6 Preparation of the patient for surgery
the hospital experience
• To explore the continuity of care from a pre-admission assessment to being admitted for surgery
• To explore the care delivery after admission to hospital and being prepared for the operating theatre
• To determine all the preoperative procedures and protocols required to ensure a safe transfer from ward to anaesthetic room and operating theatre
• To consider the actual and potential problems that patients may experience prior to undergoing surgery
Introduction
Chapter 5 introduced you to what happens prior to patients being admitted for surgery, including pre-admission assessment and identifying what may be required in readiness for their discharge home from hospital. This chapter focuses on what happens when someone actually enters the hospital, undergoes admission to the ward or unit where they are to stay prior to and after surgery and their preparation prior to surgery. For most patients and their families, this can be a very stressful time, and even more so if their admission to hospital has been an emergency.
Care of the patient on admission to hospital
Admission to hospital is part of the ‘perioperative’ period of care (i.e. three phases of preoperative, intraoperative and postoperative) (Pudner 2010). The admission may be planned, with most patients having had a preoperative assessment to ensure specific needs or problems are identified, stress is reduced by information sharing and, in these times, to reduce the risk of a hospital-acquired infection (Pudner 2010:3). Another term for this is ‘elective’ surgery. It may also be an admission for ‘emergency’ surgery which has not been planned.
Read Gilmour's (2010) explanation in Box 6.1 before considering the nursing care aspect of the preoperative period.
Box 6.1 Elective or emergency surgery (Gilmour 2010:18)
Elective surgery aims to be performed when the patient is in optimal health but before the surgery affects the quality and threatens their life: e.g. an inguinal hernia can become life-threatening if the bowel becomes obstructed within the sac. Clinicians decide if a planned procedure is urgent or can be arranged at a time convenient for the surgeon and patient (Phillips 2004).
Emergency surgery may be as a result of trauma or an accident, gastrointestinal obstruction or from perforated viscera. The injury may be immediately life-threatening, and therefore the procedure will be carried out with 1–2 hours from admission. Other emergencies may require procedures within 24–48 hours following the injury, but in both instances the preoperative time for preparing the patient is significantly reduced and changes to the patient's condition occur rapidly. Information may be limited; the perioperative nurse must be prepared for any event or occurrence, and therefore communication within the perioperative team is essential to coordinate the delivery of safe patient care during this potentially traumatic period (MacDonald 2005).
So what role does the nurse play in a planned admission?

If this is your first or second surgical placement, find out prior to your first week what kind of surgical procedures are identified as planned or ‘elective’. Your university placement learning website may offer some information but you may also need to visit the placement, introducing yourself to staff at the same time. Make a list in your notebook and find out as much as you can about the underlying pathophysiology (i.e. what has gone wrong with the body's normal physiology) and what procedures the surgeon is likely to undertake. (See Further Reading for some medical textbooks illustrating surgical procedures, and websites for further examples.)
Planned admission
Patients may undergo planned surgery on a day care basis, a short stay basis or they may stay longer in hospital. It is important to consider the impact of introducing a ‘surgical’ journey which can now take place in a single day. In the past, most surgical procedures required patients to stay in for longer. The parallel developments in surgical techniques and technology have revolutionised care and the kinds of experiences students now experience in clinical practice placements.
It should be noted, however, that changes to length of stay in hospital have created different expectations of nurses who work in a community setting. If your placement is in a community setting, you will meet patients who now require a higher level of nursing care or observation postoperatively, including support for their carer at this time. In the past patients would stay in hospital for nurses to observe for postoperative complications such as wound infection and removal of sutures. This has become more the responsibility of the community team.
Care of the patient within 12 hours of being prepared for surgery
Most patients arrive at hospital with a relative or friend. Some patients who have been in hospital a long time ago may expect to be asked to change into their pyjamas, slippers and dressing gown as soon as they arrive! This is no longer always the case, unless of course they may have to undergo tests or examinations as soon as they arrive in the ward. It is important to remember, however, that some elderly patients faced with a hospital stay may have purchased new nightclothes to be a patient – they may not feel that they are ‘properly ill’ or a ‘proper patient’ unless they are dressed for bed. Being sensitive to their needs is important.
Instructions sent to patients by the hospital inform them of what clothes to bring in and other important information (see Box 6.2 for examples). Knowing this information is helpful during the assessment of a patient on admission to hospital.
Box 6.2 Key patient information for hospital admission for surgery
Pre-arrival
Patients should complete any documentation sent pre-admission to take with them – this may include special dietary needs and any recent infections.
Patients may have been advised to give up smoking, lose weight or have other health problems checked for stability, for example diabetes.
Clothing and personal items: information on what to bring, such as pyjamas or nightdress, dressing gown, slippers, personal toiletries. If a longer stay is possible, patients should bring some casual clothes for their time of recuperation pre-discharge home. If having knee or hip surgery, for example, they could also be asked to bring shorts or track suit type clothes plus comfortable supportive shoes for wearing during postoperative physiotherapy sessions.
Medications: it is very important that patients bring all their medications (plus any original information).
Valuables: patients are advised not to bring valuables or large sums of money if at all possible.
Mobile phones and any electrical equipment: these may interfere with hospital equipment and their use may be restricted in key areas.
On arrival
If arriving on the day of surgery or the day before, patients will be admitted by a nurse and all information about them checked, especially their understanding of the impending surgery. Contact details are obtained and a patient identity bracelet must be worn at all times during the stay.
The day before: patients may be allowed to eat and drink as normal until told otherwise and depending on the type of surgery.
The same day: patients may not be allowed to eat for at least 6 hours prior to surgery and may only drink clear fluids up to 2 hours preoperatively. Again this is dependent on the type of surgery.
Patients should be informed about the surgery, possible side effects such as nausea/vomiting, pain and pain control, specific postoperative exercises, avoiding deep vein thrombosis and advice on smoking. Depending on the type of surgery, there may be further information.
Going to the operating theatre
Informed consent: the patient will need to understand the nature of their surgery and sign a consent form either in the pre-admission assessment or on admission following a visit by the anaesthetist or consultant surgeon. It is important to check this.
The anaesthetic procedure should be explained to the patient as well as what will happen in the operating theatre and why they may get pain postoperatively. The effects of anaesthesia should also be explained, especially nausea and why the throat may be sore post-operatively after having an endotracheal tube in place during the anaesthetic.
Their named nurse and/or student may accompany patients to the operating theatre along with theatre personnel.
After surgery
A brief explanation of what happens in the operating theatre, who is present and what to expect postoperatively on the ward may be included. The effects of surgery and anaesthesia should be explained briefly as well.
Going home
Going home from hospital following surgery will already have been discussed on admission – it is essential that patients consider this before surgery and discuss with the nurse on admission any issues relating to home care and, possibly, home care facilities and requirements on discharge home. Some types of surgery will have specific going home instructions, e.g. after removal of part of the bowel, patients will be advised how to manage dietary intake and stoma care (if they have one).

When you begin your placement experience, find out what hospital policies are in place with regards to patients admitted for surgery and, in particular, any that directly involve the role of the nurse and other healthcare professionals. Discuss how to obtain access to these with your mentor.
Find out as much information as you can about patient information leaflets available for patients on your ward so that you are prepared to answer their questions.
A NHS Choices video explains how patients can prepare for admission to hospital:
http://www.nhs.uk/Video/Pages/Preparingforhospital.aspx (accessed December 2011).
Here are some other approaches linked to care delivery that you may come across in practice or in your reading. Identify their meaning and make some notes. These are often used as part of student assignments involving delivery of patient care (see Appendix 1 at the end of this chapter for brief notes on each):
Appendix 1 Brief meaning of nursing care approaches
1. Named nurse: this term is used mainly in the UK and, according to some authors, has been adopted to mean the same in terms of care delivery as primary nursing has in the USA. The patient is allocated a named nurse on admission to hospital, and Shebini et al (2008) cite the Scottish Office (1992) definition as: ‘A registered nurse, midwife or health visitor who is responsible for assessing, planning, implementing, evaluating and coordinating patient care on an individual basis with a patient or a caseload of patients from admission/transfer/discharge’.
2. Primary nursing: this is a system where the total care of an individual patient and his/her family is the responsibility of one nurse – the primary nurse. They are accountable for the overall care and have the authority to make decisions as the ‘leader’ of the care provided. They are possibly the primary nurse for a small group of patients, delivering individualised and patient-centred care for the whole of their contact with the patient. They are supported by secondary nurses who carry out the care planned by the primary nurse, even when the primary nurse is not available due to off-duty rotas, for example. Some secondary nurses are also primary nurses for their own patients, and decision making and leadership is therefore an integral part of the primary nursing approach to care delivery. The original philosophy of primary nursing is described in a YouTube clip by Professor Marie Manthey (who led a project about the development of this approach and has since become known as the originator of it internationally): http://www.encyclopedia.com/video/kr7t8E5MMoM-primary-nursing-short-story-by.aspx (accessed December 2011).
3. Team nursing: this is a system of providing care as a group of healthcare workers (registered and non-registered) where there is a nominated team leader, normally a qualified nurse. The team leader is responsible for leading the team's work and also for taking overall responsibility for the planning, delivery and evaluation of the care given. The team leader normally agrees the assignment of care duties with the team and reports directly to the ward manager/sister or person in charge. Team nursing enables development of leadership and management skills, but individual members of the team remain individually accountable and/or responsible for the care they give.
4. Patient allocation: this is a system where each nurse is allocated a small group of patients to deliver care to, usually on a shift-by-shift or day rota basis. It is not as defined as team nursing where the team leader's role is normally a set one and the team leader's name is identified on the staff rota list. It allows for an opportunity, in particular, for student nurses to take responsibility for a small group to patients under the guidance and supervision of their mentors, learning not only about the delivery of quality care but also a range of skills such as those adopted by a team leader (e.g. delegation skills, working with others, communication and accountability).
5. Task allocation: this is a very ‘traditional’ method of care delivery and is focused not on the individual patient and their care but on the task required in their care. For example, a member of staff could be allocated to take every patient's temperature, pulse and respiration, another to take everyone's blood pressure and another could be tasked with ‘doing the medicines or medicine round’. Task allocation often leads to a hierarchy of tasks and who does them, with less junior staff being delegated those which are considered ‘mundane’ or less important than others.
It is important to note that in many care delivery settings, a combination of these approaches can be found working very well in accordance with patients' needs as well as ensuring that quality care is delivered.
Depending on the ward/unit, patients may be allocated a ‘named nurse’ who will coordinate the delivery of care from admission to discharge home. The named nurse approach to care delivery is one of many terms you will come across during your learning in practice and in theory.
Once a patient has been shown to his or her bed and shown around the ward/unit so that they are familiar with bathroom facilities and the day room, the nurse can introduce them to other patients if appropriate. If the patient is going to theatre on the same day they are admitted to hospital, they will not have much time to communicate with others but will have to undergo preoperative preparation by the nurse.
It is important for relatives or carers to know visiting times or the best time to phone to find out how the patient is, as people accompanying patients on arrival soon have to leave. Even prior to the formal patient assessment, it is important to determine any special and immediate needs of patients or anything relatives might wish to let the nurses know about. One example could be whether the patient requires a translator or not and whether they speak or read English. During the assessment process, it is essential that all patients are able to understand what is being asked of them or what they may be required to sign. It may be that someone attending with the patient is required to stay with them until they actually leave the ward to go to the operating theatre.
Imagine you are a student nurse on placement in a female general surgical ward. Your mentor has asked if you would like to assist her in admitting a woman to the ward who is to go to theatre later that afternoon for a thyroidectomy. She has already attended a pre-admission clinic 2 weeks previously and is likely to have to stay in hospital for at least 2 days postoperatively. You agree to work with your mentor as this is one of the learning goals you have set yourself on this placement. You also agree with your mentor that this would be an excellent opportunity to follow a patient's journey and care until she is discharged from hospital. Your mentor has agreement from the theatre team for you to attend the surgery and immediate postoperative care with the patient in the recovery ward.
1. What do you think is essential to know prior to meeting the patient and undertaking the admission assessment?
2. What approach to assessment is the mentor likely to consider to help her make a full assessment of the patient?
3. As a student nurse, what will be your priority within the team to discuss with the patient?
4. What specific potential problems is this patient at risk of developing postoperatively and what observations will nurses be undertaking to detect them?
Some general issues to consider
It is essential to know the patient's pre-admission assessment information, which should include the physiological, psychological and social needs of the patient, and any information which could be important for her wellbeing during and after her operation. Familiarising yourself with this information is very important in order to ensure that any sensitive issues are noted as well as important health ones.
1. A key check with the patient is to ensure that she has followed the specific pre-admission instructions she was given with regards to preoperative fasting. The Royal College of Nursing (RCN) guideline on perioperative fasting in adults and children, which is based on a range of evidence, recommends for adults: ‘Intake of water up to 2 hours before induction of anaesthesia and a minimum preoperative fasting time of 6 hours for food (solids, milk and milk-containing drinks’ (RCN 2005:4).
Contact details of relatives or other carers are important.
2. Your mentor will use the assessment document and procedure used in your particular placement. This may use a standard care plan, an integrated care pathway document, an electronic assessment tool and/or a nursing model/framework for assessment (e.g. the Roper, Logan and Tierney model of nursing (Holland et al 2008)). Regardless of how the assessment is documented, it is important to consider the nursing process of assessment, planning, implementing and evaluating in devising both the assessment stage and the care plan generally. Your mentor will also ensure that the patient has signed the consent form for surgery and that she fully understands the surgery to be undertaken.
3. As a student, it is important to ensure that the patient is aware that you are a student nurse and a team member. It is also important to let her know that you will be going with her to the operating theatre, anaesthetic room and staying with her until she is back on the ward again. Ensuring she is happy with this arrangement can be discussed with your mentor.
4. Postoperative problems and detection: in the immediate postoperative period, there are general postoperative problems that can occur for any patient who has undergone an anaesthetic and surgical intervention that nurses have to be alert to. Examples are shock, pain, nausea or difficulty breathing. For someone who has had a thyroidectomy, there are specific potential ones such as damage to the laryngeal nerve, a haematoma pressing on the trachea, thyroid crisis, risk of tetany (Refer to Ch. 13 in Pudner (2010) for an excellent outline of the total nursing care of patients using the Roper, Logan and Tierney model of nursing).
With regards to the exercises above, see also Ch. 5 in this book for more general comments on pre-operative assessment.
Immediate preoperative care of the patient prior to surgery
Once a patient has been assessed and any immediate needs identified, they will need to undergo preparation for transfer to the operating theatre.
There are a number of books which consider this (see Further Reading), so here we consider the main issues while some others are considered in earlier chapters.
Depending on the kind of surgical intervention the patient is having, there are both general and specific preoperative preparation needs. For example, someone going for an operation involving their hip joint will need different considerations to someone undergoing surgery on their eyes. Let us look at what you will be involved in as general preoperative preparation.
Depending on where your main placement is in the perioperative period and also the kind of surgery that takes place there, you will meet patients at a number of different stages. Understanding the whole pathway of care is essential for understanding the experience patients undergo. For example, if you are caring for a patient in a ward, being able to explain why they may feel bruised or have ‘aches and pains’ in places they didn't expect – as a result of their positioning on the operating table for a period of time – will help to allay their fears.
A brief introduction is offered here together with further reading for you to pursue prior to commencement of your placement.
General preparation
Psychological preparation
We use the term ‘psychological’ here to outline some of the reassuring activities you can undertake regarding the impending surgery, as opposed to the physical preparation activities that you are required to undertake.
Consider the example given in Box 6.3 and think about what could have helped this patient to be less anxious.
Box 6.3 Practice example: preoperative preparation of a patient going to theatre
Mrs Peters, a 45-year-old woman, was admitted to hospital for a hysterectomy. Her initial pre-admission assessment showed that the outcome of this surgery had been discussed with her, and the possibility that the gynaecologist would also have to remove both her ovaries, thus causing an early menopause. Some literature had been given to her to read about this by the pre-admission assessment nurse, but she hadn't fully understood the implications of this. She had had no time to discuss it with anyone as she was admitted for surgery 2 weeks after the assessment. She signed the consent form at this time as well, thinking she was clear about her surgery.
On admission to the ward, the nurse (your mentor) undertook a further assessment of her immediate preoperative needs and this worry and anxiety about not having her ovaries after the surgery was highlighted. She made every attempt to reassure the patient and contacted the consultant and his team but none had been available to come to the ward to talk to her.
The pre-surgery physical preparation had to continue despite her concerns in order to ensure she would be ready when it was her turn to go to theatre. She was still anxious when you and your mentor took her to the operating theatre/anaesthetic room.
Read the articles by Leinonen and Leino-Kilpi (1999), Mitchell (2000) and Pritchard (2009) (see References) to help you to provide an evidence-based response for reducing preoperative anxiety.
Physical preparation
As well as managing potential anxiety and worries preoperatively, there are specific preparation requirements that nurses and others have to undertake. It is not possible to offer specific preoperative preparation for all types of surgery here, so we mainly focus on the general but give some specific examples. It is important that you read about the kinds of surgery you will encounter on your clinical placement and focus on understanding both general and specific preoperative preparation of patients, why they must take place and the possible outcomes if they are not undertaken. It is also important to adopt an evidence-based approach to nursing practice (Holland 2010). The main physical preparations to consider are:
Preoperative fasting
Patients can normally have clear fluids up to 2 hours preoperatively and solid food/milky drinks up to 6 hours preoperatively (RCN 2005), but this depends very much on the nature of the surgery to be undertaken. For example, patients undergoing major bowel surgery will have more intensive preoperative preparation than someone undergoing surgery for removal of varicose veins.
Preoperative fasting is important to ‘ensure safety during induction of general anaesthesia by preventing inhalation of acid stomach contents into the lungs when the gag reflex is lost’ (Amos & Waugh 2007:686) (see Chs 7 and 8 for further explanation).
Find out about the care of a patient with diabetes who is undergoing surgery.
Imagine you are the named nurse (supervised by your mentor) for a patient with diabetes who is to undergo major surgery, a below-the-knee amputation. Make a plan of his preoperative care needs and how you will manage his care relating to the stabilisation of his diabetes during the perioperative period.
An excellent resource for undertaking this exercise is the NHS Diabetes website: http://www.diabetes.nhs.uk (accessed December 2011). Search for ‘Management of adults with diabetes undergoing surgery and elective procedures: improving standards’ (NHS 2011) to download the pdf.
In terms of your role in the preoperative preparation of a patient who is not allowed fluids, you can ensure that the water jug is not left on the patient's bedside table. In many hospitals, you will find a sign above the patient's bed saying ‘nil by mouth’, meaning they must have nothing to drink or eat. It is also important to note that some patients are at risk when they are unable to eat or drink: in particular, patients who are diabetic and insulin dependent. They will have their normal routine disturbed by the lack of food and drink, and may have intravenous fluid and nourishment, intensive monitoring of their glucose levels and linked insulin dosage (sliding scale of insulin) during the whole of the perioperative period.
Bowel preparation
Preparation of the bowel prior to surgery, in particular abdominal surgery, is important for the following reasons (Amos & Waugh 2007:688):
• Defecation during anaesthesia.
• Faecal contamination during surgery, particularly for surgery on the gastrointestinal tract.
• Postoperative stress on the wound.
• Postoperative discomfort or constipation due to a full rectum.
Patients may be given laxatives to take prior to coming into hospital as part of their bowel preparation, especially if going to the operating theatre not long after admission. Patients who are admitted the day before surgery and require more extensive preparation may be given oral and/or bowel laxatives to aid the process.
Skin preparation (including hair removal)
Preoperative skin care is undertaken at two levels: cleaning the skin itself and removing body hair from the surgical site (Amos & Waugh 2007). If a patient has to self-prepare prior to admission for immediate surgery, they are advised ‘to have a bath or shower to remove dirt and microbes from the skin and to wash their hair, because this can act as a reservoir for bacteria (Simmons 1998)’ (Scott et al 2007). If the patient is already in hospital, they will require a similar preparation and as part of the immediate preoperative preparation will be given a clean theatre gown to wear and required to remove all clothing as necessary. Scott et al (2007) state that the evidence is inconclusive with regards to removal of body hair – one view is that it should be removed because hair harbours bacteria which could be introduced into the wound, and the other view is that getting rid of hair increases the risk of infection by reducing the body's natural defence mechanisms.
It is important to understand that removing body hair is not allowed in some cultures, for example the Sikh religion. This would be an issue for negotiation with the patient and possibly the Sikh chaplain (see http://www.sikhchaplaincy.org.uk/Booklet.pdf (accessed December 2011)).
Read the articles by Dean and Fawcett (2002), Murkin (2009) and the RCN (2005) (see References) which are relevant to these areas of preoperative preparation. Make notes on the key points of the underpinning evidence base to nursing actions in each case.
Final preoperative preparation of the patient (identified in Amos & Waugh 2007)
Emptying the bladder
It is important that patients go to the toilet immediately prior to going to theatre, to ensure they do not become incontinent during surgery (if there is a long delay, they may need to go again). ‘For patients having extensive pelvic surgery and an epidural or spinal anaesthesia, a urinary catheter is passed (usually in theatre) to ensure that the bladder remains empty and that urinary output can be measured accurately postoperatively’ (Amos & Waugh 2007:691).
Theatre clothing
As noted earlier, patients are required to put on a clean operating theatre gown. Antiembolic stockings may also be required (and patients need to wear the right size).
Find out about the policy on your placement with regards to wearing antiembolic stockings and ask your mentor to show you how to measure and put these on a patient prior to surgery.
The information on the NHS Choices website will help you with the National Institute for Health and Clinical Excellence (NICE) evidence base for wearing antiembolic stockings:
http://www.nhs.uk/chq/Pages/2609.aspx?CategoryID=69&SubCategoryID=692 (accessed December 2011).
Removal of cosmetics, jewellery and prostheses
All cosmetics must be removed so that any pallor can be seen and, importantly, nail varnish must be removed to ensure any signs of cyanosis can be seen. Jewellery is also removed but, if requested, a wedding ring can be kept on and taped securely. Any jewellery removed is either sent home with relatives or kept in a hospital safe, depending on hospital policy. Removal of metal objects prevents contact burns from diathermy equipment or damage to the patient if caught on a piece of equipment (Amos & Waugh 2007).
Allergies
Allergies should be checked again as patients may have forgotten to mention these if worried about their impending surgery. Some allergies can be caused by skin preparation liquids used in theatre.
Identity bands
Patients must wear these on admission as they are vital to ensure that the right patient goes to the operating theatre. They are very important when a patient is unable to communicate effectively as a result of anaesthesia.
Premedication
If a patient has been admitted for day surgery, premedication is not normally used. Other patients may receive a light sedative to reduce anxiety, and some are also ‘given an anticholinergic drug, such as hyoscine, to reduce oral and bronchial secretions and vagal overactivity’ (Amos and Waugh 2007) prior to an anaesthetic and to reduce incidence of inhalation when the gag reflex is lost.
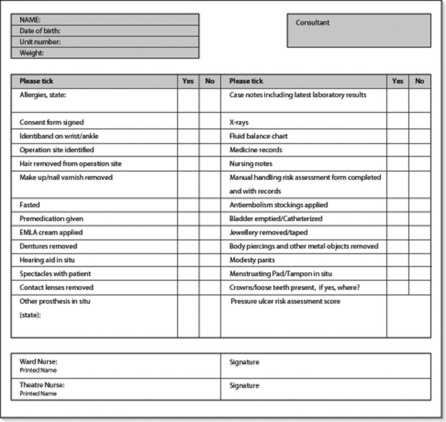
Final preoperative checks
Prior to a patient being transported to the operating theatre, it is important to check again that all necessary activities have been undertaken and a broad checklist is provided in Figure 6.1.
Transfer of the patient from the ward to the operating theatre
Actually leaving the ward area and being transported on a trolley, or sometimes on their own hospital bed, with unfamiliar people can be one of the most frightening and stressful experiences for patients. Oakley and Pudner (2010:47) state that ‘the benefits of reducing anxiety in the surgical patient are not disputed; if a patient is nervous they may experience more pain following surgery, as increased anxiety leads to increased muscle tension, which in turn leads to increased pain as well as to an increase in blood pressure’.
If you are looking after patients who are going to theatre, you may have planned with your mentor to be with a patient during the whole perioperative period. If this is a learning goal, then accompanying the patient from the ward to the operating theatre and anaesthetic room is absolutely essential. It also means that the patient has someone they know with them during this anxious time who will also be with them when they wake up from the anaesthetic.
We have considered the journey of patients who have a planned admission for surgery. We now consider the emergency admission of a patient for surgery.
Discuss with your mentor a plan for total patient care and experiencing the patient pathway throughout the perioperative period. Explain it to the patient and gain their permission to be with them and present during their surgery. If it is major surgery, make sure you eat and drink beforehand, as standing in the operating theatre for a long time on an empty stomach, in a gown, mask and hat, can be extremely uncomfortable and may cause you to faint. If you feel faint (see later chapters), it is important that you leave the operating theatre immediately.
When you arrive at the operating theatre, you will ‘hand over’ the patient to the anaesthetic nurse or operating department assistant. Prior to your visit, it is important that everyone is aware you will be staying to observe the surgery and be with the patient in the postoperative recovery area.
Emergency admission
In many instances, a patient who is considered an emergency admission may be transferred immediately to the operating theatre from the accident and emergency department. The first time you meet them may be during your operating theatre placement or when they return to the ward where you are on a surgical placement.
Some patients, however, may need to be stabilised first and may be admitted to a short-stay emergency care ward or a surgical ward prior to their surgery. For example, an elderly lady who has fallen in the street and fractured her femur may be taken to the orthopaedic ward prior to surgery.
Emergency surgery patients may undergo further tests and be under very close observation and monitoring. If they are conscious, they will be very anxious, and your role in their care involves making sure they are kept informed as appropriate about what is happening to them. Their family/relatives may not be aware of their admission and this may be dealt with by the police or by the senior ward staff.
Information about the general health of emergency surgical patients may be unknown, especially if they are not fully aware of what is happening to them. Tests to see if they are diabetic or not, for example, will be vital.
Some patients carry vital health information with them as well as information about medications such as steroids. They may also carry a donor card.
How critical a patient is will determine when they are taken to the operating theatre.
Summary
This chapter provided a brief overview of the care of the patient who is to undergo surgery. There have been major advances in surgical techniques over the past 20 years, with patients requiring less time in hospital for major surgery. Day surgery is now common and other patients may go home more quickly than an agreed stay in hospital. If your placement is in a surgical unit, you will have an opportunity to engage in one-to-one care of individual patients during their journey. You will also learn about different types of surgery and the various preparations required in order to manage actual and potential postoperative problems likely to be encountered. Chapter 7 explores another stage in the patient journey: the anaesthetic room.
Amos A., Waugh A. Caring for the person having surgery. In: Brooker C., Waugh A. Foundations of nursing practice. Edinburgh: Mosby, 2007. 681–702
Dean A., Fawcett T. Nurses' use of evidence in pre-operative fasting. Nursing Standard Art and Science. 2002;17(12):33–37.
Gilmour D. Perioperative care. Pudner R., ed. Nursing the surgical patient, 3rd ed., Edinburgh: Baillière Tindall, 2010.
Holland K. Evidence-based practice and its implementation in nursing. In: Holland K., Rees C. Nursing: evidence-based practice skills. Oxford: Oxford University Press, 2010. 197–221
Holland K., Jenkins J., Solomon J., Whittam S. Applying the Roper, Logan and Tierney model in practice. Edinburgh: Churchill Livingstone; 2008.
Leinonen T., Leino-Kilpi H. Research in peri-operative nursing care. Journal of Clinical Nursing. 1999;8(2):123–138.
Mitchell M. Anxiety management: a distinct nursing role in day surgery. Ambulatory Surgery. 2000;8(3):119–127.
Murkin C. Pre-operative antiseptic skin preparation. British Journal of Nursing. 2009;18(11):665–669.
Oakley M., Pudner R. Preoperative stress and anxiety in the surgical patient. Pudner R., ed. Nursing the surgical patient, third ed., Edinburgh: Baillière Tindall, 2010. 45–51
Pritchard M.J. Managing anxiety in the elective surgical patient. British Journal of Nursing. 2009;18(7):416–419.
Pudner R. Nursing the surgical patient. Edinburgh: Baillière Tindall; 2010.
Royal College of Nursing. Perioperative fasting in adults and children: an RCN guideline for the multidisciplinary team. In Clinical Practice Guidelines Series. London: RCN; 2005.
Scott C., McArthur-Rouse F.J., McLean J. Pre-operative assessment and preparation. In: McArthur-Rouse F., Prosser S. Assessing and managing the acutely ill adult surgical patient. Oxford: Blackwell, 2007. 3–16
Shebini N., Aggarwal R., Gandhi A. Improved patient awareness of named nursing through audit. Nursing Times. 2008;104(21):30–31.
Simmons M. Preoperative skin preparation. Professional Nurse. 1998;13:447.
Gibson C. The patient facing surgery. In: Alexander M., Fawcett J.N., Runciman P.J. Nursing practice, the hospital and home: the adult. Edinburgh: Churchill Livingstone, 2006. 901–943
Royal College of Nursing. Defending dignity: challenges and opportunities for nursing. Online. Available at www.rcn.org.uk/__data/assets/pdf_file/0011/166655/003257.pdf, 2008. (accessed December 2011)
NHS Choices videos – an excellent site for listening to patient stories of their health experiences, including surgical procedures: http://www.nhs.uk/video/pages/MediaLibrary.aspx (accessed April 2011).
The Royal College of Surgeons website – very informative for patient information pre- and post-surgery for adults and children: http://www.rcseng.ac.uk/patient_information (accessed April 2011).
NHS Scotland Clinical Governance: http://www.clinicalgovernance.scot.nhs.uk/ (accessed December 2011).
An NHS website explaining aspects of clinical governance and patient care, plus a number of excellent links to other resources: http://nhslocal.nhs.uk/our-nhs/hospital-care (accessed April 2011).
Pre- and postoperative care after bowel surgery – a two-part video from a UK hospital in partnership with Coloplast UK for prospective patients to be admitted to hospital. It uses ‘lay’ language that service users can understand without all the technical ‘jargon’: http://www.youtube.com/watch?v=flgO6mUaHbM (accessed December 2011).