Chapter 2 Using Theory in Practice
Overview
Occupational therapists react and respond in a variety of ways to the day-to-day occupation-focused decisions that need to be made in practice. The variety of responses are triggered and challenged by the environmental contexts, the conceptual thinking and technical ability of the practitioner, in addition to the presenting needs of the clients.
In this chapter we will illustrate the choices and issues that occupational therapists encounter when making decisions about the theories to support their occupation-focused, evidenced-based choices. To illustrate this we will provide a case overview of an organizational approach to practice scholarship. The voices of occupational therapists who are embracing the challenge and celebrating the benefit of using theory in their practice will be presented in the second part of the chapter together with a summary of measures to assist practitioners engage with theory in practice.
Historical context
Scholarly work to locate the theoretical concepts underpinning the practice of occupational therapy has gathered pace only in recent times (Duncan 2006). Despite these advances, there continues a debate in the profession about the perceived gap between theory and practice (Forsyth et al 2005a, Duncan 2006). Implied here is that practitioners have found it difficult to engage in or value theory (Mattingly and Fleming 1994) and that academics have detected that theory and research is not used routinely in practice (Fisher 1998, Wood 1998, Christiansen 1999). To support theoretically oriented occupational therapy practice, Kielhofner (2004) presented a contemporary, synthesized overview of the development, current position and future of knowledge available to support practice. In this valuable, in-depth précis Kielhofner describes the conceptual foundations of occupational therapy, outlines the historic difficulty that the field has experienced in infusing theory into practice and makes suggestions for further development. Despite this contribution calls continue for the profession to embrace the use of theory in practice in order to raise standards and to meet the growing opportunities presented to empower those who require occupational therapy intervention (Forsyth et al 2005a). We aim to support this position through the presentation of this chapter.
Introduction
First we examine the nature and importance of putting theory into practice. We acknowledge that therapists find this challenging. We argue that using a scholarship of practice philosophy which supports conceptual models of practice, supports effective occupational therapy by shaping theory-driven actions and drawing from the available evidence base. We suggest that the use of conceptual models of practice is important in order to provide a practice framework for decision making, to make practice relevant for service users and for occupational therapists to develop expertise.
We then turn to a case study of applying the scholarship of practice approach to encourage the use and development of theory in daily practice. Through the explanation of practitioner quotes we will argue that the application of theory to practice is multidimensional and is influenced by the therapists’ attributes, the support available within the environmental context and the mechanisms that therapists have available and choose to engage in. We conclude with suggestions of practical ideas that therapists can consider when seeking to develop their practice through the understanding and application of occupational therapy conceptual theory.
What are theories and why do they matter?
Theories are connected sets of ideas that form the basis for action. Theories explain the way things are and predict what will happen if we make changes. Because they provide explanation and prediction theories can be scrutinized, debated and tested. This is important because it is the way in which knowledge and understanding move forward, guiding actions by making them better-informed.
Let us stray outside occupational therapy for a short while to look at a vivid example without being weighed down by professional knowledge or ‘baggage’. Worries about climate change are spawning many competing and complementary theories. These theories are not irrelevant intellectual exercises. Mankind is genuinely concerned about the possible existence and consequences of global warming. The explanations and predictions provided by these climate-related theories are highlighting the importance of changing behaviour and attitudes; and further, suggesting the nature of the required changes. This generates (heated!) debate which challenges and refines the theories: their explanations and predictions. We begin to think about things differently and do things differently: these changes affect the course of the future.
The alternative is not thinking very much about things that appear to be OK for the moment, or that feel too big or too difficult to change. This often entails doing more or less the same as in the past and achieving similar results to the past. This becomes a problem when it is combined with changing circumstances. In our example of climate change the central problem is an acceleration effect: the rapid growth of damaging behaviours caused by rapid ‘development’. In health and social care the changing circumstances are linked to relatively rapid changes in the age profile and family structures of the population; healthcare developments that enable more people to live for much longer with significant impairments; changed social expectations about the delivery of care and so on. We need to scrutinize what we do now to discover our implicit explanations of how things work and fit together, unearthing our views about what is really important. This enables predictions and informed choices to be made.
To complete our use of the climate change example; there is a theory which might be summarized as follows: There is a role for ‘green’ taxation of air travel in efforts to combat global warming. Broadly, the elements of explanation in this theory are twofold:
Many testable predictions can be made about the effects of increasing taxation of air travel, for example:
We are not expecting anyone to be convinced by this scant account of green taxation: far greater scientific and economic rigour would be required. The point is simply that the theory provides testable explanations and predictions that can be debated and can guide actions.
Debate about really big questions should be communal so that many perspectives are brought into the process of refining ideas and actions. Debate in day-to-day occupational therapy practice will sometimes be social (e.g. within multidisciplinary team meetings, during clinical supervision or as part of continuing professional development (CPD) or when reconfiguring services) but often the debate will be inside the head of the therapist during ‘reflection’ or ‘critical thinking’ (see Chapter 5).
Good therapists never stop debating with themselves and others about how things fit together, what should be regarded as important, what interventions are predicted to be most effective, how their earlier interventions worked out and so on. If we stop thinking about explanations, predictions and the consequences of actions, the development of our professional practice ceases and it gradually becomes outdated, out of touch with changed circumstances and less effective for clients. Without thinking with underpinning theory professional practice is guesswork (Higgs et al 2001). Thus it is no surprise that the Health Professions Council (2003) has identified that registrant occupational therapists must be able to use ‘the established theories, models, frameworks and concepts of occupational therapy’ in order to demonstrate their clinical proficiency at formulating and delivering plans to meet service user need. These theories and models provide a rigorously built framework to help us to choose what we should do and explain these choices to others. Making well-informed decisions and convincing others of their worth lies at the heart of professional practice. In most cases your therapeutic interventions will be thwarted if your client cannot see their worth. In addition you will not be able to provide the service that you would wish to provide for clients if you cannot convince colleagues and other stakeholders that your actions and plans are well informed.
Every discipline develops a specialized knowledge base, important concepts, models and theories to help busy practitioners make rapid but well-informed decisions about their practice. Examples of specialized knowledge in occupational therapy include the relationship between a person’s belief in their ability to undertake a task on their performance ability or how a person with motor limitations can be augmented to maximize their function by adapting their environment (Kielhofner 2004). Particular perspectives on key concepts in occupational therapy might embrace occupational performance and volition. Finally, some examples of models or theories that synthesise the knowledge and concepts in occupational therapy are the Model of Human Occupation (MoHO) (Kielhofner 2008) and the Canadian Model of Occupational Performance (Townsend and Polatajko 2007). We argue that the ability to think within a defined framework of conceptual ideas assists the therapist in a number of ways. These include:
So are there problems with integrating theory into occupational therapy practice?
In short, yes – at least for the present. Despite the acknowledged importance of infusing practice with insights derived from research evidence, conceptual models and pertinent theories (Cusick 2001, Duncan 2006), practitioners have expressed disillusionment with the relevance of theory to their practice (Closs and Cheater 1999, Kielhofner 2005) while academics observe that existing knowledge in the field is not being systemically applied in practice (Fisher 1998, Wood 1998, Christiansen 1999). Therapists might, therefore, be viewing theory as more ‘ornamental’ than ‘instrumental’ to their practice. Why might practitioners not find theory relevant to their everyday work?
There is little doubt that the definition of ‘theory’ poses challenges in many disciplines (Nixon and Creek 2006). Other issues include the demands and constraints of practice settings that leave limited time for reflection and innovation (Oxman et al 1995, McCluskey and Cusick 2002). Moreover, traditional models of theory building are based on ‘technical rationality’, the idea that practical action flows naturally from basic knowledge (Schön 1991). In fact intermediate work is required to reformulate basic knowledge in ways that make its relevance and application to practice more certain and obvious (see Chapter 15).
We too have heard therapists proclaim that they are uncomfortable with theory. The reasons for this are expressed in different ways. Some therapists suggest that:
In addition, the need to learn, appraise, synthesize and use the various theory bases which apply to occupational therapy practice can be overwhelming. For instance, the differences in some of the conceptual definitions can be minimal and might challenge the reader to wonder why separate frameworks were established. Equally, the differences can be huge and challenge the reader to wonder whether they relate to the same therapeutic intervention at all.
So what do all these concerns about applying theory to occupational therapy practice indicate? Almost certainly, we should view the knowledge, conceptual and theoretical bases of occupational therapy as not yet as fully developed as practitioners need. Work needs to be done to better articulate key conceptual models and theories. Accessible presentation will encourage use and scrutiny, in turn encouraging development of both theory and practice. Secondly, habits and confidence are important. Initial support to think clearly with the supportive framework of a well-grounded conceptual model or theory can help well-informed reflective practice to become a good habit and source of professional pride.
A potential way forward: Scholarship of Practice
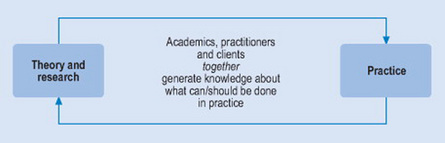
There is growing recognition that the kind of knowledge required for decision-making in practice is different from the kind of knowledge that is generated to explain phenomena; that is, knowing about something is not the same as knowing how to do something (Schön 1991, Higgs et al 2001). In response to this, the ‘Scholarship of Practice’ has been used recently in some occupational therapy services in the UK and is defined as delivering and generating evidence for practice through a partnership between academia and practice (Forsyth et al 2005a) (see Figure 2.1). In this way theory is built in practice and considerations include both the generation of theory and the use of theory in practice. In addition the Scholarship of Practice pays attention to building tools for practice such as standardized assessments or visual representations that synthesize ideas and act as reminders. Scholarship of Practice gradually builds conceptual models of practice that are informed by challenges from practice, reflective wisdom, evidence from research and the abstract thinking of theory building.
Focusing on conceptual models
It has been argued that conceptual models of practice link theory to practice within a scholarship of practice philosophy (Kielhofner 2004, Duncan 2006). Relatively abstract and general theories are formulated into concepts and propositions which support practice-based action and skills, providing guidance as to how to use theory in practice. Thus a conceptual model of practice includes both theory in addition to practice-based tools for application of theory. Most disciplines will have more than one conceptual model and these will function to help professionals understand complex practice-based challenges and how to formulate decisions about bespoke intervention packages for individuals. The aim here is to ensure skilled practice action (Figure 2.2). One example of a conceptual model which describes occupational therapy concepts is the Model of Human Occupation (MoHO) (Kielhofner 2008). The MoHO seeks to explain how human occupation is motivated, patterned and performed. It assists occupational therapists to understand their client’s ability to perform their occupations with their own temporal, physical and sociocultural environment. Within the framework conceptualized in the MoHO, 20 assessment tools have been developed, to date, for clinical practice application. The literature about these concepts has over 25 years of history which adds weight to the claim that the model provides professional knowledge that is a comprehensive and evidence-based framework for occupational therapy practice.

Figure 2.2 An equation to illustrate the importance of theoretical knowledge synthesised with understanding of the individual and their environment in order to deliver the best practice solutions for and with each service user.
Conceptual models are useful as tools for thinking and become a key element for problem setting and problem solving (Parham 1987, Munoz et al 1993). Where a clinician is challenged to make sense of an uncertain situation that initially makes no sense (Schön 1991) a robust, relevant and well-understood model of practice can assist. It offers a means of identifying and rationalizing what is being observed and a set of ideas within which to frame practice decision-making. Thus the articulation of specific professional knowledge and service user outcomes can be made with greater clarity.
Maximizing a person’s opportunity to gain benefit from intervention is generally and rightly the purpose of a clinician’s decision making in practice (Lloyd Smith 1997, Tickle-Degnen 1998). Included here is the goal to make interventions cost effective and based on the best available evidence (Law et al 2001). If therapists are able to use models of practice judiciously and reflectively it follows that they will be better positioned to understand and use the associated practice skills of assessment and intervention. A robust conceptual model of practice facilitates constructive critique of ‘custom and practice’ and the integration of research evidence. This can result in occupationally conceptualized, theoretically based, evidence-informed thinking.
Models of practice can bring a fresh perspective, stimulating a practitioner’s understanding of a person’s occupational need at a higher level of sophistication and creativity. It seems logical then for occupational therapists, who are working with people who have challenges with their occupational participation through illness or disability, to use a set of conceptual ideas to help them to understand and formulate the information that they are gathering about a client’s needs. No therapy would however be complete without the therapist being able to communicate the purpose, process and outcomes of intervention to service users and colleagues. A conceptual practice model, used thoughtfully, will help this communication to be clearly articulated thus raising the profile of the clients’ requirements and the best practice solutions available via occupational therapy intervention.
So how can this be achieved?
Conceptual models of practice have a structure that is supportive of reflective and theoretically formulated practice. What can facilitate and support therapists’ use of conceptual models within everyday clinical work? We now turn to a case study of applying the scholarship of practice model. The main points that will be drawn out through the case study will be that therapists can consider their own attributes and attitudes towards the use of theory in their practice; that leaders within an organisational context can support the use of theory to enhance practice standards and that therapists can expect, develop and use various mechanisms to extend their understanding and practical application of theory for practice.
Lessons from a case study
In this case study we use quotations from practitioners to illustrate the supports that can assist therapists to develop skills in the use of conceptual models of practice. The practice setting illustrated is Gloucestershire Partnership NHS Foundation Trust (GPT). Occupational therapists who work in this service have been collaborating with the UK Centre for Outcomes Research and Education (UK CORE). This collaboration provides support in the use of a particular conceptual model of practice as the main informing body of knowledge. After appraising the available theoretical perspectives, occupational therapists in GPT selected the Model of Human Occupation (Kielhofner 2008) to underpin their practice.
Whilst we use illustrations from this practice area, we hope that the supporting mechanisms illustrated will be relevant for the majority of therapists in most settings. We want to emphasise that therapists can still be successful in developing skills to use theory in practice even if some elements of the case study are not present within their context. Our illustrations here are about:
(i) The attributes that therapists can develop to be successful at using new or developing theories in practice
Little research has been undertaken to examine the attributes of occupational therapists who are successful in implementing new ideas. Chard (2006) touches on the matter in her research by suggesting that the attitudes of single-mindedness, tenacity and the ability to re-conceptualise new ways of working seem to be the most important characteristics for applying innovation. Arguably, therapists who have the ability to be clear about their role can more easily adapt to change as they will have confidence in the boundaries of their knowledge and expertise. Perhaps the first feature of the therapist who can drive forward the development of their practice is ability and desire to be proactive, taking personal responsibility for the learning and development required for theoretically oriented practice. Without this intrinsic motivation to adapt and advance their practice therapists might be perceived as disinterested or resistant (Rogers 2003) (see Vignette 2.1).
Vignette 2.1 Example of an occupational therapist who is able to articulate her position about the use of theory in practice thus illustrating her single-mindedness, tenacity and clarity about her way of working
‘I mean its about knowing what you can do as an occupational therapist, who you are as an occupational therapist, what your place is in the world of [field of work], and what you can offer people really, your role in the team. But then also what resources you have and to be able to use those effectively, in terms of both who you see and then what the next steps are with them… I am able to talk about what I do and why and to be a very strong advocate for what I do and if someone says well “why are you doing that?” I can now say “and here’s the evidence for it and this is what we’re doing and why”.’
(ii) Helpful elements of the environmental context
It appears to be the social environment in particular that might act as a support to therapists’ development of theoretically orientated practice. Where there is management support for investment in updating practice a multitude of learning opportunities can be created by knowledgeable professional leaders. Having confidence in occupational therapy leaders to support theoretical developments over time is pivotal to foster a facilitative environment (Chard 2000) (see Vignette 2.2).
Vignette 2.2 Example of an occupational therapist articulating her observation of the work context, particularly the occupational therapy leadership support for her use of theory in practice
‘I’d say it [the organisation] definitely does support it [practice development]. Obviously the professional side of occupational therapy very much supports it and that’s very, very strong. And that’s not just on MoHO but it could be Sensory Integration or whatever.’
1 Obtaining the available theory to support practice
Having the knowledge about what contemporary theories are available to support practice action is fundamental to theoretically oriented practice. Therapists have a responsibility to keep up to date with practice developments (College of Occupational Therapists 2005) and therefore have a responsibility to seek out innovation. It appears though that not all occupational therapists are independently investing time to find out about the theoretical or evidence-based developments that will support their own advancement in practice despite the fact that they are conscientious about their responsibilities (Metcalf et al 2001, Taylor 2007). This suggests that occupational therapists might find emerging knowledge more accessible if it is repackaged in a variety of ways. For example, 80% of the sample of occupational therapists surveyed in one study appealed for brief summaries of relevant practice information to be provided for them rather than them having to search the literature themselves (Bennett et al 2003).
Accessing theoretical concepts is also facilitated by clinicians having contemporary tools available in the workplace. These include acquiring theoretically based, practice-oriented textbooks; web-based information; and assessment manuals that summarize theoretical underpinnings. In addition clinical forums or special interest groups for discussion of relevant theories and their application with knowledgeable practice and academic leaders serve to underpin knowledge within practice.
We have observed that practitioners working collaboratively with academics have prompted the creation of resources which help to collectively explain the theory that the service is adopting. For example in GPT, an animated, power point picture was developed, locally known as ‘the pin-man’ which has been consistently used to illustrate case study material allowing therapists to engage with ‘thinking with theory’ in a practical way (Figure 2.3) (see Vignette 2.3).
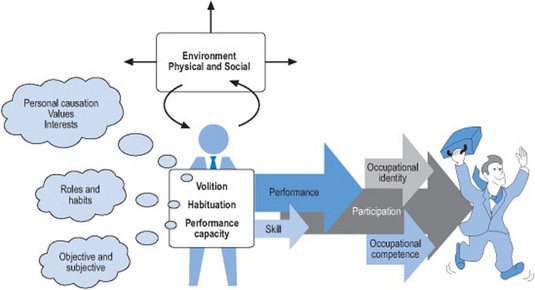
Figure 2.3 An example of a locally produced powerpoint tool used in practice to explain theoretical concepts. ‘The MOHO Pin-man’
Adapted from: The Model of Human Occupation (MOHO) Kielhofner (2002).
Vignette 2.3 Example of an occupational therapist articulating the way in which she has been obtaining the available theory to support her practice
‘It [theory] makes it a lot clearer and when I feel a bit confused or a bit too laid back and not as organised as I would like to be, I can just take a step back and look at the case and what I am doing with people and try to put it into the context of the Model of Human Occupation or I use the little ‘pin-man’ to see how that applies to somebody.’
2 Accessing appropriate continuing education
Occupational therapists commonly discuss the benefits of attending training courses for specific new techniques (Curtin and Jaramazovic 2001). Attending external training courses can be a costly process and it is clear that not all knowledge gained in attending courses is used in the practice setting (Chard 2004). A question can be posed about the prudence of investing service resources in education delivered this way if some therapists are not subsequently able to integrate knowledge into practice. It could be argued that learning as a local group is more effective in transferring new knowledge into practice. Common action points can be negotiated amongst participants and subsequent change managed in practice. Therapists can not only develop knowledge about the new practice development but can also develop skills by becoming competent in sharing that knowledge locally with their colleagues. Building and sharing practice-based knowledge within the practice area assists the organisation to have a community of practice scholars.
By adopting a strategic approach to the continuing education opportunities for occupational therapists, working in partnership with academic colleagues who are schooled in understanding the theory of occupational therapy, GPT have been able to offer locally delivered, problem-based learning courses (Forsyth et al 2005b). The skills of practitioners within the Trust have been drawn upon to provide a variety of workshops, didactic and experiential teaching. This has enabled therapists to engage with theory and its associated assessments. Specifically, the mechanism where therapists have a short time out of clinical work to concentrate on learning in a small group and then have a set time to implement before reporting back upon their new practice learning has been a successful system (see Vignette 2.4).
Vignette 2.4 Example of an occupational therapist articulating the way in which she has benefited from locally constructed and delivered continuing education
‘I’ve recently attended another session which was the Volitional Questionnaire training and I’ve also attended the follow up session in January. This morning I’ve also had a meeting with someone else about doing the “train the trainers” for the Model of Human Occupation Screening Tool. So I’d say that’s been quite a dramatic development actually for learning. As I say, I’ve always used the Model of Human Occupation right from being a student but since the Scholarship of Practice [practice development initiative] has been in place I’ve certainly developed an awful lot more skills and competency in using the assessments and I’m now feeling confident enough to train other people to do that too. It is quite a big change.’
3 Using professional supervision
Clinical supervision practised well can be helpful in enhancing occupational therapy practice (Sweeney et al 2001) (see Chapter 22). Indeed, practice based on the idea of ‘reflection in action’ or reflective practice has been argued to be an underpinning mechanism of professional problem solving (Schön 1991, Roberts 2002) (see Chapter 10) and developing professional craft knowledge (Smith 2001). It is perhaps no surprise then that occupational therapists are expected to participate in professional supervision in order to ensure the quality of practice (Department of Health 1998, College of Occupational Therapists 2005). The mechanism that we propose here is a particular, structured technique of reflecting on clinical scenarios using occupational therapy theory as part of a discussion with colleagues who have experience at using theory in practice. Examples from the literature (Wimpenny et al 2006) support the message from our case illustration which shows that the routine of thinking within a particular theoretical framework can be strengthened if therapists have the opportunity to reflect on their practice in this way (see Vignette 2.5).
Vignette 2.5 Example of an occupational therapist articulating the benefits with her understanding of occupational therapy theory that she has felt from engaging in professional supervision
‘you can only do so much yourself, you can sort of “download your head” but then it’s only your view on things and then I think it’s important to have the opportunity to talk through things. It often clarifies things a lot more than just thinking it through by yourself.’
4 Practise in practice
Occupational therapists and other healthcare practitioners with clinical responsibilities locate their priorities within direct client care (LeMay et al 1998, Metcalf et al 2001). Undertaking theoretically orientated initiatives can be perceived as an ‘added extra’ to core practice rather than as an essential component to best practice (Melton et al 2003). Research has demonstrated that some services enable therapists to access new therapeutic initiatives but that those services do not necessarily have any overt governance or support for the new learning to be followed through in practice (Chard 2004). By changing the culture to expect therapists to put new knowledge appropriately into action, services can demonstrate the use of theory and evidence to practice, enhance the practice skills of staff and use resources to best effect. Thus, this position supports therapists to use their time in ‘hands on’ practice as a priority whilst also expecting that the practice is developed (see Vignette 2.6).
Vignette 2.6 Example of an occupational therapist articulating her perception of the value and use of ‘practise in practice’ to support her learning
‘Mmmm, the thing that immediately comes to mind is how important it is to actually put it [new knowledge of theory and assessments for practice] into practice … I think that whilst you can go a long way in isolation in taking on broad theory, when you get to the tools and when you get to the application you really need to be in regular contact with clients with whom you’re applying that.’
5 Setting practice standards
The development and use of practice guidelines has been heralded as a strategy to improve standards of practice and enhance professional development (Cusick and McCluskey 2000). In order for this to be undertaken successfully practitioners ideally need to agree to the standards and form their practice actions accordingly. Time has been invested in GPT to document both pictorial and narrative care pathway standards that occupational therapists are expected to follow, where appropriate, in their practice. Taking a corporate approach to practice development, occupational therapists and support staff in GPT have been assisted to develop theoretically based assessment and intervention pathways to guide their practice. These practice standards do not in any way remove the therapist’s responsibility for clinical reasoning with the information that they generate through assessment procedures. Rather the information that they gather and have available acts as a supporting mechanism to generate intervention goals with service users. In addition the care pathways form a structure to facilitate the appropriate use of the assessment tools developed within a theoretical framework and foster the interpretation of assessment results to be articulated within the associated theoretical base (see Vignette 2.7).
Vignette 2.7 Example of an occupational therapist articulating her use of practise standards to support her practice and development
‘The care pathway has just become part of supervision and it’s really worked. We’ve sat down and especially when we’ve done caseload management and we say, “well what are we doing with people” in terms of articulating what you’re doing and why you are doing it. I know I’m doing it for the right reasons.’
Summary of measures to assist practitioners engage with theory in practice
We conclude with a final remark from an occupational therapist from GPT who has successfully engaged in the mechanisms for client-centred, theory-driven, occupational therapy practice development (see Vignette 2.8).
Vignette 2.8
‘I have to say that my clinical reasoning is probably very much informed by the Model of Human Occupation at the moment and if I think about before that it was probably not underpinned by anything terribly much if I’m honest. I think that I was one of those people who didn’t really think too much about it. I’d see the person, I’d ask about how they were going in terms of their occupational function like their Activities of Daily Living and their interests and their worth and stuff and how their going with that and I might have looked at things that were issues for them that they want to work on. I don’t know that I was as client focused as I am now in terms of trying to draw out what is really meaningful for them and where their motivation and their personal causation particularly lie. I think it was more that I might have just made more assumptions than I do now. I wouldn’t necessarily have looked at the depth that I do now.’
Summary
Throughout this chapter we have argued that there is the potential for positive outcomes and benefits for service users, therapists and services as occupational therapists grasp the challenge of integrating theory into their practice. The extent of this challenge is not underestimated in the busy schedule of occupational therapists in practice. We have illustrated though that with carefully considered practice development mechanisms and partnerships with academic colleagues, therapists can seek opportunities which enable their service users to benefit from occupational therapy practice which is underpinned by appropriate, occupation-focused theory.
Bennett S, Tooth L, McKenna K, et al. Perceptions of evidence-based practice: A survey of Australian occupational therapists. Australian Journal of Occupational Therapy. 2003;50:13-22.
Canadian Association of Occupational Therapists. Enabling Occupation: an Occupational Therapy Perspective. Ottawa: CAOT Publications ACE, 1997.
Chard G. An investigation into the use of the Assessment of Motor and Process Skills (AMPS) in clinical practice. British Journal of Occupational Therapy. 2000;63(10):481-488.
Chard G. Implementing the Assessment of Motor and Process Skills (AMPS) in the workplace: a comparison of the experiences of occupational therapists and new graduates. British Journal of Occupational Therapy. 2004;67(2):54-64.
Chard G. Adopting the Assessment of Motor and Process Skills into practice: therapists’ voices. British Journal of Occupational Therapy. 2006;69(2):50-57.
Christiansen C. Defining lives: Occupation as identity: An essay on competence, coherence and the creation of meaning. American Journal of Occupational Therapy. 1999;53(6):547-558.
College of Occupational Therapists. Code of Ethics and Professional Conduct. London: College of Occupational Therapists, 2005.
Closs SJ, Cheater FM. Evidence based nursing practice: a clarification of issues. Journal of Advanced Nursing. 1999;30:10-17.
Curtin M, Jaramazovic E. Occupational therapists’ view and perceptions of evidence-based practice. The British Journal of Occupational Therapy. 2001;64(5):214-222.
Cusick A. The research sensitive practitioner. In: Higgs J, Titchen A, editors. Professional Practice in Health, Education and the Creative Arts. Cornwall, UK: Blackwell Science; 2001:125-135.
Cusick A, McCluskey A. Becoming an evidence-based practitioner through professional development. Australian Occupational Therapy Journal. 2000;47:159-170.
Department of Health. A First Class Service. In Quality in the NHS. London: HMSO; 1998.
Duncan EAS, editor. Foundations for Practice in Occupational Therapy, 4th edn., London: Elsevier, 2006.
Fisher AG. Uniting practice and theory in an occupational framework. American Journal of Occupational Therapy. 1998;52(7):509-521.
Forsyth K, Summerfield Mann L, Kielhofner G. Scholarship of practice: making occupation-focused, theory driven and evidenced-based practice a reality. British Journal of Occupational Therapy. 2005;68(6):1-9.
Forsyth K, Melton J, Summerfield Mann L. Achieving evidence based practice; An innovative process of continuing education through practitioner-academic partnership. Occupational Therapy in Health Care. 2005;19(1–2):211-227.
Forsyth K, Duncan EAS, Summerfield Mann L. Scholarship of Practice in the United Kingdom: an occupational therapy service case study. Occupational Therapy in Health Care. 2005;19(1–2):17-29.
Health Professions Council. Standards of Proficiency, Occupational Therapists. London: HPC, 2003;11.
Higgs J, Titchen A, Neville V. Professional practice and knowledge. In: Higgs J, Titchen A, editors. Practice Knowledge and Expertise in the Health Professions. Oxford, UK: Butterworth Heinemann; 2001:3-9.
Kielhofner G. The Model of Human Occupation, Theory and Application, 3rd edn. Maryland: Lippincott, Williams and Wilkins. 2002.
Kielhofner G. Conceptual Foundations of Occupational Therapy, 3rd edn. Philadelphia: FA Davis Company. 2004.
Kielhofner G. Scholarship of Practice: creating discourse between theory, research and practice. Occupational Therapy in Health Care. 2005;19(1–2):7-16.
Kielhofner G. The Model of Human Occupation, Theory and Application, 4th edn. Maryland: Lippincott, Williams and Wilkins. 2008.
Law M, Baum C, Dunn W. Measuring Occupational Performance, Supporting Best Practice in Occupational Therapy. NJ: Slack, 2001.
Le May A, Mulhall A, Alexander C. Bridging the research–practice gap: exploring the research cultures of practitioners and managers. Journal of Advanced Nursing. 1998;28(2):428-437.
Lloyd-Smith W. Evidence-based practice and occupational therapy. British Journal of Occupational Therapy. 1997;60(11):474-478.
Mattingly C, Fleming M. Clinical reasoning: Forms of inquiry in a therapeutic practice. Philadelphia: F A Davis Press, 1994.
McCluskey A, Cusick A. Strategies for introducing evidence-based practice and changing clinician behaviours: a manager’s toolbox. Australian Journal of Occupational Therapy. 2002;49(2):63-70.
Melton J, Forsyth K, Summerfield Mann L. Delivering evidence-based practice: no money, no time, no skill? [editorial]. The British Journal of Occupational Therapy. 2003;66(10):439.
Metcalf C, Lewin RJP, Wisher S, et al. Barriers to implementing the evidence base in four NHS therapies. Physiotherapy. 2001;87(8):433-441.
Munoz JP, Lawlor M, Kielhofner G. Use of the MoHO: a survey of therapists in psychiatric practice. Occupational Therapy Journal of Research. 1993;13(2):117-139.
Nixon J, Creek J. Towards a theory of practice. British Journal of Occupational Therapy. 2006;69(2):77-80.
Oxman A, Davis D, Hayes R. No magic bullets: a systematic review of 102 trials of intervention to help health professions deliver services more effectively or efficiently. Canadian Medical Association Journal. 1995;153:1423-1443.
Parham D. Toward professionalism: the reflective therapist. American Journal of Occupational Therapy. 1987;41(9):555-561.
Parham LD. Applying theory to practice. In: American Occupational Therapy Association Occupational Therapy Education: Target 2000. Rockville, MD: AOTA; 1986.
Roberts AE. Advancing practice through continuing education: the case for reflection. British Journal of Occupational Therapy. 2002;65(5):237-241.
Rogers EM. Diffusion of Innovation, 5th edn. The Free Press New York. 2003.
Schön DA. The Reflective Practitioner: How Professionals Think in Action. England: Ashgate Publishing, 1991.
Smith DL. Facilitating the development of professional craft knowledge. In: Higgs J, Titchen A, editors. Practice Knowledge and Expertise in the Health Professions. Oxford, UK: Butterworth Heinemann; 2001:172-177.
Sweeney G, Webley P, Treacher A. Supervision in occupational therapy, Part 3: accommodating the supervisor and the supervisee. The British Journal of Occupational Therapy. 2001;64(9):426-431.
Taylor MC. Evidence-Based Practice for Occupational Therapists, 2nd edn. Oxford, UK: Blackwell Publishing. 2007.
Tickle-Degnen L. Using research evidence in planning treatment for the individual client. Canadian Journal of Occupational Therapy. 1998;65(3):152-159.
Townsend EA, Polatajko JH. Enabling Occupation II. Advancing an Occupational Therapy Vision for Health, Wellbeing and Justice through Occupation. Ottawa, Canada: Canadian Association of Occupational Therapists, 2007.
Wimpenny K, Forsyth K, Jones C, et al. Group reflective supervision: thinking with theory to develop practice. British Journal of Occupational Therapy. 2006;69(9):1-6.
Wood W. It is jump time for occupational therapy. American Journal of Occupational Therapy. 1998;52:403-411.