Appendix: Nimmo, chiropractic and myofascial pain
Introduction
Raymond Nimmo was a pioneering research clinician and practitioner whose background in chiropractic offered him a sound understanding (at the time) of the way the nervous system operated in relation to musculoskeletal pain. Nimmo’s work with trigger points paralleled that of Janet Travell, with whom he communicated. In this appendix there are three documents:
1. A short extract from a book from 2001 on Nimmo’s work, compiled with two of his chiropractic colleagues and collaborators, Drs Michael Schneider DC and Jeffrey Cohen DC that sets out in summary form his ideas on technique.
2. An article by Jeffrey Cohen and Russell W. Gibbons (1998) that expands on these introductory notes and offers information on Nimmo’s history.
3. An article by Howard Vernon and Michael Schneider (2009) that provides a context in chiropractic for treatment of myofascial pain, including reference to Nimmo.
These articles are published within the context of this text on Modern Neuromuscular Techniques, in order to increase awareness of the multiple strands that have contributed to current knowledge.
Nimmo notes on technique
Michael Schneider DC, Jeffrey Cohen DC
The application of the Receptor-Tonus Method consists of the following:
1. The detection and elimination of noxious points which generate nerve impulses. Such impulses coming from sources other than proper centres are physiologically unlawful. They set up devious routes in the nervous system and may produce trouble anywhere in the body. In the autonomics, they produce vasoconstriction of blood vessels, with consequent ischaemia, hypoxia, pain and cellular degeneration. They apparently invade any system of nerves, including the cranial nerves, or even brain centres.
2. The elimination of hyper- or hypotonia of muscles. Only when this is accomplished is it possible for osseous structures to assume normal relationships. Aberration of the tonus system is the cause of skeletal misalignment and curvature.
3. The normalizing of ligaments and tendons. When under tension from muscle or joint pull, these structures are affected. Being rich in nerve supply, especially sensory and proprioceptors, they become foci of irritation to the nervous system.
All work is specific to, and exclusive to, the nervous system. It does not make any difference where you begin the corrective treatment, however, it would be well to begin in the area of the patient’s chief complaint of pain.
Hold manual pressure for about three to eight seconds. Five seconds is probably best. Nothing is gained by holding a long contact. These points do not leave while pressure is being applied, but later. Treatment starts the process. It is far better to hold a point several times at five seconds at a time, than it is to hold it for thirty or sixty seconds. Prolonged pressure produces a pressure anesthesia which will beguile the operator into thinking he has eliminated the trigger point. When this occurs, the point will more than likely return.
Some say that a rubbing, stroking, circular movement, or a vibrating contact should be used. This is merely complicating the process, and gaining nothing. Those who say this are trying to camouflage this work, and usually call it something else. What is being done here is inhibition. You are trying to inhibit a facilitated process. You are trying to achieve quiescence in these particular points. What is accomplished is a raising of the stimuli threshold so that the point will cease firing impulses into the nervous system.
When normal, muscles palpate as soft, homogenous, relaxed, and are not painful to properly applied pressure. This is true of all palpable muscles. Never treat a point that is not painful, for then the treatment itself may become the irritant. When no longer painful, the job is done. Leave it alone. If you over treat a muscle, all you can do is leave it alone. This rule applies to all trigger points, and all muscles.
Pressure is what clears the muscles of hypermyotonia. Gliding on the longer muscles, after lubrication, so one will not pull hair or skin, which is very painful, is merely distributing the pressure equally over the muscle. The effect on lymph is not important. You are not, so-called, ‘milking’ the muscle. You are merely applying pressure, just as in any other place. Pressure, used correctly, clears out all these conditions, which are trigger points, hypermyotonia, and hypomyotonia. Whenever a hypertonic muscle is released, normal tonus appears in its opposite according to the working of Davis’ Law; likewise, if a stimulus is made in a hypotonic muscle, hypertonus is temporarily released in the antagonist. The so-called ‘weak’ muscle regains its strength instantly. This is an aberration of the tonus function, which has been set into operation by abnormal stimuli, acting in accordance with Davis’ Law.
Raymond L. Nimmo and the evolution of trigger point therapy, 1929–1986
Jeffrey H, Cohen DC,1 Russell W, Gibbons Litt D2
Dr. Raymond L. Nimmo (1904–86) was the definitive chiropractic pioneer in the now widely accepted field of soft tissue and trigger point therapy. This article explores how Nimmo was able to make the radical conceptual leap from moving bones to working with muscles that move the bones. Also discussed are the neurophysiological explanations that Nimmo evolved in the 1950s for the trigger point phenomenon, formulations that are still regarded as highly sophisticated half a century later. Finally, the article describes how Nimmo, with a basic chiropractic education absent of much of the background in the biological and physical sciences of today’s preparation, was able to combine his clinical experiences and intellectual formulation to arrive at a theory that became widely accepted. (J Manipulative Physiol Ther 1998; 21:167–72).
Introduction
On November 20, 1980, William Bachop, Ph.D., chairman of the Department of Anatomy at National College of Chiropractic, wrote to Raymond L. Nimmo, D.C., of Granbury, Texas and posed the following question, a question suggesting the seemingly ever-present conflict between laboratory research and clinical practice outcomes in the ‘technique’ wars of chiropractic for most of this century:
The Nimmo technique is used in all parts of the chiropractic world, and I asked why should a chiropractor in private practice in a small town in Texas make a discovery that had seemingly eluded the chiropractors on the faculties of the colleges…with the time, funding and facilities to do research (Bachop 1980)?
Nimmo’s reply explored many of the issues involving research techniques within the profession in its formative years, but in some respects he did not address another central question that could be raised about Nimmo and the practitioners who have been credited with ‘discoveries’ of other techniques. That question should have some significance and interest in this postcentennial period of chiropractic, when the profession can correctly claim to having elevated its preclinical, professional and clinical studies to standards that have achieved parity in the health care community.
Nimmo was one of the many chiropractors trained in the second and third decades of this century who had virtually no prechiropractic academic training in the basic sciences, and whose instruction in anatomy, physiology, neurology and the other fundamentals for treating the human body were under chiropractors (although some of these did have university training). Their own backgrounds did not suggest lives of research, writing and clinical instruction, yet they each became important in the lexicon of chiropractic technique after the initial debates between D. D. Palmer and his early associates, Willard Carver, S. M. Langworthy, Alva Gregory, Joy Loban and A. P. Davis (Gatterman & Lee 1995).
Discussion
Raymond L. Nimmo (1904–86) (Fig. 1) was a 1926 Palmer graduate who was to become the definitive pioneer in the now widely accepted area of soft tissue and trigger point therapy. His history and experience is similar to others who evolved specific technique research in this period. Among them were Joy Loban (1889–19?), who advocated an early nonforce technique (Gibbons 1991); Leo Spears (1894–1956), largely known for his hospital but an early formulator of ‘painless’ adjustments (Rehm 1991); Thomas Lake (1887–1950), who developed endonasal therapy (Gibbons & Thomas 1995); and Frederick W. Illi (1901–1984), developer of the sacroiliac physiology of spinal biomechanics (Gaucher-Peslherbe 1995).
Nimmo’s background is known. His contemporaries shared with him an absence of a grounding in the basic sciences or even in academics (although the early lives of Loban and Lake have still to be fleshed out). They advocated specific technique instruction with a passionate fervour that gained thousands of followers during their lives. Unlike them, Nimmo’s technique, termed Receptor-Tonus (RT), has survived its founder (Illi’s work may correctly have evolved into conceptual chiropractic theory rather than a technique). Although other techniques have become either discarded or little-used, Nimmo’s technique survived. Although developed in the limited chiropractic world of the 1950s, his concepts are compatible with contemporary medical thought in this area. Nimmo was born in Fort Worth in 1904, where he lived most of his life, with the exception of his college and military experience. He attended Tarleton State University in Stephenville in 1923 and a year later entered the Palmer School of Chiropractic, receiving his D.C. in 1926. That decade the Palmer School graduated several individuals who introduced new chiropractic techniques—Spears, Gonstead, Gillet—although other schools would also produce contemporaries (Hugh and Vinton Logan and Illi at Universal; DeJarnette at the Nebraska College).
Although he travelled in the Navy, and briefly practised in Illinois, Oklahoma and Georgia, Nimmo practised for 30 years in Fort Worth. He moved to suburban Granbury in 1956. In his invited essay response to National College anatomist Bachop, Nimmo traced the evolution of his theoretical and clinical process to RT, much of which involved instruction by those who had originated other techniques:
In 1935 I took what Logan called Basic Technique, which he took from Dr. John Hurley’s Aquarian Age Healing. Dr. Hugh and Dr. Vinton were in Hurley’s first class. I subsequently taught BT for a while … [I practiced] what was called Chromaffin Synapse Therapy … which we thought was the sacral ganglia, but was actually releasing muscles … [yet both] got results, sometimes spectacularly (Nimmo 1981).
A review of chiropractic techniques by Lee and Gatterman (Gatterman & Lee 1995) listed almost 100, with multiple developers in many instances, yet some explored by Nimmo were not included:
I took what was called Bio-Engineering … D. C. McIntosh taught what he called the McIntosh system of Fascia Release … we would palpate for tensed fascia, then release it. What it was, of course, was tensed musculature (Nimmo 1981).
Later Nimmo met Ida Rolf, Ph.D., the founder of the Rolfing school, and investigated her methods. Rolf’s work led Nimmo to speculate:
[In Rolfing,] the theory was that muscles were bound down by connective tissue, and had to be freed … [I determined] that certain muscles were not affected. Rolf worked on all of them, even on the ribs where there were no muscles. When I found that muscles such as the latissimus and the hamstrings were not affected, I sought to discover why, and determined that these muscles are affected, just not as often. I eventually solved all of this. A piece in Scientific American explained tonus, which has never been taught in the schools. It is hypermyotonia which causes the so-called subluxation and other distortions (Nimmo 1981, 1971).
In his practice, Nimmo observed ‘spots on the shoulders which when pressed on referred pain to various areas, and the results were spectacular in case after case’ (Nimmo 1981). He called these ‘Noxious Generative Points.’ In 1952, he discovered the work of Janet Travell, M.D., perhaps the foremost physician to research myofascial pain and dysfunction, who became prominent in the 1960s as personal physician to President John F. Kennedy. Travell related her fascination with examining muscles in cadavers in the dissection laboratory.
Travell, who had on several occasions expressed to one of the authors (J.H.C.) her admiration for Nimmo’s work (Travell J., personal communication), discussed trigger points in a Symposium on Connective Tissue. This apparently prompted Nimmo to search the literature further and to reach his thesis that became the foundation for the Receptor-Tonus therapy:
I realized what every patient can understand, but many chiropractors seemingly cannot, that no bone can move unless a muscle moves it, and no muscle moves a bone unless a nerve impulse reaches it. I decided the lumbar lordosis was due to tight sacrospinalis muscles. I would release them, but the patient would go back into the same position, with return of pain. I looked for muscles that pulled down the front of the pelvis, which were of course, the quadriceps … (Travell J. Personal communications, 1991 Oct 20 and 1990 Apr 26) (Nimmo 1981).
Thus, a Texan with a year of college and 18 months of classroom and clinic experience during the Palmer School’s classical period entered a decades-long quest to eliminate or at least control pain. In his 1980 letter to Bachop, Nimmo said that he found it difficult to write, yet he came through with quotable expressions, such as ‘… there are certain essentials necessary in order for us to escape from the mossy-fingered grip of orthodoxy and improve when a superior method is evident’ (Nimmo 1981).
in Receptor-Tonus we strive to teach nothing that does not have a physiological basis. The discovery of certain laws gives validity and substance to this principle of practice. It is ensconced in physiology, and consequently can stand the white light of scientific scrutiny (Nimmo 1981).
His therapy was summarized from a chiropractic perspective by Gatterman and Lee (Fig. A.1):
Nimmo found noxious generative points in muscles that referred pain in characteristic patterns. Viewing these hypersensitive areas, the trigger points of Travell, as abnormal reflex arcs he developed a manual technique designed to reduce the irritable loci. He referred to the inter-relationship of muscle tonus and the central nervous system as ‘reverberating circuits,’ whereby the stimulus was self-perpetuating until the cycle was broken… . This procedure referred to by Travell as ischemic compression offers a noninvasive chiropractic technique instead of the common medical practice of injection of the painful trigger points (Gatterman & Lee 1995).
The following is a brief description of the neurophysiology on which RT is based, according to Nimmo in 1986, the year of his death:
Although it is generally called the Nimmo Technique, the correct designation is Receptor-Tonus Technique for the reason that it deals exclusively with muscle tonus and nerve receptors which initiate pain. The early development of the method was necessarily somewhat experimental and empirical. It was different from anything I had ever been taught but it was the most efficient method and permanent release from pain I had ever used or observed (Nimmo 1986).
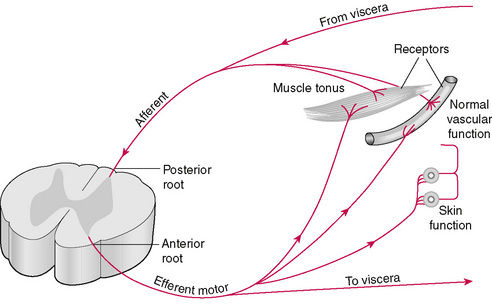
To fully understand RT, one must have a basic understanding of the concept of tonus (Fig. A.2):
Tonus is not an exclusive property of isolated muscle. It is an interaction between a muscle and the spinal cord by the sympathetics. Muscles project a continuous stream of impulses through the posterior root to the gray matter of the cord where the internuncial neurons increase the stimuli which are transmitted through the anterior root and upon reaching the muscle produce a slight pull. This is normal tonus. Tersely stated, the internuncial neurons in the cord are highly excitatory. In their reactive relationships with one another there is a self re-exiting process, which increases and prolongs the motor discharge induced by the incoming stimuli from sensory nerves. Livingston observed that when a volley of sensory stimuli entered the cord for two milliseconds, the discharge through the ventral root lasted 20 milliseconds—in this case ten times longer. Guyton called this the after discharge (Nimmo 1986).
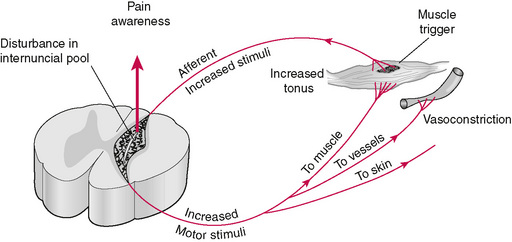
The malfunction of this normal process results in a hypertonic muscle (Fig. A.3). Nimmo states,
Hypermyotonia may result from various insults such as accidents, exposure to cold drafts or from occupations requiring prolonged periods of postural strain such as typing or driving an automobile for many hours without rest (Nimmo 1986).
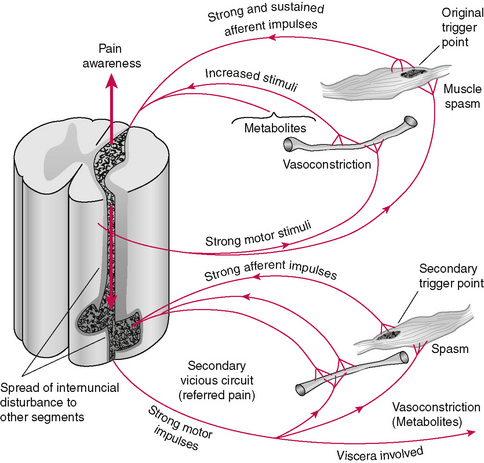
Figure A.3 Vicious physiopathological reflex circuit arising from peripheral structures with referred phenomena (Nimmo 1971).
Increased sensory input to the cord from such ‘insults’ results in an increased stream of efferent impulses to the muscles, causing a constant state of abnormal contraction.
This in turn causes additional increase in sensory impulses back to the cord, which are again amplified in the internuncial pool, causing even more efferent impulses to the muscle. The result is a vicious, self-perpetuating cycle, with the muscle getting tighter and tighter. This process, occurring in the sympathetic nerves, is beyond voluntary control. Reflex spillover in the sympathetic nerves also causes local vasoconstriction, trapping metabolites in the area (Nimmo 1986).
The focus of irritability within this area of abnormal muscle contraction and vasoconstriction becomes the trigger point. As this process continues, it spreads to other levels of the cord, causing secondary trigger points to develop in other muscles as well as the well known phenomenon of referred pain (Fig. A.4). It is fascinating to compare this diagram with Figure 5, which is from Travell and Simon’s 1983 masterpiece Myofascial Pain and Dysfunction—The Trigger Point Manual (Travell & Simons 1983). The similarities are striking and suggest one concept developed concurrently by two outstanding independent researchers.
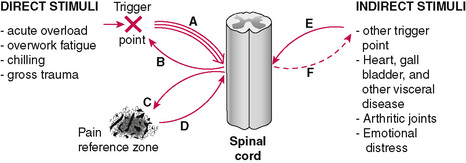
Figure A.4 Direct and indirect stimuli.
(Reprinted by permission from Travell JG, Simons DG. Myofascial pain and dysfunction: the trigger point manual. Vol. 1. Baltimore: Williams & Wilkins; 1983 p. 15.)
The difference between Nimmo’s and Travell’s treatment methods is significant. Travell advocated injections to the trigger point and later spray and stretch and ‘ischemic compression’ to relax the involved muscle. On the other hand, Nimmo states, ‘I have found that a proper degree of pressure, sequentially applied, causes the nervous system to release a hypertonic muscle’ (italics are Nimmo’s). Nimmo did not see the trigger point as an object to be injected, stretched, massaged or dissolved by ultrasound (Cohen & Schneider 1990; Nimmo 1981).
He saw the trigger point as the result of a neurological chain of events that must be approached through the nervous system. This puts RT squarely in the realm of chiropractic; it is not merely an adjunctive therapy, as is so often thought. Nimmo spent 30 years evolving and refining this approach empirically. Every time a patient presented with a new problem, he painstakingly figured out which muscles were involved, consulted his anatomy books, and developed a method of applying pressure to that muscle, as well as muscles seemingly remote from the primary problem that contained secondary trigger points. Nimmo determined that all primary and secondary trigger points must be eliminated to eliminate this vicious cycle. This requires precise application of proper pressure to all involved muscles in the appropriate sequence (Nimmo 1986, Cohen & Schneider 1990, Nimmo 1981).
In a videotape made in the early 1980s, Nimmo explored the philosophical and the scientific approach of his practice and research methodology, recalling that his philosophy classes departed from anatomical and physiological facts to make questionable deductions for the subluxation theory ‘which was then upper cervical and later HIO.’ Nimmo declared that ‘understanding the principles upon which Receptor-Tonus is based has simplified many problems, and brought explanation to many others. We can now explain how D. D. Palmer restored hearing to Harvey Lillard by making a thrust to the fourth thoracic vertebra’ (Nimmo 1984).
Nimmo circulated a paper published in 1957 by Arizona practitioner Stanley Hayes, in which Hayes proposed a ‘new hypothesis for consideration’ of the chiropractic subluxation concept. Citing the Lillard case, Hayes said that the traditional chiropractic adjustment was:
based on the idea that force should be used to remove nerve disturbance at any point in the spine where such disturbance appears to exist. Most clinical results are actually secured by releasing abnormal states of tension in the ligaments (and possibly muscles) closely associated with the spine (Hayes 1957).
Later in 1957, Nimmo would also author an article in the Journal of the NCA titled ‘Receptors, effectors and tonus—a new approach’ (Nimmo 1957), which he subsequently reprinted as the first number of an occasional RT newsletter called The Receptor. In this paper, Nimmo made this conclusion about his work:
I believe that a full knowledge of this approach will give one the anatomical and physiological right to fully eighty percent of all illness. I have subscribed to many techniques, putting all to thorough test, and I have found almost all of them valuable. After much experience working with this principle I am convinced that it is anatomically and physiologically sound (Nimmo 1957).
Nimmo stressed the necessity of cooperation with the larger health care community even at a time when there was evidence of the overt and covert antichiropractic activity within many parts of mainline medicine. ‘Chiropractic cannot be insular,’ he declared many times in a lengthy videotape (Nimmo 1984). He cited not only Travell but Bonica, head of the Department of Anesthesiology at the University of Washington medical school, whom he quoted as saying that ‘medicine does not know the basic principles of pain,’ lamenting the absence of any teaching in medical schools and any widely-supported pain research (Travell & Simon 1983; Nimmo 1984, 1969).
Travell’s work in The American Practitioner and her 1983 book Myofascial Pain and Dysfunction: The Trigger Point Manual were frequently referenced. Nimmo stressed dialogue with medicine and cited cases in which he had recommended surgery even after attending surgeons had not recommended that course. His departure from medical procedures for low back pain was essentially the trigger point injection, asserting that conservative manipulative procedures utilizing RT could effect the same results. Three medical researchers at George Washington University Medical Center conducted a ‘randomized, double-blind evaluation of trigger point injection’ in 1988, concluding that ‘this study indicates that the critical factor in giving relief of pain is not the injected substance but rather, some type of mechanical stimulus to the trigger point’ (Garvey et al. 1989).
Nimmo summarized the RT Method as being based on two main principles: a method that removes the origin of nerve impulses producing abnormal, painful and pathological processes in the body. In 1970, he wrote of RT that
It clears trigger points, those described in the current literature, but many more not yet known, as well as inaccessible to the methods of other professions. It eliminates those factors which hold the body or parts thereof in a state of misalignment and distortion. The first frees the body from pain, the second further frees it of pain and straightens it up.
What may be exceptional about Nimmo’s technique is the wide acceptance that it achieved through the series of classes which he conducted throughout the United States and Canada, starting in 1958. Nimmo declared that ‘no other concept introduced to our profession has had so great an impact upon our professional thinking in a like period of time’ (Nimmo 1963). In the same publication, Nimmo wrote that he had received a request from the Department of Health, Education and Welfare (which preceded the present Health & Human Services) for all copies of The Receptor, to ‘be placed in the Department of New Medical Discoveries of the Library of Congress.’
A striking example of the advanced state of Nimmo’s thought appeared recently in the journal Advances in Physical Therapy (Makous 1995). What is described as a ‘unique intraoral approach’ to treating temporomandibular joint disorder discusses a manual trigger point treatment for tensor veli palatini muscle. This technique, along with methods for treating all the muscles of mastication, was taught by Nimmo in his seminars throughout the 1960s and 70s and was published in The Receptor in 1980 (Nimmo 1981).
Conclusion
Several conclusions are offered about Raymond Nimmo and his technique, from the collaborative effort of both a practitioner of his teaching and a lay observer of the history of the profession (Fig. A.5).
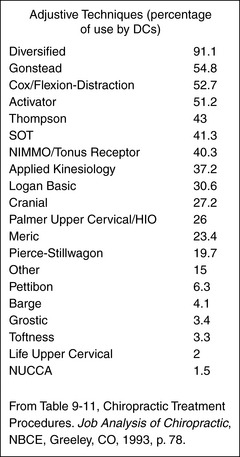
Adjustive Techniques (percentage of use by DCs)
| Diversified | 91.1 |
| Gonstead | 54.8 |
| Cox/Flexion-Distraction | 52.7 |
| Activator | 51.2 |
| Thompson | 43 |
| SOT | 41.3 |
| NIMMO/Tonus Receptor | 40.3 |
| Applied Kinesiology | 37.2 |
| Logan Basic | 30.6 |
| Cranial | 27.2 |
| Palmer Upper Cervical/HIO | 26 |
| Meric | 23.4 |
| Pierce-Stillwagon | 19.7 |
| Other | 15 |
| Pettibon | 6.3 |
| Barge | 4.1 |
| Grostic | 3.4 |
| Toftness | 3.3 |
| Life Upper Cervical | 2 |
| NUCCA | 1.5 |
From Table 9-11, Chiropractic Treatment Procedures. Job Analysis of Chiropractic, NBCE, Greeley, CO, 1993, p. 78.
1. Nimmo, although a pioneer graduate with but a rudimentary exposure to anatomy, physiology and neurology, evolved a sophisticated approach to technique in the alleviation of myofascial pain. This approach was a dramatic paradigm shift from the traditional chiropractic theories of the day, which emphasized the ‘bone on nerve’ concept.
2. As a chiropractor, he introduced basic concepts in trigger point therapy that were complementary to those being advanced by such recognized medical pioneers as Travell. He supported these concepts with extensive medical references and was completely up to date on current scientific literature (Travell J. Personal communications, 1991 Oct 20 and 1990 Apr 26) (Nimmo 1963).
3. The Nimmo technique, in competition with many contemporary adjustive procedures, has survived for almost half of the profession’s history and is currently used by 40 percent of chiropractors according to a study conducted in 1993 by the National Board of Chiropractic Examiners (Job analysis of chiropractic 1993).
In time, the ‘small town chiropractor from Texas’ may obtain some posthumous recognition in the larger literature of the healing arts, for Raymond Nimmo was a legitimate pioneer in the identification and treatment of pain, which remains as a primary challenge to practitioners of all schools in these final years of the twentieth century.
Council on chiropractic guidelines and practice parameters
Chiropractic management of myofascial trigger points and myofascial pain syndrome: a systematic review of the literature
Howard Vernon, DC, PhD,a and Michael Schneider, DCb
Abstract
Objectives: Myofascial pain syndrome (MPS) and myofascial trigger points (MTrPs) are important aspects of musculoskeletal medicine, including chiropractic. The purpose of this study was to review the most commonly used treatment procedures in chiropractic for MPS and MTrPs.
Methods: The Scientific Commission of the Council on Chiropractic Guidelines and Practice Parameters (CCGPP) was charged with developing literature syntheses, organized by anatomical region, to evaluate and report on the evidence base for chiropractic care. This article is the outcome of this charge. As part of the CCGPP process, preliminary drafts of these articles were posted on the CCGPP website www.ccgpp.org (2006-8) to allow for an open process and the broadest possible mechanism for stakeholder input. PubMed, Excerpta Medica Database, Cumulative Index to Nursing and Allied Health Literature, and databases for systematic reviews and clinical guidelines were searched. Separate searches were conducted for (1) manual palpation and algometry, (2) chiropractic and other manual therapies, and (3) other conservative and complementary/alternative therapies. Studies were screened for relevance and rated using the Oxford Scale and Scottish Intercollegiate Guidelines Network rating system.
Results: A total of 112 articles were identified. Review of these articles resulted in the following recommendations regarding treatment: Moderately strong evidence supports manipulation and ischaemic pressure for immediate pain relief at MTrPs, but only limited evidence exists for long-term pain relief at MTrPs. Evidence supports laser therapy (strong), transcutaneous electrical nerve stimulation, acupuncture, and magnet therapy (all moderate) for MTrPs and MPS, although the duration of relief varies among therapies. Limited evidence supports electrical muscle stimulation, high-voltage galvanic stimulation, interferential current, and frequency modulated neural stimulation in the treatment of MTrPs and MPS. Evidence is weak for ultrasound therapy.
Conclusions: Manual-type therapies and some physiologic therapeutic modalities have acceptable evidentiary support in the treatment of MPS and TrPs (J Manipulative Physiol Ther 2009;32:14-24).
Key Indexing Terms: Myofascial Pain Syndromes; Myofascial Trigger Points; Chiropractic; Musculoskeletal Manipulations.
Ever since the seminal work of Travell and Rinzler (1952) in 1952, the role of myofascial trigger points (TrPs) in myofascial pain syndrome (MPS) has become an accepted part of musculoskeletal clinical practice. Along with Simons (Travell & Simons 1983), Travell first identified the importance of myofascial pain and its localization in what they termed trigger points, providing the first classification of diagnostic criteria for TrPs. They also provided detailed maps of the pain referral patterns from TrPs in all the muscles of the body. Myofascial pain syndrome is currently thought to be the leading diagnosis among pain management specialists (Harden et al. 2000) and the leading diagnosis in pain patients reporting to general practitioners (Skootsky et al. 1989).
Interest in myofascial tenderness extends throughout the history of chiropractic. It might be said that local paraspinal tenderness, as part of the manifestations of the ‘subluxation,’ was a central feature of chiropractic thinking from its inception. Arguably, the work of Ray Nimmo (Nimmo 1962, 1984, 1992) represents the earliest and perhaps still most established thinking on this topic among chiropractors. Cohen and Gibbons (Cohen et al. 1998) describe his work as ‘a conceptual leap from moving bones to working with muscles that move bones.’ Schneider (1994, 2001) has provided a collection and review of all of Nimmo’s works. Nimmo’s explanations in the 1950s of the pathophysiology of TrPs are still regarded as accurate and highly sophisticated.
Other chiropractic authors who have written on this topic include Schneider (Schneider 1990, 1994, 1995, 2001), Perle (Perle 1989, 1995), Hains (Hains 2002, 2002), and Hammer (Hammer 2007) whose seminal textbook is now in its third printing. There are also numerous case reports and technical reports relating to various soft tissue techniques in chiropractic. In the field of MPS, chiropractic is generally regarded as one of the complementary and alternative medical (CAM) therapies. The CAM therapies are quite commonly used in the treatment of myofascial pain and TrPs (Harris & Clauw 2002), and there is considerable overlap between chiropractic approaches and CAM therapies in this field.
Methods
The search strategy for this review was constrained by the need to identify only those studies of chiropractic treatments (manual therapy and other conservative therapies) that were not directed at clinical complaints associated with any of the specific body regions that have been designated as other reviews in the Council on Chiropractic Guidelines and Practice Parameters (CCGPP) process. In other words, no study was selected of the effect of a chiropractic treatment specifically indicated for back pain, neck pain, upper limb pain (shoulder, elbow, wrist), and lower limb pain (hip, knee, ankle, and foot) of any kind (i.e., for any category of diagnosis). Only studies of chiropractic treatments for MPS and TrPs were considered. Therefore, the inclusion criteria for this search were as follows: manual therapies, trigger points, myofascial pain syndrome (MeSH headings: musculoskeletal manipulations, myofascial pain syndrome [not exploded to temporomandibular joint]), conservative therapies, laser, acupuncture, ultrasound (US), electrotherapy, naturopathy; 1965 to 2007; English, German; human studies.
After the primary search was conducted, a number of secondary searches were conducted based upon ‘related links,’ especially emphasizing systematic or clinical reviews, randomized clinical trials, and conservative treatments (vs musculoskeletal manipulations only), as well as searches of additional works by the authors identified in the primary search. Finally, citation reviews were conducted manually to identify any additional suitable studies.
This search was conducted in the PubMed; Cumulative Index to Nursing and Allied Health Literature; Index to Chiropractic Literature (ICL); Manual, Alternative, and Natural Therapy System (MANTIS); Excerpta Medica Database; National Guidelines Clearinghouse; Database of Abstracts of Reviews of Effects; and Turning Research Into Practice databases. Selected publications were rated on the Oxford Rating Scale (Phillips et al. 2001, Sackett et al. 2000) as well as the Scottish Intercollegiate Guidelines Network (SIGN) Checklist (Fig. A.6).
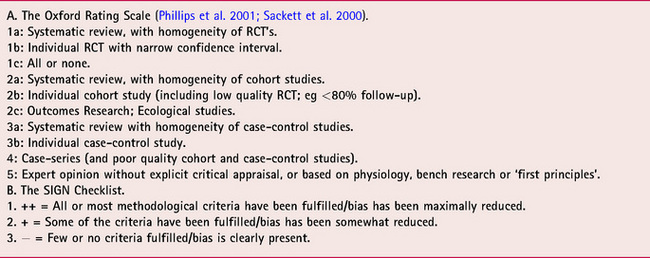
This review accepted all levels of published evidence for narrative description: clinical guidelines, systematic reviews, clinical trials, cohort or case series, case studies, and clinical reviews. For evidence rating, recommendations were constructed and rated according to the Oxford Rating Scale (Phillips et al. 2001, Sackett et al. 2000) as follows:
Results
Manual Therapies
Systematic Reviews of Manual Therapies. Two completed systematic reviews were identified (Fernandez de las Penas et al. 2005, Rickards 2006). These reviews were rated (Oxford Scale) as 1a evidence with a 2+ quality rating on the SIGN Checklist.
Fernandez de las Penas et al. (2005) used the following selection criteria for acceptable studies:
clinical or randomized controlled trials in which some form of manual therapy (strain/counterstrain, ischemic compression, transverse friction massage, spray and stretch, muscle energy technique) was used to treat (myofascial trigger points) MTrPs (p. 29).
Mobilization and manipulation were apparently not explicitly included. It should be noted that the criterion applied to the ‘clinical category’ in this search was ‘MTrPs,’ although MPS was referenced later in their review. No additional, more specific criteria related to clinical complaints in any of the body regions (i.e., back pain, neck pain, limb pain, etc.) were used. It would appear that this search strategy is consistent with the one devised for this review, as other CCGPP reviews dealt with the chiropractic management of pain complaints specific to these body regions.
Fernandez de las Penas et al. (2005) identified 7 acceptable trials (SIGN = 2+/Oxford Scale ratings = 1b), 4 of which obtained a sufficiently high quality score (>5/10 on the Physiotherapy Evidence Database Scale).
• Gam et al. (1998) (Physiotherapy Evidence Database score = 6/10)
• Jaeger & Reeves (1986) (2/10)
• Hanten et al. (2000) (3/10)
• Hong et al. (1993) (6/10)
• Hou et al. (2002) (5/10)
• Hanten et al. (1997) (5/10)
• Dardzinski et al. (2000) (1/10)
The interventions used in these studies were as follows (number of studies in parentheses): spray and stretch (2), soft tissue massage (2), ischaemic compression (2), occipital release exercises (1), strain/counterstrain (SCS) (1), and myofascial release (1). An important finding was:
Only 2 studies … test(ed) the specific efficacy (efficacy beyond placebo) of various manual therapies in the treatment of MPS (Gam et al., 1998 [massage] and Hanten et al., 2000 [occipital release]). These studies found no difference between interventions (p. 30) (Fernandez de las Penas et al. 2005).
Another important issue from this group of studies is the duration of treatment. Most of these studies (4) investigated only the immediate effects on pain and tenderness (Jaeger & Reeves 1986, Hong et al. 1993, Hou et al. 2002, Hanten et al. 1997). One study investigated the short-term treatment effects of ischaemic compression vs exercises over 5 treatments (Hanten et al. 2000), whereas 2 investigated longer-term effects (6 months) of a course of, in one case, massage added to US therapy (Gam et al. 1998) and, in the other case, SCS in addition to exercises (Dardzinski et al. 2000). In both of the latter studies of a course of therapy, the manual therapy used (massage or SCS) was included among other therapies, making it impossible to identify the distinct contribution of the manual therapy to the reported outcomes.
Fernandez de las Penas et al. (2005) conclude that there are very few randomized controlled studies (RCTs) of any type of manual therapy in the treatment of MTrP (MPS) and, as a result, ‘the hypothesis that manual therapies have specific efficacy beyond placebo in the management of MPS caused by MTrPs is neither supported or refuted by the research to date’ (p. 33). They do acknowledge that there is some evidence for improvement in some groups within these trials and that this warrants further research.
In Rickards’ (2006) review, the inclusion criteria included RCTs of a conservative (in this section: manual only) therapy for active TrPs, not latent TrPs, in which a patient-related pain outcome was used and in which an explicit diagnosis of TrP was made including at least local tenderness and a taut muscle band. Studies were rated on a 20-point scale; however, no cutoff score was used for inclusion. Rickards included the following studies: Chatchawan et al. (2005), Fernandez de las Penas et al. (2006), Hanten et al. (1997), Hou et al. (2002), and Edwards & Knowles (2003).
For the purposes of the present review, the following comments apply to this group of studies: (1) The study of Chatchawan et al. (2005) of massage therapies clearly identified the target group as chronic low back pain and would be included in the CCGPP review on low back pain. (2) The study of Fernandez de las Penas et al. (2006) is included below. (3) The studies of Hanten et al and Hou et al are included in the review by Fernandez de las Penas et al above. (4) Edwards and Knowles’ trial (2003) did not include a manual therapy (only active stretching and dry needling were investigated). Therefore, for manual therapies, Rickards’ review does not add anything substantial to the present review.
A Cochrane Collaboration Protocol entitled ‘Non-invasive physical treatments of myofascial pain’ Kilkenny et al. (2007) was identified. This protocol currently contains no results. However, it was used as a source of additional references, particularly on published clinical trials and systematic reviews.
Practice Guidelines on Manual Therapy. The following practice guidelines were identified:
Institute for Clinical Systems Improvement (ICSI). Assessment and management of chronic pain. Bloomington (MN): Institute for Clinical Systems Improvement (ICSI); 2005 Nov. p. 77 No recommendation for physical (manual) therapies in the treatment of MPS or TrPs.
Work Loss Data Institute. Pain (chronic). Corpus Christi (TX): Work Loss Data Institute; 2006. 261 p. Myofascial pain syndrome, physical therapy: 14-21 days.
RCTs of Manual Therapy. In addition to Fernandez de las Penas et al (Gam et al. 1998), our search identified 3 RCTs (Oxford Scale rating = 1b or 2b) of the effect of spinal manipulation on local paraspinal muscular tenderness in the dorsal spine (Terrett & Vernon 1984 [2+/2b]), cervical spine (Vernon et al. 1990 [2+/2b]), and lumbopelvic area (Cote et al. 1994 [2+/2b]). All 3 studies investigated only the immediate effect of the interventions on local muscular pain thresholds (electrical stimulus in Terrett and Vernon (1984) and pressure stimulus in Vernon et al. (1990) and Cote et al. (1994). Immediate and statistically significant increases in pain thresholds were found for spinal manipulation as compared with mobilization in the cervical and dorsal paraspinal muscles, but not in the lumbopelvic soft tissues.
Vicenzino et al. (1996) (2+/1b) reported on the immediate effect of a cervical mobilization on pressure pain threshold (PPT) of tender points on the lateral epicondyle in patients with ‘tennis elbow.’ Only the mobilization (described as ‘manipulation’ in this study) resulted in statistically significant increases in lateral epicondyle PPTs vs placebo and control conditions.
Greene et al. (1990) (2+/1b) investigated the effect of 4 different treatments given 3 times over 3 days on skin resistance levels. Subjects with thoracic TrPs were randomized to receive osteopathic manipulative treatment (OMT), laser treatment, OMT plus laser, and sham laser. No significant differences in effects were noted between these groups.
Atienza Meseguer et al. (2006) (2+/1b) studied 54 subjects with trapezius TrP treated with classic SCS, modified SCS, and control. Both treatment groups showed immediate improvement in PPT vs controls, but not vs each other.
Fryer and Hodgson (2005) (2+/1b) compared manual pressure release to sham myofascial release in 37 subjects with upper trapezius myofascial TrPs. A statistically significant increase in PPT was obtained immediately after the intervention in the manual pressure group vs controls that was found to be due to a change in tissue sensitivity.
Fernandez de las Penas et al. (2006) (2+/1b) compared ischaemic compression to transverse friction massage in 40 subjects with myofascial TrPs in the upper trapezius muscle. Both groups obtained significant improvement in PPT within 2 minutes. No difference was found between the groups.
Conclusion: RCTs
A total of 14 RCTs were retrieved. Quality scores ranged widely for the 7 trials reviewed by Fernandez de las Penas et al. (2005). Ten of 14 trials we identified involved only immediate changes in TrP or tender point ratings. Two other trials reported outcomes for short courses of treatments over 3 to 5 days (Hanten et al. 2000, Greene et al. 1990), whereas 2 others reported outcomes at 6 months (Gam et al. 1998, Dardzinski et al. 2000). The outcomes of the ‘immediate’ trials can be summarized as demonstrating effectiveness in reducing tenderness for spinal manipulation (2 of 3 trials), spray and stretch (2 trials), ischaemic compression (3 trials), transverse friction massage (1 trial), and SCS (1 trial). One trial of mobilization failed to show any significant changes in tenderness scores vs controls. It would appear that there is moderately strong evidence to support the use of some manual therapies in the immediate relief of TrP tenderness.
The 2 trials of short-term effects (3–5 days) demonstrated the effectiveness of osteopathic manipulation and ischaemic compression, respectively, in reducing TrP tenderness. One long-term trial reported that SCS demonstrates clinically important changes in TrP tenderness and general pain over 6 months, whereas the other showed that massage produced limited effect. It would appear that there is only limited evidence to support the use of manual therapies over longer courses of treatments in the management of TrPs and MPS.
Case Reports of Manual Therapy Twenty-six case reports in the chiropractic literature were identified from ICL or MANTIS (Appendix A). These reports covered TrP treatments in patients with hand pain, low back pain due to a TrP in the quadratus lumborum muscle, wrist pain, fibromyalgia, upper quarter syndrome, MPS, and general TrPs.
Clinical Reviews of Manual Therapy Up-to-date clinical reviews (Hong 2004, Gerwin 2005, Alvarez & Rockwell 2002, Simons 2002, Harden 2007, Lavelle et al. 2007) by noted experts in the field of myofascial pain have endorsed the use of a variety of manual therapies in the treatment of TrPs and MPS. These are classed as level 5 (Oxford Rating) evidence.
Harden (2007) notes that the principal aims of therapy for MPS are relief of pain and inflammation, prevention of further injury, reducing spasm, correcting abnormal postures, and improving circulation. He endorses the following therapeutic modalities for accomplishing these aims:

• Postural and ergonomic education
• Exercises and postural correction
Hong (2004) recommends that the first principle of treatment of MPS is the identification and treatment of the presumed primary lesion (section 1). Only after this has been done, and if there is persistence of pain from the active TrPs, should direct treatment to the TrPs be performed. Hong suggests that, at this point in the therapeutic process, release of muscle tightness is the first objective. He identifies 7 steps in the treatment process for the active TrPs themselves:
i. Pain recognition: treating the active TrPs and not the latent ones.
ii. Identify the key TrP: Among active TrPs, one will be the most painful and most provocative of referred pain.
iii. Conservative vs aggressive treatment: This principle applies to the treatment of the primary lesion as well as the key TrP. Treatment should begin with what he describes as ‘non-invasive treatment including physiotherapy’ and progress toward more invasive forms of therapy.
iv. Acute vs chronic TrPs: Distinguishing these helps guide therapy in the acute vs chronic stages of pain.
v. Superficial vs deep TrPs: Different therapeutic modalities are needed the more deeply located is the TrP.
vi. Individual preference: Each patient may have levels of comfort and familiarity with various forms of treatment that should then be tailored to this need.
Hong places considerable importance on manual therapies for TrPs. He indicates the following as important aspects of manual therapy (p. 40):
Gerwin (2005) also endorses the treatment protocol that separately addresses therapies for the local TrP vs therapies for the perpetuating factors. In the former category, he specifically endorses manual TrP compression for focal TrP release, followed by myofascial release techniques for local stretching and then ‘therapeutic stretch’ for the longer-range elongation of the body segments. In the case of perpetuating factors, he includes correction of postural faults as well as joint dysfunction. This should be followed by an active programme of physical conditioning, stretching, and endurance, including preventative strategies. Unfortunately, no studies were provided as evidence for this approach.
Simons (2002) reviews the mechanisms of TrP formation and perpetuation to guide the appropriate treatment approach. The therapies endorsed in his review are as follows:
• Postisometric relaxation and release
• Trigger point (manual) pressure release
Only the work of Lewit (1986) is cited as support for this approach. Other noninvasive therapies that Simons merely mentions as additional to the approach described above include facilitatory techniques, acupuncture, SCS, microcurrent, US, and laser.
Alvarez and Rockwell’s (2002) review only provides a list of noninvasive treatment modalities that include acupuncture, osteopathic manual medicine techniques [sic], massage, acupressure, US, heat, ice, diathermy, transcutaneous electrical nerve stimulation (TENS), and ‘spray and stretch’ techniques. For these modalities, no clinical trial evidence was provided. The only support was a reference to the authoritative work described in Travell and Simons’ (1983) manual.
Lavelle et al. (2007) endorse the following treatments as efficacious: spray and stretch, TENS, physical therapy, and massage.
Critique of Clinical Reviews
Manual Therapies. All 6 reviews from within the last 5 years endorsed manual therapies for TrP treatment in MPS. None of these reviews provided a single reference to a clinical trial to support this position. None of the 11 trials reviewed above was cited in any of these reviews. As such, there is discordance, even at the level of renowned experts’ reviews, between the apparent consensus on the use and types of manual therapies in treating TrPs vs the evidence from the published literature.
Other therapies. Only Harden (2007) cites the clinical trial of Esenyel et al. (2000) (US + stretching vs dry needling + stretching vs stretching alone) and the case series of Simunovic et al. (1998) (laser therapy) as clinical studies of these sorts of therapies as well as the review of laser therapy by Gam et al. (1998). The other reviews provide no support in the form of any clinical study for their recommendation on noninvasive therapies for TrPs.
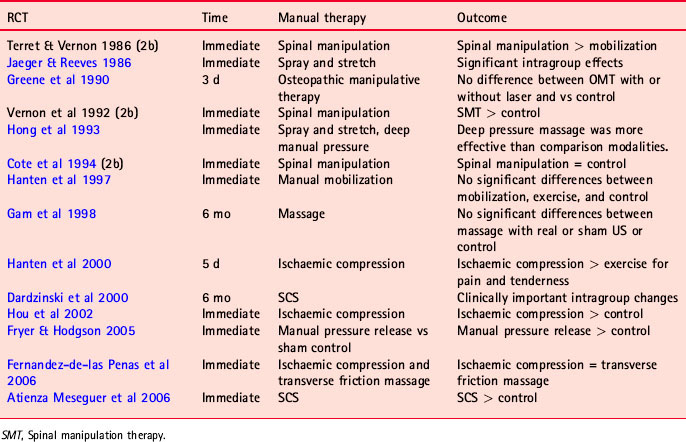
Evidence Synthesis of Manual Therapies. Tables A.1 and A.2 summarize the literature retrieved in this review.
Table A.1 Literature review: all studies
| Study type | Oxford level | Number |
|---|---|---|
| Systematic reviews | 1a | 2 |
| Systematic review protocols | 1 | |
| Practice guidelines | 1a | 2 |
| RCTs | 1b | 11 |
| RCTs | 2b | 3 |
| Case series | 4 | 3 (Grobli; Anderson; Crawford) |
| Case reports | 5 | 17 |
| Clinical reviews (selected: 2000-2005) | 5 | 6 |
Table A.2 Literature review: randomized clinical trials of manual therapy for MPS or TrPs (all rated as Oxford 1b, unless otherwise noted as 2b)
Clinical Practice Recommendations of Manual Therapies.
1. There is moderately strong evidence to support the use of some manual therapies in providing immediate pain relief at TrPs. The evidence level is B.
2. There is only limited evidence to support the use of manual therapies over longer courses of treatment in the management of TrPs and MPS. The evidence level is C.
Other Conservative Therapies
Systematic Reviews of Other Conservative Therapies. Two published reviews were identified for treatment methods other than manual therapies (Rickards 2006, Cummings & White 2001). In Rickards’ (2006) review, the inclusion criteria included RCTs of a conservative therapy for active TrPs, not latent TrPs, in which a patient-related pain outcome was used and in which an explicit diagnosis of TrP was made including at least local tenderness and a taut muscle band. Studies were rated on a 20-point scale; however, no cutoff score was used for inclusion. It should be noted that no trials for acupuncture were included in this review (below). A total of 18 trials were included in this review (Tables A.3-A.6). Rickards’ (2006) conclusions were based on the following schema:
• Significant evidence: consistent findings in multiple high-quality RCTs
• Moderate evidence: consistent findings in multiple lower-quality evidence and/or a single high-quality RCT
• Limited evidence: a single low-quality RCT
• Unclear evidence: inconsistent or conflicting results from multiple RCTs
• No evidence: no evidence identified
• Evidence of adverse effect: RCTs with lasting negative changes
Table A.3 Studies of laser therapy from Rickards (2006) (n = 6 studies)
| Study | Treatments | Outcomes |
|---|---|---|
| Gur et al. (2004) | Laser vs placebo | Laser > placebo |
| Snyder-Mackler et al. (1989) | Laser vs placebo | Laser > placebo |
| Ceccherelli et al. (1989) | Laser vs placebo | Laser > placebo |
| Hakguder et al. (2003) | Laser and stretching vs placebo and stretching | Laser > placebo |
| Ilbuldu et al. (2003) | Laser vs dry needling vs placebo | Laser > dry needling Laser > placebo |
| Altan et al. (2003) | Laser + exercise + stretching vs placebo + exercise + stretching | Laser = placebo (other treatments thought to contribute to improvement) |
Table A.4 Studies of electrotherapy from Rickards (2006) (n = 5 studies)
| Study | Treatments | Outcomes |
|---|---|---|
| Graff-Radford et al. (1986) | A: TENS mode A | B > C, D > A, E |
| B: TENS mode B | (B = 100 Hz) | |
| C: TENS mode C | ||
| D: TENS mode D | ||
| E: Placebo TENS | ||
| Farina et al. (2004) | FREMS vs TENS | FREMS = TENS |
| Hsueh et al. (1997) | A : Placebo electrotherapy | TENS > EMS, placebo |
| B : TENS | ||
| C : EMS | ||
| Ardic et al. (2002) | A: TENS + stretching | A = B > C |
| B: EMS + stretching | ||
| C: Stretching | ||
| Tanrikut et al. (2003) | A: HVGS + exercise | A > B, C |
| B: Placebo HVGS + exercise | ||
| C: Exercise |
Table A.5 Studies of magnet therapy from Rickards (2006) (n = 3 studies)
| Study | Treatments | Outcomes |
|---|---|---|
| Brown et al. (2002) | Magnets vs placebo | Magnets > placebo |
| Smania et al. (2005) | A: RMS | A > B > C |
| B: TENS | ||
| C: Placebo US | ||
| Smania et al. (2003) | A: RMS | A > B |
| B: Placebo RMS |
RMS, Repetitive magnetic stimulation.
Table A.6 Studies of US therapy from Rickards (2006) (n = 4 studies)
| Study | Treatments | Outcomes |
|---|---|---|
| Gam et al. (1998) | A: US + massage + exercise | A = B = C |
| B: Placebo US + massage + exercise | ||
| C: Control | ||
| Maljesi & Unalan (2004) | A: High-power US | A > B |
| B: Conventional US | ||
| Lee et al. (1997) | A: Placebo US | C > A |
| B: US | ||
| C: Electrotherapy | ||
| D: US + electrotherapy | ||
| Esenyel et al. (2000) | A: US + stretching | A, B > C |
| B: TrP injection + stretching | ||
| C: Stretching |
Rickards’ conclusions for each therapy were as follows:
Laser: Significant evidence that laser may be effective in the short term. Type, dose, and frequency of treatments require additional research.
TENS: Evidence (unqualified?) that TENS may be effective in providing immediate relief at TrPs.
Other electrotherapies: Limited evidence for the effectiveness of frequency modulated neural stimulation (FREMS), high-voltage galvanic stimulation (HVGS), electrical muscle stimulation (EMS), and interferential current (IFC).
US: Moderate evidence that US is no more effective than placebo.
Magnets: Preliminary evidence that magnets may be effective.
It was noted that most trials involved either immediate or short-term effects and that much more research, especially on the longer-term effects, was needed.
Cummings and White (2001) reviewed all trials up to 2000 of ‘Needling Therapies’ for myofascial pain. Three of these trials involved what could be described as ‘standard’ acupuncture typical of the type used by some chiropractors. This is distinguished from deep dry needling and any injection-type therapies that would not be standard chiropractic treatment approaches. For the present review, any trials that specifically identified one of the regional complaint areas in the CCGPP (i.e., low back pain, neck pain) without specifying the treatment of TrPs were excluded (Table A.7). Cummings and White (2001) concluded that marked improvements were demonstrated in most treatment groups. However, dry needling techniques alone did not appear to be superior to other treatments in the treatment of myofascial TrPs. As well, they could not find evidence for a specific efficacy of these techniques beyond placebo. They called for more placebo-controlled trials.
Table A.7 Studies of acupuncture therapy from Cummings and White (2001) (n = 3)
| Study | Treatments | Outcomes |
|---|---|---|
| Birch & Jamison (1998) (neck pain) | A: Superficial acupuncture + heat | At 3 mo: |
| B: Wrong point superficial acupuncture | A > B, C | |
| C: NSAID | ||
| Johannson et al. (1991) (facial pain or headache) | A: Acupuncture | At 3 mo: |
| B: Occlusal splint | A = B > C | |
| C: No treatment control | ||
| Kisiel & Lindh (1996) (neck pain) | A: Manual acupuncture | At 6 mo: |
| B: Physiotherapy | A = B |
IP,;NSAID, nonsteroidal anti-inflammatory drug.
A Cochrane Collaboration Protocol entitled ‘Non-invasive physical treatments of myofascial pain’ (Kilkenny et al. 2007) was identified. This protocol currently contains no results. However, it was used as a source of additional references, particularly on published clinical trials and systematic reviews.
RCTs of Other Conservative Therapies. Both Rickards (Rickards 2006) and Cummings and White (Cummings & White 2001) used specific inclusion and exclusion criteria that resulted in the exclusion of numerous studies, either because they were not RCTs or for various methodologic reasons. These excluded trials will not be listed or reviewed here, as that would both duplicate and undermine the methods and conclusions of these reviews. Several trials have been identified in the present search that either have been published since these reviews or were not identified at all in these reviews (probably because of the inclusion of MANTIS and ICL databases in the present search) in the following areas:
Acupuncture
There is some additional evidence that a course of deep acupuncture to TrPs is effective in the treatment of myofascial pain for up to 3 months (Table A.8).
Table A.8 Additional acupuncture trials
| Study | Treatments | Outcomes |
|---|---|---|
| Ceccherelli et al. (2006) (neck pain) | A: Somatic acupuncture | At 1 and 3 mo: A = B (both = positive effect on pain) |
| B: Somatic acupuncture + auricular acupuncture | ||
| Itoh et al. (2004) (low back pain) | A: Acupuncture at traditional points | At 3 mo: A > B, C (not statistically significant) |
| B: Superficial acupuncture at TrPs | ||
| C: Deep acupuncture at TrPs | ||
| Ceccherelli et al. (2002) (low back pain) | A: Superficial acupuncture to TrP | At 3 mo: B > A |
| B: Deep acupuncture to TrP | ||
| Goddard et al. (2002) (jaw pain) | A: Acupuncture | Immediately: A = B |
| B: Sham acupuncture | ||
| Ceccherelli et al. (2001) (shoulder) | A: Superficial acupuncture to TrP | At 1 and 3 mo: B > D |
| B: Deep acupuncture to TrP |
Laser
The study of Greene et al. (1990) of laser vs osteopathic manipulation (OMT) alone vs OMT + laser vs sham laser to thoracic paraspinal muscle TrPs over 3 days involved measuring only local skin resistance. No measures of pain or tenderness response were made. This study would not have qualified for Rickards’ review and does not, as well, for the present review.
Olavi et al. (1989) compared infrared laser to placebo laser over various active TrPs located throughout the body. Pressure pain thresholds were measured immediately after and then 15 minutes after treatment. A statistically significant difference favouring the laser group was found, especially at 15 minutes.
Exercise
No additional studies not already included in Rickards (2006) under ‘physical therapies’ were retrieved.
Spray and stretch
The study of Hou et al. (2002) was included in section 3 and was included in the reviews of both Fernandez de las Penas et al. (2005) and Rickards (Kilkenny et al. 2007) under the category of manual therapy. This is because most treatment groups received ischaemic compression with or without a variety of other physiologic therapies. One of these therapies was spray and stretch, making Hou et al. (2002) the only published clinical trial to investigate this therapy. Hou et al found that the addition of spray and stretch to ischaemic compression provided immediate benefit in reducing TrP sensitivity. There are no other published clinical trials of spray and stretch therapy for management of pain from TrPs. Notwithstanding this, it is often cited by clinical experts as a valuable treatment of TrPs.
Ultrasound
Srbely and Dickey (2005, 2007) applied therapeutic-intensity vs low-intensity US to trapezius TrPs in 44 subjects. Pressure pain thresholds over trapezius TrPs increased 44% (14.2%) in the first group, whereas no increase was obtained in the second group.
Evidence Synthesis of Other Conservative Therapies. Table A.9 summarizes the evidence retrieved in this review.
Table A.9 Literature review: all studies of other conservative therapies
| Study type | Oxford level | Number |
|---|---|---|
| Systematic reviews | 1a | 2 |
| Systematic review protocols | 1 | |
| Practice guidelines | 1a | 2 |
| RCTs | 1b | 29 |
Clinical Practice Recommendations.
1. Laser: There is substantial evidence that laser therapy is effective in the treatment of TrPs and MPS. The evidence level is A.
2. TENS: There is moderately strong evidence that TENS may be effective in providing immediate relief at TrPs. The evidence level is B.
3. There is limited evidence for the effectiveness of other forms of electrotherapy: FREMS, HVGS, EMS, and IFC. The evidence level is C.
4. US: There is conflicting evidence as to whether US is no more effective than placebo or is somewhat more effective than other therapies in the treatment of TrPs and MPS. The evidence level is C.
5. Magnets: There is some evidence that magnets may be effective in the treatment of TrPs and MPS. The evidence level is B.
6. Acupuncture: There is some evidence that a course of deep acupuncture to TrPs is effective in the treatment of myofascial pain for up to 3 months. The evidence level is B.
Conclusion
The published evidence for the treatment of MPS and TrPs by common chiropractic treatments has been reviewed. Although publications ranging from systematic reviews and clinical trials to clinical reviews were included in the review, the evidence ratings were developed only on the basis of the clinical trial evidence. Manual-type therapies and some physiologic therapeutic modalities have acceptable evidentiary support in the treatment of MPS and TrPs (Table A.10).
Table A.10 Summary of recommendations
| Topic | Conclusion and strength of evidence rating |
|---|---|
| Manipulation/mobilization | Rating B: short-term relief |
| There is moderately strong evidence to support the use of some manual therapies (manipulation, ischaemic pressure) in providing immediate relief of pain at MTrPs. | |
| Rating C: long-term relief | |
| There is limited evidence to support the use of some manual therapies in providing long-term relief of pain at MTrPs. | |
| Conservative nonmanipulation | Rating A: laser therapies |
| There is strong evidence that laser therapy (various types of lasers) is effective in the treatment of MTrPs and MPS. | |
| Rating B: TENS, magnets, and acupuncture | |
| There is moderately strong evidence that TENS is effective in the short-term relief of pain at MTrPs. | |
| There is moderately strong evidence that magnet therapy is effective in the relief of pain at MTrP and in MPS. | |
| There is moderately strong evidence that a course of deep acupuncture to MTrPs is effective in the treatment of MTrPs and MPS for up to 3 mo. | |
| Rating C: electrotherapies, US | |
| There is limited evidence for the effectiveness of EMS, HVGS, IFC, and FREMS in the treatment of MTrPs and MPS. | |
| There is conflicting evidence that US is no more effective than placebo or is somewhat more effective than other therapies in the treatment of MTrPs and MPS. |
Altan L., Bingol U., Aydae M., Yurtkuran M. Investigation of the effect of GA AS laser therapy on cervical myofascial pain syndrome. Rheumatol Int. 2003;25:23-27.
Alvarez D.J., Rockwell P.G. Trigger points: diagnosis and management. Am Fam Physician. 2002;65:653-660.
Ardic F., Sarhus M., Topuz O. Comparison of two different techniques of electrotherapy on myofascial pain. J Back Musculoskelet Rehabil. 2002;16:11-16.
Atienza Meseguer A., Fernandez de las Penas C., Navarro-Poza J.L., Rodriguez-Blanco C., Bosca Gandia J.J. Immediate effects of the strain/counterstrain technique in local pain evoked by tender points in the upper trapezius muscle. Clin Chiropr. 2006;9:112-118.
Bachop W. Letter to Raymond Nimmo. Nov 20, 1980.
Birch S., Jamison R.N. Controlled trial of Japanese acupuncture for chronic myofascial neck pain: assessment of specific and nonspecific effects of treatment. Clin J Pain. 1998;14:248-255.
Brown C.S., Ling F.W., Wan J.Y., et al. Efficacy of static magnetic field therapy in chronic pelvic pain: a double-blind pilot study. Am J Obstet Gynecol. 2002;187:1581-1587.
Ceccherelli F., Altafini L., Lo Castro G., et al. Diode laser in cervical myofascial pain: a double-blind study versus placebo. Clin J Pain. 1989;5:301-304.
Ceccherelli F., Bordin M., Gagliardi G., et al. Comparison between superficial and deep acupuncture in the treatment of shoulder myofascial pain: a randomized and controlled study. Acupunct Electrother Res. 2001;26:229-238.
Ceccherelli F., Rigoni M.T., et al. Comparison of superficial and deep acupuncture in the treatment of lumbar myofascial pain: a double-blind randomized controlled study. Clin J Pain. 2002;18:149-153.
Ceccherelli F., Tortora P., Nassimbeni C., et al. The therapeutic efficacy of somatic acupuncture is not increased by auriculotherapy: a randomised, blind control study in cervical myofascial pain. Complement Ther Med. 2006;14:47-52.
Chatchawan U., Thinkhamrop B., Kharmawan S., et al. Effectiveness of traditional Thai massage versus Swedish massage among patients with back pain associated with myofascial trigger points. J Bodywork Mov Ther. 2005;9:298-309.
Cohen J., Gibbons R., Raymond L. Nimmo and the Evolution of Trigger Point Therapy, 1929-1986. J Manipulative Physiol Ther. 21(3), 1998.
Cohen J.H., Schneider M. Receptor-tonus technique: an overview. Chiropr Technique. 1990;2:13-16.
Cote P., Mior S.A., Vernon H. The short-term effect of a spinal manipulation on pain/pressure threshold in patients with chronic mechanical low back pain. J Manipulative Physiol Ther. 1994;17:364-368.
Cummings T.M., White A.R. Needling therapies in the management of myofascial trigger point pain: a systematic review. Arch Phys Med Rehabil. 2001;82:986-992.
Dardzinski J.A., Ostrov B.E., Hamann L.S. Myofascial pain unresponsive to standard treatment. Successful use of strain and counterstrain technique in physical therapy. J Clin Rheum. 2000;6:169-174.
Edwards J., Knowles N. Superficial dry needling and active stretching in the treatment of myofascial pain—a randomised controlled trial. Acupunct Med. 2003;21:80-86.
Esenyel M., Caglar N., Aldemir T. Treatment of myofascial pain. Am J Phys Med Rehabil. 2000;79:48-52.
Farina S., Casarotto M., Bennelle M., et al. A randomised controlled study on the effect of two different treatments (FREMS and TENS) in myofascial pain syndrome. Eura Medicophys. 2004;40:293-301.
Fernandez de las Penas C., Alonso-Blanco C., Fernandez-Camero J., et al. The immediate effect of ischemic compression technique and transverse friction massage on tenderness of active and latent myofascial trigger points: a pilot study. J Bodywork Mov Ther. 2006;10:3-9.
Fernandez de las Penas C., Sohrbeck Campo M., Fernandez Carnero J., et al. Manual therapies in myofascial trigger point treatment: a systematic review. J Bodywork Mov Ther. 2005;9:27-34.
Fryer G., Hodgson L. The effect of manual pressure release on myofascial trigger points in the upper trapezius muscle. J Bodywork Mov Ther. 2005;9:248-255.
Gam A.N., Warming S., Larsen L.H. Treatment of myofascial trigger points with ultrasound combined with massage and exercise: a randomized controlled trial. Pain. 1998;77:73-79.
Garvey T.A., Marks M.R., Wiesel S.W. A prospective randomized, double-blind evaluation of trigger-point injection therapy for low-back pain. Spine. 1989;14:962-964.
Gatterman M., Lee H.K. Chiropractic adjusting techniques. In: Peterson D., Weise G., editors. Chiropractic: an illustrated history. Chicago: Mosby; 1995:240-261.
Gaucher-Peslherbe P.L. Fred Illi and sacroiliac dynamics. Lombard, IL: Lecture at the National College of Chiropractic, 1995.
Gerwin R.D. A review of myofascial pain and fibromyalgia—factors that promote their persistence. Acupunct Med. 2005;23:121-134.
Gibbons R.W. Joy Loban and Andrew P Davis: itinerant healers and schoolmen. Chiropr History. 1991;11(1):23.
Gibbons R.W., Thomas T. Lake and endo-nasal therapy. Lombard, IL: Paper delivered at National College of Chiropractic, 1995.
Goddard G., Karibe H., McNeill C., et al. Acupuncture and sham acupuncture reduce muscle pain in myofascial pain patients. J Orofac Pain. 2002;16:71-76.
Graff-Radford S.B., Reeves J.L., Jaeger B. Management of head and neck pain: the effectiveness of altering perpetuating factors in myofascial pain. Headache. 1986;27:186-190.
Greene C., Debias D., Helig D., et al. The effect of helium-neon laser and osteopathic manipulation on soft-tissue trigger points. J Am Osteopath Assoc. 1990;90:638-639.
Gur A., Sarac A.J., Cevik R., et al. Efficacy of 904 nm gallium arsenide low level laser therapy in the management of chronic myofascial pain in the neck: a double-blind and randomized controlled trial. Lasers Surg Med. 2004;35:229-235.
Hains G. Chiropractic management of shoulder pain and dysfunction of myofascial origin using ischemic compression techniques. J Can Chiropr Assoc. 2002;46:192-200.
Hains G. Locating and treating low back pain of myofascial origin by ischemic compression. J Can Chiropr Assoc. 2002;46:257-264.
Hakguder A., Birtane M., Gurcan S., et al. Efficacy of low level laser therapy in myofascial pain syndrome: an algometric and thermographic evaluation. Lasers Surg Med. 2003;33:339-343.
Hammer W. Functional soft tissue examination & treatment by manual methods, ed 3. Sudbury (Mass): Jones & Bartlett, 2007.
Hanten W., Olson S., Butts N., et al. Effectiveness of a home program of ischemic pressure followed by sustained stretch for treatment of myofascial trigger points. Phys Ther. 2000;80:997-1003.
Hanten W.P., Barret M., Gillespie-Plesko M., et al. Effects of active head retraction with retraction/extension and occipital release on the pressure pain threshold of cervical and scapular trigger points. Physiother Theory Pract. 1997;13:285-291.
Harden R.N. Muscle pain syndromes. Am J Phys Med Rehabil. 2007;86(Suppl):S47-S58.
Harden R.N., Bruehl S.P., Gass S., et al. Signs and symptoms of the myofascial pain syndrome: a national survey of pain management providers. Clin J Pain. 2000;16:64-72.
Harris R.E., Clauw D.J. The use of complementary medical therapies in the management of myofascial pain disorders. Curr Pain Headache Rep. 2002;6:370-374.
Hayes S. A new hypothesis for consideration on the subluxation. J Natl Chiropr Assoc. 1957;27(7):9-11. 68–69
Hong C.Z. Myofascial pain therapy. J Musculoskelet Pain. 2004;12:37-43.
Hong C.Z., Chen Y.C., Pon C.H., et al. Immediate effects of various physical medicine modalities on pain threshold of an active myofascial trigger point. J Musculoskelet Pain. 1993;1:37-53.
Hou C.R., Tsai L.C., Cheng K.F., et al. Immediate effects of various physical therapy modalities on cervical myofascial pain and trigger point sensitivity. Arch Phys Med Rehabil. 2002;83:1406-1414.
Hsueh T.C., Cheng P.T., Kuan T.S., et al. The immediate effectiveness of electrical nerve stimulation and electrical muscle stimulation on myofascial trigger points. Am J Phys Med Rehabil. 1997;76:471-476.
Ilbuldu E., Cakmak A., Disci R., et al. Comparison of laser, dry needling and placebo laser treatments in myofascial pain syndrome. Rheumatol Int. 2003;25:23-27.
Itoh K., Katsumi Y., Kitakoji H. Trigger point acupuncture treatment of chronic low back pain in elderly patients—a blinded RCT. Acupunct Med. 2004;22:170-177.
Jaeger B., Reeves J.L. Quantification of changes in myofascial trigger point sensitivity with the pressure algometer following passive stretch. Pain. 1986;27:203-210.
Job analysis of chiropractic. Greeley (CO): National Board of Chiropractic Examiners; 1993:78.
Johannson A., Wenneberg B., Wagersten C., et al. Acupuncture in treatment of facial muscular pain. Acta Odontol Scand. 1991;49:153-158.
Kilkenny M.B., Deane K., Smith K.A., et al. Non-invasive physical treatments of myofascial pain (protocol). Cochrane Library. 2007.
Kisiel C., Lindh C. Smartlindring med fysikalsk terapi och manuell akupnktur vid myofasciella nackoch skuldersmartor. Sjukgymnasten. 1996;12(Suppl):24-31.
Lavelle E.D., Lavelle W., Smith H.S. Myofascial trigger points. Med Clin North Am. 2007;91:229-239.
Lee J.C., Dt Lin, Hong C. The effectiveness of simultaneous thermotherapy with ultrasound and electrotherapy with combined AC and DC current on the immediate pain relief of myofascial trigger points. J Musculoskelet Pain. 1997;5:81-90.
Lewit K. Post-isometric relaxation in combination with other methods of muscular facilitation and inhibition. Man Med. 1986;2:101-104.
Makous E. Treating temporomandibular joint disorder with unique intraoral approach. Adv Phys Ther. 1995;6:6-7.
Maljesi J., Unalan H. High power pain threshold ultrasound technique in the treatment of active myofascial trigger points: a randomized, double-blind case-control study. Arch Phys Med Rehabil. 2004;85:833-836.
Nimmo R.L. A technique for the correction of muscular imbalance of the temporomandibular joints. Granbury (TX): The Receptor. 1981;2(2):1-8.
Nimmo R.L. An open letter to the chiropractic profession. Dig Chiropr Econ. 1969;1:51.
Nimmo R.L. Development of chiropractic (video cassette). Pasadena (TX): Texas College of Chiropractic, 1984.
Nimmo R.L. Receptors, effectors, and tonus: a new approach. J Natl Chiropr Assoc. 1957;27(11):21.
Nimmo R.L. Some remarks on the development of receptor-tonus technique. Privately circulated response to Bachop. Granbury (TX): R. L. Nimmo, 1981.
Nimmo R.L. Specificity and the law of facilitation in the nervous system. Granbury (TX): The Receptor. 1971;2(1):1-8.
Nimmo R.L. Technique for the immediate release of headache and neck pain. Granbury (TX): The Receptor. 1986;2(3):1-15.
Nimmo R.L. The development of chiropractic through the perspective of Dr. Raymond Nimmo [videorecording]. Pasadena (Tex): Texas Chiropractic College, 1984.
Nimmo R.L. The receptor-tonus method course of instruction. Distributed at seminars. 1963. Included in letter to Dr. Stanley Hayes, Tucson (AZ)
Nimmo R.L. The receptor-tonus method. Pasedena (Tex): Texas Chiropractic College, 1992.
Nimmo R.L. The receptor-tonus method: directory. Self-published, 1962.
Olavi A., Pekka G., Pertti K., et al. Effects of infrared laser therapy at treated and non-treated trigger points. Acupunct Electrother Res. 1989;14:9-14.
Perle S.M. Myofascial trigger points. Chiropr Sports Med. 1995;9:106-108.
Perle S.M. Understanding trigger points: key to relieving myotogenous pain. Chiropr J. 1989;3:17.
Phillips B., Ball C., Sackett D., et al. Levels of evidence. Oxford, UK: Oxford Centre for Evidence-based Medicine, 2001.
Rehm W.S. Price of dissension: the private wars of Leo L. Spears. Chiropr History. 1991;15(1):33.
Rickards L.D. The effectiveness of non-invasive treatments for active myofascial trigger point pain: a systematic review of the literature. Int J Osteopath Med. 2006;9:120-136.
Sackett D.L., Straus S.E., Richardson, et al. Evidence-based medicine: how to practice and teach EBM. Edinburgh, Scotland: Churchill Livingstone, 2000.
Schneider M. Receptor-tonus technique assessment. Chiropr Tech. 1994;6:156-159.
Schneider M. Tender points/fibromyalgia vs trigger points/myofascial pain syndrome: a need for clarity in terminology and differential diagnosis. J Manipulative Physiol Ther. 1995;18:398-406.
Schneider M., Cohen J. The Collected Writings of Nimmo & Vannerson. J Manipulative Physiol Ther. 2001;32(1):14-24.
Schneider M.J. Snapping hip syndrome in a marathon runner: treatment by manual trigger point therapy—a case study. Chiropr Sports Med. 1990;4:54-58.
Simons D.G. Understanding effective treatments of myofascial trigger points. J Bodywork Mov Ther. 2002;6:81-88.
Simunovic Z., Trobonjaca T., Trobonjaca Z. Treatment of medial and lateral epicondylitis—tennis and golfer’s elbow—with low level laser therapy: a multicentre double-blind, placebo-controlled clinical study on 324 patients. J Clin Laser Med Surg. 1998;16:145-151.
Skootsky S.A., Jaeger B., Oye R.K. Prevalence of myofascial pain in general internal medicine. West J Med. 1989;151:157-160.
Smania N., Corato E., Fiaschi A., et al. Repetitive magnetic stimulation: a novel approach for myofascial pain syndrome. J Neurol. 2005;252:307-314.
Smania N., Corato E., Fiaschi A., et al. Therapeutic effects of peripheral repetitive magnetic stimulation on myofascial pain syndrome. Clin Neurophysiol. 2003;114:350-358.
Snyder-Mackler L., Barry A.J., Perkins A.I., et al. The effects of helium-neon laser irradiation on skin resistance and pain in patients with trigger points in the neck or back. Phys Ther. 1989;69:336-341.
Srbely J., Dickey J.P. Randomized controlled study of the antinociceptive effect of ultrasound on trigger point sensitivity: novel applications in myofascial therapy. Clin Rehabil. 2007;21:411-417.
Srbely J., Dickey J.P. Stimulation of myofascial trigger points causes systemic physiologic effects [abstract]. J Can Chiropr Assoc. 2005;49:75.
Tanrikut A., Ozaras N., Ali Kaptan H., et al. High voltage galvanic stimulation in myofascial pain syndrome. J Musculoskelet Pain. 2003;11:11-15.
Terrett A.C., Vernon H. Manipulation and pain tolerance. A controlled study of the effect of spinal manipulation on paraspinal cutaneous pain tolerance levels. Am J Phys Med. 1984;63:217-225.
Travell J.G., Simons D.G. Myofascial pain and dysfunction: the trigger point manual. Baltimore: Williams & Wilkins, 1983.
Travell J., Rinzler S. The myofascial genesis of pain. Postgrad Med. 1952;11:425-434.
Travell J., Simons D.G. Myofascial pain and dysfunction: the trigger point manual. Baltimore Md: Williams and Wilkens, 1983.
Vernon H.T., Aker P., Burns S., et al. Pressure pain threshold evaluation of the effect of spinal manipulation in the treatment of chronic neck pain: a pilot study. J Manipulative Physiol Ther. 1990;13:13-16.
Vicenzino B., Collins D., Wright A. The initial effects of a cervical spine manipulative physiotherapy treatment on the pain and dysfunction of lateral epicondylalgia. Pain. 1996;68:69-74.
Anderson R.U., Wise D., Sawyer T., et al. Integration of myofascial trigger point release and paradoxical relaxation training treatment of chronic pelvic pain in men. J Urol. 2005;174(1):155-160.
Brewer G., Kampschroeder F., Moore L. Trigger point and transverse frictional massage: a case report. Chiropr. 1990;6:40-42.
Cohen J.H., Gibbons R.W., Raymond L. Nimmo and the evolution of trigger point therapy, 1929–1986. J Manipulative Physiol Ther. 1998;21:167-172.
Crawford J.S., Simpson J., Crawford P. Myofascial release provides symptomatic relief from chest wall tenderness occasionally seen following lumpectomy and radiation in breast cancer patients. Int J Radiat Oncol Biol Phys. 1996;34(5):1188-1189.
Daniells E., Wood T. Chiropractic care protocol versus stretching in the treatment of active trigger point in the extensor muscles of the hand and fingers. Proceedings of the World Federation of Chiropractic, 7th Biennial Congress. 2003:311-312. Toronto, ON
Davies C. Trigger point therapy for carpal tunnel syndrome: self-applied massage of the forearms and scalenes. J Am Chiropr Assoc. 2002;39:18-23.
De Franca G., Levine L. Quadratus lumborum and low back pain. J Manipulative Physiol Therap. 1991;14:142-149.
Grobli C., Dejung B. Non-medical therapy of myofascial pain. Schmerz. 2003;17:475-480.
Han S.C., Harrison P. Myofascial pain syndrome and trigger point management. Reg Anaesth. 1997;22:89-101.
Hong C. Specific sequential myofascial trigger point therapy in the treatment of a patient with myofascial pain syndrome associated with reflex sympathetic dystrophy. Australas Chiropr Osteopath. 2000;9:7-11.
Howitt S.D., Wong J., Zabukovec S. The conservative treatment of trigger thumb using Graston Technique and Active Release Techniques®. J Can Chiropr Assoc. 2006;50:249-254.
Hsieh H., Hong C. Effect of chiropractic manipulation on the pain threshold of myofascial trigger point: a pilot study. Proceedings of: International Conference on Spinal Manipulation. 1990:359-363.
Hunter G. Specific soft tissue mobilization in the management of soft tissue dysfunction. Man Ther. 1998;3:2-11.
Hyde T. Graston technique: a soft tissue treatment for athletic injuries. DC Tracts. 2003. Fall
Kasunich N.J. Changes in low back pain in a long distance runner after stretching the iliotibial band. J Chiropr Med. 2003;2:37-40.
Kaye M.J. Evaluation and treatment of a patient with upper quarter myofascial pain syndrome. J Sports Chiropr Rehabil. 2001;15:26-33.
Leahy P. Improved treatments for carpal tunnel and related syndromes. Chiropr Sports Med. 1995;9(1):6-9.
Leahy P.M. Active release techniques: soft tissue management system for the upper extremity. Colorado Springs, CO: Self-published, 1996.
Leahy P.M., Mock L.E. Myofascial release technique and mechanical compromise of peripheral nerves of the upper extremity. Chiropr Sports Med. 1992;6:139-150.
Melham T.J., Sevier T.L., Malnofski M.J., et al. Chronic ankle pain and fibrosis successfully treated with a new noninvasive augmented soft tissue mobilization technique (ASTM): a case report. Med Sci Sports Exerc. 1998;30(6):801-804.
Mock L.E. Myofascial release treatment of specific muscles of the upper extremity. Part 1. Clin Bull Myofasc Ther. 1997;2(1):5-23.
Mock L.E. Myofascial release treatment of specific muscles of the upper extremity. Part 2. Clin Bull Myofasc Ther. 1997;2(2/3):5-22.
Mock L.E. Myofascial release treatment of specific muscles of the upper extremity. Part 3. Clin Bull Myofasc Ther. 1997;2(4):51-69.
Mock L.E. Myofascial release treatment of specific muscles of the upper extremity. Part 4. Clin Bull Myofasc Ther. 1998;3(1):71-93.
Mulcahy R., Johnson J., Witt R. Treatment of myofascial pain utilizing an activator instrument on trigger points. Chiropractic. 1994;9:45-46.
Schneider M. The collected writings of Nimmo and Vannerson: pioneers of chiropractic trigger point therapy. Pittsburgh (Pa): Michael Schneider, 2001.
Such G.W. Manual care of the hyoid complex. Top Clin Chirop. 2002;9:54-62. c/r
Vernon H., Schneider M. The Collected Writings of Nimmo & Vannerson. J Manipulative Physiol Ther. 2009;32(1):14-24.
Walsh M.J., Wise P. Chiropractic treatment of fibromyalgia: two case studies. Chiropr J Aust. 2001;31:42-46.