CHAPTER 14 The descending tracts
Basic anatomy and function of the main descending tracts
The descending tracts originate from various regions of the brain stem and cerebral cortex and in the main synapse upon the alpha motor neurons (AMN) in the ventral horn of the spinal cord (S2.13). Ultimately, the AMN innervates various muscles to produce a motor contraction and achieve a motor goal. However, the descending tracts are not just a relay system as their influence via interneuron connections also gives precise control of motor output.
The descending tracts can functionally be divided into:
Medial
These synapse on AMNs in a ventromedial position within the ventral horn of the grey matter of the spinal cord and innervate the muscles of the neck, trunk and proximal limb girdles.
Lateral
These synapse on the AMNs in a dorsolateral position within the ventral horn of the grey matter of the spinal cord and innervate the muscles of the distal limbs.
Basic structure of a descending tract
Most descending tracts show typical features within their anatomical structure:
The precise detail of each individual descending tract is beyond the scope of this book, however the function of each tract is shown in Table 14.1. Knowledge of the basic structure and anatomical orientation (Fig. 14.1) of the descending tracts, especially where each tract decussates, is important in understanding the clinical presentation of a patient with a lesion involving the spinal cord.
Table 14.1 The basic functions of the main descending tracts
| Name of tract | Effector | Function |
|---|---|---|
| Medial corticospinal (10% of fibres) | Alpha motor neuron (AMN) of cervical and upper thoracic regions. Contralateral muscles of neck and trunk. Note: approx. 10% of fibres remain ipsilateral | Primary tract concerned with voluntary movement, specifically skilled movement |
| Lateral corticospinal (90% of fibres) | Role in fine precise movements and ability to fractionate. | |
| Lateral/pontine reticulospinal tracts | The medial and lateral tracts act together to modulate postural tone for the goal of postural stability as a background for distal movement. This is achieved by generally adjusting the level of tone and more specifically the antigravity muscles | |
| Medial/medullary/reticulospinal tracts | ||
| Medial vestibulospinal tract | AMN or indirectly via interneurons of cervical and lumbar regions. Ipsilateral. Excitatory to extensor muscles and inhibitory to flexors (neck, trunk and proximal limb) | The medial and lateral vestibulospinal tracts work with the reticulospinal tracts to govern muscle tone and more specifically extensor tone related to the vestibular system’s role in balance. Branches to the cranial nuclei (III, VI) control the vestibulo-ocular reflex |
| Lateral vestibulospinal tract | AMN or indirectly via interneuron. Ipsilateral. Excitation of extensor muscles (neck, trunk and proximal limb) | |
| Tectospinal tract | AMN of upper cervical segments. Contralateral neck muscles | Important in coordinating head movements with visual stimuli |
| Cortico-rubrospinal tract | AMN of cervical and upper thoracic region.Contralateral. Excitatory to flexor muscles and inhibitory to extensor muscles of the upper limb | Primarily supports the the action of the corticospinal tract |
| Cortico-bulbar tract | Terminate at the reticular formation on the motor neurons of cranial nuclei. Ipsilateral or contralateral | Specific function relates to the function of the cranial nuclei. |
| Cortico-olivary tract | Cerebellum. Ipsilateral | The inferior olivary nucleus plays a role in error detection and correction for learning. |
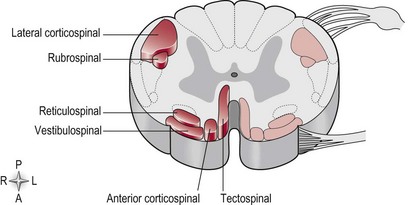
Figure 14.1 A cross-section of the spinal cord showing the orientation of the main descending tracts.
For example, a situation may arise whereby an incomplete spinal cord injury such as a spinal tumour may result in damage to a specific region. The consequent motor loss will be related to the particular descending tract or tracts infiltrated by the tumour (Fig. 14.1) and their specific function (Table 14.1). Depending on the level of decussation, the motor loss may be contralateral or ipsilateral to the lesion.