Chapter 5 Applying the biopsychosocial model to the management of rheumatic disease
KEY POINTS
INTRODUCTION
Living with a chronic condition, such as rheumatoid arthritis (RA), impacts all functional domains. Health professionals help patients develop coping skills to minimise the condition’s effects on physical and psychological wellbeing. To do this effectively health professionals must understand why and how people adopt or reject certain health behaviours. By utilising the biopsychosocial model of care, illness impact on physical, psychological and social aspects of function is addressed and a wider range of therapeutic options offered that have meaning and relevance to the individual.
This chapter is divided into four sections addressing: the biopsychosocial model; the impact of arthritis; pain; and social cognition models that help explain health behaviour.
SECTION 1: THE BIOPSYCHOSOCIAL MODEL AND ITS IMPORTANCE IN ARTHRITIS MANAGEMENT
Recognition that understanding patient’s beliefs, feelings, thoughts and health behaviour is necessary to aid our understanding of the patient’s condition has led to a move from a disease model to a biopsychosocial model of care, which acknowledges the importance of psychological and social factors as well as the physical impact of living with arthritis. For example, physical impact can include symptoms of pain, stiffness and fatigue. Psychological effects may include feelings of frustration, low mood and give rise to concerns about the future, whilst social implications can include concerns about work, role within the family and continuing to engage in valued leisure activities.
Adopting a biopsychosocial approach to care has increased the range of therapeutic options for patients. Cognitive behavioural therapy (CBT), which aims to identify and change maladaptive patterns of thought and behaviour, is of benefit in patients with RA. In newly diagnosed RA patients, CBT improves a patient’s sense of control regarding their condition and prevents development of negative illness perceptions (Sharpe et al 2003). CBT is also useful for patients with depression (Parker et al 2003).
Other psychological interventions involve improving confidence in carrying out specific behaviours, i.e. self efficacy, which will be discussed in Section 4. If a person believes they can play an active role in managing some of the impact of their condition, through employing strategies such as pacing, goal setting and exercise, they are more likely to do so than a patient with little or no such confidence. Active self-management is associated with higher levels of adherence. Even if the intended goal is not achieved, the process of striving for it leads to better outcomes (Jerant 2005).
Involving significant others in care management can also have a positive effect on outcomes. If the family is unaware why an individual is encouraged to pace their activities, this may be perceived as ‘laziness’ and lead to family conflict. Spouses of patients attending an education programme to increase their knowledge of RA experienced a change in their perceptions towards the condition, which were largely negative before the programme (Phelan et al 1994). The importance of the family on outcome was illustrated in a study of the benefits of behavioural interventions to minimise pain in patients with RA. Intervention incorporating family support was more effective in reducing pain than the intervention with the family alone (Radojenic et al 1992). Adopting a biopsychosocial model of care ensures all factors influencing a patient’s ability to manage and cope with their condition can be identified and, where possible, addressed.
SECTION 2: THE IMPACT OF RHEUMATOLOGICAL CONDITIONS
Patients are individuals with a life history, beliefs, standards and expectations (Bendor 1999). RA cannot be considered solely in terms of its physical consequences. The potential psychological, social and economic impact must be considered.
WORK
Work disability can occur early in arthritis (Fex et al 1998). People with a musculoskeletal condition are more likely to stop working if they:
Cox (2004), focusing on the needs of newly diagnosed RA patients, found that being able to continue working was a major concern: ‘The only question I could think of, is the question I really want answering - am I going to get back to work full-time?’. A National Rheumatoid Arthritis Society (2003) survey showed 54% of participants attributed not being in full-time work to RA and 30% of employed participants worked part-time because of RA. Mancuso et al (2000) found those seemingly successfully employed still faced major challenges, made major adaptations in order to stay at work and still perceived their jobs to be in jeopardy. Early intervention through liaison with employers, consideration of alternative ways of working, work place assessment and if necessary retraining is important to keep patients at work (see Ch. 9: Occupational therapy). Vocational issues that may need considering are shown in Box 5.1.
LEISURE
Engaging in a specific leisure activity will be influenced by the individual’s level of motivation, and the belief participation can be done to a reasonable standard. The physical and psychological impact of arthritis, such as pain, reduced muscle strength, fatigue and reduced self esteem, may hinder both the desire and ability to partake in leisure. Many difficulties are faced participating in leisure (Fex et al 1998, Hakkinen et al 2003, Wikstrom et al 2005). Inaccessible facilities, lack of transport, absence of support or negative attitudes from others may all impact negatively on leisure (Specht et al 2002).
MOOD
Depression in RA is 2–3 times higher than in the general population (Dickens & Creed 2001). Data from baseline co-morbidity levels in over 7,000 patients starting biologic treatments found 19% had a formal diagnosis of depression at any one time (Hyrich et al 2006).
Depression in RA is linked to:
(Dickens & Creed 2001, Lowe et al 2004, Sheehy et al. 2006).
If depression is suspected it must be assessed and treated. It is not acceptable to acknowledge it is associated with RA and not treat it. In Stoke-on-Trent in the UK, a combined liaison psychiatry clinic run by a liaison psychiatrist and a rheumatology nurse consultant assesses for mental health problems and advises on appropriate treatment. For depression this involves anti-depressants and/or CBT.
SOCIAL SUPPORT
Interpersonal relationships contribute to physical, psychological and social state wellbeing. Through our social support systems we validate beliefs, emotions, action and seek information and advice. Core activities carried out within social networks include:
Ryan et al (2003) demonstrated that patients wanted to remain active in both domains. Aspects of social support enhancing control perceptions include:
Many inflammatory conditions are characterised by unpredictability regarding symptom occurrence, treatment efficacy and overall prognosis. Different levels of support will be required from health professionals related to patients’ identified needs (Box 5.2).
SEXUALITY AND BODY IMAGE
Sexuality is an individual self-concept expressed as feelings, attitude, beliefs and behaviour (RCN 2000). RA features which impact negatively on sexuality and body image include joint pain and stiffness, fatigue, low mood, physical changes and treatment visibility, including splints (Hill et al 2003). Patients indicate they would like the opportunity to discuss sexuality concerns with healthcare professionals (Hill et al 2003) but due to a lack of privacy, time, knowledge and skills, this often does not occur. Many types of arthritis extensively affect people’s lives. Living with chronic pain considerably contributes to this.
SECTION 3: PAIN
Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage (International Association for the Study of Pain (IASP) 1994). It is a common symptom across rheumatic conditions. It is a unique, subjective and unverifiable person experience (Turk & Melzack 1992). Acute pain is often transient and the source of pain is identifiable and treatable, e.g. active synovitis of the knee. Chronic pain is an ongoing experience associated with a plethora of other symptoms including anxiety, depression and sleep disturbance.
Patients with RA cite pain as their most important symptom (Minnock et al, 2003). Pain is associated with impaired quality of life, depression and disability in both RA and OA (Spranglers et al 2000). Chronic pain in fibromyalgia results in reduced physical activities, increased mood symptoms, withdrawal from the workplace and increased use of health care services (Hughes et al 2006). When helping patients manage their pain, a biopsychosocial model aids fully comprehending the pain experience and enables planning care that is meaningful for the patient.
PAIN MECHANISMS
The ‘specificity theory’ attributed to Descartes in 1664 reflects early understanding of pain mechanisms. In this model, skin pain receptors are activated by a painful stimulus and messages conveyed to the brain enabling action to be taken, e.g. removing the hand from a fire. Pain is purely a physical phenomenon with a direct relationship between the amount of stimulation (damage) to nociceptors and pain experienced. But this does not explain the variation in pain experience for a given stimulus or injury. Why do some patients take longer to recover from whiplash than others? Why does pain persist beyond the time of tissue healing?
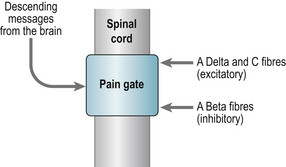
Melzack and Wall’s gate control theory of pain (1965) revolutionised understanding of pain mechanisms (Fig. 5.1). This demonstrated that the transmission of pain messages could be modulated within the spinal cord via descending messages from the brain (our cognitions and emotions) or altered by activating another source of sensory receptor (e.g. exercise to release endorphins).
PAIN RECEPTORS
Sensory receptors are situated in the tissues of the skin, synovium of joints and arterial walls. These are activated by various stimuli including:
Peripheral sensory nerves transmit signals from the peripheries to the central nervous system enabling stimulus identification. Alpha delta fibres (thin and myelinated) transmit the sharp pain of an acute injury and slower C-fibres (unmyelinated) produce the dull aching pain of a more persistent problem or the burning quality of neuropathic pain (McCabe 2004).
Sensory nerves deliver information from the peripheries to the dorsal horn where they terminate. This information is then interpreted by transmission cells (T-cells) transmitting information to the local reflex circuits and the brain. When the Alpha delta and C fibres are stimulated T cells are activated resulting in the substantia gelatinosa (SG) being suppressed so that the ‘pain gate’ opens and messages pass to the brain to be perceived as pain. When large fibres become activated (Alpha beta) they suppress T cell activity and close the gate. Alpha beta fibres transmit the sensation of touch. Acupuncture and electrical nerve stimulation work on the same principle and excite large fibre activity. Nerve impulses descending from the brain can also operate ‘the gate’.
CASE STUDY 5.1 POSSIBLE PAIN PATHWAYS IN A CASE STUDY OF A PATIENT WITH RA (BASED ON AN EXAMPLE BY MCCABE 2004)
Mrs Jones is a 44-year-old women diagnosed with RA 5 years ago. She works as a legal assistant in a busy law firm. She has had to take time off which is worrying her. Mrs Jones is married with no children. Over the last 3 months she has experienced more early morning stiffness (from 30 minutes to 2 hours) and has pain and inflammation in both wrists and her right knee. Mrs Jones describes her pain as ‘burning and tender to touch’. The pain disturbs her sleep and she has difficulty with mobility.
Peripheral mechanisms
The inflammatory process (demonstrated by swelling, pain and stiffness) has generated peripheral sensitization. Reporting burning pain indicates activation of the C fibres or changes in the dorsal horn resulting in central sensitization. Problems with mobility may be due to changes in knee intra-articular pressure.
Central mechanisms
Generalised tenderness indicates a lowering of the Alpha beta fibre threshold and may have been induced by the duration of symptoms. Changes in proprioception due to knee swelling may create a mismatch in the motor and sensory systems. This mechanism has been proposed as an explanation for the perception of stiffness in RA (Haigh et al 2003). Other factors that may influence Mrs Jones’ pain are her lack of sleep and work concerns.
PERIPHERAL AND CENTRAL SENSITIZATION
The gate theory of pain is portrayed as a hard-wired system but we know this is not the case (McCabe 2004). If persistent stimulation occurs the Alpha delta and C fibres will be activated by weak non-noxious stimuli (Devor & Seltzer 1999). This sensitization occurs in the peripheries due to tissue damage or release of chemical inflammatory mediators (e.g. substance P) into the skin from damaged C fibres and the increase in the activity of calcium channels within the spinal cord. The presence of allodynia (pain from a non noxious stimuli) and hyperalgesia (increased response to a painful stimulus) can occur due to a lowering in the Alpha beta threshold so that pain now becomes a painful stimulus (McCabe 2004).
Pain is affected by many physical, psychological and social factors. Effective pain control using a variety of approaches is thus essential in biopsychosocial management of arthritis. These approaches are discussed in subsequent chapters.
SECTION 4: HEALTH BEHAVIOUR, COPING AND CONCORDANCE
Health behaviour refers to the ways in which people with arthritis perceive, understand and manage their condition. Understanding factors affecting health behaviours, coping and concordance helps maximise effective biopsychosocial management. Influences on health behaviours include:
There are several psychological models, known as social cognition models, developed to predict and explain health behaviour. The most commonly used are:
THE HEALTH BELIEF MODEL
This model is based on two aspects of health behaviour (Fig. 5.2):
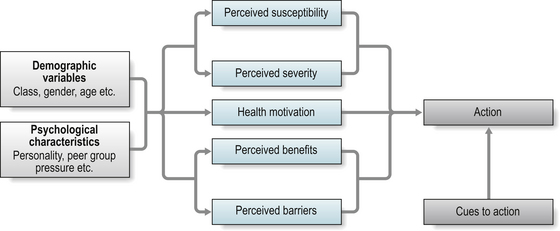
Cues to action can trigger performance of health behaviours if the underlying beliefs about threat perception and behavioural evaluation are favourable (Becker et al 1977).
Take, for example, a patient whose RA is affecting ability to work. They believe that without some form of drug treatment they will become progressively disabled (high threat). They know there are several treatment options. Despite concerns about medications (costs) they believe some are very effective (benefits). Media reports of a new wonder treatment for RA may prompt them to seek treatment (cues to action).
The HBM has been used as a basis for the Beliefs about Medicine Questionnaire (Horne et al 1999). This focuses on the perceived threat of illness and medication and the consequences of taking or not taking medication. It has been used to explain/predict adherence to medication. For example, if arthritis pain is perceived as severe and medication is perceived as effective and relatively safe, patients are more likely to take it to manage their pain (Horne, Mitchell, Weinman, 2001 personal communication).
HEALTH LOCUS OF CONTROL
The Health Locus of Control model is based on Rotter’s Social Learning Theory (Rotter 1954). It proposes that health behaviours are predicted by the extent to which an individual believes they can perform the behaviour and that it will be effective. Individuals with an internal locus of control (LOC) are more likely to take action to manage their symptoms than an individual with more external LOC who believes their symptoms are a result of chance and looks to other sources, such as the doctor, to manage their symptoms. However, this model has been tested in a wide range of therapeutic areas with conflicting results.
The most widely used measure is the Multiple Health Locus of Control (MHLC) Scale (Wallston et al 1978), evaluating beliefs about health behaviours in general, and the variance in results might relate to individuals holding different beliefs depending on the situation. For example, an individual might have a high internal LOC for weight loss (i.e. they believe they are responsible and have the ability to reduce their weight) but a high external LOC for managing their arthritis, believing this is the doctor’s responsibility. Ryan et al (2003) found that within a medical consultation, contrary to the HLC model, an external LOC increased the patient’s perceived control over their ability to live with their arthritis. This may be because patients view their condition as too unpredictable and mutifacted to manage without external professional support and view the consultation as a partnership where their issues could be voiced and management appropriate to their needs provided.
In an attempt to make the HLC a stronger predictor of health behaviour it has been adapted to include: the value the individual places on their health and the extent to which an individual is confident in carrying out behaviours they believe will be effective. In other words, for an individual to engage in health behaviour, such as exercise, they need to value their health, believe they are responsible for it, be confident they can exercise and believe exercise will be effective.
SOCIAL COGNITIVE THEORY
In this model health behaviour is seen as the result of three sets of beliefs:
Self-efficacy (SE) has a direct effect on behaviour: an individual’s beliefs that he/she can perform a behaviour predict performance of it. It can also influence intention to perform a behaviour. Studies have demonstrated individuals intend to perform behaviours they are confident they can achieve (Bandura 1992, Schwarzer 1992).
Self-efficacy has been widely applied in arthritis to:
Questionnaire measures of self-efficacy include the
THEORY OF PLANNED BEHAVIOUR
The Theory of Planned Behaviour (TPB) is an extension of the Theory of Reasoned Action (TRA) (Fishbein & Ajzen 1975, Ajzen & Fishbein 1980). Both models are based on the premise that individuals make logical, reasoned decisions to engage in specific behaviours by evaluating the information available to them. The performance of a behaviour is determined by the individual’s intention to engage in it (influenced by the value the individual places on the behaviour, the ease with which it can be performed and the views of significant others) and the perception that the behaviour is within his/her control. In RA a TPB model based on attitudes, social support, self efficacy and intention was moderately successful in predicting and explaining self management of arthritis (Strating et al 2006). Whilst no validated questionnaires are available, a comprehensive guide to developing measures of TPB components is given in Ajzen (1991). A challenge in TPB measurement is the difficulty in conceptualising and capturing attitudes.
THE SELF-REGULATORY MODEL AND ILLNESS BELIEFS
The Self-Regulatory model (SRM) (Leventhal et al 1997) describes how biological, psychological and social factors interact to influence how individuals perceive their symptoms and illness and the health behaviours they subsequently adopt (Fig. 5.3). These perceptions, or illness representations, are a set of beliefs, emotions and disease experiences which individuals use to evaluate information about their disease and to regulate their subsequent behaviour. The SRM differs from the other social cognition models in placing equal importance on the emotional reaction to health threats.
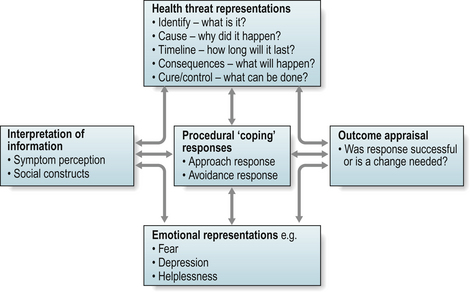
Studies of people’s illness representations have identified five categories of illness beliefs:
The illness perceptions questionnaire (IPQ) (Weinman et al 1996) was originally developed to quantify these. It has been used to understand patients’ responses to illness and predict or explain treatment adherence. It has since been revised to improve its psychometric properties (Moss-Morris et al 2002) and consists of eight categories:
In addition to use in research, it could be used in practice to identify misperceptions of treatment/illness or lack of understanding affecting adherence to treatment/lifestyle advice that might be addressed through educational interventions.
COMMONALITIES BETWEEN THE SOCIAL COGNITION MODELS (SCMs)
Whilst there are many similarities between these, the main differences are the underlying psychological theory. There are specific patient-completed questionnaires available to capture each construct and they can be, and often are, used in combination. However, this is not always helpful. For example, in a study of patients with either OA or RA self-efficacy, but not locus of control, was associated with health status in patients with RA, whilst in patients with OA, locus of control was a better predictor of health status (Cross et al 2006). It is unclear how findings can be meaningfully interpreted in a clinical setting. Moreover, interventions aimed at changing behaviour (such as promoting exercise, increasing medication adherence) may draw on several SCMs. The most commonly applied theories are Social Cognitive Theory and the Health Belief Model, with increasing interest in the Self-Regulatory Model.
HEALTH BEHAVIOURS (COPING, CONCORDANCE, HEALTH BELIEFS)
Coping
Coping is the ability to generate and maintain psychological well-being despite living with a serious condition (Folkman 1997) and is linked to better psychological adjustment outcomes (Smith et al 1997). People with arthritis live with the physical, social and economic consequences of the disease over long periods and may have to cope with uncertainty about long term outcome as well as unpredictability of recurrent fluctuations in disease activity. How people with RA cope has been shown to influence current and long-term psychological and physical adjustment (Burckhardt et al 1997, Smith & Wallston 1992, Smith et al 1997, Zautra & Manne 1992).
Coping behaviours have been extensively studied in chronic disease and are typically classified as active (good) coping strategies, such as information-seeking and self management, and passive (bad) coping strategies, such as catastrophising and wishful thinking. In arthritis studies, effective coping has been equated with perceived control over arthritis and its impact on daily life (Felton & Revenson 1984) and with self efficacy for pain and other arthritis symptoms (Keefe et al 1997, Lefebvre et al 1999). Coping behaviours are influenced by the individual’s appraisal of the threat and the coping options available. Whilst it is assumed that active coping behaviours are more effective in helping patients adapt to and manage their condition, there is more evidence to support ineffectiveness of passive coping.
Questionnaires which identify coping strategies:
Concordance
Concordance describes a partnership between the health professional and patient in which both work together to agree optimal treatment based on a balance of treatment risks and benefits and compatibility with the patient’s goals and preferences. Concordance is increasingly used instead of ‘compliance’ which is viewed as excluding patients from being equal partners in treatment decisions. It is unclear how frequently concordance occurs in clinical practice. It is limited by many factors including:
Treatment decisions based on concordance may increase effective use of treatment.
Between 30–70% of patients take their medication according to the prescribed regimen (Conrad 1985, Donovan & Blake 1992, Hill et al 2001, Viller et al 1999). Figures are similar for non-pharmacological interventions such as exercise (O’Reilly et al 1999). Factors influencing how patients use treatments are complex and often independent of age, gender or disease severity (Kraag et al 1994, Rejeski et al 1997). They include:
Patient health beliefs about disease and treatment
Many patients with RA and OA do not initially interpret their symptoms as evidence of disease but instead attribute them to stress, or more commonly, normalise them in terms of their age and activities (Goodwin et al 1999, Hampson 1994, Sakalys 1997). Even where patients interpret their symptoms as evidence of underlying disease, their family, friends and even health professionals may not. In a study of newly referred patients with RA, more than 50% reported that family, friends or doctors had normalised, minimised or disbelieved their symptoms (Sakalys 1997).
RA patients’ beliefs have been associated with medication use (Neame & Hammond 2005). In general, patients perform cost–benefit analyses on their prescribed medication (Donovan 1991) and are more likely to take this when their perception of the necessity for medication (effectiveness and the perceived consequences of untreated illness) outweighs concerns about it (side-effects, addiction and development of tolerance) (Horne & Weinman 1999, Neame & Hammond 2005). Sixty percent of patients with RA report fear of side-effects is a major factor influencing their decisions to alter dose or frequency (Donovan & Blake 1992). Patients often allow themselves a ‘trial of treatment’ during which they adhere to the treatment regimen, evaluating its effectiveness against their beliefs and expectations (Donovan & Blake 1992). Where outcome does not meet expectations, they may be more likely to change regimen or stop treatment.
THE CLINICAL CONSULTATION
High levels of non-adherence may occur if interventions have not addressed underlying health and treatment beliefs driving patient behaviour. It would be useful within the clinical consultation if patients’ beliefs about illness and treatment are elicited, their expectations of treatment are identified and realistic treatment goals negotiated (Carr & Donovan 1998, Horne 1999). A consultation guide has been developed based on the evidence for factors influencing adherence (Daltroy 1993) but its effectiveness in promoting adherence or concordance has not been evaluated (Box 5.3).
BOX 5.3 Stepwise model of a consultation to improve adherence
(from Daltroy 1993)
Step 1 The patient is encouraged to express all concerns
Step 2 The patients’ concerns are discussed
Step 3 Doctor and patient share their models (beliefs) of disease and symptoms
Step 4 Doctor and patient share their goals for treatment
Step 5 Treatment goals are agreed and priorities are set
Step 6 Doctor and patient share their models (beliefs) of treatment
Step 7 Potential barriers to adherence are identified
Step 8 Plans are made to overcome these
Step 9 The doctor provides written information on disease and the treatment regimen, annotated with individual patients’ detail/concerns
Concordance, i.e. an equal partnership between patient and health professional in which treatment goals are negotiated on the basis of patient preference and priorities, is promoted by addressing these.
Questionnaires for assessing adherence and concordance
Whilst useful in identifying how patients take their medicines (de Klerk et al 1999), their usefulness in promoting adherence is limited because they provide little information about why patients take their medications in this way, or why they choose not to follow their prescribed treatment regimen at all. Established, validated questionnaires that elicit some of the health beliefs underlying adherence can be used to identify misperceptions and reasons for non-adherence. These include the IPQ and IPQ-R (Moss-Morris et al 2002, Weinman et al 1996) and the Beliefs about Medication Questionnaire (Horne et al 1999).
 Take a case history from a patient with a rheumatological condition and identity its psychological and social impact using a biopsychosocial approach. Using the gate control theory of pain, record how you would explain to a patient how their thoughts can affect their perception of pain. After reading section 4, list the factors that may influence whether a patient will engage in a specific health behaviour, such as exercise.
Take a case history from a patient with a rheumatological condition and identity its psychological and social impact using a biopsychosocial approach. Using the gate control theory of pain, record how you would explain to a patient how their thoughts can affect their perception of pain. After reading section 4, list the factors that may influence whether a patient will engage in a specific health behaviour, such as exercise.Understanding theories of health behaviour and factors influencing coping and concordance enhance effectiveness of treatment and planning and delivering effective patient education.
CONCLUSION
The ways in which people with arthritis perceive, understand and manage their condition, how active they are, which treatments they use, whether and how they take their prescribed medication and how they cope with the symptoms of their arthritis, are influenced by a complex interaction of many factors. By increasing the health professional’s knowledge in this area a relationship based on concordance principles can be introduced into clinical care and patients will be able to cope more effectively with the physical, psychological and social impact of their condition.
References and further reading
Abraham C., Sheeran P. The health belief model. In: Conner M., Norman P., editors. Predicting Health Behaviour. Milton Keynes: Open University Press; 2005:28-80.
Ajzen A., Fishbein M. Understanding Attitudes and Predicting Social Behaviour. Englewood Cliffs, NJ: Prentice-Hall, 1980.
Ajzen I. The theory of planned behaviour. Organ. Behav. Hum. Dec. Process.. 1991;50:179-211.
Bandura A. Self-efficacy mechanism in psychobiologic functioning. In: Schwarzer R., editor. Self-efficacy: Thought control of action. Washington DC: Hemisphere; 1992:335-394.
Barlow J.H., Williams B., Wright C. The generalised self-efficacy scale in people with arthritis. Arthritis. Care Res.. 1996;9(3):189-196.
Barlow J.H., Williams B., Wright CC. The reliability and validity of the arthritis self-efficacy scale in a UK context. Psychol. Health Med.. 1997;2(1):3-17.
Becker M.H., Haefner D.P., Kasl S.V., et al. Selected psychosocial models and correlates of individual health-related behaviours. Med. Care. 1977;15:27-46.
Bendor R. Arthritis and I. Ann.Intern. Med.. 1999;131(2):150-152.
Burckhardt C., Clark S., O’Reilly S., Bennett R. Pain coping strategies of women with fibromyalgia: Relationship to pain, fatigue and quality of life. J. Musculoskelet. Pain. 1997;5(3):5-21.
Carr A.J., Donovan J.L. Why doctors and patients disagree. Br.J. Rheumatol.. 1998;37:1-6.
Carr A.J., Thompson P.W., Cooper C. Factors associated with adherence and persistence to bisphosphonate therapy in osteoporosis: a cross-sectional survey. Osteoporos. Int.. 2006;17(11):1638-1644.
Conrad P. The meaning of medications: another look at compliance. Soc. Sci. Med.. 1985;20:29-37.
Cox M. The development of a user led clinical service for newly diagnosed RA patients. Musculoskel. Care. 2004;2(4):229-239.
Cross M., March L., Lapsley H., et al. Patient self-efficacy and health locus of control: relationships with health status and arthritis-related expenditure. Rheumatology. 2006;45(1):92-96.
Daltroy L.H. Doctor patient communication in rheumatological disorders. Bailliere’s Clin. Rheumatol.. 1993;7:221-239.
De Klerk E., van der Heijde D., van der Tempel H., et al. Development of a questionnaire to investigate patient compliance with antirheumatic drug therapy. J. Rheumatol.. 1999;26:2635-2641.
Devor M., Seltzer Z. Pathophysiology of damaged nerves in relation to chronic pain. In: Wall P.D., Melzack R., editors. Textbook of Pain. fourth ed. Edinburgh: Churchill Livingstone; 1999:129-163.
Dickens C., Creed F. The burden of depression in patients with RA. Rheumatology. 2001;40:1327-1330.
Donovan J. Patient education and the consultation: the importance of lay beliefs. Ann. Rheum. Dis.. 1991;50:418-421.
Donovan J.C.L., Blake D.R. Patient non-compliance: deviance or reasoned decision-making. Soc. Sci. Med.. 1992;34:507-513.
Felton B.J., Revenson T.A. Coping with chronic illness: a study of illness controllability and the influence of coping strategies on psychological adjustment. J. Counsel. Clin. Psychol.. 1984;52:343-353.
Fex E., Larson B.M., Nived K., et al. Effect of arthritis on work status and social and leisure time activities in patients followed 8 years from onset. J. Rheumatol.. 1998;25(1):44-50.
Fishbein M., Ajzen I. Belief, Attitude, Intention and Behaviour. New York: John Wiley & Sons; 1975.
Folkman S. Positive psychological states and coping with severe stress. Soc. Sci. Med.. 1997;45(8):1207-1221.
Folkman S., Lazarus R.S. Manual of the Ways of Coping Questionnaire. Paolo Alto, CA: Consulting Psychologists Press; 1988.
Goodwin J.S., Black S.A., Satish S. Aging versus disease: the opinions of older black, hispanic and non-hispanic white Americans about the causes and treatment of common medical conditions. J. Am. Geriatric Soc.. 1999;47:973-979.
Gordon P.A., Stoelb M., Chiriboga J. The vocational implication of two common rheumatic diseases. J. Rehabil.. 1997;63(1):15-19.
Haigh R.C., McCabe C.S., Halligan P., Blake D.R. Joint stiffness in a phantom limb: Evidence of central nervous system involvement in rheumatoid arthritis. Rheumatology. 2003;42:888-892.
Hakkinen A., Hannonen P.J., Nyman K., et al. Aerobic and neuromuscular performance capacity of physically active females with early or long term rheumatoid arthritis compared to matched healthy women. Scand. J. Rheumatol.. 2003;31:345-350.
Hampson S.E., Glasgow R.E., Zeiss A.M. Personal models of osteoarthritis and their relation to self-management and quality of life. J. Behav. Med.. 1994;17:143-158.
Hewlett S., Cockshott Z., Kirwan J., et al. Development and validation of a self-efficacy scale for use in British patients with rheumatoid arthritis (RASE). Rheumatology. 2001;40(11):1221-1230.
Hill J., Bird H., Johnson S. Effect of patient education on adherence to drug treatment for rheumatoid arthritis: A randomised controlled trial. Ann. Rheum. Dis.. 2001;60:869-875.
Hill J., Bird H., Thorpe R. Effects of rheumatoid arthritis on sexual activity and relationships. Rheumatology. 2003;42:280-286.
Hobro N., Weinman J., Hankins J. Using the self-regulatory model to cluster chronic pain patients: the first step towards identifying relevant treatments. Pain. 2004;108:276-283.
Horne R. Patients’ beliefs about treatment: The hidden determinant of treatment outcome. J. Psychosom. Res.. 1999;47:491-495.
Horne R., Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J. Psychosom. Res.. 1999;47:555-567.
Horne R., Weinman J., Hankins M. The Beliefs about Medicines Questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol. Health. 1999;14:1-24.
Hughes G., Martinez C., Myon E., et al. The impact of a diagnosis on fibromyalgia on health care resource use by primary care patients in the UK. Arthritis. Rheum.. 2006;54(1):177-182.
Hyrich K., Symmons D., Watson K., et al. Baseline co-morbidity rates levels in biologic and standard DMARD treated patients with RA: results from a national register. Ann. Rheum. Dis.. 2006;65:895-898.
International Association for the Study of Pain (IASP). Classification of chronic pain. Description of chronic pain syndromes and definitions of pain terms, second ed. Seattle: IASP; 1994.
Jerant A.F., von Friederichs-Fitzwater M.M., Moore M. Patients’ perceived barriers to active self management of chronic conditions. Patient Educ. Couns.. 2005;57:300-307.
Katz P.P., Yelin E.H. Activity loss and the onset of depressive symptoms; do some activities matter more than others. Arthrit. Rheum.. 2004;44:1194-1202.
Keefe F.J., Kashikar-Zuck S., Robinson E., et al. Pain coping strategies that predict patients’ and spouses’ ratings of patients’ self-efficacy. Pain. 1997;73(2):191-199.
Kraag G.R., Gordon D.A., Menard H.A., et al. Patient compliance with tenoxicam in family practice. Clin. Ther.. 1994;16:581-593.
Lefebvre J.C., Keefe F.J., Affleck G., et al. The relationship of arthritis self-efficacy to daily pain, daily mood and daily pain coping in rheumatoid arthritis patients. Pain. 1999;80(1-2):425-435.
Leventhal H., Benyamini Y., Brownlee S., et al. Illness representations: Theoretical foundations. In: Petrie K.J., Weinman J.A., editors. Perceptions of Health and Illness. The Netherlands: Harwood, 1997.
Lowe B., Willand L., Eich W., et al. Psychiatric comorbidity and work disability in patients with inflammatory diseases. Psychosom. Med.. 2004;66:395-402.
McCabe C.S. Pain mechanisms and the rheumatic diseases. Musculoskel Care. 2004;2(2):75-89.
Mancuso C.A., Paget S.A., Charlson M.E. Adaptations made by RA patients to continue working. Arthritis. Care Res.. 2000;13(2):89-99.
Melzack R., Wall P.D. Pain mechanisms: A new theory. Science. 1965;150:971-979.
Minnock P., Fitzgerald O., Bresnihan B. Women with established RA perceive pain as the predominant impairment in health status. Rheumatology. 2003;42:995-1000.
Moss-Morris R., Weinman J., Petrie K.J., et al. The revised Illness Perceptions Questionnaire (IPQ-r). Psychol. Health. 2002;17:1-16.
National Rheumatoid Arthritis Society. The National Rheumatoid Arthritis Society Survey. Berkshire: NRAS; April 2003.
Neame R., Hammond A. Beliefs about medications: a questionnaire survey of people with rheumatoid arthritis. Rheumatology. 2005;44:762-767.
Newman S., Fitzpatrick R., Lamb R., et al. Patterns of coping in RA. Psychol. Health. 1990;4:187-200.
Nicassio P.M., Wallston K.A., Callahan L.F., et al. The measurement of helplessness in RA: the development of the arthritis helplessness index. J. Rheumatol.. 1985;12:462-467.
O’Reilly S., Muir K., Doherty M. Effectiveness of home exercise on pain and disability from osteoarthritis of the knee: a randomised controlled trial. Ann. Rheum. Dis.. 1999;58:15-19.
Parker J.C., Smarr K.L., Slaughter J.R., et al. Management of depression in rheumatoid arthritis: a combined pharmacologic and cognitive behavioural approach. Arthritis. Rheum.. 2003;49:766-777.
Phelan, M., Campbell, A., Byrne, J., et al., 1994. The effect of an education programme on the perception of arthritis by spouses of patients with rheumatoid arthritis. Scand. J. Rheumatol. 74 (Suppl).
Radojenic V., Nicassio P.M., Weisman M.H. Behavioural interventions with and without family support for rheumatoid arthritis. Behav. Ther.. 1992;23:13-30.
Rejeski W.J., Brawley L.R., Ettinger W., et al. Compliance to exercise therapy in older participants with knee osteoarthritis: implications for treating disability. Med. Sci. Sport. Exerc.. 1997;29:977-985.
Rosenstiel A.K., Keefe F.J. The use of coping strategies in chronic low back pain patients: relationship to patient characteristics and current adjustment. Pain. 1983;17(1):33-44.
Rotter J.B. Social Learning and Clinical Psychology. Englewood Cliffs, NJ; 1954.
Royal College of Nursing (RCN). Sexuality and Sexual Health in Nursing practice. London: Royal College of Nursing; 2000.
Ryan S., Hassell A., Dawes P., et al. Control perceptions in patients with rheumatoid arthritis: the role of social support. Care. 2003;1(2):108-118.
Sakalys J.A. Illness behaviour in rheumatoid arthritis. Arthritis Care Res.. 1997;10:229-237.
Schwarzer R. Self-efficacy in the adoption and maintenance of health behaviours: Theoretical approaches and a new model. In: Schwarzer R., editor. Self-efficacy: thought control of action. Washington DC: Hemisphere; 1992:217-241.
Sharpe L., Sensky T., Timberlake N., et al. Long-term efficacy of a cognitive behavioural treatment from a randomised controlled trial for patients recently diagnosed with rheumatoid arthritis. Rheumatology. 2003;42:435-441.
Sheehy C., Murphy E., Barry M. Depression in RA-underscoring the problem. Rheumatology. 2006;45:1325-1327.
Smith C., Wallston K. Adaptation in patients with chronic rheumatoid arthritis: Application of a general model. Health Psychol.. 1992;11(3):151-162.
Smith C., Wallston K., Dwyer K., et al. Beyond good and bad coping: A multidimensional examination of copping with pain in persons with rheumatoid arthritis. Ann. Behav. Med.. 1997;19(1):1-11.
Specht J., King G., Brown E., et al. The importance of leisure in the lives of persons with cognitive physical disability. Am. J. Occup. Ther.. 2002;56(4):436-445.
Spranglers M.A., de Regt E.B., Andries F., et al. What chronic conditions are associated with better or poorer quality of life. J. Clin. Epidemiol.. 2000;53(9):895-907.
Strating M., van Schurr W., Suurmeijer T. Contribution of partner support in self-management of rheumatoid arthritis patients. An application of the theory of planned behaviour. J. Behav. Med.. 2006;29(1):51-60.
Turk D.C., Melzack R. Handbook of Pain Assessment. New York: Guildford; 1992.
Viller F., Guillemin F., Briancon S., et al. Compliance to drug treatment of patients with RA : a 3 year longitudinal study. J. Rheumatol.. 1999;26:2114-2122.
Wallston K.A., Wallston B.S., DeVellis R. Development of multidimensional health locus of control (MHLC) scales. Health Educ. Monogr.. 1978;6:160-170.
Weinman J., Petrie K.J., Moss-Morris R., et al. The Illness Perception questionnaire: a new method for assessing cognitive representation of illness. Psychol. Health. 1996;11:114-129.
Wikstrom I., Jacobsson L.T.H., Arvidsson B. How people with rheumatoid arthritis perceive leisure activities: a qualitative study. Care. 2005;3(2):74-84.
Yelin E. Musculoskeletal conditions and employment. Arthritis. Care Res.. 1995;8(4):311-317.
Zautra A., Manne S. Coping with rheumatoid arthritis: A review of a decade of research. Ann. Behav. Med.. 1992;14:31-39.