Chapter 5 Reflective Practice
doing, being and becoming a reflective practitioner
Overview
Reflection and reflective practice are terms that we all hear in our daily practice; we could assume that we all consider that they mean the same thing to all – this may not be the case. This chapter returns to the basics regarding reflection and reflective practice, its historical development and its importance and relevance to professional practice today are explored. The concept of doing reflection, being reflective and becoming a reflective practitioner are integrated throughout the chapter. The terms will be defined and the key theorists discussed. The significance of reflection to individual and importantly, teams of practitioners will be highlighted as a method for bringing about change in service delivery. Types of reflection, models and methods to facilitate reflection are explored. Throughout the chapter ‘promoting reflection’ activities are introduced; these can be done individually or with peers and offer strategies for enhancing doing reflection. The chapter concludes with highlighting signs and outcomes of reflection practice.
Introduction
I am delighted that this chapter is near the start of this text: why you ask? The answer is that often reflection is seen as only a retrospective activity (something to do after the event) but that is only part of the story. Reflection is much more than just looking back; that is to say having reflected on an experience or an event what does it mean for you now: in what ways will your thinking or behaviours be different? Reflection importantly, is about shaping your future thinking and actions.
By being near the beginning of this text it sets in place the notion that reflection is something that can be used prior to events as well as post experiences. So as you read, whether you are a reader of books from beginning to end, or a dipper into selected chapters – reflection should be part of the process so that you can make meaning of the chapter material in relation to your knowledge and experiences. As you read consider: What does this mean for me? Could this be useful to my practice now or in the future? What could I bring into my practice or my team’s practice now?
We are all familiar with the concept of the reflective practitioner; the reflection process is something built throughout your professional career. Therefore, it is good to establish this habit early on whether you are a student, a novice therapist or an expert practitioner. Throughout this chapter there are Promoting Reflection exercises for you to work on individually or with others. By completing these you will be developing or enhancing your reflective abilities. By the end of this chapter you will be able to:
This chapter will consider the theoretical basis of reflection and why it is important to individual occupational therapists and teams. The chapter will present various models to facilitate reflection and discuss activities for ‘doing’ reflecting in and on practice to assist the development of becoming and being a reflective practitioner. Try the exercise in Box 5.1 below.
Box 5.1
Before we begin I would like you to think back on some personal experience from the past 3 months. Take a few minutes to remember it, what happened, who was involved, when and where did it take place, why? Now take some time to recall what you felt and thought about that at the time: concentrate on the thoughts and the feelings.
To assist you to become a reflective practitioner two therapists will be presented throughout the chapter at different stages in their career: David and Caroline.
David is 25. He is 6 months from qualifying from his pre-registration Masters in Occupational Therapy. David worked previously as a residential care worker with teenagers and he has a degree in Sociology. He is currently finishing his research thesis and he has one more placement to complete to qualification. David is single.
Michelle is an expert practitioner having worked for 15 years with children. She is recognized by the profession as a specialist in autism. She has worked in Australia and the USA. She has decided that she would like to take her professional development further and is considering returning to education. She is 36 years old, married with two boys aged 7 and 10 years old.
So why is reflection important?
Reflection is an essential component for the competent and capable therapist practising in the 21st century. Developing reflective practitioners is now a requirement for pre-registration health programmes in the UK (Quality Assurance Agency for Higher Education 2001). Furthermore the Health Professions Council (HPC) (2004) incorporates reflection into the Standards of Proficiency for Occupational Therapists specifically Section 2.2 states that the registrant must ‘be able to audit, reflect on and review practice’ (p. 5); furthermore, this is expanded in section 2c2 to ‘understand the value of reflection on clinical practice and the need to record the outcome of such reflection’ (p. 13). Reflective practice is identified as a key component of work-based learning to maintain a registrant’s continuing professional development as part of their lifelong learning (HPC 2006). Practitioners are expected to self-reflect critically on personal performance and adopt a reflexive approach to problem solving. Reflecting on performance and acting on reflection is a professional imperative. Eraut (1994) highlights that the failure not to engage in regular reflection is professionally irresponsible.
Today, it is important that professionals are not only competent to practise but also that they are educated for capability (Fraser and Greenhaugh 2001). By that, I mean that given ever-changing practice contexts; against a backdrop of health and social care systems and processes that are constantly scrutinised for cost effectiveness: practitioners have to think and operate at the higher cognitive level, that is they have to engage in self-evaluation and critical analysis of self. Practitioners require to compare their practice against their own experience and knowledge of theory in their specialist area; thus reflection is about the process of therapy not just about evaluating an intervention with a client (Kuit et al 2001). Reflection is a bridge to linking the theory–practice gap; reflection on your own practice is an essential skill for lifelong learning.
Developing the capability and capacity to adapt to meet changing needs is key to educating practitioners, therefore most professional educational programmes incorporate the factors Cowan (2006) identifies below as essential for developing capability into their curricula. Curricula will include opportunities for learners to:
Through engagement in such activities throughout their pre-registration education both in university and also importantly, in practice settings, entry-level practitioners are enabled to begin their professional careers more ready to negotiate the reality of the practice world.
Individual reflection on ‘doing’ practice
Whilst the factors above are embedded in pre-registration education, at an individual level therapists, whether novices or experts, still require to develop their critical thinking abilities through purposefully engaging in thinking about why and what it is they do in practice? What were they trying to achieve? How well it was done? And how can their practice be different or improved in the future? Critical thinking is achieved through active learning methods including the development of reflective processes; it is through reflection we integrate our thoughts and actions. The reflective process involves us in thinking about and critically analysing our actions with the goal of improving our professional performance and therefore our practice. Engaging in reflective practice requires individuals to assume the stance of observer of their own practice. This allows them to be able to identify the assumptions and feelings underlying their practice, to speculate about how these assumptions and feelings affect practice and how these can be modified for future practice (Osterman 1990). Practitioners are the experts in what they learned from their varied professional experiences; whether these are through practice, reading, course attendance or research. Being reflective involves you as an active participant not a passive recipient (Kinsella 2000).
Multiple voices reflecting on ‘doing’ practice
The reflective process is often regarded as an individual activity; for example we often hear of being a reflective practitioner, but rarely about a reflective team. However, there are compelling reasons for reflection to be done in collaboration with others: it is through working together as a team, or as a community of practitioners, that we can work to transform practice (Freire 1972). As all our continued professional development occurs in cultural, social and political contexts, the health and social care teams in which occupational therapists work are rich grounds for learning. Teams can share and discuss practice, to make change to improve services for clients through collective reflection and subsequent collaborative action. Through working with others we are open to the possibility of change: our ways of understanding can be explored, challenged and alternatives created. Winpenny et al (2006) offer an illuminating account of group reflection. Through sharing our practice stories with others we become participants in our joint practice: gaining additional perspectives of a situation or an event and discovering new meanings or insights. This is necessary, if we only reflect individually we run the risk of navel gazing. Bolton (2001) stresses this ‘reflective practice work can … become politically, socially as well as psychologically useful, rather than a mere quietest navel-gazing exercise’ (p. 3). Boud (2006) too, highlights that there is a need for new methods of reflection that move the focus from the individual learner in the workplace to systems that support team and organisational reflection and action in the workplace: namely, productive reflection. Productive reflection should lead to action with and for others for the advantage of all involved including the service users, the organisation and wider society (Cressey and Boud 2006).
In summary, active reflection can enable individual practitioners and teams to monitor, evaluate and adapt their performance: as a result their professional practice can be enhanced and the quality of service delivery to clients improved.
What is reflection?
Reflection is one of those words that is often used indiscriminately and that has many different meanings according to the user’s perspective. In a recent exercise, practitioners were asked for their personal definitions of reflection: a sample is included below (see Box 5.2).
Box 5.2 Therapists’ definitions of reflection
The practitioners above identified key aspects of reflection: reviewing their performance, examining it in detail, relating to their past knowledge and experiences and future actions. Their definitions concentrate on retrospective reflection or ‘reflection on action’. Similarly, when students completed this exercise the majority of their views of reflection were also retrospective (see Box 5.3).
Box 5.3 Students’ definitions of reflection
Reflection is important to look back…what have you done right and what treatment you could improve in the future
Reflection enables the person to return to the experience and analyse those experiences both good and bad.
To look back on your treatment and change it to adapt to different individuals – if it worked.
Defining reflection
For clarity, it is useful to go back to dictionary definitions. Kirkpatrick (1988) defines ‘Reflect’ as ‘…to give an image of as in a mirror’ (p. 1087). The idea of holding a mirror up to gain a picture of practice is useful but limited as it only focuses on a specific frame in time. ‘Reflect’ is also defined as ‘to consider meditatively’ (p.1087), this develops the process from looking at – to thinking about in a more in-depth and in an intentional manner. Kirkpatrick (1988) goes on to describe ‘Reflection’ as ‘…the action of the mind by which it’s conscious of its own operations’ (p. 1087). Here an individual is actively thinking about or examining their thinking: this process is meta-cognition (Eraut 1994).
In relation to learning from experience, Boud et al (1993) defined reflection as a term that describes the processes used in exploring experience as a method of enhancing understanding. Osterman (1990) considered reflection as the essential part of the learning process as it results in making sense of or extracting meaning from the experience. More recently reflection is defined as the consideration of an experience or of learning to enhance understanding or to inform action (Fry et al 2006). All incorporate essential elements such as enhanced understanding, or a means of making meaning, however, Fry et al (2006) make explicit the informing action component that is vital to take practice forward.
An overview of reflective practice
The notion of reflective practice is now embedded in educators’ and practitioners’ thinking. It is found frequently in occupational therapy literature and elsewhere in nursing (Somerville and Keeling 2004), medicine (Fraser and Greenhaugh 2001) and education (Cowan 2006). It is however not strongly supported by empirical evidence. Nonetheless it maintains a strong component of education and practice. Dewey (1910) initially discussed reflection. Others have developed this concept over time, most notably, Schön (1983, 1987), Kolb (1984), Boud and Walker (1991), Fish et al (1989, 1991) and, Johns (1998). Several models of reflection will be highlighted; these have been selected as occupational therapists and other health practitioners most often use them. The work of Brookfield will be presented and the importance of story telling as a reflective method will be examined (Mattingly 1991). In relation to occupational therapy specifically the work of Alsop and Ryan (1996), Kinsella (2000) and most recently Brown and Ryan (2003) are all worthy of further investigation by the reader.
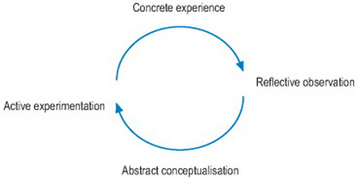
Kolb’s (1984) work on the learning cycle will be considered first, as it is a useful starting point to examine experiential learning and how to develop understanding further. It provides a foundation from which reflective practice can be promoted (see Figure 5.1).
To illustrate the essentials of Kolb’s work complete the task in Box 5.4.
Box 5.4
In pairs, think about a recent clinical event that occurred in your practice, or whilst on placement. Take turns and tell your story of that event.
Note at all stages partners may ask for clarification or ask questions. With stages three and four partners may offer alternative courses of actions for consideration.
Through completion of this task you have completed one full turn of Kolb’s cycle. Stages three and four provide further input into concrete experience and the learning cycle begins again. New understanding or learning is dependent upon the integration of such experiences in relation to practice theory through reflection.
The influence of Schön
It is impossible to examine reflective practice without recognising the work of Donald Schön who brought reflective practice, the reflective practitioner to the fore; as well as the concepts of ‘reflection in action’ and ‘reflection on action’ (Schön 1983, 1987).
Schön examined the relationship between professional knowledge and professional competence; he proposed that practitioners should examine artistry in their own profession through observing and learning through reflection. Such ‘reflection on action’ or practice is core to professional development as recognised experts in a profession demonstrate artistry that cannot be taught through traditional methods (Fry et al 2006). Furthermore, when working with non-complex cases or situations Schön proposed that experts demonstrate near automatic performance or ‘knowing in action’. As experts in their specialist area, they know more than they can say or make verbally explicit, they are skilled and spontaneous in their performance but are often unable to articulate the dynamics of their practice fully. When questioned about their practice: they often describe the rules and procedures that underpin their practice – not what they did or what guided their thinking, such rules and procedures remain static and unchanged and do not reveal how or why they performed in that manner.
This process of rethinking some part of our ‘knowing in action’ leads to on the spot experimentation when the practitioner acts and thinks simultaneously or ‘reflection in action’. This process involves the practitioner in reshaping their actions in the midst of the action. Schön considered that ‘reflection in action’ was often a consequence of surprise when engaged in an experience that challenged our usual assumptions or knowledge. This process may also be recognized as ‘thinking on your feet’ (Fish et al 1991) (Box 5.5).
Box 5.5
Can you recall the last time you were aware of ‘thinking on your feet’ in your practice? Revisit that event, what prompted you to ‘think on your feet’ and why? What was the outcome?
Schön proposed a ‘reflection in action’ coaching method for practitioners to use with learners, whether students or new staff, in their workplace to acquire new skills and insights. It involves three stages:
Some aspects described above may be familiar strategies to you, you probably do not use the language described above. Nonetheless, using this method allows the learner and the coach to work collaboratively in developing ‘reflection in action’.
Types of reflection
In discussing reflection it becomes clear that there are some debates in the literature. These often centre on reflection and its relationship to meta cognition (Eraut 1995). Kember (2000) proposes that meta-cognition involves some self-reflection to monitor one’s own thinking. What is important is that reflection needs time, space, structure and support to be developed. Three distinct types of reflection in relation to continuing professional development can be identified in the literature namely (Kinsella 2000, Cowan 2006, Fade 2007):
To illustrate the above consider the following. You are contemplating a change of job, you browse the professional journals and websites: this gives you an idea about what is out there, the jobs available, the location and type of clients and the range of staff you might be working with (Anticipatory). You go on a visit to a particular job location: while there, you stop to think about how you would complement or fit into this team. What could you offer here and in what ways would this post help your career? What would it be like to work here? (Reflection in action). Once the visit is completed you review the experience: Who did you meet? What might you contribute? What was it like? (Reflection on action). Now you have to decide to apply or not to apply.
Let’s return now to David and Michelle:
David has just been informed that his final placement will be in a forensic mental health setting in a specialist hospital. What are his anticipatory reflections? These may include thoughts regarding: anxiety about the setting or client group, what are the clients like? What have they done? What will the environment be like? What can I bring from my past experiences to this placement? What others can you think of?
Michelle has decided to explore further study options. She has a BSc (Hons) and has completed practice-related courses throughout her career. Now she is interested in Master level study. She is unaware of what the possible routes may be to a Master level qualification. In anticipation of returning to study she is examining her work and life balance. What would be feasible for her? What skills or knowledge does she already have? How can she structure her family life to ensure she can cope with returning to study? Is funding available? Will she be able to have study leave? And will her manager support her decision? What others can you think of?
Often we engage in anticipatory reflection without being aware of doing it; however conscious forward thinking can help you prepare for a particular event or help you to decide on possible courses of action. As Cowan (2006) states this type of reflection can ‘establish goals for subsequent learning or development by identifying needs, aspirations and objectives which will subsequently be prominent in the mind’ (p. 51) (Box 5.6).
Models of reflection
This next section explores a number of models that can aid your ability to reflect on your own or with peers or team members. They offer you strategies and structures to guide and develop your skill as a reflective practitioner. These models offer a logical framework to make sense of complex information. Alternatively, there are other methods that are also useful to explore to enhance your reflective abilities such as the use of metaphors, literature (medical humanities), drawing and photography (Mattingly 1998, Murray et al 2000, Denshire 2005, McIntosh and Webb 2006).
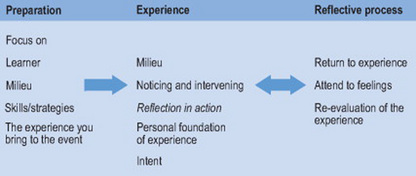
The model developed by Boud and colleagues (Boud et al 1985, Boud 1991) states that reflection is grounded in the personal foundation of experience of the learner (Boud and Knights 1996) that is, the belief that all experiences to date have contributed to shaping who that person is now. Furthermore, it also includes the notion of intent, what is the learner’s intent in relation to the learning experience as this gives a particular focus for that learning context (Fig. 5.2).
Preparation
Boud’s model places emphasis on preparation prior to a learning event, and this mirrors anticipatory reflection, as discussed previously. However, here there is a more in-depth approach to consideration of the learner, the milieu or the environment that the event will take place, and importantly the learner’s skills set and strategies. Giving time to consider strategies, which one may use in that event can help preparation and flexibility when in the situation. David’s experience illuminates this aspect (see Box 5.7).
In David’s final placement his intent to learning may differ if he feels this is his last hurdle to professional practice or alternatively this is an area in which he feels he would like to specialize, in the future.
David as learner
Thought has to be given to the skills and strategies that David has and the experiences he can draw on from his past (both personal and professional), as well as his knowledge in relation to the setting, e.g. forensic psychiatry. David recognizes that he has had some experience working with clients in a mental health community team, but this was in a very different setting. Similarly, he has worked with teenagers who were challenging so he may be able to utilize some of those experiences. He has to consider what other skills and strategies he can take into this learning experience?
The milieu
This involves thinking about the placement setting thoroughly the types of clients, the scope of occupational therapy, environment, staff and security.
For example, if David considers what it is like to work in a secure environment this will heighten his awareness of possible risks and safety. He may discuss this issue with his fellow students who have been to that, or similar placements previously and who may offer useful practical advice. Alternatively he may ask his educator for advice when he starts the placement.
Experience
The middle section of the model deals with the learning experience. Learning occurs in context, which encompasses both the human and physical environment, we learn through our interactions within the environment. When in a specific context it is important to notice what is happening to ourselves in relation to the external factors, learners can be assisted to do this by others highlighting aspects that may be important. For example, a practitioner may draw the learner’s attention to how a client is positioned in a group task, or to how they are sitting in their chair. You may intervene in an external way (do something) for example: you talk with someone; or it may be that you assist someone to complete a task as you become aware that they are having difficulties. Alternatively you may intervene internally (think something) for example noting some follow-up activity, such as reading more about a condition or a treatment. Self-vigilance for the person involved is key, being aware of how they are acting and modifying their actions in the midst of experience is ‘Reflection in action’. Here too David’s experience helps us understand this aspect further (see Box 5.8).
Box 5.8 David’s reflecting on ‘reflection in action’
At a supervision session in week 6 of an 8-week placement, David’s supervisor asks him to discuss why he changed the format of a group session he had conducted the previous day. David explained that he had planned to do a group collage with a number of the men on the ward. He had decided to hold the session in the ward treatment area, as he was aware that some people could not be engaged in treatment sessions off the ward. He had chosen to do a group collage about football, as it was a constant subject on the ward, with most men contributing on their team and its progress through the season.
The group collage was an activity that had many levels of engagement and would also allow for those who had difficulty attending and concentrating for long periods, an opportunity to dip in and out of the session as they needed to.
He explained that his original plan for the session was that each would work for 10 minutes on their own football themes and that this would then progress to each member contributing their individual work to the group collage; followed by a discussion of everyone’s work. However, David observed that at 10 minutes into the task the four men were really engaged with creating their own collage, he felt that if he had stopped them to move to the group task this would disrupt their engagement with the task. He decided to go with the flow of the activity and take his lead from them. Approximately 20 minutes into the task most seemed to have completed their creating phase, David decided instead of making the group collage he would stay with the individual focus. He asked someone to discuss what they had created and its significance to them and a lively discussion followed.
David acknowledged that his strategy of going with the flow could have been problematic, however, he felt that the group had its own volition and he was prepared to go with them at that moment in time. He felt that he was skilled enough to work with the unfolding situation and support the members and the task.
David’s supervisor asked if he would have chosen this course of action at the start of his placement? David considered his response; he felt possibly not but reflected that his experiences over the past weeks of being part of the group, and gradually taking more responsibility for leading the sessions had given him a level of confidence and a feel for the participants that supported his ‘on the spot’ decision.
The final aspect of the model is the reflective processes; this is ‘reflection on action’. Following the event the learner returns to the experience reviewing and describing what happened in as much detail as possible. The learner needs to attend to their feelings – how it felt for them. They must re-evaluate the experience – What it means now? What may it mean for their future actions or behaviour.
The strands of reflection
Another model commonly used by practitioners that was developed by Fish et al (1991) is entitled ‘strands of reflection’. This model differs from Boud et al (1985) in that it concentrates on providing a structured and systematic method to review an event or experience: there is no implicit anticipatory reflection component. From my experience of working with practitioners this model is often regarded positively and seems to offer a useful method to assist them in detailed and contextualised ‘reflection on action’.
To aid the use of the model it is useful to think of your experiences, like a rope that is made up of several strings or strands; these strands are woven together and build a stronger or richer perspective to the reflective process. Within the model, four key strands come together to help reflection in an organised manner: factual strand, retrospective strand, sub-stratum strand and the connective strand. Together they provide a means of reflecting upon your practice. They are not intended to be used independently; they seek to facilitate practitioners to interpret their practice experiences. By separating the four strands, each can be looked at closely and then all four can be reformed as a whole from which the practitioner can move forward.
The factual strand: This acts to set the scene; briefly it describes the context of the practice situation. Events are recalled in time order; what happened; how did you feel, think and why? Practitioners are asked to pinpoint any critical incidents that arose during the situation.
The retrospective strand: This considers what patterns are visible in the practice as a whole. It asks what aims were set, and were these achieved. It asks practitioners to see themselves in relation to the practice event.
The sub-stratum strand: This requires practitioners to review what customs, traditions, beliefs were brought into a situation or were already there? Furthermore, what assumptions, beliefs or values underpinned the actions they took and the decisions they made.
The connective strand: This brings it all together: what has been learnt from this practice experience and how will it relate to future practice? How might thoughts and actions specific to this situation be modified in light of experiences or further thought or reading? Finally, it considers the implications for future practice (Box 5.9).
Box 5.9 Illustrating strands of reflection – Michelle’s school visit
The factual strand: Michelle recently took over a small number of children who were on the caseload of a practitioner who has left the service. Michelle has become involved with these specific children as they have outstanding areas of occupational performance to be assessed. Michelle visited one child (Fiona) in a mainstream school. Following a 30-minute session with Fiona that was conducted in the therapy room Michelle returned Fiona to the class as she wished to discuss her performance with the class teacher. It was just before lunchtime. Michelle waited till the class had gone and then fed back to the teacher on her session with Fiona. This took about 10 minutes. Michelle made suggestions to help Fiona in the classroom. The teacher listened, thanked her and then left for lunch. Michelle was surprised by what she perceived as a lack of interest from the teacher.
So let’s unpack what happened here, the retrospective strand: Michelle went about her business as she always did when assessing children in school. She always reported back to the class teacher offering some suggestions if possible. She had aimed to assess the child and this was completed successfully. Michelle reflected that this was her usual approach. Why was the teacher uninterested in her input? The substratum strand: Michelle considered what beliefs and customs she brought to this situation or that were already there. As she thought through the exchange, she considered that although she had worked in her normal manner this was a new school to her and a teacher whom she had not worked with before. Michelle began to recognise that although she had positive relationships in the schools where she worked this was a new area for her and perhaps she needed to spend more time with the teachers: finding out what they already knew about occupational therapy, explaining how she hoped to work with the children and them. She began to consider that perhaps she should have done more preparatory work both for herself going into a new school with the school staff. She also realised that she had assumed that the previous therapist had worked in a similar manner to her, which may not have been the case. The connective strand: Michelle decided that to build collaborative relations with the teachers here and to learn how best to work with them to support the child in their classroom she would have to do some work with this school. This could involve Michelle doing some information sessions with the staff either in small groups or individually to explore how they could all best work together.
The strands of reflection model and the process undertaken by Michelle are described as the DATA method (Peter, 1991). DATA outlines the four stages of the process namely:
This provides a useful shorthand way to remember those reflective steps.
The final model discussed comes from nursing, Johns (1998, 2000, 2004) developed the ‘model of structured reflection’ (MSR) which like the strands of reflection model is composed of a series of questions, in a logical order to help the reflective practitioner tune into an experience and to understand the different ways of knowing, e.g. personal, ethical, empiric; that inform their practice – when practitioners share their stories they describe their aesthetic response. The MSR is as Johns (1998) states a ‘device to enable practitioners to penetrate the essence of reflection on experience’ (p. 3). The model commences by focusing in on the self, which encourages the practitioner to pause amidst their busy practice and find a quiet space to focus on their thoughts and feelings. The main part of the MSR is ‘looking out’ which offers a series of reflective cues that focus the practitioner’s attention on significant issues within their work-based experience (Box 5.10).
Box 5.10 Model for Structured reflection –14th Edition (Johns 2004)
| Reflective cue | Way of knowing |
|---|---|
| Bring the mind home | Aesthetics |
| Focus on a description of an experience that seems significant in some way | |
| What particular issues seem significant to pay attention to? | Aesthetics |
| How were others feeling and what made them feel that way? | Aesthetics |
| How was I feeling and what made me feel that way? | Personal |
| What was I trying to achieve and did I respond effectively? | Aesthetics |
| What were the consequences of my action on the patient/client, others and myself? | Aesthetics |
| What factors influenced the way I was feeling, thinking or responding? | Personal |
| What knowledge did or might have informed me? | Empirics |
| To what extent did I act for the best and in tune with my values? | Ethics |
| How does this situation connect with previous experiences? | Reflexivity |
| How might I respond more effectively given this situation again? | Reflexivity |
| What would be the consequences of alternative actions for the patient/client, others and myself? | Reflexivity |
| How do I NOW feel about this experience | Reflexivity |
| Am I more able to support myself and others better as a consequence? | Reflexivity |
| Am I more able to realize desirable practice monitored using reflexivity | |
| Appropriate frameworks such as framing perspectives, | |
| Carper’s fundamental ways of knowing, other maps? | |
The ‘model for structured reflection’ is not meant to be used prescriptively (Johns 2004). Johns (2004) offers an illuminative discussion of the model’s use in practice and those interested should read further.
Other methods for promoting reflection
The models discussed in this chapter are not meant to be taken as the only methods for reflecting, many other models exist, practitioners can choose the model that they find most useful. We each tune into different elements so diversity is required. Moving away from specific models of reflection it is worthwhile considering two other distinct methods that can assist in developing reflection further; story telling (see the work of Mattingly) and critical incidents (see the work of Brookfield) both these methods encourage sharing practice with others.
Telling stories
We all tell stories of our practice informally with our colleagues on a daily basis. Telling stories or narrative is proposed as the primary form by which human experience is made meaningful (Polkinghorne 1988). As personal meaning is offered through the individual’s story, Mattingly (1991) considers stories are particularly useful for addressing experiences and are therefore a useful tool for reflection. Mattingly (1998) regards story telling as being ‘event and experience-centred, which create experiences for the listener or audience’ (p. 8). Therefore the sharing and discussion of stories can aid all participants’ reflections. Stories hold our experiences together, allowing links to the past, present and crucially, to the future. Through our own practice stories we are trying to make sense or give coherence to our actions and experiences and importantly give coherence and meaning to our clients’ stories (Mattingly 1998). Thus using stories to promote reflection is vital for practitioners to develop their practice. Stories can be written or verbal: they can be sketches/vignettes or portraits of practice in words (Fish 1998) that capture the essence of the story or can be developed to give detailed accounts of our practice, for example, writing reflective journals. Recalling our stories may be part of an individual’s supervision session or a feature of team meetings. Living (1999) offers perspectives of a specific client from a range of different team members; each offering a slightly different view. Reflecting on our stories highlights the cognitive, affective and temporal aspects of experience (Johns and Freshwater 1998) sharing our practice stories illustrates our thinking, our practice and promotes reflection.
Exploring critical incidents
Critical incidents are not exactly what they sound like; they are not dramatic events such as life and death situations or crisis; indeed they are often small or indeed common events that are meaningful to an individual, often, because these incidents touch them at an emotional level. The critical incident’s significance lies with the practitioner and what they do following the event (Brookfield 1990). The incident is described verbally or written, shared with others and the question asked – why was the incident critical? McAllister (2003) offers a guideline for the analysis of critical incidents to promote advance practice. These include:
Critical incidents by their nature are unplanned, it is important that they are explored as such incidents can be a powerful learning tool for those involved.
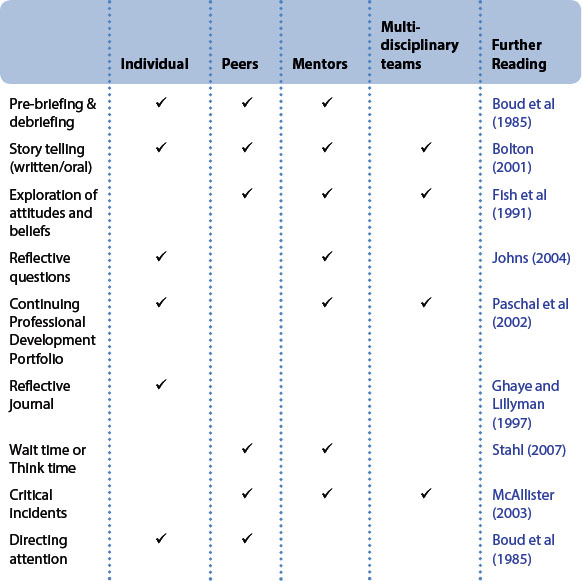
When and how to reflect are questions often asked by practitioners. Reflection should take place when you are involved in something that is new or surprising, when faced with complex or difficult situations, and after CPD activities. What is important is that you take the time to reflect on such activities. Table 5.1 summarises a range of strategies for developing reflection both as an individual practitioner and as a shared task for peers and teams.
Signs of reflections
This chapter has looked at various ways of ‘doing and being’ reflective. A question often asked is how do we know that we are reflecting? Reflective processes can be observed in several ways; for example, the intensity of a discussion may be evidence of reflection. Alternatively it may be the quality of silence, or it may be the nature of questions asked. For example:
You can of course think of others in relation to your own or your team’s practice. Changes in practice and reconstructing a different way forward may also be evidence of a reflective process in action. Such changes may of course be small and cumulative and as a result they may not be noticed immediately by others, so it is important that you note such changes and share them with your colleagues.
Outcomes of reflection
The above models, storytelling, critical incidents, and other strategies identified all must lead to action by the individual or by the team. It is imperative that action follows reflection, otherwise the reflective process becomes a closed activity. The actions that result from reflection may take a number of forms but they all have implications for practitioners and their practice.
Reflection takes active involvement, time, structure and support from others. It is important that reflection leads to action – those actions have implications for your practice and ongoing continued professional development. Doing reflection is after all a professional imperative to being a reflective practitioner. To conclude the words of Drucker, an American educator, are fitting ‘Follow effective action with quiet reflection. From the quiet reflection will come even more effective action’.
Summary
This chapter has reviewed reflection and reflective practice; it has considered the significance of reflective practice for the practitioner, both, at an individual and at a team level. Being a reflective practitioner is a key skill in today’s health and social care environment. Reflection on practice and experience is necessary for continuing professional development. Key theorists have been included to trace the historical and recent development of reflective practice. A number of models and a range of methods for developing reflection in practice have been introduced and illustrated. Readers are encouraged to use the ‘Promoting Reflection’ activities in their work setting.
Alsop A, Ryan S. Making the most of fieldwork education: a practical guide. Cheltenham, UK: Nelson Thornes, 1996.
Bolton G. Reflective practice: writing and professional development. London: Paul Chapman Publishing Ltd., 2001.
Boud D. Relocating reflection in the context of practice: Rehabilitation or rejection?. Paper presented at Professional Lifelong Learning: Beyond Reflective practice. 2006. July 2006 http://www.leeds.ac.uk/medicine/meu/lifelong06/ 28 June 2007
Boud D, Knights S. Course design for reflective practice. In: Gould NG, Taylor I, editors. Reflective Learning for Social Work: Research, Theory and Practice. Aldershot, UK: Arena; 1996:23-34.
Boud D, Walker D. In the midst of experience: developing a model to aid learners and facilitators. Paper presented at the National Conference on Experiential Learning empowerment through experiential learning: explorations of good practice. University of Surrey. 1991:16-18. July 1991
Boud D, Keogh R, Walker D. Promoting reflection in learning: a model. In: Boud D, Keogh R, Walker D, editors. Reflection: Turning Experience into Learning. London: Kogan Page, 1985.
Boud D, Cohen R, Walker D. Using Experience for Learning. UK, Open University Press: Milton Keynes, 1993.
Brookfield S. Using critical incidents to explore learners’ assumptions. and associates. Mezirow J, editor. Fostering Critical Reflection in Adulthood: A Guide to Transformative and Emancipatory Learning. San Francisco, CA: Jossey-Bass, 1990.
Brown G, Ryan SE. Enhancing reflective abilities: interweaving reflection into practice. In: Brown G, Esdaile SA, Ryan SE, editors. Becoming an Advanced Practitioner. Edinburgh, UK: Butterworth Heinemann; 2003:118-144.
Cowan J. On becoming an innovative university teacher: Reflection in action. Berkshire: Society for Research into Higher Education & Open University Press, 2006.
Cressey P, Boud D. The emergence of productive reflection. In: Boud D, Cressey P, Docherty P, editors. Productive Reflection at Work: Learning for Changing Organisations. London: Routledge, 2006.
Denshire S. ‘This is a hospital, not a circus’: Reflecting on generative metaphors for a deeper understanding of professional practice. International Journal of Critical Psychology Issue 13: Critical Professional. 2005;13:158-178.
Dewey J. How we Think. Chicago: University of Chicago, 1910.
Drucker P. Accessed on 04/07/2007 http://www.brainyquote.com/quotes/authors/p/peter_f_drucker.html, 2007.
Eraut M. Developing Professional Knowledge and Competence. London: The Falmer Press, 1994.
Eraut M. Knowledge creation and knowledge use in professional contexts. Studies in Higher Education. 1995;10:117-133.
Fade S. Learning and assessing through reflection: a practical guide. Making practice-based work. 2007. www.practicebasedlearning.org. accessed 24 February 2007
Fish D. Appreciating practice in the caring profession: Refocusing professional development and practitioner research. Oxford: Butterworth Heinemann, 1998.
Fish D, Twinn S, Purr B. How to Enable Learning Through Professional Practice. London: West London Press, 1989.
Fish D, Twinn S, Purr B. Promoting Reflection: Improving the Supervision of Practice in Health Visiting and Initial Teacher Training. London: West London Institute, 1991.
Fraser SW, Greenhaugh T. Coping with complexity: educating for capability. British Medical Journal. 2001;323:799-803.
Freire P. Pedagogy of the Oppressed. London: Penguin, 1972.
Fry H, Ketteridge S, Marshall S. A handbook for teaching and learning in higher education. In Enhancing academic practice. London: RoutledgeFalmer; 2006.
Ghaye T, Lillyman S. Learning journals and critical incidents: reflective practice for healthcare professionals. Dinton: Quay Books, 1997.
Health Professions Council. Standards of Proficiency: Occupational Therapists. London: Health Professions Council, 2004.
Health Professions Council. Your guide to our standards for continuing professional development. London: Health Professions Council, 2006.
Johns C. Opening the doors of perception. In: Johns C, Freshwater D, editors. Transforming nursing through reflective practice. Oxford: Blackwell Science, 1998.
Johns C. Becoming a Reflective Practitioner A Reflective and Holistic Approach to Clinical Nursing. In Practice Development and Clinical Supervision. Oxford: Blackwell Science; 2000.
Johns C. Becoming a Reflective Practitioner. Oxford: Blackwell Science, 2004.
Johns C, Freshwater D. Transforming nursing through reflective practice. Oxford: Blackwell Science, 1998.
Kember D. Reflective teaching and learning in the health professions: action research in professional education. Oxford: Blackwell Science, 2000.
Kinsella EA. Professional development and reflective practice: Strategies for learning through professional experience – A workbook for practitioners. Ottawa, Ontario: CAOT Publications ACE, 2000.
Kirkpatrick EM. Chambers 20th Century Dictionary. Edinburgh: Chambers, 1988.
Kolb DA. Experiential learning; Experience as the source of learning and development. NJ, Prentice Hall: Englewood Cliffs, 1984.
Kuit JA, Reay G, Freeman R. Experiences of reflective teaching. Active Learning in Higher Education. 2001;2(2):128-142.
Living R. The team’s story of a client’s experience of anorexia nervosa. In: Ryan SE, McKay EA, editors. Thinking and reasoning in therapy. Cheltenham, UK: Stanley Thornes, 1999.
Mattingly C. Narrative reflection on practical actions: Two learning experiments in reflective storytelling. In: Schön DA, editor. The Reflective Turn. San Francisco, CA: Jossey Bass, 1991.
Mattingly C. Healing dramas and clinical plots. In The narrative structure of experience. Cambridge, UK: Cambridge University Press; 1998.
McAllister L. Using adult education theories: facilitating others’ learning in professional practice settings. In: Brown G, Esdaile SA, Ryan SE, editors. Becoming an advance healthcare practitioner. Edinburgh, UK: Butterworth Heinemann, 2003.
McIntosh P, Webb C. Creativity and reflection: An approach to reflexivity in practice. Paper presented at Professional Lifelong Learning: Beyond Reflective practice. 2006. July 2006 http://www.leeds.ac.uk/medicine/meu/lifelong06/ 28 June 2007
Murray R, McKay E, Thompson S, et al. Practising reflection: a medical humanities approach to occupational therapist education. Medical Teacher. 2000;22(3):276-281.
Osterman KF. Reflective Practice: A new agenda for education. Education and Urban Society. 1990;22(2):133-152.
Paschal KA, Jensen GM, Mostrom E. Building portfolios: a means for developing habits of reflective practice in physical therapy education. Journal of Physical Therapy Education. 2002;16(3):38-53.
Peters J. Strategies for reflective practice. In: Brocket R, editor. Professional development for educators of adult and continuing learning, No.51. San Francisco: CA, Jossey Bass, 1991.
Polkinghorne D. Narrative knowing and the human sciences. Albany, NY: State University of New York Press, 1988.
Quality Assurance Agency for Higher Education. Benchmark statement: Health care programmes phase 1, occupational therapy subject bench marking group. Gloucester, UK: Quality Assurance Agency for Higher Education, 2001.
Schön D. The Reflective Practitioner: how professionals think in action. New York: Basic Books, 1983.
Schön D. Educating the Reflective Practitioner. San Francisco, CA: Jossey Bass, 1987.
Somerville D, Keeling J. A practical approach to promote reflective practice within nursing. Nursing Times. 2004;100(12):42-45.
Stalh RJ. Using think time and wait time skillfully in the classroom. 2007. Available at http://atozteacherstuff.com/pages/1884.shtml accessed 6 July 2007
Winpenny K, Forsyth K, Jones C, et al. Group reflective supervision: Thinking with theory to develop practice. British Journal of Occupational Therapy. 2006;69(9):423-428.