4 Mental health practice learning
• To gain an understanding of the nature of various mental health practice areas
• To identify the possible learning opportunities which will enable you to optimise your placement experience and meet your Nursing and Midwifery Council competencies and essential skills clusters
• To consider the views of students and mentors who have experience of working within the practice area
• To develop skills in action planning for placements in order to direct your experience in line with your learning needs
Introduction
This chapter will introduce a variety of mental health placements which you may be given the opportunity to experience as a pre-registration student. The chapter is made up of contributions from students and mentors who have practised in the various clinical areas. The specific name of a service or the way it is structured may vary in your area, however the insights offered by students and practitioners will be helpful in preparing for your placement and getting the most of the learning experience.
Practice learning (placements) may be organised slightly differently depending on the university that you are studying at. These might be in placement blocks of so many weeks in which you rotate around different practice areas with time spent in university during these placements or in between (e.g. one placement in services working with older people, one in a community mental health team and one in an acute in-patient service). Practice learning may have also been organised so that you have a caseload of service users who you follow throughout your training. The changing nature of health care is also facilitating the increasing use of a different structure of practice learning.
The NHS next-stage review outlined a new direction for the configuration of health and social care services promoting increased integration and partnership, requiring health professionals to work across service boundaries (Darzi 2008). In the future, healthcare services will be required to meet a number of challenges including an ageing population, the delivery of care in different environments and rapidly changing technology (Longley et al 2007). In order to help nurses of the

Have a look through your student handbook alongside your course information and read the sections on practice learning.
1. Identify what approach to practice learning is used in your university.
2. Identify what ‘type’ of practice settings you might be going to on your course.
3. Consider what you already know about these settings and what you might need to know to help you plan your learning for these areas (Ch. 5 will help you with this).
4. Check the chapter aims and outcomes for Section 2 and highlight the chapters you feel will be most relevant.
5. Write an action plan for how you will find out any further information you need about the practice areas where you will be on placement.
future meet some of the challenges, the Nursing and Midwifery Council (NMC) stipulates that practice learning for students undertaking pre-registration education must reflect the service users' journey in order to support the practitioners of the future to work in reconfigured service structures (NMC 2010).
This means that rather than blocks of placements, universities and the care providers they work in partnership with are increasingly moving towards structuring placements to more closely follow a pathway that a service user may take through services. This might mean that, as a student, you spend longer time working with one mentor, service user or service. One of the important implications of this is identifying how the skills that you are learning can be used effectively in different settings (some of which you might not get the opportunity to spend lots of time in during your education). This emphasis on how skills can be used in working with individuals in different settings is reflected in the structure of this book, through its focus on approaches and skills important for mental health nursing across service boundaries.
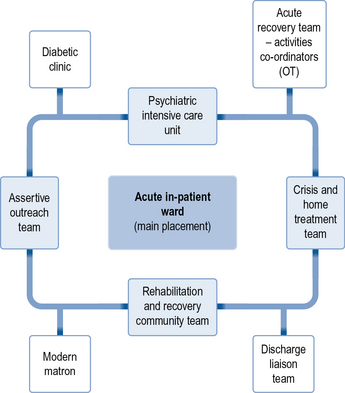
In some courses this pathways approach will mean you are based in one practice area for longer, spending a few weeks during this time in practice areas that link with this service. This might also include shorter insight visits where you may have the opportunity to spend time with different professionals or in settings outside health care (such as the coroner's court). Figure 4.1 shows what this might look like. The centre box represents the main placement area, the lightly shaded boxes may be the practice areas where you could spend a few weeks and the unshaded boxes may be where you link with for insight visits. Depending on your course, this could be arranged for you, or it may be something that you have the opportunity to get involved in arranging yourself following discussion with your mentor.
Routes into mental health services
Mental health support is provided to individuals across the age span in a variety of settings within healthcare services. The manner in which individuals gain access to this support is to a certain extent defined by the nature and priority of their need (in a similar way to access to all health services). However, given some of the tensions that may be associated with mental health care, including care delivered to individuals detained under the Mental Health Act, the means through which initial contact is established could have major implications for the development of the therapeutic relationship and the delivery of the required support.
GPs remain one of the main gatekeepers to mental health services and, in many respects, GP surgeries are a major provider of mental health support. However, GPs refer to both primary and secondary mental health services (there will be some local variations in the design of these services). Counselling and psychotherapy services are delivered by mental health nurses and specially trained mental health workers in GP surgeries. These practitioners provide support for individuals with common mental health problems or who may be experiencing trauma and can gain psychological input for their experiences on a short-term basis. GPs will refer directly to these practitioners. They may also refer people on to community mental health teams of which there are a number of different types (see Ch. 6). The circumstances and diagnosis of each individual may define where they are referred. Here, professionals working in the community (commonly mental health nurses) will conduct an assessment to decide whether they are the appropriate people to provide support. For people who are highly distressed and in immediate need, GPs can also refer directly to a crisis and home treatment team. This service can provide short-term and intensive support to the individual in his or her own home until the crisis period is over. They can also work towards securing an admission to hospital for the individual if this is required.
For access to mental health services, support or hospital admission out of hours, the accident and emergency department might be a first port of call which can result in an assessment by a psychiatrist, referral to a crisis team or, in some areas, short-term input from a specialist accident and emergency liaison team.
People can also come into contact with mental health services via the police and the criminal justice system. Mental health services have received criticism due to the inequalities in access among different ethnic groups, as Afro-Caribbean men are more likely to come into contact with mental health services via the police. Rates of mental health problems are high among prisoners and this group is at particularly high risk in relation to suicide. Prison in-reach teams may take on referrals from people in prison experiencing mental distress. At times this can result in individuals who require support being moved to forensic secure units or hospitals. If an individual is arrested and there is concern they may have mental health problems, forensic or court liaison teams may conduct assessments to identify whether the person requires the input of specialist mental health services.
Care delivery environments
The environment in which a service is delivered will have a significant impact on the learning opportunities available. Each environment offers unique experiences and can also present specific challenges. This section will highlight some of these points by considering the impact of community and in-patient environments on student learning.
Community placements
The key advantage of many community placements is that they offer you the opportunity to visit people in their own homes. This helps you to gain an insight into how the person's mental health problems are influenced by their environment and social circumstances. It can often provide pieces to the jigsaw puzzle which you would never have known if assessment and contact with the person only happened in an office or a ward environment. Therefore, a more holistic picture is gained of the person by paying attention not only to what they say, but also to your observations of their surroundings and how they interact within their community.
This does, however, have an influence on the dynamics of the relationship you build with the person and how you communicate with them. Most significantly the person is inviting you into their home and, therefore, it is important to respect their rules and routines. In an in-patient setting, the organisation sets the rules and the person who is using the service is expected to adhere to them. In the community, the person is setting the rules and, therefore, you have the opportunity to begin an interaction based on a more equal footing. For example, is there a particular chair that they would rather you sat in? Would they prefer it if you took your shoes off? These simple acts have significant implications for the nature of the relationship you begin to build.
It is also important to remember that the person may not wish to see you that day and, provided that you are not concerned about their safety, they have every right not to allow you into their home. This also reinforces the person's position of choice and emphasises the importance of investing time to engage with the person rather than taking for granted your right to be invited into their personal space.
A further benefit of community placements is the opportunity for you to engage in one-to-one time with the service user without the interruptions or distractions associated with in-patient settings. This can offer you the opportunity to build significant relationships with people and advance your communication skills. You may be encouraged by your mentor to visit someone independently or lead the interaction. This will allow you to take a more active role and move beyond chit-chat to more autonomous and focused interactions. Many students say this opportunity is very beneficial for the development of their confidence as they begin to think of themselves more as a responsible practitioner.
The nature of the one-to-one time you spend with a person can vary widely depending on their current needs and care plan. Students often take advantage of having more time to engage in supporting a person to achieve a specific goal. Some interventions you may be involved in will take place in the community and will be focused on supporting the person to develop independence and confidence or to combat social anxiety. At times, some students find it challenging to see the purpose of their involvement with the person in terms of their learning and feel that they are fulfilling the role of a support worker. It is, therefore, important to be clear about the rationale for the contact you are having with the person so you can ensure you are working within the overall plan of care rather than creating a more socially supportive relationship, which cannot be sustained due to the length of your placement.
The nature of community placements sometimes means that you are not spending as much time in direct contact with service users. This could be because your mentor is completing paperwork, the service user is reluctant for you to visit them or your mentor does not feel it is appropriate for you to be present. During these periods, some students find it difficult to know how to use this time effectively. In order to combat this, we suggest taking a more self-directed and proactive approach to this placement. Once you have identified the times when you will not be working directly with your mentor, you are then able to approach other members of the team for additional opportunities. Many members of the multidisciplinary team will be very happy to spend time with you or take you with them on visits. You can also use your time to develop your skills in record keeping, becoming familiar with documentation or liaising with other members of the care team. You may also want to organise to visit a service which is linked to the placement area you are in. Whatever you choose, with a little planning you can utilise this time effectively.
In-patient placements
The term ‘in-patient area’, when used in the context of mental health services, can be taken to mean a setting for mental health care that involves a level of service delivery that is of higher intensity than in a community context. The intensity is heightened in terms of the following aspects:
• Service users are perceived as needing assessment and treatment in a contained setting rather than the service user's home environment.
• The Mental Health Act (1983) may be used at some point during the service user's assessment and treatment.
• Interaction with, and interventions by, a range of mental health professionals is a given.
• The potential for disturbance, annoyance, irritation and aggression from other service users is ever present.
• Opportunities for copycat behaviour and infection by other service users' pathologies are increased.
• Lack of continuity and consistency is an inevitable consequence of the shift systems used in many institutional care settings.
• Activities of daily living such as sleeping, eating, activity and so on may be compromised for most service users in some way.
The student nurse may at first see the above list as intimidating and disadvantageous for their learning opportunities as compared with the more autonomous work setting of the community practitioner. However, you will find that many of your mentors may hold the view that the institutional setting, despite its many disadvantages and discomforts for service users and professional carers, can be a source of similarly intense learning experiences for students. If that idea is applied to the seven areas above, the opportunities for students can be as follows:
• The contained environment is needed to facilitate, primarily, safety and security for the service user. In most instances the reason to assess and treat someone in a hospital environment rather than in their own home means that they are too distressed or disturbed at the time of assessment to be helped in their own home. It is likely, therefore, that the student will see service users being admitted and treated who are often clearly more distressed or disturbed than can be seen in community settings.
• The use of the Mental Health Act (1983) inevitably produces tension between healthcare workers and service users who are being subjected to detention or treatment orders. The ways that experienced and effective professionals strive to maintain therapeutic relationships with service users, despite often being the implementers of the law, can provide rich learning opportunities.
• Institutional healthcare settings, by definition, are sustained by other institutional systems. For example, a typical mental health ward will be serviced by social workers, psychiatrists, occupational therapists, psychologists, phlebotomists, pharmacists, clerks, domestics and so on. The effective mental health nurse must sustain a constructive working relationship with all of these different visitors, in order to provide the best possible service to the client group. As the nurse does this, she provides a role model for the observant student, as well as evidence that the job of a qualified mental health nurse involves skills such as diplomacy, assertiveness and so on, as much as knowledge of medications and Mental Health Act Sections.
Student nurse: I've just been sitting with Jim and he says he wants to die …
Staff nurse: Oh don't worry. He's always saying that to new staff – especially students.
Student nurse: Hi Jim. How's it going today? You were a bit down yesterday.
Jim: I've really had it. I can't go on like this. You're the only one that seems to be listening to me …
The above dialogue illustrates the kind of dilemma that student mental health nurses can easily find themselves in. Do you take Jim's comments at face value, or do you trust the experience of the staff nurse and ‘ignore’ what he is saying?
Mental health placement learning areas
Adult community mental health care services
In 1999 the Department of Health published the National Service Framework for Mental Health which outlined a new structure for community mental health services. Traditionally community teams worked within a location (often called a catchment area) to provide support to people with a vast variety of problems and at different points in their experiences of distress. In order to promote a recovery approach to delivering community services, a new structure was defined which involved a number of more specialised teams who would focus on specific client groups and provide interventions during defined periods of their distress.
The following section will provide information from students and mentors on these services with a focus on what you should know before commencing the placement, a description of what you might experience and hints and tips on how to make the most of the learning opportunities. Further descriptions of services can be found at the Mind Website (http://www.mind.org.uk).
Placement 1: Crisis intervention and home treatment team: a student experience
Denise Sproat, second-year mental health branch student nurse
The service offers 24-hour crisis intervention and home treatment for people experiencing a severe mental health crisis. People are referred by other services such as their GP and the team are known as the ‘gatekeepers’ to other services. If the referral meets the criteria initially, the team have to respond within 4 hours and carry out an assessment of the person's mental health. On the whole I found that people presented with thoughts of suicide, or had made an attempt to end their life, and so were high risk. The service is an alternative to hospital and where a person is taken on by the team they are usually assessed daily over a 72-hour period. Assessments are carried out by two nurses so, as a student, you will be the second person. People are treated at home from anywhere between 2 weeks and 2 months and supported holistically to recovery from their crisis. However, sometimes people can deteriorate and be admitted to hospital.
Melissa Wheeler, second-year mental health branch student nurse
My time as a student nurse with the crisis team was one of the most intense periods of my training within practice. Having the opportunity to work alongside such experienced nurses and multidisciplinary team members on a one-to-one basis was invaluable and made me appreciate the versatility and skills of the team when adapting care to an individual client.
While there I gained a greater understanding of assessments, including mental health examinations, risk assessment and written documentation, and became familiar with a variety of therapeutic approaches and interventions. Time spent with the consultant psychiatrist was extremely rewarding as was attending home visits: both offered opportunities for learning, developed my knowledge base and strengthened my skills of care delivery within changing environments.
I found that many of the crisis team members proved to be supportive role models who were able to facilitate my personal learning and, on reflection, provided me with a greater self-awareness and understanding of others. Although often challenging and hard work, I felt privileged to have been given such a valuable learning opportunity.
Placement 2: Adult community mental health teams (CMHTs)
Rosie Robinson, third-year mental health branch student nurse
In my second year I did two community placements. There are many learning opportunities in a community setting such as working in a team which involves other
Melissa and Denise identify a number of learning opportunities which they encountered while working with the crisis team. Identify up to three of these learning opportunities which you would prioritise for your placement and consider what prior reading may be helpful in enabling you to achieve these.
Within Melissa and Denise's narratives there may be some roles, definitions or language that you have not heard before. Use the jargon and acronyms buster in Appendices 1 and 2 to identify what these terms mean in a mental health context.
professions such as psychologists, occupational therapists, social workers and psychiatrists. This includes multidisciplinary meetings in which you can participate. I had the opportunity to develop my confidence in administering depot medication. The key learning opportunity for me was that you have the chance to visit people in their own homes and support their carers. I also got much more comfortable with using the Care Programme Approach paperwork, including notes, assessment documentation and care plans along with participating in initial assessments.
I hope you enjoy your community time as much as I did and have a great experience!
Rosie describes the benefits of working with the various professionals who work within the CMHT. Before starting your community placement, identify the role of each of these professions and consider how you might benefit from working with them on your placement and what learning outcomes you might achieve.
Placement 3: Early intervention team
Gabriella Maria Burton, second-year mental health branch student nurse
During my second year as a student nurse I got the opportunity to go on placement with an Early Interventions in Psychosis Team. They predominantly work with 15–35-year-olds, suffering with their first untreated psychotic episode. They work to detect early, and intervene to prevent further, damage to the service user's life. This involves intensive work with the service user, families and carers.
Many service users in the service can have a dual diagnosis or no diagnosis at all. This can be many people's first involvement with mental health services and often a very confusing time for them. Due to this, some service users may present angry, scared or confused about the current situation they find themselves in, which is understandable, so you need to educate, support and empathise with them. Although saying this, many service users have been with the team for some time and have built a therapeutic relationship with their care coordinator and there will be various people that you can work closely with and build your own therapeutic relationship with.
There are many learning opportunities as there are so many different professionals in the team such as family therapists and cognitive behavioural therapists. Opportunities I came across incorporated initial assessments, depots, social groups, care plan reviews, social circumstance reports and many more interventions.

Placement 4: Assertive outreach team
Amy Ramful, third-year mental health branch student nurse
During my second year of training I had a placement with the Assertive Outreach Community Team. Assertive Outreach work with service users with severe and enduring mental illness who have difficulties engaging with services. Some service users may also have a forensic background or dual diagnosis. The team tends to have smaller case loads compared to a CMHT, which allows for more intensive treatment which helps with engagement issues.
As a student, don't be surprised if some service users aren't keen on having you involved in their care. This is the nature of the client group. When I first started the placement my mentor told me to expect a lot of unanswered doors and running around trying to get hold of people. However, don't let this put you off because, of the work the team does with clients, many have built very good therapeutic relationships with the team, and there will be plenty of opportunities for you to work closely with some of them, and you may even have the chance to have your own mini caseload.
Other learning opportunities I came across included depot administration, Care Programme Approach reviews, risk assessments, Mental Health Act assessments, care planning and doing individual work with service users.
Adult 24-hour care services
A key aim of the National Service Framework for Mental Health (Department of Health 1999) was to design services which provide mental health care in the least restrictive environment. Over the past 30 years the number of hospital beds has significantly decreased and every effort is made to support people who are in distress to remain in their own homes. This model of mental health care aims to reduce the disruption a period of crisis may have to a person's life and limit the effects of continuous admission to hospital. People who have previously experienced this type of care are often referred to as ‘revolving door patients’. This label inevitably has negative connotations for the person's potential for recovery.
There are, however, times when hospital admission is thought to be unavoidable. This may be due to the person's safety towards themselves or others or due to requiring assessment and treatment under Section 2 or 3 of the Mental Health Act. Alternatively, a person may have recovered from their period of crisis but require additional support to enable them to regain the skills, roles and relationships required for them to move on from mental health services. In these circumstances the following 24-hour care services are available.
Placement 5: Crisis admission, treatment and therapy ward (acute ward)
Sharon Taylor, third-year mental health branch student nurse
My placement on an acute in-patient ward proved to be the most challenging, stimulating and rewarding experience in my student career. Generally speaking, people are admitted to the ward at their most distressed and vulnerable, and for a short period of time. This meant the ward was often busy and intense with a high patient turnover. I learnt a lot about the power of human kindness in bringing comfort to people; listening with compassionate understanding to people's lived experience of illness, treatment and recovery; and what it means to be a patient on an acute ward. This helped me to develop a more responsive approach to individual patient care.
I liked and benefited from the pace and variety of experiences acute nursing offers; one minute I could be doing a depot, the next minute an MDT, then reading patients their rights under the Mental Health Act. I enjoyed being part of the team; working with other health professionals was inspiring and taught me what it means to work collaboratively, particularly approaching problem solving and risk management as a shared experience.
Sharon tells us that she was involved in ‘reading patients their rights under the Mental Health Act’. Use the links in Chapter 3 and discussion with your mentor to find out what she means by this and what it would entail.
Placement 6: Psychiatric intensive care unit
Tanya Ames, third-year mental health branch student nurse
Often students are apprehensive about a placement on a psychiatric intensive care unit (PICU). This is often due to having a limited knowledge, being misinformed and having negative preconceived ideas. After feeling particularly fearful and nervous about this placement, I reluctantly agreed and, in hindsight, it has been an invaluable placement experience.
The PICU where I was placed provides 24-hour care in a low-stimulus environment for 20 males aged 18–65, accommodated on two sides and contained within a secure, locked unit: side A (8 intensive care beds) and side B (12 forensic rehabilitation beds). Side A manages patients who need initial assessment, high levels of nursing intervention and exhibit challenging behaviour. Side B is a low-security unit offering ongoing assessments and support for patients needing longer term treatment or preparation for resettlement.
Care and treatment are provided for those who cannot be managed on acute wards or other settings such as prisons. The service users are assessed as presenting a high risk to themselves or others and are at risk of absconding. The majority of patients have a primary diagnosis of a psychosis, many have a secondary diagnosis such as substance misuse and many have a forensic history. Most patients are detained on Section 3 of the Mental Health Act. As there are a limited number of beds, the staff:patient ratio is very high, as are levels of observation. ‘Incidents’ are infrequent, and any which do occur are quickly and effectively contained.
There are plenty of opportunities to meet practice outcomes/competencies such as liaising with other agencies, forming and maintaining therapeutic relationships with patients and their families, accurately recording documentation, undertaking initial and ongoing assessments, monitoring patients on high-observation levels, dispensing oral medication and administering depot injections, participating in ward rounds and multidisciplinary team meetings. Additional learning opportunities include insight visits to local prisons, acute wards and observing electroconvulsive treatment.
Although I had initially viewed my impending placement with trepidation, it soon became apparent that my fears were unjustified. The nursing team was very welcoming and supportive, understood my apprehension and soon put my mind at rest. My advice would be to start this placement with an open mind and take advantage of all the learning opportunities available to you.
Placement 7: Residential rehabilitation and recovery services
Emily Trivett, third-year mental health branch student nurse
During my first year I started my placement in a rehabilitation community unit. The placement itself was a house set in the community that provided accommodation for adults with mental health problems. The setting allowed the people to be surrounded by a nursing team, complete with occupational therapists, healthcare assistants and a cook. People come to learn new skills and master skills they have lost, such as learning to cook, clean and do their own washing – something we take for granted.
I was able to get fully involved with the nursing staff and actually help the patients to learn valuable skills during their stay. The patients stay normally for an assessment process of 8 weeks and this is reviewed to see how they have managed and whether they can move on to independent living. This is the aim for all the residents who reside at the house. Some come for 2 weeks at a time and come for the staying-well programme (SWP) to keep them well and to prevent relapse.
The service user develops a programme of what activities they are expected to do for the week, a combination of cooking their own meals, going on walks, budgeting when buying ingredients and using public transport. Also they are required to attend in-house meetings and do activities within the house, such as tidying their rooms, doing their washing and cleaning up after they have cooked meals.
I was able to experience what it is like working closely with people, encouraging them to make their own meals and motivating them to try new things. I gave them ideas for what they could cook and assessed their ability to cook on their own. I also took part in art and crafts, and ran my own groups with some of the staff. I also accompanied the service users on walks to parks and to shops to buy cooking ingredients.
The placement allowed me to be able to complete paperwork and do certain tasks on my own, once I had seen them done by someone else, such as completing risk assessments, admission forms, etc. I thoroughly enjoyed this placement as it enabled me to feel fully involved with both the team of staff and the service users. It was also a chance for me to begin to understand how mental health nurses work and to be involved with different professionals such as doctors and occupational therapists.
Older adult mental health care services
Older adult mental healthcare services provide assessment and treatment to people over the age of 65. People who access the service may have the types of mental health issues you would see in adult care settings such as low mood, anxiety, psychosis or poor coping strategies. These are often referred to in this practice area as functional mental health problems. Some people will have developed these issues in the later years of their life, however some may have been involved with mental health services for many years. Alternatively, people may require support from mental health services due to issues resulting from deterioration in the function of the brain such as memory problems, dementia and Alzheimer's disease. These are often termed organic mental health problems.
Placement 8: 24-hour care assessment units
Charlotte Kawalek, third-year mental health branch student nurse
As a first-year student, with some prior experience in the mental health field, I felt going into an elderly in-patient admission ward was a brilliant opportunity for me to be able to gain a basic grounding into a range of mental health problems and what effect they had on the individual and the carers and, indeed, how the nursing staff and others within the multidisciplinary team interacted with the client, as part of their treatment.
When most people hear ‘elderly’, they have visions of people who are physically unwell and who require a lot of help with their personal care. While this can be true, the reality is that they too are people, who have complex mental health needs which can be accompanied by these physical ailments, but these are certainly not the beginning and end of in-patient care for the elderly. The wards do tend to be busy places but they are a great place to gain the basic principles of patient care which are fundamental to nursing.
The key learning opportunities I experienced were, first, completing assessment documentation (from taking people's life history and physical health checks to completing risk screens and care plans). I found these provide a great basis for the whole of the nursing course, and the earlier you get involved in completing them, the more comfortable you are in asking people questions, and developing your own style for completing the documentation. I found observing lots of nurses complete this process very helpful, as it allows you to reflect upon the parts you thought worked well/did not work well so you can develop in your own practice as your confidence and experience grow.
I also developed an understanding of the Mental Health Act. This is a really good placement to look into the Mental Health Act and all of the different Sections, so take all opportunities to see any assessments and regarding of Sections as they provide an invaluable experience.
There are lots of opportunities for taking physical observations in this placement area. These opportunities do not come about as often as I certainly expected, so my advice would be to grasp the opportunity to practise taking people's baseline observations whenever possible, as it is all important to nursing care. I also found looking at medications and their side effects useful in relation to physical health, such as hypertension, which is certainly common in the elderly but it can also be a side effect of medication so it is important to ask about these.
In relation to personal care, the issues of maintaining privacy and dignity of the clients was really important and also gaining consent for permission to be involved in people's care. This all required me to develop my communication skills both with the people who were using the service and the multidisciplinary team.
Placement 9: Older adult community mental health services
Charlotte Kawalek, third-year mental health branch student nurse
While this area differs from the ward-based placements, it too has many elements in common, and personally was a fantastic placement, allowing me to develop my skills as a practitioner and to increase my confidence in assessments leading to me completing a number of these with little assistance and doing home visits alone.
It is a great place to be able to really get stuck in and apply all that is taught in university and how this can be applied in the context of people's own homes. It can be challenging, but is also a very stimulating area to work.
The placement offers many opportunities. First, to see how people cope in their own home and to offer support to enable them to continue doing this. The development of working relationships is vital as there are normally a number of professionals involved and it is all good management skills. The assessment process and assessing risk is slightly different and it's good to ask mentors to explain this to you, as it is their role if they are care coordinator. The placement also offered a range of experiences seeing individuals with functional and organic illness, and involved close working with carers, which enabled development of communication skills.
Placement 10: Older adult day hospital
Charlotte Kawalek, third-year mental health branch student nurse
This is often thought of as ‘day care’ and can be viewed in a negative light; where people view their main role as providing a few activities, tea and biscuits. However, my experience of working at a day hospital was very different to this assumption.
I found that it was a professionally challenging placement, if you apply what you have learnt over the course of your training to the placement area. I found I was able to complete assessments, work effectively within the multidisciplinary team and apply evidence-based research into practice, which is a fundamental component of nursing today. It was also a brilliant way of again developing interpersonal skills and learning to work as an effective member of the multidisciplinary team, working alongside community psychiatric nurses, the wards and occupational therapists within the team. It also allowed me to attend many review meetings where families were involved and to be able to see how the different services within mental health services all complemented each other and how they work together to aim to provide holistic care.
I learnt that the role of the day hospital is to provide different activities dependent on the client group. On days where people with organic problems attended, the days tended to focus on providing meaningful occupation, including reminiscent activities, exercises and promoting the maintenance of independent living skills; along with assessing clients for day care, or alternative services as a form of respite for carers. On the days where people with functional problems attended, we tended to focus on promoting independent living skills and rehabilitation on a small scale for people, as an interim often between hospital and home.
The day hospital also provided occupation in meaningful activities, but these tended to be focused on art activities and management of different mental illnesses as a form of education for the clients. Furthermore, a memory clinic also ran at the day hospital, which provided assessment of individuals referred to the service by their GP. In addition, a memory support group ran where individuals could attend after being newly diagnosed with a memory problem in order to provide them with education about the illness and planning for the future.
Charlotte describes three different placement settings which involve working with older adults. From her descriptions and discussion with your mentor, try to identify what factors would be considered when assessing which service would be most beneficial to the older adult. You may wish to consider both social and healthcare needs.
Forensic services
Placement 11: Secure 24-hour care settings
Lucy Mangnall, third-year mental health branch student nurse
During my third year I was given the opportunity to have a placement at a high-security forensic special hospital as part of my complex needs placement.
I found the learning opportunities available at this placement were vast and included the chance to spend one-on-one time with psychiatrists and gain a more in-depth understanding of their role. I had opportunities to learn basic pharmacology and relate it to psychotropic medication. I also contributed highly to the care of my mentor's caseload. Along with taking part and taking the lead in ward rounds, security liaison meetings and Care Programme Approach reviews, I also developed my knowledge of the relevant sections of the Mental Health Act and how this was implemented in this area.
A key area in this setting is around risk management and risk reduction and I was able to gain experiences in working with individual patients who had severely challenging behaviours. This may involve escorting a patient outside of the secure area and the difficulties that this imposes, managing a patient who has been assessed as requiring high levels of observation and also observing how the nurse manages a patient in seclusion.
Lucy describes observing how the nurse manages a patient in seclusion.
1. What is your understanding of this term?
2. What does the seclusion policy state in your healthcare trust?
3. When do you think this would be a justified intervention?
4. What are your perceptions of seclusion as an intervention?
5. What do your student colleagues think about seclusion as an intervention?
Complex care settings
Clinical areas of this nature provide interventions and approaches which are developed to meet the needs of a specific client group or mental health difficulty. They often involve nurses and healthcare professionals who have undertaken further education in approaches which are adopted in these areas. Many work in conjunction with other mental health services to give specialist input or provide components of the person's care. The range of these types of services is vast and continuously growing in both the statutory and private sector. Below are some of the most common types of complex care settings which are most likely to be available in your area.
Placement 12: Substance misuse services
Tony Moore, third-year mental health branch student nurse
I spent my specialist placement with the substance misuse service, primarily on a 13-bed in-patient drug and alcohol detox ward, which specialises in drug detoxification and stabilisation and alcohol detoxification. I have always had an interest in substance misuse and people with substance misuse problems. Unlike other placements I undertook, mental health issues, if present, are secondary to substance misuse issues but are still monitored and addressed when necessary. I found the client group extremely interesting and generally they were more than happy to discuss their life and the circumstances that led them to misuse drugs and alcohol. As a student mental health nurse, I was anticipating stories of self-medication for mental health issues, tragic life events and deprived upbringing. Although this is the case with some of the patients, I found that the majority of people took drugs and drank because they enjoyed it but it had become problematic with extensive use.
The ward provides an excellent opportunity to understand the types of illicit drugs used and the process of addiction, detoxification and the medication used, stabilisation on opiate substitutes and blockers. As the ward has only 13 beds and the patients are admitted for between 7 and 21 days, there is ample opportunity to form therapeutic relationships, and by the end of the placement you should be able to perform preadmission assessments and devise individual treatment plans for patients. One of the most difficult aspects of the placement, in my opinion, is trying to convince a patient, who wishes to self-discharge before completing treatment, to stay on the ward. This can be very challenging if the patient, is craving drugs or alcohol as they will be very fixated on this and it can be extremely difficult to talk them around. A real positive aspect is seeing both the physical and mental improvement in people as the treatment, progresses and this can be very rewarding. Although the field of substance misuse may not be ‘proper’ mental health, it is an interesting and progressive service and makes an excellent placement.
Tony describes his placement working with a substance misuse team, however we have also heard other students talk about working with people with a ‘dual diagnosis’. This often refers to people who have a mental health problem and a substance misuse problem. The link between the two is contentious and there is a high level of debate surrounding this issue.
1. How do you think substance misuse can impact on mental health?
2. What is your impression of what the media say about how substances can affect mental health?
3. Discuss this with your mentor and identify how the media might influence your perception towards people with a dual diagnosis and the way you would work with them.
Placement 13: Child and adolescent services
Tim Westwood, third-year mental health branch student nurse
I found child and adolescent mental health services (CAMHS) a strange place when I started my placement as it was so different to adult placements I had been on. I was amazed at the absence of clients with diagnoses. Where were the schizophrenics, clinically depressed and the personality disorders? The truth was that children usually don't have a diagnosis as there is no benefit in giving children adult labels. What you are left with is the sad children, the angry children and the ‘not doing as well as they should be’ children.
The absence of a diagnosis means that treatment is non-medication based and the most surprising thing of all is that the first treatment offered is not for the child at all but for their parents. Parents are offered training on how best to support their child. Talking treatments then focus on the family dynamics and identifying any traumatic events that have occurred in the child's life. Treatment is a long-term commitment for the family and CAMHS. The symptoms of childhood mental distress I observed included poor concentration levels at school, anger towards parents and siblings, hyperactivity and nightmares.
What you get with a CAMHS placement is a chance to work with individuals at the early stages of mental distress. You will be working with the unformed mind and success at this stage could prevent the child enduring mental illness in the future. It is a challenging placement as dealing with childhood distress is difficult. You will hear stories that will break your heart but, saying that, I can't recommend it enough and it is an experience not to be missed.
Tim describes finding working with children personally challenging as a result of working with children in distress. It is evident, however, that he found this experience a valuable learning opportunity.
In order to prepare for a placement working with children, what might you need to consider in terms of your own support needs?
Placement 14: Mental health liaison teams
Ben Thompson, first-year mental health branch student nurse, and Keith Waters, mental health liaison team leader
A placement with the mental health liaison team offers a wide range of learning opportunities, with exposure to a full spectrum of mental health presentations, often occurring in crisis, many of which will be coming into contact with services for the first time. It provides an excellent chance to develop and consolidate assessment and diagnosis skills, and regular exposure to risk management and recommending treatment options. The team works largely in isolation although there is some multidisciplinary working with other mental health services. However, there is regular interaction with colleagues operating within the general hospital setting including exposure to areas of general nursing you would not normally see, including the emergency department, medical wards and intensive care units.
The placement can be emotionally demanding as the student is often working with clients who are experiencing extreme emotional distress. In many ways it is a privilege to be present and influential at what is a pivotal life event for many clients and it can be rewarding when clients express gratitude for the assistance and support the team provides. The work of the team is also well received and much respected by medical staff in the hospital who may have minimal mental health training and can find managing mental health clients an anxious and difficult experience.
The workload on the team is variable and unpredictable which means there are quiet times. Take this opportunity to pick up on any questions you may have, or to do some background reading. The flip side of this is that at busy times you may not always get away on time.
Ben describes how this placement offered him the opportunity to work with colleagues from the adult field of nursing in settings such as the emergency department. Before commencing your placement, reflect with your student colleagues on the following points:
1. If you have mental health problems or are extremely emotionally distressed, how might you feel in the emergency room environment?
2. How might this influence the way you might act or respond to healthcare professionals?
3. What approaches might be helpful when working with a person with mental health problems in this environment? You might want to consider:
Placement 15: Motherhood and mental health
Charlotte Bridges, third-year mental health branch student nurse
The mother and baby ward is an acute mental health ward that cares for mothers that have become mentally unwell or relapsed due to pregnancy or birth. On the ward that I was on, the mother and baby come to the ward together – the mother is not admitted without the baby. The criteria are that the baby must be under 7 months old and mothers are admitted during pregnancy. The ward and the mother and baby community team work very closely together to ensure that all staff are informed of potential admissions or supported discharges. The aim of the service is to provide a safe environment for the mother and baby that aids the recovery of the mother, promotes bonding between mother and baby and offers support and advice about care of the baby. This is done by medication, therapies/interventions, support and education.
The placement has really opened my eyes to working with positive risk. The mothers need to keep contact with their babies to aid with the bonding process, however, when a mother is mentally unwell, this can pose many risks to the baby. This is also applicable when breastfeeding; some medications advise that mothers don't breastfeed therefore you need to look at whether they really need that medication or whether they can change to a different one and consider the different debates that arise from this type of dilemma.
Charlotte mentions that medication is used to help mothers recover from the mental health problems they are experiencing. Some medications are not used if the woman is pregnant or breastfeeding, due to the potential harm they could cause the baby.
Use the British National Formulary (BNF) 2011 and discussion with your mentor to identify these medications and what alternative medications or interventions are used.
There are some mental health problems which are only experienced by women who are pregnant or have had a baby, such as postnatal depression and puerperal psychosis.
Use the International Classification of Mental and Behavioural Disorder (ICD) 10 and discussion with your mentor to identify what these mental health problems are and how a person who is experiencing one of these problems may act and feel.
Advice for students from Polly Murray, a staff nurse working in a mother and baby in-patient unit
• Look at the mother's care plans and talk to staff about how much support is needed with baby care. Some women may require lots of support to meet their baby's needs; others may request lots of help but may actually be more capable then they think they are. In the latter instances, you may feel that you are helping by ‘taking over’ baby care, however it is not necessarily in the mother or baby's best interests. Intervening can reduce the mother's confidence, prevent maternal bonds from forming and, if this is maintained, there is even a danger that the baby may start to bond with you. Instead, offer to stay with the mother, talk her through the task in hand and reinforce how capable she is.
• Try to have a basic understanding of maternity issues and baby care prior to starting the placement, or get someone to explain issues (such as feeding, weaning, winding and changing nappies) to you at the start of the placement. Maybe look back at your documentation from your maternity placements.
• The majority of women who use the unit do not pose ongoing/significant risks to their children, however occasionally referrals will be made to social services regarding safeguarding issues. This is a great opportunity for students to learn how to assess risk, make referrals to children's services, the role of children's services and how social and mental health services support families to reduce such risks.
• Attend allocations meetings where the community team discusses new referrals to the service. This will give you a good understanding of the referral criteria and the variety of mental health problems which the service caters for.
• Organise to go on home visits with specialist perinatal community psychiatric nurses. This will develop your understanding of assessments, the different presentations of women treated at home and in hospital and how risk is managed in the community.
Placement 16: Psychotherapy
Sarah Moore, third-year mental health branch student nurse
As a third-year student and having an interest in cognitive behavioural therapy for some years, I felt gaining a placement with a psychological therapies service was an invaluable opportunity for me to be able to gain experience in how different therapies work and what sort of mental health problems they are particularly useful for. The service employed counsellors, psychodynamic therapists, low-intensity cognitive behavioural therapists and high-intensity cognitive behavioural therapists.
Some people may think therapies are about a client talking and the therapist listening. Listening is a key skill in any therapy but by no means is this the be all and end all. With any therapy it is about gathering information about the client and details of what the problem is, sometimes supporting the client to find where the problem lies. However, all therapies are underlined with different theories and these alter the techniques used by different therapists.
My main aim when on placement was to find out more about cognitive behavioural therapy, the theories that underline it, how it is used and what mental health problems it works best with. During my time I had the opportunity to discover these. Other learning opportunities included completing assessment documentation (from taking people's life histories, important events, mental and physical questions, risk screening and treatment plans). The more of this you get involved with the more comfortable you become with carrying it out. This would be called gradual exposure and is actually a cognitive behavioural technique used in anxiety-related problems. Different practitioners have different methods of completing assessments and observing many has helped develop the way I prefer to carry them out.
Being involved in providing therapy is definitely a great opportunity to develop communication skills such as verbal, listening, body language and even knowing when to divert away from a particular subject when it is too much for the client.
I was able to understand how different therapies worked and why different therapies worked better with some mental health problems than others. I had a great experience and I plan on doing my cognitive behavioural training in the near future.
Placements 17: Voluntary sector
Mark Lambert, Team Leader, Framework Housing Association
Placements in the voluntary sector are very different to placements within a NHS setting, because a person's mental health and how that is managed is not the primary focus of the support provided. The support provided within the voluntary sector focuses on the practical aspects of daily living/issues while taking into account how a person's mental health can impact on their ability to manage these issues. Therefore, within these placement settings, you get to see the whole person as an individual and not just the person and their illness.
Voluntary services are based in a community setting and are reliant upon developing good lines of communication with statutory services which are responsible for supporting people with their mental health. The voluntary services are typically hostels which provide support housing solutions or floating support services which support people in their own homes. Services such as these are typically funded from central government funds that are prioritised to area of need as defined by individual local authorities. (This is not inclusive of all voluntary sector organisations but is true for those that are funded to provide support around housing/independent living.)
The support in services funded in this manner focuses on housing needs, money management – budgeting, debt, maximising income, getting into work – and social inclusion.
As the voluntary sector is based within a community setting you meet people who are at differing stages of their recovery and are therefore linked in to differing statutory services which you would liaise with (i.e. acute wards, CMHTs, day centres, out-patient clinics).
You also have the opportunity to support people to contact benefit agencies, housing departments and agencies connected to debt (be that specialist support agencies, a person's creditors, debt collectors, etc.). This will enable you to gain a good insight into the aspects of daily living that impact upon a person's mental health and how a person's mental health impacts on their ability to manage situations and their day-to-day life.
Currently services in the voluntary sector are privileged to be able to spend a greater amount of time with individuals than workers within community mental health teams, therefore grasp this opportunity.
Top tips
The following top tips are from student mental health nurses and aim to help you make the most out of your mental health placement.
Placement support
• Use the supervision offered to discuss any issues that arise during the placement – it can be distressing to hear service users talk about their experiences.
• Seek support from your mentor or personal tutor if you experience difficult or challenging situations that have the potential to affect you in a negative way.
Attitude
• The main thing which is helpful is respecting the service user as an individual and seeing past the diagnosis.
• Don't make assumptions or have preconceived ideas based upon what you have heard or been told. Remain open minded and make your own judgements based upon your own personal experiences of the placement.
• Empathise, don't judge. Try and understand how they are feeling and put yourself in their situation. Showing someone you care means so much.
Approach
• A good way of developing effective therapeutic relationships is through working on documenting the person's life history. This provides insight into the person and allows care to be more holistic.
• Speaking to carers/family members is also a key role of the nurse. Also it allows you a deeper insight into the service and, thus, you are able to engage them in holistic care as you have a greater understanding of them as a person.
Enhancing learning opportunities
• Remember that, as with every placement, you will get out of it what you put into it. See each day and every opportunity as a new learning experience. You only have the chance to be a student nurse once!
• Know what you want from this placement – the opportunities are there for the taking.
• Learn from the good practice of existing staff.
• Opt for a variety of shifts to become familiar with the different dynamics of working environments. Also at weekends there will be more time for discussion and learning support.
• Use reflective practice within portfolio work to reflect on and establish your new learning – you'll be surprised at how many aspects of learning you cover in a day.
• Answer the office telephone. This gives you the opportunity to engage with a range of multiagencies. Following up on jobs created through this process will create opportunities for further learning.
• Don't be afraid to take a lead and ask your mentor and the rest of the team if there are any suitable service users for you to work with as a named nurse.
• Volunteer to do the notes. The nurse will appreciate the help with the paperwork and you will learn how to document and think about what this means for your accountability. Read previous entries to see how others have written and documented their contacts.
• If you feel confident, ask to do more. It may seem daunting, but things such as speaking up in the multidisciplinary meetings and actually taking the lead in initial assessments will build your confidence and give you the experiences you need.
• In the community, the car journeys are a great time to ask questions about your mentor's experiences as a nurse and current issues in mental health. Mentors prefer students who are inquisitive and want to learn.
• Be prepared to challenge and educate people's current views – this could be a service user, family member or anyone involved in the service user's care.
• Try to do some background reading of the assessment approaches, theories and models that underpin different therapies.
• Be prepared for quiet times – have a book to hand and keep a list of questions for reference that you may not have had a chance to ask at the time.
• Revise your knowledge of sections of the Mental Health Act and the Mental Capacity Act and look at the duty of care under common law and broader ethical issues.
• Go on visits with as many different members of the team as possible. As everyone works differently, you will get to witness lots of different styles and see how people have to adapt to different clients.
Working effectively with your mentor
The following questions aim to help you develop a shared understanding with your mentor of the mentorship process and how it will work in your individual circumstances. These questions should be discussed within the first week of placement and completed as a record of your agreement which you can revisit and revise throughout.
• What are our expectations of each other?
• What are our expectations of the mentoring process?
• How often will we plan to meet both formally and informally?
• How will we communicate in between meetings?
• What time will be available for learning individually in the workplace?
• How will feedback be given on aspects of my practice?
• How will we organise additional support following a challenging situation?
• Are there any other areas that we feel are important to identify to support learning in this placement area?
Action planning
As you move through your programme you will become increasingly aware of your developing learning needs. It is important to define these and communicate them to your mentor. It is also an effective skill for the future as it will encourage you to be a more self-directive learner and less reliant on your mentor to identify learning opportunities. Here are some suggestions of things you may want to think about:
Professional development
• What are the priorities for learning that I have already identified from previous placements?
• Which competencies am I focused upon achieving?
• What immediate learning opportunities are there in this practice area that will enable me to meet these competencies?
• What additional learning opportunities will I need to seek elsewhere to enable me to meet these competencies?
• What support will I need from the team to settle into the practice area and achieve my competencies?
• What evidence will demonstrate I have achieved these competencies?
Clinical development
• How will I engage with current service users in the practice area?
• How will I develop my independence and confidence in this practice area?
• How will I enhance my confidence in clinical skills?
• What are the specific clinical skills that I am concerned about?
• How will I enhance my skills and confidence in leadership and case management?
Personal development
• What are my career aspirations and how will I work towards these?
• What are the practice development opportunities I would like to be involved in?
• How will I develop professional networks relevant to my role?
• How will my progress in this area contribute to my portfolio?
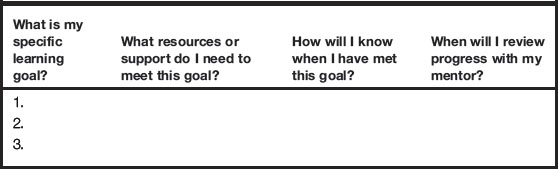
For each of the learning needs you identify you should consider the questions given in Table 4.1 and summarise your answers to discuss with your mentor.
Darzi A. High quality care for all. NHS next stage review final report, summary. London: Department of Health; 2008.
Department of Health. National service framework for mental health: modern standards and service models. London: HMSO; 1999.
Longley M., Shaw C., Dolan G. Nursing: towards 2015. Alternative scenarios for healthcare, nursing and nurse education in the UK in 2015. Pontypridd: Welsh Institute for Health and Social Care; 2007.
Nursing and Midwifery Council. Standards for pre-registration education. London: NMC; 2010.
Biernacki C. Dementia:metamorphosis in care. West Sussex: John Wiley & Sons, 2007.
Dogra N., Leighton S. Nursing in child and adolescent mental health. Blackwell,Oxford, 2009.
Dogra N., Parkin A., Gale F., Frake C. A multi-disciplinary handbook of child and adolescent mental health for front-line professionals, 2nd ed., London: Jessica Kingsley, 2008.
Kitwood T. Dementia reconsidered: the person comes first (rethinking aging). Buckingham: Open University Press; 1997.
Levett-Jones T., Bourgeois S. The clinical placement: a nursing survival guide, 2nd ed. London: Elsevier; 2009.
McDougall T., ed. Child and adolescent mental health nursing. Blackwell, Oxford, 2006.
McGarry, J., Clissett, P., Porrock, D., (In press). Pocket placement guide for care of the older person. Elsevier, London.
Royal Pharmaceutical Society. British National Formulary 61. London: Pharmaceutical Press; 2010. Online. Available at: http://bnf.org/bnf/bnf/current (accessed June 2011)
Sharples K. Learning to learn in practice. Exeter: Learning Matters; 2009.
World Health Organisation. International classification of mental and behavioural disorder (ICD) 10. Geneva: WHO; 2007. Online. Available at: http://apps.who.int/classifications/apps/icd/icd10online (accessed June 2011)