chapter 4 Psychological Aspects of Aging
Physical milestones measure a person’s age in years, but indications of mental aging are less clear. Learning about the psychological aspects of aging enhances the certified occupational therapy assistant’s (COTA’s) ability to deal effectively and empathetically with elders. This chapter explores key concepts about the psychology of aging that assist in understanding elders and enhancing empathy when working with elders.
Myths and Facts about Aging
The way elders are perceived significantly affects the way they are treated. Stereotypes are rigid concepts, exaggerated images, and inaccurate judgments used to make generalizations about groups of people. Positive and negative stereotypes create false images of aging. Western culture often perpetuates negative views of aging. Both positive and negative stereotypes can affect elders. In fact, some elders are empowered by positive stereotypes, and others are motivated to be an example of an active elder and dispel the negative stereotypes. “Seniors who are well educated, maintain a high level of health, and live in a city environment that welcomes seniors may result in individuals who are more resistant to negative characterizations. Such seniors may be the best antidote to negative stereotypes.1
Buying into the erroneous beliefs and myths of aging produces a biased negative perception of elders and colors objectivity when working with elders. “Stereotypes about aging and the old, both negative and positive, have significant influence upon the older people themselves.”2 This is a form of ageism and can deter from a realistic approach in working with elders. “Negative aging stereotypes have the power to influence reactions toward older people, creating assumptions in the midst of others about their limited or poor abilities, judgment, and behaviors.”2 Clarifying misperceptions about elders is the first step in developing effective rapport when working with this population. Consider the following myths about the psychological aspects of aging.
Myth 1: Chronological Age Determines the Way an Elder Acts and Feels
Melissa, a COTA, receives a referral to see Simone who is 89 years of age. Melissa has images of an elderly, cranky woman sitting in a chair with her head bowed, responding in a belligerent way about receiving treatment. Melissa enters the room of the assistive living center that Simone shares with her roommate Julia. The room is filled with sports mementos, photos, and awards from both of their respective grandchildren. Julia taps Melissa’s shoulder and says, “If you’re looking for Simone, she’s in the sun room teaching dance lessons. You have to get up pretty early to catch up with Simone or she’ll leave you in the dust!”
The aging process varies with each individual, and each person has different perceptions about it. Some elders do believe that their minds will deteriorate along with their bodies. Personality, lived experiences, natural responses to actual losses, expected reactions to one’s own aging process and death, and predictable emotional reactions to physical illness are separate aspects of aging. The truth is that elders are in a time of transition. Persons who are elderly should be treated as individuals and within their particular contexts, history, and circumstances. Refrain from generalizing that all elders approach aging in the same way.
For example, the stereotype that elders should avoid engaging in any strenuous exercise because their organs will fail or bones will break is a myth. Exercise is beneficial for most and dangerous for a few elders only (Figure 4-1). One study concluded that in “general elderly populations, moderate or high physical activity, compared with no physical activity, is independently associated with a lower risk of developing incident cognitive impairment after two years of follow-up.”3 Elders should check with their physician before they begin an exercise program for any limitations and recognize that the body does change in terms of stamina and flexibility in aging. It is not uncommon for elders to start exercising in later life even if they have been inactive for years.4 From a therapeutic perspective, the elder should:
 Be aware of the safety concerns of beginning to exercise
Be aware of the safety concerns of beginning to exercise
Set realistic goals and expectations
Warm up and stretch before exercising and cool down and stretch following exercise
Gradually progress to add more time or slightly more difficulty to the exercise routine
Consider strengthening as well as aerobic activity as exercise
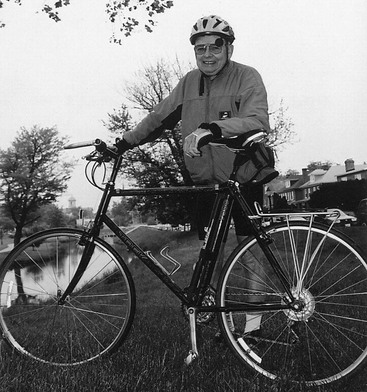
FIGURE 4-1 This elder remains physically active by regularly competing in races.
(Courtesy of Truby La Garde.)
COTAs should encourage elders to take brisk walks, consider new activities such as Tai Chi or water aerobics, and enjoy life. Increased mobility, strength, and flexibility may lead to better overall health, a decrease in fall risk, and may hold off the need for long-term care.
Myth 2: You Can’t Teach an Old Dog New Tricks
The applause is thunderous as the graduates walk across the stage. It is a very special day for both Emily and Eugenia Meyer as they receive their Bachelor of Science degrees in accounting. Eugenia Meyer is 68 years of age. Emily is her 24-year-old granddaughter. Eugenia experienced a heart attack and her granddaughter was her caregiver during her rehabilitation. Eugenia often expressed regret about not finishing college. Emily encouraged Eugenia to follow her dreams of furthering her education.
The potential of an elder should not be underestimated. One delightful example of the passion for lifelong learning can be found in Douglas’s story. Douglas, 74 years old, was married to his wife for 53 years when she passed away. He moved to a retirement community after his wife’s death. After recovering from his wife’s death, Douglas desired a new challenge. He decided to go back to school and earn a master’s degree in theology. He was concerned about the pace of school, the technology, and the way others would view him, but the concerns did not stop him from diving in. He first took a computer course for older adults and practiced his skills with his new friends at the retirement community. In his theology courses, he found that his younger colleagues valued his stories and life experiences he shared.
Douglas is not out of the norm of the capabilities of the typically aging brain. The ability to learn does not decline with age. In fact, the current number of persons older than age 55 years in noncredit continuing education courses is continuing to grow. According to Williamson,5 the desire to learn is an uppermost priority for elders. Learning strategies and preferences may differ for elderly students and their younger classmates; however, the richness in experience that elders bring to the classroom can be beneficial to all learners—“Many older adults want to participate in a learning process and become actively engaged in that process when it is interesting, relevant, and recognizes the experience they bring to the education context.”6
Crystallized and fluid intelligence must be considered in an elder learning environment. Crystallized intelligence comes from lived experiences, from which elders can tap into the wisdom gained. Fluid intelligence is new learning on the spot, such as in a classroom setting when learning a new concept. There may be increased time needed by the elder to grasp a new concept, technique, or skill. The COTA should remember that age-related changes in learning should be considered in the context that they occur and with regard to each individual, within a classroom setting, but also within the context of education when the elder is a client of occupational therapy services and must be educated on a variety of things. Education materials and presentation of the information must be modified to reflect the needs of the elder learner.
Biological changes also may affect learning. For example, elders may be unable to sit for long periods because of back or hip problems. Elders may tire quickly and demonstrate decreased physical stamina. With increased use of computers, good ergonomics with regard to the computer station will decrease fatigue and neck or back stiffness associated with sustained computer use.
As a result of poor vision or hearing skills, elders may not accurately process all sensory information. Elders may need additional time to organize and process new information. People may quickly assume that an elder is confused when the information recalled seems jumbled or inaccurate. Although there may be some cognitive decline with aging because of particular medical conditions, in many ways elders may be better learners.4 Elders can integrate life experience and a broader perspective with new knowledge that younger persons often do not consider. The COTA can make an outstanding contribution in preserving the skills and fully using the lived experiences of elders. COTAs can assist by adjusting the environment or technique of completing a task to the capacities of the elder.
Elders who feel threatened by new situations may have poor self-confidence in learning situations. New situations require decision making and risk taking. Elders may avoid learning opportunities that may result in embarrassment, frustration, or conflict. In times of stress, elders may be less flexible in problem solving and rely on set ways and habits of dealing with situations. Ultimately, the elder must want to learn, be willing to recognize any limitations, and explore other learning techniques such as keeping the brain exercised with problem-solving tasks, crossword puzzles, board games, and “neurobic” exercises (see Chapter 3 for more information on cognitive changes with aging).
Myth 3: As You Age, You Naturally Become Older and Wiser
It was most disturbing to Jerry that he could not remember what he was doing sometimes. After all, Jerry was a former professor of chemistry and retired from teaching only last year. Now his body seemed slower and his mind so forgetful. His forgetfulness started with little things like losing his keys and progressed to forgetting the road home after driving to the store. Finally, one day Jerry became upset and confused in the grocery store parking lot, unable to recall the kind of car he owned. What was happening? His daughter feared that Jerry was experiencing early stages of Alzheimer’s disease. Neither Jerry nor his daughter could understand why this was happening, especially because Jerry had always been so active and was only 63 years of age. Jerry has been an accomplished author and teacher and prided himself on his intellectual abilities.
Positive stereotyping can be as detrimental as negative stereotyping. Unrealistic expectations that elders can and should continue to perform as they did when they were younger may cause an elder to feel like a failure. Stating that all elders will be wiser or that all elders will become senile is not true. These contradictory statements prove that elders should not be lumped into one homogeneous group.
Intelligence does not decline with age. Studies done in the 1920s by Bayley and Bradway7 indicate that intelligence quotient (IQ) scores increase until the twenties, then level off and remain unchanged until late in life. Continued intellectual stimulation promotes successful aging. Staying active socially and engaged in activities make an elderly person less vulnerable to psychosocial situations.8 With aging, it is important to determine which behaviors are caused by medical conditions versus personality traits or natural aging processes.9
Myth 4: Elders Are Not Productive, Especially at Work
Initially, all the young employees at the local burger place called the new employment program “adopt a geezer.” Paul, the manager and owner of a thriving fast food restaurant located across from the high school, often came home and complained to his wife about the unreliability of many of the youth he hired to fill the shifts. Paul said that “it was as if the kids just wanted the paycheck and had no real concern about the quality of their work.”
Paul’s wife, Michelle, a COTA who worked 3 days a week at the senior citizen center, suggested a mutually beneficial program that would financially help elders who were interested and capable of fulfilling a part-time position. Paul would be able to fill shifts open during the school day with steady, reliable help.
To the amazement of the young employees, the elder employees were efficient and demonstrated stamina. In fact, the young employees often remarked, “They’re cool!”
The opportunity for young employees to work beside their older counterparts will continue to increase. Between 2000 and 2015, the number of workers age 55 years and older will increase by 72%.10 Work is not only a social or leisure pursuit of elders, but also a necessity to maintain a lifestyle they desire. The psychological adaptation to the new role of retiree can be either dreaded or embraced. For some elders, retirement is anticipated as a withdrawal from traditional, stressful workday events. They are capable of learning new skills and effectively solving problems in new situations. Upon retiring, many elders engage in social activities, community service or volunteer work, or become employed in a different line of work on a part-time basis to feel productive. According to the American Association of Retired Persons Work and Career Study, 60% of older persons plan to work in some capacity during their retirement years.11 The study also indicates that elderly workers feel undervalued at work and want the opportunity to use their skills and talents (Figure 4-2). With challenges in the economy about job security and possible discrimination against elders in the workplace, older workers may feel vulnerable. After retirement, elders often seek new areas of employment. They are capable of learning new skills and effectively solving problems in new situations. COTAs can promote integration and participation of an older worker into the job successfully by looking at adaptations to the environment, supplies, and training required to fulfill the job description. For example, an elder who would like to work in the reception area of an office may answer phones and greet customers but may need additional time and training in computer data entry needed for the job.

Retirement is sometimes a paradox when elders may have time and energy but lack financial means to be active. Conversely, when elders have the financial means and have retired from their jobs, they may desire socialization or interesting activities. According to Kielhofner (2008),23 elders may be challenged in their activity choices by lack of transportation, finances, companions, or self-limiting fears. Finch and Robinson12 believe “training older adults in how to use technology can help reduce some of the fears that limit them from adopting technologies, including assistive technology in the workplace.”13 COTAs can help retired elders create a plan for managing added leisure hours (Figure 4-3, A). Productive engagement can help elders continue to be involved in their communities. Volunteerism in the community can be a wonderful channel for leadership and organizational skills gained over a career lifetime and can be an economic and social contribution to society (Figure 4-3, B).14

Myth 5: Elders Become More Conservative as They Age
Organizing a neighborhood petition to get an overpass built over the busy street next to the elementary school was the last thing Elena thought she would be doing on her 80th birthday. But here she was in the midst of neighbors and community workers stacking flyers, affixing petition forms to clipboards, and filling out a shift schedule. For years, Elena had observed many close calls when children crossing the street were almost hit by automobiles. She thought, “I could never forgive myself if one of those kids got hurt and I just sat here and watched from my front window.”
Contrary to myth, many elders are receptive to new ideas and accept fresh roles. In fact, many elders become more politically active and even seek political office to initiate social change (Figure 4-4). According to the continuity theory, adults learn continuously from their life experiences and may pursue new interests and goals.15 Even though habits and preferences contribute to a consistency in personality, developmental psychologists note that personality may be influenced as individuals deal with crisis points in each phase of life and add to their repertoires of adaptive skills. According to Canja,16 it is untrue that elders do not want to be active, contributing members of society and that the later years of life should be reserved for idleness.

Myth 6: Elders Prefer Quiet and Tranquil Daily Lives
Jose looked around the reception area of Applewood Manor on his first day of work as a COTA. Only the sounds of a television murmuring the chant of a daily game show and the shuffling of residents down the hall broke the silence. The head nurse, Mrs. Kessler, walked up to Jose and said, “Isn’t it wonderful how quiet and peaceful it is here? We work very hard to preserve a sense of tranquility in the sunset years of one’s life.”
Jose interviewed all of the residents during the week to determine activities he could develop based on their interests. Not surprisingly, more than half of the residents wanted less sedentary activities than they currently were experiencing. Some even wanted organized sports like tennis. Other residents wanted a piano and perhaps a jazz hour scheduled.
Another incorrect generalization is that all elders prefer a sedentary lifestyle. An elder who has experienced a rather staid and uneventful life before retirement will not necessarily continue that type of lifestyle. Elders often move in with their children’s families, and their lives may become rather frenzied (Figure 4-5). Some pursue totally new interests that they may not have had time for earlier because of career and family demands. Many elders continue with vibrant lifestyles and do not sit awaiting death. Staying active is a key to healthy psychological aging.

Myth 7: All Elders Become Senile
The expression “senior moment” infers to an idea that as one ages, memory lapses become commonplace. Harry has always been a proud, independent man. He was decorated twice during his participation in World War II. After experiencing a heart attack, Harry adjusted to the many lifestyle changes that were suggested by the health care team. Today Harry sighed as he walked with multiple pieces of paper toward the receptionist in the Occupational Therapy department. This was the third stop in a confusing, mazelike journey inside the Veterans’ Administration Hospital. The hospital was under reorganization again, and procedures for appointments had changed. Previously, Harry always called for an appointment, showed up characteristically 10 minutes early, and cheerfully greeted the young COTA who assisted with the treatments. Today a young man at the front desk rattled off multiple instructions about the new procedures and handed Harry a photocopied map of the building along with a stack of new forms to be completed. Harry was still trying to understand the map when he asked the young man to slowly repeat the instructions. The young man repeated himself in a louder tone and pointed Harry in the direction of the elevators. The young man muttered, “These senile old guys.”
When elders appear confused or require more time to understand directions, misunderstandings often result. Getting older is not synonymous with feeble-mindedness or imbecility. Brain damage may be evident as a result of physical illness. However, senility is a label often used inaccurately to describe specific psychosocial disorders that elders may be dealing with, such as depression, grief, anxiety, or dementia. People age at different rates. Evidence points to the connection between engagement in physical exercise, a leisure time activity, and the overall health of older adults.”17
Stressors, Losses, and Emotions Associated with Aging
Elders often must deal with major life crises such as retirement, loss of spouse, economic changes, residence relocation, physical illness, loss of friends, and the reality of mortality. There are predictable shifts that occur in occupational patterns across the life span in regard to developmental processes and life stages.18 The significant occupational shifts or changes in meaningful activities, associated with aging may include dealing with financial burden, emotional losses, variance in roles, adapting to different routines and habits, diminishing physical and mental performance, and challenges to adaptation.18,19,20 Lieberman and Tobin21 found that “events that lead to loss and require a major disruption to customary modes of behavior seem to be the most stressful for elders.” Hayslip22 identified the following personal factors that may influence stressors: flexibility, recognition of personal needs and limits, internal locus of control, perceived family support, and willingness to acknowledge feelings about death and dying (Box 4-1). More recent studies have attempted to measure other aspects of life events and stress levels. COTA s must consider the ways various life events affect elders to understand what motivates certain behaviors.
BOX 4-1
Stressors that Affect Elders
Moving to live with family members
Relocation to a nursing home because of illness
Chronic conditions that reduce mobility or self-care
Data from MacDonald, K., & Davis, L. (1988). Psychopathology and aging. In L. Davis & M. Kirkland (Eds.). ROTE: The Role of Occupational Therapy with the Elderly. Rockville, MD: American Occupational Therapy Association.
According to Kielhofner,23 role changes can sometimes be involuntary, such as the unexpected death of a loved one, and elders struggle with the loss or diminishment of accompanying roles. Elders may need to adapt to shifts in occupational patterns possibly related to atypical or unpredictable life events and developmental aging. For example, unexpected economic demise of a company may lead to the unforeseen loss of a job and retirement funds. This significantly impacts a person’s occupation, inherent roles, and habits.
Need for Social Support
Pivotal to the ability of an elder to cope with a major life change is the social support of family, friends, church members, and neighbors. Although stressors may not be avoided, social support can help elders deal with losses.
The support an elder receives with the death of a loved one often diminishes to a large extent after the funeral or mourning period. The reality of the loss may not occur until later, when the elder is alone. The survivor may grieve over the loss of finances and possible change in residence, social status, or role associated with the death of the loved one. COTAs can assist the surviving spouse in adjusting to new roles, habits, and routines, as well as developing a strong network of social support.
Loneliness is a form of emotional isolation. Elders may experience increased social isolation with retirement, as family members relocate or as friends move or die. Social interactions with pets, weekly church services, grocery shopping trips, or occasional visits from family members may not be emotionally fulfilling enough for an elder. COTAs can assist in exploring and structuring more frequent or new areas of social interaction in the community. Community centers offer a variety of activities such as cooking and art classes, trips to local attractions, and classes specifically designed for grandparents and grandchildren to attend together.
Elders may become reclusive and socially paralyzed with anxiety as a result of increasing neighborhood violence. Intensifying anger is a common emotional problem experienced by many elders as they feel a loss of control over their lives. Elders may be viewed as cantankerous or verbally aggressive when in fact they may be using angry words to express feelings of helplessness. This anger also may be founded on fear and sadness over losses.
Other changes in environment such as new living arrangements, whether imposed or by choice, also may be a challenge for elders. According to Kielhofner,23 elders develop habits sustained over a long period often in a stable environment; when the environment changes, demands to shift habits are stressful. Or the physical or mental ability to sustain previous habits in a new environment also may be diminished.
Physical Illness
Elders may need to cope with a chronic disease or a serious physical illness. A serious physical illness with a sudden onset may be more debilitating to the elder in terms of independence and self-care. A chronic illness is no less stressful; however, the elder may have adapted to the illness more gradually. Box 4-2 lists stressors associated with common physical illnesses of elders.
BOX 4-2
Stressors Associated with Physical Illness Common to Elders
Adapted from Davis, L. (1988). Coping with illness. In L. Davis L & M. Kirkland (Eds.). ROTE: The Role of Occupational Therapy with the Elderly. Rockville, MD: American Occupational Therapy Association.
Petra, an 81-year-old woman, who was legally blind, was receiving occupational therapy services in her home. She lived by herself in a cozy one-bedroom apartment. Petra was known to the home health care team to be quite rude; in fact, she had “fired” several home health nurses and therapists that had come to provide services for her in her home. The occupational therapist asked the COTA to see Petra one Saturday for her. Petra was on Rodney’s caseload. Almost immediately after Rodney introduced himself, Petra told him she never met a health care worker that could think for themselves. She continued to insult his profession and his coworkers. Rodney tried to understand more about Petra and to find out reasons for her behavior. He learned from her past medical history that Petra’s blindness has become progressively worse. In fact, she stopped leaving her home all together because she was embarrassed that she could not fix her hair and makeup the way she used to. Rodney took the time to speak to her about this and to offer suggestions for how he could assist her in being able to do those again. He was the first person to look beyond her sarcastic remarks and rude exterior and notice that she was really scared and confronting her own mortality. Rodney continued to see Petra and work with her on coming to terms with her blindness and need for assistance. He felt that he made a difference in her life. He shared his experience with other members of the health care team so that they, too, could better understand Petra.
An elder person copes with physical illness through a psychosocial process. A negative perception of the situation and a hopeless attitude will adversely affect the way a person deals with the illness. Cohen and Larazus24 pointed out that those elders who view a physical illness as a challenge cope better than those who view it as a punishment.
A grief process in dealing with any illness is to be expected. Five stages to the grief process originally identified by Kubler-Ross25 continue to help health professionals better understand and help their clients: denial, anger, depression, bargaining, and acceptance.26 This grief process may not be linear—that is, the elder may become depressed and then become angry or deny the situation again before accepting the illness.
An elder’s ability to adapt is contingent on physical health, personality, life experiences, and level of social support.9,27,28 To successfully deal with a chronic condition, an elder should adopt the following important concepts:
Recognize permanent changes such as diet, lifestyle, work habits, or exercise that may promote recovery
Mentally deal with losses caused by the illness
Identify and express feelings such as anger, fear, and guilt
Seek out and maintain social support from family and friends
COTAs can help an elder deal with a chronic illness in the following ways:
Reduce fears about the illness through education
Listen and be sensitive to the feelings expressed verbally and nonverbally
Assist in the development of creative yet realistic ways for elders to gain more control over their illnesses or losses associated with an illness
Identify ways to reduce stress and to promote social support
Surround the elder who has moved to a nursing care facility as a result of the illness with familiar objects, which may help maintain a sense of continuity, provide comfort and security, and aid memory
Learned Helplessness
When elders perceive that they have no control over a particular outcome or multiple stresses in their life, they may give up hope and become dependent on others to fulfill their needs.29 A person with an external locus of control frequently feels powerless over decisions and actions, and the more this belief is reinforced, the more likely that learned helplessness occurs. Elders who experience loss of control also experience diminishing coping skills and are at risk for illness.19,20 Health care workers and family members often contribute to this state of learned helplessness in the following ways:
Expecting elders to be unable to do for themselves and completing tasks for them, thereby promoting dependence
Imposing routines on elders for the sake of convenience, such as giving them a bath at 2:00 p.m.
Showing a negative attitude by making condescending remarks about physical appearance or behaviors
Perpetuating the sick or institutional role by validating somatic complaints or disapproving decisions
Learned helplessness often results when the elder believes a situation is permanent, and then depression and a marked lack of self-esteem follow. COTAs can encourage independence and self-care activities. As elders regain a feeling of competence, learned helplessness can be reversed. Robnett and Chop9 suggest giving choices and options as much as possible and to challenge the client to work at a greater level than currently functioning. The concept of the client advocating for herself or himself enhances personal control in everyday life and should be integrated into daily therapy. COTAs can empower elders by creative problem solving to assist the elder in being as independent as possible.
Sena is an 88-year-old woman who is in a skilled nursing facility after falling at home. Shannon, the COTA, works with her daily and is aware of what Sena can and cannot do physically by herself. She continues to be fed because she is just too tired. Shannon knows that she can feed herself, and may well be tired, but does not oblige her request. While documenting later that afternoon, Shannon sees Sena’s son eating dinner with her, and he is feeding her with a spoon. The COTA observes the interaction but does not say anything to Sena’s son. The next evening Shannon observes the same scenario and decides to address the situation with Sena’s son and explain to him that his mother is able to feed herself. Shannon is respectful of him but talks to him about learned helplessness and what he can do to help his mother. The COTA must relinquish some of the power and control as a health care advocate and empower the elder and their family members to engage in independent problem solving. One of the key concepts in preventing learned helplessness is for the COTA to be aware of his or her own beliefs about aging and mortality and to consider stereotypes that may bias attitudes toward working with elders.
Conclusion
Old age can be a time of self-reflection and exploration of new interests. It also can be a time of dealing with great losses and severe stress. Changes occur throughout the life span, and the way a person copes with changes and adapts to transitions ultimately determines his or her ability to psychologically cope with aging. Keeping active can help minimize the effects of the aging process. By clarifying assumptions and myths about aging, gaining awareness of the different stressors and losses associated with aging, and understanding the ways elders cope with serious illnesses, COTAs can help elders enhance their quality of life as they experience aging.
Case Study
Margaret, 79 years of age, sits in the sun porch clutching a pot of orchids. This is the last day she will enjoy this scene because today Margaret is moving to an assisted living facility in a town 260 miles away, which is close to her son John. Margaret had lived in this home for almost 35 years with her husband Phillip. When Phillip died 2 years ago of pancreatic cancer, it was a shock almost too great for Margaret to bear. Phillip had been her rock. Margaret had been Phillip’s primary caretaker while he was ill. During their 40-year marriage, Margaret and Phillip had traveled all over the world and shared lifelong interests, including cooking, golf, and cultivating orchids in their custom built greenhouse. Margaret had been a volunteer with the children at the homeless shelter downtown until Phillip required her full-time care. The walls in their den were covered with awards and letters of appreciation for her work with the children. Now the house has been sold and many of her mementos have been packed up, sold, or given away.
Margaret had been an energetic high school history teacher and Phillip had been a chemist. They had two children, John and Karen. Karen is married and lives in London with her two daughters. Margaret and Phillip loved to travel to London to visit their grandchildren. John is recently divorced and is busy managing his new safety consulting company. Margaret has a beloved 9-year-old Labrador retriever named Henry, but she is unable to take Henry with her to the assistive living facility.
In the last 3 years, Margaret has been diagnosed with arthritis, vertigo, and early stages of dementia. Margaret fell 6 months ago and fractured her hip. She had begun to forget things such as paying bills, which caused her electricity to be turned off; leaving the stove on, which caused a small fire; and not remembering to take her medication regularly. John and Karen decided it was time to move their mother into a safer, more supervised environment. Margaret became depressed and less active after the decision was made. It seemed as if Margaret resigned herself to a situation beyond her control physically and socially. Margaret spent much of her time sleeping or sitting in the sun porch staring out the picture window. Moving to the new town meant saying goodbye to friends, relatives, and her beloved pet, as well as Phillip.
Case Study Review Questions
1. Identify the losses Margaret has experienced.
2. Describe the stressors or emotional problems that may be related to these losses. What impact would this have on her occupations? Describe shifts in occupational patterns that are linked to the changes in her life. Consider changes in roles, habits, routines, relationships, work, and leisure interests and activities.
3. Discuss what the COTA could do to help Margaret deal with these losses in terms of attitude, education, and activities.
Exercises
The following are a few activities to help the COTA gain empathy and rapport with the elderly.
Into Aging
“Into Aging” is a commercially available game that focuses on building empathy for those who are growing old. The manual describes the game as a way for players to increase awareness of elders’ problems by simulating experiences with similar problems, such as loss, isolation, powerlessness, dependency on others, and ageism. This game is available through Slack, Inc. (Thorofare, NJ).
Role Playing
Role playing is a useful activity for groups to understand aging-related issues. In preparation for the activity, each of the myths of aging discussed in the chapter should be written on index cards. Each small group will be given a set of index cards. Members of each group then enact some of the myths and stereotypes associated with the psychological aspects of aging. Each example should be followed with a discussion of feelings and thoughts about the stereotype or myth. What misconceptions did you have about aging before the activity that was subsequently clarified? What concept or concern is still puzzling or needs further exploration? How can you use the information learned in the role play in occupational therapy practice?
Stereotype Exercise
Each member of a group should list the first six or seven images that immediately come to mind with the word elder. Group members should think about advertisements, movies, and personal experiences that influence their perceptions of elders. Each member should share the images with the group and explain the reasons the images are so vivid. All group members should discuss whether the images are realistic or stereotypical. Discuss how these stereotypes may bias the way a COTA would approach treatment with elders or with caregivers. Group members should brainstorm different ways to change stereotypical images to make them more realistic.
Field Trip Imagery
Place yourself comfortably in a quiet room. You may sit in a comfortable chair or lie down. Take three deep breaths. As you exhale, clear your mind of any concerns and concentrate on the directions. Give yourself permission to use the next 10 to 15 minutes to explore what it would feel like to be 75 years old.
Pretend that you are looking into a large mirror. Imagine your physical appearance at age 75 years. What physical changes have taken place? Do you need any assistance with self-care? What emotions are you experiencing as a result of these changes?
What changes have occurred in your living arrangements? Do you live alone? Identify any changes in lifestyle as a result of finances.
What have you accomplished in your life thus far? Do you regret any events? Do you regret not achieving certain goals? Are you satisfied with your life?
Remember what you have just experienced with the visual imagery. Now slowly count to 10. As you get closer to 10, you will become more awake and tuned to the sounds of the room you are in. When you reach 10, gently open your eyes.
Free write for the next 5 minutes. It may be poetry, prose, or just phrases of what you remember of your visual imagery trip to age 75. Reflect on what key concepts of aging were apparent in the imagery. Describe your feelings.
Resources
Older adult resources for mental health and wellness are available through Wellness Reproductions & Publishing, LLC (a Guidance Channel Company). This is a wonderful compilation of books, music cassettes, games, products, and tools to help those who work with the elderly deal with stress, aging, caregiving, and other challenges of older adults.
1. Does chronological aging determine psychological aging? Discuss your position.
2. Identify aspects of aging that may affect learning for elders.
3. Coping with a serious illness can be especially stressful for an elder. Discuss any resulting occupational shifts and what a COTA can do to help elders understand change.
4. What is learned helplessness, and what can COTAs do to help elders vulnerable to learned helplessness?
1 Horton S., Baker J., Pearce W., Deakin J. Immunity to popular stereotypes of aging? Seniors and stereotype threat. Educational Gerontology. 2010;36(5):353-371.
2 Bennett T., Gaines J. Believing what you hear: The impact of aging stereotypes upon the old. Educational Gerontology. 2010;35:435-445.
3 Etgen T., Sander D., Huntgeburth U., Poppert H. Physical activity and incident cognitive impairment in elderly persons. Archives of Internal Medicine. 2010;170(2):186-193.
4 Tufts University. You can’t teach an old dog new tricks and other myths about the aging process. Tufts University Health & Nutrition Letter. 2002;20:1-3.
5 Williamson A. Gender issues in older adults’ participation on learning: Viewpoints and experiences of learners in the University of the Third Age (U3A). Educational Gerontology. 2000;26:49-66.
6 Bonder B.R., Dal Bello-Haas V. Functional Performance in Older Adults, 3rd ed. Philadelphia: FA Davis; 2009.
7 Teichner G., Wagner M. The Test of Memory Malingering (TOMM): Normative data from cognitively intact, cognitively impaired, and elderly patients with dementia. Archives of Clinical Neuropsychology. 2009;24(3):455-464.
8 Bergua V., Fabrigoule C., Barberger-Gateau P., Dartigues JF. Preferences for routines in older people: Associations with cognitive and psychological vulnerability. International Journal of Geriatric Psychiatry. 2006;21(10):990-998.
9 Robnett R., Chop W. Gerontology for the Health Care Professional, 2nd ed. Sudbury, MA: Jones and Bartlett; 2010.
10 Dohm A., Shniper L. Occupational employment projections to 2016. Monthly Labor Review. Retrieved June 10, 2010, from. http://www.bls.gov/opub/mlr/2007/11/art5full.pdf, 2007.
11 American Association of Retired Persons. Staying ahead of the curve: The AARP work and career study [WWW page]. URL http://research.aarp.org/econ/multiwork.html, 2003.
12 Finch J., Robinson M. Aging and late-onset disability: Addressing workplace accommodations. Journal of Rehabilitation. 2003;69(2):38-42.
13 Gupta J., Sabata D. Maximizing occupational performance of older workers. OT Practice. 2010;15(7):1-8. CE
14 Gonzalez E., Morrow-Howell N. Productive engagement in aging-friendly communities. Journal of the American Society on Aging. 2009;33(2):51-58.
15 Atchley R. Continuity and Adaptation in Aging: Creating Positive Experiences. Baltimore: Johns Hopkins University Press; 1999.
16 Canja E. Aging in the 21st century: Myths and challenges. Executive Speeches. 2001;16:24-27.
17 Simone P., Haas A. Cognition and leisure time activities of older adults. Osher Lifelong Learning Institute. 2009:22-28.
18 Royeen C. The human life cycle: Paradigmatic shifts in occupation. In: Royeen C., editor. The Practice of the Future: Putting Occupation Back into Therapy. Bethesda, MD: American Occupational Therapy Association, 1995.
19 Hays P., Bernstein I. The Hayes and Lohse Depression Scale: Validity evidence. Clinical Gerontologist. 2001;24(1-2):39-54.
20 Metcalfe J,. Metacognition of agency across the lifespan. Cognition. 2010;116(2):267-282.
21 Lieberman M.A., Tobin S.S. The Experience of Old Age. New York: Basic Books; 1983.
22 Hayslip B. The Aged Patient: A Sourcebook for the Allied Health Professional. St. Louis: Mosby; 1983.
23 Kielhofner G. A Model of Human Occupation: Theory and Application, 4th ed. Baltimore: Lippincott Williams & Wilkins; 2008.
24 Davis L. Coping with illness. In: Davis L., Kirkland M., editors. ROTE: The Role of Occupational Therapy with the Elderly. Rockville, MD: The American Occupational Therapy Association, 1988.
25 Kubler-Ross E. On Death and Dying. New York: Macmillan; 1969.
26 Kubler-Ross E., Kessler D. On Grief and Grieving: Finding Meaning of Grief Through the Five Stages of Loss. New York: Scribner; 2007.
27 Higgins L., Mansell J. Quality of life in group homes and older persons homes. British Journal of Learning Disabilities. 2009;37(3):207-212.
28 Taylor M. Involvement in occupations among older adults with physical and functional impairments is influenced by positive belief and a sense of hope. Australian Occupational Therapy Journal. 2003;50(2):111-122.
29 Punwar A. Elder care. In Punwar A.J., Peloquin S.M., editors: Occupational Therapy Principles and Practice, 3rd ed, Philadelphia: Lippincott Williams & Wilkins, 2000.