissue may form onto the tendons themselves or the musculotendinous junction (Fig. 18.6).
Keypoint
Tennis elbow affects: (i) the tendon of extensor carpi radialis brevis at the epicondyle; (ii) tendon of extensor carpi radialis longus onto the supracondylar ridge.
Pathophysiology
The pathological features of tendinopathy have been covered in previous chapters for the Achilles (Chapter 10), patellar tendon (Chapter 9) and rotator cuff (Chapter 17). In the case of tennis elbow local tendon pathology is that of immature and dysfunctional healing called angiofibroblastic hyperplasia. This process has four key elements: (i) Collagen cell numbers and the amount of ground substance increase, (ii) vascular hyperplasia (neovascularization) is seen, (iii) there is an increase in the concentration of local neurochemicals and (iv) collagen is both disorganized and immature (Coombes, Bissel and Vicenzino, 2009). In line with other types of tendinopathy, standard inflammatory markers are not present, although neurogenic inflammation has been identified (Fredberg and Stengaard-Pedersen, 2008).
Definition
Neurogenic inflammation occurs when there is a local release of inflammatory chemicals from sensory (afferent) nerves. Chemicals involved include substance P, calcitonin gene-related peptide (CGRP) and glutamate.
Stress imposed on the affected tissues is not uniform, with the deeper tendon regions being placed under lesser load (stress shielding). These areas may be open to overload, and in the case of ECRB the deep and anterior fibres have been highlighted as potentially problematic.
In addition to tendon pathology both pain system change and motor impairment have been proposed as important for a multimodal treatment approach (Coombes, Bissel and Vicenzino, 2009). As with many painful conditions tennis elbow is characterized by an exaggerated response to noxious stimuli (hyperalgesia). Testing local pain response using pressure, tennis elbow sufferers have been shown to have a lower pain threshold (66%) on the injured side compared to the uninjured side (Pienimäki et al., 2002). This change in pain threshold is often bilateral implying an alteration in central sensitization. In addition tennis elbow sufferers often have positive cervical joint signs and/or positive radial nerve bias upper limb tension test (ULTT), suggesting that neural involvement is not restricted to the local tissues.
Morphological changes in the muscles affected by tennis elbow include fibre necrosis, increased fast twitch fibre ratio and muscle fibre regeneration (Coombes, Bissel and Vicenzino, 2009), consistent with the finding that grip strength is reduced in tennis elbow patients. In addition motor control changes occur with wrist position changing during standard grip task with less extension being present. Normal grip requires the wrist extensors to stabilize the wrist against the strong pull of the long finger flexors which tend to flex the wrist. In a group of 40 subjects Bisset et al. (2006) showed wrist postures that were less extended (mean value 11°) and upper-limb reaction times which were significantly altered.
Clinical presentation
Tennis elbow usually presents as pain over the region of the lateral epicondyle, extending distally. The pain may build up slowly (overuse) or be the result of a single incident (trauma). Pain is usually increased with resisted wrist extension. Depending on the site of the lesion, pain can be made worse by adding forearm supination (but see radial tunnel syndrome, below), and radial deviation of the wrist (Halle, Franklin and Karalfa, 1986). Performing resisted wrist extension with the elbow fully extended will usually elicit pain, even in mild cases. Resisting the 3rd metacarpal places the emphasis on ECRB rather than ECRL which attaches to the base of the 2nd metacarpal (Maudsley’s test).
The condition is most common with athletes over 30 years of age, and occurs normally when repeated wrist extension is combined with forearm supination. Racquet sports involve this action, but several occupational stresses can also be causal factors. Hammering, painting and using heavy spanners will all exacerbate the problem, so any training modification which is prescribed must also take into account an athlete’s job. Pain usually increases when small objects are gripped, as this hand position places additional stretch on the forearm extensors.
Keypoint
Tennis elbow is exacerbated by activities involving repeated wrist extension while gripping a thin object.
As with most overuse syndromes, the ache may initially subside when the stressful activity is discontinued, but as the condition progresses pain even occurs at rest. Patients complain of a weak grip, and wasting of the affected muscles may be seen in long-standing cases. Close inspection will often reveal slight swelling over the affected area, but this is rarely obvious to the patient.
Treatment
Acute phase
Treatment aims initially to reduce pain and swelling. The PRICE protocol is used, and several authors have reported good results by using ultrasound, alone or with hydrocortisone gel (Griffen and Touchstone, 1963; Kleinkort and Wood, 1975; Halle, Franklin and Karalfa, 1986). Reducing the stress applied to the tendon is important. Rest from exacerbating activities and the use of counterforce bracing are effective. The counterforce brace consists of a tight strap which is placed around the upper forearm to create a lateral pressure when an object is gripped. The aim is to redirect and disperse overload to healthy tissue or to the band itself, and in so doing reduce painful inhibition and permit a more forceful contraction. Using this technique, grip strength has been shown to improve (Burton, 1985; Wadsworth et al., 1989), and a positive effect has been shown using biomechanical analysis and technique correction of tennis serves and backhand strokes (Groppel and Nirschl, 1986).
The use of nitric oxide given in a transdermal patch as glyceryl trinitrate (GTN) has been described in the treatment of tennis elbow (Paoloni et al., 2003). When compared to placebo patients in the glyceryl trinitrate group had significantly reduced pain with activity, reduced epicondylar tenderness and increased wrist extensor force. A concentration of 1.25 mg/24 hours is traditionally used, cutting a 0.5 mg patch into four and applying this quarter of a patch each day. However, a more recent study (Paoloni et al., 2009) did not support these earlier results, showing a significant decrease in elbow pain with activity using GTN at a concentration of 0.72 mg/day compared to placebo, but not with 1.25 mg/24 hours, 1.44 mg/24 hours or 3.6 mg/24 hours. In addition GTN patches can give complications including headache, weakness, dizziness and skin irritation causing 12% of patients to discontinue treatment as a result of these side effects (Coombes, Bissel and Vicenzino, 2009).
Exercise
As the local swelling adheres and shrinks, inelastic scar tissue is formed. Stretching exercises are therefore of particular value. A useful forearm extensor stretch may be performed with the athlete facing a wall (Fig. 18.7A). The dorsum of the hand is placed flat onto the wall, and the elbow remains locked. By leaning forwards the wrist is forced into 90° flexion, stretching the posterior forearm tissues. Wrist flexion may be combined with a pronation stretch (Fig. 18.7B). Keeping the elbow locked, the forearm is maximally pronated and the wrist flexed. Overpressure is applied with the other hand and a static stretch performed. The scar tissue is more pliable when warm and so the athlete is advised to practise stretching after a hot bath or shower. Resistance exercises (weight or powerband) are used to re-strengthen the forearm extensors. Wrist extension may be performed holding a small (2 kg) dumb-bell. The forearm is supported on a block or over the couch side and full range movement is attempted (Fig. 18.7C). Initially this is performed with the elbow flexed to reduce pain on the affected muscle (ECRL), and as pain allows the elbow is extended. Powerband extension is performed with the athlete sitting. One end of the band is placed beneath the foot and the other end gripped. The forearm is supported along the athlete’s thigh (Fig. 18.7D). Initially, eccentric contractions are likely to be less painful than concentric, and the use of ice massage to produce a temporary anaesthesia before exercise is applied (cryokinetics) is often used.
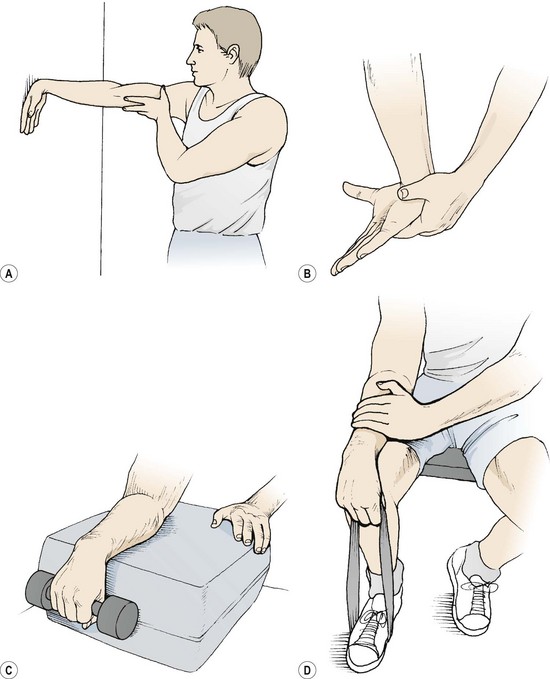
Figure 18.7 Exercise therapy for tennis elbow. (A) Forearm extensor stretch against wall. (B) Combined flexion−pronation of wrist. (C) Resisted forearm extension (dumb-bell). (D) Resisted extension (band).
One word of caution: negative transfer effects have been described by Nirschl (1988) when using high weight, low repetition training following tennis elbow. To avoid this Nirschl (1988) recommended the use of high speed skill training as part of the total rehabilitation programme.
Use of an 8-week programme of stretching and strengthening involving a progression of slow wrist and forearm stretching, muscle conditioning and occupational exercises (Pienimäki at al., 1996) has been shown to result in significantly less pain both at rest and under strain and an improved subjective ability to work when compared to a group using ultrasound alone. Comparing supervised exercise, Cyriax treatment (manual therapy and friction massage) and light therapy (Bioptron) given three times per week over a 4-week period, Stasinopoulos and Stasinopoulos (2006) found that the supervised exercise programme produced the largest effect in terms of pain reduction and improvement of function.
Manual therapy
Manual therapy, including local massage to reduce swelling and produce hyperaemia, and transverse frictions to form a mobile scar are both of use. It is important to locate the exact site of injury for transverse frictions to be effective. The forearm should be pronated and supinated while the area is palpated to find the exact site of the CEO. The lateral epicondyle should be identified as should the supracondylar ridge, and each considered as a possible source of pain. The teno-osseous junction is best frictioned with the forearm in mid-position to let the CEO relax slightly and allow the palpating finger to get right onto the bony surface. The tendon itself is treated on stretch with the elbow and wrist flexed, and forearm pronated (Fig. 18.8A).
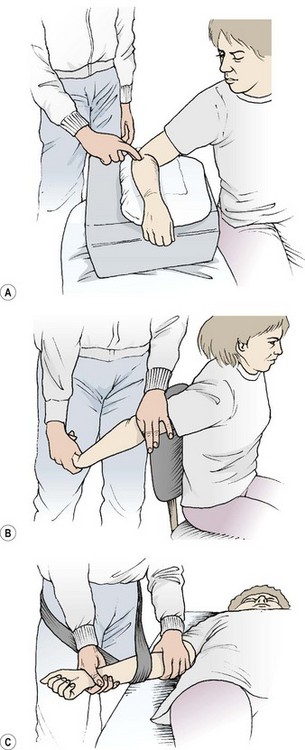
Figure 18.8 Manual therapy for tennis elbow. (A) Deep transverse friction to the common extensor origin. (B) Mills manipulation. (C) Mobilization with movement using belt.
Mills manipulation (Mills, 1928), although originally designed to stress the annular ligament, can be performed to stretch the CEO. The patient’s arm is held in extension at the shoulder, with the elbow comfortably flexed and wrist and forearm fully flexed and pronated (Fig. 18.8B). A high velocity low amplitude thrust is applied to the elbow to fully extend it. Cyriax and Cyriax (1983) claimed this procedure would pull apart the tissue surfaces joined by a painful scar, the fresh tear being replaced by new fibrous tissue under no tension.
Mobilization with movement has been shown to be an effective treatment for this condition (Vicenzino and Wright, 1995). In this technique, a sustained mobilization is applied to a joint, normally at 90° to the plane of movement, to correct joint tracking (Mulligan, 1989). The mobilization is applied at the same time as the patient performs a painful action with the affected joint. In the case of tennis elbow, this action is normally extension of the wrist or fingers (especially the 3rd finger). This technique has been shown to be effective in the treatment of tennis elbow. In a study of 25 subjects Abbott, Patla and Jensen (2001) used a single mobilization with movement (MWM) treatment and found less pain with active motion, greater pain-free grip strength and improved maximum grip in 92% of subjects.
With the patient in a supine position, the therapist wraps a belt around his or her own hips and the athlete’s forearm. The proximal edge of the belt is level with the elbow joint. The humerus and forearm are stabilized by the therapist’s hands. The mobilization (lateral glide of the ulna) is carried out by the therapist gently leaning back (Fig. 18.8A). The aim is to reduce the pain of the finger extension action, initially while the mobilization is applied and eventually during free movement.
Keypoint
Research supports the use of mobilization with movement (MWM) in the treatment of tennis elbow.
Where general elbow stiffness is present as a result of previous inflammation, joint mobilization may be required. Overpressure to either flexion or extension may be combined with adduction and abduction to regain accessory movement. Mobilization of the radial head may also be useful in cases of tennis elbow, and end-range pronation and supination with overpressure may be performed. Direct palpation may be given to the radial head using the therapist’s thumbs. For a PA (posteroanterior) glide, the patient’s elbow is flexed and the bony contour of the radial head is easily palpable. AP (anteroposterior) glides are performed with the patient’s arm extended, and the radial head is palpated through the anterior soft tissues.
Treatment note 18.1 Trigger points and acupuncture points in the treatment of tennis elbow
Both classical acupuncture points and trigger points (TrPs) are extremely useful in the treatment of tennis elbow, and have been shown to be superior to sham points (Molsberger and Hille, 1994; Fink et al., 2002). TrPs in the extensor carpi radialis longus and brevis may be palpated with the elbow flexed and hand unsupported. Begin over the common extensor origin and palpate distally. Central points are located on the ulnar side of the brachioradialis muscle 4–5 cm distal to the elbow crease (at the approximate point of the classical points LI-10, LI-9 and LI-8) while attachment TrPs are located at the common extensor origin. The TrP may be pressed against the radius and flicked transversely to produce a twitch response, causing the patient’s wrist to extend and radially deviate.
The TrP may be treated with either dry needling or deep massage. For massage, the therapist’s thumbs are used beginning over the patient’s supracondylar ridge and epicondyle, extending into the muscle belly. The whole of the area may be treated using a muscle stripping technique pressing in a line from the epicondyle to the thumb. Ischaemic compression may be used over a single active point using a plunger and the patient may be taught self-palpation (Fig. 18.9).
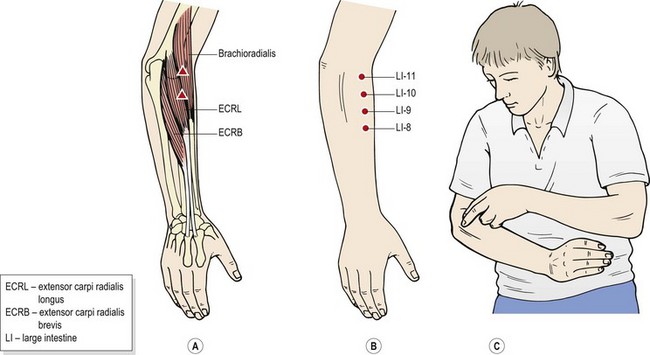
Figure 18.9 Tennis elbow treatment. (A) Trigger points. (B) Classical acupuncture points. (C) Self-treatment.
Dry needling uses either an intramuscular technique to a depth of 0.5–1.5 cm depending on muscle bulk, or needling close to the epicondyle with the intention of striking the bone using a periosteal technique. Here, the aim is to stimulate the richly innervated periosteum to give pain relief (Mann, 1992).
Biomechanics
The extensor carpi radialis brevis is under maximum tension when it contracts in a position of forearm pronation, wrist flexion and ulna deviation (Briggs and Elliott, 1985). This is a typical position for a backhand shot in racquet sports, and elements of this anatomical alignment are seen in many repetitive actions in sport. Repeated practice will cause hypertrophy of this muscle and often a resultant loss of flexibility. In addition, an imbalance frequently exists between the forearm flexors and extensors. Normally, the wrist extensors should be at least 50% of the flexors, but in many recreational sports an individual may have considerably weaker wrist extensors in proportion to flexors. The combination of weaker and less flexible wrist extensors placed in a demanding situation of the backhand stroke (or similar occupational action) exceeds the adaptability of the tissues. One action an athlete may take as part of a preventive programme for this condition, therefore, is to maintain the flexibility of the wrist musculature, and build up the strength of the wrist extensors to as much as 75% of the flexor strength (Reid, 1992).
Ergonomics plays an important part in the management of this condition. Enlarging the grip of any object being held, be it a racquet or a spanner, is important in most cases. The correct grip size can be calculated by measuring from the tip of the ring finger to the bottom lateral crease of the palm, directly below (Fig. 18.10). The figure obtained represents the circumference of the racquet handle. Placing a thick piece of sponge around a handle is also useful to enlarge the grip and reduce shock travelling from the handle to the hand. In some cases a grip which is too large may also be a problem, so to assess if grip size is a relevant feature, ask the patient to grip a thin object (a pencil) and a large one (a bottle) and find which gives less pain. In general terms, when prolonged grip is applied, the therapist should be able to place one finger between the tips of the athlete’s fingers and thumb.

Figure 18.10 Hand measurement to determine proper grip handle size. The distance from the proximal palmar crease to the tip of the middle finger determines the proper size.
From Nirschl (1988), with permission.
In tennis, higher impact and torsion forces are produced by a wet, heavy ball or a racquet which is too tightly strung. The closer the ball is to the centre of percussion (the mathematical point on the racquet face where no torsion will occur on impact), the less strain on the elbow tissues.
Keypoint
Prevention of tennis elbow requires increased forearm extensor strength and flexibility. In addition, the circumference of the object being gripped should be increased, so that one finger width can be placed between the athlete’s fingers and thumb.
Oversize racquets, by increasing the likelihood of keeping the ball away from the frame, may reduce torsion and in turn overload stress on the elbow. In addition, leverage forces may be reduced in these racquets by moving the centre of percussion closer to the racquet handle (Nirschl, 1988). A heavier racquet will have more momentum, and will place a greater strain on the forearm. Nirschl (1988) recommended a mid-sized (90–100 square inch) graphite composite light-weight racquet to give the best protection, and Bullard (1982) recommended fibreglass or graphite as the best materials to absorb vibration.
Osteochondrosis
The most common site for osteochondrosis in the elbow is the anterolateral surface of the capitulum (Panner’s disease). The aetiology is generally either traumatic or vascular, although some familial tendency may be present. The condition is most commonly related to throwing or racquet sports. In throwing, the angular velocity experienced at the joint may exceed 300°/s (Jobe and Nuber, 1986). This, coupled with a valgus force and an extension stress, causes the radial head to impinge against the capitulum. Ultimately, a breakdown can occur in the capitulum surface and the radial head may hypertrophy.
The vascular supply to the area can be disrupted by this repeated trauma. Up until the age of 5 years the capitulum has a good blood supply, but later the nucleus of the capitulum receives only one or two vessels. These pass into the area posteriorly through soft, compressible cartilage—a possible site of damage. Early stages of osteochondrosis (see Chapter 1) show as a radiolucent (more transparent) area with an open capitellar growth plate. Later stages show as a closed growth plate. Normally x-rays are taken with the elbow flexed to 45° to visualize the capitulum changes.
The typical patient is an athlete in early adolescence (usually male) who shows limitation of elbow extension with local swelling. Onset is often insidious and the patient may have been experiencing difficulties over a protracted period. If the osteochondrotic fragment is free within the joint, locking or catching may be experienced with certain movements. Radiographs may show blunting of the capitulum with enlargement of the radial head. Often an island of bone is seen surrounded by an area of rarefaction. Premature epiphyseal closure may also be noted to either the humerus or the proximal radius.
In the initial stages of the condition with a young athlete, rest is all that is required, splinting being indicated if the patient fails to heed this advice. If stress has been allowed to continue and bony degeneration has occurred, drilling or grafting of the attached fragment may be required. In late stage conditions loose bodies may need to be removed, and unfortunately the prognosis is sometimes poor.
Keypoint
With Panner’s disease (osteochondritis of the elbow): (i) the patient is typically a male, involved in a throwing sport, and in early adolescence, (ii) pain comes on gradually, (iii) extension is reduced, and (iv) there may be local swelling.
Conservative management consists of avoidance of heavy usage of the elbow, usually for a 6-month period. In a study of 176 competitive baseball players, Matsuura et al. (2008) showed healing in 90.5% of stage (I) patients and 52.9% of stage (II) patients with the mean healing period being 14.9 and 12.3 months, respectively. Mihara et al. (2009) showed spontaneous healing of the capitellar growth plate in 25 out of 30 early stage lesions, but only 1 out of 9 advanced stage lesions. These authors recommended surgery to achieve healing in advanced cases.
Medial pain
Lesions to the medial side of the joint occur most often with throwing actions. Although different sports demand different throwing techniques, similarities still exist. Initially, the shoulder is abducted and taken into extreme external rotation and extension, while the elbow remains flexed (cocking phase). Then, the shoulder and trunk rapidly move forward, leaving the arm behind (acceleration phase). This action imposes a valgus stress on the joint and stretches the ulnar collateral ligament in particular. The shoulder flexors and internal rotators contract powerfully, flinging the arm forward resulting in stress to the olecranon as the arm extends rapidly to full range (deceleration phase and follow-through).
The throwing action imposes a number of stresses on the elbow (Fig. 18.11). The lateral joint line is subjected to compression forces, in the olecranon fossa there are shearing forces, while the medial joint line experiences tensile forces (Jobe and Nuber, 1986). These forces, if repeated, can give rise to specific injuries and general degeneration reflecting the stress imposed on the elbow structures (Table 18.3).
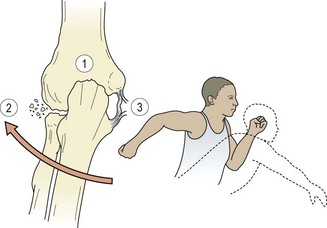
Figure 18.11 Forces on the elbow during throwing. 1. Hypertension − olecranon shear. 2. Valgus − compresses laterally, radial head damage. 3. Valgus − distracts medially, collateral ligament damage.
Table 18.3 Throwing injuries to the elbow
| Medial tension | Lateral compression | Posterior shear |
|---|---|---|
| Muscular overuse | Osteochondrosis | Muscular strain |
| Ligamentous injury | Fractured capitulum | Impingement |
| Capsular injury | Lateral epicondylitis | Olecranon fracture |
| Ulnar traction spur | Bony hypertrophy | |
| Medial epicondylitis | Loose bodies |
Medial epicondylitis
This is a lesion of the common flexor origin (CFO) on the medial epicondyle, and is commonly called golfer’s elbow. The primary site is the origin of pronator teres and flexor carpi radialis on the medial epicondyle hence the term flexor/pronator tendinopathy. The flexor carpi ulnaris may occasionally be affected. Golfer’s elbow is less common than tennis elbow, occurring at a ratio of about 1 : 15 (Coorad and Hooper, 1973). The injury can be complicated by ulnar nerve involvement, the nerve being compressed at a point distal to the medial epicondyle.
Keypoint
Golfer’s elbow (medial epicondylitis) mainly affects the pronator teres and flexor carpi radialis muscle. Flexor carpi ulnaris is affected less often, and ulnar nerve involvement may also occur.
Sensory symptoms are often present and Tinel’s sign (tapping the ulnar nerve at the elbow to produce pain or tingling in the ulnar portion of the hand) is positive (Nirschl, 1986). Chronic conditions may see calcium deposits developing within the tendon itself (Leach and Miller, 1987).
Pain is felt more locally than with tennis elbow, and is increased on resisted wrist flexion and sometimes forearm pronation. The condition may be differentiated from chronic medial ligament sprain by applying the valgus stress test which should not give pain or laxity in epicondylitis.
The treatment is for the most part like that for tennis elbow, including soft tissue manipulation and biomechanical changes. Transverse frictions are now performed with the elbow and wrist in extension, with the forearm supinated. Counterforce bracing is again used, but this time the brace extends up to the medial epicondyle to avoid interfering with elbow flexion.
Medial collateral ligament (thrower’s elbow)
Repetitive stresses to this ligament are common in throwing athletes, particularly in events such as the javelin. Pain is generally quite localized over the medial joint line, and exacerbated by applying an elbow abduction stress test, forcing a valgus strain on the joint in 20° flexion. With severe injuries, gapping of the joint may be apparent.
Keypoint
Pain in the MCL of the elbow is reproduced using the passive elbow abduction test. For this a valgus (inner opening) strain is placed on the joint in slight flexion.
Initial treatment is to remove the causal stress and rest from throwing. Operative repair of a ruptured medial collateral ligament is often recommended for athletes and those involved in heavy manual labour. The theory is that instability may produce problems later in life. However, Kuroda and Sakamaki (1986) reported surgical repair in 10 patients and conservative management in three others. Before surgery, valgus instability averaged 14.9°. Those treated surgically later showed average laxity of 5.1° while those managed conservatively had average values of 8.0°. With figures for instability which are so similar, it may be questionable whether surgery offers substantial advantage over conservative management in many cases.
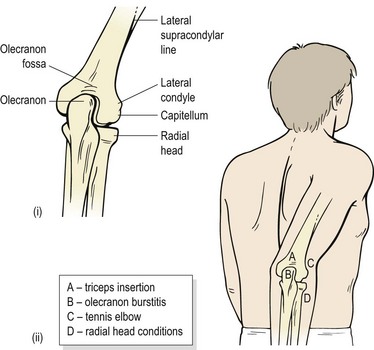
Posterior elbow pain
Pain at the back of the elbow is common in sports which rapidly extend or hyperextend the joint. These include the throwing sports, punching in martial arts and pressing actions in weight training. Structures involved, either individually or in combination, include the insertion of the triceps, the olecranon bursa and the olecranon itself (Fig. 18.12).
Olecranon bursitis
The olecranon bursa is placed at the bony point of the elbow, over the olecranon process subcutaneously. A deeper bursa is sometimes present between the capsule and triceps. When the elbow is extended, the margins of the olecranon bursa cause a circular ridge of skin about 1.5–2 cm in diameter to be pulled up on the posterior aspect of the elbow.
The bursa can become inflamed by leaning on the elbow for a prolonged period (student’s elbow), or from a direct fall onto the point of the elbow. This latter case may induce haemorrhage into the bursal sac itself. Examination of the joint reveals no abnormality, but pain and thickening occur to direct palpation over the bursa. Treatment is to remove the cause, pad the point of the elbow and aspirate the fluid.
Where the bursa becomes infected (septic bursitis), immediate drainage (aspiration) and/or surgical washout is required followed by immobilization and oral antibiotics (Stell, 1996). Signs of bursal infection include local erythema and warmth, marked swelling and sudden symptom exacerbation. General fever and cellulitis of the surrounding skin may also be present.
Triceps insertion
Triceps tendinitis may occur in throwing athletes (especially javelin) and weight-lifters. Inflammation and microtrauma are usually limited to the olecranon insertion of the muscle. Damage is usually to the musculotendinous or teno-osseous junctions, and cessation of activity and correction of technique, coupled with modalities to reduce local inflammation and pain, are usually curative. Unusually, the medial head of the triceps may sublux over the medial epicondyle during flexion causing a snapping sensation (’snapping elbow syndrome’; Dreyfuss and Kessler, 1978). This must be distinguished from subluxation of the ulnar nerve from its groove, which is common in 16% of the population (Reid, 1992). Subluxation is normally due to laxity of the ulnar collateral ligament and/or a shallow ulnar groove.
Keypoint
Laxity of the ulnar collateral ligament and a shallow ulnar groove can allow the ulnar nerve to sublux and causes neurological symptoms into the 4th and 5th fingers.
Rupture of the triceps tendon, either partial or complete, is unusual, and the muscle belly itself is even less frequently injured. When rupture does occur, there is usually a palpable defect in the musculotendinous junction of the muscle, with scarring in the chronic injury. Active extension is lost, and a large haematoma, later developing into bruising, is noted locally. The majority of patients are in their 30s or 40s, and the injury almost always occurs either following a fall onto the outstretched hand or a ‘chopping’ action. In either case, the stress is one of deceleration imposed on an already contracting muscle.
A small fragment of the olecranon may be avulsed and show up on a lateral radiograph of the elbow, and occasionally radial head fractures are associated with the condition. Conservative management is reserved for partial ruptures (Bach, Warren and Wickiewicz, 1987) distinguished by an ability to partially extend the arm against gravity. Surgical management for avulsion injuries involves drilling the olecranon and suturing the muscle. Postoperatively, the patient is immobilized for 3–4 weeks in a cast or splint at 30–45° elbow flexion.
Posterior impingement
Posterior impingement of the olecranon into its fossa is common in sports where the elbow is ‘snapped back’. This is especially the case with rapid weight (circuit) training, and martial arts, where athletes reach upwards as if ‘punching the air’ while performing forms. Throwing events will tend to cause impingement of the medial aspect of the olecranon on the follow-through movement.
Examination usually reveals point tenderness over the posterior or posteromedial aspect of the olecranon (see Fig. 18.12). This is made worse by forced extension, and extension/abduction. Chronic injuries may show osteophyte formation posteromedially. Cortical thickening is also usually seen on radiograph, but this is thought to represent adaptation of the bone to repetitive stress (Garrick and Webb, 1990).
Treatment is initially to limit extension and valgus stress by strapping, or if this fails, to rest the elbow completely. The elbow flexors are strengthened (especially eccentrically) to enhance their action as decelerators of elbow extension, and to shorten them and therefore limit hyperextension.
Stress fracture of the olecranon is a rare but often overlooked outcome of posterior impingement, and has been described in javelin throwers (Hulkko, Orava and Nikula, 1968) and baseball pitchers (Nuber and Diment, 1992). Pain usually follows the pattern typical of a stress fracture, eventually limiting performance. Many lesions will respond to rest and splinting, but some require surgery including excision of the olecranon tip and inlaid bone block graft (Torg, 1993). Traumatic fracture of the olecranon may occur through a fall onto the point of the elbow. Where the fragment is undisplaced, immobilization in a posterior splint is normally the treatment of choice. Displaced olecranon fractures require open reduction and internal fixation.
Muscular injury
The biceps, triceps and brachialis may all be injured in sport. The most common injury for the biceps is to its long head (see Chapter 17), but its lower insertion may also be injured occasionally. Pain is reproduced to resisted elbow flexion and supination, and passive pronation, resisted shoulder flexion may also be added. If resisted flexion is painful but supination is not, the brachialis is indicated. The site of pain is the centre of the front of the arm, often radiating as far as the wrist in severe cases.
The usual site for injury to the triceps is the musculotendinous junction, but the belly may be injured. Pain on resisted elbow (and shoulder) extension is the clinical sign, but when this test gives pain in the upper arm felt nearer to the shoulder, referred pain from impingement of a shoulder structure should be considered. In this case the triceps contraction pulls the humerus up into the acromion approximating the joint.
Myositis ossificans traumatica
Injury to the brachialis should always be treated with caution, because this muscle shares with the quadriceps the potential for myositis development.
The history is usually that of a direct blow, for example from a knee or head in rugby or a foot in martial arts. Most commonly, a second blow has been experienced to the same area. The typical findings are tenderness persisting for 2–3 weeks after injury, and difficulty in regaining full range motion. On examination, a fibrous mass is often palpable within the muscle over the anterior aspect of the arm.
Keypoint
The possibility of myositis in the brachialis muscle exists when: (i) there is a history of a number of direct blows to the same area; (ii) tenderness has persisted for 2–3 weeks after injury; (iii) full range of motion cannot be regained; (iv) there is a palpable mass over the anterior aspect of the arm when compared to the uninjured side.
Where these findings are present, x-ray is required. Often heterotrophic bone formation is seen, showing a diffuse fluffy callus. As the callus matures it will shrink and its margins become better defined. Bone scan will reveal whether the condition is still active.
Management aims initially to minimize the damage. Local swelling is reduced where possible, and activity limited. Mobility exercise is begun with caution when radiographic evidence shows that the condition is no longer active. Resisted work is the last exercise to be started, and when sport is resumed, the area is protected with padding. Rehabilitation of this type emphasizing joint mobilization and eccentric strengthening especially has been shown to give full range of motion at the elbow after 9 weeks. Follow-up (9 months) showed nearly complete bone maturation and a full return to competitive sport (De Carlo et al., 1992).
Elbow dislocations
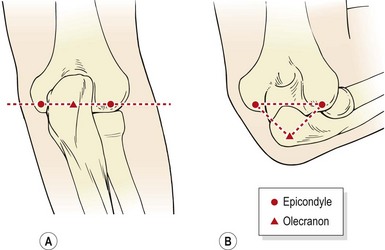
Posterior or posterolateral dislocation of the elbow is seen following a fall onto the outstretched arm, sometimes associated with a fracture to the olecranon or coronoid process. This is common when falling from a horse or bicycle, and from gymnastic accidents. Roller-skating and skateboarding are also prime causes, as the athlete usually falls backwards onto an abducted straight arm. There is often a snap or crack at the time of injury with immediate swelling. On examination, the arm is held flexed, and a gross deformity is apparent on the posterior aspect of the elbow. The normal triangular alignment of the olecranon and two epicondyles is lost (Fig. 18.13). Radiographic examination is required to assess bony damage, and on no account should reduction on the field be attempted because of the risk of neural complications. Reduction is achieved by downward pressure on the forearm initially to disengage the coronoid from the olecranon fossa and then the forearm is brought forwards. As with the shoulder, reduction, unless immediate, will usually require analgesia.
Operative intervention has often been recommended where reduction is unstable due to ligament avulsion. However, Josefsson et al. (1987) compared the results of patients treated by primary surgical repair to those treated by closed reduction. Although the surgery group included those with complete collateral ligament ruptures or avulsions (all patients) and muscle origin tears from the humeral epicondyles (half the patients), the results from the two groups were the same. Surgery is therefore not usually recommended in cases where there is no associated fracture.
If the arm is immobilized for more than a week, the resting position should be in as much extension as possible (Garrick and Webb, 1990). This is important because reduced flexion is far easier to regain during rehabilitation than is extension. With an uncomplicated injury, gentle isometric exercise is begun as pain and swelling settles. After 2–3 days, active mobility exercise is started with caution in the pain-free range, the athlete remaining in a sling between exercise periods for protection.
Early mobilization of this injury is essential. Mehlhoff et al. (1988) described 52 adults with elbow dislocation. Those immobilized for less than 18 days showed significantly better results than those inactive for longer periods, and patients immobilized for more than 4 weeks all showed only fair or poor results. None of the patients redislocated.
Following this injury, there is normally a slight loss of extension. If the elbow has previously hyperextended, this is not usually a problem. However, where the arm remains slightly flexed, weight-bearing activities, such as handstands and cartwheels, will tend to push the arm into flexion. To stabilize the arm and obtain some degree of functional locking, the triceps must be built up extensively.
Radial head
Compression fracture of the radial head may occur with a vertical fall onto the outstretched arm, but more commonly the injury which affects the radial head is a dislocation. This is usually seen in children, where the radial head is pulled through the annular ligament, limiting extension. The peak incidence of injury occurs between the ages of 2 and 3 years, this being the age when the annular ligament is thinner and more easily disrupted. The injury is twice as common in girls as in boys (Quan and Marcuse, 1985), and the left elbow is affected more often than the right (Corrigan and Maitland, 1994). The mechanism of injury is a sudden traction applied to an extended and pronated arm as an adult lifts the child while gripping the child’s hand.
Reduction, if carried out before muscle spasm sets in, may be performed by holding the elbow flexed to 90° and lightly rotating the forearm. The therapist holds the child’s elbow in his or her cupped hand and places the thumb over the radial head. The other hand holds the child’s hand, and the manipulation is produced with a high velocity supination of the patient’s forearm while maintaining thumb pressure over the radial head. At the same time, the radius and humerus are gently pulled together and the radial head is felt to click back beneath the annular ligament on full supination. Often this condition reduces spontaneously.
Nerve involvement
Ulnar nerve
The ulnar nerve may be involved with medial collateral ligament injuries of the elbow, as outlined above. Friction against this nerve or its sheath may give rise to symptoms, described by Wadsworth and Williams (1973) as the ‘cubital tunnel syndrome’. Since the sensory fibres of the ulnar nerve are more superficial than the motor fibres, sensory symptoms are more prevalent, with paraesthesia occurring in the fourth and fifth fingers.
The nerve passes through the groove behind the medial epicondyle and is covered by a fibrous sheath, forming the cubital tunnel (Fig. 18.14A). The roof of the tunnel is the aponeurosis of the two heads of flexor carpi ulnaris. This is taut at 90° flexion, constricting the tunnel, and slack on extension. The floor of the cubital tunnel is formed from the tip of the trochlea and the medial collateral ligament. The ligament bulges with elbow flexion, an additional factor leading to nerve compression, especially with prolonged periods of end-range flexion.
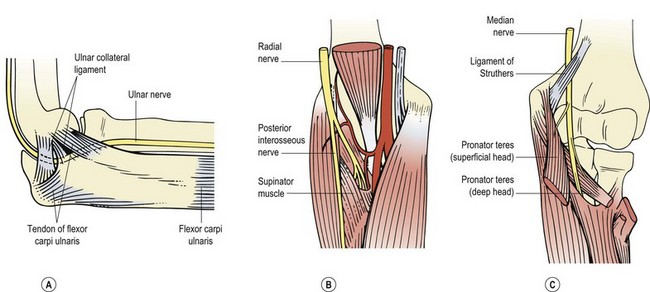
Figure 18.14 Nerve compression in the elbow. (A) Ulnar nerve, cubital tunnel. (B) Radial nerve, arcade of Frohse. (C) Median nerve, pronator teres.
Definition
Cubital tunnel syndrome occurs when there is friction of the ulnar nerve or its sheath. Altered sensation and tingling (paraesthesia) occurs in the 4th and 5th fingers.
Dislocation of the nerve from the ulnar groove can also occur following fracture and is accompanied by a persistent tingling sensation with certain elbow actions. If motor symptoms are present, wasting may be seen in the hypothenar eminence and the first dorsal interosseous space. Tinel’s sign and the elbow flexion test may be positive. This latter test involves maximal flexion of the elbow for 5 minutes to compress the cubital tunnel. Symptoms produced, including pain, altered sensation and numbness, constitute a positive test.
Management depends very much on the severity of the symptoms. Often rest and elbow padding to avoid irritation in contact sports may be all that is required for frictional neuritis. Corticosteroid injection along the cubital tunnel may be useful (Corrigan and Maitland, 1994). Surgery, if performed early, can be successful. Nerve transposition combined with excision of a portion of the medial epicondyle and division of the tendinous origin of the flexor carpi ulnaris has been described (Hirsch and Thanki, 1985).
Radial nerve
The radial nerve can be injured in the elbow region. The nerve travels in front of the lateral condyle of the humerus to divide into deep (posterior interosseous) and superficial branches. The superficial branch may be exposed to direct trauma, sometimes being damaged as a complication of fractures to the radial head or neck.
Radial tunnel syndrome (Roles and Maudsley, 1972) occurs when the deep branch of the radial nerve is compressed as it passes under the origin of the extensor carpi radialis brevis and along the fibrous edge of the supinator muscle (arcade of Frohse, Fig. 18.14B). Pain is produced when the arm is fully pronated with the wrist flexed.
Differential diagnosis of radial tunnel syndrome is made by eliciting pain by palpation of the radial head, and pain on resisted supination. True tennis elbow will give pain over the lateral epicondyle (not the radial head), with pain on resisted wrist extension but not supination alone (Lee, 1986). The condition is seen following repeated contraction of the wrist extensors and forearm supinators against resistance, as in racquet sports in a novice sportsperson (Cailliet, 1983).
Treatment by both local injection and surgery has been described (Moss and Switzer, 1983).
Median nerve
In general usage, the medial nerve is most commonly injured by laceration at the wrist, giving an inability to abduct the thumb, a classic ‘pointing (index) finger’ and sensory loss over the radial 312 digits. In sport, however, medial nerve compression may occur, although it is unusual. At the elbow, the median nerve passes beneath the ligament of Struthers. This is an anomaly found in about 1% of the general population running from a bony spur on the shaft of the humerus to the medial epicondyle (Fig. 18.14C). Symptoms are generally sensory, with paraesthesia in the forearm and hand. If left, motor symptoms affecting the thumb and forefinger may also occur. Lower down the forearm the medial nerve passes between the two heads of pronator teres, and it may be compressed here. Resisted pronation may be weak, more noticeably if the movement is maintained for 30–60 seconds, and sensory symptoms may be seen as before. The condition usually responds to an alteration in training, but surgical release may be required.
Testing the elbow following injury
A sportsperson must be able to perform actions relevant to his or her sport and to his or her competitive role within that sport (Wright, 1981). Maximal functional work of the biceps may be performed by the subject chinning a bar, and for the triceps dipping between two chairs or performing a push-up with the feet on a chair; both of these actions should be slow and controlled until confidence is built. Faster, more demanding actions include press-ups with a clap in between each repetition, and walking hand to hand while hanging at arm’s length from a horizontal ladder.
Racquet sportspeople should mimic their stroke action with a weighted racquet or heavy club, and can assess their resilience to jarring strains by hitting a club or bat against a firm surface (a medicine ball is ideal). The elbow must be able to take repeated traction and approximation strains, and be pain-free when the arm is locked while holding a weight at arm’s length.
Abbott J.H., Patla C., Jensen J. The initial effects of an elbow mobilization with movement technique on grip strength in subjects with lateral epicondylalgia. Manual Therapy. 2001;6(3):163-169.
Bach B.R., Warren R.F., Wickiewicz T.L. Triceps rupture: a case report and literature review. American Journal of Sports Medicine. 1987;15(3):285-289.
Bisset L.M., Russell T., Bradley S., et al. Bilateral sensorimotor abnormalities in unilateral lateral epicondylalgia. Archives of Physical Medicine and Rehabilitation. 2006;87(4):490-495.
Briggs C.A., Elliott B.G. Lateral epicondylitis: a review of structures associated with tennis elbow. Anatomia Clinica. 1985;7:149.
Bullard J.A.A. Tennis elbow. Canadian Family Physician. 1982;28:961-963.
Burton A.K. Grip strength and forearm straps in tennis elbow. British Journal of Sports Medicine. 1985;19:37-38.
Cailliet R. Soft Tissue Pain and Disability. Philadelphia: F.A. Davis; 1983.
Coombes B.K., Bissel L., Vicenzino B. A new integrative model of lateral epicondylalgia. British Journal of Sports Medicine. 2009;43:252-258.
Coorad R.W., Hooper W.R. Tennis elbow: course, natural history, conservative and surgical management. Journal of Bone and Joint Surgery. 1973;55A:1177.
Corrigan B., Maitland G.D. Musculoskeletal and Sports Injuries. Oxford: Butterworth-Heinemann; 1994.
Cyriax J. Pathology and treatment of tennis elbow. Journal of Bone and Joint Surgery. 1936;18A:921.
Cyriax J.H., Cyriax P.J. Illustrated Manual of Orthopaedic Medicine. London: Butterworth; 1983.
De Carlo M.S., Misamore G.W., Carrell K.R., Sell K.E. Rehabilitation of myositis ossificans in the brachialis muscle. Journal of Athletic Training. 1992;27(1):76-79.
Dreyfuss U., Kessler I. Snapping elbow due to dislocation of the medial head of triceps. Journal of Bone and Joint Surgery. 1978;60B:56.
Fink M., Wolkenstein E., Karst M., Gehrke A. Acupuncture in chronic epicondylitis. Rheumatology. 2002;41(2):205-209.
Fredberg U., Stengaard-Pedersen K. Chronic tendinopathy, pain mechanisms, and etiology with a special focus on inflammation. Scandinavian Journal of Medicine and Science in Sports. 2008;18(1):3-15.
Garrick J.G., Webb D.R. Sports Injuries: Diagnosis and Management. Philadelphia: W.B. Saunders; 1990.
Griffen J.E., Touchstone J.C. Ultrasonic movement of cortisol into pig tissues. (I). Movement into skeletal muscle. American Journal of Physical Medicine. 1963;43:77.
Groppel J.L., Nirschl R.P. A mechanical and electromyographical analysis of the effects of various joint counterforce braces on the tennis player. American Journal of Sports Medicine. 1986;14:195-200.
Halle J.S., Franklin R.J., Karalfa B.L. Comparison of four treatment approaches for lateral epicondylitis of the elbow. Journal of Orthopaedic and Sports Physical Therapy. 1986;8(2):62-69.
Hirsch L.F., Thanki A. Ulnar nerve entrapment at the elbow: tailoring the treatment to the cause. Postgraduate Medicine. 1985;77:211-215.
Hulkko A., Orava S., Nikula P. Stress fractures of the olecranon in javelin throwers. International Journal of Sports Medicine. 1968;7:210.
Jobe F.W., Nuber G. Throwing injuries of the elbow. Sports Medicine. 1986;5(4):621-635.
Josefsson P.O., Gentz C., Johnell O., Wendeberg B. Surgical versus non-surgical treatment of ligamentous injuries following dislocation of the elbow joint: a prospective randomized study. Journal of Bone and Joint Surgery. 1987;69A:605-608.
Kleinkort J.B., Wood F. Phonophoresis with 1% versus 10% hydrocortisone. Physical Therapy. 1975;55:1320.
Kuroda S., Sakamaki K. Ulnar collateral ligament tears of the elbow joint. Clinical Orthopaedics and Related Research. 1986;208:266-271.
Leach R.E., Miller J.K. Lateral and medial epicondylitis of the elbow. Clinics in Sports Medicine. 1987;6(2):259-272.
Lee D.G. Tennis elbow: a manual therapist’s perspective. Journal of Orthopaedic and Sports Physical Therapy. 1986;12(2):81-87.
Mann F. Reinventing Acupuncture. Oxford: Butterworth Heinemann; 1992.
Matsuura T., Kashiwaguchi S., Iwase T., et al. Conservative treatment for osteochondrosis of the humeral capitellum. American Journal of Sports Medicine. 2008;36(5):868-872.
Mehlhoff T.L., Noble P.C., Bennett J.B., Tullos H.S. Simple dislocation of the elbow in the adult: results after closed treatment. Journal of Bone and Joint Surgery. 1988;70A:244-249.
Mihara K., Tsutsui H., Nishinaka N., Yamaguchi K. Nonoperative treatment for osteochondritis dissecans of the capitellum. American Journal of Sports Medicine. 2009;37(2):298-304. Feb
Mills G.P. Treatment of tennis elbow. British Medical Journal. 1(12), 1928.
Molsberger A., Hille E. The analgesic effect of acupuncture in chronic tennis elbow pain. British Journal of Rheumatology. 1994;33(12):1162-1165.
Morrey B.F., Kai-Nan A. Articular and ligamentous contributions to the stability of the elbow joint. American Journal of Sports Medicine. 1983;11:315-318.
Moss S.H., Switzer H.E. Radial tunnel syndrome: a spectrum of clinical presentations. Journal of Hand Surgery. 1983;8:414-420.
Mulligan B.R. Manual Therapy. Wellington, New Zealand: Plane View Services; 1989.
Nirschl R.P. Soft tissue injuries about the elbow. Clinics in Sports Medicine. 1986;5(4):637-652.
Nirschl R.P. Prevention and treatment of elbow and shoulder injuries in the tennis player. Clinics in Sports Medicine. 1988;7(2):289-309.
Nuber G.W., Diment M.T. Olecranon stress fractures in throwers: a report of two cases and a review of the literature. Clinical Orthopaedics and Related Research. 1992;278:58-61.
Palastanga N., Field D., Soames R. Anatomy and Human Movement. Oxford: Heinemann Medical; 1989.
Paoloni J.A., Appleyard R.C., Nelson J., Murrell G. Topical nitric oxide application in the treatment of chronic extensor tendinosis at the elbow: a randomized double blinded placebo controlled clinical trial. American Journal of Sports Medicine. 2003;31(6):915-920.
Paoloni J.A., Murrell G.A., Burch R.M., Ang R.Y. Randomised, double-blind, placebo-controlled clinical trial of a new topical glyceryl trinitrate patch for chronic lateral epicondylosis. British Journal of Sports Medicine. 2009;43(4):299-302.
Pienimäki T.T., Tarvainen T., Siira P., Vanharanta H. Progressive strengthening and stretching exercises and ultrasound for chronic lateral epicondylitis. Physiotherapy. 1996;82(9):522-530.
Pienimäki T., Tarvainen T., Siira P., et al. Associations between pain, grip strength, and manual tests in the treatment evaluation of chronic tennis elbow. Clinical Journal of Pain. 2002;18(3):164-170.
Quan L., Marcuse E.K. The epidemiology and treatment of radial head subluxation. American Journal of Diseases of Children. 1985;139:1194-1197.
Reid D.C. Sports Injury Assessment and Rehabilitation. Edinburgh: Churchill Livingstone; 1992.
Roles N.C., Maudsley R.H. Radial tunnel syndrome: resistant tennis elbow as a nerve entrapment. Journal of Bone and Joint Surgery. 1972;54B:499-508.
Stasinopoulos D., Stasinopoulos I. Comparison of effects of Cyriax physiotherapy, a supervised exercise programme and polarized polychromatic non-coherent light (Bioptron light) for the treatment of lateral epicondylitis. Clinical Rehabilitation. 2006;20(1):12-23. Jan
Stell I.M. Septic and non-septic olecranon bursitis in the accident and emergency department – an approach to management. Journal of Accident and Emergency Medicine. 1996;13(5):351-353.
Torg J.S. Yearbook of Sports Medicine Comment. St Louis: C.V. Mosby, 1993 p. 72
Vicenzino B., Wright A. Effects of a novel manipulative physiotherapy technique on tennis elbow: a single case study. Manual Therapy. 1995;1:30-35.
Wadsworth C.T., Nielsen D.H., Burns L.T., Krull J.D., Thompson C.G. Effect of the counterforce armband on wrist extension and grip strength and pain in subjects with tennis elbow. Journal of Orthopaedic and Sports Physical Therapy. 1989;11:192-197.
Wadsworth T.G., Williams J.R. Cubital tunnel external compression syndrome. British Medical Journal. 1973;1:662.
Wright D. Fitness testing after injury. In: Reilly T., editor. Sports Fitness and Sports Injuries. London: Faber and Faber, 1981.