5 Flea allergic dermatitis
INTRODUCTION
In some parts of the world, flea allergic dermatitis (FAD) is the most common allergic disease and a major cause of pruritus in dogs and cats. In other parts it is a significant problem only at certain times of the year. Although allergic dermatitis is the main condition associated with fleas, a distinction between pruritus resulting from severe flea infestation and a hypersensitivity response should be made. In very young puppies and kittens, severe flea infestations provoke varying degree of pruritus, but more often patients exhibit signs of weakness, lethargy and anaemia. Fleas are also vectors of infectious organisms such as Bartonella, Rickettsia felis and Haemoplasma spp.
CASE HISTORY
This varies between individuals but most pruritic dogs are presented with a history of pruritus and varying lesions affecting the lumbo-sacral region. As the flea life cycle is affected by environmental factors such as temperature and humidity, seasonal exacerbations may occur. Often flea control is only intermittently used and in-contact animals, especially cats, are inadequately treated. The history in this particular case was long and complex. The most relevant parts were:
CLINICAL EXAMINATION
A whole range of clinical signs, from primary lesions such as papules and pustules, to severe secondary hyperpigmentation, lichenification and fibropruritic nodules are seen, depending on the chronicity of the disease. Self-induced alopecia due to over-grooming and secondary bacterial infection is often seen in affected dogs. Atopic dogs are predisposed to flea bite hypersensitivity, even those that have been well managed. Some dogs will present with pyotraumatic dermatitis on the rump, or at other sites.
The clinical findings in this case were:





In this case, given the clinical signs and the distribution of the lesions, there was evidence for more than one type of hypersensitivity. The facial, pedal and ventral distribution suggested atopic dermatitis, and that affecting the dorsal aspect, flea allergy dermatitis. A concurrent adverse food reaction could also have been contributing to the pruritus. The other differentials included:
CASE WORK-UP
A number of the differential diagnoses were ruled out with simple in-house tests:
In addition to atopic dermatitis, the history, clinical signs and distribution of lesions were suggestive of flea allergic dermatitis. The diagnosis of flea allergy dermatitis is supported with additional tests and with response to aggressive flea control. The simplest test is the demonstration of fleas or flea faeces using a flea comb; however, about a third of animals fail to show any evidence of fleas, for various reasons:
In these cases further diagnostic tests may be of value; however, it is important to remember their limitations and ultimately a positive response to aggressive flea control is needed to confirm the diagnosis.
In vitro testing: In this case an in vitro Allercept IgE ELISA test using recombinant flea saliva revealed a markedly elevated flea allergen specific IgE concentration, which was consistent with flea allergy dermatitis and suggested current flea exposure. However, the specificity and the sensitivity of the testing are variable, and the test does not recognize those animals with cell-mediated hypersensitivity immune responses. It is useful as a diagnostic aid but a negative test should not necessarily rule out FAD. It is estimated that about 15–30% of individuals may show just cell-mediated immune responses. In addition, a serum IgE test for other allergens was performed (see Chapter 3) to assess the role of environmental allergens. This revealed high levels of IgE to house dust and storage mite allergens.
Intradermal testing: Intradermal testing with whole-body flea antigen or flea saliva may also support the diagnosis. This test produces immediate reactions (15–30 minutes), or late-phase reactions (4–6 hours) or delayed reactions (24–48 hours) to specific antigens injected intradermally. The test site should be examined at the appropriate times. Late-phase and delayed-type reactions are recognized either by an erythematous ring at the site of injection and/or a raised wheal. In this case this test was not deemed to be suitable for either flea antigen or other environmental allergens, because the last injection of methylprednisolone acetate had been given only 2 months prior to the initial examination by the dermatologist. The duration of action of this drug is anything between 4 and 6 weeks, and varies between individuals. Ideally, intradermal testing should be carried out not less than 12 weeks after the injection of a reposital glucocorticoid.
DIAGNOSIS
The diagnosis in this case was that of bacterial pyoderma, flea allergic dermatitis and atopic dermatitis.
PROGNOSIS
The long-term prognosis was good, provided the owner was able to maintain thorough long-term flea control on all the animals in the house and it was possible to effectively manage the concurrent atopic dermatitis. There may be flare-ups from time to time depending on the allergen load.
AETIOPATHOGENESIS OF FLEA ALLERGIC DERMATITIS
Although most cats and dogs have fleas at some point or other, not all develop clinical signs associated with hypersensitivity and it is probable that those that don’t are not sensitized to the flea saliva. However, exposure, either intermittent or continuous, to flea bites is a predisposing factor in the development of the allergic response, as is atopic dermatitis. Sensitization can occur at any age and is usually lifelong.
Several allergenic proteins identified in flea saliva can result in an individual becoming sensitized. The proteins range from 12 to 50 kDa in molecular weight. Three types of allergic responses – immediate, late-phase and delayed-type responses – have been identified.
EPIDEMIOLOGY
There is no sex predisposition and sensitization can occur at any age, but appears to be seen mainly in older animals. Intermittent exposure is associated with increased sensitization, whereas continuous exposure may result in some tolerance.
The incidence of the disease is dependent on the presence of environmental conditions in which the fleas are likely to thrive and perpetuate. An ambient temperature of 18–30ºC and high relative humidity of between 70% and 80% favours flea reproduction and survival; however, the flea’s biology is such that it ensures its own and/or its intermediate stages’ survival, even when the conditions are unfavourable. Although the flea itself is unable to survive cold temperatures, or high temperatures with low relative humidity, the pupal stage (Fig. 5.6) is able to endure them for up to 300 days. Then, when appropriate environmental conditions are encountered (see below), the adult flea emerges. The flea life cycle from egg to adulthood can therefore vary from 15 to 300 days depending on the environmental conditions.
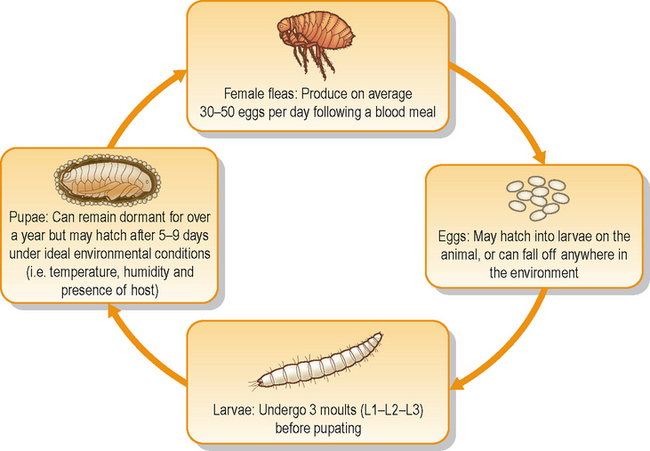
The cat flea, Ctenocephalides felis felis, is the main species implicated in flea allergic dogs and cats. Ctenocephalides canis is also reported in some countries. Less commonly, flea species that normally infest other mammals and birds may be involved (Table 5.1). The female adult flea is an obligate parasite and needs a blood meal in order to produce eggs and, if the conditions on the host are ideal, it can lay up to 30–50 eggs a day. Feeding fleas can live up to 100 days and lay as many as 2000 eggs in their lifetime.
Table 5.1 Flea species and their main hosts
| Flea species | Natural host |
|---|---|
| Ctenocephalides felis felis | Cats and dogs |
| Ctenocephalides canis | Dogs and cats |
| Pulex spp. | Humans |
| Echnidophaga galinacea | Birds |
| Spilopsysllus cuniculi | Rabbits |
| Archaeopyslla erinacei | Hedgehogs |
| Xenopsylla spp. | Small mammals |
Fleas do not jump on and off animals, but tend to live on the host. The eggs fall into the animals’ environment during grooming or scratching, as they are non-adherent. The eggs hatch into the first larval stage, which burrow deep into crevices, carpet pile, etc., as they are photophobic and geotrophic. This stage feeds on flea faecal pellets and other organic debris in the environment. There are three larval stages and the third stage transforms into the pupa. This stage is a cocooned pre-emerged flea which is protected from environmental insults (including parasiticidal agents) and will only emerge if conditions ensure that its survival is more or less guaranteed by the presence of a host. These conditions include carbon dioxide, warmth and air movements, which indicate the presence of a host.
TREATMENT OPTIONS
Multiple therapies are usually required in the early stages of treatment of flea allergy dermatitis. They include those that limit pruritus, deal with any secondary infections and those that specifically kill the flea and its intermediate stages, both on the animal and in the environment.
Flea control: Both the treatment of all animals in the house and that of the environment should go hand in hand, at least during the initial stages. The treatment should be tailored to suit each case, depending on the number of animals within the household, the ability of the owner to use the products as indicated and the cost.
Fipronil: Fipronil belongs to the phenylpyrazole family and its mode of action is by blocking the pre- and postsynaptic transfer of chloride ions through the cell membrane, thus acting as an insect GABA antagonist. It has both insecticidal and acaricidal activity. It is available in spray and spot-on formulations and kills fleas within 24 hours, and tick and other insects within 48 hours. It is combined with s-methoprene, an insect growth regulator which inhibits the development of immature stages by mimicking the juvenile hormone.
Nitenpyram: Nitenpyram is used as a fast-acting, orally administered insecticide, which kills fleas on the animal as soon as 15 minutes after administration and has an efficacy of up to 100% kill within 24 hours. It acts by inhibiting specific nicotinic acetylcholine receptors. It is a useful product to achieve quick kill in cases such as this one, but is not designed to be used on its own. It can, however, be combined with lufenuron to provide integrated flea control.
Imidacloprid: Imidacloprid belongs to the group of chloronicotinyl compounds. Its mode of action is to bind to the nicotinergic acetylcholine receptors on the postsynaptic region of the insect nervous system, thereby stopping the acetylcholine from binding to the receptors. This results in the paralysis and death of the insect. Imidacloprid is effective against adult fleas as well as larval flea stages. It is available as a spot-on formulation and the label permits weekly use of this product.
Selamectin: Selamectin is a semi-synthetic avermectin with a broad spectrum of activity against endoparasites as well as ectoparasites. It is an adulticide with larvicidal and ovicidal properties. The product is absorbed percutaneously and then redistributed back to the cutaneous tissue via the circulation.
Metaflumizone: Metaflumizone belongs to the semicarbozone group of compounds and is available as a spot-on treatment against fleas. It is a sodium channel blocker which prevents the flow of sodium ions across the nerve cell membrane. This disrupts the transmission of nerve impulses and the eventual result is death by paralysis. For use in dogs, it is combined with amitraz to provide action against fleas and ticks. On its own, it is available for use in cats.
Pyriprole: Pyriprole belongs to the phenylpyrazole group of compounds. It is a spot-on formulation that has both insecticidal and acaricidal activity and its mode of action is similar to that of fipronil (see above). It is licensed for use against fleas and ticks in dogs only.
Pyrethrins: Pyrethrins are naturally occurring flea repellents and pyrethroids synthetic ones. A combination of permethrin, a pyrethroid and imidacloprid has a veterinary licence for use in dogs (contraindicated in cats).
Environmental control
Insect growth regulators: Insect growth regulators such as fenoxycarb, methoprene and pyriproxyfen are analogues of the juvenile hormone, which allows pupation when its concentration falls. Excessive concentrations prevent metamorphosis and thereby break the life cycle. These products are available as environmental aerosol sprays combined with an adulticide for effective control and in the case of methoprene as a spot-on treatment for the animal combined with fipronil.
Insect growth inhibitors such as lufenuron inhibit the synthesis of chitin, thus preventing successive larval moults.
Summary of environmental treatment: Aerosol sprays, pump sprays and foggers are available, which generally contain permethrin plus an insect growth inhibitor or regulator.
Treatment in this case
In this case the long-term treatment also included allergen-specific immunotherapy for the management of the atopic dermatitis.
Many clients will discuss their concerns with the nurse, or lay staff, rather than the vet. They should be able, tactfully, to reassure them and give them the correct advice. A good grasp of the flea life cycle, together with knowledge of the range of flea products on the veterinary market and their modes of action, is the key to giving correct advice to the client. Flea control within an individual household should be tailored to its needs. Many owners who are registered with the practice will call in to buy products during the summer months when the problem is most apparent. It is at this point, when they recognize the problem, that the client is most receptive to advice on supplementing topical therapy with environmental treatment.
The environment was treated twice 2 weeks apart with a spray containing permethrin and methoprene. The cats and the dog were treated with a spot-on solution containing fipronil and methoprene every 2 weeks for four occasions (extra-label use), then every 3–4 weeks. At the start of the treatment, all the animals (three in-contact cats and the dog) were given 3 days of nitenpyram orally to ensure quick kill and reduction in the flea population as soon as possible.
Antibiotic treatment: In this case cefalexin (15 mg/kg b.i.d.) was prescribed for 3 weeks, without any antipruritic treatment. At the end of the course, clinical examination and tape-strip preparations did not reveal any bacteria and antipruritic treatment was started (see below).
Antipruritic treatment: Given the severe pruritus and its effects on the animal’s welfare, 1 mg/kg every 24 hours of prednisolone was prescribed for 7 days, after which it was reduced to alternate-day treatment. After 4 weeks it was reduced to 0.5 mg/kg on alternate days and stopped once the dog reached the maintenance phase of the allergen-specific immunotherapy.
FOLLOW-UP
Long-term flea control was maintained on all the animals in the household. The pedal pruritus persisted even after 1 year on allergen-specific immunotherapy and so 0.1 mg/kg of prednisolone was administered as a concurrent treatment. The dog has been successfully managed on this combination at the time of writing. It is possible that this dog has a concurrent adverse food reaction as well, but the owner was unwilling to repeat a diet trial.