9 Working with people to make choices about their treatment
• To recognise the differences between compliance and concordance approaches to making choices about treatment options
• To discuss the values and skills which aid and support concordance approaches in practice
• To identify the potential benefits of adopting a concordance approach to the management of medication
• To identify the challenges of implementing concordance approaches when applied to a mental health context
Introduction
Throughout this book we have written about approaches which encourage practice-based partnership and cooperation with the service user. The medical model has been criticised for contradicting this approach, due to the perception that decisions are often being made by medical practitioners about the best course of treatment based upon their professional expertise regardless of the service user's views. This approach is known as promoting ‘compliance’ and involves encouraging the person to adhere to a treatment regime which has been prescribed for them.
This chapter will discuss ways of working which support the service user to make choices about their treatment options based on knowledge and information given to them by the mental health practitioner. This is known as promoting ‘concordance’. The principles of concordance approaches apply to making decisions about all treatment options, however this chapter will focus primarily on how it can aid the management of medication.
Compliance
Compliance in the context of health care is defined as ‘The extent to which a person's behavior in terms of taking medications, following diets, or executing lifestyle changes, coincides with medical or health advice’ (Haynes et al 1979).
In a mental health setting, people are sometimes reluctant to adhere to medical advice for a number of reasons:
• They may disagree that they have a mental health problem and therefore do not see the need to follow the advice or treatment plans devised by mental health professionals.
• They may experience negative side effects of prescribed treatments which they feel are more disabling than the problem itself.
• They may view the treatment prescribed as unhelpful and not appropriate to address the problem as they perceive it.
• They may want to maintain their current lifestyle or some elements of their mental health problems as it gives them pleasure or is a significant aspect of their identity.

1. Consider an aspect of your lifestyle which you enjoy, for example a hobby, social activity or a way of relaxing.
2. Reflect upon how you would feel if you were asked not to engage in this activity any more because you were told it is potentially damaging to your health or may impact negatively on your social functioning.
3. What would influence your decision whether or not to follow the advice?
A number of service users have expressed their dissatisfaction with this approach to practice. It has been identified as disempowering as it doesn't acknowledge the person's perspective or take into consideration their knowledge of themselves (Perkins & Repper 1996). Furthermore, if the person does not agree with the treatment, they are unlikely to follow the plan as prescribed and therefore medication may be thrown away or appointments missed which can be a waste of resources.
In some circumstances a person may have been viewed as unable to contribute to a decision regarding their treatment due to the seriousness of their mental health problem. In these situations it would be appropriate for a Mental Health Act assessment to be undertaken or an assessment of the personal mental capacity. Parts of this legislation allow professionals to administer treatment against the person's will if it is deemed in their best interests (see Ch. 4). However, it is important to acknowledge that if this is not the case, the person has the right to make an autonomous decision about their treatment even if the mental health professional feels that they could be putting their health at risk. See the scenarios below for examples.
1. John attends a drug and alcohol support service during the day and engages in the various therapeutic interventions which are aimed at reducing his drug use. However, in the evenings with his friends, he continues to smoke cannabis. The quantity and strength of the cannabis he smokes is seriously affecting both his physical and mental health, however it is how he keeps in contact with his friends and so he is reluctant to stop.
2. Sarah has been prescribed an antipsychotic which is known for causing weight gain. Despite the difficulties she is having with her voices, she is very conscious of her weight and feels her appearance is important to her self-esteem and wellbeing. She decides not to take her medication but will not discuss this with her care team because she is sure they will force her to go into hospital.
3. Wesley has been referred by his social worker to a group for young people who have experienced domestic violence. However, he doesn't want to talk about his feelings to a group of strangers. In order to avoid going to the group he has been missing appointments with his social worker and refusing to talk to his mum about how he is feeling. He is becoming extremely isolated, his mood is getting consistently worse and he is having thoughts of suicide.
In these examples it is evident that the service users are not complying with their treatment plan for a range of reasons which is having a detrimental effect on both their mental health and their engagement with mental health services. In these types of circumstances it is proposed a concordance approach would be more beneficial.
Concordance
Weiss and Britten (2003) state that ‘concordance is fundamentally different from either compliance or adherence in two important areas: it focuses on the consultation process rather than on a specific patient behaviour, and it has an underlying ethos of a shared approach to decision making rather than paternalism … it is not possible to have a non-concordant patient’.
If we break this statement down, there are a range of skills and values which are required if we are to promote concordance.
1. A willingness to work in partnership with the service user and acknowledge their values, perspective and expertise.
2. An awareness of how the service user may view you as a professional and how this may impact on their willingness to be open with you about their views of their treatment.
3. A purposeful effort to engage with the person and build a therapeutic relationship.
4. The use of communication skills which enable the person to be open with you about their perceptions of the treatment options available.
In addition to these core elements, there are areas of knowledge and various tools which can aid this approach. The first of these is knowledge of the treatment options available.
In relation to medication management, it is beyond the scope of this book to provide you with a detailed explanation of each of the medications used in mental health services and how they work. Box 9.1 contains a brief explanation of the groups of medications commonly used in mental health services.
Box 9.1 Medications commonly used in mental health services
Antipsychotics/neuroleptics
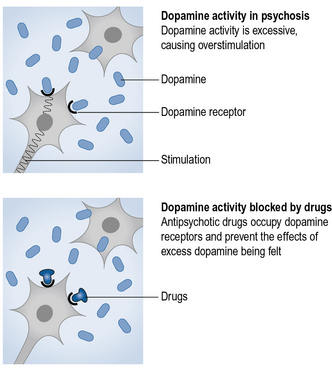
These drugs are used to treat psychosis which is characterised by the experience of unusual thoughts, perceptions and voices. People who experience these symptoms are often diagnosed with schizophrenia which is thought to be partly caused by an increase in communication between brain cells due to the overactivity of an excitatory chemical called dopamine. Antipsychotics bind to receptors in the brain to reduce the transmission of nerve signals and therefore make nerve cells less sensitive to dopamine. They can also cause disturbances to other chemicals in the brain which leads to side effects such as restlessness, parkinsonism, low blood pressure and erectile dysfunction. Long-term use can lead to permanent side effects such as tardive dyskinesia which is characterised by repeated jerky movements. Different antipsychotics can be tried in order to reduce side effects and the lowest possible dose should be administered. Newer antipsychotics claim to cause fewer side effects because they act more selectively on the dopamine receptors. These are known as atypical antipsychotics.
Antidepressants
These drugs are used to treat moderate and severe depression which is thought to be partly caused by a reduced level of neurotransmitters in the brain which stimulate brain activity (e.g. serotonin). Antidepressants work by increasing the level of these excitatory neurotransmitters by blocking their reuptake or preventing them from being broken down. It takes 10 to 14 days for antidepressants to reach a therapeutic level, however temporary side effects can happen immediately. There are three main types of antidepressants: tricyclic (TCAs), selective serotonin reuptake inhibitors (SSRIs) and monoamine oxidase inhibitors (MAOIs). TCAs can be very dangerous in overdose and MAOIs react with certain foods such as cheese to cause high blood pressure and headaches. As a result of this, SSRIs and TCAs are most commonly prescribed.
Mood stabilisers
These drugs are given to people who experience extreme fluctuations in their mood and are often diagnosed with bipolar affective disorder (also known as manic depression). The medication reduces the intensity of the extreme moods and helps to reduce the frequency of mood fluctuations. Lithium is commonly prescribed as a mood stabiliser which requires careful blood level monitoring due to its potential to be toxic. It can lead to side effects such as nausea, drowsiness and weight gain. If the person experiences side effects such as blurred vision or a rash, the medication should be stopped. It may also affect the function of the kidney and thyroid, therefore these are also monitored. Other mood stabilisers are available if lithium therapy is unsuccessful or unsuitable for the person.
Anxiolytics/antianxiety
These drugs are used for short-term relief of severe anxiety. There are two types of drugs used to reduce anxiety: benzodiazepines and beta blockers. Benzodiazepines reduce the brain activity to induce a sedative effect which aids relaxation. Beta blockers reduce the physical symptoms of anxiety such as increased heart rate and palpitations by blocking receptors and stopping the effects of adrenaline on the body. Benzodiazepines can cause low motivation, slower reactions and dizziness. If they are withdrawn quickly, they can cause increased anxiety, restlessness and nightmares.
Hypnotics
These drugs are prescribed for people who are persistently having difficulty getting to sleep or staying asleep. They are recommended if alternative non-medication options have not been effective and lack of sleep is having a detrimental effect on health. They should be used as a short-term remedy to reestablish sleep patterns. They work by depressing the brain function by reducing communication between the nerve cells which slows brain activity. The type of sleep that is induced when taking hypnotics is different to normal sleep and therefore people often describe feeling hungover the following morning. They can cause dependence and they become less effective over time which leads to people needing an increased dose. Withdrawal from hypnotics can also be very distressing as a result of possible increased anxiety, nightmares and hallucinations. A common hypnotic medication used in mental health service is zopiclone. Alternatively, benzodiazepines can be used.
Antidementia
These drugs are prescribed for people who have a diagnosis of Alzheimer's disease to improve the symptoms of dementia. They work by preventing the breakdown of a chemical in the brain called acetylcholine which increases the person's alertness and slows down deterioration in the brain associated with Alzheimer's disease. They do not prevent the long-term progression of dementia and there is a gradual loss in improvement after they have been stopped. Side effects can include difficulties with urinating, vomiting and diarrhoea.
We recommend that in order to develop your knowledge base in this area, you complete and repeat the following activity. We suggest that this will enable you to relate the information regarding medication to people you meet, which is a helpful way of remembering this material. It also contributes to your learning in achieving your Nursing and Midwifery Council (NMC) competencies and essential skills (NMC 2010). We have recommended some texts which may be helpful in this area at the end of the chapter.

1. Consider a small number of service users you meet in practice on each placement.
2. Identify their diagnosis and the medications that they have been prescribed.
3. Use the British National Formulary (BNF), medication-focused texts, National Institute for Health and Clinical Excellence (NICE) guidelines and the person themselves to identify:

Once you have developed your knowledge of the medication options, it is then important to consider how you will present this information to the service user in a way in which they can understand the potential benefits and limitations. This aims to enable the service user to make an informed choice about their medication and is known as an educational intervention. Below you can see an example of how you might describe an atypical antipsychotic.
Example: describing an atypical antipsychotic
Nurse:
Hi Jenny. Last time we met we said we would have a chat about the medication you have been taking. You said you are having some doubts about continuing to take it. Is that still OK with you?
Jenny:
To be honest, I'm not sure I want to take anything. I've heard some really scary things about what these tablets can do to your mind and I would rather stick with my herbal stuff.
Nurse:
OK, I would be interested to hear what you have heard about the medication and the herbal remedies you mentioned. But before you make a decision, shall I tell you a bit more about the medication and you can see what you think.
Nurse:
Well, the medication that Dr Petal has prescribed for you is an atypical antipsychotic. This means it is one of the newer types of antipsychotic medications which work in a different way to the older types. The theory is that the voices that you hear are partly caused by a chemical in your brain called dopamine. This is a type of neurotransmitter which has been found to influence thoughts, emotions, mood and perceptions. It carries messages across the nervous system and sends signals which tell your brain how to respond. Some people have too much of the chemical and some people are very sensitive to it and so the medication works by blocking the chemical or reducing the amount that is produced. This doesn't fix the problem but can reduce the symptoms you might experience like your voices.
Nurse:
This is because of the side effects of the medication. It can also disrupt how other chemicals in your brain work and everybody seems to respond differently. What Dr Petal has done is started you off on a small dose and he will gradually increase it until it makes a difference to your voices. At the same time we would be monitoring any side effects. If the side effects were causing you problems then we would try a different type of medication.
Key features of the interaction
• Jenny has started taking the medication without a clear idea of how it works or how it might affect her. This was affecting her beliefs about her medication and her motivation to continue taking it.
• Jenny is considering stopping her medication but feels able to speak openly with the nurse about this. This illustrates the presence of a therapeutic relationship and allows the nurse to discuss Jenny's beliefs about her medication.
• Jenny has got some ideas about alternative treatment options. The nurse acknowledges this and is open to exploring her ambivalence and uncertainty about her treatment.
• Information about how the medication works is given in a clear and factual way.
• Different methods of presenting the information are used.
• Jenny is given the opportunity to ask questions and there is a focus on what is important to her (i.e. side effects, practical issues).
• Her perception about how the medication is affecting her is the central feature in the decision-making process illustrating a collaborative approach to decision making.
• The option to make changes based on her views of how her medication is affecting her is clearly given.
• The conversation is left open and plans are made to revisit it at the next session.
Other ways of promoting concordance are known as ‘behavioural interventions’ which aim to help service users think about how medication best fits with their daily routines. This might involve working with a person who finds it difficult to remember to take their medication. This may mean they are not getting a therapeutic dose or that they are taking extra to compensate when they have forgotten. Behavioural interventions would look at ways of reminding the service user and helping them to integrate taking medication into their daily routine. Alternatively the service user may be finding that the side effects of the medication are interfering with their day-to-day lives. In Jenny's case, a behavioural intervention might look like this:
Key features of this interaction
• The nurse revisits the area that is important to Jenny and explores her current views.
• The nurse uses language which reinforces that this is a partnership process.
• The nurse answers Jenny's questions with a simple and accurate answer.
• The problem is approached collaboratively. Jenny is encouraged to think of solutions and an action plan is made on how to implement the solution.
• Plans are put in place to evaluate the success of the solution.
The final element of concordance is around making longer term plans with the service user about how their medication fits with future goals. For some people, alternative coping skills will be developed and they may wish to reduce their medication and eventually stop taking it. By using the skills identified above, this can be a highly positive process whereby the person feels in control of their mental health and supported in developing their independence from mental health services. For others, the continuation of medication may be helpful and it is important to consider with them how it will continue to be an assistance rather than a hindrance to them reaching their desired future.
Haynes R.B., Taylor D.W., Sackett D.L. Compliance in health care. Baltimore: Johns Hopkins University Press; 1979.
Nursing and Midwifery Council. Standards for pre-registration nursing education. London: NMC; 2010.
Perkins R., Repper J. Working alongside people with long term mental health problems. Cheltenham: Stanley Thornes; 1996.
Weiss M., Britten N. What Is concordance? Pharmaceutical Journal. 2003;271:493.
British Medical Association and Royal Pharmaceutical Society. British national formulary. London: BMJ; 2010.
Bressington D., Wilbourn M. Medication management. In: Callaghan P., Playle J., Cooper L. Mental health nursing skills. Oxford: Oxford University Press, 2009.
Healey D. Psychiatric drugs explained. Edinburgh: Elsevier; 2008.
NICE guidance on medication adherence: http://www.nice.org.uk.
Mind: service user information and opinion on medications used in mental health: http://www.mind.org.uk.