12 Introduction to crusting and scaling
The outermost layer of the skin, the epidermis, is made up of multiple layers of cells (Fig. 12.1). The predominant cell type is the keratinocyte, and the epidermis is divided into basal, spinous, granular (variably present in dogs and cats) and cornified layers depending on the morphological features keratinocytes assume as they undergo progressive differentiation to form the stratum corneum.
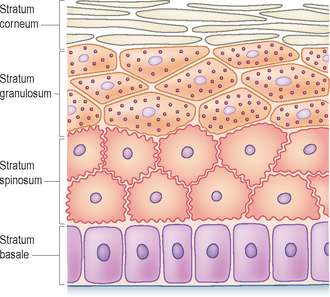
Under normal circumstances, the epidermis is replaced every 3–4 weeks. The process of keratinocyte migration and differentiation is complex and carefully controlled. Daughter keratinocytes produced by stem cells of the basal layer of the epidermis travel up through the various layers of the epidermis and undergo a process of maturation and differentiation. The end products of this process are fully keratinized corneocytes, the cells that make up the stratum corneum. The cornified cell is packed with filamentous proteins; it normally does not have a nucleus and is imperceptibly shed from the surface of the stratum corneum, either as an individual cell or as small clusters of cells not visible to the naked eye. This desquamation process is the result of enzymatic breakdown of both the desmosomes (the small connections that bind the cells together) and the intercellular lipid ‘glue’ (present in the stratum corneum).
SCALING
Scaling is the visible accumulation of flakes of stratum corneum on the skin surface or in the hair coat, and can occur for many different reasons. Scale varies in colour and consistency, and may be white, silver, yellow or brown to grey. Scale may be branny, fine, powdery, flaky, greasy, dry, loose, adherent or ‘nit-like’. Scaling may be focal, multifocal or diffuse in distribution.
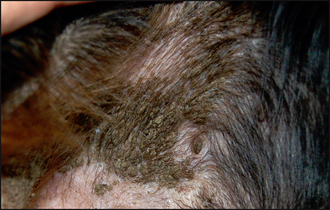
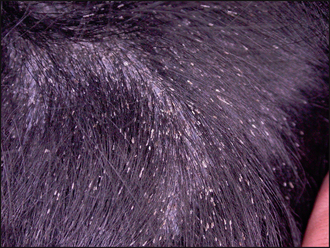
Many diseases affect the normal maturation, differentiation and desquamation processes, and can result in scaling. The appearance and distribution of the scale varies depending on the causative disease. Diffuse dorsal scaling is seen in association with pruritus as a result of cheyletiellosis (see Chapter 5). Another common cause of scaling with a multifocal distribution is as a result of epidermal collarette formation. These are circular rims of scale that are the remains of pustules after they have ruptured (Fig. 12.2). Diseases associated with epidermal collarettes include pyoderma, demodicosis, dermatophytosis and pemphigus foliaceus. Multifocal patches of scaling evident over the dorsal trunk commonly arise from sites of pyoderma and are due to the formation of epidermal collarettes. Tightly adherent patches of scale which are difficult to remove are seen in some forms of ichthyosis, a rare, congenital disorder occurring mainly in young dogs associated with a failure of breakdown of intercorneocyte adhesion (Fig. 12.3). Follicular casts, nit-like accumulations of scale surrounding hair shafts, are representative of hair follicle pathology and are seen in follicular diseases such as sebaceous adenitis and vitamin A-responsive dermatitis (Fig. 12.4).

After an insult, one of the defence and repair mechanisms of the skin is to increase the rate of production of keratinocytes, so that all the layers of the epidermis become thicker. There may then be increased and abnormal desquamation of larger clusters of corneocytes that become visible to the naked eye as scale. In this altered process of keratinization the corneocytes may retain their nuclei. This is known as parakeratosis, a more primitive pattern of cornification (the initial stratum corneum in foetal skin is parakeratotic). Some metabolic diseases, including zinc-responsive dermatosis, necrolytic migratory erythema and lethal acrodermatitis of bull terriers, result in thickening of the stratum corneum with marked confluent layers of parakeratotic corneocytes (parakeratotic hyperkeratosis) and resultant visible adherent scale.
CRUST
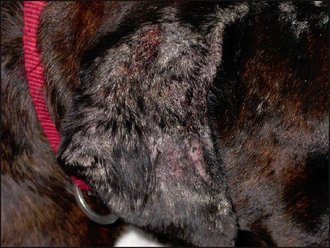
Crust is formed from the accumulation of dried serum, pus or haemorrhage, along with hair, cells and sometimes medication, on the skin surface. Crust is representative of a breach of epithelial integrity and there are many diseases that can result in its formation, including vesicular, pustular, erosive or ulcerative disorders. Serous crusts tend to be yellow or honey coloured and may be seen in excoriation due to self-trauma and in scabies (Fig. 12.5). Crust formed from pus tends to be yellow to brown, or green, in colour. Pustular diseases such as pyoderma and pemphigus foliaceus produce focal, often circular, crusts, the crust forming from the pustule contents after it ruptures (Figs 12.6 and 12.7). Dark brown- or red-coloured crusts tend to have a large component of blood within them and would be indicative of deeper tissue damage. German shepherd pyoderma (Fig. 12.8), a particularly severe form of deep pyoderma, and vasculitis (Fig. 12.9) are examples of diseases that may result in the formation of haemorrhagic crusts. Tightly adherent crusts are characteristic of zinc-responsive dermatosis and necrolytic migratory erythema (Fig. 12.10).