14 What have I learnt in a surgical nursing placement?
• To reflect on learning experience in a surgical nursing placement
• To establish what knowledge and skills you have gained during the placement
• To consider how what you have learnt in your surgical nursing placement can be utilised in a range of other placements and in various fields of practice
• To identify the experiences your mentor will use to establish whether you have met your learning goals and/or competences for the placement
Introduction
Reflecting on your learning is an essential skill to establish early on in your programme of study, to discus with your personal tutor at university and with your mentor in practice. During your time on placement, you will be assessed in accordance with your programme requirements and, most importantly, the Nursing and Midwifery Council (NMC) standards in the four domains and their generic and field-specific competencies.
This chapter explores the above aims through a range of exercises, references to other chapters and new learning experiences. To begin with, we can re-visit what reflection means and how you do this, in particular reflection on being a student nurse, reflection in the practice of actually ‘doing’ nursing and what goals you now need to set for the future.
Reflection
Most of you will have come across the term ‘reflection’ in your programme of study, but what does it mean in the context of learning in clinical practice? How important is it to your learning to become a nurse? We consider these two questions in the context of undertaking any placement experience and also a surgical one.
At the beginning of your programme of study, you will have been given a practical assessment document to be used by yourself, your mentor and personal tutor to assess, record and discuss your learning in practice to meet the requirements of your course and, most importantly, to meet the requirements of the NMC. Along with this document will be some kind of personal portfolio and personal and professional development documentation in which to document your learning experiences throughout your journey to becoming a qualified nurse. You will be expected to continue this practice following successful registration as a qualified nurse, as maintaining your professional development is an NMC requirement to remain a registered nurse, as well as being part of your annual appraisal requirement by your employer if you work in the NHS.
Timmins (2008:1) offers the following definition of what a portfolio is:
A portfolio is a collection and cohesive account of work-based learning that contains relevant evidence from practice and critical reflection on this evidence. Its primary purpose is to display achievement of your learning and knowledge development. Most commonly the portfolio is a hand-held document, such as a ring binder, that you, as a student, carry with you to prepare and complete while you are actually gaining your practical clinical experience within the clinical practice environment; it can also be in electronic format.
The key words, highlighted in bold, link to the idea of learning from your experiences in clinical placement (workplace learning), evidencing this in some way as written work but, most importantly, reflecting on what you have written about your learning through analysing the experience rather than just describing it. Describing your experiences and what you have learnt from them are both important, but considering them in relation to previous experiences and/or theoretical knowledge can help you to understand what took place or what you felt during the experiences.
It is beyond the scope of this book to discuss reflection and reflective practice in full, but you will find specific texts and articles, such as Timmins (2008) and Hart (2010), to help you at the end of the chapter.
Your portfolio will contain a range of important documents that you are required to have in order to become a nurse registered with the NMC as well as evidence of your personal and professional growth over the course of your programme of study.
What then is reflection? Schon (1983) wrote that there are two types of reflection in relation to clinical practice learning: reflection-in-action and reflection-on-action. The latter is the one we focus on in this chapter but it is also important to consider reflection-in-action as well. Consider the definition of reflection offered by Price and Harrington (2010:25):
… a process whereby experience is examined in ways that give meaning to interaction. We might examine the experience in real time or in retrospect. Because experience engages the emotions as well as reasoning, reflection needs to take account of the feelings engendered within an interaction and to allow that perceptions (how we interpret matters) may sometimes prove erroneous. While reflection is most closely associated with human interactions and especially clinical events, it is not limited to these. We may, for instance, reflect upon the written accounts of experiences, such as those shared by dying patients. Reflection may be used in the service of different nursing goals – those that are designed to tell us something about how we think, what we value and with regard to ways in which practice could be improved.
Reflection, then, involves thinking about what you have done, taking the activity ‘out of the box’ and looking at it both in terms of how you felt about it when looking at it and actually experiencing or doing it. This is reflection-on-action, the one which you will be asked to write about if doing this for an assignment, to critically review it in terms of evidence, i.e. supporting the rationale for why you did what you did through theoretical concepts or supporting research.
For example, imagine you wrote the following as part of your reflection on an experience with a patient who was going to theatre: ‘I asked the patient whether she had any concerns about going to the operating theatre. She wanted to know what would happen in the theatre and so I explained to her the procedure that would be carried out. She seemed relieved to know that it was perfectly normal to feel afraid that she wouldn't wake up’. We know from previous Chapters the importance of talking to patients and reassuring them before surgery, and the importance of explaining what will happen, for example we would add to the above reflection in the following way to demonstrate critical reflection or reflection based on evidence.
Critical reflection: evidence based
‘… She wanted to know what would happen in the theatre and so I explained to her the procedure that would be carried out.’
Miller and Webb (2010:59) refer to this as ‘attending’ to the patient, whereby ‘active listening and attending rely on being able to communicate to the other person that we are listening, understanding, remembering, and even interested in what they are communicating.’
Examining the reflection in ‘real time’ is actually harder to contemplate, as it is reflection-in-action, not actually visible to others nor easily expressed, and refers to looking at what you are doing as it actually happens. What you might be reflecting -in-action on may well involve personal feelings of your own or something related specifically to the patient or the situation you have not dealt with before. Imagine a scenario where someone on your ward is having a cardiac arrest. You have never seen one before and only know the key steps to take when it happens, such as calling for help, phoning the right number for the cardiac arrest team and helping the team as required. You watch all the nurses and doctors immediately taking action to save the person's life and it seems as if they know exactly what to do. Nobody is talking out loud; they are all just ‘doing’ things. You wonder how they can do this and how they know what the right thing to do is. What you can't see is the nurses or doctors ‘reflecting-in-action’. They may be:
• drawing on a number of similar previous experiences
• examining which one is most similar to the one they are now managing
• possibly considering evidence on new medication
• deciding how to manage the environment they are in
• remembering how they felt the last time they had to undertake a similar situation and telling themselves ‘this time I am going to manage this well … now what do I need … I need to keep talking to him as well, even though he is probably not really hearing me … hang on, I think I can feel a pulse … must mean his heart is now working … best tell Dr Bloggs that it is thready and fast though, and I think missing beats as well … best get the monitor attached … now he is coming round … in order to see what his heart trace is doing …’.
In other words, they are using previous knowledge and experiences to influence their actions in the present situation. All of this probably takes place in a very short space of time – but you can see how much reflection-in-action is taking place. Speaking your thoughts out loud is not appropriate in a cardiac arrest situation or in other situations such as breaking bad news. Reflecting-in-action involves private and personal thoughts and feelings.
Banning (2008) suggests that a ‘think out loud’ approach may be an excellent way to get student nurses to learn as they problem-solve a case study, just as they would in real life practice.
However, reflection-on-action requires a set of skills that can be learned, such as self-awareness which is fundamental to learning from experiences in practice, as is being able to recognise what you did well or need to work on should you experience a similar situation in the future. Using a framwork to guide you in writing your reflection of an event or an observation is helpful.
Models/frameworks to help you reflect on practice learning
There are a number of models that can be used based on theories of reflection. We can consider two here that may be useful to you or that your University asks you to use to reflect on your learning.

Look at your programme handbook, your personal and professional development document or information in the virtual learning environment at your university. Identify which model or framework is being advocated at the stage of learning you are at. There may also be helpful sheets that you can print out on which to document your reflections of situations or events.
Situations that have a significant impact on your experience and learning are often known as ‘critical incidents’ – which can be so-called positive or negative situations – hence the word ‘critical’, in the sense of being important. This is not to be confused with ‘critical incident recording’ in the clinical area whereby an incident is critical in the sense of being important which has also triggered a serious situation requiring investigation. For example, say a patient had been left on their own in the bathroom when the nurse went to get something. The nurse didn't make sure there was someone to stay with the patient and they later became dizzy, collapsed and broke their leg. This led to them having to go back to the operating theatre, move to an orthopaedic ward and stay in hospital for a further 2 weeks. Such an incident would have to be reported, written down in a factual way and then signed by the nurse, and subsequently investigated by a senior member of staff.
Consider this example of a critical incident and reflect on what happened. What can you infer from the ‘second hand’ description above, and what do you think would have been the description of the event by the actual nurse in question?
A helpful model for reflecting on practice learning (upon which many others are based) is Gibb's (1988) ‘reflective cycle’ (see Fig. 14.1).
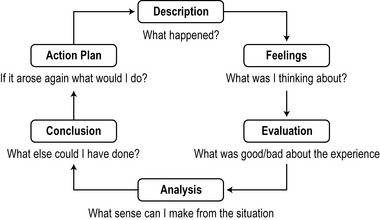
A simpler version of this model for reflection is that by John Driscoll (1994). His framework is based on three stages: What? So what? And now what?
(See http://www.supervisionandcoaching.com/pdf/reflectivelearning.pdf.)
In brief, you have an experience in practice and then ask yourself the three questions relating to this experience:
1. What? This is your account or description of the experience or event that took place, making considered judgements on what you think happened and why it happened (description).
2. So what? This is when you consider how you felt and decide if it was a good experience or a bad experience and why. You decide what you think you learnt from the experience or the event (feelings, evaluation and analysis).
3. Now what? This is where you decide what you are going to do in relation to learning from this experience or event. You decide what actions may be necessary, such as: discussing it with someone else; reporting aspects of the experience officially to another person; or developing your knowledge and skills to manage the situation better or differently next time something similar happens (conclusion and action plan).
Consider an experience in your surgical placement and use Gibb's and Driscoll's models of reflection. Write the reflective cycle experiences in your reflective diary, which will either be part of your portfolio or part of your personal and professional development document. Discuss this with your mentor and personal tutor (normally a requirement of your programme). If you have to write a critical reflection essay or similar, you may want to read Chapter 4 in Gimenez (2011) (see References).
Establishing knowledge and skills gained in practice
You now have a framework for reflection on practice learning in your surgical placement. From a clinical perspective, it is also important to consider what you have learnt from this book (or individual chapters) and actually caring for patients undergoing surgical interventions.
You may have agreed a learning plan with your personal tutor prior to the placement and discussed it with your mentor, who would then facilitate achievement of the learning plan as far as possible. At the end of your placement, you may have to provide evidence for achieving this or your mentor may have to do so, or both, identifying areas for further development in general and on future clinical placements. An example can be seen in Box 14.1.
Box 14.1 Example of a learning agreement for a surgical placement experience
Learning outcome
To assess, plan and contribute to implementing and evaluating the care of a patient undergoing surgery.
Experiences to be gained
1. Exposure to new situations which involve preparation of patients undergoing surgery.
2. Discuss with mentor pre- and postoperative care protocols in place.
3. Assess the needs of a patient who is admitted for surgery.
4. Plan the care and record in the patient care plan under supervision.
5. Obtain and read current research findings on wound care specific to different patient groups.
Criteria for success
1. Should be able to assess the needs and plan the care for a patient undergoing surgery.
2. By demonstrating, under supervision, the total preparation of one patient undergoing surgery.
3. Can give a rationale for three nursing interventions which are linked to current research findings.
All of the above would be agreed with your personal tutor prior to commencing your placement experience and discussed and agreed with your mentor when you meet to discuss your learning needs and goals and how they can support you in achieving them.
Evidence of achievement
1. (Name: e.g. Jane) has assessed and planned the care of four patients during this placement and has ‘followed through’ two of these from preoperative preparation to the patient being discharged home from hospital. This included a visit to the operating theatre and a day with the stoma nurse.
2. The diary summary for this placement indicates that (e.g. Jane) was distressed by one incident which she also highlighted as a critical incident record (discussed with her).
3. She accepts support and constructive criticism in care planning, then acts upon it in a positive way.
4. She has been able to identify the evidence-base research for three interventions as agreed plus many others (handwashing, preoperative fasting and assessment of pain).
Areas for further development
1. Needs to discuss with her personal tutor the issues raised within this experience, especially those in the reflective diary records.
2. Her aseptic technique skills need to be extended/applied to many new areas of practice.
3. Very positive attitude to learning and achieving her goals. Main area to develop is writing her reflections on events that can lead to consideration of the role of others in patient care.
Transferrable practice and knowledge
Throughout this book, there are many activities to test your knowledge as you progress through the patient journey in the perioperative period. The intention of this chapter is to use reflection to help you consider what you have learnt and to offer additional learning exercises to test your knowledge, together with some case scenarios that you can use to develop your notes on all aspects of perioperative care. Some of these may be potential examination questions which can be used for revision purposes.
Self assessment questions: perioperative care
14.1. List 10 possible preoperative care procedures that are necessary to ensure the safe environment of the patient is maintained prior to surgery.
14.2. In the transfer of patients to theatre, what can the nurse do to maintain the safety of the patient?
14.3. Immediately postoperatively, what is the nurse's role in maintaining the safety of the patient?
14.4. List 10 actual or potential problems than could occur postoperatively after major surgery.
The acutely ill adult: planning care following surgery
Case history
Mr William Smith, age 58, was taken to the operating theatre for removal of a large malignant tumour from his large colon. The possibility of a permanent colostomy had been discussed with him and his wife. During the operation, Mr Smith experienced a cardiac arrest which the anaesthetist believed was due to a myocardial infarction (evidence seen on the cardiac monitor). He was successfully resuscitated and the surgeon completed the planned surgery which took longer than planned. He was taken to the recovery room for close observation until the anaesthetist decided when it was safe to transfer him to the ward or, preferably, given the cardiac arrest, a high dependency unit (HDU). Unfortunately, no HDU bed was available at the time so, with reassurance from the ward that they could maintain close 24-hour observation on his progress, the anaesthetist agreed that he could be returned to the ward once his observations were stable and he was awake and responsive.
On his return to the ward, you and your mentor, a staff nurse with intensive care unit experience, were assigned by the team leader to look after him. You had already prepared the bed area for his return and it had been possible to re-allocate him to a small single-bedded room near the nurse's station. His wife and daughter were already waiting for his return and had been informed by the surgical registrar, who had assisted during the surgery, about his cardiac arrest and the need for close monitoring. Despite being distressed by this news, they remained positive about the care he would receive on his return and were pleased that he was coming back to be cared for by staff who knew him.
Specific information you need for the following activity related to the case history
The postoperative plan from theatre for Mr Smith includes the following information (in brief):
• Removal of tumour (malignant as per preoperative investigations); end-to-end anastomosis of large intestine–sigmoid colon (no colostomy formed).
• Cardiac arrest due to myocardial infarction – effects enhanced by the surgical intervention. Successfully resuscitated (2 minutes) and vital signs stabilised. Two-hour period in recovery room.
Instructions for nursing staff regarding observations are as follows:
• Cardiac monitoring to continue, as well as all other observations.
• Pulse and blood pressure: quarter-hourly for 2 hours then reassess; if stable for that 2 hours, nursing staff to determine observations either half-hourly or hourly as other physiological status requires. Continuous re-evaluation as necessary and surgical registrar to be contacted if any changes in cardiac monitoring and function. Cardiac medical team will be attending the patient to assess myocardial infarction status and long-term rehabilitation needs.
• Patient was slightly hypothermic postoperatively at a temperature of 35.6°C; to restabilise slowly until his ‘normal’ body temperature is re-established.
• Counteract fluid loss during surgery: he is to have an IV infusion of dextrose/saline and normal saline to alternate every 4–6 hours as blood pressure and fluid output determine.
• For the first 6 hours postoperatively, he requires central venous pressure measurements taken and he will then be reviewed by the anaesthetist who wishes to be kept informed of his general ongoing postoperatively status.
• He has a nasogastric tube in situ and aspirations initially are hourly.
• Due to the complications in the operating theatre, he has a catheter in situ as well for 24 hours, until his cardiac problems have been stabilised. Hourly measurements to be taken and recorded.
• He has a patient-controlled analgesia (PCA) machine which he had explained to him preoperatively and the nurses are to monitor his use of it given that he has had the myocardial infarction.
• He has a wound drain in situ and his wound has been closed with clips.
He has been fully conscious on his return to the ward and has been made comfortable, although he is aware that there is a lot of equipment around his bed and he is reluctant to move. He is aware of his condition and his wife and daughter are with him.
Based on this very brief insight into Mr Smith's physiological status and postoperative situation, consider the following questions and exercises. Use other chapters and resources identified in this book to help you consider all of the issues raised in this scenario and information offered.
• Plan his care in order of priority and use an appropriate nursing model as a framework for his care. Do this for the first 12 hours postoperatively, then 48 hours, then 7 days.
• Determine what equipment you will need in order to ensure his internal and external safe environment.
• Explain the effects of hypovolaemia on the body and how it determines the importance of nursing observations, including how the signs of hypovolaemia would be noted.
• Explain the effects that a myocardial infarction has on the muscle and blood supply of the heart.
• Determine what needs Mr Smith will have problems in meeting during the first 24 hours, 36 hours and 7 days postoperatively.
• How would you and your mentor organise the care of Mr Smith in order to allow:
Discuss this with your mentor as a hypothetical patient situation, but one where you can identify some specific learning needs and goals to achieve in order to establish prior knowledge and skills should a situation like this arise either in your current or future placements.
Transferring knowledge and skills
Whether this is your first placement or your final one, you will be able to use what you have learnt in this surgical placement to help you in either your next placement or in your role as a qualified nurse.
Make a list of all you have learnt in this surgical placement, and record it as part of your practice achievements in your practice assessment document. Discuss with your mentor how this can contribute to your ongoing record of achievement (NMC 2010). If it is your final placement, you will be assessed by your nominated sign off mentor.
If you are pursuing a programme leading to registration as a nurse in any of the four fields of practice, please refer to the generic NMC domains and competences for identifying how undertaking a surgical placement can be of value in relation to your own specific field of practice and the patients/clients/children/young people/adults that you meet and care for.
Summary
Wherever you are in your stage of learning, it is important to recognise the interdependence of knowledge and skills gained in other placements, the knowledge and skills you learn in the university setting and their application in the reality of clinical practice. This book can help you only as a guide to the possibilities of caring for different patients and in very different surgical placement contexts. Remember, every placement is very different, every day is very different, every patient is very different and every event is very different. You can, however, develop knowledge and skills to enable you to adapt to this uncertain environment and become a competent decision maker and problem solver as well as a caring, knowledgeable student nurse ready to take on the responsibilities of becoming and being a registered nurse.
Banning M. The think aloud approach as an educational tool to develop and assess clinical reasoning in undergraduate students. Nurse Educ. Today. 2008;28(1):8–14.
Driscoll J. Reflective practice for practise – a framework of structured reflection for clinical areas. Senior Nurse. 1994;14(1):47–50.
Gibbs G. Learning by doing: a guide to teaching and learning methods. Oxford Polytechnic, Oxford: Further Education Unit; 1988.
Gimenez J. Writing for nursing and midwifery students, 2nd ed. Basingstoke: Palgrave Macmillan; 2011.
Hart S. Nursing: study and placement learning skills. Oxford: Oxford University Press; 2010.
Miller E., Webb L. Active listening and attending: communication skills and the healthcare environment. In: Webb L., ed. Nursing: communication skills in practice. Oxford: Oxford University Press, 2010.
Nursing and Midwifery Council. Standards for pre-registration nursing education. London: NMC; 2010. Online. Available at: http://standards.nmc-uk.org/PreRegNursing/statutory/background/Pages/introduction.aspx (accessed September 2011)
Price B., Harrington A. Critical thinking and writing for nursing students. Exeter: Learning Matters; 2010.
Schon D.A. The reflective practitioner. New York: Basic Books; 1983.
Timmins F. Making sense of portfolios – a guide for student nurses. Maidenhead: Open University Press; 2008.
Webb L. Nursing: communication skills in practice. Oxford: Oxford University Press; 2010.
Aston L., Wakefield J., McGowan R. The student nurse guide to decision making in practice. Maidenhead: Open University Press; 2010.
Wilding M. Reflective practice: a learning tool for student nurses. British Journal of Nursing. 2008;17(11):720–724.
See John Driscoll's Website for resources, including a presentation on reflection to students at the University of Salford and a range of articles: http://www.supervisionandcoaching.com/ (accessed September 2011)
Reflection on Practice: an excellent resource as part of the Making Practice Based-Learning Work project led by the University of Ulster: http://www.science.ulster.ac.uk/nursing/mentorship/docs/learning/reflectiononpractice.pdf (accessed December 2011)
Learning and Assessing through Reflection – as above: http://www.science.ulster.ac.uk/nursing/mentorship/docs/learning/RoyalBromptonV3.pdf (accessed December 2011)
Online resources from Webb (2010). This is one of a series of books which can help with specific aspects of learning as a student nurse. Most of these have online resources which can be accessed independently but may require some linking to key information in the text itself: http://www.oup.com/uk/orc/bin/9780199582723/01student/practice/ (accessed December 2011)
NMC advice on use of social networking sites: http://www.nmc-uk.org/Nurses-and-midwives/Advice-by-topic/A/Advice/Social-networking-sites/ (accessed December 2011)
Answers to self-assessment questions
(Note: these are not definitive answers. Please read the relevant chapters for full details.)
14.1
1. Assessment and recording on admission of blood pressure, pulse, respiration and temperature (and note these baseline observations).
2. Urine analysis is undertaken and weight is measured and recorded.
3. Check that the informed consent form has been signed by the patient and is in the patient notes.
5. Check if the patient has been given information and time to ask questions regarding the impending surgery.
6. Check preoperative instructions from the surgeon and all premedication and postoperative medication written.
7. Immediately prior to taking the patient to theatre, check the name band, and that the name and date of birth of the patient in the notes matches the name band and patient response.
8. Any X-rays are with the patient notes.
9. When the patient last ate or drank.
10. Check that any drug or other allergies have been noted either at the pre-admission clinic or on admission to the ward. Allergies recorded in the theatre ‘checklist’ including latex allergy or specific drugs/antibiotics. Any false teeth removed and any loose teeth recorded, jewellery removed or secured (e.g. wedding ring) so as not to interfere with surgery or to adhere to religious customs, ensure any prostheses are removed and any nursing and medical records are up to date and complete to go with the patient to theatre. (See Chapter 6 for more details.)
14.2
1. Talk to the patient and reassure.
2. If on a theatre trolley, ensure the patient is unable to roll off the trolley (ensure any trolley side arms are secure to prevent this); if on their own bed, ensure the same thing; ensure arms and/or legs are not hanging over the sides where they may be damaged.
3. Check for any signs of obvious physical distress especially if the patient is sedated or has known cardiac or respiratory problems.
4. On arrival in the anaesthetic room, ensure that the verbal handover includes all information and that you stay with the patient if that would allay further anxiety.
5. All nursing and medical notes and X-rays handed over and checked.
14.3
1. Maintain a safe internal environment:
14.4
(Note: this is in brief and not in any specific order)
• Shock due to pain (neurogenic) or haemorrhage/fluid loss (hypovolaemic) or heart problems (cardiogenic).
• Inadequate breathing and potential hypoxia.
• Dehydration or fluid overload.
• Impaired nutritional status/malnutrition.
The following books/chapters can be used to check all of these and find out the actions to either prevent or manage these postoperatively. Make notes against each one for your placement file/notebook. This is not a definitive list and needs to be considered against individual patients and the type of surgery they experience. There will be many actual and potential problems related to specific types of surgery discussed in this book.
Amos A, Waugh A (2007) Caring for the person having surgery. In: Brooker C, Waugh A Foundations of nursing practice. Mosby, Edinburgh
Pudner R (2010) Nursing the surgical patient Baillière Tindall, Edinburgh
Wicker P, O'Neill J (2010) Caring for the perioperative patient, 2nd edn. Wiley-Blackwell, Oxford