chapter 16 Working with Elders Who Have Hearing Impairments
1. Describe sensorineural and conductive hearing losses.
2. Describe ways that slow, progressive changes in the auditory system interfere with occupations that require communication.
3. List environmental modifications that reduce background noise in homes and institutions.
4. Describe possible safety recommendations for home and institutional environments where hearing-impaired elders reside.
5. Describe the effect of age-related hearing loss on socialization, communication, and travel and its possible contribution to feelings of isolation for hearing-impaired elders.
6. List suggestions for improving communication with hearing-impaired elders.
7. Describe possible behaviors that may indicate hearing impairment.
sensorineural hearing loss (sensory, neural, mechanical), conductive hearing loss, cochlear implants, tinnitus, hearing aid, assistive listening device, audiologist
The voice of a loved one, the chimes of a grandfather clock, a violin concerto—these are sounds many people not only enjoy, but also take for granted. For elders who have hearing impairments, these sounds may be either misinterpreted or missed altogether.
Hearing impairments may also be associated with the reduced ability to hear warning signals, ambulation difficulties, and difficulties with instrumental activities of daily living (IADL), balance problems, and increased incidence of falls.1-3 Hearing impairments can contribute to social isolation. Safety related to hearing impairments may become a concern when elders are unable to hear alarms and other warning signals.4
Among the elderly, hearing loss is the third most prevalent chronic condition following arthritis and hypertension.5 In the United States by the year 2050, 52.9 million people are expected to have hearing loss.6 Although persons of all ages experience hearing impairments, in terms of a health disparity, elders are a primary concern.7 Approximately one-third of elders between ages 65 and 74 years experience hearing loss. This percentage increases to 47% for those older than 75 years.8 Furthermore, some studies indicate that 85% to 90% of nursing home residents have hearing impairments that limit function.4
Even though hearing impairments are more prevalent than vision loss, they are often more difficult to distinguish. Changes in hearing are often subtle and occur gradually. Many elders with significant hearing losses often wait as long as 5 years before seeking assistance with their hearing.9 Elders, family members, and health care personnel may not recognize hearing losses. Some may accept the loss as an inevitable and unalterable aspect of aging.
According to the Occupational Therapy Practice Framework: Domain and Process (2nd ed.) hearing is addressed in the client factors table as a body function under the sensory functions and pain category, and auditory is listed in the performance skills table as a sensory perceptual skill.10 Hearing loss can have a profound effect on engagement in occupations and activities of daily living (ADL). Certified occupational therapy assistants (COTAs) have the opportunity to diminish the impact of hearing loss on functional performance by becoming educated about hearing loss. Learning accommodations that may benefit the patient can make working with hearing impaired individuals easier and improve performance in functional tasks.11
Because elders seldom seek assistance or plan interventions to enhance their hearing, COTAs must be able to distinguish the various types of hearing impairments. In addition, COTAs should be aware of interventions, services, devices, and activities that can enhance occupational performance for elders who are hearing impaired.
This chapter provides an overview of the most common types of hearing losses that affect elders. The possible psychosocial effects that a hearing impairment may have on elders, their families, and their friends also are addressed. Rehabilitation considerations are discussed, including communicating with an elder who has a hearing impairment, methods for modifying home, public spaces, and institutional environments, and recommendations for assisting elders in the use of hearing aids and assisted listening devices (ALD).
Hearing Conditions Associated with Aging
If any hearing loss is suspected, individuals should visit their primary care physician (PCP) to be screened and/or treated for any other underlying pathological processes.5 The term presbycusis is often used when diagnosing elders with hearing loss. According to the National Institute on Deafness and Other Communication Disorders (NIDCD),12 the term presbycusis is the gradual loss of hearing as an individual grows older. Generally, hearing losses are divided into the three following areas: sensorineural, conductive, and mixed. These conditions may affect one or both ears.
The most common type of presbycusis or hearing loss in elders is the result of sensorineural damage to the hearing organ itself or to the peripheral or central nervous system (or both).12 Although elders rarely have just one type of sensorineural loss, the most common type of loss is caused by hair cell damage or loss of the sensory hair cells of the cochlea. As individuals age, these hair cells are slowly lost, and the ability to hear high-frequency sounds is diminished. One of the most frustrating and handicapping aspect of this loss is the ways sounds are changed or distorted. Although the elder may hear someone speaking, the signals that allow him or her to understand what is being said are not clear. Such losses can have serious consequences in both social and therapeutic settings. For example, at a party someone may say, “How are you?” and the elder may respond, “Eighty-one.” An elder in a clinic setting who is asked to hand the COTA a “dime” may respond with the correct “time.” Such responses often raise questions about mental status and often lead to a loss of confidence in interacting with others.12,13 In such situations, the COTA should seek assistance to rule out the presence of sensorineural loss before questioning the elder’s orientation or ability to follow directions. If proper audiological services are not available, the elderly individual can experience decreased mobility, social isolation, and increased cognitive decline.14 In addition, because women’s voices are usually higher pitched than men’s, female COTAs must understand that their voices could contribute to decreased comprehension by elders.
Elders living in areas with low exposure to loud or high-pitched noise levels may experience less sensorineural hearing loss than those living in noisy, industrial areas. Although those with better overall health seem less likely to experience this type of loss, some sensorineural loss eventually affects elders regardless of environmental conditions. However, continued exposure to loud noises for long periods may cause permanent damage.15 For instance, current research indicates that 15% of college graduates exhibit hearing loss equal to or greater than that of their parents due to exposure to high volume MP3 music players.16
Three types of sensorineural hearing loss have been identified: sensory, neural, and mechanical.13,15 Sensory loss is caused by atrophy and degeneration of the hair cells at the base of the basilar membrane. It produces a loss of high-frequency sounds but does not interfere with the discrimination of speech. Neural loss is caused by the loss of auditory nerve fibers. It affects the ability to distinguish speech sounds, especially in the higher frequencies, but does not affect the ability to hear pure tones. Mechanical loss is characterized by the degeneration of the vibrating membrane within the cochlea. This type of loss leads to the gradual impairment of hearing in all frequencies. In situations where several sounds in various frequencies are present at the same time, the ability to distinguish between the sounds becomes increasingly difficult. Table 16-1 lists common hearing conditions of elders.
TABLE 16-1 Common Hearing Conditions of Elders
| Condition | Cause | Symptoms |
|---|---|---|
| Sensorineural losses | Atrophy and degeneration of the hair cells at the base of the basilar membrane | Loss of high frequency sounds; condition does not interfere with speech discrimination |
| Neural | Loss of auditory nerve fibers | Condition affects ability to distinguish speech sounds in higher frequencies; does not affect ability to hear pure tones |
| Mechanical | Degeneration of the vibrating membrane within the cochlea | Condition leads to gradual loss of hearing in all frequencies; ability to distinguish sounds becomes increasingly difficult |
| Conductive hearing loss | Inability of the external ear to conduct sound waves to the inner ear; may be related to buildup of earwax, fluid accumulation in the middle ear, or upper respiratory infection | Condition can often be corrected by cleaning the ear, medications, or surgery; hearing aids or cochlear implants may be considered |
| Tinnitus | May be related to conductive or sensorineural loss, Ménière’s, otosclerosis, presbycusis, earwax buildup, lesions, or fluid in middle ear | Buzzing, ringing, whistle, roar in ears, most noticeable at night; may be necessary to rule out underlying conditions before implementing interventions designed to symptoms |
A sensorineural hearing loss may be unnoticed in the early stages because the high-frequency tones that are initially lost are above the functional range used in most environments. As the condition progresses, elders may notice that they cannot hear the ringing of the telephone, the buzz of the doorbell, the ticking of a clock, or the water dripping from a faucet. With further progression, the sounds of certain consonants such as s, z, t, f, and g become increasingly difficult to distinguish. Eventually, elders may strain to hear and understand conversations and one-syllable words.13,15
A second hearing condition, conductive hearing loss, results in an inability of the external ear to conduct sound waves to the inner ear. Conductive hearing losses may be related to the buildup of cerumen (earwax), fluid accumulation in the middle ear from eustachian tube dysfunction, or an upper respiratory infection. These conductive problems often can be corrected by cleaning the ear, administering medications, or performing surgery. Hearing aids may be effective for persons who have an untreatable or residual conductive hearing loss. A hearing aid amplifies incoming sound and requires functioning hair cells and an intact nerve to transmit the sound to the central auditory pathways. For older adults whose residual hearing is greatly limited because of an absence of hair cells, cochlear implants may be considered.4 Cochlear implants are appropriate when only minimal or no benefit is possible when a conventional hearing aid is used. Cochlear implants are prosthetic replacements for the functions of the lost hair cells by converting mechanical energy (sound waves) into electrical energy capable of exciting the auditory nerve. Cochlear implants are placed within the inner ear. They bypass the hair cells of the cochlea and directly stimulate the endings of the auditory nerve. The system consists of an external microphone, processor, and transmitter, and an internal receiver–stimulator and electrode. Figure 16-1 shows the external (Figure 16-1, A) and internal (Figure 16-1, B) placements for a cochlear implant.

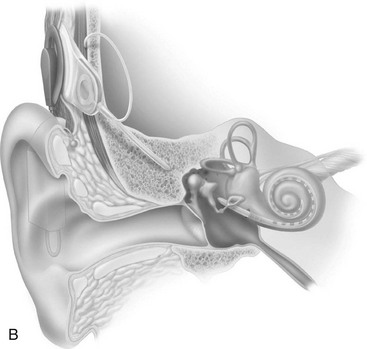
FIGURE 16-1 Cochlear implant. A, External placement. B, Internal placement.
(Courtesy of Cochlear Ltd, Englewood, CO.)
Tinnitus is a subjective auditory problem consisting of a ringing, whistling, buzzing, or roaring noise in the ears. Tinnitus may occur as part of a conductive or sensorineural hearing loss. It may also be associated with Ménière’s disease, otosclerosis, sensorineural loss, an accumulation of cerumen pressing on the eardrum, tympanic membrane lesions, and fluid in the middle ear. Medications such as the doses of aspirin prescribed for arthritis or other medical conditions can be additional contributing factors.15 Before planning interventions to mask the symptoms of tinnitus, possible underlying conditions such as cardiovascular disease, anemia, and hypothyroidism should be ruled out by a physician.
Tinnitus is often most noticeable at night when other noises are reduced. Ear or masking of environment noises may be an effective strategy. A radio, tape recording, or appropriate hearing aid may mask the tinnitus so the individual can fall asleep. Other therapeutic interventions may include relaxation techniques and biofeedback.2,15
Psychosocial Aspects of Hearing Impairments
Even though much information about the environment is learned through the sense of hearing, the importance of hearing during travel, while working, and in personal and social situations often goes unnoticed. Some researchers suggest that when hearing loss is the only loss elders experience, they can adjust well.13 Others suggest that a hearing loss may lead to isolation and even paranoia.2,17 Unfortunately, many elders experience other losses or lifestyle changes at the same time hearing loss occurs. Retirement may lead to a loss of role identity, income, and social contacts. Adjusting to the death of a spouse or undergoing changes in vision or mobility may take priority over a loss of hearing. Elders who are predisposed to loneliness or have difficulty in initiating or maintaining relationships may become more isolated or avoid interpersonal relationships if they experience a hearing loss. This can result in an increased sense of loneliness or isolation, especially if the hearing impairment is associated with other losses.13 Early assessment of a perceived hearing loss and recommendations for adaptations may help reduce an elder’s sense of loneliness.
The elder with a hearing loss often guesses at or misses the content of conversations, is reluctant to ask for clarification, or is embarrassed when mistakes are made because of a misunderstanding. This can occur when an elder with a hearing impairment is traveling. Studies involving elderly airline travelers have found that misunderstanding or not hearing overhead paging information has resulted in missed flights.18 Hearing changes also make it difficult to detect and understand speech in crowded and stressful situations. Limited hearing may decrease an elder’s sense of security and increase feelings of vulnerability, making travel more difficult. As a result, some elders may either limit their travel or stop engaging in that occupation.2
Communication can be exhausting for elders with a hearing impairment. For example, an 85-year-old man registering for occupational therapy (OT) interventions at a rehabilitation clinic will likely be embarrassed if he misinterprets the receptionist’s request for his address as a request to undress. He may also experience isolation if his accompanying family member interrupts and answers all remaining questions. Repeated frustrating and embarrassing experiences can contribute to feelings of vulnerability, insecurity, and doubts related to self-esteem that can lead to withdrawal from travel, social, cultural, and family contacts.
Some elders with hearing impairments may hear well at home and only struggle to hear in other social settings. Others may be isolated not only from family and friends but also from the broader world because they cannot get information from television, radio, movies, and even telephone conversations. Elders may become increasingly frustrated as family, friends, and even health care workers begin to make decisions for them.
An age-related hearing loss may only further complicate the effects of illnesses and mental health conditions such as Alzheimer’s disease. Hearing loss in elders can lead to or exacerbate paranoid ideas, suspicions, and loss of contact with reality, and related tendencies.13 Corso19 stated that a hearing loss can magnify previously existing paranoid personality attributes. Continued expression of suspicions, hostilities, and accusations of lying may result in friends and family members avoiding the hearing-impaired elder.
Rehabilitation and theHearing-Impaired Elder
Hearing loss usually accompanies other conditions and should be considered in intervention to facilitate a successful experience. Interventions based on the Occupational Therapy Practice Framework (2nd ed.)10 address areas of occupations that have value and meaning for elders.
Managing hearing loss is about much more than the simple provision of a hearing aid. Rehabilitation for the hearing-impaired individual examines the individual’s participation in a variety of activities and functions.20 The effectiveness of rehabilitation for maximizing occupational independence is based on many factors. Those related to hearing loss may include age-related changes at the time of onset of the hearing impairment, such as vision and mobility losses, retirement, death of a spouse, and loss of clearly defined life roles. Other factors include the severity and rapidity of the loss, the degree of residual hearing, the presence of other medical conditions, and the involvement of the individual and family members in the rehabilitative process.
COTA and registered occupational therapist (OTR) teams may work together along with others on the treatment team to identify elders who have hearing impairments through an observation of behaviors (Box 16-1). The Self-Rating Hearing Inventory also can be an effective tool for assessing the effects of a hearing impairment on perceived occupational performance.21 The American Academy of Otolaryngology–Head and Neck Surgery has developed a 5-minute hearing test to determine the need for a referral to a hearing specialist (Figure 16-2). Beyond the scope of therapy practice for more profound hearing losses, a consultation and referral to a hearing specialist regarding the use of a hearing aid, individual or computerized training in speech reading (lip reading), and instruction regarding the use of an ALD may be needed. In addition, referrals for accessing both formal and informal support services through public and community agencies may be beneficial. Individuals for whom none of these interventions are effective may be candidates for cochlear implants.
BOX 16-1
Observable Behaviors That May Indicate Hearing Loss
 Inappropriate volume increase when speaking—for example, appearing to shout while talking to a person nearby
Inappropriate volume increase when speaking—for example, appearing to shout while talking to a person nearby
Turning the television or radio volume inordinately high when there is no one else in the room and no noises in the background
Turning in a chair or turning the head to get a better hearing position when being addressed
Consistently asking for statements to be repeated
Not responding to verbal questions or conversation
Responding to verbal questions only when there is accompanying visual cueing
Looking disoriented or confused or giving inappropriate responses to questions—for example, answering “yes” to a multiple choice question
Answering questions addressed to another person when there are several persons conversing simultaneously in the same room
Withdrawing from social situations
Exhibiting short attention span, which is especially apparent when two people are talking simultaneously
Adapted from Kane, R. L., Ouslander, J. G., & Abrass, I. B. (1999). Essentials of Clinical Geriatrics, 4th ed. New York: McGraw-Hill.
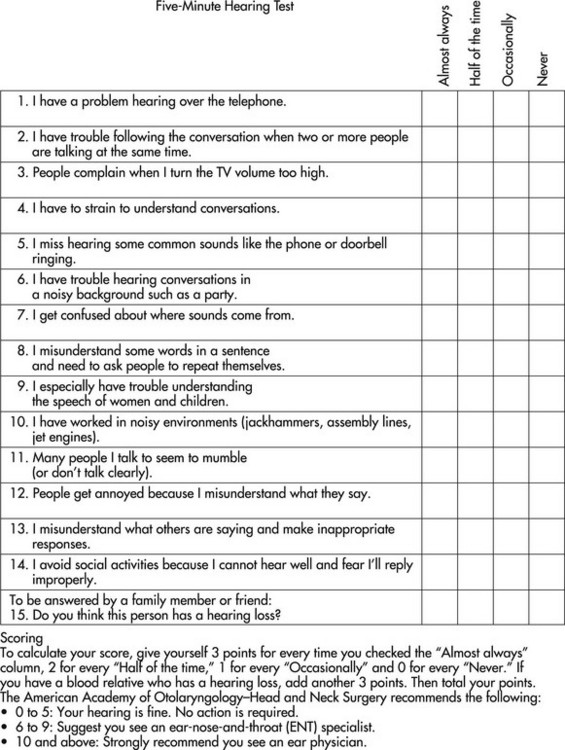
FIGURE 16-2 Five-minute hearing test.
(Courtesy of the American Academy of Otolaryngology–Head and Neck Surgery, Alexandria, VA.)
COTAs are involved in direct interventions for other primary reasons than for hearing impairment but regardless they should address hearing issues as they impact engagement in occupations. They may also assist in adapting environments for individuals, groups, or institutional facilities. The skills and experience of COTAs may be directed toward designing and implementing individual or institutional activities. These recommendations, intended to promote successful adaptation for hearing-impaired elders, also can assist families, friends, and institutional personnel. As always, safety is a consideration with intervention. Please refer to Box 16-2 for safety tips.
BOX 16-2
Safety Gems for the Hearing Impaired
Make sure that the elder’s hearing has been properly evaluated.
Check that hearing aids are working. This would be especially important during activities requiring hearing ability for safety, such as with driving.
Evaluate the person with a hearing deficit for fall risk. Consider balance and gait, and adapt the environment to prevent falls (e.g., remove clutter, increase lighting).
Instruct others to be aware that approaching hearing-impaired elders from the back may startle them and may cause loss of balance.
Encourage elders to discuss with their physicians and or pharmacists medications that may have side effects related to hearing issues, such as tinnitus.
Encourage elders to use vision (if vision is not a problem) as a compensatory safety aid in the environment. Teach scanning of the environment.
Problem solve with elders a safety plan for fires or other issues.
Use visual alert alarm systems (flashing lights) for awareness that someone is at the door, or that the phone is ringing.
For fire safety in a home or facility, consider installing visual alarms with strobe lights or vibration apparatuses. Vibrating beds or pillows can help awaken the person.
Data from National Institute on Aging. 2009. Hearing loss. Retrieved from http://www.nia.nih.gov/HealthInformation/Publications/hearing.htm; TriData Corporation. (1999). Fire risks for the deaf or hard of hearing. Retrieved from http://www.usfa.dhs.gov/downloads/pdf/publications/hearing.pdf; and White, M., Russell, D., Saisan, J., & Kemp, G. M. (2009). Senior driving safety tips, warning signs, and knowing when to stop. Retrieved from http://www.helpguide.org/elder/senior_citizen_driving.htm.
Recommendations for Improving Elder Communication
Psychosocial issues associated with hearing impairments often affect family members and friends, as well as the hearing-impaired elder. Information and education about the various types of age-related hearing losses and conditions may help COTAs in assisting elders to develop coping strategies.15 The COTA should encourage family members and friends to be involved in the education and consultation process so that conversational and environmental adaptations that encourage inclusion of the elder can be promoted.
Hearing-impaired elders may need to gain confidence in requesting adaptations that help them adjust to their hearing losses. Having elders role-play situations in which they request specific needs or adaptations may increase self-confidence for reentering social situations that they may have been avoiding.
Environmental adaptations should first center on identifying and minimizing the influence of background noises because competing background noises are considered to be a difficult listening condition.17 With a hearing difficulty, background noises greatly limit enjoyment of conversations and often contribute to an elder’s avoidance of social gatherings.22 Common sources of background noise in institutions include music, conversations on television or of persons in the room, dishes being clanked, fans in use, outside traffic, overhead intercoms in use, and ice machines in use. Personnel shifts and changes in the institutional environment may also create background noise.
COTAs can recommend environments that reduce background noise. Examples include going to restaurants during times that they are less crowded, requesting to sit in less crowded areas, or sitting away from distracting background noises such as kitchen traffic or music (Table 16-2). When traveling, to help compensate for difficulty in hearing overhead paging systems, elders can be encouraged to frequently check overhead flight monitors, or check in with airport staff, or both. Using theaters and church communities that offer ALDs that amplify specific sounds is another way to reduce interference from background noises in public spaces.
TABLE 16-2 Environmental Adaptations for the Hearing-Impaired Elder
| Problem | Intervention |
|---|---|
| Background noises | Add carpeting to floors, acoustical tiles to ceilings, and drapes on windows, and replace (institutional and home) wood and metal furniture with upholstered furniture. |
| Background noises | Hang banners from ceilings; add insulating sheetrock around kitchens, maintenance, and (institutional) mechanical areas; tighten window weather seals. In dining rooms, seat no more than four persons at a table and add padded room dividers between tables to absorb sound. On special care units, eliminate ringing telephones, televisions, and intercoms; serve meals in small groups; pass medications at times other than meal times. |
| Background noises | Go to restaurants at less crowded times; request to sit in areas (public places) away from music and kitchen. Seek out theaters and churches that offer listening devices to amplify specific sounds. |
| Communication | Position to reduce glare, add closed captioning, use assisted listening devices. Use remote controls (television, radio, music) to select programming, and alternate between music, television, and radio. |
Personal environmental modifications for reducing background noise include adding carpet to floors and acoustical tiles to ceilings, hanging drapes on windows, hanging banners from high ceilings, and replacing wood or metal furniture with upholstered furniture. Although these recommendations are intended to help absorb sound, they also can add aesthetic appeal to a home or institution.22
Additional interior modifications to reduce background noise within institutions include adding insulated sheetrock around noisy areas such as kitchen, maintenance, and mechanical areas, and tightening window weather seals. COTAs can assist individuals, families, and facility administrators in weighing the benefits of certain recommendations against the expenses of purchasing them. COTAs also can point out that, in some situations, background noises may provide helpful cues to locations of activity rooms, lounges, and beauty shops.
Environmental safety issues and concerns may center on the difficulties that hearing-impaired elders may have in locating the source of sounds in their home. The inability to locate sounds may contribute to a sense of insecurity in an individual’s own environment and to the possibility of auditory illusions. This can lead to a decrease in the person’s safety. For instance, elders may not be able to hear alarms or people moving about around them.15 Fire and smoke alarms tend to have high-pitched sounds that are difficult for persons with sensorineural losses to hear.4 Adding visual cues such as flashing lights is recommended for alarms.17 Flashing lights, lower-pitched rings, or low-toned musical chimes are also available options for telephones and doorbells. COTAs should recommend adapting telephones with volume and tone controls for persons who need these modifications. Cell (portable) phones, although convenient for some individuals, may add to the confusion and frustration for persons with hearing impairments. The ring of the phone may not be heard or the phones may be difficult to locate if needed for an emergency.23 Putting a cell phone on a vibration setting or trying text messaging with elders who can read the screen and have adequate finger dexterity might be a good communication option. Elders can download their own ring tone and set it on “loud” for recognition. Some cell phones can be adapted for hearing aids and for amplification of sound. Cell phones can also be adapted to be used with a TTY or Voice Carry Over devise.
Research indicates hearing loss can increase the individuals risk of falling when compared to individuals who are not hearing-impaired.3,24 Studies indicate that instruction in ways to substitute visual cues for hearing cues reduces the incidence of falls. COTAs also should make family members and health care providers aware that approaching hearing-impaired elders from the back and talking to and touching them may startle them and possibly cause them to lose balance. COTAs should recommend that hearing-impaired individuals be approached from the front, where visual contact can be made before beginning a conversation or expecting a response to a question.
To enhance conversations in areas where groups gather, COTAs should recommend that hearing-impaired individuals stay away from windows and plaster walls. Standing or sitting near soft materials that absorb sound, such as draperies, bookshelves, and upholstered furniture, also is recommended. Sitting in high-backed, upholstered chairs can help shield background noise. Focusing on the speaker’s lips during conversation can help increase comprehension. If an individual has more impairment in one ear than the other, the individual can find the position that maximizes hearing with the unaffected ear.13
For family members and friends who want to improve communication with hearing-impaired elders, COTAs should recommend that they position themselves in the elder’s field of vision and get the elder’s attention before speaking. While conversing, they should look directly at the elder, reduce the rate of speech, and speak distinctly with a low tone. Additional recommendations include asking the elder to repeat what was said and providing written instructions to reinforce verbal directions. COTAs should stress that a hearing impairment does not reduce an individual’s intelligence. Accommodations for the hearing impairment should not be over exaggerated or simplified to the point that elders with hearing loss feel that their intelligence or judgment is in question.
Because sensorineural hearing loss and its corresponding reduction in the ability to hear high-pitched sounds is the most common hearing disorder in elders, lowering the voice is especially important for women who address hearing-impaired elders. Increasing volume only increases tone and contributes to personal and social embarrassment (Box 16-3).
BOX 16-3
Communication Tips for Working with the Hearing Impaired
Face the elder so that the individual can see clearly your facial features with communication.
Speak to the elder in a well lit area. This helps the elder with a hearing impairment observe body language and facial expressions, all of which provide clues for understanding communication.
During conversations, limit background noise by turning off the radio or television.
In public places sit far away from the crowded or noisy areas.
Avoid communication when chewing food.
Speak somewhat in a louder tone than normal, but avoid shouting because that may distort speech.
Speak at a regular rate, not faster or slower, and do not overstress sounds.
Give the elder with hearing loss clues about the topic of conversation whenever possible.
Try to keep statements short and simple if the elder with hearing loss is struggling to understand the conversation. Repeat sentences as necessary.
Adapted from NIDCD. (2008). Presbycusis. National Institute on Deafness and Other Communication Disorders. Retrieved from http://www.nidcd.nih.gov/health/hearing/presbycusis.asp.
In restaurants and institutional dining rooms, seating no more than four persons at a table so eye contact can be easily made can enhance the social aspects derived from conversations during meals. In larger dining rooms, padded room dividers between tables can absorb sounds from surrounding tables. General recommendations regarding reduction of background noises also should be considered.
The effects of glare on the visual and nonverbal cues that enhance auditory communication should be considered when speaking with hearing-impaired elders. Sources of glare may include windows, lights, and glass surfaces either from behind the person speaking or reflected from eyeglasses. Before beginning a conversation, the COTA, family member, or friend should adjust blinds or shades, adjust lighting, and reposition seating arrangements as needed (see Chapter 15 for more information on visual adaptations with aging).
Entertainment through television, music, websites with sounds on the internet, and radio offers opportunities for stimulation that are not dependent on other people. When elders control the times and selections for television and radio programs and music, the cognitive stimulation can be rewarding. When televisions and radios are on constantly or programs selected are not those the elder would choose, they become an additional source of background noise rather than a source of stimulation.4,23 Closed-captioned television is an additional option to suggest. COTAs should identify and reduce sources of glare on the screen when positioning elders for television viewing. ALDs offer a means of controlling the volume for the hearing-impaired elder without disturbing others. Adjusting the volume and sound for music for those individuals with sensorineural hearing loss requires increasing the bass and decreasing the treble. Developments in technology have made the cost of these devices quite reasonable when weighed against the potential benefits.23 Refer to Table 16-2 for ideas for environmental adaptations.
Providing Assistive Hearing Devices
One of the most common assistive devices for persons with a hearing impairment is a hearing aid. An audiologist assists in determining whether a hearing aid would be appropriate. If a hearing aid would be beneficial, the audiologist works with the individual to choose the type of hearing aid that will maximize the individual’s hearing and understanding of speech based on the individual’s type of hearing loss.12 Additionally, the audiologist also determines whether other factors associated with aging, lifestyle, and personality are compatible with a hearing aid. COTAs may refer elders to a physician or audiologist for assessment and evaluation. Advise patients to find out whether insurance will cover the cost of a hearing aid, and tell patients to ask whether a trial period is allowed so that the product can be tried out before it is purchased. Several visits to an audiologist may be required to get everything correct so the device is comfortable and the individual is comfortable using the hearing aid.25
Recent improvements in hearing aid technology have made hearing aids more acceptable. The improved devices are smaller and fit in the ear and therefore are more cosmetically appealing (Figure 16-3). In addition, hearing aids dampen certain frequencies. Some evidence indicates that younger individuals report more satisfaction than do elders with hearing aids.26-28 This increased satisfaction may result from several factors. The onset of age-related hearing loss is often gradual, and elders may have accommodated to their hearing loss over an extended period, eventually finding the sudden amplification of all sound to be invasive and disturbing. In addition, the fine finger-and-hand dexterity required to manipulate volume and frequency controls and change batteries makes the hearing aid difficult to operate. Possible cognitive changes and short-term memory loss may affect the elder’s ability to remember to turn the device on and off. The cost of replacement batteries and the elder’s acceptance of new technologies are other factors to consider when determining the appropriateness of a hearing aid.23,28 Goals for an elder who uses a hearing aid may include identifying alternative ways of operating it, building handles for tools used with the controls, changing or testing batteries with less difficulty, and learning the proper way to insert the device. (See the Appendix for additional information on hearing aids.)

(From Bingham, B. J. G., Hawke, M., & Kwok, P. [1991]. Atlas of clinical otolaryngology. St. Louis, MO: Mosby.)
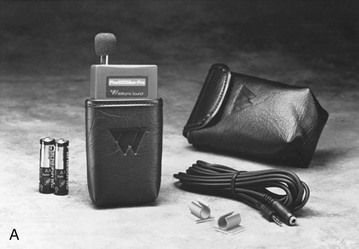
Even with improved technology, hearing aids may not be effective for some individuals. For others, sound distortions may be louder with a hearing aid. When hearing aids are not effective, ALDs may be used. ALDs consist of a microphone to capture spoken sounds, an amplifier to increase sound volume, and a headset worn by the hearing-impaired person (Figure 16-4, A and B). Because the amplified sound from an ALD reaches the ear directly, background noises are reduced.29 ALDs can augment hearing in a noisy clinic or hospital room. When an ALD is plugged into a television, the sound is amplified for the hearing-impaired person only. Use of an ALD also should be considered when visual impairment does not allow the elder to read lips or to supplement hearing loss by responding to other nonverbal cues. In addition to ALDs, there are some newer options for the hearing impaired such as computer assisted real-time transcription (CART), visual and tactile alarms, and volume controlled or caption phones.30 COTAs can inform the elder with a hearing impairment about Telecommunications Relay Services. These services available throughout the United States allow the person to place telephone calls with the use of computers or other technology. Operators (communication assistants) facilitate these calls by converting text to voice or vice versa. There is a variety of methods available to do this type of telephone communication to meet the needs of the hearing-impaired population.31

Conclusion
As the number of elders with hearing impairments increases, the challenges and opportunities for COTAs continue to grow. The occupational performance and psychosocial and environmental issues that surround a hearing impairment demand that COTAs are informed and able to recommend appropriate interventions. COTAs can assist elders in attaining both performance and quality of life expectations by identifying limitations in hearing, referring elders for additional evaluation and intervention, and providing appropriate interventions.
Case Study
Joe is an 89-year-old man who has resided at the Garden View Nursing Home for the past 7 years. His diagnoses include dementia (early stages), diabetes, congestive heart failure, and most recently an increase in hearing loss. Until recently, Joe’s social history had been active and included participation in recreational activities and daily socializing with staff and other patients. At a recent care conference, the recreation director reported that Joe’s participation in activity groups had decreased from nine to four groups a week. The nurse working with Joe stated that he was less social during meals and had started to sleep in the afternoons. The social worker shared her current assessments of Joe and stated that he seemed to be isolating himself from others, including his roommate. When the social worker and other staff asked him how he was doing, he seemed to have difficulty understanding the question and changed the subject to talk about the weather. The staff thought his dementia could be contributing to the confusion or perhaps to changes in the level of his hearing loss. The team recommended referrals for a professional hearing evaluation and an OT assessment. The referral for OT included an evaluation of Joe’s current level of occupational functioning and suggestions for adapting his environment. In addition, staff was seeking suggestions from OT on how staff and others might interact more effectively with Joe. The OTR is a new graduate and has been at the Garden View Nursing Home for 2 months only. She has asked the COTA who has worked at the nursing home for 5 of the 7 years that Joe has been a resident at the home to assist her with the assessment.
Case Study Questions
1. Using information from the case study and the chapter, identify why staff would think that Joe’s hearing loss might have an effect on his social interaction with others.
2. Describe how Joe’s recent decrease in social interaction may be influencing his mood.
3. As the long-standing COTA member of the OT department, what assistance can you provide for the OTR? For Joe?
4. Using information from the chapter, identify assessments that may be useful for Joe.
5. What recommendations would you consider to adapt Joe’s environment to make it more purposeful and accommodating for him?
6. What types of assistive devices would be considered for Joe?
7. You have been asked to prepare an in-service on hearing impairments and elders and provide recommendations that will assist all staff to be more effective when interacting with those who have a hearing impairment.
1. Referring to the chapter, what are some age-related hearing changes in elders?
2. How do age-related hearing impairments in elders affect their communication and socialization skills, as well as their safety?
3. How can COTAs contribute to improving communication and socialization skills in hearing-impaired elders?
4. What safety concerns should COTAs be aware of when working with an elder who has a hearing impairment?
5. What environmental modifications can COTAs suggest to reduce background noises in an elder’s home?
6. What environmental modifications in an institution might be used to reduce confusion caused by hearing impairments?
7. Why might an elder prefer not to use a hearing aid?
8. Explain how a cochlear implant would improve the hearing of some elders?
9. How might a COTA use an ALD to help an elder in a clinic setting?
1 Grue E.V., Ranhoff A.H., Noro A., Finne-Soveri H., Jensdóttir A.B., Ljunggren G., et al. Vision and hearing impairments and their associations with falling and loss of instrumental activities in daily living in acute hospitalized older persons in five Nordic hospitals. Scandinavian Journal of Caring Sciences. 2009;23(4):635-643.
2 Garstecki D.C., Erler S.F. Hearing and aging. Topics in Geriatric Rehabilitation. 1998;14(2):1-17.
3 Tobis J.S., Block M., Steinhaus-Donham C., Reinsch S., Tamaru K., Weil D. Falling among the sensorially impaired elderly. Archives of Physical Medicine and Rehabilitation. 1990;71(2):144.
4 Hooper C.R. Sensory and sensory integrative development. In: Bonder B.R., Wagner M.B., editors. Functional Performance in Older Adults. Philadelphia: FA Davis, 2001.
5 Johnson C., Danhauer J., Bennet M., Harrison J. Systematic review of physicians’ knowledge of, participation in, and attitudes toward hearing and balance screening in the elderly population. Seminars in Hearing. 2009;30(3):193-206.
6 Kochkin S. MarkeTrak VII: Hearing loss population tops 31 million people. Hearing Review. 2005;12(7):16-29.
7 U.S. Department of Health and Human Services. Office of Disease Prevention and Health Promotion. Healthy People 2010. Retrieved from n.d. http://www.healthypeople.gov/document/HTML/Volume2/28Vision.htm
8 NIH Senior Health. Hearing loss. National Institutes of Health. Retrieved from http://nihseniorhealth.gov/hearingloss/toc.html, 2009.
9 Lichtenstein M.J., Bess F.H., Logan S.A. Screening the elderly for hearing impairment. In: Ripich D., editor. Handbook of Geriatric Communication Disorders. Austin, TX: Pro-Ed, 1991.
10 American Occupational Therapy Association. Occupational therapy practice framework: Domain and process, 2nd ed. American Journal of Occupational Therapy. 2008;62:625-683.
11 Meriano C., Latella D. Occupational Therapy Interventions: Function and Occupations. Thorofare, NJ: Slack; 2007.
12 NIDCD. Presbycusis. National Institute on Deafness and Other Communication Disorders. Retrieved from http://www.nidcd.nih.gov/health/hearing/presbycusis.asp, 2008.
13 Cherney L.R. The effects of aging on communication. In Lewis C.B., editor: Aging: The Health Care Challenge, 4th ed, Philadelphia: FA Davis, 2002.
14 Burkhalter C.L., Allen R.S., Skaar D.C., Crittenden J., Burgio L.D. Examining the effectiveness of traditional audiological assessments for nursing home residents with dementia-related behaviors. Journal of the American Academy of Audiology. 2009;20(9):529-538.
15 Hooper C.R., Bello-Haas V.D. Sensory and sensory integrative development. In: Bonder B.R., Bello-Haas V.D., editors. Functional Performance in Older Adults. Philadelphia: FA Davis, 2008.
16 Vogel I., Brug J., van der Ploeg C., Ratt H. Strategies for the prevention of MP3-induced hearing loss among adolescents: Expert opinions from a Delphi study. Pediatrics. 2009;123(5):1257-1262.
17 Bance M. Hearing and aging. Canadian Medical Association Journal. 2007;176(7):925-927.
18 Canadian Transportation Agency. A look at barriers to communication facing persons with disabilities who travel by air [WWW page]. URL http://www.cta-otc.gc.ca/air-aerien/mdex_e.html, 1997.
19 Corso J.F. Sensory-perceptual processes and aging. In Schaie K.W., Eisdorfer C., editors: Annual Review of Gerontology, 2nd ed, New York: Springer, 1990.
20 Howarth A., Shone G.R. Ageing and the auditory system. Postgraduate Medicine. 2006;82(1):166-171.
21 Janken J.K., Cullinan C.L. Auditory, sensory, and perceptual alteration: Suggested revision of defining characteristics. Nursing Diagnosis. 1990;1(4):147.
22 Christenson M.A., Taira E. Aging in the Designed Environment. New York: Haworth Press; 1990.
23 Stach B.A., Stoner W.R. Sensory aids for the hearing impaired elderly. In: Ripich D., editor. Handbook of Geriatric Communication Disorders. Austin, TX: Pro-Ed, 1991.
24 Kulmala J., Viljanen A., Sipilä S., Pajala S., Pärssinen O., Kauppinen M., et al. Poor vision accompanied with other sensory impairments as a predictor of falls in older women. Age and Ageing. 2009;38:162-167.
25 National Institute on Aging. Hearing loss. Retrieved from http://www.nia.nih.gov/HealthInformation/Publications/hearing.htm, 2009.
26 Kane R.L., Ouslander J.G., Abrass I.B. Essentials of Clinical Geriatrics, 4th ed. New York: McGraw-Hill; 1989.
27 Rieske R.J., Hostege H. Growing Older in America. New York: McGraw-Hill; 1996.
28 Stoneham M.A. Technology and disability. Andover Medica. 1994;13(1):47.
29 American Speech-Language-Hearing Association. Hearing assistive technology. Retrieved from http://www.asha.org/public/hearing/treatment/assist_tech.htm, 2009.
30 Hearing Loss Association of America. Assessability. Retrieved from n.d. http://www.hearingloss.org/advocacy/accessibility.asp
31 Federal Communications Commission. Telecommunications Relay Services. Retrieved from n.d. http://www.fcc.gov/cgb/consumerfacts/trs.html