chapter 13 Use of Medications by Elders
1. Identify factors that predispose elders to adverse drug events, and discuss strategies to detect medication problems.
2. Define polypharmacy and identify recommended interventions to diminish drug-related problems of polypharmacy in elders.
3. Identify classes of medications commonly associated with adverse drug reactions in elders.
4. Identify and describe skills needed for safe self-medication.
5. Apply the OT Practice Framework: Domain and Process, second edition, to analyze self-medication for individuals with various conditions.
6. Explain the ways that adaptive devices compensate for skills needed for safe self-medication.
7. Describe elder and caregiver education needs regarding self-medication.
self-medication, over-the-counter, polypharmacy, adverse drug reactions, side effects, drug interactions
Ashley is a certified occupational therapy assistant (COTA) working in a skilled nursing facility 3 days a week. Her time for seeing the residents is dependent upon the needs of the facility. One of the residents she follows is Anna, a 79-year-old woman with a history of a recent stroke, high blood pressure, depression, and insomnia. Ashley has noticed changes in Anna’s alertness and behavior, based on the time of day that she is seen for intervention. When Ashley follows Anna in the morning, she seems very tired, unfocused, and often complains of dizziness. Ashley has found such morning therapy sessions to be less productive toward meeting Anna’s intervention goals. When she sees Anna in the afternoon, she seems to be almost a completely different person, exhibiting much more energy and enthusiasm to do intervention tasks. Ashley began to question the inconsistency of Anna’s behaviors. Could Anna be experiencing poor sleep, resulting in the morning fatigue? But why the dizziness? Is Anna more depressed? If that is the case, why does she seem to be in a much better mood in the afternoon? Ashley also questions whether the behavioral differences could be related to the medications that Anna is taking. Ashley decides to consult with the treatment team about Anna’s inconsistent behavior and her dizziness.
The other health care practitioners on the treatment team are a physical therapist, a nurse, a speech therapist, and a pharmacist. There is much discussion about Anna because other members of the treatment team have noticed her inconsistent behavior, too. Some members suggest asking for lab work to review lab level values. The pharmacist, Roger, looks at Anna’s medications and points out a possible correlation between the timing and the dosages of the medications with the behaviors that Anna is exhibiting. He questions whether Anna is experiencing some common side effects from the medications that she is taking and informs the team that he plans to consult about Anna’s medication with her physician. The following week when Ashley follows Anna for the morning intervention sessions, she is much better focused. Ashley learns that as a result of the team meeting, Anna’s medications were readjusted.
COTAs often work with elders on a daily basis in a variety of treatment settings. Because COTAs spend a considerable amount of time with the elder population, they are a valuable asset in addressing medication routines. COTAs also may convey vital information regarding medications and side effects to the health care team. When specific medication information is required, advice should be sought from a pharmacist or other medication expert. Common medications and medication-related problems encountered by elders are discussed in the chapter. Skills for self-medication and intervention programs for elders and caregivers are also discussed.
Factors Affecting Medication Risk in Elders
Elders consume the majority of prescription and over-the-counter (OTC) medications in the United States. Because of the aging population and individuals are living longer, often with chronic diseases that require medication therapy, it is no surprise that over 40% of elders in the community take at least five prescription medications.1 When OTCs are included, the number of medications consumed per day often exceeds 10 or more. It is important to note that natural products (such as health foods, supplements, and vitamins) may also be consumed by this population. Yet because they are erroneously not considered medications by some, they may not be reported when an elder is questioned about medication use.
Polypharmacy
Several components contribute to the incidence of polypharmacy (use of multiple medications in a single individual). Sometimes the use of many medications is the right thing for patients to control their diseases and ensure a better quality of life. However, there are risks associated with polypharmacy. Drug interactions happen with increased frequency the more drugs that a person consumes. These interactions may include the increase or decrease in effectiveness of one drug caused by another or a more pronounced manifestation of an adverse event due to the elder taking two drugs that have a similar side-effect profile. In addition, sometimes new medications are introduced for the specific reason of offsetting a troublesome effect caused by another. Providing new medications may be appropriate, but this scenario often occurs because the problem is not recognized as drug-induced. Risk factors that contribute to polypharmacy include the use of multiple physicians with different specialties who may prescribe similar medications, the use of multiple pharmacies, inappropriate medication reconciliation upon discharge from the hospital, and the fact that elders often have multiple conditions requiring medication therapy.
Physiology and the Aging Process
Many factors are involved in the increased incidence of medication-related adverse events in elders. With aging, kidney and liver functions decline. Many medications are excreted by the kidney and metabolized, or degraded, by the liver. Therefore, changes in organ function may frequently lead to drug accumulation in the body. This accumulation may result in toxic levels of drugs. To avoid drug accumulation, it is imperative that consideration be given to modifying doses for older individuals.
Although not all of the reasons are well understood, older persons tend to be more sensitive to the effects of certain medications. Body composition (lean tissue to fat ratio) changes as we age. Changes in body composition may result in alterations in how the body distributes a medication, making more or less of the drug available to have an effect. This is true for both the desired effects and for unwanted side effects. The adage “start low, go slow” should generally be used when initiating a new medication therapy in an older person.
Elder Medication Use and Implications for the COTA
When medical records are available, COTAs should always check the medication section to determine which medications are being used. This information helps COTAs be aware of possible side effects and drug interactions that might be observed with clinical intervention. COTAs should contact the elders’ physicians and pharmacies with any medication-related concerns or questions. (Common drug-related abbreviations and definitions are listed in Table 13-1. Medications commonly used by elders are listed in Table 13-2. Note that this is not an all-inclusive listing of medications used by elders or those that may contribute to side effects. Only generic names are listed, and they should be cross-referenced with trade names when necessary.)
TABLE 13-1 Common Drug-Related Terminology
| Abbreviations | Definitions |
|---|---|
| PO | By mouth |
| IM | Intramuscular |
| IV | Intravenous |
| SC or SQ | Subcutaneous |
| PR | Rectally |
| SL | Sublingually (under the tongue) |
| QD or Q Day | Once a day |
| BID | Twice daily |
| TID | Three times daily |
| QID | Four times daily |
| QOD | Every other day |
| PRN | As needed |
| AC | Before meals |
| PC | After meals |
TABLE 13-2 Disease States, Medications, and Common Side Effects
Cardiovascular diseases (high blood pressure, congestive heart failure, irregular heart rhythm, chest pain, heart attack, and stroke) are common in the older population. Medications used to treat these diseases may alter a patient’s blood pressure and/or heart rate, resulting in dizziness and the potential for falls. One class of medication, the diuretics, may cause excessive urination. As such it is recommended that nighttime dosing be avoided because of the risk of falls and interruption in rest. COTAs may notice that the client needs frequent breaks during therapy to use the restroom, and that the timing of the medication dose may need to be altered to avoid this. Persons taking one or more of the medication types mentioned previously should be closely monitored during therapy for the emergence of side effects, and consideration should be given to routine monitoring of blood pressure by the COTA. In addition, many of these same clients will be using medications to treat high cholesterol. Some of these drugs may cause diffuse muscle pain when they are started, with a dose increase, or with the addition of another medication, which may increase blood levels of the former. The COTA can help identify this type of drug-induced musculoskeletal pain and see to it that it is addressed by the appropriate individual because, in some cases, the consequences of this side effect can be severe and even life threatening.
Drugs that affect the blood’s ability to clot are also frequently used in persons with cardiovascular diseases. The COTA must be aware that the client is using one of these agents as the risk of a serious bleed is increased and therapy may have to be adjusted. One sign associated with the use of these medications is easy bruising. This is not necessarily unexpected, but if the COTA believes that the amount of bruising is excessive, he or she may wish to refer the patient to have the medication therapy evaluated.
Another common complaint of elders is pain, which can be either chronic (such as arthritis pain) or short-term because of an acute injury. The use of OTC pain medications is common when elders choose to self-treat. These medications include acetaminophen, aspirin, ibuprofen, and naproxen. Commonly observed side effects associated with these agents include gastrointestinal distress (which may be a symptom of a more serious condition such as a stomach ulcer) and increases in blood pressure because some of these medications can cause fluid retention. With more severe pain, prescription medications are used. Most prescription pain medications (primarily narcotics such as codeine, hydrocodone, oxycodone, and morphine) exert their action in the central nervous system and therefore may cause dizziness, drowsiness, and confusion. These symptoms add to the risk of falls and may make successful therapeutic intervention by the COTA a challenge if the client is unable to fully participate because of cognitive impairment.
Many older persons experience a variety of psychosocial, psychiatric, and cognitive disorders. Drugs that may be used to treat such diagnoses include antipsychotics, antidepressants, anti-anxiety agents, and medications used to slow the progression of cognitive impairment, such as those used in the treatment of Alzheimer’s dementia. These medications are all active in the central nervous system and therefore have the potential to affect sensorium, alertness, and balance. Additionally, some of them may have effects on other body systems causing disturbances in sleep and bodily functions (dry eyes, dry mouth, urinary retention, constipation, elevated heart rate, and the inability to perspire). Some of the agents used to treat psychosis also cause extrapyramidal symptoms that may manifest as abnormal movements of the limbs, head, neck, and the tongue. Sometimes these symptoms can be controlled with another medication or by discontinuing the offending agent. However, other times the benefit of continuing the medication may outweigh the risk associated with developing these symptoms, and the client and COTA may need to find a way to work around them. Furthermore, use of these medications is likely to aid the COTA in working with a client when symptoms of these types of disorders are controlled.
Sleep disturbances are frequently encountered by the older person. Such disturbances include the inability to fall asleep, early morning awakening, and daytime drowsiness. Sleep-inducing medications are often used to help older persons sleep. However, it is important to note that as people age, they need fewer hours of sleep, and education of elders is necessary to help them differentiate between insomnia and the normal aging process as it pertains to sleep. Some sleep agents may cause clients to be drowsy during the morning hours, which may interfere with the therapy process. Proper sleep hygiene (going to bed and getting up at the same time each day, minimizing daytime napping, using the bed for sleep and sex only, and avoidance of caffeine and exercise late in the day) can make a large difference in the client’s ability to fully participate in therapy. If daytime drowsiness is a concern, the COTA may wish to inquire about the use of sleep agents (both prescription and OTC) to determine whether a change needs to be made.
As persons age, the diagnosis of diabetes becomes more common. Drugs used for the treatment of elevated blood glucose are associated with several side effects that may be observed by the COTA. The most common of these is hypoglycemia, or low-blood glucose. Symptoms associated with hypoglycemia include sweating, dizziness, weakness, tremor, elevated heart rate, and confusion. These symptoms may be more common if the client has not had a normal amount of food before therapy. Additionally, diabetes can cause impaired sensation in the extremities, also known as neuropathy. This can result in numbness or extreme pain and may present a substantial challenge for the COTA. It is important that therapy be tailored for elders with impaired sensation to ensure that they remain safe during therapy and in their living environment. Medications are available to help with the pain of neuropathy, and the COTA may wish to refer patients if the pain interferes with quality of life.
Although not a normal part of aging, urinary incontinence may be frequently encountered in the elderly population. Incontinence presents its own challenges such as those associated with frequent toileting and skin breakdown as a result of excessive exposure to moisture. Medications used to treat one type of incontinence, overactive bladder or “urge” incontinence, can cause a multitude of side effects similar to those mentioned as associated with the psychoactive medications (dry eyes, dry mouth, urinary retention, constipation, elevated heart rate, and the inability to perspire).
Strategies for Minimizing Medication Problems in Elders
There are multiple reasons why older adults may be at higher risk for medication problems than younger persons. It is imperative that health care providers ensure that clients can safely manage their medications. Psychiatric diagnoses, such as dementia and depression, are common in this population and may affect the client’s ability to manage drug therapy without assistance. Often the first indication that there may be a problem in this area is the inability to manage other daily tasks such as keeping good finances or managing basic household responsibilities.
The older generation is often apprehensive when it comes to questioning health care providers, and this may lead to a lack of active participation in their own care. In many cases, a medication regimen can be simplified, but if the health care provider is not asked to do this, it is unlikely to occur. Additionally, if information about medications or their side effects is not readily offered, an older person might not directly ask about such things, and this may lead to underrecognition of side effects. It is also important that clients understand why they are taking each medication and its intended purpose so that they may self-monitor for problems.
There are many reasons that clients may not adhere to a medication regimen as prescribed. Over-adherence may occur, either by mistake because clients cannot remember whether a medication has already been taken, or because they may believe that “if a little is good, more must be better.” On the other hand, under-adherence also occurs for various reasons. Avoidance of side effects may lead a client to skip doses. Additionally, if money is a concern, clients may choose to alter their regimen by deliberately taking a medication less often than recommended. Cutting pills in half and taking partial doses is another common occurrence when saving money is an issue.
Self-treatment of symptoms or side effects with OTC medications may also result in problems. Although OTC medications are available without a prescription, it is incorrect to believe that they are without risks. Drug interactions may occur with medications that have previously been prescribed. It is also incorrect to believe that “natural” products are inherently safe because they, too, may interact with other drugs and cause side effects that may be more difficult to recognize because of a lack of regulation and standardization.
Application of the Occupational Therapy Process to Self-Medication
Medication routines of clients are often not addressed by OT.2 This is evident in the lack of literature on self-medication programs and OT interventions with medication routines. Medication routines are instrumental activities of daily living (IADL). According to the Occupational Therapy Practice Framework: Domain and Process (second edition), medication routines are classified as a health management and maintenance IADL.3 Thus, assessment of routines and instruction in proper use of medication should be dealt with as part of activities of daily living (ADL) routines.4 Participation in one’s medication routine includes obtaining medication, opening and closing containers, following prescribed schedules, taking correct quantities, reporting problems and adverse effects, and administering correct quantities by using prescribed methods.
Client Factors
Values, beliefs, spirituality, body functions, and body structures that reside within the client and may affect performance in medication routines should be analyzed by the registered occupational therapist (OTR) and COTA. This section overviews how each of these client factors can potentially impact one’s medication routine.
Values, Beliefs, and Spirituality
A variety of factors related to adherence to medication routines has been researched, including people’s values and beliefs. The self-regulations theory5,6 is a patient-centered understanding to such factors that affect adherence. The theory suggests that people attempt to understand their illness by developing a representation of their illness, its causes, its effects, the duration of the illness, and whether the illness can be cured or controlled. In this view, it is thought that people are motivated to reduce their health-related risks and will work on eliminating health threats in ways that are congruent with their perceptions.
In addition to forming representations of illness, it is hypothesized that clients also form representations of their treatments.7 Researchers have demonstrated the link between values and behaviors.8-10 Decisions about taking medication are likely to be affected by the beliefs about the medicines, the illness, and the treatment providers.11 Values are often the underpinnings of behaviors. People typically decide what is important for them and then act on such decisions. Although a paucity of literature exists on the influence of spirituality on medication routines, persons diagnosed with terminal illnesses have reported a high level of spirituality (and they have been correlated highly with psychological adaptation and positive health outcomes).12-14
Bodily Functions
Bodily functions are “physiological functions of body systems (including psychological functions)” (p. 635).3 Bodily functions affect one’s ability to perform and participate in an occupation. Medication routines require extensive performance from multiple bodily functions, including the following:
Mental Functions
Both long-term and a working memory15 are required for independent self-medication. Elders need long-term memory to understand which condition is being treated and the purpose for the medication(s) they take. Understanding and remembering the nature of the regimen also is required for self-medication. Elders use long-term memory to remember where the medication is stored. Working memory, which includes simultaneous storing and processing of information, is needed to avoid under medication or overmedication. This frequently occurs when elders do not remember whether they took a medication. Various items such as programmable alarms or auditory devices that exclaim, “time to take your pill,” and pill storage boxes can aid self-medication. Home health aides and pharmacists may assist in filling self-medication boxes. A fee may be charged for this service. One advantage of involving home health aid or a pharmacist is that they can make sure the elder is actually taking the medicine, as prescribed, when it is time to refill the storage container.
A great deal of problem solving is needed to properly self-medicate. Elders must decide whether to contact the physician when changes in a condition occur. For example, Ken goes to his physician because he wonders whether his frequent headaches indicate that his blood pressure medication is not working or whether he needs a new prescription for his glasses. Problem solving also is needed to determine when refills need to be obtained and how to safely store medication. Even more complex is the problem solving that is needed to determine Medicare prescription plan options.16 Some pharmacies and health care agencies will provide individualized consults for elders who need assistance in understanding and choosing such plans.
Elders must be motivated to comply with their medication regimen. Depression, uncertainty, misunderstanding, financial worries, lack of confidence, side effects, and social or cultural taboos are all factors that may contribute to a lack of motivation. For example, Hazel, a 74-year-old woman with a history of heart failure and high blood pressure, sometimes takes her captopril tablets once a day instead of three times a day. Hazel does this when she feels “better” to save money. In addition, some elders are embarrassed by the diagnosis of depression, or other emotional disorders, and are reluctant to take prescribed antidepressants or other medicines used to treat psychological problems.
Sensory Functions and Pain
Visual perception skills may be required by elders who take multiple medications. Visual perception skills include color discrimination, depth perception, and figure-ground perception. Visual acuity and perception are required to distinguish between different containers of medication and to read instruction labels. If needed, glasses should be worn when elders self-medicate. Adaptations may be used to assist elders who have visual impairments (Figure 13-1). Magnifying lenses and large type or contrasting print may be helpful. For severe visual impairments, different size, different shape, or multicolor containers can be used for medication storage. Instructions for administration can be tape recorded to relay information that cannot be read. Depth perception skills are needed to obtain pills in a multipartition container. Figure-ground perception also is needed to see white pills in a white pill box. COTAs should suggest that elders use colored pill containers for white pills.
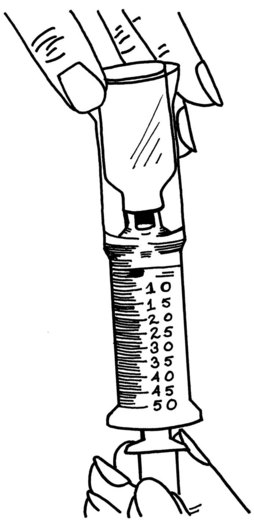
FIGURE 13-1 This magnifier device consists of a plastic cylinder in which the medication and syringe fit at each end and permits elders with visual impairments to view amounts easily.
According to the Deafness Research Foundation, there is a relationship between age and hearing loss. For example, 30% of adults who are ages 65 to 74 years and 47% of adults age 75 years and older have a hearing impairment.17 COTAs should remember this when educating elders, family members, and caregivers. The ability to hear is important for elders to understand patient education, medication dosages, and changes. COTAs should provide both verbal and written instructions when educating elders. For example, Kathy, a COTA, meets with Vladimir, who has difficulty hearing, to review his discharge program. She first checks to make sure Vladimir is wearing his hearing aid and then reviews the information in his client education packet. Kathy speaks slowly and clearly and is sitting directly at eye level with Vladimir. She also frequently asks Vladimir whether he has any questions and encourages him to repeat back to her what he understands (see Chapter 16).
Neuromusculoskeletal and Movement-Related Functions
Usually a great deal of fine motor coordination, finger dexterity, and some degree of strength are needed to open and close medication containers and use syringes. Fine grasp patterns are required when picking up pills or tablets. Therefore, elders with conditions such as rheumatoid arthritis or Parkinson’s disease may have difficulty opening childproof containers. Non-childproof tops can be provided by the pharmacist, if requested. If nonsafety caps are dispensed by the pharmacist, it is essential that elders store their medication out of the reach of children.
Manipulating medication containers requires strength. Occasionally, a medication routine involves crushing pills or splitting them in half. Such assists as pill crushers and pill splinters can help an elder who has poor hand strength. Elders should never use a razor blade to cut tablets. Many medications are released over time (known as extended or sustained release) and should not be crushed. A pharmacist is an invaluable resource person to find out whether a tablet can be crushed. Furthermore, sometimes a liquid form of the medication (if available) may be a better choice for an elder who needs to crush several medicines.
Elders taking medications need to have a way of getting prescriptions filled on a regular basis. Elders who do not drive or are wheelchair-bound may need to seek out community resources to obtain rides to medical appointments and the pharmacy. Some pharmacies will deliver medications for a fee. In addition, some communities have volunteer programs that provide this transportation service at no cost. For example, Antonio is unable to drive because of his poor vision, but he is able to renew prescriptions by using a free transportation service provided by his church. Automated systems are available at many pharmacies, which allow people to renew their prescriptions over the phone. Some pharmacies also provide automatic refill service for maintenance prescription medications.
It is estimated that 35% to 68% of persons over age 65 have some degree of swallowing dysfunction.18 Patients and caregivers (N = 477) were surveyed about swallowing medicine. Results of the survey included 68% of persons reported opening a capsule or crushing a tablet, whereas 64% reported not taking their medication because of difficulty swallowing. Health professionals must facilitate medication routines of patients who cannot properly swallow medications by reviewing regimens, omitting medications that are unnecessary, and determining alterative forms of medications when needed.
Cardiovascular, Hematological, Immunological, and Respiratory System Function
Some medications, including nebulizers and inhalers, require the ability to inhale medication through the mouth or nostrils. Inhalers are used to deliver medication directly to the lungs. A nebulizer is a type of inhaler that is used to spray a fine mist of medication through the use of a mask. A mouthpiece is often connected to a machine and plastic tubing to deliver the medication to the person. Inspiration must be satisfactory to receive the medication.
Voice and Speech Functions
Elders must be able to communicate their medication regimen with health care providers and caregivers. Health care providers must reciprocate communication in an effective manner. Demonstration, web-based, verbal, and written formats can be used for communication. Elders may find it helpful to keep names, phone numbers, and addresses of health care providers and agencies in a regular place so they are available for emergencies. Posting this information on the refrigerator may also be helpful. For example, Greta has been deaf since birth but is able to communicate by using a notebook that contains information regarding her past and present medical condition. She stores this notebook in a drawer in the nightstand by her bed. She also has notified family members where the notebook is located in case of an emergency.
Activity Demands
Medication routines involve activity demands. According to the Occupational Therapy Practice Framework, activity demands are “aspects of an activity, which include the objects and their properties, space, social demands, sequencing or timing, required actions and skills, and required underlying body functions and body structure needed to carry out the activity” (p. 638).3 Aspects of activity demands include the following:
Table 13-3 offers examples of activity demands typically involved in medication routines.
TABLE 13-3 Activity Demands and Examples Related to Medication Routines
| Activity demand aspect | Examples related to medication routine |
|---|---|
| Objects and their properties | Common objects used in medication routines include pill bottles, pill storage boxes, syringes, inhalers, tubes, gloves, etc. |
| Space demands | Space to complete a medication routine commonly requires appropriate lighting to see what one is doing, ample room to manipulate any equipment or objects used, and proper space for medication storage. Occasionally, medication must be stored in special environments—for example, environments that adhere to recommended temperature ranges and restricted exposure to sunlight. |
| Social demands | Medication routines require communicating when one may need medication to refill prescriptions or report outcomes or concerns to one’s physician(s). |
| Sequence and timing | Medication routines often require timing of medication. Occasionally, medications must be taken properly throughout the day. For example, sequencing the medication routine involves selecting the container, opening the container, securing the medication tablet, and swallowing the medication. |
| Required actions and performance skills | Skills used to perform medication routines include opening and closing containers, manipulating any objects needed in medication routines, etc. |
| Required body functions | Body functions needed in medication routine often include mental, neuromusculoskeletal, and speech functions. |
| Required body structures | Body structures often needed to perform medication routines include use of hands, eyes, etc. |
Performance Skills
Performance skills include the abilities demonstrated while performing the actions.3 Skills include motor and praxis, sensory perceptual, emotional regulation, cognitive, and communication and social skills. Examples of performance skills required during medication routines are presented in Table 13-4.
TABLE 13-4 Examples of Skills Needed for Medication Routines
| Skill | Example |
|---|---|
| Motor and praxis skills | Planning and executing movements to successfully open and close medication containers; maintaining balance while taking medication; adjusting posture, for example, to extend neck when applying eye drops. |
| Sensory perceptual skills | Sensing that a pill is on your tongue and ready to be swallowed; feeling relief after an anti-itch cream has been applied to an itchy and irritated area; seeing the volume marks on a syringe. |
| Cognitive skills | Ability to recognize when one needs a prescription refill; ability to remember taking medication, judging whether the symptoms being addressed are getting better, worse, or staying the same. |
| Communication and social skills | Ability to communicate with family, caretakers, pharmacists, and physicians about one’s medication routine; ability to answer questions posed by health care providers and caretakers about medication routine. |
Occupational Therapy Process
According to the Occupational Therapy Practice Framework,3 evaluation, intervention, and outcomes comprise the process of occupational therapy. Evaluation includes the occupational profile and analysis of occupational performance. Intervention constitutes the plan, implementation, and review. Finally, the outcomes are the determination of success of the desired outcomes. The following outlines the process as applied to medication routines.
The occupational profile is “the initial step in the evaluation process that provides an understanding of the client’s occupational history and experiences, patterns of daily living, interests, values, and needs. The client’s problems and concerns about performing occupations and daily life activities are identified, and the client’s priorities are determined” (p. 646).3 COTAs often assist in gathering information from the client during the profile. Questions and items to be used as part of the occupational profile related to medication routines include the following:
 Tell me about any medications you take. Don’t forget to include prescriptions, OTC medications, supplements, and natural products.
Tell me about any medications you take. Don’t forget to include prescriptions, OTC medications, supplements, and natural products.
Tell me about any vitamins or nutritional supplements you use.
Describe your routine of taking medications.
Describe any concerns you might have about your medication routine.
Depending on the issues that arise from the occupational profile, the therapist may determine to analyze the person’s performance related to the medication routine. Analysis of occupational performance is “the step in the evaluation process during which the client’s assets, problems, or potential problems are more specifically identified. Actual performance is often observed in context to identify what supports performance and what hinders performance. Performance skills, performance patterns, context or contexts, activity demands, and client factors are all considered, but only selected aspects may be specifically assessed. Targeted outcomes are identified” (p. 646).3 For example, a therapist may suspect that the elder’s grip strength is insufficient to open a medication container and thus test grip strength using a dynamometer or asking the person to open his or her medication container(s). Based on the analysis of occupational performance, the therapist is able to plan intervention.
The intervention plan consists of “a plan that will guide actions taken and that is developed in collaboration with the client. It is based on selected theories, frames of reference, and evidence. Outcomes to be targeted are confirmed” (p. 646).3 For example, the therapist may use a rehabilitative frame of reference and focus on the person’s abilities and compensate for disability. Thus, the therapist may decide that the person’s grip strength is not sufficient to open childproof medication containers and has the client practice opening a container that is not childproof. The therapist may provide information on how to request such containers for future prescriptions. This action is the intervention implementation, or the “ongoing actions taken to influence and support improved client performance. Interventions are directed at identified outcomes. Client’s response is monitored and documented” (p. 646).3 The therapist will then review “the implementation plan and process as well as its progress toward targeted outcomes” (p. 646).3 The following section addresses ideas for medication intervention with elders.
Assistive Aids for Self-Medication
Many commercial or homemade aids can assist individuals with self-medication.19 Each aid has advantages and disadvantages.
Commercial Aids
Calendars
Calendars are helpful for tracking medication schedules. A pocket calendar or a calendar hung near the place where medication is taken can be used to mark each time medication is taken. At the end of the day, marks are counted to make sure that the medication schedule was followed. The advantage of using calendars is that the medications are stored in their original containers and remain properly labeled. Calendars are also inexpensive and readily available. The disadvantage of using a calendar is that it requires some basic reading, comprehension, and memory skills to mark the calendar each time medications are taken.19
Pill storage boxes/storage boxes
For people who take medications on a regular basis, a pill box or pill reminder is a useful item. Pill storage boxes are containers with compartments in which to put medications (Figure 13-2). Pill boxes are easy to use and can be useful to adhere to one’s medication schedule regardless of whether one is at home or traveling. Pill boxes are organized daily, weekly, or monthly. Some have the capacity to organize medications throughout the day (e.g., breakfast, lunch, and dinner). Added features such as locks or timers and alarms can be ideal when safety is a concern or when a cognitive reminder is needed. Some boxes are made to look like jewelry. There is certainly one likely to be available to suit one’s needs and style.

FIGURE 13-2 Various pill boxes are available with compartments for single or multiple daily and weekly doses.
Pill boxes require manual dexterity skills to open and close and to manipulate pills. Visual discrimination also is required to identify desired pills. Pill boxes usually do not provide tight storage for medications that require tight containers, such as nitroglycerin. In addition, the pills are no longer in labeled, childproof containers.
There are advantages and disadvantages for using daily and 7-day pill boxes.19 An advantage of a daily pill box is a better chance of taking all daily doses. Any errors made in setting up this pill box would be experienced for one day only. A disadvantage of a daily pill box is that each compartment could contain several unlabeled pills. The elder would have to identify the medication(s) by physical appearance. This is a serious safety concern if pills are similar in size, shape, or color, especially if the elder has impaired vision or is easily confused.
Weekly pill boxes store medication for 7 days. The design of some pill boxes allows the separation of multiple daily doses. These boxes often consist of four rows and seven columns. The four rows are marked with times of the day (morning, noon, evening, and bedtime), and the seven columns are marked with the day of the week. The advantage of using a 7-day pill box is that setup is required once a week only. The disadvantage is that setup requires more accuracy.19 If there is a mistake, it may occur seven times.
A pill box with an alarm is an option for elders who must take their medication at specific times. The advantage of this type of pill box is that it alerts elders of the medication schedule. A disadvantage is that elders must be able to read, understand, and follow in-depth instructions. These devices often need to be programmed and may require very fine manipulation to set the clock or the alarm. If the device breaks, repairs may be difficult and expensive. Another disadvantage is the risk of not hearing the alarm when it sounds.
Insulin holders
Insulin holders are intended for one-handed use. The device holds an insulin bottle so that a person can manipulate a syringe to obtain the proper amount of fluid. Often the device has suction cups or a nonskid surface to prevent the device from sliding on a table top.
Pill splitters
Pill splitters are useful devices when a pill must be split for proper dosage or to reduce the pill size for easier swallowing (when appropriate). Pill splitters are often lightweight and use a leverage design to reduce the amount of strength needed to use it. As previously stated, a razor blade should never be used to cut a tablet.
Pill crushers
A pill crusher is a device used to pulverize tablets into a fine powder. Similar to the design of pill splitters, pill crushers use a leverage system so that an abundance of strength is not required. Pill crushers can be beneficial when individuals have difficulty swallowing whole tablets. (Remember that not all tablets can be crushed or split.)
Talking and shaking alarms, watches, and prescription bottles
For elders who experience difficulty remembering to take their medications or what their medication routine is, several devices such as talking or shaking alarms and talking prescription bottles may be beneficial. Talking alarms are devices that are programmed to send a “beep,” voice message, or visual cue when it is time to take a medication. Shaking alarms can be clipped to the bedding to wake elders when it is time to take their medication. The device can be put in one’s pocket when in public and it will provide a quiet vibration to indicate the medication time. A talking prescription bottle is a device attached to a prescription bottle. A pharmacist or physician records the prescription information into the device. To operate, one pushes a button on the device to play a recorded message about the contents; how many pills to take, when, and what for; and any warnings. The talking prescription bottle is intended for those who have low vision or hearing impairments. It is also beneficial for elders for whom English is a second language or for elders who have difficulty reading.
Homemade Aids
Medication diary
A medication diary is another aid for tracking medication use (Table 13-5).
TABLE 13-5 Contents of a Medication Diary
| Section | Information |
|---|---|
| 1: Demographics | |
| 2: Health care providers | |
| 3: Past medications | |
| 4: Special equipment | |
| 5: Recent medications | |
| 6: Over-the-counter medications | |
| 7: Questions for health care providers |
COTAs may assist elders in making a diary, which can be kept in a notebook. This information can then be shared with other health care professionals, as needed.
Storage cups
Storage cups can be made at home by using small plastic or paper cups that are stacked and ordered according to the number of times the medication must be taken throughout the day. The cups should be marked in relation to when medications are taken (for example, morning, noon, dinner, and bedtime) (Figure 13-3). After the morning medication is taken, the “morning” cup is moved to the bottom of the stack. This allows the next medication dose to be on the top. This system requires that elders have good manual dexterity, visual-perceptual, and memory skills. A similar system can be made using egg cartons. For liquid or powder medications, a system can be set up using small, labeled, airtight containers. Using a homemade system is simple and inexpensive. However, using a homemade system may cause medication to be exposed to improper storage conditions.19 Also, pills in open view may tempt small children who live in or visit the elder’s home. This risk can be reduced by storing the medication out of view and reach.

Self-Medication Program
A formal self-medication program may prevent problems with polypharmacy.2 The program is designed to (1) use an interdisciplinary team approach, (2) educate elders about their medications, (3) develop elders’ motor skills for proper administration, (4) offer practice opportunities to elders, (5) assess elders for any adaptive devices that may be useful, and (6) evaluate elders’ skills in medication administration before discharge.
The elders’ intervention plan should include interventions to maximize independence with self-medication. Depending on elders’ limitations and deficits, COTAs should engage them in simulated medication tasks. An example of such a task is using small, colored candy pieces to practice color discrimination and fine prehensile patterns. Reading and comprehending general labels can aid in reading medication labels. Opening and closing medication containers should be practiced. In addition, elders should master any adaptive aids before being discharged from OT.
Relatives, friends, and home care personnel who assist in the delivery of medications often have not been included in discussions of medications.20 Family and caregivers should be able to name the elder’s medications, describe the purpose of each medication, and describe any precautions associated with each medication. COTAs can refer to Box 13-1 to help educate family and other caregivers. Box 13-2 addresses safety issues for COTAs’ consideration.
BOX 13-1 Guidelines for Caregivers Who Administer Medications
Elders most at risk to experience problems with medications are those who are:
Keep track of the following information on the elder(s) you are caring for:
All of the prescription drugs the elder is taking
All of the nonprescription (OTC) drugs the elder is taking
All other medicinal items the elder uses from a health food store or supermarket
When and how much medicine to give
What results to expect from the medicine
Any physical or mental change in the elder (report to physician)
Prescriptions
The need for the medications should be reevaluated at least every 3 to 6 months.
Do not save unused medication for future use without the physician’s approval. Take the entire course of any antibiotic that is prescribed.
Do not share medications with anyone. Closely check expiration dates and dispose of expired medicine.
If you are not clear about what the directions you are given mean, clarify them with your pharmacist or the prescriber. For instance, look at the following directions:
What does four times a day really mean?
Does it mean every 6 hours? Does it mean with meals and at bedtime?
Does before meals mean before each meal or on an empty stomach?
How often is it safe to take a medication prescribed on an “as needed” basis?
These are the types of questions that a patient or caregiver should ask.
Written directions should always be given, and “take as directed” should not be considered adequate direction.
To reduce the risk for aspiration and swallowing problems, never give tablets or capsules while the elder is lying down. Always give medications with plenty of fluids to reduce stomach upset unless directed otherwise.
Medication storage
Store medications properly. Keep them in a cool, dry place, away from the sunlight and away from children. Keep the label on the medication container until all medicine is used or destroyed. If traveling, take the original medicine container with you in case of an emergency.
Medication disposal
Do not flush medications down the toilet unless the label or instructions specifically tell you to do so. Find out whether there is a drug take-back program in your community by calling your city or county. If such a program is not available, discard medications as follows:
Take the drugs out of their original containers. Mix them with an undesirable substance (kitty litter, used coffee grounds). Seal the mixture in a disposable container and place in the trash. Make sure that personal information and prescription numbers are made illegible, and discard the original medication containers.
Take precautions with the following:
Chewable tablets: Elders often do not like chewable tablets because they can interfere with dentures. One option is to have the elder suck on the tablet to dissolve it. Chewable tablets should not be swallowed whole.
Crushing tablets or opening capsules: Many pills should not be crushed because they are designed to be long-acting. Other pills should not be crushed because the contents may cause stomach upset or inflammation.
Always check with the pharmacist. Occasionally, a liquid substitute is available.
Liquid medications: Because liquid medications are difficult to measure accurately, ask the pharmacist for a measuring device to ensure the correct dose.
Applying ointments: Because medications applied to the elder’s skin will have an effect on your skin, wash hands after each application. Use gauze or gloves to apply.
Applying patches: Always remove old patches. Know how often and where to apply the patch on the body. Remove old patches gently because elders have delicate skin. Notify the pharmacist if the skin becomes irritated or the patch does not stick.
Giving injections: Practice administration techniques with a nurse or pharmacist.
Tube feedings: Tube feedings with medication require special instructions. Liquid medications, if available, work best when medicine needs to be given down a feeding tube. Some medications may actually directly interact with the enterable supplement. Contact the pharmacist for instructions on exactly how to give the medication.
Discharge plans from the hospital or nursing home
This can be a very confusing time! Medications often change while the elder is in the hospital. Everyone must know which medications to take and which not to take.
Know about any generic drugs. Tablets or capsules may look different and have a different name, but the medications contain the same ingredient in the same amount. Keep an accurate list or bring all of the medications when visiting every doctor. Shop at one pharmacy to avoid medication duplication. If moving to another area, ask the pharmacist to forward your prescription records to your new pharmacist.
Monitor the elder’s nutrition, diet, and fluids. Pay attention to the elder’s appetite, and notify the physician if there are any concerns such as weight gain or loss. Know whether the elder requires a special diet, including foods/liquids to avoid and to encourage. Administer medication by offering plenty of liquids, unless otherwise instructed.
BOX 13-2 Safety Gems for COTAs to Consider with Medication Provision and Elders
Critically consider and bring forward concerns about possible common medication side effects for symptoms that the elder may be exhibiting.
Be aware of possible medication side effects that may cause symptoms that could lead to safety issues such as falls or cognitive impairment. (Refer to Table 13-2.)
Share results of assessments (particularly cognitive, communication skills, neuromuscular and movement, and sensory assessment findings) with members of the treatment team to help inform others about the elder’s ability to safely manage and self-administer medications.
Communicate any medication issues, such as the alteration of medications to save money or difficulty with a particular dosage form (for instance, those that need to be swallowed), with appropriate team members.
Make appropriate adaptations so that elders can safely take medications.
Case Study
Pat is an 83-year-old woman living at home with her 85-year-old husband. Pat is currently under the care of two physicians: her primary medical physician and a psychiatrist. Pat has a recent history of falls and has significant bruising on her forehead. One of her falls occurred in the middle of the night while she was attempting to walk to the bathroom. Additionally, she complains of dizziness and pain in her knees, which affects her ability to participate in events outside of her home.
Two weeks ago Pat fell and fractured her hip. Her mental status fluctuates. Her husband is in charge of administering medications. Her problems and medications are listed as follows:
| Disease state | Medication | Dosage |
|---|---|---|
| Congestive heart failure | Furosemide (diuretic or water pill) | 40 mg po bid |
| Metoprolol XL (beta blocker) | 100 mg po once daily | |
| Lisinopril (ace inhibitor) | 10 mg po once daily | |
| Anxiety | Lorazepam (anti-anxiety) | 0.5 mg po tid |
| Osteoarthritis | Naproxen (pain reliever) | 500 mg po bid |
| Depression | Sertraline (antidepressant) | 50 mg po once daily |
| Insomnia | Diphenhydramine (nonprescription sleep aid) | 25 mg po hs prn |
| Prevention of blood clots after surgery | Warfarin (blood thinner) | 2.5 mg po once daily |
Case Study Questions
1. Which medication-related problems might be of concern to COTAs?
2. Could any of Pat’s current medical problems be caused by her medications? If so, which medications cause which side effects? (Refer to Table 13-2.)
3. What other factors may place Pat at risk for polypharmacy and medication-related problems?
4. The COTA is concerned about the frequency of Pat’s falls and the risk for another hip fracture but is unsure whether any medications are contributing to the falls. What is a reasonable course of action to address this plausible medication-related concern?
5. What skills for safe self-medication are affected in Pat’s case?
6. What assistive devices may help with her medication routine and why?
7. Who should be involved in a self-medication program to help Pat with her medications?
1. Considering the information in the chapter, explain why the COTA is an important player in the health care team to address medication issues with elders.
2. What are some reasons for polypharmacy among elders?
3. What is one side effect of each of the following: diuretics, OTC and prescription pain relievers, antidepressants/antipsychotics, and insulin? (Refer to Table 13-2.)
4. What resources and personnel are available to address the concerns or questions of COTAs regarding medications?
5. Explain skills needed for safe self-medication.
6. What aids are available to elders with poor vision, memory, or hearing, or lack of transportation?
7. What should be included in a medication diary?
8. What are some essential components to a self-medication program?
9. What information should COTAs provide to educate caregivers?
1 Wilson I.B., Schoen C., Neuman P., Strollo M.K., Rogers W.H., Chang H., et al. Physician-patient communication about prescription medication nonadherence: A 50-state study of America’s seniors. Journal of General Internal Medicine. 2007;22:6-12.
2 Potts J.M. Developing a patient self-medication program for the rehabilitation setting. Rehabilitation Nursing. 1994;19:344.
3 American Occupational Therapy Association. Occupational therapy practice framework: Domain and process, 2nd ed. American Journal of Occupational Therapy. 2008;62:625-683.
4 Lewis S.C. Elder Care in Occupational Therapy. Thorofare, NJ: Slack; 1989.
5 Diefenbach M.A., Leventhal H. The common-sense model of illness representation: Theoretical and practical considerations. Journal of Social Distress and the Homeless. 1996;5:11-38.
6 Leventhal H., Benyamini Y., Brownlee S., Diefenbach M., Leventhal E.A., Patrick-Miller L., et al. Illness representations: Theoretical foundations. In: Petrie K.J., Weinman J.A., editors. Perceptions of Health and Illness: Current Research and Applications. Singapore: Harwood Academic; 1997:19-45.
7 Gauchet A., Tarquinio C., Fischer G. Psychosocial predictors of medication adherence among persons living with HIV. International Journal of Behavioral Medicine. 2007;14(3):141-150.
8 Church R.M. Pharmacy practice in the Indian Health Service. American Journal of Hospital Pharmacy. 1987;44(4):771-775.
9 Lefley H.P. Culture and chronic mental illness. Hospital and Community Psychiatry. 1990;41(3):277-286.
10 Whetstone W.R., Reid J.C. Health promotion of older adults: Perceived barriers. Journal of Advanced Nursing. 1991;16(11):1343-1349.
11 Horne R. Representations of medication and treatment: Advances in theory and measurement. In: Petrie K.J., Weinman J., editors. Perceptions of Health and Illness: Current Research and Applications. London: Harwood Academic; 1997:155-187.
12 Margolin A., Schuman-Olivier Z., Beitel M., Arnold R.M., Fulwiler C.E., et al. A preliminary study of spiritual self-schema (3-S[+]) therapy for reducing impulsivity of HIV-positive drug users. Journal of Clinical Psychology. 2007;63(10):979-999.
13 Ironson G., Stuetzle R., Fletcher M.A. An increase in religiousness/spirituality occurs after HIV diagnosis and predicts slower disease progression over 4 years in people with HIV. Journal of General Internal Medicine. 2006;21(Suppl 5):S62-S68.
14 Leach C.R., Schoenbery N.E. Striving for control: Cognitive, self-care, and faith strategies employed by vulnerable black and white older adults with multiple chronic conditions. Journal of Cross-Cultural Gerontology. 2008;23(4):377-399.
15 Andiel C., Liu L. Working memory and older adults: Implications for occupational therapy. American Journal of Occupational Therapy. 1995;49:681-686.
16 Tseng C.W., Dudley R.A., Brook R.H., Keeler E., Hixon A.L., Manlucu L.R., Mangione C.M. Elderly patients’ knowledge of drug benefit caps and communication with providers about exceeding caps. Journal of the American Geriatric Society. 2009;57:848-854.
17 Deafness Research Foundation. Statistics. Retrieved January 27, 2010, from http://www.drf.org/Statistics, 2008.
18 Kelly J., D’Cruz G., Wright D. A qualitative study of the problems surrounding medication administration to patients with dysphagia. Dysphagia. 2009;24:49-56.
19 Meyer M.E. Coping with medications. San Diego, CA: Singular; 1993.
20 Wieder A.J., Wolf-Klein G.P. When medications change, tell the caregiver, too. Geriatrics. 1994;49:48.