12 Case study 2
caring for a patient in a general surgical ward
• To enable you to reflect on prior learning from other chapters
• To explore in more detail through one specific case study the kind of surgical interventions you may come across in caring for patients in a general surgical ward
• To focus on the total care of a patient who may be admitted onto a general surgical ward, from pre-admission to discharge home and care in the community
• To enable you to identify learning opportunities as well as meeting your practice learning outcomes
Introduction
Patients admitted to a general surgical ward have a short-term stay of a few days or a longer stay of a week or more, depending on the type of surgery and whether any perioperative complications occur. In this chapter, we explore the care of a patient who has had a medical diagnosis of cancer of the bowel, identified following the NHS over-60s bowel screening initiative (NHS Bowel Cancer Screening Programme 2009). It is beyond the scope of this book to cover everything with regards to caring for someone after major abdominal surgery. It is advisable, therefore, that you supplement the information in this chapter with that in other chapters plus relevant further reading.
As with the other case studies, it is important to consider them as ‘insights’ into possible learning experiences in practice placements, where you may meet the patient at any stage in that journey. It is important to learn about the whole of a patient's journey and experience in order to be able to help them at the stage at which you meet them.
Introduction to patient and clinical problem
Mrs Nadira Ahmad is a 62-year-old woman who responded to the over-60s bowel screening initiative after seeing an advert for it at her local hospital. A test kit was sent to her and she found this helpful as it meant she could do it in the privacy of her own home, even though she still found it embarrassing. She had been concerned as she had experienced some rectal bleeding and had not told anyone, but she knew from information in her GP centre that ‘something was not right’ – the poster in the hospital had triggered further inquiry when she realised she could do something without alerting too many people, especially her family. She had been experiencing a change in her normal bowel movements and some discomfort on the right side of her abdomen which she had put down to ingesting the wrong kind of food and ‘wind’. She had also been very tired which she had put down to her age.
Two weeks later, Nadira Ahmad receives a letter telling her that she needs to contact the screening service

Access the NHS Cancer Screening site and read the information about the initiative and the process prior to the patient receiving the screening test kit. See the link to the information and the kit instructions. A short animated film can also be found there as well as instructions in different languages:
http://www.cancerscreening.nhs.uk/bowel/ (accessed December 2011).
Information for GPs is also available for this initiative as they are not directly involved in the delivery of the programme:
http://www.cancerscreening.nhs.uk/bowel/ipc-pack.html (accessed December 2011).
to make an appointment to see a specialist nurse. She is informed that her GP has been sent a letter as well explaining why she needs to contact the nurse. If she prefers, she may go to her GP who knows her and her family as well as her health history.
She is now very concerned. She has asked her daughter, who she eventually confided in, to look for any information on the Internet, and a link from the cancer screening programme site led them to video information about the bowel, polyps and possible investigation of colonoscopy for cancer. This is in her own language of Urdu, which helps her: http://www.remedica.com/bowel/default.aspx (accessed December 2011).
In order to help patients such as Nadira Ahmad, you need to understand the physiology of the gastrointestinal tract as well as the nature of polyps and why they can turn cancerous.
If you are in a day surgery unit or an outpatient department where colonoscopies are carried out, you will need to communicate effectively with patients and be mindful of different cultural and religious backgrounds as well as your own communication skills.
View the online explanation for the physician about polyps and colonoscopies on the same site:
http://www.remedica.com/bowel/default.aspx (accessed December 2011).
See Box 12.1 for an explanation of what the NHS screening site states about colonoscopy for service users and the general public.
Box 12.1 What is a colonoscopy?
A colonoscopy is an investigation that involves looking directly at the lining of the large bowel. A thin flexible tube with a tiny camera attached (a colonoscope) is passed into the back passage and guided around the bowel. If polyps are found, most can be removed painlessly using a wire tube passed down the colonoscope tube.
Read the definition in Box 12.1 and compose a more detailed explanation in order to teach another student what happens in a colonoscopy. What would you say differently? For example, would you use the term ‘back passage’ in your explanation or would the word ‘rectum’ be more appropriate?
Do not forget how important words are. In some languages, direct translation is not possible, so other non-verbal explanations or illustrations might be required. Again, this is a skill that is transferrable to other situations.
There are references to physiology textbooks throughout this book and you may have one that you have a personal preference for. To help patients like Nadira Ahmad, it is important that you are fully prepared to answer any questions you feel confident to answer within your sphere of knowledge and responsibility. Being knowledgeable about how the bowel works and what happens in a colonoscopy is essential both pre- and postoperatively should she require major surgery.
Communicating with her in a culturally appropriate way is also very important, as it is with all patients.
Attending for a colonoscopy
After contacting the specialist nurse at the local screening centre, Nadira Ahmad arranges an appointment and her daughter accompanies her. Here is what happens at the clinic.
This is a 45 minute consultation to allow you to discuss with the Specialist Screening Practitioner any concerns you may have about your results. The Nurse will explain about the next investigation which is called colonoscopy.
She will assess your health to see whether you are suitable to have the next investigation. A Health Questionnaire will be completed so it is important to bring information with you about the tablets you take.
The Nurse will also explain about the diet you need to follow three days before colonoscopy and the bowel preparation you need to take 24 hours before your investigation. (From http://www.mccn.nhs.uk/patients/tests/screening/bowel-screening-process.php (accessed December 2011)).
During your clinical placement in either surgical nursing or community nursing, organising an insight day or a 2–3-day spoke placement is very helpful for understanding the patient experience, communication skills and the role of the nurse in this type of new screening service. It is also important for understanding health policy such as that which has influenced the introduction of this screening programme across the UK.
Read the article by Coutts (2010) (see References) for the main report explaining the rationale for the initiation of the bowel screening programme.
In addition there is a report on Ethnicity and Uptake of Bowel Cancer Screening Pilot study (NHS 2003) which will help you consider some of the experiences of Nadira Ahmad. Read also the systematic review of the evidence of the uptake of cancer screening services internationally.
http://www.cancerscreening.nhs.uk/bowel/ethnicity-finalreport.pdf (accessed December 2011).
Nadira Ahmad agrees to attend for a colonoscopy following the meeting with the nurse and her daughter agrees to share this with the rest of the family – her two brothers and their wives. Her husband died 2 years previously at age 68 from lung cancer, so she was very aware of what might happen if she had not responded to her concerns.
An appointment is made for the following week's colonoscopy clinic and instructions given to her regarding bowel preparation and her diet in the week before the investigation.
The colonoscopy
Re-visit the online information on this procedure at http://www.remedica.com/bowel/default.aspx (accessed December 2011).
Colonoscopies are normally carried out in a specialised endoscopy unit. This is somewhere you and your mentor could discuss as a possible insight visit or you may actually have a longer placement in a unit like this. In any case, you will gain excellent learning opportunities in patient care, including sedation and post-procedure care, communication skills and multidisciplinary team working.
Following the procedure, Nadira Ahmad and her daughter are asked to speak to the doctor, which obviously upsets them. He explains that he has found an unusual mass which he has diagnosed as cancer of the bowel. He also explains that early detection of bowel cancer normally results in a 90% chance of it being treated successfully.
He discusses with her the main outcome of this finding – the necessity for surgical intervention – and tells her she will need to come for surgery as soon as possible. The nurse then advises her that she will receive a letter inviting her to come to the pre-assessment clinic in the next few days, when more detailed information can be discussed.
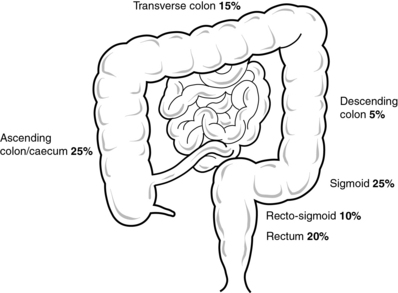
Bowel cancer can be found anywhere in the large bowel (see Fig. 12.1).
Surgery possibilities
Nadira Ahmad's tumour was located in the right ascending colon of the large bowel, and there did not appear to be any lymphatic involvement. She was advised that the surgery would probably be a right hemicolectomy – removing the tumour from the ascending colon, the part of the bowel ending in the caecum. In this procedure, a section of the large intestine is removed, including the normal bowel on either side of the diseased part, and the remainder is attached to the lower end of the small intestine (called an anastomosis), usually with stitches or by stapling them together. There would also be external clips or stitches on the abdominal wound which will need to be removed 7–12 days postoperatively (this will likely take place in the community but it depends on her postoperative recovery). She does not require a permanent colostomy/stoma.
It is possible that Nadira Ahmad will stay in hospital from 7 to 10 days after surgery. She is given information from the hospital about the surgery and postoperative care. She is also advised that as she will have major abdominal surgery, she needs to consider postoperative care once she is discharged home from hospital (see Ch. 10). She is given an urgent appointment to attend the pre-admission assessment clinic at the hospital.
Pre-admission assessment
Nadira Ahmad attends the pre-assessment clinic a week prior to admission for her surgery. The clinic she attends is a nurse-led clinic where the nurses organise a chest X-ray, an electrocardiograph (ECG) and blood tests, as well as taking blood pressure measurements. These were determined to be normal for her age.
Given the nature of the surgery, she is also informed of any special requirements with regards to eating, drinking and eliminating, to prepare herself and her bowel for surgery (such as a special diet in the days before surgery and an enema to ensure the bowel is empty, etc. – see Box 12.2) (Hibberts 2010).
Box 12.2 Specific issues related to preoperative bowel preparation (if required)
 Potential risk of infection if bowel not adequately cleansed.
Potential risk of infection if bowel not adequately cleansed.
Operation cancelled due to inadequate preparation.
Potential loss of fluid and electrolytes due to physical preparation/dehydration from the cleansing solutions.
Potential risk of abdominal pain caused by physical preparation.
Specific objective will be to ensure that the bowel is clean prior to surgery and to minimise the side effects of vomiting and abdominal pain.
Nursing intervention and rationale
Ensure the physical cleansing preparation procedure is correctly carried out and instructions for any laxatives or irrigation are carefully followed and monitored. The result of the preparation should be fully documented, and any difficulty in carrying out the procedure should be reported to the surgeon who is performing the surgery.
All fluid loss associated with diarrhoea and vomiting should be recorded on appropriate documentation, thereby ensuring that fluid and electrolytes can be replaced by intravenous infusion. Antiemetics may be used to relieve excessive nausea and vomiting.
Identify characteristics of the abdominal pain, duration and intensity, and provide appropriate analgesics, ensuring effectiveness is evaluated. Any associated discomfort through diarrhoea is relieved by ensuring the anal area is clean and dry following any bowel action and by providing anaesthetic creams and protective barrier creams.
(From Hibberts 2010:341)
A very important task undertaken by the anaesthetist and her doctor is obtaining informed consent (see Ch. 6). They must ensure that she completely understands the intended surgery and that, if necessary, they are allowed to make other decisions based on what they find during the surgery itself.
Her daughter is also involved at this stage.
Re-read Chapter 5 on pre-admission to hospital and undertake a plan of care for Nadira Ahmad from your experiences and/or using the information in that chapter.
Preoperative care
Nadira Ahmad is admitted to hospital (where you are undertaking a clinical placement) a week later. She has followed the regime set out for her prior to admission and has been admitted the day before her surgery so she can become familiar with the ward and staff and meet one of the hospital interpreters who may be required to help her understand explanations of procedures or aspects of care, if necessary (see Holland & Hogg (2010) for discussion of the interpreter role).
Your mentor is her named nurse and has asked you to become her co-named nurse during the patient's stay in hospital.
If Nadira Ahmad was your patient, agree with your mentor how you can experience all aspects of her care in hospital, and subsequently visit her in the community on her discharge home. You and your mentor would be able to liaise with the community team as she lives close to the hospital.
Work out one SMART (Specific, Measurable, Attainable, Relevant and Timely) goal to meet your learning needs with regards to a patient undergoing major abdominal surgery.
Note: a SMART Goal is one that is: S = Specific (clear and well defined); M = Measurable (can see how much time you are going to take to do it); A = Attainable (Achievable - possible to achieve them in the time set); R = Relevant (need to be relevant to the placement experience and your learning needs) and T = Time-bound (have a deadline by the time you need to complete it).
Theatre and recovery
Nadira Ahmad is escorted to the anaesthetic room by yourself and the operating theatre practitioner who has been sent to bring her to the anaesthetic room.
Re-visit Chapter 7 to see what happens in the anaesthetic room.
You tell Nadira Ahmad that you will stay with her during the whole of the surgery, including the operation and the recovery room time. She is obviously much relieved by this and keeps hold of your hand until the anaesthesia has begun to work and she is wheeled into the operating theatre.
Re-visit theatre practice and the gowning up process. You may get an opportunity to see the surgeon performing the surgery which is an excellent opportunity to link the theory of anatomy and physiology of the bowel. It will also allow you to explain to Nadira Ahmad postoperatively why she may experience symptoms such as pain and why she can't eat immediately afterwards.
Postoperative care
Nadira Ahmad returns to the ward with you accompanying her, following a good recovery in theatre. Back on the ward, she is given postoperative analgesia and an antiemetic. She is commenced on a pain pump. You explain to her, through the interpreter as her daughter has gone home to put her children to bed, how this works and how she can use it.
She is receiving intravenous fluids to replace fluid and electrolytes lost in theatre, and has already had 2 units of blood in the recovery room to replace some blood loss.
You commence observations according to the instructions of the anaesthetist and these are found to be within normal limits for her and for the postoperative period following major surgery. She is recovering well. She is given hourly mouth care as she is not drinking and her mouth, to begin with, is very dry.
Watch the videos identified in previous chapters on all aspects of postoperative care, such as:
http://www.cetl.org.uk/learning/tutorials.html (accessed December 2011).
Another website with additional clinical skills resources and material on observations, injection giving and other skills is:
http://www.oup.com/uk/orc/bin/9780199237838/01student/video/ (accessed December 2011).
Nadira Ahmad has returned from surgery with a catheter in place due to events during the operation and the surgeon has given instructions that it should be removed after 48 hours.
She keeps asking for a drink of water but you explain that, at the moment, she is unable to have this. You make sure her mouth is cared for to stimulate saliva and make her mouth feel refreshed.
Bowel sounds are heard after 48 hours and she passes flatus (wind) which means that she can commence fluids and, once tolerated, she will be started on an appropriate diet postoperatively and according to her cultural needs. Her catheter is removed and although she initially finds it difficult to pass urine, she eventually manages to do so.
She does not experience a paralytic ileus due to the handling of the bowel in surgery (see Hibberts 2010:341), and is making a very good postoperative recovery.
Her wound has a drain which is checked regularly and managed according to the amount of drainage along with observation of the fluid exudate. No infection is noted and the drain is removed after 4 days, when drainage is less that 50 ml per day (Endacott et al 2009: 116–123).
Plan Nadira Ahmad's care after the first 48 hours. Include aspects of sexuality and changing body image, pain management, elimination, managing her diet, postoperatively following major abdominal surgery. In addition wound management and principles of wound care (see Endacott et al 2009: 114–123).
Key aspects can be found in Sections 1 and 2 but you may need to read further about the specific care of a patient who has had a hemicolectomy for bowel cancer. It is also important to consider all her care in relation to her cultural needs (see Holland et al 2008).
Discharge home from hospital
Because of Nadira Ahmad's good postoperative recovery and having someone to help her at home, she is discharged home 7 days after surgery.
She is tolerating a light diet, passing water and has had two bowel movements resulting in soft stools after beginning to eat and commencing free fluids.
Some of her sutures (interrupted) are removed before she is discharged home, but your mentor has decided that at least three of them need to remain for at least another 2 days. They will require removal after her discharge home by the district/community nurse.
Instructions about her postoperative recovery and follow-up nursing treatments are given to Nadira Ahmad and also sent to her GP and the district nurse.
Undertake a plan of discharge from hospital for Nadira Ahmad and then one for a patient of your choice following major surgery as part of your assessment of competency in nursing practice and decision making (Nursing and Midwifery Council 2010).
Recovery from surgery at home
Once home, Nadira Ahmad is apprehensive about her wound and diet, and wants to know whether her cancer has gone. She has an appointment in the outpatient clinic in 6 weeks' time but tries to allay some of her concerns by asking her daughter to phone the health centre and make an appointment to see her GP. The district nurse has already visited, and as Nadira Ahmad is visiting her GP in 2 days time, she organises to take her sutures out in the health centre at the same time. She also organises for her to see the specialist nurse who she saw at the beginning of her surgical journey in order to answer more specific questions related to her bowel cancer and future monitoring of her susceptibility to the disease.
Summary
This case history is a brief introduction to the care of a patient who has undergone major surgery. By following a patient's journey in this way, you can maximise your learning by thinking of this as a placement learning pathway. You might discuss with your mentor the possibility of doing the same with a patient you are caring for in your surgical placement.
Coutts A. The bowel cancer screening programme: Understanding the rationale. Gastrointestinal Nursing. 2010;8(3):38–41.
Endacott R., Jevon P., Cooper S. Clinical nursing skills: core and advanced. Oxford: Oxford University Press; 2009.
Hibberts F. Patients requiring colorectal and anal surgery. In: Pudner R., ed. Nursing the surgical patient. Edinburgh: Baillière Tindall; 2010:325–348.
Holland K., Hogg C. Cultural awareness in nursing and healthcare, 2nd ed. London: Arnold; 2010.
Holland K., Jenkins J., Solomon J., Whittam S. Applying the Roper, Logan and Tierney model in practice. Edinburgh: Churchill Livingstone; 2008.
NHS Bowel Cancer Screening Programme. Online. Available at: http://www.cancerscreening.nhs.uk/bowel/, 2009. (accessed December 2011)
Nursing and Midwifery Council. Standards for pre-registration nursing education. [Online. Available at:]. NMC: London, 2010. http://standards.nmc-uk.org/PreRegNursing/statutory/background/Pages/introduction.aspx, (accessed September 2011)
Black P. Cultural and religious beliefs in stoma care nursing. British Journal of Nursing. 2009;18(13):790–793.
Narayanasamy A. Transcultural nursing: how do nurses respond to cultural needs? British Journal of Nursing. 2003;12(3):185–194.
NHS Choices website. Stories of life experiences of having been diagnosed or treated with bowel cancer: http://www.nhs.uk/Conditions/Cancer-of-the-colon-rectum-or-bowel/Pages/Lindas-story.aspx (accessed December 2011).
Merseyside and Cheshire NHS Cancer Network. Nurse led screening service: http://www.mccn.nhs.uk/patients/tests/screening/bowel-screening-process.php (accessed August 2011).