16 Facial pain and temporomandibular disorders
ASSUMED KNOWLEDGE
It is assumed that at this stage you will have knowledge/competencies in the following areas:
If you think that you are not well equipped in these areas, revise them before reading this chapter or cross-check with texts on those subjects as you read.
INTENDED LEARNING OUTCOMES
At the end of this chapter you should be able to:
PAIN OF DENTAL ORIGIN
Whilst it is not the purpose of this book to reiterate the diagnosis of common dental disorders, it is worth restating some features of these conditions to aid in the distinction from pain not caused by disease of the teeth (see Table 16.1).
Table 16.1 Distinguishing pain of temporomandibular disorders from that of dental origin
| Dental pain | Pain associated with temporomandibular disorders | |
|---|---|---|
| Site | Teeth or alveolus. Almost always unilateral | Preauricular, temple, angle of mandible. May be bilateral |
| Duration | Hours to days | Weeks to months |
| Aggravated by | Thermal stimulation or pressure on a specific tooth | Jaw movement, chewing, yawning, cold windy weather |
| Relation to time of day | No | Often yes |
In general, pain of dental origin is of relatively rapid onset (hours to days) and very well localized to the causative quadrant of the mouth or even to the tooth itself. Pulpal pain is typically worsened by thermal stimulation. Periodontal pain (apical or lateral) is associated with tenderness of (usually) one tooth to biting or to finger pressure. There are other specific features that may be sought, such as caries, loss of vitality and radiographic signs of periodontal bone loss. Even in the case of more difficult diagnoses such as cracked teeth, local signs may be elicited.
Soft-tissue disorders such as aphthous ulceration, pericoronal infection and acute ulcerative gingivitis can occasionally be confusing, but nonetheless tend to have a short natural history, or at least rapidly make themselves obvious.
It is also worth noting that studies that have attempted to distinguish dental disorders from each other on the basis of the nature of the pain have shown little success.
CLINICAL FEATURES OF TEMPOROMANDIBULAR DISORDERS
The term ‘temporomandibular disorders’ encompasses a group of conditions which can be the source of great controversy. As far as possible, this chapter will deal in fact, accepting that almost anything written may be challenged. It is the intention of the author to give enough information to allow the reader a basic understanding, sufficient to deal with those patients attending a general dental practice and to read further on the subject.
The group is recognized by one or more of three principal clinical features:
Unfortunately, each of these characteristics may take a variety of forms. This not only causes confusion for the learner but is partly responsible for the controversies concerning terminology and classification so common amongst the ‘experts’ in the field. Patients too may have considerable difficulty putting into words the experiences associated with their suffering.
Pain
Pain of muscular origin is often described as aching, but may also be throbbing or sharp, or described as ‘burning’, ‘stiffness’, ‘tightness’, ‘pressure’, ‘fullness’ or even ‘numbness’. It may be unilateral, but is the only common pain of the head and neck experienced bilaterally (Table 16.1). That may aid distinction from pain derived from third molar infection, which is rarely bilateral (at any one time). Muscular pain may be clearly localized to a ‘trigger point’ centred in one muscle (e.g. masseter), or may be less well defined in distribution in, for example, the preauricular or temporal areas.
The time scale of the pain is also important as it rarely develops to a point which causes a patient to seek help over less than a few weeks, in contrast to pain of pulpal or periodontal origin, which tends to develop over hours to days. Activities involving stretching or use of the masticatory muscles, such as chewing, yawning, laughing or singing, usually worsen the pain. Variation over time is common, with pain often being worse in the mornings, but this is by no means always so.
Pain may also derive from the TMJ itself, in which case it tends to be more localized to the joint (but is not always), may be sharp, aching or throbbing, tends to vary less during the day and is usually worsened by joint movement.
Tenderness of the muscles or joints
Sites of origin of pain are often tender to gentle palpation. Masseter and temporalis muscles are accessible to palpation over most of their surfaces. Medial pterygoid can only readily be felt on the midpoint of its anterior border (a finger can be run back along the occlusal surfaces of the teeth until it meets the muscle) or possibly where it joins the pterygomasseteric sling beneath the mandible. Access to the lateral pterygoid, however, is very restricted, it being found by passing a small finger between the maxillary tuberosity and the coronoid process of the mandible. Caution is needed in interpreting apparent tenderness of the masticatory muscles, as normal muscles may be quite sensitive to firm palpation; a major difference between the sides of the face is usually of diagnostic value.
Noises
The most common noise associated with the TMJ is clicking (or snapping, cracking, bumping or popping). The noise may be experienced by the sufferer only or may be audible to others, but is always associated with joint movement. The clinician may detect inaudible sounds by palpation or auscultation over the joints during joint movement. Often clicking is worse during eating and occasionally it is audible to others over the sound of conversation at a considerable distance.
A number of surveys have demonstrated that clicking of the TMJ is common, possibly affecting one-third of the adult population. Most people with a clicking TMJ do not ‘suffer’ from their joint noise to the point that they seek help, and that brings us to one of our difficulties. If a majority of people who have a clicking TMJ do not seek help about them, can clicking per se be regarded as an abnormality? The resolution of that question is probably beyond the scope of this book, but it is right to caution against the automatic treatment of all people with a clicking TMJ.
Other noises encountered come under the general term ‘crepitus’ and may be described by the patient as ‘grating’, ‘grinding’, ‘crackling’, ‘rubbing’ and other terms. Such noises are rarely audible to others, but again may be detected by palpation or auscultation. These noises should be clearly distinguished from clicking-type noises as they almost certainly represent different aspects of disease.
Limitation of jaw movement
This may take the form of ‘stiffness’ or pain on attempted mouth opening, thus restricting mobility. Where this is associated with muscular problems, it is often slow in onset (and recovery) and variable in severity.
Muscular stiffness should be distinguished from ‘locking’, which is very sudden in onset (and, if relieved, recovery is also instantaneous).
To determine the degree of restriction some measure of the normal, which is itself very variable, is required. A reasonable measure of the lower limit of interincisal opening for an adult with a class 1 occlusion is 40 mm, measured between the upper and lower incisal edges. The upper limit of the range is about 65 mm. However, these values should be used with caution as some normal people have measures outside this range. Lateral excursive and protrusive movements give some degree of measure of translatory movement within the joints and may be less affected than interincisal opening by muscular influences. Lower limits for these measures are approximately 7 mm. Some allowance should be made for variation in incisor relationship and for bodily size (the larger the body, the greater the opening).
A CLASSIFICATION OF TEMPOROMANDIBULAR DISORDERS
Classification of temporomandibular disorders is one area in which controversy is rife. It is worth taking a little time to consider the value of classification before suggesting a pragmatic approach to these disorders.
The setting of a variety of entities into more or less coherent groups enables rules to be drawn concerning the behaviour of these groups. As far as disease is concerned, this should allow a prognosis to be offered, specific treatments to be selected and research to be conducted, particularly to determine whether treatments are predictably successful. If a group of very different disorders is considered as if they are one condition, prognosis, treatment and research results are likely to be very confused. It is the case with temporomandibular disorders that disease is defined in terms of a wide range of over-lapping and ill-defined symptoms and physical signs, and both causes and predisposing factors are poorly understood. It should not be surprising that there remains uncertainty as to whether one, three or many conditions are being dealt with.
It is clear, however, that some distinctions can be made. Young adult patients do present with pain, muscle tenderness, variable stiffness, but no clicking or locking; similarly there are young patients with clicking and/or locking of the TMJ with no history of muscle-associated pain or stiffness; a third group is also seen with onset in middle life of joint-associated pain, joint tenderness, crepitus and radiological signs of bone loss within the joints. It is difficult to see these three ‘pure’ forms as parts of the same disorder, although ‘pure’ forms are relatively uncommon. There is also evidence that these disorders do interact with each other in some patients and some practitioners believe that there is a strong element of progression from one type to another.
At the other extreme there is a temptation to continue to subdivide and subdivide each category, which, without a clear understanding of the nature of the disorders, runs the risk of creating an unwieldy and confusing hierarchy of conditions when it cannot be certain they are all different.
The classification used in this chapter is pragmatic and based on that recommended by the American Academy for Orofacial Pain (McNeil 1993).
MYOFASCIAL PAIN DYSFUNCTION
Diagnosis
In its pure form this is a condition affecting only the muscles, though it may affect neck and scalp musculature as well as masticatory ones and is probably analogous to ‘fibromyalgia’ affecting more distant muscle groups. It is predominantly a young patient’s condition and (at least as far as hospital practice is concerned) affects women far more commonly than men. Muscles are painful, particularly during use, often particularly so in the mornings. Specific tender spots (trigger points) may be found in individual muscles, or many muscles may be tender. The condition often develops over weeks to months but with some degree of variation in severity over that time.
Mouth opening is often, but not always restricted, but interincisal opening is rarely less than 15 mm. There is usually some capacity to extend opening with passive stretching by finger pressure; this is also often accompanied by a hesitant or jerky jaw movement. Occasionally the condition appears in a severe form of rapid onset. In this case mouth opening may be restricted to a few millimetres.
The condition appears to be almost always self-limiting over a period of a few weeks to a few years, although for some patients the condition can be remarkably persistent. The cause(s) is unknown. However, several factors have been linked to it:
Almost certainly each of these factors is of some importance in individual cases, but no one factor has been shown to be consistently present in all cases, nor are all those who exhibit these features affected by myofascial pain dysfunction. This inconsistency must shed some doubt on either the causative role of these factors or the coherence of the diagnostic category, and probably implies some form of ‘susceptibility’ which as yet is not understood.
Treatment
Apparently successful treatment may take many forms. It is usual to recommend a range of conservative measures: keeping the muscles warm, minimizing chewing, analgesics (NSAIDs if the patient can tolerate them) as well as asking the patient to watch for and control daytime parafunctional activity.
A common second line is the soft vinyl mouthguard (Fig. 16.1), which, although claimed by some to worsen bruxism, does appear to work for many patients and is both inexpensive and simple to construct, requiring only one lower impression. The author recommends this appliance for night use only, for about 6 weeks: as it cannot be adjusted precisely to the occlusion, wearing the appliance 24 hours per day does result in uneven tooth movement. If it has not brought any improvement in 6 weeks, the likelihood of success is small and its use should be discontinued. Many other designs of appliance are used for this condition and it is beyond the scope of this book to review them all. The occlusally balanced or stabilization appliance is a rigid acrylic device made to fit closely into the occlusal surfaces of both upper and lower teeth when the jaw is held in a retruded position with the teeth marginally apart. It may be retained with clasps or ball cleats attached to the teeth. It can be worn all day, but there is little evidence that results are better than that achieved by night use only.

Physiotherapy of various forms has been shown to be effective in reducing pain and increasing mobility. It is, however, expensive to provide and often inconvenient for the patient because repeated visits are needed.
Antidepressant medications such as amitriptyline, dothiepin, fluoxetine or paroxetine have been used with considerable success for some patients and it has been argued that some such drugs may act more by altering the pain experience centrally than by having a direct antidepressant effect in this condition.
It is certainly worthwhile treating any obvious local causes, such as pericoronal infection affecting a third molar close to the affected muscle, or a high restoration. However, the practitioner should not undertake irreversible treatments, particularly if the factor being treated does not seem related in time to the onset of the condition.
If there are considerable signs of associated anxiety, depression or psychiatric disturbance, help should be sought from a psychologist or psychiatrist; this may generally be better done through the general medical practitioner.
DISC DISPLACEMENT WITH REDUCTION
Diagnosis
Most clicking of the TMJ has been shown to be associated with disc displacement.
Many anatomy texts show the disc within the TMJ to be superior and slightly anterior to the condylar head when the teeth are in occlusion, with the two main ridges of the disc placed one behind and one in front of the condyle (Fig. 16.2). During mouth opening the condyle rotates against the disc and the disc slides forwards and downwards along the articular eminence, but the ridges on the disc remain on either side of the condylar head (Fig. 16.3). This forward slide in the upper joint space is called translation. In general, much of the early part of mouth opening occurs as a hinge movement in the lower joint space and later in opening a greater part of the movement is translatory.
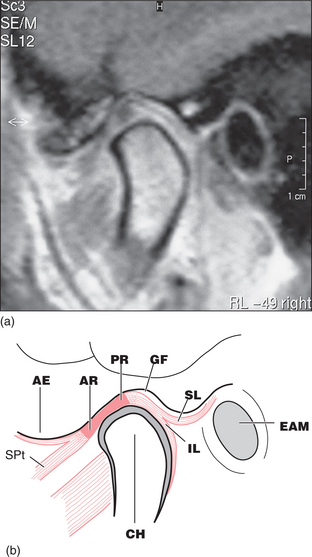
Fig. 16.2 (a) MRI of the normal disc/condyle relation, mouth closed. (b) Diagram of the same. AE = articular eminence; AR = anterior ridge of disc; PR = posterior ridge of disc; GF = glenoid fossa; SL = upper lamina of posterior attachment; EAM = external auditory meatus; IL = lower lamina of posterior attachment; CH = condylar head; SPt = superior pterygoid muscle.
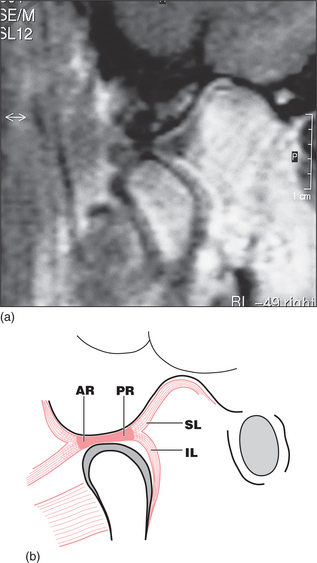
Fig. 16.3 (a) MRI of the normal disc/condyle relation, mouth open. (b) Diagram of the same. Abbreviations as defined in the legend to Fig. 16.2.
For most people with a clicking TMJ the disc is not in the position described above when the teeth are together. In these people the disc is anteriorly displaced (or anteromedially displaced). This means that the posterior ridge of the disc is actually just in front of the condyle when the teeth are in occlusion (Fig. 16.4). On mouth opening the disc displacement reduces (Fig. 16.5): the disc moves back and the condyle forward relative to each other, in a sudden movement, resulting in the click and a ‘normal’ relationship between the condyle and the disc. This anterior disc displacement with reduction has been demonstrated by cadaveric dissection, arthrography and MRI scanning as the major event associated with clicking of the TMJ. However, it is quite possible for joints without discs (such as finger joints) to click and therefore some clicks of the TMJ are probably due to other joint surface inconsistencies. When the individual with a reducing disc displacement closes their teeth together the disc is again displaced anteriorly.
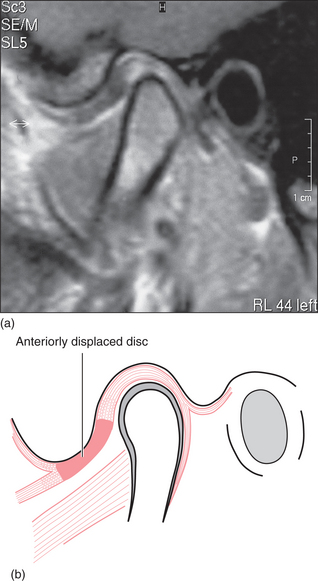
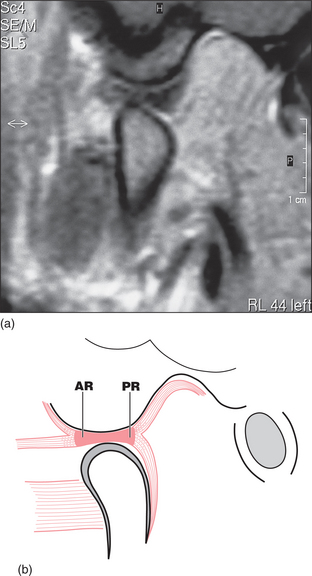
Fig. 16.5 (a) MRI showing reduction of disc displacement on mouth opening in the patient in Fig. 16.4. (b) Diagram of the same.
Often the click heard on closing is much softer than that on opening and may be imperceptible to both subject and examiner, but on occasion it may be equally loud. Clicks that occur at the same time, on both opening and closing, may be described as reciprocal.
Causes of the condition are unclear. Associations have been made with occlusal factors, parafunction and peripheral joint hypermobility, but it is not known whether any of these is strictly causative.
There is immense variation in clicking of the TMJ. At one extreme a click may be barely perceptible to the subject and cause no distress whatever. It may on occasion, however, become much louder, be heard and remarked upon by others, become uncomfortable or frankly painful, be difficult for the subject to open past, or actually lock. There is also variation in the pattern of disturbance the problem causes over time. The age of onset may be in childhood (even in those patients who seek help in their thirties or forties), but it can appear at almost any age.
Plain radiographs are of no value in determining the position of the disc. This may be done by arthrography, arthroscopy or MRI, but for almost all cases diagnosis on clinical grounds alone is quite satisfactory.
Treatment
Treatment of disc displacement disorders can be controversial. Whereas few would argue that the patient with a persistently painful joint should be offered what reasonable treatment is available, there are big differences of opinion as to the approach that should be taken to the symptomless click.
Where disc displacement with reduction appears to be the cause of suffering, it can be treated with relatively conservative methods, some of which achieve success. The anterior repositioning appliance (Fig. 16.6) is an acrylic device similar to the stabilization splint described earlier, but constructed to fit the occlusion with the mandible protruded and the teeth just not in contact. The mandible must be protruded beyond the click, so this appliance is not of value for very late opening clicks. The appliance is worn 24 hours a day for a period of 2 months. However, this results in difficulty with talking and eating and a high risk of caries beneath the appliance. It is essential that the device is removed for cleaning of itself and the teeth after any food intake. The problem appears to be what is done at the end of the 2-month period. It is common to wean the patient off the device over a period of weeks to months. Temptation to rebuild the occlusion orthodontically or with exotic restorative procedures should be resisted, as there is evidence that teeth move and bone remodels back towards the original positions after this treatment.

For many patients who present with painful clicking, however, the problem is a complex one in which a myofascial pain dysfunction and a disc displacement disorder coexist. Where muscle tone is increased, any clicking will be both louder and more difficult to get past, making the disc displacement disorder more obvious and perhaps more painful. In such cases it is worth treating the condition as if it were entirely muscular in the first instance and reassessing after a reasonable period. It is probably equally true that inflammation within the joint secondary to a damaging disc displacement disorder is likely to aggravate the local musculature.
For a few patients clicking remains a major source of distress—whether by pain, noise or sheer difficulty in getting past the click during normal activities. These will include some patients with intra-articular adhesions. For patients with resistant physical problems a surgical solution may be sought (see Ch. 17). In these cases further imaging of the disc position before irreversible treatment may be reassuring to both patient and surgeon.
DISC DISPLACEMENT WITHOUT REDUCTION (CLOSED LOCK)
Diagnosis
For those with a click, there may be no substantial change over decades (this is probably the vast majority of people with clicks) or there may be progression along one of two main paths. Intermittent painless locking may develop over months to years, with locks becoming longer and more frequent until eventually it becomes impossible to open past the click. Alternatively, joint pain is associated with the clicking, which worsens over weeks to years and leads to locking, often as a sudden event.
In these situations, the disc remains anteriorly displaced despite the patient’s best effort at opening; in other words, there is no reduction (Fig. 16.7).
If this is considered a likely diagnosis, great care should be taken to exclude restriction of mouth opening simply due to muscular activity. In general, when locked, mouth opening will be in the range 20–30 mm (hinge movement in the lower joint space permits opening of about 20 mm). Clinical tests might include determining whether opening could be increased by passive stretching (increased opening, particularly with ‘hesitation’, suggests muscular restriction) and looking for signs that translatory movement in the joint is reduced (lateral and protrusive movement, rather than opening). Imaging of the disc position by MRI is valuable.
Treatment
Conservative treatment of a true closed lock is not effective in repositioning the disc or increasing mobility. However, there are people whose TMJ discs are anteriorly displaced, non-reducing, but non-painful and associated with apparently normal mobility! Up to 50% of those who develop a closed lock eventually do return to normal, comfortable mobility, without clicking, and many more will see their symptoms improve over a few years. Unfortunately predicting which ones will improve and over what time scale is an inaccurate science.
For those with severe and persistent symptoms surgical options should be considered (see Ch. 17).
DEGENERATIVE JOINT DISEASE
Diagnosis
This condition has close parallels with osteoarthritis as seen elsewhere in the body. In general onset is in middle age. The joint(s) is generally very painful, especially on movement and is often quite tender on palpation of the lateral pole or endaurally. Limitation of movement, particularly translational movement, is often severe with interincisal opening often around 20 mm and sometimes less than that. There is often (but not always) a grating or crackling crepitus on joint movement and the patient will often describe a ‘grinding’ or ‘grating’ noise in the joint. Onset is over a few weeks and there is rarely a discrete history of symptomatic temporomandibular disorder before this event.
There is evidence that large-scale molar tooth loss may be associated with this condition, although tooth loss is so common and this condition so uncommon that tooth loss alone cannot be the cause; it is assumed that there must be some form of susceptibility.
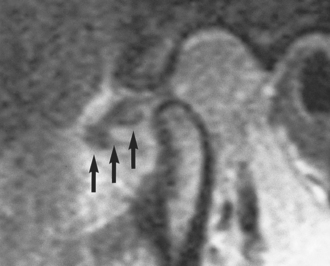
This is a temporomandibular disorder in which radiography helps to confirm the diagnosis. There may be erosion, osteophytes or traction spurs in active disease (Fig. 16.8) and marked irregularity of the condylar surface in the resolving phase.
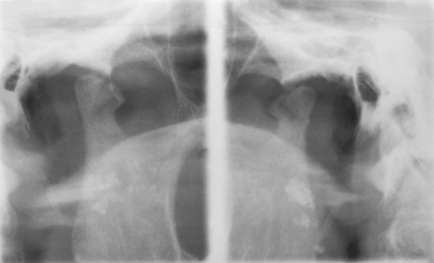
Fig. 16.8 Radiograph illustrating degenerative joint disease. Both condyles have a flattened, irregular superior surface; there is an active erosion centrally in the right condyle.
It is now recognized that the disorder has a natural history. A painful inflammatory, erosive, phase lasting up to 3 years is followed by a phase of resolution in which the bone surfaces recover and to some degree smooth out again.
Treatment
The principle of treatment is to maintain comfort with analgesics (NSAIDs if tolerated) and taking load off the joint by ensuring maximum occlusal support, while awaiting natural resolution. Note that this is likely to take many months. For a few patients it is not possible to achieve satisfactory pain relief in this way and consideration may be given to irrigation of and injection into the joint of steroids, or more invasive surgery. In general, these actions are better taken by those with experience of intra-articular procedures.
SYSTEMIC ARTHROPATHIES
The TMJ may be affected by a wide variety of systemic arthropathies. The juvenile form of rheumatoid arthritis can be very destructive, but fortunately the adult form is rarely so. Ankylosing spondylitis, reactive arthritis, gout, systemic lupus erythematosus and psoriatic arthritis are all seen in the TMJ periodically and all have the capacity to cause permanent damage to joint surfaces with loss of condylar height (Fig. 16.9). Reactive arthritis seems particularly prone to causing adhesions in the joint.

Fig. 16.9 Radiograph showing destruction of the condyle due to ankylosing spondylitis. White arrows show the sigmoid notch, the black arrows show the margin of what remains of the condyle.
Treatment of the TMJ problem is best taken as part of the overall management of the arthropathy and is therefore usually left in the hands of the rheumatologist. It can, however, be beneficial to reduce loading on the affected joint if that is possible. Sometimes surgical treatment local to the TMJ is appropriate.
ATYPICAL FACIAL PAIN AND OTHER NON-DENTAL CAUSES OF PAIN
The remaining disorders mentioned in this chapter are included primarily for purposes of differential diagnosis and to clarify what the dentist is, or is not, fitted to assist with.
Atypical facial pain
Atypical facial pain was originally a ‘dustbin’ diagnosis; that is, when all other possible causes of pain had been carefully considered and excluded, the pain was considered to be ‘atypical’. It is now recognized that the group of patients who describe this painful condition often describe a similar pattern of events and there are sufficient common features to consider this as one disorder.
The origin of the pain is often associated with an item of dental treatment, although sometimes careful questioning reveals a significant period of pain that caused the patient to seek treatment. The pain persists, despite the best efforts of the dentist, who may restore the tooth, root fill it or extract it, all to no benefit. The author’s experience is that dry socket is commonly diagnosed after extraction and that this too seems uncommonly delayed in resolution. It is not unusual for such wounds to be surgically explored without abnormal findings. There may be some brief respite in the pain but soon it is back at the same site or nearby, prompting the patient’s response that the wrong tooth has been removed and that something more must be done to put the condition right. Further local dental treatment does not bring that relief.
It is not surprising that the patient becomes frustrated by the apparent ineffectiveness of the dentist, often then migrating from dentist to dentist, and doctor to doctor in a vain search for relief.
The pain itself is variable in nature and in severity but remarkably chronic in duration, lasting for years. Indeed it is often more than a year before the diagnosis is made. In general the pain is continuous. It may be sharp, aching, throbbing, burning, with some variation in intensity over time and responds poorly to common analgesics. It is often associated with allodynia (pain experienced as a result of stimuli not normally capable of causing pain), but there are no local signs such as inflammation or discharge. The pain may also migrate from one site to another although generally it remains within the same quadrant.
There is a strong predilection for women and the more common age for diagnosis is the late forties or fifties. There is a strong association between this condition and anxiety and depression, although there has never been any proof that the psychological disturbances are causative. There is also a strong element in these patients of ‘somatization’, suggesting a mechanism by which pain might result from psychological sources. It is probable that the process of neuronal plasticity plays a role in the development and maintenance of the condition, though why these particular people are afflicted is not known.
No investigations are of great value in diagnosis, except where they actively exclude other local causes of pain. For that reason the practitioner must be on the lookout for pain that does not correspond to local disease and the pattern of poor response to treatment described above.
Treatment of atypical facial pain
Treatment of atypical facial pain may take the form of general analgesics, antidepressant therapy, referral to a psychologist or psychiatrist, transcutaneous electrical nerve stimulation (TENS) or other pain management strategies. Beware, though! Great care should be taken in treatment planning not to give the impression that the pain is in any way ‘imagined’ or not real, or that the dentist is washing their hands of a troublesome patient. These patients suffer very real pain, are deserving of proper attention and require thorough evaluation. However, also beware the opposite extreme. It is possible, by repeatedly attempting dental solutions where none will bring relief, to reinforce the patient’s belief that this is a dental condition and that the practitioner is patently incompetent, failing to cure the condition.
Three statistical rules or guidelines on chronic facial pain may be of help:
These guidelines may appear fatuous, but they can help to prevent the unwary practitioner from being pushed into unhelpful treatments and hence delaying treatments offering the best chance of benefit.
Atypical facial pain should be clearly distinguished from well-defined neurological and central causes of facial pain.
Trigeminal neuralgia
The pain of trigeminal neuralgia is experienced within the distribution of the trigeminal nerve, usually either the maxillary or mandibular division and usually unilaterally. Classically it is severe, sharp, electrical or needle-like in quality, coming in multiple short bursts, usually on light touch or gentle stimulation of a skin or mucosal surface (a trigger zone). There may be after-pain, but usually there is relief between episodes. Sometimes firm palpation of the trigger zone fails to elicit the pain.
The condition is treated with anticonvulsants, the first line being carbamazepine, but phenytoin and sodium valproate are also used successfully. The author’s view is that this condition is better managed in the longer term by a neurologist, although it is acknowledged that, provided thorough monitoring is carried out, it may be managed by a dental specialist. There has been a vogue for surgical resection or cryotherapy of the peripheral nerves in the distribution of the pain, but the pain relief these treatments bring is of relatively short duration (1–2 years). They also cause numbness which the patient sometimes finds almost as bad as the pain. Radiofrequency lesions of the trigeminal ganglion or, in extreme cases, dissection of the trigeminal nerve roots in the posterior cranial fossa appears more valuable in cases resistant to medical management.
Trigeminal neuralgia is almost exclusively a condition of the older person. Therefore, when the diagnosis is made in someone under 50 years of age, early referral to a neurologist is wise to exclude disorders such as multiple sclerosis or intracranial neoplasms.
Migraine and cluster headache
Migraine is a very common condition, but is generally a cause of headache rather than facial pain. Classic migraine associated with nausea, visual disturbance and photophobia is relatively uncommon, most migraines being what is called ‘common migraine’ which is a periodic headache without these additional features. Common migraine is thought to be of vascular origin and usually responds to prophylactic treatment with triptans (5HT1 antagonists). It is also treated with simple analgesics in many sufferers. The chief distinction to be made for the dentist is that from myofascial pain, particularly where the latter affects the temporalis muscle (or occipitofrontalis) and thus causes headache. There is evidence that some migraine responds to treatment with occlusal appliances; this is a controversial area for dental involvement.
Cluster headache is a very similar pain that may be experienced in the head and face, sometimes associated with flushing of the skin, congestion and running of the nose.
Giant-cell arteritis
This is one of very few painful conditions of the face for which early diagnosis can make a major difference to the outcome. The condition, which affects only elderly people is recognized by pain that is severe, inflammatory in type and centred over the worst affected arteries. There is a severe vasculitis, which, although it may present primarily in the head and neck region, is a systemic disorder. This is confirmed by biopsy. The superficial temporal artery, if affected, is enlarged, hardened and tender. If untreated, the risk of occlusion of the retinal arteries is high, with resultant permanent blindness: early treatment with systemic steroids is very effective in preventing this.
Referred pain
Occasionally pain in the face may be referred from more distant sites. The typical example cited in textbooks is of pain due to angina pectoris being felt in the left mandible, in addition to the more classical sites for anginal pain (centrally in the chest, at the left shoulder and down the inner aspect of the left upper arm). The author has also witnessed a patient requesting extraction of a lower left molar tooth, when the cause of pain was a left-sided spontaneous pneumothorax. Pain in the jaws may also derive from the pharynx, ear and neck.
It is beyond the scope of this book to deal in detail with all possible non-dental causes of facial pain, but dentists should be aware of the possibility that pain felt in the jaws may not be caused within their area. Great care should therefore be exercised if diffculty is being experienced in diagnosis.
Feinmann C., Harris M. Psychogenic facial pain. Part 1: the clinical presentation. British Dental Journal. 1984;156:165-168.
Feinmann C., Harris M. Psychogenic facial pain. Part 2: management and prognosis. British Dental Journal. 1984;156:205-208.
Gray R.J.M., Davies S.J., Quayle A.A. Temporomandibular disorders: a clinical approach. London: British Dental Journal, 1995.
Hall E.H., Terezhalmy G.T., Pelleu G.B. A set of descriptors for the diagnosis of dental pain syndromes. Oral Surgery. 1986;61:153-157.
Harrison S.D. Atypical facial pain and atypical odontalgia. Zakrewska J.M., Harrison S.D., editors. Assessment and management of orofacial pain. Pain Research and Clinical Management, Vol 14. Elsevier, Amsterdam, Netherlands, 2002;255-266.
Helkimo M. Epidemiological surveys of the masticatory system. In: Melcher A.H., Zarb G.A., editors. Oral Sciences Reviews No 7 Temporomandibular joint function and dysfunction III. Copenhagen, Denmark: Munksgaard; 1976:7. 54–69.
Kurita K., Westesson P-L., Yuasa H., Toyama M., Machida J., Ogi N. Natural course of untreated symptomatic temporomandibular joint disk displacement without reduction. Journal of Dental Research. 1998;77:361-365.
McNeill C., editor. Temporomandibular Disorders. Guidelines for classification, assessment and management. Chicago, IL: Quintessence, 1993.
Morris S., Benjamin S., Gray R.J.M., Bennett D. Physical, psychiatric and social characteristics of the temporomandibular disorder pain dysfunction syndrome: the relationship of mental disorders to presentation. British Dental Journal. 1997;182:255-260.
Nitzan D.W., Samson B., Better H. Long-term outcome of arthrocentesis for sudden onset, persistent, severe closed lock of the temporomandibular joint. Journal of Oral and Maxillofacial Surgery. 1997;55:151-157.
Okeson J.P. Management of temporomandibular disorders and occlusion, 4th edn. St Louis, MO: Mosby, 1989.
Okeson J.P., Bell W.E., editors. Bell’s orofacial pain, 5th edn., Chicago, IL: Quintessence, 1995.
Sarnat B.G., Laskin D.M. The temporomandibular joint. A biological basis for clinical practice, 4th edn. Philadelphia, PA: Saunders, 1992.
Schnurr R.F., Brooke R.I. Atypical odontalgia: update and comment on long-term follow-up. Oral Surgery. 1992;73:445-448.
Seligman D.A., Pullinger A.G. The role of functional occlusal relationships in temporomandibular disorders: a review. Journal of Craniomandibular Disorders. 1991;5:265-279.
Westling L. Temporomandibular joint dysfunction and systemic joint laxity. Swedish Dental Journal. 1992;Supplement 81:1-79.
SELF-ASSESSMENT
Answers on page 270.