13 Sebaceous adenitis
INTRODUCTION
Sebaceous adenitis is a scaling, variably pruritic skin disorder of uncertain aetiology. The disease results in the inflammation and destruction of sebaceous glands, follicular hyperkeratosis and commonly, secondary pyoderma. Grossly, the disease results in a scaling skin disorder associated with follicular cast formation and variable alopecia.
CASE HISTORY
There are marked breed variations in the way sebaceous adenitis presents, but typically the owner will report a gradual onset of skin lesions with variable scaling, alopecia and pruritus. The head and pinnae are often the first areas to be affected. The earlier signs of the disease may go relatively unnoticed and the dog may be presented with more severe lesions due to secondary pyoderma. There are no systemic signs associated with the disease.
The relevant history in this case was as follows:
CLINICAL EXAMINATION
There are substantial variations in the clinical appearance of sebaceous adenitis between breeds.
Longer-haired dogs present with variable scaling, alopecia and usually marked follicular cast formation (Fig. 12.4), and a fine silvery scale on the inner aspects of the pinnae is commonly seen in springer spaniels. Lesions can progress to large patches of broken hairs and tightly adherent scale. The pinnae, trunk, temporal region and tail tend to be affected in the early stages, but severe disease can result in generalized involvement.
In short-haired dogs such as the Hungarian viszla, lesions consist of focal, coalescing, annular plaques of scaling and partial alopecia.
Feline sebaceous adenitis is a rare disease characterized by multifocal annular areas of alopecia, scaling, crusting and follicular casts. Pruritus can be absent to marked, and tends to be more severe if there is secondary pyoderma.
The physical examination was within normal limits.
Examination of the skin revealed:

Figure 13.1 Sebaceous adenitis. Alopecia over the periorbital skin and adjacent to the nasal planum.


Figure 13.3 Sebaceous adenitis resulting in partial alopecia and discolouration due to follicular cast formation.
This was a diffuse, partial alopecia involving scaling and follicular cast formation. Follicular casts are made up of keratosebaceous material, and are literally a cast of the hair follicle lumen that forms a collar around the hair shaft and is extruded from the hair follicle as the hair grows (see Chapter 12). They represent follicular pathology, in particular follicular hyperkeratosis.
There are several diseases that can result in follicular cast formation and alopecia, including:
CASE WORK-UP
The definitive diagnosis of sebaceous adenitis is made on histopathological examination, but skin scrapes, fungal culture and trichographic examination were also indicated.
The following diagnostic tests were performed:
DIAGNOSIS
The history, clinical signs and histopathological examination were consistent with a diagnosis of sebaceous adenitis.
PROGNOSIS
Sebaceous adenitis is an incurable disease that is likely to require lifelong management. In most cases, the symptoms can be satisfactorily controlled. Although dogs experience pruritus that can affect quality of life, there is no systemic involvement. The disease does have a tendency to wax and wane, and interpretation of any apparent response to treatment should be made with this in mind.
ANATOMY AND PHYSIOLOGY REFRESHER
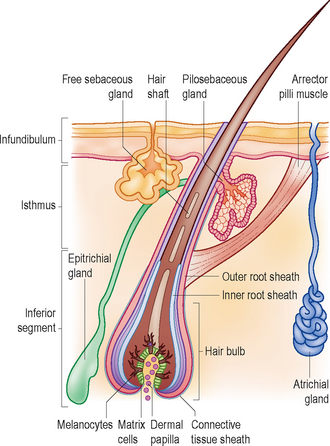
Sebaceous glands are alveolar glands that open and secrete their contents into the hair follicle infundibulum by way of the pilosebaceous duct (Fig. 13.4). They secrete a mixture of lipids, known as sebum, into the follicular lumen. This mixture coats the hair shaft and exits from the opening of the follicle onto the stratum corneum, where it comprises the most abundant lipids present on the skin surface. Sebum forms a surface emulsion with secretions from atrichial sweat glands that spreads over the skin surface, keeping it soft and pliable. It also spreads over hair shafts and gives the hair coat a glossy sheen. The fact that the pilosebaceous duct opens into the hair follicle at the base of the infundibulum (rather than near the surface of the skin) suggests that sebum may also have a role within the hair follicle, as well as on the surface of the epidermis. Diseases in which sebaceous glands are absent are associated with keratin plugging of the follicular infundibulum. In dogs with sebaceous adenitis, the lack of lubrication results in infundibular cornified material becoming attached to the exiting hair shaft, thus forming the distinctive follicular cast.
It has been suggested that sebaceous adenitis is the result of an immune-mediated pathogenesis resulting in inflammation and destruction of sebaceous glands. However, other possible causes include a hereditary and developmental inflammatory destruction of sebaceous glands, a cornification abnormality leading to sebaceous duct and sebaceous gland inflammation and atrophy, and an anatomical defect in sebaceous glands leading to lipid leakage and a resulting foreign body response. Indeed, the variable clinical appearance between breeds could suggest differing underlying aetiologies.
EPIDEMIOLOGY
There are strong breed predilections for sebaceous adenitis in the standard poodle, Hungarian viszla, Japanese akita, samoyed and English springer spaniel. This suggests a genetic basis for the disease, and an autosomal recessive mode of inheritance has been proposed in the standard poodle. Interestingly, sebaceous adenitis seems to be commonly recognized in the English springer spaniel in the UK but not in the USA. The disease is most frequently seen in young adults, but there are no sex predilections.
TREATMENT OPTIONS
Therapy is aimed at treating pyoderma, minimizing the inflammatory response directed towards the sebaceous glands, rehydration of the skin and reduction of scaling. The response to therapy tends to vary between breeds, and perhaps depends on the severity and duration of the disease. As already stated, the tendency for the symptoms to spontaneously wax and wane further complicates the assessment of efficacy.
A number of different treatments have been reported to be of value in sebaceous adenitis.
Antibacterial therapy: If there is evidence of pyoderma, a minimum of 3 weeks of systemic antibacterial therapy is indicated, which may result in significant clinical improvement.
Topical therapy: Shampoos containing sulphur and/or salicylic acid help to reduce scaling. Initially, treatments should be two or three times weekly, reducing to once weekly for maintenance therapy. The shampoo should be followed by thorough rinsing in clean water and a final humectant rinse. Humectants moisturize the stratum corneum by absorbing water. Propylene glycol has both antiseborrhoeic and humectant properties. There are commercially available preparations containing propylene glycol that can be applied as a final rinse following shampoo treatment, or as a spray that may be applied daily to the skin.
Essential fatty acid supplements: Essential fatty acid (EFA) supplementation of omega-6 and omega-3 fatty acids has been reported to be of variable value in the treatment of sebaceous adenitis; it is usually combined with the use of topical therapy. The mode of action is unclear, but EFAs have mild anti-inflammatory actions and they may also be of benefit in the replacement of fatty acids in the skin and hair coat. The author’s preferred initial treatment for sebaceous adenitis is to start topical treatment as described above in conjunction with EFA supplementation.
Vitamin A and retinoids: Vitamin A and synthetic retinoids regulate the growth and differentiation of epithelial tissues and have effects on keratinocytes. They have antiproliferative, anti-inflammatory and immunomodulatory properties, and have been shown to be useful in the treatment of sebaceous adenitis.
Reported dosages for vitamin A are somewhat empirical, but it is most commonly used at a dosage of 1000 IU/kg q24 h. A dose rate of 10 000 IU b.i.d. per dog has also been used and this was increased to 20–30 000 IU b.i.d. in cases that did not respond satisfactorily. Reported response rates were that 80% of dogs showed an improvement within 3 months.
Isotretinoin is a synthetic retinoid and is effective for the treatment of some cases of canine sebaceous adenitis at a dosage of 1–3 mg/kg q24 h. Around 50% of cases can be expected to benefit with reduced scaling and hair regrowth. One drawback in the use of synthetic retinoids is their expense.
Vitamin A and synthetic retinoids have numerous side-effects in man, including teratogenicity, cheilitis, inflammation and xerosis of the skin, decreased tear production, hepatotoxicity and hyperlipidaemia. The incidence of side-effects in the dog appears to be low, but routine biochemistry including triglycerides, and a Schirmer tear test, should be performed prior to starting therapy. Biochemistry should be repeated 1 and 2 months after starting treatment, and tear production should be monitored monthly for the first 6 months. These tests should then be repeated every 6–12 months. Both high-dose vitamin A and isotretinoin are highly teratogenic and their use should be avoided in any dogs intended for breeding, because as well as being teratogenic, they can also result in decreased spermatogenesis. Clients should be warned of the risk of accidental ingestion of these drugs and, clearly, great care must be taken by women of child-bearing age in the handling of synthetic retinoids.
Corticosteroids: Some texts have reported that corticosteroids are of no value in the treatment of sebaceous adenitis, but the author’s experience is that at anti-inflammatory doses of 0.5–1.0 mg/kg they can be helpful in the management of some cases.
Ciclosporin: Ciclosporin at a dosage of 5 mg/kg has been a useful therapy for the treatment of canine and feline sebaceous adenitis. Treatment in dogs was associated with apparent regeneration of sebaceous glands. In the UK this is an unlicensed use for this drug, and in view of its expense and potent immunosuppressive effects, it should not be considered a first-line treatment. The efficacy of ciclosporin probably stems from the fact that, as well as its anti-inflammatory and immunomodulatory effects, it also stimulates hair growth by inducing anagen.
Treatment in this case: Initial treatment consisted of clindamycin at a dosage of 10 mg/kg b.i.d. for 3 weeks, supplemented with daily essential fatty acid supplements, three times weekly salicylic acid shampoos and daily propylene glycol sprays. The essential fatty acid supplements and topical therapies were continued for 3 months.
Re-examination after 3 months of topical therapy revealed further hair loss and the persistence of scaling and follicular cast formation over the pinnal margins, face and tail. At this point, systemic vitamin A therapy was introduced at a dosage of 1000 IU/kg q24 h. Prior to starting the treatment, a Schirmer tear test and full haematological and biochemical examinations were performed.
After 12 weeks of vitamin A therapy there was reduction in scaling and some hair regrowth over the tail. A repeat Schirmer tear test showed a marked decrease in tear production and the vitamin A therapy was discontinued. The tear production subsequently recovered to pretreatment levels.
After discussion with the owner, the dog was started on ciclosporin therapy at a dosage of 5 mg/kg s.i.d. The essential fatty acid supplements, salicylic acid shampoos and propylene glycol sprays were continued.
Six months after starting the ciclosporin therapy, there was excellent regrowth of hair over all previously affected areas (Fig. 13.5).

As with all histopathological examination, it is important to take sufficient samples so that many adnexal structures may be observed. If the histopathologist is able to observe inflammation directly targeting the sebaceous gland, then the diagnosis is straightforward. However, in longer-standing cases, there may be a complete absence of sebaceous glands without inflammation in most sections, and many sections need to be examined to confirm that the absence of glands is widespread before being able to confirm the diagnosis. Thus, it is advisable to submit four or five punch biopsy samples from different areas of skin, even if the lesions in different areas appear similar.
When applied as a spray or mist, large volumes of propylene glycol are required to treat large-breed dogs with sebaceous adenitis. Propylene glycol is available in bulk quantities from veterinary wholesalers, and this product may be safely used diluted 50 : 50 with water and applied to the dog using a plant hand sprayer.
FOLLOW-UP
Ciclosporin was continued, but the frequency of ad-ministration of ciclosporin was gradually reduced to 50 mg every fourth day. The dog has been maintained on this dosage for 3 years, with no recurrence of disease. Although it was discussed, the owner was reluctant to withdraw therapy altogether in case of recrudescence.