Chapter 9 Occupational therapy
Treatment options in rheumatology
KEY POINTS
 The role of the occupational therapist in rheumatology is to: improve a person’s ability to perform daily tasks and valued life roles; facilitate successful adaptation to disruption in lifestyle, prevent loss of function and improve or maintain psychological status With its focus on occupational performance the link between biological, psychological, social factors and activity is central to OT interventions which are characterized by a patient centred approach Interventions are informed by the use of accurate and timely assessment to identify areas of activity limitation of relevance to the individual Some of the main approaches used by occupational therapists focus on improving occupational performance by:
The role of the occupational therapist in rheumatology is to: improve a person’s ability to perform daily tasks and valued life roles; facilitate successful adaptation to disruption in lifestyle, prevent loss of function and improve or maintain psychological status With its focus on occupational performance the link between biological, psychological, social factors and activity is central to OT interventions which are characterized by a patient centred approach Interventions are informed by the use of accurate and timely assessment to identify areas of activity limitation of relevance to the individual Some of the main approaches used by occupational therapists focus on improving occupational performance by:

INTRODUCTION
Occupational therapy aims to help a person with a rheumatic disease be who they want to be and do the things they want to do, need to do or are expected to do (Law et al 2005). The role of the occupational therapist in rheumatology is to: improve a person’s ability to perform daily tasks and valued life roles; facilitate successful adaptation to disruption in lifestyle, prevent loss of function and improve or maintain psychological status (College of Occupational Therapists 2003). This is achieved by promoting health and well being through occupation across the life course. This chapter will explore some of the primary interventions used by occupational therapists to achieve this aim focusing on key occupational roles.
THE IMPACT OF RHEUMATOID ARTHRITIS ON OCCUPATIONAL PERFORMANCE
Longitudinal cohort studies of people with rheumatoid arthritis (RA) highlight its significant impact in terms of activity limitation with up to 49% of participants experiencing moderate disability after 10 years (Symmons & Silman 2006, Wolfe 2000). Whilst the model of progressive disability suggests that this occurs as a consequence of disease over time, recent work has questioned this linear model. Some evidence suggests that most disability occurs in the first 3 years of diagnosis whilst the work by Wolfe suggests that, on an individual basis, the impact of RA on activity limitation may be more variable and chaotic and less linear (Wolfe 2000). Routine assessment of activity is important therefore to identify early when activity limitation starts to occur in a person’s illness trajectory.
Many studies provide insights into the significant challenges faced by people living with rheumatic diseases in terms of its impact on all areas of activity. Longitudinal studies suggest that over a five year period people with RA can lose the ability to undertake 10% of the activities they value (Katz 1995). Approximately one-third of people with RA report stopping work within 3 years of being diagnosed (Young et al 2000) and leisure activities are also affected profoundly. Fex et al 1998 found that 75% of the 106 patients in their study had to alter leisure time activities and 50% were not satisfied with their recreation.
OCCUPATIONAL THERAPY MANAGEMENT
Factors including age, stage of disease, life context, personal priorities, beliefs and culture all influence a person’s illness experience and the specific challenges they face. There is therefore no standard approach to the occupational therapy management of a person with a rheumatic disease. Emphasis is placed on conducting accurate and timely assessment to identify areas of activity limitation of relevance to the individual.
Theoretical models underpinning occupational therapy such as the Canadian Model of Occupational Performance (Canadian Association of Occupational Therapists 1997) (Fig. 9.1), the Person Environment Occupational Performance Model (Christiansen et al 2005), the Model of Human Occupation (Kielhofner 2002) and the newer Kawa model (Iwama 2006) are aligned closely to the biopsychosocial model described in chapter 5. With its focus on occupational performance the link between biological, psychological, social factors and activity is central to OT interventions which are characterised by a patient centred approach.
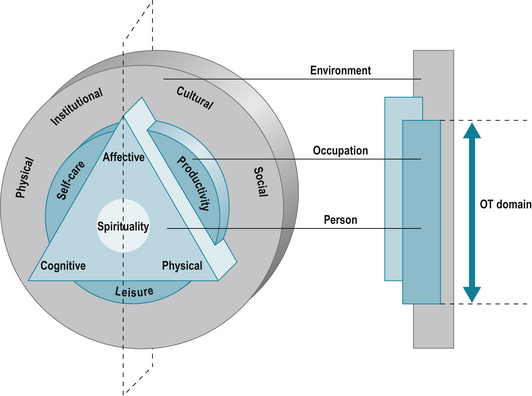
Figure 9.1 The Canadian Occupational Performance Model.
Reproduced from The Canadian Model of Occupational Performance and Engagement. In: Townsend E, Polatajko H (2007) Enabling Occupation II: Advancing an Occupational Therapy Vision for Health, Well-being & Justice through Occupation. CAOT Publications ACE, Ottawa, ON p. 23 with permission of CAOT Publications ACE.
THE EVIDENCE BASE
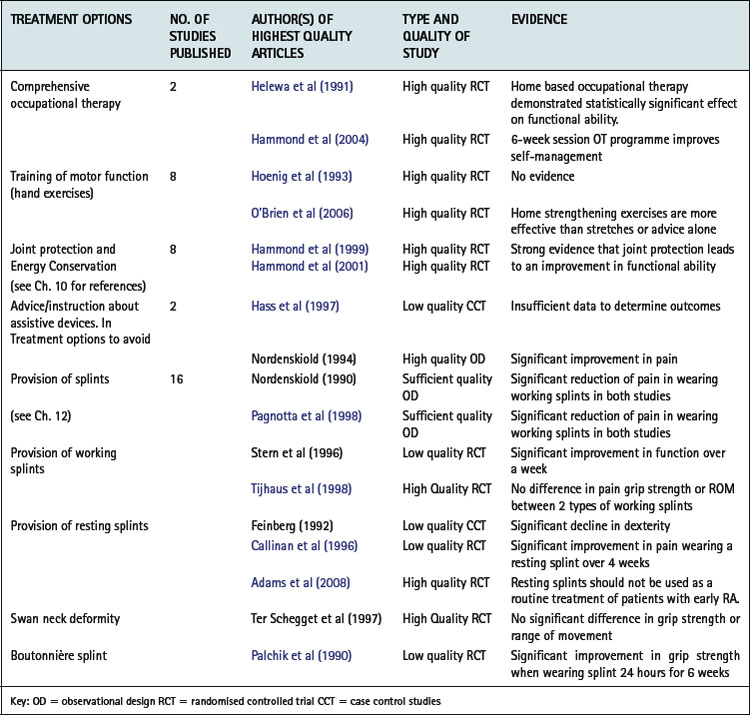
There is a growing body of evidence relating to the efficacy of occupational therapy interventions which allows therapists, clinicians and managers as well as the service user to make informed decisions about the best treatment options and design their interventions and services accordingly. Steultjens et al (2004) found varying degrees of evidence for the effectiveness of occupational therapy (Table 9.1), most of which is derived from work undertaken with people with inflammatory arthritis. Some areas of practice, such as work and leisure, remain under evaluated and further research is required in these areas.
ASSESSMENT OF ACTIVITY LIMITATION
Assessment is fundamental to the planning of interventions and the evaluation of their efficacy. The focus of assessments used by occupational therapists is on identifying areas of activity limitation defined by the World Health Organization (WHO) as difficulties an individual may have in executing activity (WHO 2001). Assessment of activity limitation can broadly be categorised as the use of standardized assessments and the use of structured interviews.
THE INITIAL INTERVIEW
Occupational therapy interventions are based upon information gathered in the structured initial interview. Therapists use this interview to gain background information about the person and explore the context of their lives, e.g. family and social support, employment, hobbies and interests, type of housing, current use of assistive devices and adaptations, benefits, self-management and coping strategies as well as relevant information about their impairment and the treatment they are receiving. This process information may also be supplemented with standard assessments or a structured interview exploring specific areas of activity in detail. This identifies specific areas of activity limitation to inform treatment planning.
STANDARDIZED ASSESSMENT
Standardized assessments of activity limitation are used extensively in research and clinical contexts to:
Many of the quality of life assessments used in rheumatology incorporate subscales for activities of daily living alongside measures of psychological well-being and symptoms. For example, the Arthritis Impact Measurement Scale 2 (AIMS2) has subscales assessing physical activity, dexterity, household activity, social activities and activities of daily living (Meenan et al 1992). Some measures focus specifically on activity limitation and have been developed for use with a number of different rheumatic diseases e.g. the Disability Index of the Health Assessment Questionnaire (HAQ) (Fries et al 1980). Others are disease specific, such as the Bath Ankylosing Spondylitis Functional Index (Calin et al 1994).
Whilst some assessments, such as the HAQ, cover a broad range of activities others focus on specific domains of activity, e.g. The Rheumatoid Arthritis Work Instability Scale (Gilworth et al 2003) or the Parenting Disability Indices (Katz et al 2003). These may be used as an additional assessment when more detailed information is required about a specific area of activity limitation. Other measures focus on activity limitation associated with specific regions of the body, such as the Oxford Hip Score (Dawson et al 1996) or The Disabilities of the Arm Shoulder and Hand (Hudak et al 1996).
Standardized assessments have been evaluated extensively to ensure that they are valid, (measuring what they claim to measure), reliable (are as accurate as possible) and sensitive to change (able to detect change when change has occurred). Many of the measures described above are self-complete questionnaires comprising a range of predefined activities against which a person rates the level of difficulty they experience when completing each activity. However some assessment may include observation or assessment of a person completing specific activities. Others incorporate an element of measurement such as grip strength or range of movement, e.g. The Jebsen Test of Hand Function (Jebsen et al 1969). Whilst standardized measures have demonstrated efficacy in clinical and research contexts one of the criticisms of their use in a clinical context is their inability to capture activities which are important to clients (Hewlett 2003).
A recent development has been the patient generated index which enables each person to identify areas of activity limitation of greatest concern to them. Two examples relevant to activity limitation are the MACTAR Patient Preference Disability Questionnaire (Tugwell et al 1987) and the Canadian Occupational Performance Measure (COPM) (Law et al 1990, 2005). The COPM is informed by a semi-structured interview during which people are asked to identify areas of activity limitation and rank them in order of importance. For the top five activities, they rate their current performance of the activity and satisfaction with their current performance. These activities inform the treatment programme and the person is reassessed to evaluate the efficacy of the intervention. The COPM is congruent with a person centred approach and does not constrain the activities a client can identify (see Ch. 4 for further information on patient reported outcome measures).
SEMI-STRUCTURED INTERVIEWS
Whilst the use of standardized assessments is encouraged as a basis for assessment many therapists, in a clinical context, continue to use a semi- structured interview format exploring a wide range of areas of activity. Such interviews are often formulated on a departmental basis. However, this in-depth information cannot be used as an accurate measure against which treatment outcomes can be assessed. Therefore increasingly therapists are using a combination of initial interview and standardized measures to inform their interventions
PROMOTING INDEPENDENCE IN KEY ACTIVITIES
This section explores some of the main areas of activity limitation experienced by people with rheumatic diseases and provides insights into the ways in which such limitations can be reduced. The use of joint protection, energy conservation, orthotics and psychological support are addressed in other chapters but are inherent to maintaining independence.
THE IMPACT OF RHEUMATIC DISEASES ON SELF CARE AND HOUSEHOLD ACTIVITIES
The loss of ability to perform activities of daily living is one of the most documented consequences of rheumatic diseases (Symmons & Silman 2006, Wolfe 2000). Sokka et al (2003) demonstrated that patients with rheumatoid arthritis have a 7-fold risk of functional disability in self care activities as measured by the HAQ compared to the normal population.
OCCUPATIONAL THERAPY INTERVENTIONS
The strongest evidence in rheumatology occupational therapy is also informed by the impact of interventions on activities of daily living (Hammond et al 1999, 2001, Helewa et al 1991). Some of the main approaches used by occupational therapists focus on improving occupational performance by:
Using alternative methods
The development of skills in joint protection and energy conservation is one of the main occupational therapy interventions to maintain levels of activity and is described in chapter 10.
Using assistive devices
People with arthritis are one of the largest user groups of assistive devices (Rogers & Holmes 1992). These are used to:
Devices are usually provided on a permanent basis but, in some instances, may only be required for a short period, e.g. post joint replacement surgery. Studies suggest that up to a third of devices provided remain unused (Scherer 2002). A number of factors contribute to non-use, such as changes in the person’s condition, the impact of comorbidities, lack of involvement in the assessment process, inadequacy of the device, embarrassment and a preference for person assistance (Wielandt & Strong 2000). Therefore, careful assessment is required considering factors relevant to:

Figure 9.2 Key factors to consider when assessing for assistive technology.
(adapted from the Trusted Assessor Framework Winchcombe & Ballinger 2005)
The majority of large devices, such as bath lifts, are supplied via statutory services. Depending on where a person lives, smaller items may have to be purchased privately. As designers and manufacturers are starting to accommodate the needs of a wide range of users in product design more mainstream household products and appliances are becoming increasingly accessible and easy to use for people with arthritis.
Adapting the environment
In some circumstances it is necessary to carry out minor adaptations or more extensive building work within the person’s home or work place. Common adaptations for people with rheumatic diseases include the installation of level access showers, stairlifts and the creation of easier access into the home. Such work can be undertaken through statutory services or people may choose to fund such work privately.
As people develop an understanding of the problems associated with living with arthritis they often make changes to their home environment when undertaking renovation work. For example, installing lever taps, easier door handles and locks, raising electric sockets, designing easily accessible and energy saving kitchens, raising toilet height and installing a downstairs toilet (see Box 9.1 and Fig. 9.3).
BOX 9.1 Additional resources related to assistive devices and adaptations
Disabled Living Foundation: provides information and advice about assistive devices and a wide range of fact sheets can be downloaded from their website. The DLF also produces DLF Data the main national database for assistive devices. Assist UK leads a national network of demonstration centres across the country that provide impartial information and advice on AT and inclusive design. Research Institute for Consume Affairs (RICAbility) produce a variety of consumer reports related to a range of consumer products including: Easier Living; Ins and outs of bathing; Making your kitchen easier to use; Choosing a vacuum cleaner that’s easier to use; Choosing a washing machine that’s easier to use; Choosing an iron that’s easier to use; Choosing an electric kettle that’s easier to use; Motoring and arthritis Arthritis Care provides a range of leaflets and online information. Titles include Independent Living and Arthritis. Working with Arthritis and Home Sweet Home. Arthritis Research Campaign publishes a range of leaflets: Looking after your Joints when you have Arthritis and Gardening and Arthritis. National Rheumatoid Arthritis Society provides information and advice relating to lifestyle issues. Publications include: Rheumatoid arthritis and computing; I Want to Work. A Self-Help Guide for People with Rheumatoid Arthritis; When an Employee has Rheumatoid Arthritis: An Employers Guide and I Want to Work, Report from the 2007 Work Survey.Note: website addresses can be found at the end of the chapter.

THE IMPACT OF RHEUMATIC DISEASES ON FAMILY ROLES
Studies exploring impact on parenting roles consistently identify the challenges faced with different aspects of childcare (Backman et al 2007, Grant 2001, Katz et al 2003). These studies highlight practical problems and also the psychological consequences of being unable to fulfil perceived parenting roles. Whilst attention has focused on the experiences of women with RA, recent studies have also explored the experiences of women with ankylosing spondylitis (AS), systemic lupus erythematosus (SLE) and juvenile idiopathic arthritis (Backman et al 2007). Problems are also experienced by men undertaking fathering roles and by men and women in relation to grandparenting roles (Barlow et al 1999). A survey of 231 women with RA identified that greater parenting disability was associated with poorer general function, more pain and fatigue, more parenting stress and greater psychological distress (Katz 2003).
ASSESSMENT
Few standardized assessments of parenting disability exist. One example is the Parenting Disability Index (Katz 2003). Assessment may take place when problems arise, but also therapists can work with mothers during pregnancy to help prepare for the arrival of their child, advise on the purchase of appropriate childcare equipment, put in place the necessary practical support and advise on fatigue management.
INTERVENTIONS
Practical problems, especially with regard to caring for babies and younger children, are experienced in all aspects of childcare such as holding, lifting, carrying, bathing and changing, dressing and feeding. For women with RA these problems can be exacerbated in the early months of motherhood by an increase in their disease activity. Careful selection of products can help to reduce the problems experienced. There is a wide variation in the design and usability of prams, car seats, cots and feeding equipment and guiding parents to think about such features as weight, size, design of controls, fastenings, switches and general ease of use when selecting products can save a great deal of money.
As children grow, parents with arthritis may experience problems in taking part in the wider aspects of the child’s life such as school or club activities, family outings and holidays. Studies exploring parenting with rheumatic conditions highlight the emotional consequences associated with being unable to fulfil such activities (Backman et al 2007, Grant 2001, Katz et al 2003). Psychological support is therefore an important aspect of working with parents. This may be provided by the therapist but also facilitated through referral to a voluntary sector organisation such as Arthritis Care, The Disabled Parents Network or the National Rheumatoid Arthritis Society (Box 9.2).
BOX 9.2 Additional resources for parenting with arthritis
Research Institute for Consumer Affairs (RICAbility) produce a range of consumer reports for disabled parents on childcare products including: pushchairs, highchairs, baby carriers, bottle warmers and sterilisers; safety gates National Rheumatoid Arthritis Society (NRAS)- website has a section on pregnancy which provides a range of information on aspects of pregnancy, childbirth and childcare including: My Experience of Pregnancy, Birth and Caring for a Small Baby whilst coping with Rheumatoid Arthritis: a members story, Coping with your Baby when you have Rheumatoid Arthritis and Handy TipsNote: website addresses can be found at the end of the chapter.
THE IMPACT OF RHEUMATIC DISEASES ON EMPLOYMENT
Despite medical advances (Bejarano et al 2008, Puolakka et al 2004) the incidence of work disability in rheumatoid arthritis is still significant (Eberhardt et al 2007, Young et al 2000). The National Rheumatoid Arthritis Society (NRAS) ‘I want to work’ survey (2007) reported that only 54.8% of respondents were in employment - nearly 30% less than the Government’s 80% target of employment for all working age adults (Department of Work and Pensions (DWP) 2007). Of those not in employment, 28.4% had given up work within 1 year and 59% were work disabled within 6 years of diagnosis. Other rheumatic diseases, such as systemic lupus erythematosus, have even higher levels of work disability with rates of 47% at diagnosis (Yelin et al 2004).These figures pose a challenge to both clinicians and policy makers with the increased emphasis on keeping people in work and extending working life beyond the current retirement age of 65.
The personal costs of unemployment from decreased quality of life and social exclusion are enormous but the socioeconomic costs are also great. The DWP report forecasted in 2007 that in 2007-2008 429,000 people with musculoskeletal diseases would claim £1.429 billion via the Employment and Support Allowance (ESA). Prognostic factors for work disability in rheumatoid arthritis include higher HAQ scores, lower educational status, older age, and manual work (Eberhardt et al 2007).
VOCATIONAL REHABILITATION
Employment issues in rheumatic diseases must therefore be addressed as early as possible (Frank and Chamberlain 2001, Nordmark et al 2006). The College of Occupational Therapy (COT) Specialist Section on Work clearly identifies the role and opportunities for occupational therapists to be involved in vocational rehabilitation (COT 2007) and this is expanded upon in the Work Matters Booklet (COT 2007). The NRAS I want to work Survey (NRAS 2007) also identified the need for more occupational therapists to be trained to provide work rehabilitation.
Work screening
Given the potential for people to experience work related problems at an early stage in their disease it is vital that work related problems are detected early and dealt with by an appropriate individual, e.g. an occupational therapist, other health professional or employment advisor. Work instability is used to describe a mismatch between a person’s functional capacity and the demands of their job (Gilworth et al 2003). The Rheumatoid Work Instability Scale (RA- WIS) (Gilworth et al 2003) is a validated screening tool developed to detect, measure and prioritise people’s work instability.
Work interview
If work problems are identified a specific work interview can be undertaken. Cynkin et al (1990) describe a potential structure for a work interview as does Melvin (1998). Box 9.3 suggests some of the information the therapist should collect.
BOX 9.3 Questions to ask in a work interview
Current employment details (job title, employers details, hours of work, shift pattern, breaks, previous and current sick leave, financial status - current pay, e.g. full/half pay and disability/or Employment Support Allowance (formerly Incapacity Benefit) etcStandardized semi-structured work interviews such as the Worker Role Interview (WRI) are also available (Velozo et al 1999).
STANDARDIZED ASSESSMENT TOOLS
Various assessment tools are available and are listed in the Work Matters booklet (COT 2007). In some instances the work interview may identify the need to carry out a more detailed assessment to determine work abilities. This can be done through a detailed job analysis (Joss 2007) using a mix of analysis tools, e.g. the Valpar Profile Analysis Guide (Valpar International Corporation 2007a) in combination with the Revised Handbook for Analyzing Jobs (US Department of Labor 1991).
A Functional Capacity Evaluation (FCE) is an all-encompassing term to describe the physical assessment of an individual’s ability to perform work- related activity (American Occupational Therapy Association 2008). Work samples such as the VALPAR Work Samples (Valpar International Corporation 2007b) are criterion referenced standardized work simulated assessments which are analysed using the methods time management (MTM) industrial performance standards. A worksite assessment is valuable for environmental, ergonomic and job demands assessment and to gain an impression of psychosocial and interpersonal issues at work. Evaluating employment interventions is essential to ensure ongoing work stability. Once a person leaves employment it is much more difficult for them to reenter it.
INTERVENTIONS: THE EVIDENCE
There has been little high quality research carried out demonstrating the positive effects of occupational therapy alone in improving work outcomes in rheumatic diseases. A small RCT (n = 28) by Macedo et al (2007) found that, at 6-month follow-up, comprehensive occupational therapy significantly improved functional ability, pain, work satisfaction and reduced work instability in rheumatoid arthritis, although there were no differences in number of days work missed or work performance.
A systematic review of vocational rehabilitation carried by de Buck et al (2002) identified six multidisciplinary rehabilitation programs, five of which showed a marked positive effect of work rehabilitation on work status (work disability, sick leave, job modification, paid occupation, retraining). Proof of benefit was limited due to limitations and differences in methodologies and none were randomized controlled trials. Allaire et al (2003) carried out a randomized controlled trial (RCT) demonstrating that people receiving vocational rehabilitation stayed in work longer compared to the control group receiving written advice only. The intervention was delivered by experienced rehabilitation counselors. It consisted of two 1.5-hour sessions with three components: job accommodation, vocational counseling and guidance, and education and self-advocacy.
De Buck et al (2004) conducted a RCT evaluating patient and occupational physician satisfaction with a multidisciplinary job retention vocational rehabilitation programme for patients with rheumatic diseases. The team included an occupational therapist. The individualized programme addressed job accommodation issues, promotion of self-efficacy, changes in medication, exercise, functional training and psychological interventions. Patients were most satisfied with the interpersonal approach and knowledge gained and least satisfied with waiting times for the final work report and application of advice. Unfortunately, the programme did not impact on work status.
The extent of work rehabilitation needed varies considerably between patients. Verbal or written advice may be all that is required. For example, explaining employees’ and employers’ rights and responsibilities under the Disability Discrimination Act (1995), issuing a copy of the Working Horizons booklets (Arthritis Care 2006) or ‘I want to work’: guide for people with arthritis/employers (NRAS 2007). More complex interventions may be required and these are described in Box 9.4.
THE IMPACT OF RHEUMATIC DISEASES ON COMMUNITY, SOCIAL AND CIVIC LIFE
The International Classification of Function Disability and Health (WHO 2001) lists community life, recreation and leisure, play, religion and spirituality, human rights and political life and citizenship as areas included in community, social and civic life.
Rheumatic diseases have a significant impact on people’s lifestyles including their leisure time and participation in community life (Fex et al 1998, Wikstrom et al 2006, Yelin et al 1987). As well as having lower rates of functional ability and lower rates of employment, people with arthritis also experience reductions in their leisure activities. Fex et al (1998) in a longitudinal survey found that 75% of people with rheumatoid arthritis had to change their leisure activities and 50% were unsatisfied with their recreation. Wikstrom et al (2006) identified that newly diagnosed RA patients performed significantly fewer leisure activities but did not have less interest in them. Predictors for low performance in leisure activities are lower education, higher age and higher HAQ score (Fries et al 1980). Loss of valued activities, including leisure, is correlated with poorer psychological status (Katz & Yelin 1994).
The term ‘leisure’ is hard to define by task alone. One person’s social or leisure activity may be another person’s paid employment, for example playing football or jewellery making. Leisure here is used to describe those activities not generally involving self-maintenance or paid employment.
OCCUPATIONAL THERAPY AND LEISURE
Occupational therapists have traditionally included the area of social participation and leisure in patient assessment. However, the political climate, the predominantly physical nature of rheumatic diseases and time constraints have led to less focus on these areas compared to self care employment and household activities. Turner et al (2000) found occupational therapists working in physical disability spent less time in assessing leisure areas compared to those working in psychosocial settings. This is alarming in view of the high incidence of psychosocial issues affecting those with rheumatic diseases.
Leisure assessment
The occupational therapy initial interview helps identify which leisure activities the person is involved in and how important they are in relation to other activities and roles. The COPM categorises leisure into three areas: quiet recreation, active recreation and socialisation. The UK Modified Interest Checklist (Heasman & Brewer 2008) is based on the Model of Human Occupation and gathers information on a client’s strength of interest and engagement in 74 activities in the past, present and future and can be used with adolescents or adults.
Leisure interventions
Joint protection, fatigue management, assistive technology, adaptations and orthotics all help to improve performance in leisure activities. Some patients may benefit from new or increased leisure activities, including aerobic exercise activities (Plasqui 2008) to assist in pain management and improve physical and psychological wellbeing. Rheumatology occupational therapy/rehabilitation assistants have a valuable role in enabling the person to achieve their leisure goals whether it be at home or in the wider community (Fig. 9.4).

CONCLUSION
The focus of occupational therapy interventions on the promotion and maintenance of independence in all areas of activity is central to the management of people with rheumatic diseases. People make sense of an illness experience not only in terms of how it makes them feel but also the impact that it has on their life. Whilst the onset of a rheumatic disease requires a person to reassess their understanding of their body in terms of how it feels and what it is capable of doing, many people manage to lead active and fulfilling lives. This is achieved through a process of learning relevant strategies and skills to manage their impairment and maximize their independence. This enables them to be and do the things they want to do, need to do or are expected to do within the context of their impairment.
Visit the rheumatoid arthritis section of healthtalkonline (www.healthtalkonline.org) and listen to the views and experiences which are being shared in this resource. A great deal of valuable information is provided on this site but listen specifically to the sections relating to occupational therapy, work, parenting and childcare and personal life and changes at home. Think about some of the products that you use in your daily life and find difficult to use. Choose one which would also be used by a person with arthritis and think about: Do some market research. Find as many examples of the product as possible on the internet, in magazines and shops and compare features such as shape, size, weight, ease of use, portability, controls. Also have a look at some of the sites highlighted in this chapter and find examples of assistive technologies which may be easier to use. Summarise your findings and thinking about the needs of a person with arthritis to identify the product which you feel would be the easiest for them to use and justify your choice. Visit the NRAS website (www.rheumatoid.org.uk) and read the two publications: ‘I want to work – a self help guide for people with rheumatoid arthritis’ and ‘When an employee has rheumatoid arthritis - a guide for employers.’Research Institute for Consumer Affairs (Ricability) www.ricability.org.uk
http://www.arthritiscare.org.uk
National Rheumatoid Arthritis Society
The Arthritis Research Campaign (arc)
References and further reading
Adams J., Burridge J., Mullee M., et al. The clinical effectiveness of static resting splints in early rheumatoid arthritis: a randomized controlled. Rheumatology. 2008;47(10):1548-1553.
Allaire S., Li W., La Valley M. Reduction of job loss in persons with rheumatic diseases receiving vocational rehabilitation: a randomized controlled trial. Arthritis Rheum.. 2003;48(11):3212-3218.
American Association of Occupational Therapy www.aota.org/Consumers/WhatisOT/WI/Facts/35117.aspx. Accessed 13/10/08.
Arthritis Care. Working Horizons. (booklet), 2nd edn. London: Arthritis Care. 2006.
Backman C., Del Fabro Smith L., Smith S., et al. ‘Sometimes I can, sometimes I can’t’: the influence of arthritis on mothers’ habits OTJR: occup. Participation Health. 2007;27(Supplement 1):775-785.
Barlow J., Cullen L.A., Foster N.E., et al. Does arthritis influence perceived ability to fulfil a parenting role? Perceptions of mothers, fathers and grandparents. Patient Educ. Couns.. 1999;37(2):141-151.
Bejarano V., Quinn M., Philip G., et al. Effect of the early use of the anti-tumor necrosis factor adalimumab on the prevention of job loss in patients with early rheumatoid arthritis. Arthritis Care Res.. 2008;59(10):1467-1474.
Calin A., Garrett S., Whitelock H., et al. A new approach to defining functional ability in ankylosing spondylitis: the development of the Bath Ankylosing Spondylitis Functional index. J. Rheumatol.. 1994;21(12):2281-2285.
Callinan N.J., Mathiowetz V. Soft versus hard resting hand splints in rheumatoid arthritis: pain relief, preference, and compliance. Am. J. Occup. Ther.. 1996;50:347-353.
Canadian Association of Occupational Therapists. Enabling Occupation: An occupational therapy perspective. Ottawa, ON: CAOT Publications; 1997.
Christiansen C.H., Baum C.M., Bass-Haugen J. Occupational Therapy: Performance, Participation, and Well-being, third ed. Thorofare, NJ: SLACK; 2005.
College of Occupational Therapists. Occupational Therapy in Vocational Rehabilitation: A Brief Guide to Current Practice in the UK. London: College of Occupational Therapists; 2007.
College of Occupational Therapists. Work Matters: Vocational Navigation for Occupational Therapy Staff. London: College of Occupational Therapists and National Inclusion Programme; 2007.
College of Occupational Therapists. Occupational Therapy Clinical Guidelines for Rheumatology. London: College of Occupational Therapists; 2003.
Cynkin S., Robinson A.M. Occupational Therapy and Activities Health: Toward Health through Activities, second ed. Boston: Little Brown Book Company; 1990.
Dawson J., Fitzpatrick R., Carr A., et al. Questionnaire on the perceptions of patients about total hip replacement. J. Bone Joint Surg.. 1996;78-B:185-190.
De Buck P., Schoones J., Allaire S., et al. Vocational rehabilitation in patients with chronic rheumatic diseases: A systematic literature review. Semin. Arthritis Rheum.. 2002;32(3):196-203.
De Buck P.D.M., Breedveld J., van der Giesen F.J., et al. A multidisciplinary job retention vocational rehabilitation programme for patients with chronic rheumatic diseases: patients’ and occupational physicians’ satisfaction. Ann. Rheum. Dis.. 2004;63(5):562-568.
Disability Discrimination Act, 1995. (c. 50), ISBN 0105450952 HMSO, London.
Department of Work and Pensions. Five Year Strategy: Opportunity and Security Throughout Life. Norwich: DWP Publications, The Stationery Office; 2005.
Eberhardt K., Larsson B., Nived K., et al. Work disability in rheumatoid arthritis-development over 15 years and evaluation of predictive factors over time. J. Rheumatol.. 2007;34(3):481-487.
Feinberg J. Effect of the arthritis health professional on compliance with use of resting hand splints by patients with rheumatoid arthritis. Arthritis Care Res.. 1992;5(1):17-23.
Fex E., Larsson B.M., Nived K., et al. Effect of rheumatoid arthritis on work status and social and leisure time activities in patients followed 8 years from onset. J. Rheumatol.. 1998;25(1):44-50.
Frank A., Chamberlain M. Keeping our patients at work: implications for the management of those with rheumatoid arthritis and musculoskeletal conditions. Rheumatology. 2001;40(11):1201-1205.
Fries J., Spitz P., Kraines R., et al. Measurement of patient outcome in arthritis. Arthritis Rheum.. 1980;23(2):137-145.
Gilworth G., Chamberlain M.A., Harvey A., et al. Development of a work instability scale for rheumatoid arthritis. Arthritis Care Res.. 2003;49(3):349-354.
Grant M. Mothers with arthritis, child care and occupational therapy: insight through case studies. Br. J. Occup Ther. 2001;64(7):322-329.
Hammond A., Lincoln N., Sutcliffe L. A crossover trial evaluating an educational-behavioural joint protection programme for people with rheumatoid arthritis. Patient Educ. Couns.. 1999;37(1):19-32.
Hammond A., Freeman K. One year outcomes of a randomised controlled trial of an educational-behavioural joint protection programme for people with rheumatoid arthritis. Rheumatology. 2001;40(9):1044-1051.
Hammond A., Young A., Kidao R. A randomised controlled trial of occupational therapy for people with early rheumatoid arthritis. Ann. Rheum. Dis.. 2004;63(1):23-30.
Hass U., Brodin H., Andersson A., et al. Assistive technology selection: a study of participation of users with rheumatoid arthritis. IEEE Trans. Rehabil. Eng.. 1997;5:263-275.
Heasman, D., Brewer, P., 2008. The UK Modified Interest Checklist www.moho.uic.edu accessed 3.2.09
Helewa A., Goldsmith C.H. Effects of occupational therapy home service on patients with rheumatoid arthritis. Lancet. 1991;337:1453-1457.
Hewlett S. Patients and clinicians have different perspectives on outcomes in arthritis. J. Rheumatol.. 2003;30(4):877-879.
Hoenig H., Groff G., Pratt K., et al. A randomized controlled trial of home exercise on the rheumatoid hand. J. Rheumatol.. 1993;20:785-789.
Hudak P., Amadio P., Bombardier C. Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) The Upper Extremity Collaborative Group (UECG). Am. J. Ind. Med.. 1996;29(6):602-608.
Iwama M. The Kawa Model. Culturally Relevant Occupational Therapy. Edinburgh: Churchill Livingstone; 2006.
Jebsen R., Taylor N., Trieschmann R., et al. An objective and standardized test of hand function. Arch. Phys. Med. Rehabil.. 1969;50(6):311-319.
Joss M. The Importance of Job Analysis in Occupational Therapy. Br. J. Occup. Ther.. 2007;70(7):301-303.
Katz P., Yelin EH. Life activities of persons with rheumatoid arthritis with and without depressive symptoms. Arthritis Care Res.. 1994;7(2):69-77.
Katz P. The impact of rheumatoid arthritis on life activities. Arthritis Care Res.. 1995;8(4):272-278.
Katz P., Pasch L., Wong B. Development of an instrument to measure disability in parenting activity among women with rheumatoid arthritis. Arthritis Care Res.. 2003;48(4):935-943.
Kielhofner G. A Model of Human Occupation: Theory and application, third ed. Baltimore: Lippincott, Williams & Wilkins; 2002.
Law M., Baptiste S., McColl M.A., et al. The canadian occupational performance measure: an outcome measure for occupational therapy. Can. J. Occup. Ther.. 1990;57(2):82-87.
Law M., Baptiste S., Carswell A., et al. Canadian Occupational Performance Measure, fourth ed. Ottawa, ON: CAOT Publications; 2005.
Macedo, A.M., Oakley, S., Panayi, G.S., et al., 2007. Functional and work outcomes improve in RA patientswho receive timely comprehensive occupational therapy. ACR Annu. Meet. http://www.rheumatology.org/annual/07wrapup.asp abstract 338. Accessed 13.1.09
Madill H., Townsend E., Schultz P. Implementing a health promotion strategy in occupational therapy education and practice. Can J. Occup. Ther.. 1989;56(2):67-72.
Meenan R.F., Mason J.H., Anderson J.J., et al. AIMS 2: the content and properties of a revised and expanded Arthritis Impact Measurement Scales health status questionnaire. Arthritis Rheum.. 1992;35(1):1-10.
Melvin J., Jensen G. Rheumatologic Rehabilitation Series: Vol 1 Assessment and Management. Bethesda, MD: American Occupational Therapy Association. 1998.
National Rheumatoid Arthritis Society. I Want to Work: a self-help guide for people with Rheumatoid Arthritis. Berkshire: National Rheumatoid Arthritis Society; 2007.
National Rheumatoid Arthritis Society. I Want to Work: Employment and Rheumatoid Arthritis. A National Survey. High Wycombe: National Rheumatoid Arthritis Society; 2007.
Nordenskiold U. Elastic wrist orthoses: reduction of pain and increase in grip force for women with rheumatoid arthritis. Arthritis Care Res.. 1990;3:158-162.
Nordenskiold U. Evaluation of assistive devices after a course in joint protection. Int. J. Technol. Assess. Health Care. 1994;10:293-304.
Nordmark B., Blomqvist P., Andersson B., et al. A 2-year follow up of work capacity in early rheumatoid arthritis: a study of multidisciplinary team care with emphasis on vocational support. Scand. J. Rheumatol.. 2006;35(1):7-14.
O’Brien A.V., Jones P., Mullis R., et al. Conservative hand therapy treatments in rheumatoid arthritis. A randomised controlled trial. Rheumatology. 2006;45(5):577-583.
Pagnotta A., Baron M., Korner-Bitensky N. The effect of a static wrist orthosis on hand function in individuals with rheumatoid arthritis. J. Rheumatol.. 1998;25:879-885.
Palchik N.S., Mitchell D.M., Gilbert N.L., et al. Non- surgical management of the boutonniere deformity. Arthritis Care Res.. 1990;3:227-232.
Plasqui G. The role of physical activity in rheumatoid arthritis. Physiol. Behav.. 2008;94(2):270-275.
Puolakka K., Kautiainen H., Möttönen T., et al. Impact of initial aggressive drug treatment with a combination of disease-modifying anti-rheumatic drugs on the development of work disability in early rheumatoid arthritis: a five-year randomized follow-up trial. Arthritis Rheum.. 2004;50(1):55-62.
Rogers J., Holmes D. Assistive technology device use in patients with rheumatic disease: a literature review. Am. J. Occup. Ther.. 1992;46(2):120-127.
Scherer M. The change in emphasis from people to person: introduction to the special issue on assistive technology. Disabil. Rehabil.. 2002;24(1,2,3):1-4.
Sokka T., Krishnan E., Hakkinen A., et al. Functional disability in rheumatoid arthritis patients compared with a community population in Finland. Arthritis Rheum.. 2003;48(1):59-63.
Stern E.B., Ytterberg S.R., Krug H.E., Mahowald M.L. Finger dexterity and hand function: effect of three commercial wrist extensor orthoses on patients with rheumatoid arthritis. Arthritis Care Res.. 1996;9(3):197-205.
Steultjens, E.M.J., Dekker, J., Bouter, L.M., et al., 2004. Occupational therapy for rheumatoid arthritis. Cochrane Database of Systematic Reviews Issue 1 Art. No.: CD003114. DOI: 10.1002/14651858.CD003114.pub2.
Symmons D., Silman A. Aspects of early arthritis. What determines the evolution of early undifferentiated arthritis and rheumatoid arthritis? An update from the Norfolk Arthritis Register. Curr. Opin. Rheumatol.. 2006;19(2):204-231.
Ter Schegget M.J., Knipping A.A. The swan-neck splint in rheumatoid arthritis. Ned Tijdschr. Ergotherapie. 1997;25:172-182.
Tijhuis G.J., Vlieland T.P.M., Zwinderman A.H., et al. A comparison of the Futuro wrist orthosis with a synthetic ThermoLyn Orthosis:utility and clinical effectiveness. Arthritis Care Res.. 1998;11(3):217-222.
Turner H., Chapman S., McSherry A., et al. Leisure assessment in occupational therapy: an exploratory study. Occup. Ther. Health Care. 2000;12:73-85.
Tugwell P., Bombardier C., Buchanan W., et al. The MACTAR Patient Preference Disability Questionnaire: an individualised functional priority approach for assessing improvement in clinical trials in rheumatoid arthritis. J. Rheumatol.. 1987;14:446-451.
US Department of Labor Employment and Training Administration. The Revised Handbook for Analysing Jobs. Indianapolis: Jist Works; 1991.
Valpar International Corporation. Valpar Profile Analysis Guide. Arizona: Valpar International Corporation Tucson; 2007.
Valpar International Corporation. Valpar Component Work Samples. Arizona: Valpar International Corporation Tucson; 2007.
Velozo C., Kielhofner G., Gern A., et al. Worker role interview: toward validation of a psychosocial work-related measure. J. Occup. Rehabil.. 1999;9(3):153-168.
Wielandt T., Strong J. Compliance with prescribed adaptive equipment: a literature review. Br. J. Occup. Ther.. 2000;63(2):65-75.
Winchcombe M., Ballinger C. A Competence Framework for Trusted Assessors. Assist UK; 2005.
Wikstrom I., Book C., Jacobsson L.T.H. Difficulties in performing leisure activities among persons with newly diagnosed rheumatoid arthritis: a prospective, controlled study. Rheumatology. 2006;45(9):1162-1166.
Wolfe F. A reappraisal of HAQ disability in rheumatoid arthritis. Arthritis Rheum.. 2000;43(12):2751-2761.
World Health Organisation. International Classification of Functioning Disability and Health. Geneva: WHO; 2001. www.who.int
Yelin, E., Trupin, L., Katz, P., 2004. Presentation: Work disability and SLE: Incidence and correlates. New York, NY: 7th International Congress on Systemic Lupus Erythematosus and Related Conditions: Session on long-term outcome: heart and vessels May 9-13 Abstract 23A www.medscape.com. Accessed 15/08/08.
Yelin E., Lubeck D., Holman H., et al. The impact of rheumatoid arthritis and osteoarthritis: the activities of patients with rheumatoid arthritis and osteoarthritis compared to controls. J. Rheumatol.. 1987;14(4):710-717.
Young A., Dixey J., Cox N., et al. How does functional disability in early rheumatoid arthritis (RA) affect patients and their lives? Results of 5 years of follow-up in 732 patients from the early RA Study (ERAS). Rheumatology. 2000;39(6):603-611.