chapter 19 Working with Elders Who Have Had Cerebrovascular Accidents
1. Discuss cerebrovascular accidents by describing the major features of strokes affecting the main arteries of the brain.
2. Discuss at least three considerations in the occupational therapy evaluation of elders who have had a stroke.
3. Describe the sequence of facilitating midline alignment while elders are supine, sitting, and standing, and explain the steps to follow when transferring elders from a supine position to the edge of the bed or from a sitting to a standing position.
4. Explain precautions for handling an elder’s hemiplegic upper extremity.
cerebrovascular accident, aphasia, midline alignment, muscle tone, hypotonicity, hypertonicity, subluxation, shoulder-hand syndrome, hemiplegia, transfers, edema, weight bearing, functional activities
Virtually every human endeavor is the result of the brain’s unceasing activity. The brain is the organ of behavior, cognition, language, learning, and movement. The sophistication of the brain’s circuitry is remarkable, if not baffling. Billions of neurons interact with each other to do the brain’s work. To appreciate the aging process, certified occupational therapy assistants (COTAs) must have an understanding of the way the brain works.1-3 Implications of neuropathological disorders for occupational therapy (OT) intervention with elders are described in this chapter. The many biological and behavioral changes that accompany normal aging are explained in other chapters in this book.
Effects of normal age-related changes in the nervous system vary greatly among individuals and are not generally associated with specific diseases. These changes clearly have little detrimental effect on many elders. Senility is not an inevitable aspect of aging. However, a number of conditions can be devastating to elders because they present serious obstacles to the process of normal, healthy aging. Some of these conditions are related to cerebrovascular accidents (CVAs). (Chapter 20 presents the issues related to Alzheimer’s disease, which is another disorder affecting the brain.)
Cerebrovascular Accidents
CVAs, or strokes, are lesions in the brain that result from a thrombus, embolus, or hemorrhage that compromises the blood supply to the brain. This inadequate supply results in brain swelling and ultimately in the death of neurons in the stroke area.
Strokes are the third leading cause of death in the United States and the leading cause of disability among adults. Although the incidence of CVA has decreased over the past 50 years, approximately 750,000 individuals experience strokes each year, and nearly 167,000 die as a result, making it the third leading cause of death in the United States.4 About 4 million individuals live with varying degrees of neurological impairment after strokes.5 The incidence of strokes increases with age, with the rate doubling every decade of life after age 55 years, and two-thirds of all strokes occur after age 65 years. Recurrent strokes account for 25% of yearly reported strokes and usually occur within 5 years.6 Black individuals have a greater risk for disability and death from stroke than other racial and ethnic groups.7 Men experience strokes more frequently than women until age 55 years, when the risk for women equals that for men; however, more women die of strokes at all ages.5
Ischemic strokes, caused by both thrombus and embolus, account for about 80% of strokes. Intracerebral and subarachnoid hemorrhagic strokes account for about 20% of strokes.8 Mortality rates associated with stroke have been declining steadily since the 1950s and are reported to be between 17% and 34% during the first 30 days after a stroke, between 25% and 40% within the first year, and between 32% and 60% during the first 3 years. Consequently, about half of the patients with first strokes live for 3 or more years, and more than one-third of individuals live for 10 years.7
Risk factors for stroke can be separated into modifiable and unmodifiable. Modifiable factors are those that can be altered by changes in lifestyle or medications, or both. These factors include hypertension, carotid artery stenosis, coronary artery disease, atrial fibrillation, congestive heart failure, cigarette smoking, alcohol and other drug consumption, obesity, diabetes mellitus, and high serum cholesterol, among others. The most preventable of these risk factors is hypertension. Unmodifiable, or fixed, risk factors include prior stroke, age, race, sex, and family history of stroke. Among these unmodifiable factors, increasing age is by far the most significant because two-thirds of strokes occur in people age 65 years and older.9
In elders, stroke can result in various neurological deficits (Table 19-1). Neurological and functional recovery occurs most rapidly in the first 3 months after a stroke; most elders continue to progress after that time but at a slower rate.10 For this reason, predicting functional recovery after stroke and which elders will benefit from rehabilitation are difficult. The World Health Organization proposes that the prognosis for recovery and successful rehabilitation should be indicated in the following order: (1) clients who spontaneously make good recovery without rehabilitation, (2) clients who can make satisfactory recovery through intensive rehabilitation only, and (3) clients with poor recovery of function regardless of the type of rehabilitation.11 Other factors that complicate prediction of recovery include comorbidity and depression.
TABLE 19-1 Incidence of Neurological Deficits after Stroke
| Neurological impairment | Incidence (%) |
|---|---|
| Sensory deficits | 55 |
| Dysarthria | 46 |
| Right hemiparesis | 47 |
| Left hemiparesis | 37 |
| Cognitive deficits | 38 |
| Visual-perceptual deficits | 34 |
| Aphasia | 30 |
| Bladder control | 29 |
| Hemianopsia | 31 |
| Ataxia | 24 |
| Dysphagia | 13 |
Adapted from U.S. Department of Health and Human Services. (2009). Stroke facts and statistics. Retrieved November 19, 2009, from http://www.cdc.gov/stroke/stroke_facts.htm.
The outcome of a stroke depends greatly on which artery supplying the brain is involved (Table 19-2). Medical treatment of a stroke depends on the type, location, and severity of the vascular lesion. In the acute stages, medical intervention is focused on maintaining an airway, rehydration, and management of hypertension. Measures are often taken to prevent the development of deep venous thrombosis (DVT)—that is, blood clots that form in the veins of the lower extremities after prolonged periods of bedrest or immobility. If such clots are released, they can become lodged in the lungs and can cause death. The COTA must be alert to any sign of DVT and should request and carefully follow mobilization and activity guidelines set by the physician. Localized signs in the lower extremity that suggest the presence of DVT include abnormal temperature, change in color and circumference, and tenderness. In addition to the use of medications, elders can prevent DVTs by wearing elastic stockings and intermittent compression garments, and through early mobilization. Because of DVT and other potential complications of stroke, the COTA should check the elder’s medical record and communicate with other team members before initiating each intervention session. By doing this, all team members are fully informed and can modify the interventions with the elder to best serve the elder’s needs.
TABLE 19-2 Impairments Resulting from Cerebrovascular Accidents of Specific Arteries
| Artery | Impairment |
|---|---|
| Middle cerebral artery | Contralateral hemiplegia Contralateral sensory deficits Contralateral hemianopsia Aphasia Deviation of head and neck toward side of lesion (if lesion is located in dominant hemisphere) Perceptual deficits including anosognosia unilateral neglect, visual spatial deficits, and perseveration (if lesion is located in non-dominant hemisphere) |
| Internal carotid artery | Contralateral hemiplegia Contralateral hemianesthesia Homonomous hemianopsia Aphasia, agraphia, acalculia, right/left confusion, and finger agnosia (if lesion is located in dominant hemisphere) Visual-perceptual dysfunction, unilateral neglect, constructional dressing apraxia, attention deficits, topographic disorientation, and anosognosia (if lesion is located in non-dominant hemisphere) |
| Anterior cerebral artery | Contralateral hemiplegia Apraxia Bowel and bladder incontinence Cortical sensory loss of the lower extremity Contralateral weakness of face and tongue Perseveration and amnesia Sucking reflex |
| Posterior cerebral artery | Homonomous hemianopsia Paresis of eye musculature Contralateral hemiplegia Topographic disorientation Involuntary movement disorders Sensory deficits |
| Cerebellar artery | Ipsilateral ataxia Nystagmus, nausea, and vomiting Decreased touch, vibration, and position sense Decreased contralateral pain and thermal sensation Ipsilateral facial paralysis |
| Vertebral artery | Decreased contralateral pain, temperature, touch, and proprioceptive sense Hemiparesis Facial weakness and numbness Ataxia Paralysis of tongue and weakness of vocal folds |
Bowel and bladder dysfunction is common during the initial phases of recovery from a stroke. Usually, a specific bowel and bladder program that includes fluid intake, stool softeners, and other remedies is ordered by the physician. The COTA may be involved in structuring a scheduled toileting program for the elders, which is essential for success. (Chapter 17 presents a more detailed discussion about bowel and bladder training programs.) Other complications during the early phases of recovery from a stroke may include respiratory difficulties and pneumonia caused by the decreased efficiency of the muscles involved in respiration and swallowing. Good pulmonary hygiene, use of antibiotics, and early mobilization are effective prevention measures. Dysphagia, or problems with swallowing, also must be addressed to prevent aspiration pneumonia (see Chapter 18).
Occupational Therapy Evaluation
Research evidence and expert opinion suggest that stroke rehabilitation should begin in the acute stage and continue long-term, extending several years after onset.12-14 OT is an essential component in this rehabilitation process.15 The COTA is an active participant in the evaluation process under the supervision of the registered occupational therapist (OTR).16 As with any client, OT evaluation is an ongoing process that occurs during each intervention session. This is particularly true for elders who have had a stroke because they may experience many changes during the first few months of recovery. These changes may be noted especially during intervention. Although motor, visual, perceptual, sensory, and cognitive deficits may all contribute to functional impairments, the psychosocial skills and performance of elders and the environment in which they live and perform are critical components of any OT assessment. In addition, the assessment should always consider elders’ performance skills, past performance patterns, occupational contexts, values, beliefs, and spirituality, not just their deficits.17 Assessment of performance skills (motor and praxis skills, sensory-perceptual skills, emotional regulation skills, cognitive skills, and communication and social skills) is done simultaneously during the performance of an activity. Although the evaluation of each discrete area may be conducted separately, the interaction of these skills and their effects on occupational participation are of primary importance to OT.17 Typical impairments are discussed in the section on intervention, but areas of necessary assessment for COTAs are discussed in the following paragraphs.
In the context of motor assessment, the COTA must have an understanding of the elder’s ability to maintain the body in an upright position and in the midline against gravity (postural reactions). To do this, the COTA must observe the elder’s degree of hypertonicity or hypotonicity, the presence of abnormal movement patterns, primitive reflexes, righting and protective reactions, equilibrium, coordination, and range of motion. The COTA should remember that all of these performance skills may be, and often are, affected by posture and endurance, and that the optimal assessment will occur when elders are upright and not too fatigued. Alignment of the trunk, pelvis, and shoulder girdle, and any voluntary motor control should be noted. Assessment of strength has limited benefit in the presence of hypotonicity or hypertonicity and can possibly increase the degree of hypertonicity.18
The sensory assessment should include the evaluation of light touch, pressure, pain, temperature, stereognosis, and proprioception. The visual and perceptual areas to be assessed include tracking (smooth pursuits), visual fields, inattention to the right or left sides, spatial relations, figure ground, motor planning, and body scheme. In addition, elders may have other visual impairments that may affect their performance (see Chapter 15 for a review of this topic). Cognitive skills often assessed include attention, initiation, memory, planning, organization, problem solving, insight, and judgment. The ability to do calculations and make abstractions may also be tested. COTAs should remember that posture can have a significant effect on sensory, visual, perceptual, and cognitive functioning, and the assessment of these areas should occur when elders are upright.
Assessment of swallowing ability and safety is crucial for all elders who have experienced a stroke. Swallowing is a complex behavior that results from the simultaneous performance of motor, sensory, perceptual, and cognitive skills, and deficits in any of these areas may result in elders being at a greater risk for aspirating food into the lungs and subsequent development of pneumonia (see Chapter 18 for a review of this topic).
Depending on the elder’s ability to communicate, an evaluation of psychosocial skills of elders may need to be completed by interviewing their family or other significant people. Knowledge of the occupations or pursuits that the elder was involved in before the stroke and of the elder’s values and interests is crucial in the selection of intervention strategies. Occupational task considerations should be made at every stage of OT intervention.
Occupational Therapy Intervention
The long-range goal of OT intervention for dysfunction caused by stroke is to facilitate maximal participation in all contexts of the elder’s life. To reach this goal, intervention is focused on the restoration of neuromuscular, visual-perceptual-cognitive, and psychosocial skills that support the elder’s ability to perform self-care and engage in all areas of occupation. The degree to which each of these areas is emphasized is determined by the previous physical and social environments of elders and their plans after hospitalization. Because each elder’s context is unique, the OT intervention plan is tailored specifically to that individual. By recognizing all of these areas of an elder’s being, the COTA is adhering to the Occupational Therapy Code of Ethics.19
Case Study
The need for tailored intervention programs is illustrated by the cases of Rose and Maria. Both women are in their late seventies and had strokes that have left them with a hemiplegic right side and difficulty verbally expressing themselves (aphasia). Their visual, perceptual, and cognitive skills appear to be intact. Rose is a widow and lives in a senior community that provides one meal a day and assists her with laundry and cleaning. Her two sons live in other states. Maria lives at home with her husband and 2 of her 8 adult daughters; 10 grandchildren, whose ages range from ages 3 to 18 years, also live in her home. Both Rose and Maria want to return to their previous living environments. The OT program for both women will address all their needs, but the emphasis in Rose’s program will be on self-care, meal preparation, and light home management tasks because she must be independent in these areas to maintain her apartment at the senior community. Maria, however, is counting on family assistance for her self-care and is more interested in cooking again for her extended family; therefore, her program will focus more on meal preparation, light home management, and social skills. The OT programs for both women will address their neuromuscular, visual-perceptual-cognitive, and psychosocial skills, but the activities chosen as therapeutic media should reflect their life contexts.
The cases of Rose and Maria illustrate another important principle in stroke rehabilitation: The more familiar the individual is with the activities selected for intervention, the more spontaneous and unconscious are the motor, visual, perceptual, cognitive, and psychosocial reorganization; consequently, changes will last longer.20 Conscious, attention-focused learning is often necessary in rehabilitation, especially when the likelihood of recovery is small and compensation strategies are more viable. However, these strategies may also slow the rehabilitation process because of the mental effort they require. To illustrate this, COTAs should do the following exercise with partners. Have your partner time you as you write your full name on a piece of paper using your dominant hand, then have your partner time you writing your name again, but this time with your non-dominant hand. Focus carefully on your body while you write your name and on the amount of mental control this task requires. The experience of rehabilitation after a stroke is similar to your experience of writing with your non-dominant hand. Although clients who are recovering from stroke may not be learning to use their non-dominant hand, they are relearning task accomplishment with a different body. The more these clients must concentrate on the task they are attempting, the longer it may take them to complete it. Engagement in automatic activities may take less time and may reinforce the automatic postural adjustments that support all actions. Consequently, whenever possible, the COTA should approach the intervention for stroke impairments with strategies designed to restore lost function in ways that use the learning and work experiences of elders before they experienced the stroke. Compensation strategies, particularly those related to the use of assistive equipment or alternative motor patterns, should be evaluated carefully because they require conscious attention and may create habits that may be difficult to break later.
Motor Deficits
Several sensorimotor approaches exist for the treatment of motor dysfunction resulting from stroke. Some of these include Brunnstrom,21,22 Bobath’s neurodevelopmental therapy and proprioceptive neuromuscular facilitation,23-26 constraint-induced movement therapy,27-29 and mirror therapy.30-32 Regardless of the approach, the goal of intervention is to facilitate normal voluntary movement and use of the affected side of the body. Thus, normal postural mechanisms must also be developed, and abnormal reflexes and movements must be inhibited.
Although hypertonicity is often the most visible sign that a person has a motor dysfunction, this problem is best addressed in the context of postural control rather than in isolation. Abnormal tone in any extremity may drastically change depending on whether the individual is lying, sitting, or standing. Therefore, motor dysfunction should be treated when the individual is in alignment. Alignment means that the individual’s pelvis is in a neutral position with no anterior or posterior tilt, that the spine is in midline alignment, and that the upper and lower extremities are in a neutral position.
The correct positioning while the elder is reclining can have a dramatic effect on muscle tone and pain, especially in the presence of shoulder-hand syndrome. (Specific issues with the hemiplegic upper extremity are discussed later in the chapter). Having elders lie on the more affected side is most helpful in inhibiting abnormal tone and pain because of the heavy pressure exerted on that side (Figure 19-1, A). However, caution must be taken to determine that the shoulder girdle is correctly aligned, the scapula is slightly abducted, and the humerus is in external rotation. The position of the bed should be rearranged (unless the elder finds the change too disorganizing) so that the elder can lie on the affected side and face the side of the bed from which transfers will occur. An added advantage of lying on the affected side is that it frees the less involved upper extremity for functional use while the elder is in this position (Figure 19-1, B).
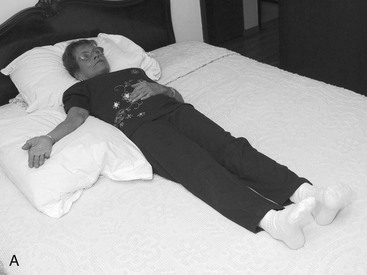
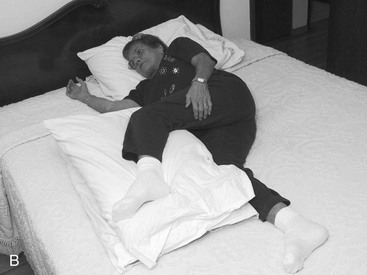
FIGURE 19-1 A, In the supine position, the trunk and upper extremities should be aligned. The hemiplegic upper extremity should be supported on pillows with the palm facing up. B, Lying on the hemiplegic upper extremity frees the less involved arm for functional use.
Body alignment should also be maintained during transitional movements, such as changing from a side-lying position to sitting at the edge of the bed and back to side-lying; transferring to and from a chair, wheelchair, toilet, or car; changing from a sitting to a standing position and back to sitting; and while walking. COTAs should follow established sequential procedures when assisting elders to change from a supine position to sitting at the edge of the bed or when doing transfers (Boxes 19-1 and 19-2). In all of these circumstances, COTAs must remember not to pull on the affected upper extremity to assist elders. COTAs should assist by holding the elder from the shoulder with the COTA’s hand on the elder’s scapula. Pulling the arm or supporting the elder from the axilla can easily cause or worsen any shoulder pain or glenohumeral subluxation. Shoulder subluxation can occur inferiorly, anteriorly, and superiorly. Alignment of the humerus in the glenohumeral fossa is evaluated by the OTR. The COTA needs to determine whether the alignment is correct before range of motion of the shoulder. Shoulder pain is a frequent problem and can occur from malalignment of the trunk, shoulder girdle, and humerus; subluxation; adhesive capsulitis; and trauma.33 Shoulder subluxation and pain can lead to other complications such as increased hypertonicity, contractures, edema, nerve injury, and shoulder-hand syndrome. Before the COTA attempts any intervention for these conditions, service competency should be established with the OTR.
BOX 19-1 Sequential Procedures for Changing from a Supine Position to Sitting at Edge of Bed
1. Plan to have elder exit bed toward hemiplegic side.
2. Gently provide passive abduction to hemiplegic scapula, and extend hemiplegic arm at side of body so that humerus is in external rotation and palm is facing up; an alternative is to have elder clasp hands and hold arms in 90-degree flexion with straight elbows and roll toward side of bed.
3. Have elder hook less affected leg under hemiplegic ankle, and slide both legs toward edge of bed.
4. Have elder roll on to hemiplegic side, facing side of bed.
5. Have elder cross less affected upper extremity in front of body and place on bed at a level slightly below chest.
6. As the elder lowers legs at the side of the bed, have elder push up with less affected hand and hemiplegic elbow (if able).
7. Once sitting at edge of bed, have elder scoot forward by alternating weight bearing on each thigh and scooting the free thigh forward until both feet are flat on floor.
BOX 19-2 Sequential Procedures for Transfers
1. If transferring from the wheelchair to another chair, toilet, or bed, place wheelchair at no more than 45 degrees (perpendicular) from destination surface; elder should transfer toward hemiplegic side whenever possible.
2. Make sure wheelchair is locked and footrests and armrests are out of the way.
3. Place both feet flat on floor.
4. Have elder sit upright so back is not against back rest.
5. Have elder scoot forward to front edge of chair by alternately shifting weight onto one thigh and scooting other thigh forward; do not permit elder to push off back of chair using back extension because this will increase abnormal muscle tone throughout the body.
6. Position elder’s feet so tips of toes are directly below knees; make sure feet remain flat on floor; if ankle dorsiflexion is limited, toes may be placed somewhat anterior to knees.
7. Have elder lean forward until shoulders are directly above knees.
8. Have elder push off from knees with both hands, if elder is able.
9. As elder leans forward, have elder stand up; if unable to stand up fully, guide elder’s body toward target chair, toilet, or bed while elder is partially weight bearing on both feet.
COTAs must pay constant attention to the elder’s body alignment during sitting because this is often the elder’s position during most activities, especially during the initial stages of rehabilitation. If the elder must sit fairly still for long periods, the therapist must ensure that the elder’s pelvis is in a neutral position and is as far back in the chair as possible. Hips should be flexed at no more than 90 degrees. Greater hip flexion will cause posterior pelvic tilt and lumbar and thoracic spine flexion, inhibiting breathing and active upper extremity control and requiring greater cervical spine extension for the person to look straight ahead. Placing a folded towel or thin pillow in the small of the back to maintain alignment may be helpful. However, too thick a pillow or support can push the lumbar spine into hyperextension, causing anterior pelvic tilt and encouraging the elder to use back extension as the primary means of posture control. When back hyperextension is the base from which the elder begins movement in the extremities, hypertonicity throughout the body is likely to increase.
Another concern when the elder is in the sitting position is lateral pelvic tilt, or lateral flexion of the spine. Because of sensory and tone changes, half of the trunk muscles may not be working well; consequently, the other side of the trunk may be overworking. The resulting misalignment causes the spine to flex toward one side. Because of this lateral flexion, the spine is no longer in midline, and weight bearing on the elder’s thighs is unequal. A pelvic tilt upward toward one side results in the shortening of the trunk on the same side and elongation of the trunk on the opposite side. Weight bearing occurs primarily on the side of the elongated trunk. The COTA must help to actively or passively align the spine toward the midline, rather than to simply build up one side of the sitting surface.
When pelvic and spine alignment are achieved, the COTA can focus on placing the feet flat on the floor or on footrests so that knee flexion and ankle dorsiflexion of no more than 90 degrees are present. The COTA should take care that the femurs are in neutral rotation (that is, there is no external or internal rotation) and that there is little or no hip abduction or adduction. Thus, the heels will be resting directly below the knees, and the knees will be aligned with the hips. Unless the elder is being pushed in a wheelchair, both feet should be placed on the floor so that they bear weight more evenly. Consequently, hemi-wheelchairs, the seats of which are slightly lower than standard wheelchairs, are recommended so that the elder’s feet can comfortably reach the floor. The use of a padded seat and backboards placed in the wheelchair also improves the elder’s sitting position and midline orientation, thus preventing the problems that may occur from poor positioning in a wheelchair.
After attending to the pelvis, spine, and lower extremities, the COTA can align the elder’s hemiplegic upper extremity. The strategies for positioning are similar for both hypotonic and hypertonic arms. The elder should be placed in front of a table or outfitted with a full or half lapboard so that the hand can be placed face down on a flat surface to benefit from the normalizing effects of weight bearing. To accomplish this, the COTA should ensure that the elder’s scapula is slightly abducted, the shoulder is flexed so the elbow is anterior to the shoulder, the humerus is in neutral or slight external rotation, the elbow is resting lightly on the lapboard to provide support for the shoulder, the forearm is pronated and positioned away from the trunk, and the hand is resting on the support surface. This permits the hand to bear weight normally. The normal weight-bearing surface of the hand includes the lateral external surface of the thumb, fingertips, lateral border of the hand, and thenar and hypothenar eminences. The COTA should maintain the arch formed by the metacarpophalangeal joints so that the hand is not flattened. The hand should not be fastened in any way to the lapboard except in extreme cases in which clear evidence indicates that the elder may otherwise be hurt. Restricting normal, spontaneous weight bearing inhibits normalization of muscle tone. In cases of extreme hypertonicity in the hand, the COTA can place a soup bowl or a ball cut in half face down on a square of nonslip material on the lapboard, thus permitting some weight bearing against a hard surface (Figure 19-2). However, the elder’s hand should never be placed on nonslip material. Such material can contribute to shoulder pain or subluxation because the hand cannot move when repositioning of the shoulder or body occurs. Caution must be used when a lapboard is used with an elder because it may be considered a form of restraint unless the elder is independently able to remove it. (See Chapter 14 for a detailed discussion on this topic.)

FIGURE 19-2 In cases of hypertonicity, the hemiplegic hand can be placed on an inverted soup bowl or ball cut in half to bear weight more comfortably.
During intervention sessions that do not require sitting for long periods, the elder should sit in a chair, on a stool, or at the edge of a mat. The concerns with alignment in this position are similar to those described earlier for sitting, but the focus of intervention will be on the elder moving into and out of alignment while participating in activities. Sitting on a stool or at the edge of the mat forces active trunk control because there are no back or armrests for support, and the base of support under the thighs is reduced. Concerns regarding lower extremity placement are the same as described previously. However, as the elder’s ability to control the trunk increases, the height of the mat can be increased, thus gradually increasing and challenging the amount of active weight bearing on the lower extremities. This gradation prepares the elder for the trunk and postural control required during standing activities. If the elder has little or no active movement of the hemiplegic upper extremity, the elder should position the limb on a table, following similar guidelines as those described previously. As the height of the mat increases, so should the height of the table or surface that supports the hand.
Although standing and ambulation training does not traditionally fall into the realm of OT, it should be considered a transitional movement that permits elders to perform and maneuver from one task or occupation to another. For example, elders may need to ambulate from the bed to the bathroom and stand to complete toileting tasks, or ambulate from the sink to the stove to the refrigerator and stand to complete a meal preparation task. Consequently, COTAs should assist in maintaining alignment in the same way as described previously. During standing and ambulation, the person’s midline shift toward the less affected side is most obvious. This is often accentuated when elders are taught to walk using a broad-based cane, and they establish the habit of maintaining the midline in the middle of the less affected side rather than in the middle of the body. Because there is less motor control or less sensory feedback, elders may hesitate to bear weight equally on each leg as they stand or take a step. The COTA should coordinate intervention with the registered physical therapist to understand what standing and ambulation pattern to reinforce with elders during OT intervention.
Special attention should be given to the hemiplegic upper extremity. This extremity should be purposefully included in any activity early during the course of intervention, even if little or no active motor control is present, because this will keep the elder’s attention on the extremity and will reduce its neglect and the development of learned nonuse.27,29 Before any active or passive motion is expected of the elder, the COTA must first passively mobilize the elder’s scapula to ensure that it glides when the arm is moved. The scapula may not glide sufficiently or may stop altogether because of muscle paralysis or hypertonus. Consequently, the COTA should never flex or abduct the shoulder of elders more than 90 degrees unless the COTA can be sure that the scapula is gliding properly. If elders do not have active scapular control, the COTA can passively move the scapula while ranging the shoulder. When the shoulder is flexed more than 90 degrees, the scapula glides downward on the posterior wall of the rib cage. In addition, the inferior border, or angle, of the scapula rotates slightly upward. When the shoulder is abducted more than 90 degrees, the scapula glides toward the vertebral column and the inferior border rotates slightly downward.
If elders have minimal or no active movement in the hemiplegic upper extremity, they should be instructed to move it by holding their hands together in one of two ways. If the elder has any active movement in the hand, clasping the hands with the thumb of the hemiplegic hand on top is recommended. If there is no movement in the hand, the uninvolved hand should be placed on the ulnar side of the hemiplegic wrist and hand and the uninvolved thumb in the palm of the hemiplegic hand. This method will protect the small joints of the hemiplegic hand and will maintain the arches in the palm. While holding onto the hands using either method, elders should be instructed to extend the elbows and hold the shoulders flexed at approximately 90 degrees. With the arms in this position, elders can go from a supine to a side-lying position, from a sitting to a standing position, or they can hold on to the knee of the hemiplegic lower extremity to cross it during dressing and bathing and during other functional activities. The COTA’s imagination and creativity are essential in assisting elders to use this two-hand technique to perform numerous functional activities such as picking up a mug to drink and mixing a cake. In addition, elders can flex or abduct the hemiplegic shoulder themselves by guiding the arm when the hands are held together. This bilateral integration assists with normalizing tone and encourages elders to actively care for the hemiplegic upper extremity.23
Elders may develop shoulder-hand syndrome if the hemiplegic upper extremity is not managed appropriately. This syndrome is characterized by swelling or edema that is usually observed in the hand but may also be present in the forearm and upper arm, tenderness, loss of range of motion, and vasomotor degradation. Pain and subluxation of the glenohumeral joint may not necessarily be present. The COTA should address all of these problems immediately to avoid irreversible atrophy of bones, skin, and muscles.23 The swelling is best decreased by filling a bucket or pail two-thirds full with crushed ice and adding cold water to the level of the ice. Elders should sit, while maintaining good alignment, with the bucket in front of them, which is placed on the floor, and should lean forward to place the hemiplegic hand and wrist in the water. The edematous hand should be kept in the water for 3 to 5 seconds, and this process should be repeated three times. The COTA should dry the hand gently with a towel. The COTA should ask the elder to flex the fingers, if possible, or the COTA should provide gentle passive ranging of the fingers and hand. The whole procedure should be done repeatedly during the day until swelling subsides. While the COTA is providing the range of motion exercise, retrograde massage while the limb is elevated can also be done, and a simple cock-up splint can be used to hold the wrist in extension (no more than 30 degrees) to help reduce the buildup of fluid in the hand when elders are not receiving therapy (Figure 19-3). Swelling also occurs from decreased muscle activity to move the fluid from the limb, dependent positioning, and trauma.
FIGURE 19-3 A modified cock-up splint holds the wrist in slight extension and helps reduce fluid buildup in the hand.
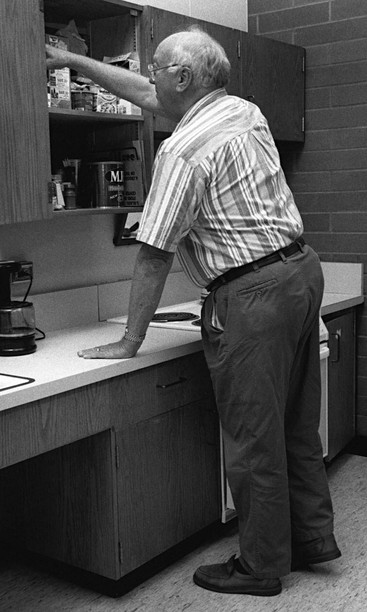
COTAs can use graded activities to facilitate voluntary control of an elder’s hemiplegic upper extremity. Such activities should be geared toward developing control in a progression from shoulder to elbow to hand. Elders may develop control in the hand before the more proximal parts of the arm. Despite the apparent control in the hand, the COTA should first facilitate active movement in the shoulder by engaging elders in activities that emphasize the body moving on the arm while the hand is maintained in weight bearing. The weight-bearing surface of the hand is limited to the lateral surface of the thumb, the thenar eminences, and the fingertips. In this position the palm of the hand is free and not in contact with the weight-bearing surface. Weight bearing on the hand does not need to be forceful, and elders should never have the hand completely flattened. Placing weight on a flat hand can lead to loss of the normal and functional arches of the hand and, consequently, can interfere with elders’ abilities to develop grasp later. Placing weight on the hand can be done in both sitting and standing positions. In a sitting position, for example, an elder’s affected hand can be placed in a weight-bearing position on the table or on a stool placed next to the elder. In a standing position, the elder should be taught to place the affected hand on a weight-bearing surface such as a table or countertop while performing functional tasks, such as putting away dishes or groceries or folding laundry (Figure 19-4). As control of the shoulder increases, activities should be introduced that emphasize free movement of the hemiplegic extremity on the more stable part of the body. During all of these activities, the COTA should continue to ensure that good body alignment is maintained and that elders are not using abnormal movements in one part of the body to obtain control in another.
COTAs should instruct elders in proper one-handed dressing techniques to protect the hemiplegic upper extremity and to avoid falling. Dressing should be done while sitting in a chair and, in general, the hemiplegic extremity should be dressed first and undressed last to avoid pulling on it or twisting it unnecessarily. Front-buttoned shirts or blouses are easiest to don by first dressing the hemiplegic arm and then draping the shirt over the shoulders by holding on to the shirt collar with the other arm. When the shirt is draped over the opposite shoulder, the elder can reach into the sleeve with the unaffected arm. This procedure is reversed when taking the shirt off. The process is similar when putting on pants, with the exception that the elder should cross the hemiplegic leg over the opposite leg to dress the hemiplegic leg first. If the elder is able to stand to pull up the pants, the elder may do so when both legs are clothed. If standing is not possible, the elder can shift weight to each side while sitting in the chair and gradually can pull the pants up over the buttocks.
All of the principles mentioned previously should be considered when training elders in functional activities or selecting assistive equipment. Although progress may seem slower at the beginning, following these principles can make a marked difference in the quality of movement that elders develop. When tasks are too difficult, elders are more likely to use abnormal movement patterns, become fatigued quickly, and become discouraged. The COTA must use good observation and clinical reasoning skills in selecting activities that challenge elders at the appropriate levels.
Visual-Perceptual-Cognitive Deficits
Although the motor deficits resulting from a stroke are the most easily observed, many less visible problems can severely hinder the rehabilitation process if not appropriately addressed. Depending on the type of brain lesion, the individual may have sensory disturbances that range from a total absence of sensation to a heightened perception of pain and other distorted sensations. These problems are accentuated when the individual has a body scheme disorder or difficulties planning motor actions, which is known as apraxia. Consequently, the individual has difficulty integrating and using any perceptual input from the hemiplegic side. Visual–perceptual deficits common in strokes include hemianopsia, poor figure ground perceptions, and difficulty with spatial relationships. Unilateral neglect results from a unique constellation of these symptoms when elders have no sense that the hemiplegic side of the body even exists, and they fail to visually scan toward that side.34,35 All of these disorders should be addressed simultaneously during intervention, using bilateral functional activities that encourage the use of the hemiplegic side of the body. The use of normal movement will provide repeated sensory stimulation to the hemiplegic side and relay information that will be processed in the brain and used as feedback in determining where each body part is and what it is doing. Consequently, the COTA should grade a variety of motor and sensory activities so that they maximize the elders’ abilities to control movement independently and provide increased sensory input. However, the activities should not be so overwhelming that they cause withdrawal reactions or increases in abnormal tone. Various textures, smells, colors, distances, and depths can be graded during most functional activities. In addition to these remedial approaches, the COTA should teach elders to compensate for deficits by providing repeated practice in establishing habits of visually scanning the hemiplegic side and methodically protecting and integrating the hemiplegic extremities in whatever activity they may be involved.
Other areas of concern for the COTA include elders’ abilities to comprehend and produce language and to plan and safely perform activities. As a result of stroke, elders may not be able to understand what others are saying, a condition known as receptive aphasia, or may not be able to produce the words they intend to utter, a condition known as expressive aphasia, or both disorders may be present, which is known as global aphasia. These disorders may also extend to nonverbal language because elders may be unable to interpret or appropriately use gestures. Language deficits are usually treated by the speech language pathologist, but strategies must be reinforced during OT intervention. When talking to elders, COTAs should keep instructions and explanations simple and concrete and should state them in an empathetic, patient way. Demonstration is usually helpful. The best way to ensure that elders have understood the instructions is to observe their performance.34,36
Cognitive dysfunction is often believed to be a major cause for failure of elders to reach rehabilitation goals and must be considered, particularly when planning for discharge.37 Safety may be compromised if elders cannot plan activities, make judgments, solve problems, or express verbally their needs for emergency care. For example, limited memory may cause elders to overmedicate themselves or not turn off the stove after cooking. Being unable to remember all of the steps involved in a task may mean that elders can often be surprised by the outcome. Elders may get stuck on a step and may be unable to determine what to do next or may neglect to realize that something dangerous could happen if an inappropriate action is taken. OT intervention, as mentioned earlier, should involve graded repetition of procedures until elders can routinely perform them safely. Emphasis should be placed on varying the context or situation in which the procedure is practiced to enhance learning.38
Emotional Adjustment
COTAs should consider the emotional adjustment of elders to the disability caused by the stroke. Depression, a common reaction to any catastrophic event, is one of the most undiagnosed and untreated responses to stroke.39,40 Depression may be caused from natural grief trying to cope with the loss of function, but also may be caused by the location of the lesion in the brain, previous or family history of depression, and social functioning before the stroke. Mild or major depression can develop from 2 months to 2 years after the stroke in up to 53% of clients.40,41 Anxiety, poor frustration tolerance, denial, anger, and emotional lability are all signs that elders are struggling to deal with the reality of their condition. COTAs must listen empathetically and supportively, while sensitively maintaining the focus on areas of realistic recovery. Permitting elders to control choices in intervention as much as possible can reinforce the sense that they can affect their environments. Although a complete recovery cannot be guaranteed, neither can a lack of recovery. COTAs must honestly explain to elders that residual limitations will probably be present, but the best chance for recovery will occur by the practice of skills. COTAs should use their creativity and ingenuity skills to help elders adapt tasks or environments that elders consider lost, thus instilling new hope and motivation in the rehabilitation process. As with any area of intervention, family and social involvement is crucial for elders to accept residual limitations and maximize their residual abilities. Ultimately, elders must see that they can continue to be effective in some measure and can still actively pursue activities and ideals they valued highly before the stroke.
Case Study
Gabriel is a 75-year-old man who recently returned home after having a left Middle Cerebral Artery stroke. He had spent three weeks in an acute care hospital followed by three weeks in a rehabilitation center. The rehabilitation team concluded that with the right supports, Gabriel would be safe at home. At the time of discharge home he had some residual weakness of the right side of his body, particularly the leg. He was able to flex the hip and knee against gravity, but continued to have the tendency to drag the foot when he walked. He still had some difficulties coordinating is right arm, and tended to ever-reach with it, on occasion knocking objects off tables, counters and shelves. The discharge report from the occupational therapists at the rehabilitation hospital indicated that Gabriel was able to feed, toilet, and dress himself independently, although on occasion became confused about the sequencing of dressing tasks.
John, an OTR, and Pam, a COTA, evaluated Gabriel as part of the home-health team and noted that Gabriel still had a slight decrease in tactile abilities with this right, dominant hand. They noted a slight droop in the right side of his face was still present, and that his lingual control toward the right side was also reduced. They confirmed that Gabriel was able to dress and toilet himself, but discovered that although he had been able to shower himself in the hospital, at home this would require transferring into an old-fashioned bathtub. This tub was higher than the standard tub in which he had been evaluated at the hospital. John and Pam determined that without grab bars for safety, Gabriel would need minimal to moderate assistance with his shower for safety.
John and Pam included an analysis of Gabriel’s home and supports in their intake evaluation. Gabriel lived in a first floor apartment which had wooden floors. There were several floor rugs that Gabriel had collected in his travels. The furniture was already arranged in a way that John and Pam believed would not interfere with Gabriel’s safety. They noted that Gabriel lived alone, although his younger brother visited every day and lived only a few blocks away. Up to the time of the stroke, Gabriel had been driving his car to get to the grocery store and move around in the community.
Case Study Review Questions
1. Should John and Pam conduct any additional evaluations to determine Gabriel’s needs? What additional information should they consider before finalizing the intervention plan?
2. What interventions should John and Pam implement to help Gabriel continue to make gains in his neuromuscular functions?
3. What strategies should be considered to assure Gabriel’s safety in the kitchen considering his remaining neuromuscular deficits?
4. What precautions should be considered given Gabriel’s facial droop and limited lingual control?
5. What safety measures should be considered in Gabriel’s home to assure it is a safe environment for him?
6. What alternatives for community access should be considered with Gabriel?
1. Sit at the edge of a bed or chair and lift up the left side of your pelvis. What happens with your spine and trunk when you do this? What occurs with the imaginary midline of the body when you sit in this position? Where on your thighs do you feel the most pressure while sitting in this position? Can you tell any difference in how your arms work while sitting this way? How would you feel after sitting in this position for 10 or 15 minutes?
2. Sitting on a firm chair, make sure that your pelvis is as far back in the chair as possible and your back is well supported. From that position, without moving forward, attempt to stand. What did you do with your arms while attempting to stand? How much work did your trunk have to do to get you to a standing position? Now repeat the activity, but first scoot to the edge of the chair before you stand. Did you notice any differences in the amount of work that your upper trunk and arms had to do to get you upright? From which position was it easier to stand?
3. Sitting at the edge of a chair with your trunk well aligned, move your feet as far forward as you can, making sure that they are flat on the floor. From that position, attempt to stand. Were you able to do so? How much work did your upper trunk and arms have to do? Return to sitting at the edge of the chair, and now attempt to stand again, but first place your feet as far back behind your knees as possible. Was standing from this position more or less difficult than your first attempt? Did you fall forward? Now return to sitting at the edge of the chair, and this time place your feet so that your toes are directly aligned below your knees and are flat on the floor. Did this help keep your midline where it should be, even during movement?
1 Orrison W. Atlas of Brain Function, 2nd ed. New York: Thieme Medical; 2008.
2 Siegel A., Sapru H. Essential Neuroscience. Baltimore: Lippincott Williams & Wilkins; 2006.
3 Umphred D. Neurological Rehabilitation, 5th ed. St. Louis, MO: Mosby; 2006.
4 Kung H., Hoyert D., Xu J., Murphy S. Deaths: Final data for 2005. Centers for Disease Control National Vital Statistics Reports. 50(20), 2008.
5 Carandang R., Seshadri S., Beiser A., Kelly-Hayes M., Kase C., Kannel W., et al. Trends in incidence, lifetime risk, severity, and 30-day mortality of stroke over the past 50 years. Journal of the American Medical Association. 2006;295:2939-2946.
6 Russo A., Andrews R. Hospital stays for stroke and other cerebrovascular diseases: Statistical brief #51. Washington, DC: Agency for Healthcare Research and Quality; 2008. Retrieved November 19, 2009, from http://www.hcup-us.ahrq.gov/reports/statbriefs/sb51.pdf
7 Centers for Disease Control and Prevention. Prevalence of stroke—United States, 2005. Morbidity and Mortality Weekly Report. 2007;56(19):469-474.
8 American Heart Association. Heart disease and stroke statistics—2008 update. Dallas, TX: Author; 2008.
9 Feigin V., Lawes C., Bennett D., Anderson S. Epidemiology of stroke. In: Stein J., Harvey R., Macko R., Winstein C., Zorowits R., editors. Stroke Recovery and Rehabilitation. New York: Demos; 2009:31-44.
10 Duncan P., Zorowitz R., Bates B., Küst J., Rietz C., Karbe H. Management of adult stroke rehabilitation care: A clinical practice guideline. Stroke. 2005;36:e100-e143.
11 Mackay J., Mensah G. Atlas of Heart Disease and Stroke. Geneva, Switzerland: World Health Organization Press; 2004.
12 Bernhardt, J., Thuy, M., Collier, J., Legg, L., 2009. Very early versus delayed mobilization after stroke. Cochrane Database of Systematic Reviews, Issue 1. Art. No.: CD006187. DOI: 10.1002/14651858.CD006187.pub2.
13 Jones S., Auton M., Burton C., Watkins C. Engaging service users in the development of stroke services: An action research study. Journal of Clinical Nursing. 2008;17(10):1270-1279.
14 Swayne O., Rothwell J., Ward N., Greenwood R. Stages of motor output reorganization after hemispheric stroke suggested by longitudinal studies of cortical physiology. Cerebral Cortex. 2008;18(8):1909-1922.
15 Legg, L., Drummond, A., Langhorne, P., 2006. Occupational therapy for patients with problems in activities of daily living after stroke. Cochrane Database of Systematic Reviews, Issue 4. Art. No.: CD003585. DOI: 10.1002/14651858.CD003585.pub2.
16 Moyers P.A. The Guide to Occupational Therapy Practice, 2nd ed. Bethesda, MD: American Occupational Therapy Association Press; 2007.
17 American Occupational Therapy Association. Occupational therapy practice framework: Domain and process, 2nd ed. American Journal of Occupational Therapy. 2008;62(6):625-683.
18 Kelley R., Borazanci A. Stroke rehabilitation. Neurological Research. 2009;31(8):832-840.
19 American Occupational Therapy Association. Occupational Therapy Code of Ethics. American Journal of Occupational Therapy. 2005;59:639-642.
20 Gillen G., Burkhardt A. Stroke Rehabilitation: A Function-Based Approach, 2nd ed. St. Louis, MO: Mosby; 2004.
21 Sawner K., Lavigne G. Brunnstrom’s Movement Therapy in Hemiplegia: A Neurophysiological Approach. Hagerstown, MD: Lippincott Williams & Wilkins; 1992.
22 Schabrun S., Hillier S. Evidence for the retraining of sensation after stroke: A systematic review. Clinical Rehabilitation. 2009;23(1):27-39.
23 Davies P. Steps to Follow: The Comprehensive Treatment of Patients with Hemiplegia, 2nd ed. New York: Springer-Verlag; 2004.
24 Adler S., Beckers D., Buck M. PDF in Practice: An Illustrated Guide, 3rd ed. New York: Springer-Verlag; 2003.
25 Thaut M., Leins A., Rice R., Argstatter H., Kenyon G., McIntosh G., et al. Rhythmic auditory stimulation improves gait more than NDT/Bobath training in near-ambulatory patients early post-stroke: A single-blind, randomized trial. Neurorehabilitation and Neural Repair. 2007;21(5):455-459.
26 Hafsteinsdóttir T., Algra A., Kappelle L., Grypdonck M. Neurodevelopmental treatment after stroke: A comparative study. Journal of Neurology, Neurosurgery. 2005;76(6):788-792.
27 Azab M., Al-Jarrah M., Nazzal M., Maayah M., Sammour M., Jamous M. Effectiveness of constraint-induced movement therapy (CIMT) as home-based therapy on Barthel Index in patients with chronic stroke. Topics in Stroke Rehabilitation. 2009;16(3):207-211.
28 Hammer A., Lindmark B. Effects of forced use on arm function in the subacute phase after stroke: A randomized, clinical pilot study. Physical Therapy. 2009;89:526-539.
29 Blanton S., Wilsey H., Wolf S. Constraint-induced movement therapy in stroke rehabilitation: Perspectives on future clinical applications. Neurorehabilitation. 2008;23(1):15-28.
30 Dohle C., Püllen J., Nakaten A., Küst J., Rietz C., Karbe H. Mirror therapy promotes recovery from severe hemiparesis: A randomized controlled trial. Neurorehabilitation and Neural Repair. 2009;23(3):209-217.
31 Ezendam D., Bongers R., Jannink M. Systematic review of the effectiveness of mirror therapy in upper extremity function. Disability & Rehabilitation. 2009;31(26):2135-2149.
32 Yavuzer G., Selles R., Sezer N., et al. Mirror therapy improves hand function in subacute stroke: A randomized controlled trial. Archives of Physical Medicine and Rehabilitation. 2008;89(3):393-398.
33 Kumar P., Swinkels A. A critical review of shoulder subluxation and its association with other post-stroke complications. Physical Therapy Reviews. 2009;14(1):13-25.
34 Wolf T., Baum C., Conner L. Changing face of stroke: Implications for occupational therapy practice. American Journal of Occupational Therapy. 2009;63(5):621-625.
35 Cappa S. Neglect rehabilitation in stroke: Not to be neglected. European Journal of Neurology. 2008;15(9):883-884.
36 Bowen, A., Lincoln, N., 2007. Cognitive rehabilitation for spatial neglect following stroke. Cochrane Database of Systematic Reviews, Issue 2. Art. No.: CD003586. DOI: 10.1002/14651858.CD003586.pub2.
37 Woodson A. Stroke. In: Trombly C., editor. Occupational Therapy for Physical Dysfunction. 6th ed. Baltimore, MD: Williams & Wilkins; 2007:1001-1041.
38 Barrett A., Buxbaum L., Coslett H., Edwards E., Heilman K., Hillis A., Milberg W., Robertson I. Cognitive rehabilitation interventions for neglect and related disorders: Moving from bench to bedside in stroke patients. Journal of Cognitive Neuroscience. 2006;18(7):1223-1236.
39 Schepers V., Post M., Visser-Meily A., van de Port I., Akhmouch M., Lindeman E. Prediction of depressive symptoms up to three years post-stroke. Journal of Rehabilitation Medicine. 2009;41(11):930-935.
40 National Institute on Mental Health. Preventive treatment may help head off depression following a stroke. Retrieved November 19, 2009, from http://www.nimh.nih.gov/science-news/2008/preventive-treatment-may-help-head-off-depression-following-a-stroke.shtml, 2008.
41 Fang J., Cheng Q. Etiological mechanisms of post-stroke depression: A review. Neurological Research. 2009;31(9):904-909.