7 Assessment of vital signs and changes in health status
• To help the student understand how to assess vital signs and recognise the changes within a patient's physical and mental health status
• To help the student to recognise and respond to the deteriorating patient on a medical placement
• To explore why a patient's health status may change and how this can affect their decision making
Introduction
Wherever you are placed during your medical placement, you will be involved in undertaking observations of patients' vital signs. Whether you are placed within an out-patient department, virtual ward, and medical ward or on medical day care, you will be undertaking physical and mental assessments of your patients from the first year to your final placement.
As students from all fields of nursing, you will have been exposed to simulated practice within the university. However, when you are undertaking observations of patients' vital signs during your medical placement, you may not find them as easy to perform as you did within simulated practice. Patients vary, and it can be daunting at first as patients are sick and your competence is also being assessed. Remember that your mentor is there to help, guide and supervise you and that you should not undertake any clinical skills alone until your mentor has assessed your competence. This assessment of competence should not be carried out on just one patient but with a variety of patients with differing health problems. Always ask for a rationale. As you progress towards your third year of training you will already be competent in the Essential Skills for years one and two (Nursing and Midwifery Council (NMC) 2010). However, your learning outcomes will be expecting you to demonstrate assessment skills, prioritisation and clinical decision making for a group of patients. Some students find this easier than others to achieve, however, good communication with your mentor regarding your learning needs can really help you to develop in this area.
Observations of vital signs and recognition of changes in your patients' health status will be an essential clinical skill within your learning outcomes regardless of your chosen field of nursing. Undertaking observations of vital signs and recognising changes in patients' health status will incorporate all of the NMC (2010) Standard Competencies – professional values, communication and interpersonal skills, clinical decision making, and leadership, management and team working. For example, within decision making, part of the standard competency states that: ‘decision making must be person-focused, and through a process of critical analysis learning to a range of technical and nursing interventions from basic to the highly complex’.
For communication, the NMC Competency states that nurses ‘must communicate safely and effectively with individuals and groups of all ages’ (NMC 2010) and you may find that your record of achievement/practice curriculum documentation has mapped the Essential Skills Clusters for care, compassion and communication with the specific competencies within the domains.
When you are undertaking your observations of vital signs, you will behave with professional values, communicate with your patients, make clinical decisions and often need to liaise with multidisciplinary teams (Box 7.1). You will also meet some of the Essential Skills Clusters while undertaking observations of vital signs, for example some of the organisational aspects of care, compassion and communication skills (NMC 2010).
Box 7.1 Some of the specific competencies that you might meet while undertaking observation of vital signs
Field Standard for Competence: Professional Values Domain, Adult:
All nurses must practise confidently according to the NMC (2010) code.
All nurses must recognise the limits of their own competence and knowledge. They must reflect on their own practice and seek advice from, or refer to, other professionals where necessary
Field Standard for Competence: Communication and Interpersonal Skills Domain
All nurses must use a range of communication skills and technologies to support person-centred care and enhance the quality and safety of health care. They must make sure that people receive all the information about their care in a language and manner that is right for them, and that allows them to make informed choices and consent to treatment.
Field Standard for Competence: Nursing Practice and Decision-Making Domain
Adult nurses must be able to carry out accurate health, clinical and nursing assessments across all ages and show the right diagnostic and decision-making skills. They must have the confidence to provide effective adult nursing care in the home, community and in the hospital settings.
Adult nurses must recognise early signs of acute illness in young people, adults and older people and accurately assess and start appropriate and timely management of those at risk of clinical deterioration, who are acutely ill or who need emergency care.
Demonstrating competence
What will your mentor expect to see you doing within the first year of your training and what will the mentor expect to see you doing differently as a more senior student? Hopefully the following will help you and your mentor to match expectations.
Within your first year
Your mentor will expect to see you do the following in your first year:
• Display the professional behaviour and conduct expected of a nurse, for example gaining agreement from the patient first and explaining what needs to be done.
• Report abnormalities – you may not understand why a patient has abnormal vital signs but you would be expected to report it.
As you progress through your first year you should try to think about the reasons why your patients' vital signs might be outside normal limits and think about the interventions that might help. If you do not know, ask your mentor and discuss the frequency of observations of vital signs, plan of care and evaluation. Also think about how this relates to pathophysiology.
Within your final year
Your mentor will expect to see you do the following in your final year:
• Demonstrate a patient-centred focus.
• Use the early warning score accurately.
• Detect changes and report, recheck, seek guidance.
• Clearly integrate theory and practice.
• Follow policy and role model professional practice behaviour.
• Be able to relate the patient's health problem to the patient, context and specialty, discuss care and articulate the rationale to the mentor.
• Initiate actions and interventions.
• Initiate, evaluate and reassess the plan of care using a structured approach.
• Be confident in communication with the multidisciplinary team.

At this point in your training, what do you think you should know about observations of vital signs? Look at your curriculum documentation for this placement and find out what your learning outcomes are with regard to vital signs and responding to changes in your patients' health status.
You will be expected to assess the physical and mental status of your patient and will be involved in assessing the following:
When we perform something very often, it is easy to forget the underlying theory and principles for practice. Here is a quick revision guide to the observations of vital signs that you undertake every day within your medical placements.
Quiz
(Answers on pp 127–133.)
Temperature
Also see this resource for a demonstration of taking a temperature:
http://www.cetl.org.uk/learning/temperature-a/player.html (accessed July 2011).
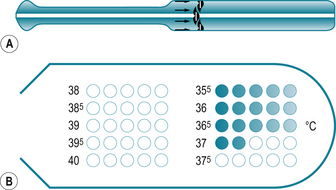
Fig 7.1 (A) Disposable chemical dot thermometer. (B) Recording area of a disposable thermometer
(Holland et al 2008, with permission)
Blood pressure
Also see these resources for a demonstration of taking BP:
http://www.cetl.org.uk/learning/bpm/player.html (accessed July 2011)
http://www.cetl.org.uk/learning/BP_Korotkoff_sounds/player.html

7.17. You are undertaking your placement on medical day care and are caring for Mustafa who has just had a gastroscopy. When you take his observations of pulse and BP, you find that he is tachycardic at 110 beats per minute and his BP has decreased to 90/60 mmHg. What are your thoughts? What could be happening to Mustafa? What nursing actions do you need to take to help Mustafa?
Respiration
7.19. What is the difference between type 1 and type 2 respiratory failure?
7.22. What is a normal respiratory rate?
7.23. How do you assess a patient's respiratory function?
7.24. What does an abnormal respiratory rate mean?
7.25. Your patient, Henry, is a patient on the virtual ward. He has a long-term health problem of chronic obstructive pulmonary disease (COPD) and when you visit him you notice that he has difficulty speaking in full sentences, has an elevated respiratory rate of 32 breaths per minute and is anxious. What nursing actions could you undertake to help Henry's breathing? Who else might you need to inform?
Peak expiratory flow rate
7.32. What is peak expiratory flow rate?
7.33. Why and how do we check it?
7.34. What is the normal peak flow reading (predicted or expected)?

7.35. Imran is a 28-year-old man admitted to the acute medical admissions ward with an acute asthma attack. His morning peak flow is 200 L/min, respiratory rate 28/min and saturations 92%. What would your nursing actions be at this point?
Also see this resource for a demonstration of peak flow monitoring:
http://www.youtube.com/watch?v=oHRTiytvuow(accessed July 2011).
Neurological status of your patient
The neurological status of your patient is equally important as an indicator of how well your patient is. One of the simplest ways of monitoring neurological status is by using a simple tool called AVPU:
Sometimes you may look after a patient for more than one shift and you may find that you notice a change in how alert they are – sometimes this can be quite a subtle change where your patient seems drowsy or there might be a very sudden change to unresponsive. Another tool that is commonly used is the Glasgow Coma Scale (Fig. 7.5), which comprises of scores for three different measurements – best verbal response, best eye response and best motor response (Brooker & Waugh 2007). The Glasgow Coma Scale takes a lot of practice and it will be helpful for you and your mentor to discuss this in detail when you are caring for a patient who requires this observation, for example a patient who has suddenly become unresponsive or has suffered a cerebral vascular accident.
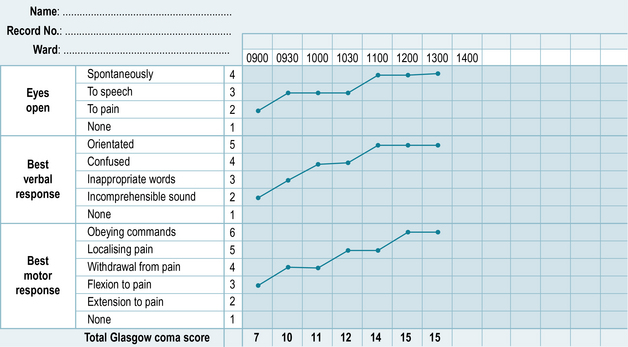
Within the best motor response, a patient may have a long-term health problem such as a cerebral vascular accident, Parkinson's disease or multiple sclerosis which will mean that they would normally not score 6/6 for that section.
Within the best verbal response, a nurse will be assessing whether a patient is confused, however, this may be a feature of a number of neurological health problems, such as dementia, and therefore the patient would never score 15/15. What is important in this case is that, within your assessment, you establish the cognitive status of your patient when they are well. It is therefore very important that you have the tools, knowledge and skills to detect a deterioration in cognitive status, e.g. delirium.
Delirium
One common syndrome you may come across during your medical placement is delirium. This may also be referred to as acute confusion. Patients suffering from delirium can sometimes be challenging to care for and it can provoke anxiety for you if this is something you have not had much experience with. It is important to remember that delirium is also very distressing for the patient and their relatives and they will need a lot of reassurance during this time. By understanding a little more about what causes delirium and how to prevent and manage it, you may be able to provide some reassurance to both your patient and their relatives.
Delirium can be characterised by ‘disturbed consciousness, cognitive function or perception, which has an acute onset and fluctuating course’ (National Institute for Health and Clinical Excellence (NICE) 2010).
Although delirium can affect about a quarter of older medical in-patients, it can also affect younger people and some patients will be more at risk of developing delirium than others, for example those who have had a stroke.
Recognising delirium is important and nurses are often those most likely to observe changes in someone's mental state or behaviour, especially if the changes are quite subtle. Delirium is often associated with severe, acute illness and may be a sign that your patient is deteriorating.
Any patient can develop delirium but some are more at risk of developing it than others. Those most at risk are the following:
• People with dementia or other cognitive impairments.
• People with sensory impairments – poor eyesight, poor hearing.
• Those who are immobile/physically frail.
This Website offers excellent explanations about this problem and links to other resources:http://www.nmhdu.org.uk/our-work/mhep/later-life/lets-respect/ (accessed July 2011).

What are the common causes of delirium you might come across in your medical placements?
How would you determine the difference between a chronic cognitive impairment such as dementia and an acute problem like delirium?
It is important to be able to determine the difference between a chronic cognitive impairment such as dementia and an acute problem like delirium. Box 7.2 shows the main features of delirium.
Box 7.2 The main features of delirium
 Rapid onset, e.g. hours, days, weeks.
Rapid onset, e.g. hours, days, weeks.
Fluctuating behaviour – comes and goes or increases/decreases in severity.
Disturbed level of consciousness, e.g. drowsy or hyperalert.
Reduced ability to focus or concentrate, easily distracted.
Rambling, incoherent, switching from one subject to another.
The confusion assessment method (CAM) is a useful screening tool to use to help identify delirium (Inouye et al 1990) (see Box 7.3).
Box 7.3 Confusion assessment method (CAM)
If features 1 and 2 and either 3 or 4 are present, your patient is likely to be suffering from delirium:
Feature 1 – acute onset and fluctuating course
This information would usually be obtained from a family member or carer and is shown by positive responses to the questions: Is there evidence of an acute change in mental status from the patient's baseline? Does the (abnormal) behaviour fluctuate during the day, that is tend to come and go, or increase and decrease in severity?
Feature 2 – inattention
This feature is shown by a positive response to the following question: Did the patient have difficulty focusing attention, for example being easily distracted or having difficulty keeping track of what was being said?
Feature 3 – disorganised thinking
This feature is shown by a positive response to the following question: Was the patient's thinking disorganised or incoherent, such as rambling or irrelevant conversation, unclear or illogical flow of ideas or unpredictable switching from subject to subject
Feature 4 – altered level of consciousness
This feature is shown by any answer other than ‘alert’ to the following question: Overall how would you rate this patient's level of consciousness? Alert (normal), vigilant (hyperalert), lethargic (drowsy, easily aroused), stupor (difficult to arouse) or coma (unarousable).
Think of a confused patient who you have cared for during your medical placement. Did you recognise any of the four features of the CAM tool? Were you aware that this patient had delirium? Consider what you might do differently in the future when caring for a confused patient.
With experience, you will be able to identify delirium quite quickly, especially if you are aware of the kinds of patients who are more likely to develop it and are actively looking out for it.
Talk to your mentor and begin to identify those patients most at risk and then start to look out for the features described in the CAM assessment.
As delirium is a sign that your patient is acutely unwell, it is vitally important that you act on it quickly. As a student nurse, your main priority should be making the nurse and doctor looking after the patient aware of your assessment. Be prepared to explain how you feel your patient's mental state has changed and refer to the CAM criteria.
Treating and managing delirium
The most important aspect of managing delirium is to identify and treat the underlying cause, for example infection, dehydration, polypharmacy (a person who is prescribed multiple medications). While the cause is being sought and treated, the management of the patient's confused state and the prevention of complications are largely the role of the nursing staff. Consider the following case history 7.1.

Mohammed is a 55-year-old male who has presented at accident and emergency with a 5-day history of worsening shortness of breath and a productive cough. He has a history of COPD. He is transferred to the medical ward accompanied by his wife. On arrival to the ward he is agitated and is trying to pull out his intravenous cannula and IV fluids. He doesn't want to stay in hospital and his wife has to persuade him to stay.
When you speak to his wife she says that he is not normally confused, but has become increasingly confused over the last 3 days, especially at night. Mohammed speaks English and when you speak to Mohammed he says he is fine and doesn't need to be in hospital. He keeps interrupting you, saying that he is being kept here against his will. He is not able to answer any questions about his usual state of wellbeing or activities of daily living and is unable to focus on what you are trying to explain to him, constantly asking to go home.
Later in the evening when his wife has left the ward, he pulls out his intravenous cannula and falls over trying to get out of bed to get to the toilet. When the nursing staff get to him, he has been incontinent of urine on the floor.
The likely underlying cause for Mohammed's delirium is a chest infection. This would be confirmed by doctors through a physical assessment, chest X-ray and blood tests.
The following should be the main themes of the nursing care and management of a patient with delirium such as Mohammed:
• Provide frequent orientation and explanations – patients may not remember where they are or why they are in hospital. Regular gentle reminders may help to relieve some anxieties. Always introduce yourself and tell the patient what you are there to do.
• Avoid any unnecessary moves within the ward or between wards. Sometimes it is necessary to move a patient to another ward, for example to receive specialist care or to another bed within a ward (to be barrier nursed or to be seen more closely from the nurses' station). This should be avoided if at all possible in a patient with delirium, as a move will disorientate them more. As a student, you will not have any control over if or where patients move, but as you progress and begin learning to manage a ward or group of patients, this will be something you need to take into consideration. Good forward planning as to which bed to place a delirious patient in before they get to the ward is ideal.
• Involve relatives – patients with delirium often respond better to people they know. Involving relatives as much as they would like in the care of the person with delirium will often help to keep the person calm during drug administration, at mealtimes, etc. Be careful not to place too much pressure on relatives to be involved, but welcome any involvement they wish to have.
• Provide reassurance and explanations – this needs to be for the family as well as the patient. The patient will be anxious as they may not remember where they are or why things are happening to them. The relatives will be anxious as they are seeing their loved one in a distressed state. Explaining why the person has delirium, what it is and how long it is likely to last will help to reassure the patient and their family.
• Reduce environmental stimulation and ensure good lighting – unfamiliar noises such as equipment beeping, call bells and telephones ringing, televisions or radios in other rooms or by other beds can confuse the person with delirium more. Therefore, keeping noise to a minimum will help to promote calm. The dark can be very disorientating and frightening for someone with delirium so, where possible, leave a night light on.
• Encourage independence and mobility – early mobilisation and return to a usual routine (e.g. toileting, washing and dressing) will prevent the person with delirium becoming too dependent and prevent functional decline. The more frail and dependent a person is, the more susceptible they are to developing delirium.
• Ensure hearing aids are working and glasses are clean – if the person with delirium has a hearing or visual impairment and this is not corrected, it will make them more confused and disorientated.
• Control pain – pain in itself can cause delirium, so managing pain appropriately is an important aspect of managing delirium.
• Ensure adequate food and fluid intake – patients with delirium often don't eat and drink as much as they should do. It is important that they are encouraged and assisted to eat and drink regularly. By employing some of the techniques above to manage agitation and allowing enough time at mealtimes and easy access to food and drink throughout the day, it should be possible to ensure an adequate food and fluid intake. But remember, depending on the underlying cause of the delirium, their fluid intake requirements may have increased so intravenous or subcutaneous fluids may be necessary too. As a patient with delirium may be agitated and likely to pull out any intravenous or subcutaneous lines, you should aim to use these as a means of hydration for as short a time as possible, encouraging oral fluids as often as you can. It may be necessary to give intravenous or subcutaneous fluids overnight if the patient is restful, as they may be less likely to pull them out.
• One-to-one nursing – sometimes it is necessary to provide one-to-one nursing for a patient with delirium, particularly if they are at high risk of falling or are not concordant with essential therapy, for example oxygen. This should only be necessary for a short period of time while the treatment for the underlying cause gets underway. If you are asked to provide one-to-one care then following the actions mentioned above should be the aim of the care you give.
You now have the knowledge to care for someone with delirium. Using this information, write a care plan for the management of Mohammed's delirium.
By adhering to the above principles of care it is also possible to prevent delirium occurring, especially in those patients that are at more risk of developing it than others.
In most patients, delirium resolves as the underlying cause is treated. You may find that some patients will remember different aspects of their delirium which they may find distressing. If they do mention this to you, don't be afraid of explaining what happened when they were delirious as this may help to reassure them that they are not imagining things that did not happen. It may help them to speak to a counsellor who specialises in this or a member of the mental health team. Speak to your mentor about the services available in your organisation and how referrals are made. In some cases, delirium doesn't resolve completely – it may take longer in some patients than others. If there is a concern that delirium is not resolving, the patient should be referred to a specialist mental health team. Again, ask your mentor if you can be involved in making the referral and, if possible, be with the patient when they are assessed by the specialist team. This will give you a good insight into how they are assessed and an opportunity to ask more questions about delirium.
Within the NMC Domain, Communication and Interpersonal Skills (NMC 2010), there are adult field-specific competencies that require nurses to demonstrate that they ‘interact with people who find it hard to communicate for any reason’ and ‘to people who are anxious or in distress’.
There are also NMC Domains for nursing practice and decision making which incorporate adult field-specific competencies that will require you to ‘recognise and interpret signs of normal and changing health, distress or capability’ and ‘recognise the early signs of acute illness in young people, adults and older people, accurately assess and start appropriate and timely management of those at risk of clinical deterioration who are acutely ill or need emergency care’.
Now look carefully at the learning outcomes for your medical placement and try to identify how caring for a patient with delirium could help you to achieve some of them. Discuss them with your mentor.
Caring for a patient with delirium can be anxiety provoking when you are unfamiliar with it so seek support from your mentor and other staff on the ward. Ask them how they approach such patients, what sort of things they find work well and what don't work so well. Watch the way they communicate with the person and seek out role models with good communication skills. As a more experienced student, use the opportunity to reassure your junior student colleagues and role model your own developing communication skills.
How to detect and recognise the deteriorating patient in your medical placement
Most hospitals will have an early warning scoring system for observations of vital signs to detect patients who are deteriorating. If a patient observation of vital signs scores a certain number, you will be expected to take action. In acute hospitals, there is usually a team of nurses and doctors who will be contactable by bleep and these teams are often called outreach teams.
Who is in the outreach team?
The outreach team usually belongs to a high-dependency or intensive care unit and are contacted by any member of the hospital staff if a patient's observations score indicates deterioration. They normally carry bleeps, hospital aircalls or mobile phones and will come and assess a patient when contacted. The team is normally made up of anaesthetists, physicians and nurses and is a 24-hour service. In some areas there may be another system for out of hours which involves contacting the site nurse practitioners or senior nurses/matrons.
The purposes of these outreach teams are to (Intensive Care Society 2002):
• Avert admission to critical care.
• Facilitate timely admission to critical care and discharge back to the ward.
• Share critical care skills and expertise through an educational partnership.
• Ensure thorough audit and evaluation of outreach services.
Find out if your placement uses an early warning score. Discuss with your mentor how to use it and how it works. Find out if there is an outreach service in your placement area? How do you contact them? Who is in the team? Is it possible for you to spend a day with them during your placement?
The purpose of this score is to improve patient outcome by detecting and acting upon early signs of deterioration in hospitalised patients. This score was developed because we do not have the facilities to monitor all patients in high-dependency or intensive care beds. It allows us to identify the deteriorating patient before the situation becomes too profound and to treat the patient in a timely fashion.
In November 2007, NICE guidelines were published stating a need for track and trigger systems. They recommended the use of a scoring system that incorporates the monitoring of oxygen saturations (NICE 2007).
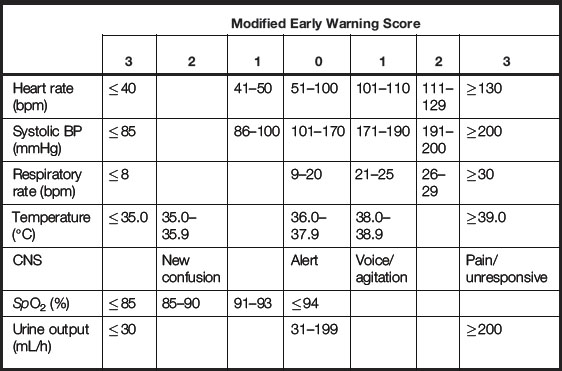
The Modified Early Warning Score (MEWS) is a simple scoring system suitable for use at the bed side; it is now based on seven physiological parameters:
This system works on a structured scoring system and simple algorithm leading to timely recognition of the deteriorating patient (Table 7.1).
The following articles will give you further insight into assessing an acutely unwell patient and the use of an early warning score:
As a student you will be undertaking the observations of vital signs and it will be important that you understand about this score and how to report and document it. Your mentor should inform you about this during your orientation to the ward and you may even get the opportunity to go round with the team or receive some teaching directly from the team.
Please use the MEWS provided and work out the score for each set of patient observations below:
1. Temperature 37 °C, BP 100/80, pulse 100, respirations 21, responds to voice and is passing 35 mL urine/hour.
2. Temperature 36.5 °C, BP 130/80, pulse 75, respirations 14, patient is alert and passing 40 mL urine/hour.
3. Temperature 36.5 °C, BP 90/60, pulse 120, respirations 26, patient is alert and hasn't passed urine for the last 5 hours.
4. Temperature 34 °C, BP 100/60, pulse 45, respirations 12, patient is responding to painful stimuli and hasn't passed urine for the last 2 hours.
Consider the medical placement scenarios on pages 124 and 125, involving Mr X and Mr R, where the outreach team was involved. These are not real life scenarios but are compiled by an outreach nurse, Claire Mcmullen, who has vast experience of working as an outreach sister. They are aimed at making you think about what your actions would be if you were the nurse undertaking these observations. Take time to think about what you would have done in the following scenarios.
Mr X is a 67-year-old man admitted via accident and emergency with a cough, shortness of breath and low O2 saturations (77%). He was discharged home from hospital 3 weeks ago following a 1-week stay on the intensive care ward.
Observations by outreach
Oxygen saturation 71% on 4-L O2 via nasal specs.
Equal air entry, bilateral wheeze, bilateral crackles.
Patient reports he has not passed any urine all day (no fluid balance chart).
Mr X was started on high-flow 15-L O2 via a reservoir bag (60%). A medical specialist registrar was called to see him, a full plan was written, nebulisers were given and IV fluid was started. He was reviewed regularly overnight and went home the next day.
Mr R is a 66-year-old man admitted to hospital with shortness of breath and treated for exacerbation of COPD. He was transferred to the medical ward.
Outreach involvement
Critical care outreach called by nursing staff as MEWS 4.
Nurse reported that she had called the doctor and he had seen Mr R. The doctor informed the nurse that Mr R was fine and just needed a bit more oxygen.
The staff nurse was not convinced that the patient was fine and decided to seek further help.
Summary
During this chapter you have been focusing on how to assess vital signs and recognise the changes within a patient's physical and mental health status. The activities and reflection points should help you to recognise and respond to the deteriorating patient on a medical placement whatever field of nursing you are in.
This chapter has also touched on the importance of communication when you are nursing your patients and this will be explored in more detail in Chapter 8.
Brooker C., Waugh A. Foundations of nursing practice: fundamentals of holistic care. Edinburgh: Mosby; 2007.
Holland K., Jenkins J., Solomon J., et al. Applying the Roper–Logan–Tierney model in practice, 2nd ed. Edinburgh: Churchill Livingstone; 2008.
Inouye S., Van Dyck C., Alessi C., et al. Clarifiying confusion: the confusion assessment method. Annals of Internal Medicine. 1990;113(12):941–948.
Intensive Care Society. Guidelines for the introduction of outreach services: standards and guidelines. London: Intensive Care Society; 2002.
Jamieson E.M., Whyte L.A., McCall J.M. Clinical nursing practices, 5th ed. Edinburgh: Churchill Livingstone; 2007.
Kelsey J., McEwing G. Clinical skills in child health practice. Edinburgh: Churchill Livingstone; 2008.
National Institute for Health and Clinical Excellence. Acutely ill patients in hospital: recognition of and response to acute illness in adults in hospital. London: NICE; 2007.
National Institute for Health and Clinical Excellence. Delirium: diagnosis, prevention and management. London: NICE; 2010.
Nunn A.J., Gregg I. New regression equations for predicting peak expiratory flow in adults. British Medical Journal. 1989;298:1068–1070.
Nursing and Midwifery Council. Standards for pre-registration nursing education. London: NMC; 2010.
Bellomo R., Goldsmith D., Uchino S., et al. Prospective controlled trial of effect of medical emergency team on postoperative morbidity and mortality rates. Critical Care Medicine. 2004;32(4):916–921.
Buist M., Bernard S., Nguyen T.V., et al. Association between clinical abnormal observations and subsequent in-hospital mortality: a prospective study. Resuscitation. 2004;62:137–141.
Cuthbertson B.H., Boroujerdi M., McKie L., et al. Can physiological variables and early warning scoring systems allow early recognition of the deteriorating surgical patient? Critical Care Medicine. 2007;35(2):402–409.
Department of Health. Comprehensive critical care. London: DH; 2000.
Fuhrmann L., Lippert A., Perner A., et al. Incidence, staff awareness and mortality of patients at risk on general wards. Resuscitation. 2008;77(3):325–330.
Goldhill D.R., White S.A., Sumner A. Physiological values and procedures in the 24 h before ICU admission from the ward. Anaesthesia. 1999;54:529–534.
Hillman K., Bristow P.J., Chey T., et al. Antecedents to hospital deaths. Internal Medicine Journal. 2001;31:343–348.
Jacques T., Harrison G.A., McLaws M.L., et al. Signs of critical health problems and emergency responses (SOCCER): a model for predicting adverse events in the inpatient setting. Resuscitation. 2006;69(2):175–183.
Kause J., Smith G., Prytherch D., et al. A comparison of antecedents to cardiac arrests, deaths and emergency intensive care admissions in Australia and New Zealand and the United Kingdom – the ACADEMIA study. Resuscitation. 2004;62:275–282.
MERIT Study Investigators. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. Lancet. 2005;365:2091–2097.
Richardson R. Clinical skills for student nurses: theory, practice and reflection. Devon: Reflect Press; 2008.
British Geriatric Society guidelines on deliriumhttp://www.bgs.org.uk(accessed July 2011)
Centre for Excellence in Teaching and Learning – a clinical skills resourcehttp://www.cetl.org.uk(accessed July 2011)
Let's Respect resourceshttp://www.nmhdu.org.uk/our-work/mhep/later-life/lets-respect/(accessed July 2011)
Answers
Temperature
7.1. Our body temperature represents the balance between heat gain and heat loss.
7.2. The body requires its temperature to remain stable for optimum cellular function. A body temperature above or below the normal range will affect total body function. It should be measured on admission and at regular intervals thereafter.
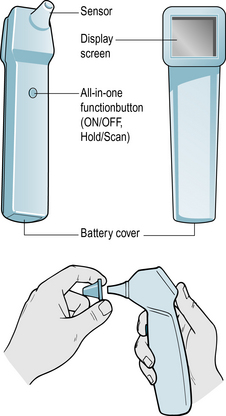
7.3. Common methods of checking temperature include tympanic thermometers and tempadots. When using any piece of equipment to check temperature, it is important to follow the manufacturer's instructions to ensure an accurate reading. When using tympanic thermometers, it is important to check the following:
Tempadot thermometers must be stored correctly in order to give accurate readings (check manufacturer's instructions).
7.4. A normal body temperature is between 36 °C and 37.5 °C.
Pulse
7.7. The pulse is a wave-like sensation that can be felt in any of the arteries lying close to the surface of the body. It reflects the heart rate.
7.8. As the pulse reflects the heart rate, any change in the pulse will indicate a change in the functioning of the heart. It is important to measure the pulse on admission and at regular intervals after that to monitor differences, detect trends or other defects.
7.9. Although dinamaps are commonly used to measure pulse rate, it is much more accurate to measure the pulse manually. The pulse most often used is the radial pulse as this is the most readily accessible. A pulse is measured by placing your second or third fingers along the appropriate artery and applying gentle pressure. The thumb and forefinger have pulses of their own that may be mistaken for the patient's pulse, so should not be used. The pulse should be counted for a full 60 seconds to give sufficient time to detect any irregularities. As well as counting the pulse rate, you should also note whether the rate is regular or irregular and whether the pulse is strong or weak. Any changes should be reported to the trained nurse looking after that patient. There is a temptation to just take the reading from the Dinamap but this will not tell you whether the pulse is regular or strong or weak.
7.10. In adults, a normal pulse rate would be 60–100 beats per minute.
7.11. A fast heart rate, over 100 beats per minute, could be the result of pain, raised temperature, stress, dehydration, bleeding, drugs and heart disease. A slow heart rate, under 60 beats per minute, could be the result of drugs or low temperature.
Blood pressure
7.12. Blood pressure is the force exerted by the blood against the walls of the blood vessels.
7.13. Blood pressure is an important indicator of cardiac function and blood volume. Consequently, changes in BP can indicate a serious deterioration of a patient's health problem. It should be monitored on admission and at regular intervals afterwards to detect any changes quickly.
7.14. Most nurses now rely on dinamaps to check a patient's BP but, where possible, you should also learn how to take BP manually. When using a dinamap, there are certain things you must do to ensure the reading is accurate:
Any changes should be reported immediately to the nurse in charge of the patient.
7.15. Blood pressure will vary between individuals and will depend on whether they are sitting, standing, have just stood up, etc. An average BP for an adult can range from 100/60 mmHg to 140/90 mmHg.
7.16. A low BP, with a systolic (top number) of less than 100, could be the result of dehydration, drugs, bleeding, hypovolaemic shock, septic shock, incompatible blood transfusion or postural drop. A high BP, with a systolic of above 170, could be the result of exercise, stress, raised temperature, pain, circulatory overload, early compensatory sign of shock or heart disease.
Respiration
7.18. The mechanism for supplying the body with oxygen and removing carbon dioxide.
7.19. You will sometimes hear the diagnosis type 1 and type 2 respiratory failure. Respiratory failure occurs when pulmonary gas exchange is sufficiently impaired to cause hypoxaemia with or without hypercarbia.
Type 2
7.20. As oxygen is a necessary requirement for all bodily functions, a change in respiratory rate is often the first indication that something is wrong with a patient's health. It will often change up to 24 hours before a change in pulse, BP or temperature. It should be checked on admission and at regular intervals thereafter.
7.21. Respiratory rate is checked by counting the total number of breaths taken in 1 minute. Inspiration and expiration count as one breath. It is important to count for a full minute to detect any irregularities, and the depth and pattern of breathing can be noted at the same time. Often patients will alter their breathing rate when they know someone is watching it, so it is easier to count the respirations after taking the pulse so the patient is not aware of what you are doing. This is one of the observations that students often find difficult to measure accurately.
7.22. A normal adult respiratory rate is 12–20 breaths per minute.
7.24. A raised respiratory rate could be the result of respiratory distress, chest infection, heart failure, sepsis, deterioration in metabolic or cardiovascular function, trauma, embolus or haemorrhage, anaemia, obstruction of the airway, chronic respiratory health problems, bronchospasm (wheeze), injury, fluid overload or cardiac failure. A low respiratory rate could be the result of respiratory depression, drugs (e.g. morphine can cause respiratory depression), central nervous system damage.
Pulse oximetry
7.26. It is a non-invasive way of measuring the level of oxygen saturation in arterial blood.
7.27. As oxygen is essential for all bodily functions, a decrease in oxygen level can have serious consequences for the patient. It should be measured on admission and at regular intervals thereafter.
7.28. Oxygen saturation is measured using an electronic device called a pulse oximeter. This transmits light from one side of the probe to the other through the finger (toes and earlobes can also be used). To ensure an accurate reading, you must do the following:
7.30. The normal range for an adult would be 95–100%, BUT this may vary depending on any underlying problems the patient may have.
7.31. A low saturation could be the result of chest infection, chronic lung disease, a decrease in peripheral circulation or deterioration of any bodily function.
Peak expiratory flow rate
7.33. To detect worsening asthma, to help diagnose asthma, to show how a client is responding to treatment.
7.34. Depends on age, height and sex:
Readings should be 20% either side.
Your organisation should have a chart with predictive readings, usually based on or adapted from Nunn and Gregg (1989).