17 Surgery of the temporomandibular joint
ASSUMED KNOWLEDGE
It is assumed that at this stage you will have knowledge/competencies in the following areas:
If you think that you are not well equipped in these areas, revise them before reading this chapter or cross-check with texts on those subjects as you read.
INTENDED LEARNING OUTCOMES
At the end of this chapter you should be able to:
MINIMALLY INVASIVE TECHNIQUES
Injection into the joint
Entry into the joint with a needle, from the skin surface, may be necessary for the instillation of steroid or local anaesthetic solution and is a prerequisite for insertion of an arthroscope as the joint needs to be distended with fluid from within.
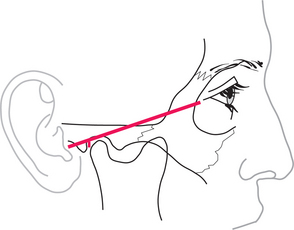
The upper joint space is most easily approached from below and behind, starting from a point 10 mm in front of the point of the tragus, just below a line that joins that point to the outer canthus (Fig. 17.1). With the mouth open, or the mandible protruded, the needle is inserted upwards, forwards and medially, until it penetrates the capsule just above and behind the condyle; this may be as deep as 2 cm from the surface. To check that the needle is in the joint, a small quantity of saline is injected then drawn back. It should be readily possible to flush fluid in and out of the joint. If no fluid can be withdrawn, the tip of the needle is unlikely to be in the joint and the position should be reassessed and adjusted. The average joint may be distended with about 2 mL of fluid.
Closed manipulation for adhesions: method and results
In cases of disc displacement without reduction, it is common that adhesions prevent the normal movement of the disc in the upper joint space. It is sometimes possible to release the lock and increase mobility by closed manipulation.
In general, pain during the procedure would be considerable if no form of anaesthesia were provided: muscle guarding in such circumstances is too powerful to permit the necessary manipulation. Local anaesthesia is often sufficient and is achieved by placing the local anaesthetic (lidocaine with epinephrine) posterior to the joint, close to the auriculotemporal nerve or in the joint itself. Patients should be warned in advance that occasionally local anaesthetic might diffuse from the site of injection to the facial nerve, giving rise to a temporary facial palsy. Should there be any weakness of the eyelids, the affected eye should be taped shut for the duration of the local anaesthetic.
It is important, after the local anaesthetic has been placed, to measure the mouth opening, in order later to be able to determine the change that has taken place. The operator stands beside the patient, who is seated and leaning slightly backwards. The operator holds the mandible, with the thumb from the opposite hand inside the patient’s mouth, resting on the posterior teeth and the fingers placed beneath the body of the mandible (Fig. 17.2). The patient’s head is held fast against the operator’s body with the other hand, the fingers of which are placed over the TMJ to feel any movement within it. The thumb is used to push down on the posterior teeth and distract the joint, then slowly the mandible is drawn forwards with increasing force until increased mobility is achieved. This often happens as one or two sudden releases. When maximum movement is achieved, mouth opening should be measured again.
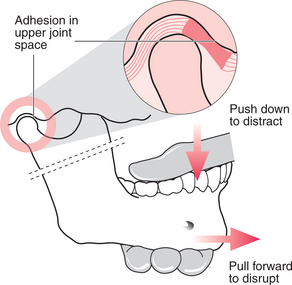
Fig. 17.2 Closed manipulation for anterior disc displacement with reduction. The thumb is placed on the posterior teeth and the fingers beneath the jaw. The joint is distracted downwards then the jaw is pulled forwards to disrupt the adhesions.
It is often possible to gain considerable mobility in closed lock by this technique. Unfortunately it can result in considerable pain over the following few days, leading to the patient moving their jaw little and the consequent reforming of adhesions. This effect can be reduced by giving NSAIDs before and after the treatment, but a considerable inflammatory exudate still remains within the joint. The pain and immobility can be eased further by irrigating the joint with saline and instilling a small quantity of steroid (see pp. 242, 245).
Arthroscopy
An arthroscope is an endoscope designed specifically for use within a joint (Fig. 17.3). TMJ arthroscopes are up to 2.8 mm in diameter and rigid. With these devices it is possible to inspect the whole of the upper joint space without formally dissecting the joint, all through a skin puncture a few millimetres in diameter.
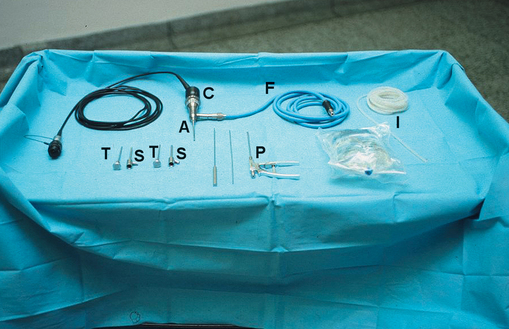
Fig. 17.3 Arthroscopy equipment. A = arthroscope; C = camera; F = fibreoptic cable; I = irrigation tubing and saline to run through; T = trocars; S = sheaths through which trocars and scope are passed; P = biopsy punch and other tools for use with arthroscope.
The joint is distended by injection of about 2 mL saline (see above). Initially the sheath is inserted through a skin puncture with a pointed but round-ended trocar inside it. This is pushed upwards, inwards and forwards until it reaches the joint capsule. At this stage the trocar may be replaced with a more round-ended one to enter the upper joint space itself. Entry into the joint is far easier if the capsule has been distended with saline and is taut. Once into the joint, the trocar is removed, leaving the sheath in place, and is replaced with the arthroscope, which is attached to the fibreoptic light source and saline for irrigation. Because there tends to be some bleeding into the joint at the point of entry, vision would rapidly deteriorate if the joint were not washed through, but at this stage there is only one portal for both entry and exit. So, now a needle (or a second arthroscope port) is placed about a centimetre further forwards and parallel to the arthroscope itself; this can act as the exit (or egress) cannula. Saline is now slowly flushed through the joint as it is examined.
The joint can be examined by direct vision, but it is more common to attach a video camera to the scope and to display what is seen on a television monitor (Fig. 17.4).
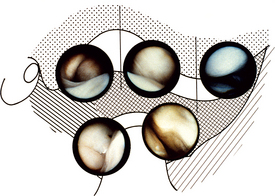
Fig. 17.4 Views of the TMJ obtained through the arthroscope. Top left = upper posterior synovial pouch; top middle = intermediate space showing disc below; top right = upper anterior synovial recess; bottom left = lower posterior synovial pouch; bottom right = lower anterior synovial pouch.
(courtesy of Dr K.-I. Murakami and Harcourt Brace Publishers)
With the simplest of equipment the joint can be inspected, usually starting with the posterior recess, looking at the position of the disc, the condition of the posterior attachment tissues and the synovium on the medial aspect of the joint. The scope is then swept anteriorly over the top of the disc to look at the anterior parts of the joint. By inspection alone it is possible to detect disc displacement, adhesions, degenerative changes in the disc and cartilage over the glenoid fossa and articular eminence and synovial inflammation. It is possible, if adhesions are detected, to replace the blunt-ended trocar and sweep around within the joint to break them down. The joint must be thoroughly irrigated at the end of the procedure and many surgeons will finally instil a steroid before leaving the joint. It is often necessary to place one suture in the skin wound.
If two arthroscope ports are used it is possible to perform surgery within the joint under direct vision. Procedures including disrupting adhesions, biopsy and smoothing roughened areas may be relatively straightforward for the expert arthroscopist, but attempts are also being made to shorten the posterior attachment tissues and reposition the disc by laser surgery. In time such procedures may become more routine.
Selection of patients is very much a matter of personal judgement. Great reliance has been placed on a failure to respond to conservative measures, with persistent pain being a central criterion. Nonetheless, if arthroscopy is intended to be therapeutic and not just a diagnostic procedure there must be some real expectation of a mechanical problem within the joint. Therefore disc displacement disorders and degenerative joint disease resistant to conservative treatments may be indications for arthroscopy, whereas painful muscular conditions are not.
Studies of the effectiveness of arthroscopy have been very encouraging, with a success rate of approximately 90%, but there have been few randomized controlled trials against conservative or more aggressive surgical treatments to allow thorough scientific evaluation. Success rates must depend upon which patients are entered into the studies, and details of patient selection in reported trials have been scanty.
Arthroscopy is a procedure associated with few serious complications. The most common problem is failure to enter the joint cleanly, or at all, although the incidence of this decreases with experience. For this reason, considerable training is recommended before independent use of arthroscopes. Poor entry into the joint results not only in physical injury to the joint capsule and/or the joint surfaces but also in greater leakage of irrigant into the surrounding tissues leading to massive swelling. Bleeding along the entry tract or into the joint is an occasional problem, but is usually readily controlled with pressure. The scope may be misdirected towards the external ear canal or upward towards the middle cranial fossa (the bone of the glenoid fossa is paper thin) or may be placed deep to the joint in the pharyngeal wall. These are serious complications and great effort must be taken with technique to avoid them.
Arthrocentesis
In view of the success of simple arthroscopy, attempts have been made to achieve the benefits without the use of extremely expensive equipment. There are several reports of great benefit from simply irrigating the joint with a considerable flow of saline.
Irrigation is best performed with two needles in the joint, placed as for arthroscopy, and can be used either alone to flush out inflammatory mediators from an inflamed joint or combined with a closed manipulation for closed lock. It is of course a ‘blind’ procedure and therefore offers little diagnostic information, and there is some risk that sharp needles within the joint over a period of an hour or more will damage joint surfaces, but it appears from clinical results that this is not a major problem.
Success rates with arthrocentesis appear comparable with those for arthroscopy for both painful non-reducing disc displacement and for degenerative joint disease, although studies of direct comparison are few and involve small numbers of subjects.
SURGICAL APPROACHES TO THE TMJ (Fig. 17.5)
Preauricular approach
The most common surgical approach by which the TMJ is entered is via a vertical incision about 3 cm in length immediately in front of the ear, extending to just below the tragus. This relatively less vascular plane gives access at its upper end to the temporalis fascia and through that to the root of the zygomatic arch. The dissection remains above the main trunk of the facial nerve and allows dissection along the zygomatic arch at a subperiosteal level, beneath the zygomatic and temporal branches of the seventh cranial nerve. The joint capsule is exposed from a posterosuperior aspect.
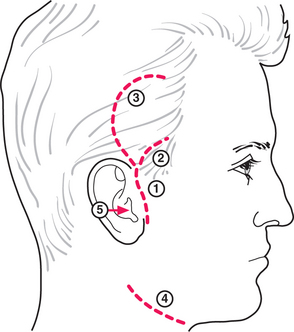
Fig. 17.5 Surgical access to the TMJ. 1. Preauricular incision; 2. temporal extension; 3. ‘question mark’ extension; 4. submandibular incision for access to the condylar neck; 5. endaural approach.
The approach is relatively simple and, provided one resists the temptation to dissect too close to the external auditory meatus (which is directed forwards as it extends inward), the risks are small. Some degree of temporary injury to the auriculotemporal nerve and the zygomatic and temporal branches of the facial nerve due to traction occasionally occurs. The incision leaves a scar on an exposed facial surface (although this is rarely unsightly).
The incision can be extended upwards and forward to give better access, or into a question mark shape to additionally minimize damage to the auriculotemporal nerve. However, most surgeons feel that the additional access gained by these extensions is of little advantage.
Submandibular approach
The preauricular approach gives good access to the joint itself, but access to the condylar neck is poor. Where such access is necessary, a submandibular approach may be made. The skin incision is usually about 5 cm in length and two finger breadths below the angle of the mandible, in a skin crease. Dissection is carried through in layers to the deep investing layer of fascia to minimize inadvertent risk to the marginal mandibular branch of the seventh nerve. Once bone is reached at the lower border of the mandible, dissection is continued at a subperiosteal plane upwards to the condylar neck. However, access is still not good.
Endaural and other approaches
Other approaches that attempt to overcome the problems of the two previously mentioned have been described. These have included entering the joint posteriorly, through the external ear canal, or by a skin incision behind the ear, folding the whole ear forwards. These may improve the visible scarring, but do relatively little for access, unless it is essential to focus on the posterior aspect of the joint and they do increase the potential for ear damage. Access to the condylar neck may be gained by an incision posterior to and nearly parallel with the posterior border of the ascending mandibular ramus, with dissection taken through parotid to masseter muscle and thence to the mandible. Access to the condylar neck is extremely good but there is an increased risk of facial nerve damage.
DISC DISPLACEMENT DISORDERS
Meniscectomy (discectomy), disc replacement or disc repositioning
For patients with persistent mechanical problems of the joint such as painful reducing or non-reducing disc displacement, or restricted mouth opening due to such disc problems it may be appropriate to open the joint surgically to reposition or remove the disc. Sometimes the disc is perforated, fragmented or so tightly tethered that it cannot be satisfactorily repositioned. Consequently it must be removed.
It has often been believed that if the disc is removed and not replaced there is an increased risk of degenerative joint disease. However, several reports of long-term follow-up of discectomy have shown few clinical signs of that. Various strategies have been employed in relation to that supposed risk. The simplest has been to accept the risk and deal with the problem if and when it arises. Alternatively, an alloplastic material such as Silastic may be placed instead of the disc. If left in the longer term this material fragments, causing multiple granulomas in the joint and a worsening problem. However, if a thin sheet is left for a period of months, a layer of fibrous tissue forms around it; this has been considered as a reasonable replacement for the disc. There is inadequate information to judge this view.
It is also possible to replace the disc with tissue, in the form of either a free graft of tissue such as dermis (from the abdomen or buttock) or local viable tissue such as temporalis fascia or muscle. The fascia tends to be rather thin and if a substantial muscle flap is brought down into the joint there tends to remain an aesthetic defect at the temple. Consideration should certainly be given to replacement of the disc if discs are to be removed from both joints, as the likelihood of developing anterior open bite is high in this situation.
Surgical access is by a preauricular approach, opening the joint capsule horizontally to gain access to both joint spaces, leaving enough capsule attached to the zygomatic arch to permit closure. The disc is mobilized and either pulled back into position, and tethered by ligating it laterally to fascia behind and lateral to the joint or is removed with or without replacement.
Disc repositioning surgery was regarded as the treatment of choice through much of the later part of the twentieth century, but it became apparent that although success in relief of pain was fairly good, the disc frequently remained malpositioned, suggesting our understanding of how such operations work was limited. All surgery to the disc within the joint carries a significant chance of failure to control symptoms.
TOTAL REPLACEMENT OF THE TMJ
With the success of replacement hip, knee and other prostheses, it is inevitable that consideration should be given to total replacement of the TMJ. Early experiences with Proplast-Teflon prostheses, however, set a very bad precedent. The surfaces of the alloplast were subject to wear, leading to loose fragments in the tissue and some very severe inflammatory reactions.
More recently, prostheses which appear to be better tolerated have been developed and the track record of the currently available prostheses is well documented. Nonetheless, total joint replacement is expensive and leaves no easy escape if the surgery is unsuccessful and symptoms continue. It should be regarded as a last resort for the few cases of true joint disease where other approaches are just not viable (such as where significant height has been lost in the condyle due to bone erosion) or where simpler surgery has been unsuccessful.
DEGENERATIVE AND INFLAMMATORY JOINT DISEASE
The recommended mainstream treatment of degenerative joint disease is conservative, as it frequently resolves spontaneously over a few years. However, in some cases pain is severe and not readily controlled by restorative and pharmaceutical approaches. In such circumstances, as a short-term measure, it may be valuable to irrigate the joint and instil a short-acting steroid (such as aqueous hydrocortisone) to reduce inflammation. Repeated use of depot steroid preparations can cause significant bone resorption and therefore is best avoided.
Now that there is good evidence that degenerative joint disease affecting the TMJ tends to have a limited period of activity, after which it tends to resolve, the role of surgery in the disorder needs to be considered carefully. If, however, there is severe bone change with roughened irregular surfaces preventing simple joint movement, operation to smooth surfaces or to interpose a soft-tissue flap between bone ends can be justified.
Where a systemic or local arthropathy has caused significant bone loss and a reduction in condylar height, an anterior open bite can result. In this situation, provided that the inflammatory process has ceased (this may be determined on repeat radiographs or by an isotope bone scan), it may be appropriate to carry out an osteotomy to lengthen the ramus or to place a prosthetic joint.
DISLOCATION OF THE TMJ
Diagnosis
Dislocation of a joint is a displacement of one component of the joint beyond its normal limits, without spontaneous return to its normal position.
Dislocation of the TMJ is a diagnosis that is simple to make and generally requires no further investigation. The history is of an event following wide mouth opening (such as yawning, vomiting, laughing, dental treatment or trauma), after which the patient can no longer close their mouth. If both joints are dislocated and the patient is dentate the mouth remains wide open, although sometimes the patient may be able to close towards a protruded position. If only one joint is dislocated there is a marked deviation to the opposite side and the teeth may be brought closer together but still nowhere near back into occlusion. For a few hours after the event there remains a depression just in front of the ear where the condyle would normally be found, but in time that fills with oedema and, although palpable, it ceases to be clearly visible. The condition is painful, may become increasingly so with time and is associated with considerable muscle guarding.
The condyle of the dislocated joint is in front of the articular eminence and the mandible is rotated downwards, leaving the posterior face of the condyle resting against the anterior aspect of the eminence (Fig. 17.6).

Treatment
The short-term treatment is manual reduction. This may be helped by local anaesthesia or sedation, but these are rarely necessary.
The author’s technique is to stand behind the patient, who is lying down on a trolley or in the dental chair, with their head at the operator’s waist level. Both thumbs are placed inside the mouth, resting on the molar teeth, with fingers of both hands beneath the patient’s chin. The operator presses down on the posterior teeth at the same time as lifting the chin occlusally. Pressure is increased steadily until the joints ‘pop’ back into place. Sometimes, if there is considerable resistance, it helps to press more on one side than the other and reduce the joints separately.
The next stage is almost as important. There is a natural tendency when the joints are reduced for the patient to immediately open their mouth wide again, reproducing the dislocation. Therefore the patient should be warned about it in advance and should keep the mouth firmly shut for about 30 seconds to a minute after reduction, only slowly easing the upward chin pressure. Redislocation is common within the first 24 hours, so patients should be warned not to open their mouth wide during this time.
Some dislocations are not repeated, but for many patients, repeated episodes of dislocation occur, despite great care. This very distressing condition may be managed entirely conservatively, either by the patient learning to avoid situations in which dislocation is likely or by training friends or family members to reduce the dislocations as they occur. For some the frequency of the events or the difficulty of reduction may warrant more active attempts to prevent further dislocation.
Some success has been reported with the injection of Botulinus toxin into the lateral pterygoid muscle. This causes prolonged muscle weakness, aimed at preventing the forward displacement associated with dislocation. It is not yet widely accepted and long-term study of its effects must be awaited. Operative surgery is the alternative.
Surgery for recurrent dislocation
Many operations have been described (this is usually a testament to a poor success rate) and it is not appropriate to deal in detail with all of them here.
The principles of their action are, however, relatively simple. Techniques fall into several categories:
All procedures have their advocates, all can be successful, all can fail and comparative success rates are not available. Selection of procedure therefore tends to be a matter of personal preference.
ANKYLOSIS OF THE TMJ
Diagnosis
The pathology of this condition is described in pathology texts, but it is worth reminding readers that ankylosis is the physical union of two bones that normally are partners in a movable joint. The union may be partial or total and either fibrous or bony (Fig. 17.7). In the TMJ the cause may be trauma (especially intracapsular fractures), infection or a systemic arthropathy such as juvenile rheumatoid or reactive arthritis.
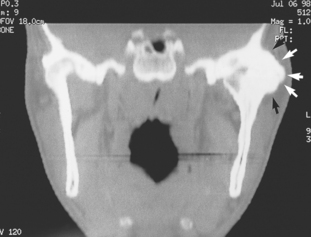
Fig. 17.7 CT scan showing ankylosis of the TMJ. An extensive mass of bone (arrows) extends around the lateral aspect of the left joint and the joint space is not visible. There is also loss of joint space in the right joint.
The principal clinical feature is severe restriction of mouth opening (no more than a few millimetres). The onset may be traced to a particular event (infective or traumatic) or it may be slowly progressive. In either event there is no relief. Investigation should include CT and/or MR imaging as well as conventional radiographs to determine the bone relationships (not only in the joint but also between the coronoid process and the zygomatic arch, maxilla and squamous temporal). Care should be taken to exclude muscular causes of limited opening and the rare hysterical reactions which do not derive from the joint at all.
Treatment
Treatment is directed either at mobilizing the existing joint, if there remains a satisfactory one, and attempting to prevent reformation of the ankylosis or at forming a false joint lower down in the mandible. Provided that the bony masses around the joint are not too extensive, particularly on the medial side (where they may encroach on the middle meningeal artery and other structures), mobilization of the joint is the preferred option.
To dissect the joint and restore its mobility may require access from both preauricular and submandibular approaches and is a time-consuming process. It is likely that both right and left joints will need to be dissected to achieve mobility and sometimes it is also necessary to section the coronoid processes to get the mouth open. Whether it is then felt necessary to interpose something (such as temporalis muscle or fascia) between the bone ends to prevent reformation of the ankylosis depends upon what is found at operation.
The construction of a false joint may be attempted at the condylar neck or lower in the ascending ramus and requires that the mandible be sectioned, the area of contact between the bone ends reduced and something interposed between the bone ends to prevent new bone formation. The construction of a false joint has the advantage of being somewhat easier to perform and with a more predictable short-term result. Its disadvantage is that hinge movement is all that can be achieved.
With surgical management of ankylosis the main problem is postoperative loss of the opening gained by surgery. Intensive physiotherapy in the form of opening exercises, which can be performed by the patient, reduces the loss but must be maintained for weeks to months. Pain relief is very important to permit therapy.
FRACTURE DISLOCATION OF THE NECK OF THE MANDIBULAR CONDYLE
Most fractures of the condylar neck of the mandible do not strictly involve the joint itself. They are of interest here because the surgical approaches to such fractures are the approaches to the TMJ and any active surgical treatment is undertaken because of effects of the fracture on the functioning of the joint (see p. 195).
In the event of bilateral fracture dislocations of the mandibular condylar neck, the elevator muscles pull the mandible up posteriorly and create an anterior open bite. If poorly treated, as many as 50% of patients with this condition are left with marked occlusal problems or persistent problems with their TMJ. Open reduction and internal fixation with plates or screws reduces the morbidity considerably.
Fractures within the capsule of the joint are more likely to result in ankylosis, but are not as amenable to open reduction and fixation.
TUMOURS
Tumours in or around the TMJ may be benign or malignant, local or secondary but are all relatively rare. Biopsy may be necessary on occasion, in which case generally the area will need to be formally dissected. Tumours here, as elsewhere, are dealt with according to their expected behaviour and extent. If resection is proposed it may be necessary to replace resected tissue with a graft, such as a costochondral free graft.
POSTSURGICAL MANAGEMENT
Mobility
Following any TMJ surgery there is a tendency for the patient to avoid opening the mouth because of pain. However, early mobilization is desirable to reduce the tendency for scar tissue formation to limit mobility in the longer term. This need for mobilization must be weighed against any likelihood that excessive movement in the early postoperative stages would place the wounds under too much strain and cause separation at suture lines.
The rate and extent of mobilization is therefore dependent upon the nature of the surgery performed. For example, following a meniscal repositioning procedure where a section of disc has been removed, mobilization should be treated with caution for a few weeks.
Active physiotherapy provided by therapists may be very helpful.
Feeding
It is also important to anticipate the patient’s inability to chew and reluctance to move their jaw by planning for a very soft or liquid diet in advance. The capacity to take in adequate food and drink should be confirmed before discharge from hospital.
Time scale of recovery
Scar tissue in the wounds develops from about 2–3 weeks onwards, gradually increasing in strength over many months. It is expected that the jaw movement will have recovered to its best level by about 2 months after surgery. If it is necessary to apply intermaxillary fixation for a period, retrieving full mobility may be much more difficult.
Complications
Surgery to the TMJ is subject to the same range of adverse events as other surgery: bleeding, wound infection, unsightly scars, etc. However, a few additional problems are specific to the site. The major complications of TMJ surgery can be anticipated from the anatomy.
Stretch injury of the branches of the facial nerve can cause weakness of orbicularis oculi, or frontalis or at the corner of the mouth. Numbness in the distribution of the auriculotemporal nerve is common.
Some occlusal disturbance is common with any intra-articular procedure, but is usually short-lived.
Injury to nearby structures such as the external auditory meatus and middle meningeal artery should be avoided but have been reported.
Probably the most irritating complication, from the patient’s point of view, is Frey’s syndrome (see also Ch. 14). This comprises flushing of the cheek or preauricular area with itching and sweating at times of gustatory stimulation (mealtimes). It is due to abnormal recovery following injury to the auriculotemporal nerve and is long lasting. Few treatments offer much relief.
Dimitroulis G. The role of surgery in the management of disorders of the temporomnadibular joint: a critical review of the literature. Parts 1 and 2. International Journal of Oral and Maxillofacial Surgery. 2005;34:107-113. 231–237.
Dolwick M.F., Sanders B. TMJ internal derangement and arthrosis: surgical atlas. St Louis, MO: Mosby, 1985.
Keith D.A. Surgery of the temporomandibular joint. Oxford, UK: Blackwell, 1988.
McCain J.P., Sanders B., Koslin M.G., et al. Temporomandibular joint arthroscopy: a 6-year multicenter retrospective study of 4,831 joints. Journal of Oral and Maxillofacial Surgery. 1992;50:926-930.
Murakami K.-I., Segami N., Moriya Y., Iizuka T. Correlation between pain and dysfunction and intra-articular adhesions in patients with internal derangement of the temporomandibular joint. Journal of Oral and Maxillofacial Surgery. 1992;50:705-708.
Nitzan D.W., Samson B., Better H. Long-term outcome of arthrocentesis for sudden onset, persistent, severe closed lock of the temporomandibular joint. Journal of Oral and Maxillofacial Surgery. 1997;55:151-157.
Rasmussen O.C. Description of population and progress of symptoms in a longitudinal study of temporomandibular arthropathy. Scandinavian Journal of Dental Research. 1981;89:196-203.
Sanders B., Murakami K.-I., Clark G.T. Diagnostic and surgical arthroscopy of the temporomandibular joint. Philadelphia, PA: Saunders, 1989.
Spruijt R.J., Hoogstraten J. The research on temporomandibular joint clicking: a methodological review. Journal of Craniomandibular Disorders and Facial Pain. 1991;5:45-50.
Takaku S., Toyoda T. Long-term evaluation of discectomy of the temporomandibular joint. Journal of Oral and Maxcillofacial Surgery. 1994;52:722-726.
Zamburlini I., Austin D. Long-term results of appliance therapies in anterior disc displacement with reduction: a review of the literature. Cranio. 1991;9:361-368.
SELF-ASSESSMENT
Answers on page 270.