8 Communication within medical placements
• To explore communication within multidisciplinary teams within medical placements
• To explore why communication is so important for the medical patient's wellbeing
• To determine the importance of accurate record keeping
• To identify learning opportunities to develop communication skills within placements
Introduction
Wherever you are in your medical placements and regardless of your field of nursing, you will have learning outcomes that require you to demonstrate competence in communication and interpersonal skills (Nursing and Midwifery Council (NMC) 2010,). Your NMC-approved programme based on the 2010 Standards and Competencies has a generic competence for communication and interpersonal skills alongside the NMC Essential Skills Clusters for ‘care, compassion and communication’ (NMC 2010). The NMC states that ‘all nurses must use excellent communication and interpersonal skills. Their communication must always be safe, effective, compassionate and respectful’ (NMC 2010, p. 15).
Some of you will be achieving competencies with the NMC (2008) Standards, which also have a significant number of competencies related to effective communication skills. As well as engaging with different sets of competencies, your curriculum documentation will be different for each university, but all of your programmes will incorporate the NMC Domains and Essential Skills Clusters. Some of you may have skills-based outcomes, activities and reflections in addition to these, and it is important that you are aware of what you need to achieve in relation to communication and interpersonal skills within your placements. You will need to adapt your communication strategies depending on who you are speaking to and where you are placed.
There are four key areas for you to focus on during your medical placement:
1. The relationship with the patient and their significant others.
2. Professional relationships with colleagues and the multidisciplinary team.
3. What information to give at handover or patient reporting period.

During the theoretical component of your course, you will have been taught about the NMC Code (NMC 2008). Now that you are in your placement, think about how this is put into practice. You could consider the following:
1. Think about why it is important to maintain and regulate professional standards.
2. Are you able to think about examples from practice? How is confidentiality maintained? What records are left by patients’ beds? How are patient records accessed and who can access them?
3. How do you answer the phone and what information are you allowed to give? Observe and listen to how other members of the nursing team deal with telephone queries.
4. Are patients asking you difficult questions? How can you answer them in a professional manner? How do other members of staff answer these questions?
Thinking back to my own practice, I can remember times when I have been providing personal care for a patient and they have asked me what is wrong with the patient in the next bed. I learnt to politely explain that I would never discuss their health problem with another patient as that would be unprofessional and, therefore, I am unable to discuss another patient's diagnosis with them.
When answering the phone it is really important to state the name/number of the ward, who you are and your title and to ask the person at the end of the phone how you can help them.
With regards to record keeping, the NMC (2009) produced very comprehensive guidelines, but it is important to remember that records at the end of a bed could be looked at by anyone visiting and should contain nothing that provides demographic data or diagnosis.
Reflective practice is now part of nursing and many of your learning outcomes will require you to reflect about your practice. There are many models of reflection that you will have been introduced to at your university (Johns 1996, Gibbs 1988). Nursing involves situations that are complex and we need to make sense of these situations in order to build on the relationship between practice and theory. Whatever model or framework you use for reflection, they normally contain the following considerations (Gibbs 1988):
• Description of the experience/event – what happened?
• Feelings – what were you thinking and feeling?
• Evaluation – what was good and bad about the experience?
• Analysis – what sense can you make of the situation?
It is important to keep a reflective journal. This may be an essential part of your professional development portfolio (PDP) recording where not only will you wish to keep a reflective diary/journal, but also those specific to your attainment of goals agreed with a personal tutor or mentor. Many students carry a small notebook with them to enable them to jot down interesting thoughts and actions. The journal can act as a prompt when you are meeting with your mentor, promote deeper learning and also be useful as evidence for future academic assignments.
Speak with your mentor and allocate some time to discuss your reflections on action during your placement.
It may help you to read the following articles about reflection and the student nurse:
O'Donovan M (2007) Implementing reflection: insights from pre-registration mental health students. Nurse Education Today 27(6):610–616
de Sales T, Beddoes L (2007) Using reflective models to enhance learning: experiences of staff and students. Nurse Education in Practice 7(3): 135–140
The relationship between nurse, patient and carers
The therapeutic relationship between nurse, patient, family and next of kin starts from the moment the patient walks through the door – how we greet, non-verbal cues, treating with respect, being polite, not overreacting or taking offence to patient comments which are often made in times of stress. Sometimes it is important to explain to the patient why some things cannot be taken care of immediately and keeping them informed about their condition. This has the overall aim of making patients feel safe and cared for and developing a relationship of trust whereby the nurse acts as the patient's advocate. We live in a diverse society and need to treat every person as an individual and seek to understand their philosophy of health and their spiritual needs while they are in hospital. This therapeutic relationship lays the foundations for future emotional support and possibly dealing with difficult questions. The following tips can help.



Professional relationship with colleagues and the multidisciplinary team
Each medical ward/placement will have its own culture and philosophy of care. You will gain far more from the placement if you seek to integrate and build relationships with the team and immerse yourself in the ward culture. You need to appreciate that your learning needs are important but patient needs will always come first for the staff on the ward, given their accountability for care delivery.
You need to take ownership of your own learning and make positive proactive contributions to the team which, in turn, will help you meet your learning outcomes. This will result in a good working relationship between mentor and student. If you can demonstrate that you are able to actively participate within the ward setting, greater opportunities will arise. Here are some examples of the learning opportunities that you could access:
• Multidisciplinary team forums – care planning meetings.
• Participating in ward rounds – usually a consultant will have set days and times for ward rounds. Ward rounds take place by the patients’ beds and a registered nurse, consultant and a team of doctors with other healthcare professionals discuss with the patient how they are progressing. A clinical assessment and examination are often made by the consultant and actions to be taken are discussed with the patient and documented.
• Making referrals under supervision of your mentor on behalf of patients to clinical nurse specialists, district nurses, discharge coordinators and others.
• Spending time with the clinical nurse specialists who link with the medical placement.
• Liaising with social workers, physiotherapists, occupational therapists, bed managers and site nurse practitioners.
In Chapter 4, patient journeys and examples of learning pathways were explored. This is an ideal opportunity for you to speak with your mentor to ensure that you are accessing all the learning opportunities possible with regard to understanding about the work of other health and social care colleagues.
You will see that you will have some learning outcomes that require you to communicate with other disciplines and to have some understanding of their role. This was one of the actions from several high-profile healthcare investigations in the UK which criticised staff for not being able to communicate effectively, such as the Bristol Royal Infirmary Inquiry (2001), the Climbie case (Department of Health 2003) and the case of Baby P (Laming 2009).
Try to think of your placement as the centre of your learning environment but also speak to your mentor and co-mentor to try to understand the opportunities that you could be accessing. Remember
Ask your mentor if you can attend a multidisciplinary forum such as a multidisciplinary meeting, care planning meeting or goal setting meeting. How did the registered nurse communicate with the team? What roles did people take within the team? What contribution did each discipline make? What was the purpose of the meeting? How were the outcomes of the meeting captured?
that your mentor is not a mind reader and it is up to you to be open about what your learning needs are and, most importantly, those you have to achieve as part of your practice assessment expectations.
The kinds of information you may gain during one of these meetings might be the following:
• A member of the medical team might have spoken about the current health status of a patient.
• The physiotherapist may have discussed the mobility needs of the patient.
• The occupational therapist may have provided information regarding their ability to self-care, the assistance they require and the condition of their home environment.
• The social worker may have discussed the resources available to support the person at home.
• The nurses will have discussed how the patient is managing their activities of daily living on the ward.
• The views and wishes of the patient and their family/significant others will have been provided either by the patient and family themselves, if present, or by any member of the team who has discussed this with them.
• A member of the team will have taken the role of record keeper to ensure that all decisions are documented.
• The outcome of the meeting will usually be plans for discharge, goals that need to be met prior to discharge and referrals to any other members of the team not present.
If you are a first-year student, your medical placement may be your first encounter with patients and you may worry about how to approach them and what to say. It can be difficult for you to determine what it is you are actually supposed to be learning, however, do not worry as this is a normal reaction. Try not to compare yourself to other students who may have a background in health care and appear confident already.
Some pre-registration nursing programmes will give you a skills schedule or booklet with various nursing competencies for you to achieve. Examples of competencies could be: ‘the student introduces himself/herself to patients’ or ‘the student introduces himself/herself to patients, staff and others in a professional manner’ which you will automatically do when you meet a patient or take over their care from someone else. You may be asked to undertake a patient's vital signs, and before you do that you will introduce yourself and explain what you would like to do and gain their agreement. This simple interaction is very important and will demonstrate that you are communicating with your patient. It also indicates that you understand about gaining a patient's consent (informed consent).
This article may help you understand what is meant by informed consent:
Chaloner C (2007). An introduction to ethics in nursing. Nursing Standard 21(32):42–46. Online. Available at: http://nursingstandard.rcnpublishing.co.uk/archive/article-an-introduction-to-ethics-in-nursing (accessed July 2011).
Observe your mentor when she/he communicates with patients. How does your mentor promote a professional yet caring image to the patient?
We live in a very diverse world where English may not be a patient's first language and within your daily communication with patients and staff you will be required to demonstrate that you are able to respect diversity and respond to differences while maintaining a person-centred approach.
You may also come across patients who live a very different life from you and you may never have come across some of the relationships or lifestyles that your patient has. Medical patients will often be admitted to the ward with a diverse range of conditions, which will affect them physically and psychosocially. Patients will come from a diverse cultural background and have different beliefs about health and living. You may find that your personal and professional values and beliefs are challenged and you may find that providing non-judgemental care is more difficult in some circumstances. It is important for you to think about the values and prejudices that you have and reflect on how this impacts on your nursing care and your ability to provide non-judgemental care.
Discuss with your mentor how you could adapt your communication skills if you were caring for a patient who did not speak very much English.
You may find this a useful book to read:
Holland K, Christine Hogg (2010). Cultural awareness in nursing and healthcare, 2nd ed. Edward Arnold, London.
Chapter 5 of this book examines culture care: knowledge and skills for implementation in practice.
An RCN publication that may also be of interest is:
This Website provides Department of Health guidance for the NHS:
Department of Health (2009) Religion or belief: a practical guide for the NHS: http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_093132.pdf (accessed July 2011).
The nursing handover
It is important for you to identify and inform your mentor about what you need to know, and sometimes to remind them of what you already know and the level you are at in your training. Medical wards can be unpredictable and fast paced with patients with a variety of health problems, and you may be overwhelmed with information and have difficulty identifying and extracting relevant information that needs to be passed on to other colleagues. You need to ensure that you communicate with the trained staff throughout the shift (see Ch. 1). The registered nurse may appear busy but is still there to support and supervise you. It is important that you recognise the resources available to you on the ward, for example other students, assistant practitioners, healthcare assistants, nurse consultants, clinical nurse specialists and therapists.
Sometimes it is difficult to know what you should be letting staff know about, but this comes with experience. You will learn to undertake risk assessments, for example risk assessments that will tell you if someone is at risk of malnutrition, falls or pressure ulcers (see Ch. 6). You will learn to inform the registered nurse and other healthcare professionals during your shift and in handover. You will begin to understand the normal values for observations for vital signs and to inform someone when they are abnormal or have returned to normal. You will learn to identify when a patient's condition changes and how soon you need to inform someone.
Much of the information is now found electronically and you will need to ask your mentor for your own log-on code to ensure that you adhere to the Data Protection Act (1998).
Between shifts, staff will have a handover period. This is done differently in different organisations and there is usually a policy to support this process. In the majority of your placements, the following will be communicated (handed over) away from the patient area to maintain confidentiality (see Table 8.1):
| Office handover | Bedside |
|---|---|
| Name Age Allergies Consultant Diagnosis Planned treatment Investigations carried out/scheduled Resuscitation status |
Allocated nurses for group of patients will receive handover from the nurses on the previous shift The patient should be included in the handover The allocated nurses must introduce themselves to the patient if they have not met that patient before Handover must include: |
Generally nurses are then allocated to a group of patients who are under the care of a team of nurses led by a team leader/named nurse. They then move to the bedside to handover more specific aspects of care using the documentation at the end of the bed or the electronic patient records. This handover usually includes patients’ reactions as well. For example, a nurse may say to a patient: ‘Did you have your chest X-ray?’ or ‘Did the physiotherapist see you this morning? How did it go?’
The shift handover period is an ideal arena for you to develop your skills and confidence when communicating about the care that has been delivered to the patients in your care while providing an opportunity for clarification of issues you may not fully understand and teaching by others. As a senior student, you are expected to contribute to handover. As a less experienced student, you should be encouraged to do this. You can make notes during handover but there should never be anything in your notes that would identify who a patient is – notes should be shredded/destroyed after your shift (NMC 2008). Many nurses carry a small pocket-sized note book.
Nursing handover can be difficult for the less experienced students to understand. Make sure that you question anything you do not understand, although maybe that would have to wait until the end of the handover itself. Take a note of various patient diagnoses reported. Some of the conditions you will come across are listed in Box 8.1.
On your medical placement, think about any handover you received from the registered nurses regarding your allocated patients. Think about what you would say if you were handing over information about the patients that you cared for that day. Ask your mentor if you can practise handing over your patients to them. Get them to ask questions about the care, why it was delivered and what evidence underpins that care. Reading about the way in which patients with certain health problems may experience the signs and symptoms of their illness and the medications they might be taking will help you with care delivery and also ensure that you are giving safe and effective care to a group of people who are in a vulnerable situation.
It will be helpful for you to look after one to three patients in an early-stage placement and try to provide person-centred care under direct supervision for these patients. This is one of the competencies expected of you at progression point 1 (NMC 2010).
As a third-year student, you should start to look after a caseload of patients and you should be contributing to multidisciplinary forums rather than just observing. You should be handing over your caseload of patients verbally and in writing under the supervision of a registered nurse. At progression point 3, you are expected to ‘inspire confidence and provide clear direction to others … manage time effectively … negotiating with others in relation to balancing competing and conflicting priorities.’
It allows me to care for a wide range of acutely ill patients with a whole variety of conditions; enables me to develop myself as a nurse who is able to work under pressure and in demanding situations, and also gives me the opportunity to work alongside various other healthcare professionals, e.g. physiotherapists, social workers, clinical nurse specialists.
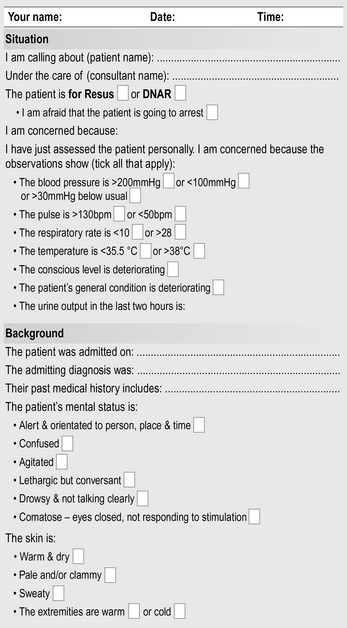
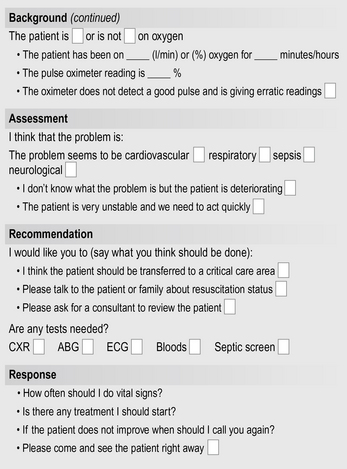
Situation, background, assessment, recommendation and response
The NHS is often criticised for poor communication, however there are few tools that actively focus on how to improve communication, in particular verbal communication. Effective handover between shifts is vital to protect patient safety and assist with delivering high standards of care. The transfer of a patient's care to another person/team is the point at which the patient is most vulnerable on their journey through the hospital. Gaps in communication can lead to breakdowns in continuity of care, inappropriate treatment and potential harm to the patient.
Originally used in the military and aviation industries, ‘situation, background, assessment, recommendation and response’ (SBARR) was developed for health care by Dr M Leonard and colleagues (2004) from Kaiser Permanente in Colorado, USA. In one healthcare setting, the incidence of harm to patients fell by 50% after implementing SBARR. SBARR is an easy to remember mechanism that can be used to frame conversations, especially critical ones. It enables you to clarify what information should be communicated between members of the team and how. It can also help develop teamwork and foster a culture of patient safety. The tool can be used to shape communication at any stage of the patients’ journey.
The tool consists of standardised prompt questions within four sections, to ensure that staff are sharing concise and focused information. It allows staff to communicate assertively and effectively:
• Situation: state what is happening at the present time.
• Background: explain the circumstances leading up to the situation.
• Assessment: state pertinent assessment findings.
• Recommendation: state what needs to be done and in what time frame.

You are looking after Mrs Hamer, a 64-year-old, who you have been caring for on medical day care. She returned to the unit a couple of hours ago having had a colonoscopy. You respond to a call from another patient and when you go back to Mrs Hamer you find her on the floor. She is alert and says she has fallen but has terrible pain in her hip. You call the registered nurse who instructs you not to move Mrs Hamer but to carry out a full assessment and then use the SBARR tool to inform the doctor.
Use the SBARR tool in Figure 8.1 to collate the information that you would need to inform the doctor of the situation.
The above situation would require documentation in the nursing notes and completion of an incident form. Record keeping is another way in which nurses are required to communicate.
Consider why and where we document (refer to Boxes 8.2 and 8.3).
Record keeping
The NMC (2009) outlines what is expected of nurses and midwives in relation to record keeping which is seen as an integral part of nursing and midwifery practice. It is no surprise then that record keeping is part of the NMC Domain, Communication and Interpersonal Skills, and is included within the NMC Essential Skill Clusters (2010). By the end of your first year, there is an expectation that you ‘communicate effectively both orally and in writing so that the meaning is always clear’ and, for entry to the register, you will be expected to provide ‘accurate and comprehensive written and verbal reports based on best available evidence’ (NMC 2010, p. 8). See Table 8.2 for examples of using appropriate language.
I ensured everything I do helped me to adhere to the Nursing and Midwifery Council code of conduct and to the trust policies. The NMC states that every care we give to patients should be documented and that before giving care consent should be sought.
(Patricia Moyo, third-year student nurse)
Table 8.2 Using objective language instead of subjective language
| Subjective | Objective |
|---|---|
| Diet taken fair | Half of diet consumed |
| Appears restless | Thrashing about in bed |
| IV running well | Dextrose 5% infusing at 125 mL per hour Site clear |
| Usual night | Requested pain medication for headache |
| Medication × 1 for pain | Oral analgesia given at 00:30 |
| Catheter minimal drainage | Catheter drained 200 mL in 6 hours |
| Sacrum red | Grade 2 pressure ulcer on sacrum measured and wound care plan implemented |
| Fair morning or no complaints | Patient has rested on bed all morning and says she feels a bit better today |
| Good night | Patient says she slept quite well last night |
| All due care given | There is no objective statement for all due care given, you must document the care you have given according to the patient's care plan |
Read the NMC (2009) Record Keeping: Guidance for Nurses and Midwives and find out how this is applied by registered nurses within your medical placement. Are there any local policies that support this NMC guidance?
Rules of good documentation
– be written in black ink, clearly, in a manner that cannot be erased
– be accurate, factual and consecutive
– be written as soon after the event has occurred as possible
– be written with patient and/or carer involvement
– be timed, signed, dated and have name printed alongside and countersigned by a registered nurse
– have any alterations crossed through with a single line, signed and dated.
Legal requirements
Patients’ records may be used as evidence in a court of law to answer a complaint or negligence claim. There are a number of policies which set out patients’ rights in accessing their healthcare records:
• Health records are defined as ‘information about the physical or mental health or condition of an identifiable individual made by or on behalf of a health professional in connection with the care of the individual’ (NMC 2009).
• Data Protection Act 1998: regulates the storage and protection of patient information. Data can only be used for the specific purpose for which it was collected. Data cannot be disclosed without patient consent. Individuals have the right of access to information held about them (subject to exemption, i.e. crime).
Data Protection Act 1998 – eight principles
1. Fairly and lawfully processed.
2. Processed for limited purposes.
3. Adequate, relevant and not excessive.
5. Not kept for longer than necessary.
6. Processed in line with rights.
8. Not transferred to other countries without adequate protection.
Consider this: you are on placement and you do not have a computer log-on code for the electronic records. You have just undertaken the vital signs for six patients and they need to be put into the computer. The registered nurse says that you can use his/her user name and password to access the information. What would your answer be?
You would have to say no and explain that you would be happy to do this if you were given your own log-on code. To input data using someone else's log-on code contravenes the Data Protection Act because the information would indicate that the registered nurse had documented these data and not you.
Freedom of Information Act 2000
This Act grants a general right of access to all types of information held by public health authorities that is not covered by the Data Protection Act. Certain information that is deemed sensitive can be withheld with a reason given.
Patients are allowed to see their medical notes and organisations will have policies in place to support this. Patients will be required to book an appointment with a consultant through his/her secretary to ensure that they have someone there who can answer any queries while they are reading their notes.
Accurate and timely record keeping is an integral part of nursing and nursing notes must be clear and complete. The patients that you are looking after will all have a plan of care and, as a student, you will be contributing to this care plan under the supervision of a registered nurse. Documentation varies depending on where you are placed and it is important that you are familiar with this.
Care planning
• What is written in the nursing notes must relate to the patient's care plan.
• If care plans are numbered, the corresponding number can be used in the nursing notes to evaluate that problem.
• Once something is no longer a problem, discontinue the care plan – you will have less to write.
Now practise writing a care plan for one of the patients you have looked after and show it to your mentor. An example of a care plan can be found in Holland et al (2008). You can use this to practise using a framework for the assessment and planning of care process.
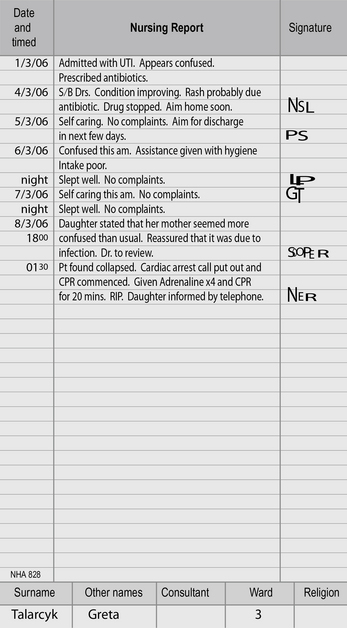
Look at the example of nursing notes in Figure 8.2. Would you consider this to be good record keeping?
Complete the wordsearch to evaluate what you have learnt.
(Answers on page 152.)
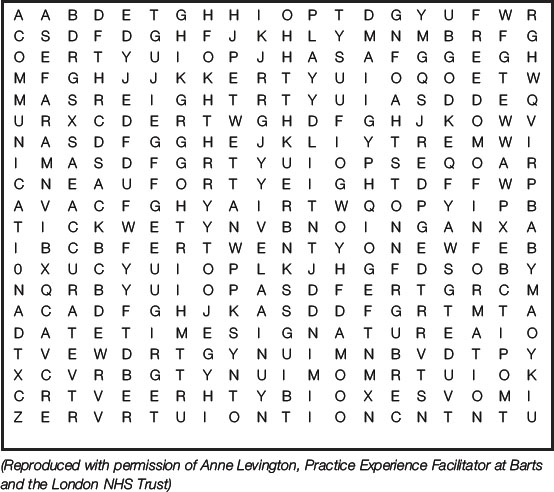
8.1. How many years does the NHS need to keep adult records? [5]
8.2. How many years does the NHS need to keep child records? [9]
8.3. What ‘C’ assists in the dissemination of information? [13]
8.4. What ‘A’ ensures that documentation is precise and concise? [8]
8.5. What is the ‘D’, ‘T’ and ‘S’ that must be documented on all patient records? [4, 4, 9]
8.6. What is the parliamentary Act the grants patients the right to request to view their records? [7, 2, 11]
8.7. Within how many hours must a patient's record be written? [10]
Summary
This chapter has explored communication within multidisciplinary teams in medical placements and why it is important for medical patients’ wellbeing. The importance of accurate record keeping has been outlined and how it is integral to the role of the nurse. Learning opportunities have been identified to help you to develop your communication skills within your placements.
Department of Health. Lord Laming: the Victoria Climbie inquiry. London: Department of Health; 2003.
Gibbs G. Learning by doing: a guide to teaching and learning methods. Oxford: Further Education Unit, Oxford Polytechnic; 1988.
Holland K., Jenkins J., Solomon J., et al. Applying the Roper–Logan–Tierney model in practice, 2nd ed. Edinburgh: Churchill Livingstone; 2008.
Johns. Using the reflective model of nursing and guided reflection. Nursing Standard. 1996;11(2):34–38.
Laming, The Lord. The protection of children in England: a progress report [Online. Available at:] The Stationary Office, London, 2009. http://news.bbc.co.uk/1/shared/bsp/hi/pdfs/12_03_09_children.pdf. (accessed July 2011)
Leonard M., Graham S., Bonacum D. The human factor: the critical importance of effective teamwork and communication in providing safe care. Quality and Safety in Healthcare. 2004;13:i85–i90.
Nursing and Midwifery Council. The code: standards of conduct, performance and ethics for nurses and midwives. London: NMC; 2008.
Nursing and Midwifery Council. Record keeping: guidance for nurses and midwives. London: NMC; 2009.
Nursing and Midwifery Council. Standards for pre-registration nursing education. London: NMC; 2010.
The Bristol Royal Infirmary Inquiry. The inquiry into the management of care of children receiving complex heart surgery at the Bristol Royal Infirmary [Online. Available at: 2001. http://www.bristol-inquiry.org.uk/. (accessed July 2011)
Arnold E.C., Boggs K.U. Interpersonal relationships: professional communication skills for nurses, 5th ed. Edinburgh: Saunders; 2007.
Burnard P., Gill P. Culture, communication, and nursing. Harlow: Pearson Education; 2008.
Caldwell P., Horwood J. From isolation to intimacy: making friends without words. London: J Kingsley; 2007.
Dunn K. Effective communication in palliative care. Nursing Standard. 2005;20(13):57–64.
Edwards K. What prevents one to care. Nursing Times. 2011;107:25–27.
Godsell M., Scarborough K. Improving communication for people with learning disibilities. Nursing Standard. 2006;20(30):58–65.
Griffith R. Putting the record straight: the importance of documentation. British journal of Community Nursing. 2004;9(3):122–125.
Kraszewski S., McEwen A. Communication skills for adult nurses. Maidenhead: Open University Press; 2010.
Mccabe C., Timmins F. Communication skills for nursing practice. Basingstoke: Palgrave Macmillan; 2006.
Moloney R., Maggs C. A systematic review of the relationship between written manual nursing care planning, record keeping and patient outcomes. Journal of Advanced Nursing. 1999;30(1):51–57.
O'Leary K., Thompson J., Landler M. Patterns of nurse–physician communication and agreement on the plan of care. Quality and Safety in Health Care. 2010;1(3):195–199.
Taylor H. An exploration of the factors that affect nurses’ record keeping. British Journal of Nursing. 2003;12(12):751–758.
Turner D., Beddoes L. Using reflective models to enhance learning: experiences of staff and students. Nurse Education in Practice. 2007;7(3):135–140.
Whittington K., Hodgson L. The complexities of caring for a patient with an ICD in end-stage heart failure. Cardiac Nursing. 2010;5(12):568–575.