chapter 15 Working with Elders Who Have Vision Impairments
1. Describe typical physiological changes affecting vision that occur with aging.
2. Name and describe the major ocular diseases affecting vision in elders.
3. Describe common vision deficits resulting from neurological insults in elders.
4. Describe psychosocial implications of vision impairments in elders, possible effects on rehabilitation, and on functional outcomes.
5. Describe the use of the Occupational Therapy Practice Framework’s1 dynamic, interactive process of evaluation, intervention, and outcomes to address functional deficits in elder clients resulting from visual impairments.
6. Identify general principles to enhance vision.
7. Identify environmental or contextual considerations and interventions to increase independence and safety in elders with low vision.
8. Identify general principles in intervention of visual dysfunction after brain insult.
9. Identify team members and community resources that registered occupational therapists (OTRs) and certified occupational therapy assistants (COTAs) may collaborate with to improve functional outcomes in elders with low vision.
cataracts, glaucoma, retina, lens, macular degeneration, diabetic retinopathy, visual acuity, contrast sensitivity, visual cognition, visual memory, pattern recognition, scanning, visual attention, oculomotor control, visual fields, eccentric viewing, scotoma, hemi-inattention, diplopia, strabismus
Case Study
Mrs. N. is an 82-year-old widow who lived alone in the two-story home that she shared with her husband for more than 50 years. At a visit to her ophthalmologist, she was told that her complaints of blurry vision with reading the mail and newspaper were due to dry macular degeneration, and that new glasses would not help her. The ophthalmologist informed her that there was nothing he could do to correct her condition.
Mrs. N. is now at a subacute rehabilitation facility following a recent knee replacement surgery, and the OTR/COTA team has been ordered to follow her. She tells them that she is a little afraid to be at home alone. She is having trouble seeing her appliance controls and the phone dial. Between her new knee replacement and her vision loss, she does not know whether she can navigate the steps in her home. She is nervous about going outdoors because she is having trouble seeing curbs and changes in walking surfaces, especially at dusk or on hazy days. She feels isolated and lonely. Her children are wondering whether she will be able to return home.
Case Study Questions
Before reading the chapter, consider your own preconceptions about vision loss.
1. Do you think someone with partial sight, like Mrs. N., can function independently?
2. What would you do if you, like Mrs. N, could not read regular print, street signs, or the controls on your appliances?
3. If you were suddenly unable to do the things mentioned previously, list three specific activities with which you might experience difficulty.
4. Now, choose one of the activities you listed and try to complete it in a darkened room or with your vision partially obscured. Have someone time you while you do it. Afterward answer the following questions:
5. What feelings did you experience as you tried to complete the activity? Frustration? Irritation? Embarrassment?
6. Did it take you longer to complete the activity than it would without partially obscuring your vision?
7. Did you have to use other senses or make adaptations to complete the activity?
Visual impairments are common in the elderly population. One in six adults age 65 and older has a visual impairment, and this number is expected to double by the year 2030.2 The odds of developing visual impairment worsen with age, as one in four adults age 75 years or older experiences either a moderate or severe visual impairment.3 In addition to vision loss from ocular disease, many adults are affected by visual impairments resulting from head trauma, stroke, or neurological insult. Between 40% and 75% of individuals with head trauma or stroke are estimated to experience visual impairments requiring rehabilitation.4 According to the Occupational Therapy Practice Framework: Domain and Process (2nd Ed.), seeing and related functions are addressed in the clients factors table as a body function under the sensory functions and pain category, and visual is listed in the Performance Skills table as a sensory perceptual skill.1 These statistics along with the inclusion of vision in the Occupational Therapy Practice Framework1 demonstrate the need for COTAs to possess a thorough understanding of the causes of vision loss and appropriate intervention techniques. Regardless of the particular setting, any COTA working with elders is likely to encounter many clients with visual impairments.
This chapter will provide information on the psychosocial effects of vision loss, effects of normal aging on vision, common conditions causing vision loss in elders, and visual dysfunction after neurological insult. The chapter also addresses the process for assessing elder clients’ occupational performance and outcomes as well as general principles used in planning interventions to help elder clients achieve their functional goals. OTRs and COTAs function as part of a team that includes physicians, other health care providers, family/caregivers, and the elder client. The chapter addresses the roles of these team members and community resources.
Psychosocial Effects of Vision Impairment
Almost 25% of adults with visual impairment report symptoms of depression compared with 10% of those without visual impairment.5 The thought of losing one’s vision is one of the most devastating disabilities imaginable. Without vision, the ability to perform many of the daily activities normally taken for granted is lost. Without vision, a means of social connectedness is lost because it is no longer possible to make eye contact or to read subtle facial expressions. The thought of vision loss conjures up a terrifying world of blackness. However, although most people think of vision loss as total blindness, most individuals with visual impairments are not totally blind. In fact, in one report, 80% of those who reported being legally blind had some degree of usable vision.6 It is often difficult for family members, friends, and the general public to understand the limitations and capabilities of those with partial sight.7 It is not uncommon for partially sighted individuals to be labeled as “fakes” when others observe that they are capable of one task that requires some degree of vision but are incapable of another task.7 This confusion about the abilities of those with partial sight may produce more psychological distress than does total blindness.7
In addition to the ambiguity associated with being partially sighted, individuals often find it difficult to adjust to their vision loss because of the uncertainty of their condition. For many, it is difficult to know whether their vision will improve, stay the same, or get worse. There is often an internal struggle with a desire to be independent and the desire to be taken care of. In some situations, elders may want assistance but feel unable to ask for it. Elders struggling with vision loss may experience mood swings. Friedman7 describes the stages of coping that individuals with vision loss experience as closely paralleling those that Kubler-Ross8 describes in her study on death and dying. These stages include initial shock and denial, then guilt, bargaining, anger, depression, and, finally, adaptation.
Perski9 describes a similar response of adaptation when he writes about the five-stage process of being a successful low vision patient. Perski9 notes “there are definite psychological stages that many persons go through before they become a successful user of visual aids. Probably the first harsh reality that a low vision person must face is that a single pair of glasses will not help his or her vision. The reality that the person must hold a magnifying glass or use separate reading glasses and hold materials very close to his or her eye is often too much to bear.”
Effects of the Normal Aging Process on Vision
Although elders are more likely to experience visual impairments because of some specific ocular and neurological pathologies, they also experience many age-related changes that affect visual functioning. These normal changes must be taken into consideration when working with this population.
The retina is a multilayered lining of neural tissue on the innermost part of the eye (Figure 15-1). It receives visual messages and transmits them through the optic nerve to the brain.10 The central area of the retina, or macula, has a concentration of cone cells that enable color vision and fine-detail discrimination. Rod cells are extremely sensitive to light and provide peripheral vision and night vision.10 As the retina ages, it gradually loses neurons. Central or peripheral vision may be affected, depending on which retinal neurons die. The rate of retinal deterioration and the resultant visual field loss vary among individuals, but, generally, elders experience shrinkage of the peripheral field, experience difficulty with light and dark adaptation, and require increased time to switch from viewing near objects to far objects (accommodation) and to recover from glare. Because pupil size and function decrease with age, elders require more illumination for fine-detail tasks.11 Many elders require three times more light than a person requires in his or her twenties or thirties.12
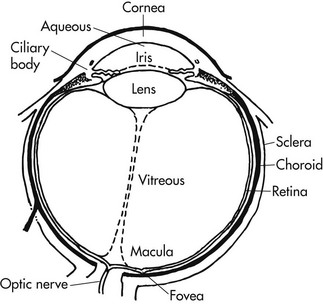
Changes may also occur in the lens of the eye with age (see Figure 15-1). The lens is responsible for properly focusing the image on the retina. It does this by changing shape according to the distance of the object being viewed.13 As the lens ages, it loses some of its elasticity, making shape change or accommodation more difficult. This condition, called presbyopia, affects focal ability at near distances, making it difficult to read print or perform close-vision tasks.14 The greatest change usually occurs between ages 40 and 45 years.14 Reading glasses or bifocals are often prescribed at this time. In addition to this loss of elasticity, the lens also becomes yellower with age. This deeper yellow can affect the ability to differentiate between colors and discriminate objects with low contrast.15
Specific Ocular Pathologies
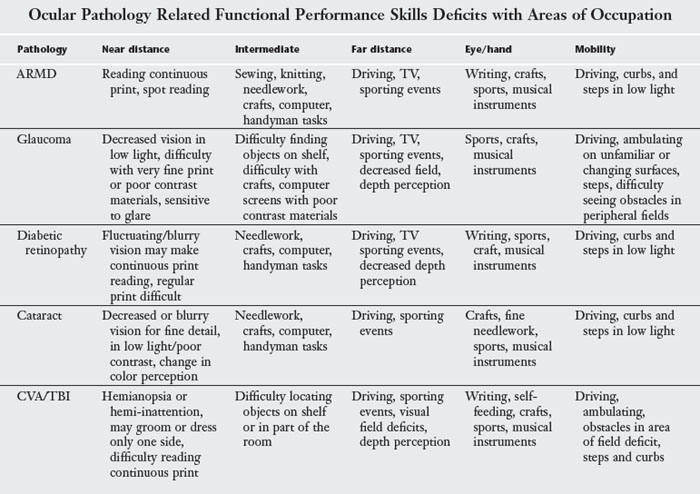
In addition to the natural aging process, specific pathological eye conditions have a more profound effect on functional visual abilities. Four major conditions that affect an elder’s vision are cataracts, age-related macular degeneration (wet or dry), glaucoma, and diabetic retinopathy. Each of these conditions can cause visual impairment when they occur in isolation, but they commonly co-occur in elders, increasing the challenge to remain functionally independent (Table 15-1). More about general intervention ideas for any ocular condition will be presented later in the chapter.
TABLE 15-1 Changes in Visual System Associated with Age
| Structural component | Age-related change | Functional implications |
|---|---|---|
| Cornea | Decreased fluid bathing cornea | Dryness, irritation |
| Accumulation of lipids | Increased astigmatism with increased blurring of vision | |
| Iris | Decreased permeability | May contribute to glaucoma |
| Ciliary muscles | Atrophy of muscles | Decreased mobility of lens causing decreased muscle effectiveness |
| Pupil | Decreased pupil size | Decreased light reaching retina; difficulty seeing dark objects or objects in dim light |
| Decreased papillary reflex | Decreased dark adaptation and recovery from glare | |
| Lens | Lens growth | Decreased accommodative ability |
| Decreased refractive index of lenses | Uneven refracture properties can result in double vision in one eye | |
| Yellowing | Reduced amount of light reaching retina, changes in light composition alters color vision | |
| Vitreous | Contracts | Increased chance of separation from retina or retinal detachment |
Adapted from Zoltan, B. (2006). Vision, Perception, and Cognition: A Manual for the Evaluation and Treatment of the Adult with Acquired Brain Injury, 4th ed. Thorofare, NJ: Slack.
Cataracts
A cataract is a clouding of the lens, the clear part of the eye that helps focus light, or an image on the retina. This clouding is related to aging and changes in the protein that, along with water, make up the lens. Protein clumps up in the lens, forming cataracts, which make vision blurry and dull by preventing adequate amounts of light from reaching the retina.16 Cataracts can be treated successfully with surgery and are no longer considered to be a major cause of permanent visual impairment in developed countries. The most common procedure is the removal of the opacified lens followed by the insertion of an intraocular lens implant.17
If an elder is struggling with cataracts before surgery or if the elder is not a surgical candidate, interventions that control glare, increase lighting, and low levels of magnification can be helpful.
Macular Degeneration or Age-Related Macular Degeneration (ARMD)
Macular degeneration is the leading cause of vision loss in older Americans.18 The macula is the central portion of the retina where the clearest vision is found. There are two types of macular degeneration: the “dry” (non-exudative or atrophic) type and the “wet” (exudative or hemorrhagic type). Dry age-related macular degeneration (ARMD) is the result of yellowish deposits, or drusen, forming under the macula. This causes the macula to thin and dry out. As cells on the macula become non-functioning, elders experience a blurry, dark, or blank spot in the center of their visual field. The wet form of ARMD is caused by the rapid growth of small blood vessels beneath the macula. These blood vessels leak and cause scarring on the macula, resulting in vision loss.18 The wet form of ARMD can sometimes be treated with photocoagulation, laser surgery, or, more recently and effectively, by intraocular injection with Macugen, Lucentis, or Avastin (drugs that dry up the leaking blood vessels and slow their regrowth). Results of the Age-Related Eye Disease Studies (AREDS) suggest that progression of dry ARMD can be slowed by the intake of anti-oxidant supplements.19 Current interventions can slow the rate of vision loss; however, there is no known intervention that prevents macular degeneration or that can reverse the loss of vision.19 Because peripheral visual fields are usually spared, ARMD does not result in total blindness.18
Common problems experienced by elders with ARMD include difficulty distinguishing faces, reading signs, or seeing traffic signals (distance tasks), or reading regular print, writing, and doing needlework (near tasks). Elders with wet ARMD often experience distortion of the central visual field that may make straight lines appear wavy (metamorphopsia). This distortion can lead to balance and mobility problems. Visual hallucinations as a result of Charles Bonnet syndrome are sometimes experienced by elders with ARMD. The hallmark of these hallucinations is that they occur and disappear spontaneously with no known external cause, and they are recognized as unreal by the elder and are nonthreatening. Some elders have described seeing “fields of flowers in my living room,” animals, or even people across the room.20 Elders experiencing Charles Bonnet syndrome may be reluctant to discuss their visual symptoms, fearing a label of mental instability or decreased cognitive function. They need to be reassured that this is not the case. Charles Bonnet syndrome has been found to affect elders with ARMD with severe loss of contrast sensitivity in both eyes.21 COTAs working with elders who have macular degeneration should be aware of specific interventions for this diagnosis (Box 15-1).
BOX 15-1 Intervention Gems for Individuals with Macular Degeneration
Elders with macular degeneration usually experience problems with loss of detail, central vision early in their vision loss. Peripheral vision is usually spared, even in more advanced stages.
 Lighting—provide training with different types of task lighting: full spectrum incandescent, fluorescent, halogen, and LED as well as positioning of lighting source so that the elder can identify which one is preferred for an activity.
Lighting—provide training with different types of task lighting: full spectrum incandescent, fluorescent, halogen, and LED as well as positioning of lighting source so that the elder can identify which one is preferred for an activity.
Reduce glare in the elder’s environment by eliminating bare or exposed light bulbs and highly polished or reflective surfaces; use light diffusing shades, blinds or curtains, and careful placement of furniture.
Use color and contrast in the elder’s environment to define objects and surfaces—a contrasting colored towel, draped on a chair can make it easier to see.
Increase object size—large numbered phones, kitchen timers, medicine organizers, large print checks make ADL easier to complete with decreased central or detail vision.
Decrease clutter, including visual clutter—clear paths from room to room and in front of furniture, counters, and appliances. Limit the number of items on countertops and tables. Limit use of bold patterns, which create visual clutter.
Magnification—when possible, elders will need referral to a low-vision ophthalmologist or optometrist to prescribe the appropriate magnification devices for near, intermediate, and distance activities. However, magnifying lamps, nail clippers with attached low powered magnifiers, and inexpensive low powered magnifiers for craft and sewing may allow the elder to complete activities with decreased vision.
Transportation options—train elders in use of alternative transportation. Many communities have paratransit systems for individuals who cannot drive or use conventional public transportation safely. Some communities offer reduced fare taxi programs for the visually impaired.
Glaucoma
Glaucoma is a group of serious ocular conditions that involve excessively high pressure inside the eyeball. This increased pressure results from a buildup of excess fluid in the eye.10 Increased intraocular pressure can eventually cause damage to the optic nerve or the blood vessels that supply the optic nerve.10 One of the first effects of this optic nerve damage is usually a loss of vision in the peripheral field (Figure 15-2). This loss of peripheral vision is often not noticed by the individual initially, and the disease frequently progresses substantially before it is noticed.22 If left undetected and untreated, this loss can lead to total blindness. Elders should be encouraged to have routine ophthalmologic visits so that glaucoma may be diagnosed at an early stage. When the diagnosis is early, individuals respond well to medication and, if necessary, surgery to improve the balance of fluid in the eye.10
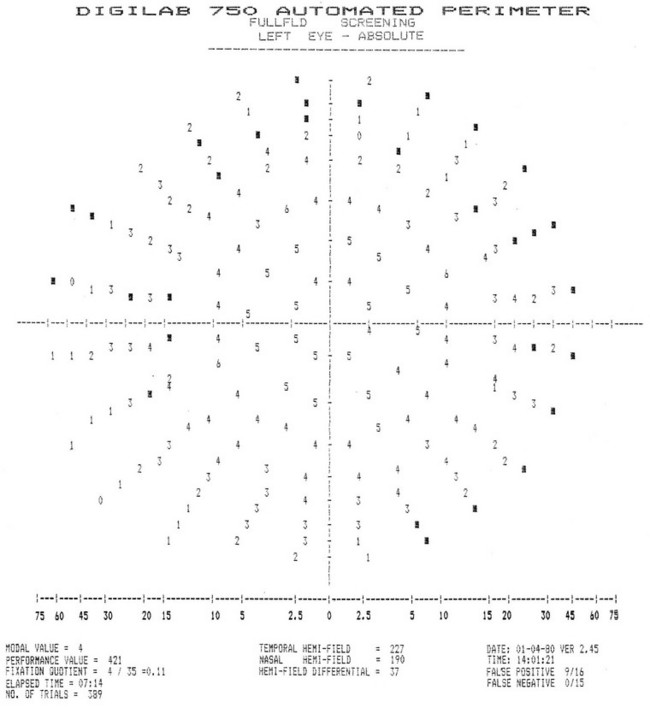
FIGURE 15-2 This printout from an automated perimeter test indicates visual loss in points marked with black squares. Note the peripheral distribution.
There are many types of glaucoma, but open-angle is the most common.10 Other types include closed-angle or narrow angle, traumatic, and low-tension glaucoma.10 Open-angle glaucoma involves an eye with normal anatomy that, for unknown reasons, is not able to drain the fluid as efficiently as it produces it. This leads to a slow, gradual buildup of intraocular pressure over time.10
Closed, or narrow-angle, glaucoma is less common. This type of glaucoma progresses rapidly, and symptoms are immediately apparent. Nausea, headaches, severe redness of the eye, and pain may be symptoms of an acute attack of narrow-angle glaucoma.23 Emergency surgery is often required to reduce the intraocular pressure.
The functional implications of glaucoma vary greatly, depending on the severity of the disease. When diagnosis is early, glaucoma can be treated and many people may have little need to adjust their lifestyles. If the disease is allowed to progress, individuals may experience decreased peripheral vision, difficulty adjusting to changing light, fluctuating and blurred vision, shadow-like halos around lights, and an increased sensitivity to glare.24,25 If glaucoma goes undiagnosed, a person may lose all of his or her vision beginning with the peripheral field and eventually extending into the central visual field. Mobility and safety can be severely compromised in elders with advanced glaucoma. Referral to an orientation and mobility teacher may be appropriate for an elder experiencing decreased mobility because of vision loss at this stage. COTAs working with elders who have glaucoma should be aware of specific interventions for this diagnosis (Box 15-2).
BOX 15-2 Intervention Gems for Individuals with Glaucoma
Most individuals with glaucoma do not experience problems with their vision until their disease is relatively advanced.
Medication management is vital—train client in nonvisual techniques, labeling, organization, talking labels, and talking reminders or alarms for self-administering oral medicines and eye drops.
Mobility problems (due to reduced peripheral vision)—address by use of contrast, reduce clutter/tripping hazards, train awareness of boundaries, and edges in environment; refer to orientation and mobility specialist for long cane (white cane) and nonsighted techniques for community mobility.
Contrast and glare—Use of yellow, amber, or light plum glasses to increase contrast, decrease glare. Reduce reflective surfaces (glass tabletops, mirrors, highly polished floors, or counters), cover exposed light bulbs, windows, and angle task light sources to decrease glare.
Low-power magnifiers—may help for small print or poor contrast materials.
Increase object size for ease of identification.
Bright colored objects will stand out if client has decreased contrast sensitivity.
Organized scanning patterns—train client to scan in horizontal left to right, zig-zag, and circular patterns to locate obstacles, edges, and objects in their reduced visual field.
Diabetic Retinopathy
Diabetic retinopathy, one of the complications of diabetes mellitus, is another leading cause of visual impairment in elders. Diabetic retinopathy has four stages: (1) mild nonproliferative retinopathy, the earliest stage in which microaneurysms occur as a small ballooning in the tiny vessels of the retina19; (2) moderate nonproliferative retinopathy, during which some blood vessels that nourish the retina are blocked; (3) severe nonproliferative retinopathy, during which many blood vessels are blocked, depriving areas of the retina of their blood supply (this causes the growth of new blood vessels to nourish the retina, leading to the next stage); and (4) proliferative retinopathy. In this most advanced stage, new blood vessels grow along the retina and along the surface of the vitreous gel that fills the inside of the eye. The new blood vessels are abnormal, with fragile walls that may leak and cause more severe changes in visual acuity. The new network of vessels and its accompanying fibrous tissue contract, and the vitreous may pull away from the retina causing further hemorrhage into the vitreous. This can also cause a retinal detachment, a serious condition requiring immediate attention and surgery to prevent vision loss.19 If fluid leaks into the center of the macula, swelling and blurred vision can occur. This condition, known as macular edema, can happen at any stage of diabetic retinopathy, causing a significant distortion and loss of vision.19
Diabetic retinopathy may be treated either by photocoagulation, injection (similar to procedures used to treat wet macular degeneration), or a procedure known as vitrectomy, during which blood is removed from the vitreous of the eye with a needle and replaced by saline solution. Many people experience improved vision after these procedures, but they do not cure diabetic retinopathy. The risk of new bleeding and vision loss remains.19
Functional implications of diabetic retinopathy, like glaucoma, vary depending on early diagnosis and severity of the disease. Some individuals with mild retinopathy may not need to make adaptations in their performance patterns, whereas others may need to learn adaptive techniques to compensate for vision loss to continue to perform activities of daily living (ADL) safely and independently. Many elders who have advanced diabetic retinopathy experience decreased contrast sensitivity, poor night vision, and fluctuating, blurry or spotty vision. Some elders may eventually need to learn nonsighted techniques for all ADL. COTAs working with elders who have diabetic retinopathy should be aware of specific interventions for this diagnosis (Box 15-3).
BOX 15-3 Intervention Gems for Individuals with Diabetic Retinopathy
Diabetic retinopathy often causes blurriness, fluctuations in vision, and may sometimes result in either central or peripheral field loss.
Medication management may require referral to a diabetes educator. Consider talking glucometers, pre-filled syringes, syringe magnifiers, insulin “pens,” large print logs for recording blood glucose readings, insulin dosage counters, and other adaptive equipment.
Increase contrast in environment, printed materials, writing materials, and on computer screen.
Control glare with yellow, amber, or light plum tinted glasses, lighting placement, and limiting reflective surfaces in environment (see Box 15-8).
Neuropathy can cause loss of sensation in extremities. Special attention to safety during kitchen and bathroom activities is an essential component of training. Adaptive equipment for kitchen tasks include knife guards that slip over the fingers of the hand that holds the item to be cut, long oven mitts, oven rack guards, oven rack pulls, long handled tongs, can openers that produce a smooth edge, and nonslip cutting boards.
Magnification or large print materials may make reading, writing, and other near tasks easier.
Vision substitution—talking books, scales, microwaves, glucometers, and other devices offer options for completing ADL with decreased vision.
Visual Dysfunction After Neurological Insult
The discussion of visual impairments in elders thus far has focused on impairments as a result of ocular conditions. However, the visual system is not composed of the eyeballs alone. To perceive visual information, the data must travel through a complex nervous system and must be processed by appropriate cerebral centers. In addition, effective control of eye movements depends on proper impulses from the brain. This includes feedback from areas that monitor body and head position and movement.26 Thus, successful adaptation to the environment through the visual sense requires the proper functioning of both ocular and neurological components (Box 15-4).
BOX 15-4 Intervention Gems for Individuals with Neurological Visual Impairments
It is essential for the COTA to have as complete a picture as possible of the visual, cognitive, and physical deficits of the elder with neurological visual impairment because they will affect interventions and functional outcomes.
Train elders and family/caregiver about the functional implications of visual field loss for safety and ADL performance—make sure they understand how much of the environment the elder may not see or be aware of.
For left-sided visual field loss, train the elder to turn head and eyes toward the “missing” side or area when beginning any activity and more frequently throughout the activity.
Train the elder to increase visual search organization and scanning patterns beginning with horizontal left to right, right to left, vertical top to bottom, and circular patterns.
Use activities that widen boundaries of visual search, and encourage use of appropriate search strategies in a variety of environments: searching for objects/signage on a wall or vacuuming to use left-to-right vertical search.
Intervention techniques for left-to-right horizontal pattern: dominoes, card search, sweeping, wiping off a counter, and looking for items on a shelf.
Intervention techniques for left-to-right vertical pattern: reading columns in sports scores or financial pages, reading ingredients in a recipe, and writing a grocery list.
Intervention techniques for circular patterns: puzzles, walking search, checkers, sorting coins, buttons, sorting laundry, looking for item in refrigerator, grocery store advertising circular.
Outline doorways, edges of furniture, and closets on side of visual deficit with bright colored tape for visual cue to scan for.
Causes of brain insult can include trauma, cancer, multiple sclerosis, and cerebrovascular accidents (CVA) or strokes. The vision system is vulnerable to strokes and other types of brain insult.27 A host of visual disorders can result from brain insult, including visual field disorders, reduced visual acuity, reduced contrast sensitivity, problems with stereopsis (depth perception), difficulty adapting to changes in light conditions, visual spatial disorders, and oculomotor dysfunction.28
Warren’s Hierarchy for Addressing Visual Dysfunction
Because of the complexity of the visual system, a framework for evaluation and intervention of visual impairments, whether ocular or neurological in nature, may be helpful. Warren27 suggests a developmental model that conceptualizes vision abilities in a hierarchy (Figure 15-3). The abilities at the bottom form the foundation for each successive level. Higher level abilities depend on the complete integration of lower level abilities for their development.
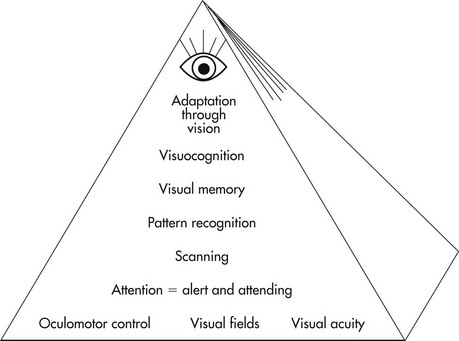
FIGURE 15-3 Hierarchy of visual perceptual skills development in the central nervous system.
(Adapted from Warren, M. L. (1993). A hierarchical model for evaluation and treatment of visual perceptual dysfunction in adult-acquired brain injury, part 1. American Journal of Occupational Therapy, 47, 42-54.)
The highest visual ability in this model is visual cognition. Visual cognition is the ability to mentally manipulate visual information and integrate it with other sensory information to solve problems, formulate writing, and solve mathematical problems.27
Visual memory is the ability directly below visual cognition in Warren’s model. Visual cognition depends on visual memory because mental manipulation of a visual stimulus requires the ability to retain a mental picture.29
To store a visual image, individuals must be able to recognize a pattern. Pattern recognition, the next ability level, involves identification of the salient features of an object.30,31 An individual must not only be able to identify the holistic aspects of an object such as its shape and contour, but also specific features of an object such as its color detail, shading, and texture.
The ability to scan the environment is necessary for effective pattern recognition. Scanning, therefore, is the fundamental ability required for pattern recognition. The eye must record systematically all of the details of a scene and follow an organized scan path.27
The ability directly below scanning is visual attention. Engagement of visual attention is necessary for proper scanning to occur. If individuals are not attending to visual stimuli in a specific space, they will not initiate scanning into that area. A classic example is the elder with a CVA with left hemi-neglect who requires constant cueing to scan to the left to avoid colliding with objects.27
Visual attention and all of the higher level abilities depend on three primary visual abilities that form the foundation for all vision functions: oculomotor control, visual fields, and visual acuity. Oculomotor control enables efficient and conjugate eye movements, which ensure the completion of accurate scan paths and “teaming” of the eyes for binocular vision. The visual field is the extent of view that a person has in front of each eye. Visual acuity describes the sharpness or clearness of vision.27 Table 15-2 addresses performance skill deficits of all of the discussed visual pathologies, and Box 15-5 is a screen that addresses performance skills with areas of occupation.
Principles of Intervention
When an occupational therapy (OT) visual screen reveals deficits affecting ADL, the client should be referred to an ophthalmologist or optometrist to obtain a comprehensive visual examination. If available records and clinical observation indicate that the client’s visual impairment is caused by an ocular disease, it would be best to refer the client to a low vision specialist (see later discussion of professionals for collaboration). If, conversely, diagnostic and clinical information indicate that the client’s visual impairment is caused by a neurological insult such as head injury or stroke, a consultation with a neuro-ophthalmologist or neuro-optometrist is recommended. If either of these scenarios is not possible, a consultation with a trusted ophthalmologist would be the next choice. Ideally, a good working relationship should be established with low vision specialists and neuro-ophthalmologists in the area to facilitate the speed of referral and communication between professionals.
The information provided by an ophthalmologist or optometrist may vary, depending on the condition and the professional’s area of specialty. A report from these professionals typically includes many of the following visual functions: visual acuity, visual field, contrast sensitivity function (the ability to distinguish subtle gradations in contrast between an object and its background), and oculomotor control. Reports may also include intraocular pressure (the pressure inside the eyeball), best correction for eyeglass prescription, dates and description of any ocular surgeries or procedures, current prescribed ophthalmic medications, and the general heath of ocular structures. Low vision specialists often also make recommendations for special optical devices to access printed materials, computer screens, or detailed eye-guided handiwork if visual acuity cannot be corrected to a functional range. This information and that gathered during the OT evaluation are invaluable in guiding intervention. Box 15-6 is a screening form for the sensory perceptual skill of vision. The following discussion addresses general interventions for many of the deficits that accompany visual loss such as decreased visual acuity, visual field loss, oculomotor dysfunction, reduced contrast sensitivity, and impaired visual attention and scanning.
BOX 15-6
Sample Screening Form for the Sensory Perceptual Skill of Vision
Is part of your visual field missing, blurry, or dark?
How long have you experienced this difficulty?
Has your eye doctor diagnosed or treated you?
When was your last eye examination?
Can you see newsprint, headlines, computer screen, details on a TV screen, faces, food on your plate?
Can you see traffic signals and street signs?
Adapted from Kern, T., & Miller, N. D. (2005). Tools for occupational therapists who work with people with low vision: Vision screening checklist. In M. Gentile (Ed.). Functional Visual Behavior in Adults: An Occupational Therapy Guide to Evaluation and Treatment Options, pp. 139-140. Bethesda, MD: AOTA Press.
Decreased Acuity
The input of an eye care specialist is crucial in addressing reduced acuity. Some elders are simply in need of an updated eyeglass prescription. In the case of a head injury or stroke, acuity may be reduced initially but often resolves spontaneously in a few months. (See Chapter 19 on the effects of traumatic brain injury [TBI]/stroke [CVA] for a full discussion of more subtle deficits on acuity and intervention.) Reduced acuity secondary to ocular diseases, such as macular degeneration, cannot be improved through a change in eyeglass prescription. Recommendations for special optical devices may be made in this case. Diabetic retinopathy often not only causes reduced acuity, but also causes fluctuating acuity. It is important to follow the advice of the eye care specialist when planning intervention related to acuity.
As mentioned earlier, one method to compensate for reduced acuity is to use special optical devices to magnify or enlarge print (Figure 15-4). It is recommended that OTRs and COTAs receive specialized training in optical devices before attempting to train individuals in their use. (See listed resources for courses geared to OTRs and OTAs.) There are many unique concepts and techniques involved in the proper use of these devices, and elders typically require very clear instructions and encouragement to become proficient in their use. Other examples of using enlargement to compensate for decreased acuity are the use of large print materials and writing larger letters with a felt tip pen.

When an elder has decreased acuity, there are other techniques to help maximize function such as the use of proper illumination, reduction of pattern and clutter in the environment, and the use of organizational systems. Proper lighting is usually critical for optimal performance. However, some individuals may be photophobic or sensitive to light, which presents a challenge in finding appropriate lighting. Good, general room lighting (ambient lighting) is necessary for ease and safety in ambulating. Task lighting sources such as a gooseneck lamp or movable track lighting is recommended for fine-detail or low-contrast tasks such as reading, sewing, handyman work, or crafts. Proper positioning of a lamp must be considered to avoid glare. Directing the light from behind the shoulder of the better-seeing eye so that the light source does not create glare often works best. Task lighting with a gooseneck lamp can be positioned closer to the reading material, even in front of it as long as the bulb is not exposed and the shade directs the light downward, concentrating it on the material to be illuminated. Position the light source opposite the dominant hand to avoid shadows when writing.
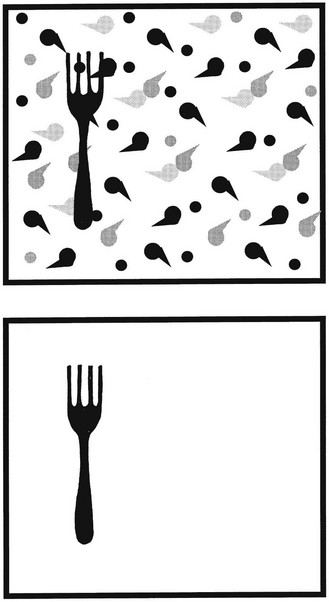
Patterned backgrounds and clutter in the environment tend to “camouflage “objects that an elder is seeking (Figure 15-5). This can be remedied by using solid colors for background surfaces such as bedspreads, place mats, tablecloths, rugs, and furniture coverings. Care should be taken to reduce clutter where possible by limiting the number of objects in the environment and arranging the remaining objects in an orderly fashion. Once the environment is rearranged and simplified, every effort should be made to keep it organized.
There are many national and local services available for those with impaired visual acuity (and other visual impairment). Most of these services are free of charge. They can be found by contacting local state services for the blind and visually impaired (search state government website). The American Foundation for the Blind and The Lighthouse are examples of services that provide books and magazines to individuals free of charge (see Appendix). There are also catalogs that offer low-tech adaptive devices for the visually impaired such as talking clocks, large print playing cards and bingo cards, and a variety of other devices for ADL (see Appendix).
Visual Field Loss
Elders who have a visual field loss may be taught to compensate for this loss in daily activities. The first step, however, is to increase the elder’s awareness of the visual field loss. Having accurate information on the extent and location of the field loss is critical for teaching elders proper methods of compensation. The exact type and scope of visual field loss will vary depending on the cause of the disorder or disease and on individual presentation. In general, those with ocular conditions experience relatively “spotty types” of field loss, whereas those with a neurological disorder exhibit more uniform or extensive field loss. Of course, there are definitely exceptions to this rule because some ocular conditions can lead to an extensive and even total loss of visual field. Small, concentrated areas of visual field loss also have been found in those with head injuries.32
Elders who have central field loss, such as that seen with macular degeneration, must learn to compensate by directing their gaze off-center of the target (either slightly above, below, or to the side of) rather than directly at the target. This technique, called eccentric viewing, enables the individual to place the target outside of the blind spot so that it can be seen. This usually requires professional assistance to identify the best area for eccentric viewing, sometimes referred to as the preferred retinal locus or PRL.33 Additional training and a conscious effort are required on the elder’s part to override the natural tendency to direct the fovea, the most central area of the retina to the target and instead place the PRL in line with the target. Central field loss usually affects fine-detail tasks but does not significantly interfere with mobility. Those with more peripheral field loss typically require intervention aimed at increasing safety and independence with mobility skills. Elders with a homonymous hemianopsia occurring after a stroke may be taught to compensate for this loss of half the visual field by systematically training them to turn the head and scan into the impaired field during functional activities such as reading, shopping, and mobility.34,35
Oculomotor Dysfunction
Intervention for oculomotor dysfunction is likely one of the most complex areas for beginning practitioners to comprehend and implement effectively. It is highly recommended that the entry level COTA attend continuing education seminars, develop a mentoring relationship, and establish service competency in this area before attempting any of the intervention strategies suggested. It is also strongly recommended that therapists and assistants work under close supervision of an optometrist or ophthalmologist when treating oculomotor impairments. Oculomotor impairments are seen in individuals who have experienced some type of neurological insult. Ocular conditions do not affect the muscular or neural mechanisms that control eye movements.
A strabismus, or misalignment of an eye,14 is often seen as a result of extraocular muscle weakness after a stroke or other neurological insult. This misalignment of the eyes results in diplopia, or double vision. The primary intervention methods used to address diplopia include occlusion, eye exercises, application of prisms, and surgery.35
Occlusion is essentially the “patching” of an eye to eliminate the double image.14 Care must be taken to follow an occlusion protocol that optimizes the elder’s comfort and reduces the likelihood of developing contractures in the muscles opposite the weak ones. Occlusion should not be carried out by simply patching the affected eye during all waking hours because this does nothing to encourage the use of the weak muscles. The protocol is typically directed by an ophthalmologist or optometrist.
Eye exercises can be used in conjunction with occlusion to help strengthen the affected muscles. One basic method would be to patch the unaffected eye and have the client track an object through all ranges of motion.35 Optometrists may suggest additional exercises to be carried out under their direction.
Another strategy to treat diplopia is the application of prisms.14 Prisms are sometimes prescribed and used to create a single image in the primary direction of gaze. The prism displaces the image to one side, causing the disparate images created by the strabismus to overlap and fuse into a single image. The prism can be permanently ground into the client’s eyeglass lens or can be temporarily applied to the eyeglass lens using press-on prisms. If the strabismus is resolving, the elder should be gradually weaned off of the prism by reducing its strength over time.14 An ophthalmologist or optometrist determines the strength of the prism and directs the intervention.
In some specific cases, surgery to correct the strabismus may be warranted.35 This is further testimony to the necessity of consulting with appropriate eye care professionals to obtain optimal intervention for the individual. In most cases, the general approach to the surgery is to make the action of one or more eye muscles weaker or stronger by changing its attachment position. This is done by an ophthalmologist who is specially trained in strabismus surgery.35
Reduced Contrast Sensitivity
Contrast sensitivity may be affected by both ocular and neurological conditions. This function is different than visual acuity, which reveals only the size of high contrast black and white letters that the individual is capable of seeing. Contrast sensitivity is the capacity to discriminate between similar shades.10 In daily life, good contrast sensitivity is necessary to see a gray car on a cloudy day, to detect unmarked curbs and steps, and to distinguish subtle contours on people’s faces to recognize them. Deficits in contrast sensitivity are typically addressed through environmental adaptation. For persons with low contrast sensitivity, the world often loses its definition. The primary technique to compensate for this deficit is to simply add contrast to the environment whenever possible. Many items used in daily activities can be changed to add more contrast and definition (Box 15-7). Proper illumination (as described earlier under “Decreased Acuity”) is also helpful in enhancing contrast. Some individuals find that full-spectrum lighting, either incandescent or fluorescent, provides the best contrast-enhancing illumination. Color filters that may be worn over prescription lenses or alone can also enhance contrast. Light yellow, medium yellow, and light or medium plum are the colors most frequently used to enhance contrast.
BOX 15-7 Examples of Modifications Using Contrast in the Environment
Use a black felt tip marker for writing.
Add strips of contrasting tape (usually orange or yellow is best) to the edge of steps.
Use a white coffee cup so the level of coffee can be seen against the white background when pouring.
Use a black and white reversible cutting board and slice light-colored items, such as onions, on the black side and vice versa.
Mark light switches with contrasting fluorescent tape to increase visibility.
Impaired Visual Attention and Scanning
Deficits in attention and scanning are seen in those with neurological involvement, not commonly in those with ocular conditions. One type of impairment in this area is hemi-inattention, or hemi-neglect. This refers to a lack of awareness of one half of a person’s visual space. Neglect of the left half of visual space is more common, but right hemi-neglect is occasionally seen.36 Individuals with hemi-inattention are not able to take in visual information in the orderly, sequential, and comprehensive pattern needed to safely complete many daily activities. Grooming, meal preparation, and functional mobility (especially driving) are common examples of ADL affected. Initial intervention of deficits in visual attention and scanning often involves increasing the elder’s awareness of the deficit followed up with appropriate compensation or remediation techniques, or both. Research has shown that individuals with left visual neglect may be trained to reorganize their scanning strategies by beginning the scan path in the impaired space.37 This is accomplished through intervention strategies similar to those described earlier in treating homonymous hemianopsia. Activities are used that require and encourage a systematic left-to-right scan pattern with a visual anchor (such as a red line or ruler) placed to the left (or right as appropriate) as a visual cue, if necessary. There is some evidence that the effects of this training on patients with hemi-inattention may be task-specific and may not generalize to overall ADL function.38,39 The presence of hemi-neglect also has been associated with poor rehabilitation outcome.40-42
Higher Level Visual-Perceptual Deficits
Warren’s27 proposed intervention for higher level visual deficits includes addressing the foundation visual skills that may affect these areas, education of the patient to increase awareness of the deficit, and instruction in the use of compensatory strategies for the deficit. (See Warren27 for a more detailed description of these techniques.) Refer to Box 15-4, Intervention Gems for Individuals with Neurological Visual Impairment.
Settings in Which Visual Impairments Are Addressed
Low-vision rehabilitation is becoming a specialty field for OTRs. OTRs may provide rehabilitation for diagnoses related to visual impairment when prescribed by an ophthalmologist, optometrist, or other physician (as of this writing, regulations vary by state). OTRs work in conjunction with other trained professionals to provide comprehensive services to individuals with vision impairments. The majority of individuals treated in low-vision clinics have impairments caused by ocular pathologies. Macular degeneration accounts for 60% of low-vision cases,14 whereas glaucoma and diabetic retinopathy are ranked second and third, respectively.43 For this reason, the term low vision is typically associated with visual impairments caused by ocular diseases. However, individuals with visual impairments secondary to neurological insult also may seek intervention in some low-vision clinics.
Because visual impairments are a common result of neurological insult and because ocular diseases are relatively common in the elderly, COTAs working in any geriatric or neurorehabilitation setting should be well educated in visual dysfunction and intervention techniques. Settings may include inpatient and outpatient rehabilitation, subacute rehabilitation facilities, long-term care facilities, and home health agencies.
COTAs working with elders with visual impairments must have specialized training in areas such as optics and use of optical devices, eccentric viewing techniques, blind techniques for ADL, and vision enhancement techniques for ADL, as well as a good working knowledge of the extensive adaptive equipment available for low-vision clients. They also must possess a good understanding of available resources to direct clients to appropriate support groups and other services.
There are many other low-vision rehabilitation professionals with whom the COTA can collaborate to provide the best functional outcomes for their clients. Orientation and mobility specialists address travel needs directly related to vision loss. They typically hold master’s degrees and have a wealth of knowledge in this area. The goal of their services is to develop independent travel skill within the client’s home, neighborhood, or community. These specialists may work in many settings, including public school systems, private agencies, and state-supported programs.
Rehabilitation teachers are professionals who are trained at the university level to address ADL that have been affected by visual impairment. They provide instruction in using adaptive techniques or adaptive equipment to increase independence in areas such as communication, household management, self-care, and other ADL. Rehabilitation teachers may work in private agencies, itinerant state services, residential schools, and independent living centers. The areas addressed and the knowledge base of these professionals may overlap at times with OT professionals. As long as there is open communication and collaboration, each profession will likely learn valuable techniques from the other, and the client will receive an optimal rehabilitation program.
Ophthalmologists and optometrists specializing in low vision ensure that comprehensive low-vision services are provided. They evaluate the client’s visual function and prescribe optical devices and training to compensate for vision loss. They may see low-vision clients in their own broader-based private practice, or they may work in low-vision clinics. (For more information regarding a program using ophthalmology and OT to provide low-vision rehabilitation in an outpatient rehabilitation setting, see Warren.44)
Conclusion
Visual impairments in elders may result from either ocular or neurological pathology. Normal physiological changes that may occur with aging include shrinkage of the peripheral field, increased time required to recover from glare, difficulty with light and dark adaptation, increased need for illumination, loss of elasticity in the lens, and yellowing of the lens. The most common ocular diseases that may occur in elders are macular degeneration, cataracts, glaucoma, and diabetic retinopathy. Elders are also at risk for CVAs, which may disrupt any of several neurological components necessary for effective visual functioning.
COTAs can play vital roles in helping elders with visual impairments learn to function as independently as possible. COTAs can provide sources for information about vision loss to help elders understand the specifics of their eye conditions. Encouraging elders to gain knowledge about their eye conditions can be an empowering first step in the process of rehabilitation. COTAs may collaborate with OTRs to provide training to compensate for vision loss in daily activities. COTAs can provide training in community resources and collaborate with other members of the intervention team to provide referral to appropriate agencies and service providers to facilitate community reintegration. Finally, COTAs may collaborate with elders, family members, and/or caregivers to make environmental adaptations, to enhance independence, and to do these safely (Box 15-8).
BOX 15-8 Environmental Adaptation Basics
Increase relative object size—Large print, bold labels, or large-sized objects.
Lighting—increase ambient and task lighting; add gooseneck lamps for task lighting where activities are completed.
Color—light colors for walls and ceilings to reflect and increase light; bright colors for tools and everyday objects to make them stand out.
Contrast—floor, walls, counters, furniture, hardware, switch-plates, and doorknobs should contrast with each other.
Reduce clutter—limit the number of objects on counters and tabletops, limit bold patterns to decrease “visual clutter,” and clear pathways between rooms and around furniture and exits.
Reduce glare by eliminating bare bulbs, reflective surfaces, using matte finishes and using light filtering window coverings and lampshades.
Texture—use bumpy or rough textured paint, tape or self-adhesive dots to label settings, or define edges and surface changes. Train elders to notice changes in the feel of carpet versus hard surfaced floors.
Audio substitution—use talking clocks, kitchen scales, timers, and other items to substitute for vision when performing ADL tasks.
The loss of vision in elders is a common occurrence, whether it results from the natural aging process, ocular disease, or disruption of neurological components. Vision loss has significant functional implications and can complicate the elder’s rehabilitation process with other physical impairments. This emphasizes the need for COTAs to familiarize themselves with the causes and types of vision loss and effective intervention techniques, whether they are working in general rehabilitation centers or acute care hospitals.
Case Study
Mark is a 67-year-old widower who lives alone and following an amputation below the right knee was just admitted to the rehabilitation unit where you work. He has diabetes mellitus and has had many complications of the disease, including the peripheral vascular disease that led to his amputation and diabetic retinopathy. Mark states that he did not manage his condition well in the past but wants to do everything he can now to keep these complications from getting any worse. He states that he finds it difficult to see the numbers and lines on his syringes when drawing his insulin. He also has some trouble seeing the blood sugar reading on his glucometer. He needs to check his blood sugar three times a day with this machine and adjust his insulin dosage accordingly. The OT visual screen reveals that Mark has moderately decreased visual acuity and decreased contrast sensitivity.
Mark has good upper body strength and uses his walker well on the unit. He will need to use the walker at discharge while waiting for his leg to heal before being fitted for a prosthesis. Fortunately, you will be able to conduct a home evaluation to make recommendations before discharge.
Case Study Questions
1. What are some specific areas of concern or potential hazards that you would look for on Mark’s home evaluation visit?
2. What are some recommendations you could make to address these concerns and improve safety and ease of functioning in Mark’s home?
3. You would like to increase Mark’s independence in his diabetic management, but you do not know what techniques or adaptive equipment is available to accomplish this. Where could you turn for help? What assistive technology might you inquire about to help Mark complete his diabetic care?
1. What are some natural age-related changes in the eye, and what implications do they have for function?
2. What are the three primary ocular conditions that account for the majority of referrals to low-vision rehabilitation clinics?
3. Which ocular conditions could potentially lead to total blindness?
4. What are some possible vision problems after a stroke or other neurological insult?
5. What are the primary vision abilities described in Mary Warren’s hierarchy that form the foundation for all other vision abilities?
6. Name three environmental adaptation strategies that could be used for clients with the primary ocular conditions most commonly encountered with elders.
7. Name three other professionals and two community or state agencies with whom the COTA could collaborate regarding a low-vision client.
1 American Occupational Therapy Association. Occupational therapy practice framework: Domain and process, 2nd ed. American Journal of Occupational Therapy. 2008;62:625-683.
2 American Foundation for the Blind. Facts about aging and vision [WWW page]. URL http://www.afb.org/info_documants.asp?kitid=8&colletionid=2, 2002.
3 The Lighthouse, Inc. The Lighthouse national survey on vision loss: The experience, attitudes, and knowledge of middle-aged and older Americans. New York: Lighthouse; 1995.
4 Warren M.L. The Brain Injury Visual Assessment Battery for Adults Test Manual. Lenexa, KS: visABILITIES Rehab Services; 1998.
5 Center on an Aging Society. Visual impairments data profile, no.3 [WWW page]. URL http://ihcrp.Georgetown.edu/agingsociety/pdfs/visual.pdf, 2002.
6 American Foundation for the Blind. Fact sheet: Statistics and sources for professionals [WWW page]. URL http://www.afb.org/info_document_view.asp?documentid=1367, 1999.
7 Friedman D.B. Psychosocial factors in vision rehabilitation. In: Albert D.M., Jakobiec J.A., editors. Principles and Practice of Ophthalmology, vol. 5. Philadelphia: WB Saunders; 2004.
8 Kubler-Ross E. Death and Dying. New York: Macmillan; 1969.
9 Perski T. The five-stage process of becoming a successful low vision patient. Retrieved from n.d. http://www.blindness.org/coping/resource/detail?res=1&id=20. Retrieved 09/14/2004
10 Mogk L.G. Eye conditions that cause low vision in adults. In: Warren M., editor. Low Vision: Occupational Therapy Interventions with the Older Adult: A Self-Paced Clinical Course from AOTA. Bethesda, MD: American Occupational Therapy Association, 2000.
11 Bennett S.H. Low vision: Clinical aspects and interventions. In: Rothman J., Levine R., editors. Prevention Practice Strategies for Physical Therapy and Occupational Therapy. New York: WB Saunders; 1992:258-269.
12 Christenson M.A. Environmental design, modification, and adaptation. In Larson K.O., Stevens-Ratchford R.G., Pedretti L., Crabtree J.L., editors: ROTE: The Role of OT with the Elderly, 2nd ed, Bethesda, MD: AOTA Press, 1995.
13 Scheiman M. Review of basic anatomy, physiology, and development of the visual system. In: Scheiman M., editor. Understanding and Managing Vision Deficits: A Guide for Occupational Therapists. Thorofare, NJ: Slack; 2002:9-15.
14 Scheiman M. Management of refractive, visual efficiency, and visual information processing disorders. In: Scheiman M., editor. Understanding and Managing Vision Deficits: A Guide for Occupational Therapists. Thorofare, NJ: Slack; 2002:117-162.
15 Lighthouse International. The Ageing Eye.[WWW page]. URL http://www.lighthouse.org, 2009.
16 NEI. Age Related Eye Disease Study—Results.[WWWpage]. URL http://www.nei.nih.gov/amd/, 2002.
17 American Foundation for the Blind. Fact sheet: Cataracts [WWWpage]. URL http://www.afb.org/info_document_view.asp?documentid=193, 1999.
18 American Foundation for the Blind. Fact sheet: Visual impairment and age-related macular degeneration [WWWpage]. URL http://www.afb.org/info_document_view.asp?documentid=202, 1999.
19 Scheiman M., Scheiman M., Whittaker S. Low Vision Rehabilitation: A Practical Guide for Occupational Therapists. Thorofare, New Jersey: Slack; 2006.
20 Mogk L.G., Mogk M. Macular Degeneration: The Complete Guide to Saving and Maximizing Your Sight. New York: Random House; 2003.
21 Jackson M.L., Bassett K., Nirmalan P.V., Syre E.C. Contrast sensitivity and visual hallucinations in patients referred to a low vision rehabilitation clinic. British Journal of Ophthalmology. 2007;91(3):296-298.
22 American Foundation for the Blind. Fact sheet: Visual impairment and glaucoma [WWWpage]. URL http://www.afb.org/info_document_view.asp?documentid=705, 1999.
23 Jose R.T. The eye and functional vision. In: Jose R.T., editor. Understanding Low Vision. New York: American Foundation for the Blind; 1985:3-42.
24 Bennett S.H. Visual changes associated with aging: Influence on practice. Occupational Therapy Practice. 1991;3(1):12.
25 Bennett S.H. Low vision: Clinical aspects and interventions. In: Rothman J., Levine R., editors. Prevention Practice Strategies for Physical Therapy and Occupational Therapy. New York: WB Saunders; 1992:258-269.
26 Zoltan B. Vision, Perception, and Cognition: A Manual for the Evaluation and Treatment of the Adult with Acquired Brain Injury, 4th ed. Thorofare, NJ: Slack; 2006.
27 Warren M.L. A hierarchical model for evaluation and treatment of visual perceptual dysfunction in adult acquired brain injury, part 1. American Journal of Occupational Therapy. 1993;47:42-54.
28 Kerkhoff G. Neurovisual rehabilitation: Recent developments and future directions. Journal of Neurology, Neurosurgery, and Psychiatry. 2000;68:691-706.
29 Ratcliff G. Perception and complex visual processes. In: Meier M.J., Benton A.L., Diller L., editors. Neuropsychological Rehabilitation. New York: Guilford, 1987.
30 Julesz B. Texton, the elements of texture perception and their interactions. Nature. 1981;290(12):91.
31 Julesz B. Preconscious and conscious processing in vision. Chagas C., Gattass R., editors. Pattern Recognition Mechanisms. Experimental Brain Research. 1985;11 (Suppl 11):333.
32 Willliams T.A. Case report: Low vision rehabilitation for a patient with traumatic brain injury. American Journal of Occupational Therapy. 1995;49(9):923-926.
33 Fletcher D.C., Suchard R.A. Preferred retinal loci relationship to macular scotomas in low-vision population. Ophthalmology. 1997;104(4):632-638.
34 Kerkhoff G., Munbinger U., Meier E. Neurovisual rehabilitation in cerebral blindness. Archives of Neurology. 1994;51:474-481.
35 Warren M.L. The Brain Injury Visual Assessment Battery for Adults Test Manual. Lenexa, KS: visABILITIES Rehab Services; 1998.
36 Diamond R. Rehabilitative management of post-stroke visuospatial inattention (review). Disability and Rehabilitation. 2001;23(10):407-412.
37 Weinberg J., Diller L., Gordon W.A., Gerstman L.J., Lieberman A., Lakin P. Visual scanning training effect on reading-related tasks in acquired right brain damage. Archives of Physical Medicine and Rehabilitation. 1979;60:479-486.
38 Gordon W.A., Hibbard M.R., Egelko S., Diller L., Shaver M.S., Lieberman A., et al. Perceptual remediation in patients with right brain damage: A comprehensive program. Archives of Physical Medicine and Rehabilitation. 1985;66:353-360.
39 Wagenaar R.C., Van Wieringen P.C.W., Netelenbos J.V., Meijer O.G., Kuik D.J. The transfer of scanning training effects in visual inattention after stroke: Five single-case studies. Disability and Rehabilitation. 1992;14:51-60.
40 Fullerton K.J., Mackenzie G., Stout R.W. Prognostic indices in stroke. Quarterly Journal of Medicine. 1988;250:147-162.
41 Kalra L., Perez L., Gupta S., Wittink M. The influence of visual neglect on stroke rehabilitation. Stroke. 1997;28:1386-1391.
42 Kaplan J., Hier D.B. Visuospatial deficits after right hemisphere stroke. American Journal of Occupational Therapy. 1982;36:314-321.
43 Stuen C. New concepts and treatments. Vision and Aging New. 1996;8(1):8.
44 Warren M.L. Providing low vision rehabilitation services with occupational therapy and ophthalmology: A program description. American Journal of Occupational Therapy. 1995;49:877-884.