Chapter 44 Practical radiation protection
Chapter contents
44.1 Aim
The aim of this chapter is to introduce the reader to the basic legal requirements for the safe use of ionizing radiation. This will cover the main documents involved in the UK and the basic organization of radiation safety in a hospital trust, and will then examine the practical ways in which these are implemented in radiology or radiotherapy departments.
44.2 Purpose and scope of radiation protection
Radiation dose rises from two sources: natural sources, which constitute the dose received by the whole population, and artificial sources. Radiation protection procedures can do little or nothing to reduce the dose from natural sources.
The principal component of radiation from artificial sources is received from exposure to radiation from medical sources. It follows from this that one of the basic tasks of radiation protection is to establish levels of risk to the population due from this source and then to take steps to keep these levels of risk from this source as low as possible.
The purpose of radiation protection in medicine is to produce and maintain an environment, both at work and in the outside world, where the levels of ionizing radiation from this source pose a minimal acceptable risk for human beings. Before beginning any discussion on radiation protection, it is important to realise that our environment can only be described as relatively safe from the effects of radiation from artificial sources.
Once the levels of risk from such radiation have been determined, appropriate dose-equivalent limits (see Sect. 44.6) may be set so that the risk associated with such radiations is no greater (and frequently is much less) than other aspects of life, e.g. the risk of injury as a result of a traffic accident. Establishing such dose-equivalent limits, and ensuring that staff work within these limits, helps to prevent suffering.
A full study of radiation protection would need to cover:
• statistical analysis of risk
• the fate and decay patterns of radioactivity released into the environment
• the absorbing power of different materials to different radiations.
Such a vast scope of study cannot be covered in a single chapter, or even in one book. Only a simplified review of practical methods of reducing radiation doses to radiation workers and their patients from the medical use of ionizing radiation will be considered here. These points are covered in the core of knowledge which all radiographic staff are expected to learn as part of their education. This consists of 11 key items as summarized in Table 44.1. Items 1–9 are of particular importance to the operator, while items 10 and 11 have particular reference to the role of the practitioner.
| 1 | Nature of ionizing radiation and its interaction with tissue |
| 2 | Genetic and somatic effects of ionizing radiation and how to assess these risks |
| 3 | The ranges of radiation dose given to a patient during the course of a particular procedure, the main factors affecting dose and methods of measuring dose |
| 4 | Principles of dose limitation and optimization |
| 5 | Principles of quality assurance applied to equipment and techniques |
| 6 | Specific requirements of children and of women who are or may be pregnant |
| 7 | Precautions necessary when handling sealed and unsealed radioactive sources |
| 8 | Organizational aspects of radiation protection and the procedure for suspected overexposure |
| 9 | Statutory responsibilities |
| 10 | Knowledge of the clinical value of the procedure requested, in relation to other available techniques |
| 11 | Importance of using radiological information, e.g. reports and images from a previous investigation |
44.3 Legal aspects
The legislation governing radiation is often confusing to the student. The International Commission for Radiation Protection (ICRP) has produced recommendations on radiation protection. These recommendations do not have the force of law. Laws based on these recommendations are then produced by the nations of the world.
In the European Union (EU), this is attained through directives, and all member states in the EU are required to implement these directives. In the UK, the following acts and regulations are concerned with radiation safety:
• Health and Safety at Work Act [HSW 1974].
• Ionizing Radiation Regulations [IRR 1999] Statuary Instrument 1999/3232.
• Radioactive Substances Act 1993 [RSA 1993].
• Ionizing Radiation (Medical Exposure) Regulations 2000 [IR (ME) R 2000] Statuary Instrument 2000/1059.
• Radioactive Substances (Hospitals) Exemption (Amendment) Order [RS (H) EO 1995].
• Ionizing Radiation (Medical Exposure) Regulations 2006 [IR (ME) R 2006] Statuary Instrument 2006/2523.
The inspectorate of the Health and Safety Executive (HSE) is responsible for ensuring that employers and employees comply with the above regulations. IRR 1999 applies to all radiation work and radiation workers in both the private and public sectors of the nuclear industry and those who may be affected by such work activities. In contrast, IR (ME) R 2000 applies whenever humans are irradiated for diagnostic, therapeutic, research or other medical or dental purposes, and where in-vitro medical tests are conducted. These regulations apply to staff, students, patients and their friends and relatives who are acting as comforters or carers, and to volunteers in research projects and members of the public. The above are all legal documents, and are often difficult for the layman to understand. ‘User friendly’ methods of meeting the requirements of these laws have been published as the Approved Codes of Practice and Guidance Notes. These do not have the force of law, but in a prosecution the defendant must be able to prove that their method of work is as good as, or better than, that recommended in the code or guidance notes.
44.3.1 Organization of radiation safety
The employer (e.g. the hospital trust) is ultimately responsible for maintaining radiation safety for staff, patients and others who may be affected by their work active activities. They have specific obligations under the regulations and meet these through a number of radiation safety experts:
• The Radiation Protection Adviser (RPA): an accredited, medically qualified physicist who is appointed by the employer to advise the employer on radiation safety and compliance with the regulations. This includes the production of local rules and written systems of work, the designation of work areas, the supervision of quality assurance programmes and acceptance testing of new equipment.
• The Radiation Protection Supervisor (RPS): every area of the trust in which ionizing radiation is used must have an RPS appointed by the employer. Each RPS must understand the specific requirements of radiation safety as applied to their area of work. Since the RPS is responsible to the employer for ensuring the safety measures are implemented and maintained, such individuals are usually departmental superintendants as they have the authority necessary to do this.
• The Radiation Safety Committee (RSC): this committee oversees all radiation safety issues, including research, and ensures that the reports of the RPA are implemented and radiation safety standards are maintained.
44.3.2 Responsibilities of the manufacturer
The manufacturers have obligations that are designed to improve the radiation protection offered by their equipment. These include such features as limiting radiation leakage from the X-ray tube so that it does not exceed 1 mSv.h−1 at a distance of 1 metre in any direction from the focus of the tube, the provision of suitable antiscatter protection, the use of low-absorption interspacing material in secondary radiation grids, the use of a high-output rectification system, provision of an automatic (preferably anatomically programmable) timer and ‘dead-man operation’ of exposure switching so that releasing the exposure switch during an exposure automatically terminates the exposure. If the equipment is capable of fluoroscopy, a pulsed fluoroscopy system must be used.
44.4 Dose-equivalent limits
Table 44.2 summarizes the dose-equivalent limits specified by the Ionizing Radiation Regulations 1999.
Table 44.2 Dose-equivalent limits (in mSv) per calendar year specified by Ionizing Radiation Regulations 1999
| CATEGORY OF PERSON | DOSE TO WHOLE BODY | DOSE TO LENS OF THE EYE | DOSE TO SKIN AVERAGED OVER AN AREA OF 1 CM2 | DOSE TO HANDS, FOREARMS, FEET AND ANKLES |
|---|---|---|---|---|
| Employee aged 18 or over | 20 | 50 | 500 | 500 |
| Trainees aged under 18 | 6 | 50 | 150 | 150 |
| General public | 1 | 15 | 50 | 50 |
| Comforter or carer: no dose limit, however the Health Protection Agency (HPA) (formerly the National Radiological Protection Board) recommends the dose should not exceed 25 mSv over a 5-year period or 5 mSv in a single exposure. | ||||
| Women of reproductive capacity who are at work: dose equivalent to the abdomen is 13 mSv in any 3-month period. The dose must not exceed 1 mSv from the date the conception is declared. | ||||
Note: These limits exclude any dose received from natural radiation sources or medical treatment of the individual concerned.
44.4.1 Designated radiation workers
If an employee is likely to receive a whole-body dose equivalent of ionizing radiation which exceeds 6 mSv per annum then that person must be designated as a classified radiation worker by the employer. A person who is a classified radiation worker must be subject to medical surveillance, with periodic reviews of health at least every 12 months.
It is not sufficient to rely on an individual’s history of doses received if they are less than the three-tenths limit. The potential doses which may be received in a set of circumstances must be assessed. The reason for designation may be that the individual works in controlled areas (see Sect. 44.5.1) but this is not, on its own, sufficient reason for designation. Even if the local rules (see Sect. 44.5), when strictly obeyed, indicate that doses in excess of the three-tenths limit will not occur, persons who work with radiation sources that are capable of producing an overdose in a few minutes will need to be classified.
The radiation dose which the classified person receives should be measured using a suitable personal dosimeter (see below) – the doses must be assessed by an approved dosimetry service on the basis of accepted national standards.
The above discussion does not mean that radiation workers who are not classified should not be monitored, but monitoring is a precaution and one which may be used to justify non-classified status, although there is no legal requirement for this.
44.4.2 Personnel dosimetry
The monitoring of radiation dose to staff is carried out by the use of thermoluminescent dosimeters (TLDs). The basic principles of thermoluminescence have already been discussed in Chapter 27. An example of a TLD badge and holder used for monitoring purposes is shown in Figure 44.1.
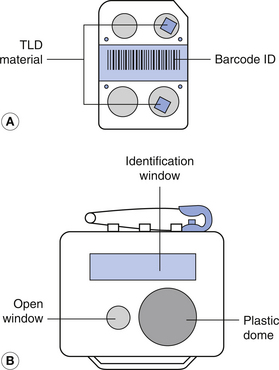
Figure 44.1 The thermoluminescent dosimeter badge as supplied by the Health Protection Agency (HPA; formerly the National Radiological Protection Board).
Figure 44.1A shows the plastic Harshaw card, without its Melinex wrapping (which has a number stamped on it in normal numbers). This wrapping protects the lithium fluoride/polytetrafluoroethylene (PTFE) TLD inserts on the card from light and alpha radiations, as well as providing chemical protection and a measure of physical protection. The card contains two discs of thermoluminescent material. One disc is positioned behind the open window of the badge while the other disc is behind the plastic dome. Note: the card is designed so that it can only be inserted into the holder in the correct way. Each card is identified by a unique barcode strip used in the automated dose-reading process.
The cardholder has two windows (Fig. 44.1B) – a long rectangular window along the top edge to display the wearer’s identity number and a circular open window that lies directly over one of the TLDs on the card. This TLD records all weak and strongly penetrating radiations, including beta radiation. This dose reading produces the Hp0.7 or whole-body dose. The other TLD lies under the dome, which is made of thick (90 mg.cm−2) plastic. This TLD is used to record the more penetrating and gamma radiations producing the Hp10 dose or depth received by the wearer.
Thermoluminescent materials may also be used to measure doses to specific organs, e.g. they can be wrapped round a finger to measure the dose to that finger.
The major disadvantage of TLDs is that they are retrospective monitors and are processed and read after exposure.
‘Real-time’ dosimeters (often called pocket dosimeters, because they can be worn in pockets of laboratory coats) can give an instant readout on a digital display. Some can provide additional data, such as a breakdown of the rate at which the dose was received, or even sound an audible alarm to indicate that radiation is being detected.
44.4.3 Employees who have been overexposed
If an employee’s annual whole-body dose exceeds 15 mSv, the RPA must notify the Health and Safety Executive (HSE) who will conduct an investigation to see if the working practices involved are in keeping with the ALARA (as low as reasonably achievable) principle (or whether improvements may be made which would lead to a reduction in the dose).
44.5 Local rules
Under IRR 1999, the employer has a legal responsibility to ensure that written local rules are produced for all departments (or areas) where employees are involved in work with ionizing radiation. These rules must be brought to the attention of all employees working in these departments. In practice, the RPA advises the employer on the formulation of these rules and it is the task of the RPS to ensure that the rules are known and put into practice by colleagues in their respective departments.
The local rules for a department should be displayed in a prominent position, or positions, within the department concerned, and should contain the following information:
• The names and contact details of the RPA and RPS for the department (or area).
• A description of each designated area in the department (see Sect. 44.5.1).
• Details of restrictions of access to such areas.
• Written systems of work detailing the procedures and protocols for the department.
44.5.1 Designated areas
There are two types of designated area (see Table 44.3): controlled and supervised areas. All designated areas must be delineated by physical boundaries, i.e. walls. However, in the case of radiography involving the use of mobile X-ray units, this requirement is dropped, provided that an area of at least 1.5 metres from the ray tube is under the continual supervision of the operator at all times. Warning signs must be posted at all entrances to the areas, preferably at eye level, and include a warning light to indicate if an X-ray unit is activated or an exposure is being made.
Table 44.3 Description of designated areas
| TYPE OF DESIGNATION | REQUIREMENTS FOR DESIGNATION | PERMITTED ACCESS |
|---|---|---|
| Controlled area | An area where any person is likely to receive an effective dose greater than 6 μSv per year or three-tenths of any relevant dose limit | A. Classified radiation workers |
| B. Radiation workers who follow a written system of work, designed to restrict significant radiation exposure in that area | ||
| C. Patients undergoing medical diagnostic or therapeutic exposures | ||
| Supervised area | A. An area where any person is likely to receive an effective dose greater than 1 mSv per year or one-tenth of any relevant dose limit | Persons whose presence is necessary during a radiation exposure |
| B. An area under review for upgrading to a controlled area | ||
| Note: a supervised area cannot be situated inside of a controlled area |
44.5.1.1 Design of designated areas
The function of the X-ray room is to provide an enclosure for the X-ray examination or treatment unit and limit access to the radiation area. It should also provide adequate shielding to the rest of the environment from the radiation produced, so that individuals outside the room do not receive a radiation dose that would exceed the annual effective dose limit to a member of the public. In diagnostic radiography, provision is made for a barrier inside the room behind which staff may be protected from the radiation while they operate the unit, while viewing the patient through a protective window. If there is more than one X-ray tube operating from the generator in a diagnostic room, there must be a visual indication (usually a warning light) to indicate which tube is in circuit and capable of producing radiation if energized. With radiotherapy treatment rooms, due to the much higher radiation energies used, the equipment is operated from outside the treatment room and the patient viewed through a closed-circuit TV system. Entry to the treatment area is through a maze and the entry of an individual into the maze during treatment automatically terminates the treatment.
The level of radiation protection given by barriers and walls is usually stated in terms of their lead-equivalent.
The lead-equivalent of an absorbing material is the thickness of lead which would absorb the same amount of radiation as the given material when exposed to radiation of the same type and quality.
The lead-equivalent gives a basis for comparing one barrier with another at a given beam energy.
In the diagnostic range of beam energies (up to 150 keV), the photoelectric absorption within lead is significant owing to its high atomic number (Z=82). For this reason, many barriers (e.g. doors) in the diagnostic X-ray room incorporate a few millimetres of lead laminated with wood to give adequate radiation protection. Lead-glass windows are often fitted to such barriers to enable a visual contact to be maintained. The protection afforded by such a window must be at least the same amount as the protective barrier itself and there must be no gaps where the radiation is able to penetrate. The siting of such a barrier to protect staff must be such that the radiation must be scattered at least twice (greatly reducing its intensity) before reaching the opening in the barrier.
Wall thicknesses between X-ray rooms and adjacent areas must be such that any transmitted radiation will not produce a dose in excess of 1 mSv per year, which is the maximum dose for the general public. This figure must be calculated for all walls, floors, ceilings and windows of the X-ray rooms and is calculated by applying a use factor. The use factor is an estimation of the time when the radiation beam will be pointing towards that area. As a result of this calculation, the maximum dose received by a person sited on the far side of the barrier may be estimated and it must not exceed 1 mSv per year. In previous legislation, there was also an occupancy factor, which looked at the fraction of time a person was likely to spend in this area, but this factor has now been discontinued.
The materials used in the construction of the walls and floor of the X-ray room may contain lead sheeting or there may be sufficient thickness of other materials, such as concrete, to provide adequate absorption of the primary and scatter radiation produced in the room. The lead-equivalent of a concrete wall 15 cm thick is approximately 1.5 mm within the diagnostic energy range – this reflects the superior absorption of lead compared with concrete in this energy range. The lead-equivalent of such walls may be increased by the use of barium sulphate plaster as a thin coating on the walls. This is because of the high atomic number of barium (Z=56).
As the beam energy increases, the advantage of lead over concrete diminishes, as there is a gradual shift from the predominance of photoelectric absorption to the predominance of Compton scattering. Thus the lead-equivalent of a barrier will increase with an increase in the photon energy – a greater thickness of lead will be required to give the same level of protection as the barrier. In the region of 1 MeV, the Compton scattering process predominates and lead has no real advantage over concrete since all materials have similar mass attenuation coefficients due to the Compton process. For this reason, many of the barriers used in radiotherapy departments are made of large thicknesses of concrete.
In conclusion, the design of a room, its wall thickness and the barriers must be such that the radiation dose received by patients, staff and members of the public is kept to a minimum in accordance with the ALARA principle. Further details of the design of diagnostic and therapy rooms will be found in specialized publications on this topic.
44.6 The role of the practitioner
The role of the practitioner is the justification of the request for the procedure. Practitioners are usually medically qualified individuals, although this role can be delegated to other radiographic professionals for some procedures, with the employer’s approval.
Before justification can commence, the practitioner must check that the referrer has supplied sufficient data of the procedure requested. This includes the following:
• The patient’s identification (and, if a female of childbearing age, the date of the patient’s last menstrual period).
• Sufficient relevant medical data to permit the practitioner to decide if there is sufficient net benefit to the patient to allow justification of the procedure and, if the patient is to undergo a procedure where radionuclides are administered, if the patient is breastfeeding an infant.
The logical suggestion is that no unnecessary radiation dose should be received by any person, but where there is a net benefit for the patient the request would be justified.
For instance, the mammography screening programme has increased the early detection rate of breast cancer, and this in turn increased the survival rate from this condition. In the case of other cancers, the risk of death to the patient is considerably higher if a course of radiotherapy treatment is not given. An undetected aneurysm may burst causing the patient’s death or other serious medical complications.
Another possibility is that the same information about the patient’s condition can be gained without using ionizing radiation (e.g. ultrasound or MRI) and, in these cases, the practitioner should suggest this change of imaging modality to the referrer.
If the patient is a female of reproductive capacity (i.e. between the ages of 12 and 40), the practitioner must consider the possibility that the patient is or may be pregnant. The operator is also responsible for checking this at the time of examination.
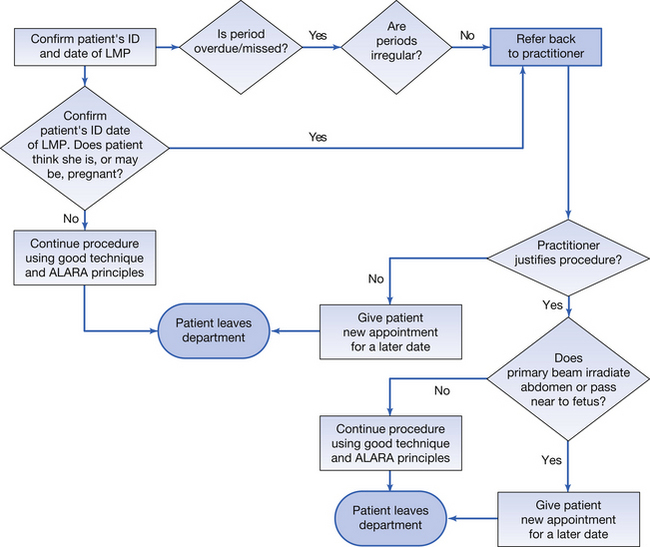
44.6.1 Radiological examinations of women of reproductive capacity
The current rules concerning radiological examinations of women of reproductive capacity are as follow:
• Any woman who has an overdue or missed period should be treated as though she were pregnant.
• If the woman cannot answer ‘no’ to the question ‘are you, or might you be, pregnant?’ then she should be treated as though she were pregnant.
• If the clinical indications are that an exposure should be made where the primary beam irradiates the fetus, then great care must be taken to minimize the number of views and the absorbed dose per view, but without jeopardizing the diagnostic value of the investigation.
• Provided good collimation is used, and equipment is properly shielded, radiographs of areas remote from the fetus (e.g. chest, skull, hand) may be done safely at any time during the pregnancy.
These recommendations do not reduce the care that should be taken in limiting the potential radiation dose to the fetus. The change in emphasis of the recommendations is that special precautions need only be taken if the woman is, or may be, pregnant – where ‘pregnant’ is defined as beginning when a menstrual period is overdue.
Other than this, there is no need for special limitations of exposures during a menstrual cycle, except for the normal requirements to keep all absorbed radiation doses as low as reasonably practicable. Good radiographic techniques should thus be used at all times to minimize radiation doses for all exposures.
A flow chart showing the progress of a woman of reproductive capacity presenting for a radiographic examination is given in Figure 44.2.
44.7 The role of the operator
The regulations define the operator as the individual (radiologist, radiographer or radiographic assistant) who is responsible for physically directing the X-ray exposure. They are the final link in the chain of radiation protection as they have a dual responsibility:
1. To keep the radiation dose to the patient, themselves and other staff and as low as reasonably practicable but consistent with the clinical requirements of the examination. This includes:
2. Once these checks have been completed, the procedure can commence. The operator should bear the points listed in Tables 44.4 and 44.5 in mind while carrying out the procedure.
Table 44.4 Methods of dose reduction to the patient
| FACTORS WITHIN THE OPERATOR’S CONTROL IN RADIOGRAPHY | FACTORS WITHIN THE OPERATOR’S CONTROL IN FLUOROSCOPY |
|---|---|
| Selection of exposure factors, preferably using an anatomically programmed timer, so that the exposure is within the diagnostic reference level produced by the employer for the examination | Use of pulsed fluorography and image storage systems |
| Use of the highest practicable kVp | Use of digital fluorography |
| Making use of secondary radiation grids to reduce scatter reaching the image receptor | |
| Use of tissue displacement techniques with obese patients | |
| Use of immobilization with patients who cannot remain in position or keep still during the exposure | |
| Limitation of field size by use of collimation | |
| Utilizing gonad shields | |
| Use of the fastest image receptor system, consistent with the requirements of the examination |
Table 44.5 Methods of dose reduction to staff
| RADIOGRAPHY | FLUOROGRAPHY |
|---|---|
| Only those whose presence is required should be in the room during exposures | All staff must wear adequate protective clothing, as specified in the written systems of work |
| All staff should stand behind the protective barrier during exposure | Use of automatic collimation |
| The X-ray tube must have adequate shielding | Staff should stand as far as possible from the primary beam |
| Operators should not expose themselves to the direct beam | Protective shielding should be incorporated in the generator to reduce dose from scattered radiation |
| Restless patients should be supported by immobilization devices | |
| Operators should not support restless patients |
Note: Many of the methods that reduce dose to the patient will also produce a reduction of dose to staff. Fluoroscopy results in higher radiation doses than conventional radiography and therefore good technique is even more essential to keep radiation doses to a minimum. The use of a modern fluoroscopic unit with pulsed fluoroscopy, image storage, automatic collimation and digitization of the image will result in a reduction of the radiation doses to patients and staff.
44.7.1 Reporting overexposure of patients
In the case of a known or suspected overexposure to a patient, the operator must inform the RPA. They will then report this to the Healthcare Commission, who will conduct an investigation into the incident and make recommendations to prevent the reoccurrence of similar incidents.
In this chapter, you should have learnt the following:
• The purpose and scope of radiation protection (see Sect. 44.2).
• An outline of the regulations affecting radiation protection (see Sect. 44.3).
• The organization of radiation safety in a hospital trust (see Sect 44.3.1).
• The responsibilities of the manufacturer (see Sect. 44.3.2).
• Dose-equivalent limits in radiation protection (see Sect. 44.4).
• The requirements for the designation of radiation workers (see Sect. 44.4.1).
• Methods of personnel monitoring (see Sect. 44.4.2).
• Procedure followed if an employee has been overexposed to radiation (see Sect. 44.4.3).
• Local rules (see Sect. 44.5).
• Designation of work areas in radiation protection (see Sect. 44.5.1).
• The design of designated areas in radiography and radiotherapy (see Sect. 44.5.1.1).
• The role of the practitioner (see Sect. 44.6).
• Special precautions in the radiological examination of women of reproductive capacity (see Sect. 44.6.1).
• The role of the operator and practical methods of radiation protection (see Sect. 44.7).
• Reporting of overexposure to a patient (see Sect. 44.7.1).
Further reading
Allisy-Roberts P. Medical and Dental Guidance Notes – A Good Practice Guide on All Aspects of Ionising Radiation Protection in the Clinical Environment. York, UK: Institute of Physics and Engineering in Medicine, 2002.
Ball J.L., Moore A.D., Turner S. Ball and Moore’s Essential Physics for Radiographers, fourth ed. London: Blackwell Scientific, 2008. (Chapter 21)
Bushong S.C. Radiologic Science for Technologists: Physics, Biology and Protection. New York: Mosby, 2004. (Chapters 33–40)
HMSO. 1999/3232 The Ionising Radiation Regulations. London: HMSO, 1999.
HMSO. Statutory Instrument 2000/1059. The Ionising Radiation (Medical Exposure) Regulations. London: HMSO, 2000.
HSE. Working with Ionising Radiation – Ionising Radiation Regulations 1999. Approved code of Practice and Guidance. Sudbury: HSE Books, 2000.
Webb S., editor. The Physics of Medical Imaging, second ed, Bristol: Institute of Physics, 2000. (Chapter 2)