Chapter 6 Assessment Skills for Practice
Overview
Accurate assessment is an essential component of occupational therapy. But what exactly is assessment and at what stage of therapy should it be carried out? And how do practitioners choose which assessments to use? These questions, amongst others, are discussed in this chapter. The chapter commences by examining why occupational therapists carry out assessments and considers why other stakeholders (such as the service manager or regularity body) feel strongly that assessment should be a core part of practice.
The chapter tackles head on the debate about whether or not conceptual models of practice should be selected prior to, or following (or not at all) the initial assessment process. Other factors that influence the selection of an assessment in occupational therapy are then described and discussed.
Assessments can be undertaken in various formats and these are each described in turn with key points highlighted for when they are appropriate to use. Finally the chapter concludes with discussion about the appropriateness of using standardised and non-standardised assessments in practice. Case vignettes are used throughout the chapter to illuminate relevant issues.
What is assessment and why assess?
Assessment is a term used to describe both a process and a tool. The process of assessment aims to develop practitioners’ understanding of clients as occupational beings, recognising their strengths and difficulties. Assessment is the initial stage of the occupational therapy process and supports practitioners to appropriately carry out the second stage of the process: developing individualised intervention strategies tailored to client’s needs. Without appropriate assessment therapy may not meet the requirements of clients (Laver Fawcett 2002, Cohn et al 2003). Assessments are used at the evaluation stage of the occupational therapy process, identifying changes from the initial assessment and determining the effectiveness of the interventions.
Assessments and the assessment process help to ensure that occupational therapy practice not only meets the needs of clients but also reflects the unique contribution that occupational therapy practitioners can make to the health and wellbeing of clients. McMillan (2006) suggests that assessments that reflect occupational therapy values should be the initial tools used by occupational therapists. These include assessments drawn from two conceptual models of practice: The Model of Human Occupation (Kielhofner 2007) and the Canadian Model of Occupational Performance and Engagement (Townsend et al 2007). This is known as a top-down approach to assessment (Mathiowetz 1993, Trombly 1995, Kramer et al 2003), where practitioners first consider clients’ occupational roles, performance and skills. Without this understanding it will be much harder to understand what the consequences of specific problems will be on clients’ lives. For example, the impact of limited grip strength will be different for a needlework artist and a manual labourer. Thereafter a practitioner may decide to further investigate specific performance components. And it is at this stage that measurement of grip strength (in this example) may or may not be appropriate.
It is often the case that practitioners will not discover anything new by conducting an assessment; the same information may have been gathered through informal conversation and observation. However by gathering information systematically through a standardised assessment a practitioner can be confident that a comprehensive review has been completed and this can then be used for comparison at a later stage of therapy.
An occupational therapy assessment may have considerable consequences for clients. It could indicate whether they are safe to be discharged from hospital or to continue living at home, or it may identify goals of getting back to work or entering education. These implications have considerable impact on clients’ lives so it is each practitioner’s professional responsibility to ensure that all assessments are conducted sensitively, thoroughly and reliably.
In addition to the direct clinical requirements of carrying out assessments, practitioners may be required to assess by service managers in order to demonstrate the service’s clinical effectiveness. Professional or regulatory bodies also insist that practitioners use assessments in practice. For example, in the UK the Health Professions Council (2007) Standards of Proficiency for Occupational Therapists requires that registrants must be able to use assessment techniques, gather, analyse and evaluate information. Assessment, therefore, as both a process and a tool, is an essential component of the occupational therapy process.
Who benefits from assessment?
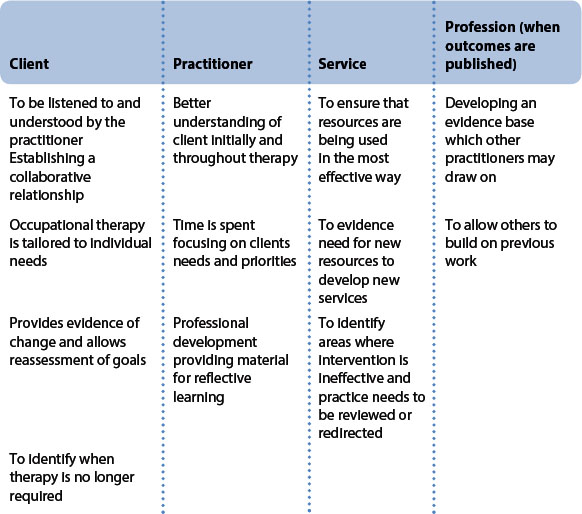
At times external influences and the drive for evidence-based practice led practitioners to consider the assessment strategies that they are using. But, whilst evaluating outcomes of intervention is important for occupational therapy services and helps demonstrate their effectiveness, it is vital not to lose sight of the value that this evaluation will have for individual clients and practitioners (Table 6.1).
Assessment may occur throughout therapy, but assessments should only be carried out when necessary. So why would an occupational therapist decide to conduct an assessment? There are various reasons. For example:
Shared (or needs) assessments
Occupational therapists may work within clinical settings where they contribute to assessments where there is a multi-professional shared responsibility to gather information. This is likely to be an important aspect of their role with other team members relying on the occupational therapist to assess a client’s independence in activities of daily living. However a therapist should consider if this shared assessment should be informed by a profession-specific assessment. Shared assessment tools tend to be global measures and are therefore useful for screening strengths and difficulties, however are insufficient to gain the detail an occupational therapist would require to plan an appropriate intervention. Supplementing the shared assessment with an occupational therapy tool will be vital as illustrated in Vignette 6.1.
Vignette 6.1
Mrs Jones attends the local day hospital, she has been suffering from depression since the death of her husband 6 months ago. She was first seen by a member of the local authority access team who conducted the locality’s single shared assessment used by both health and local authority staff. The assessment identified that Mrs Jones had needs in terms of diet and meal making and subsequently ‘Meals on Wheels’ were provided. Mrs Jones regularly expresses her frustration reporting that she does not need this service and asks for it to be discontinued.
Before contacting the home care team the occupational therapist assessed Mrs Jones, by carrying out an OCAIRS (Forsyth et al 2005), and identified that Mrs Jones missed the routine that meal preparation tasks gave her, prior to the meals on wheels she sometimes skipped meals as she couldn’t face going shopping. Before his death her husband had always driven her to the supermarket. An AMPS (Assessment of Motor and Process Skills assessment: an observational measure of activities of daily living which rates a clients effort, efficiency, safety, and independence in carrying out familiar tasks (Fisher 1999)) had demonstrated that Mrs Jones had necessary skills to prepare her meals. In discussion with the multi-professional team it was decided to arrange an alternative care package for Mrs Jones utilising a shopping service rather than Meals on Wheels. This service would collect a shopping list from Mrs Jones and then deliver her order.
How to select an assessment
There are numerous assessment tools that occupational therapists could use in practice, so how do practitioners know which to select? Practitioners use a wide variety of types of assessment the selection of which depends on the information they wish to gather. Frequently more than one type of assessment may be required in order to gain a comprehensive understanding of a situation, or client’s functioning, etc. Various factors should be considered when deciding which type of assessment to use with a client.
Conceptual models and selecting assessments
Which comes first: the assessment or the choice of conceptual model? This occupational therapy alternative to the better known chicken and egg scenario has taxed the profession for a number of years, and continues to do so today. In essence it is the argument of whether or not to use the ‘top-down’ assessment approach previously discussed.
The top-down approach suggests that an occupation-focused conceptual model of practice is selected as the first stage of the occupational therapy process (ensuring, amongst other issues, that the assessment is occupationally focused) and from that point an initial or screening assessment can take place. Following this assessment it may then be necessary to conduct further, more specific, assessments depending on the initial assessment’s findings. A good example of this way of practising and selecting assessments is outlined by Forsyth and Kielhofner (2006). These authors provide a flow chart that very clearly outlines the process of assessment selection based on the use of the Model of Human Occupation (MoHo) (Kielhofner 2008). Similarly, the Canadian Model of Occupational Performance and Engagement (CMOP-E) (Townsend et al 2007) is intrinsically linked to the Canadian Occupational Performance Measure (COPM) (Law et al 2005a). Law et al’s (2005b) argument for using the COPM as an initial assessment is that, ‘the tone of the therapeutic relationship, lets the client know you will be working as partners, and helps to focus your further assessment and intervention on the issues that the client feels are priorities’.
Both the MoHo and the CMOP-E have been developed within a generally Western societal context. Interestingly, the Western perspective of occupational therapy practice has been criticised for being excessively reductionistic, linear and scientific (Iwama 2006): But it is beyond the scope of the current chapter to consider whether the differences between Western and Eastern perspectives are truly significant in occupational therapy practice and if so what its effect on the assessment process would be.
It is important to highlight that using a top-down approach to practice does not restrict the practitioner to only using assessments that have been developed within the selected conceptual model; there may be times when an unstructured assessment is appropriate and an impromptu assessment opportunity may also occur when the practitioner has not had time to prepare a more structured assessment process. Furthermore a specific issue best understood from a specific frame of reference (for example mood and the cognitive-behavioural frame of reference) may also be appropriate after the initial conceptual model assessments are carried out. The use of a top-down approach to assessment, therefore, does not restrict practitioners to using assessments solely associated with that model.
An alternative approach to assessment is presented by Creek (2003), amongst others. In a document published by the College of Occupational Therapists, Creek presented ‘the complex content of occupational therapy practice’ (p. 7). Creek’s (2003) account makes no mention of employing a conceptual model of practice at any stage. Instead, Creek (2003) lists a broad range of factors that should be considered when assessing a client. These include:
The dozen factors listed above are a summary of the fuller list recommended by Creek (2003). Students and practitioners rightly question which of these two differing approaches is more effective? Does it matter if a top-down approach to assessment is used or not? To date, there does not appear to be any research that has rigorously studied this question. However, at a theoretical level, an argument can be made that a top-down approach is least likely to leave practitioners vulnerable to making errors through peoples’ known limitations; specifically in working memory capacity and personal biases in information gathering. In other words using a top-down approach may minimise the errors that practitioners make. Various issues leave practitioners vulnerable to making errors in assessing clients.
Given that the maximum number of pieces of information a person can hold in their working memory is 7 ± 2 (Miller 1956), it can be seen that listing an extensive range of factors that should be considered when assessing an individual (without placing them in the context of a well-developed structured assessment) is likely to lead to practitioners accidentally omitting some aspects of the assessment. Miller’s research, therefore, lends weight to the idea that practitioners should consider using a top-down approach and intentionally use a conceptual model of practice when initially conducting an assessment.
It has also been clearly evidenced in a range of studies in differing contexts that individuals are not reliable information gatherers and are biased in the manner in which information gathered from assessments is analysed (Paley et al 2007). Assuming that occupational therapists are no different (and there is no reason to assume they are) it can be seen that if practitioners do not impose an assessment structure that has been thoroughly tested they leave themselves open to bias, focusing in on areas of particular interest to themselves, potentially not giving due weight to certain issues raised by their clients, and emphasising some issues more than others when reporting the findings of their assessment. Each of these dangers is lessened when a practitioner uses a structured scoping or initial assessment founded in a conceptual model of practice. Practitioners are in effect ‘forced’ to consider the range of aspects covered in the assessment thus lessening the potential for bias or omission. For example both the Model of Human Occupation Screening Tool (Parkinson et al 2006) and the Canadian Occupational Performance Measure (Law et al 2005) contain specific questions that cover each of the aspects that are included within their respective conceptual models. This assessment structure ensures that individual practitioners gather information about the whole range of occupational functioning (as conceived by each respective model) and are less likely to succumb to personal biases and shortcuts, or accidentally omit certain aspect of the assessment.
As with so many areas of practice, research into the superiority of differing assessment approaches is needed before it can be said with confidence whether or not it is more beneficial to use a top-down assessment approach. However, the well-established literature surrounding heuristics and biases (Gilovich et al 2002) and existing knowledge about human’s limited working memory capacity (Miller 1956) lends strength to the theoretical arguments that support using a top-down assessment approach rather than a theoretical list of a multitude of factors such as those listed by Creek (2003) and others.
Work context
The area of practice an occupational therapist works in will also shape the assessment strategies they use. The priorities of the service and time available each influence the selection of appropriate assessments (see Vignette 6.2).
The rapid response team has been asked to visit Mr MacDonald by his GP. He was found, having fallen this morning, by a neighbour. The GP visited and has decided not to admit Mr MacDonald as he has only sustained minor bruising. However the GP would like occupational therapy and physiotherapy to assess him and refers Mr MacDonald to the Rapid Response Service.
The Rapid Response Service is a busy service which responds to referrals within 24 h. Their priority is to ensure peoples’ safety at home. They use a quick checklist to assess the home environment and individuals’ functional abilities. They visit Mr MacDonald in the morning spending about 30 min with him. From the assessment the occupational therapist identifies that a toilet frame, bed rail and high-back chair would improve his safety and the physiotherapist recommends a walking frame. The team is able to deliver and fit these items the same day.
The occupational therapist is confident that the situation has improved but recognises there are longer-term issues her service is not able to deal with. She recommends that Mr Macdonald be seen by the community rehabilitation service who can offer a longer-term input aiming to increase Mr Macdonald’s independence and safety. This team conducts a more thorough assessment through interview and observation over two home visits.
In a long-term setting there may be benefits in investing time in comprehensive assessments to ensure that an intervention programme is thorough, while there may not be the time available to conduct several assessments in acute settings where practitioners are required to make quick decisions based on rapid assessments. As in the case of Mr MacDonald this may result in referral onto another service where longer-term needs are suggested.
Decisions about assessments may also be influenced by the clinical specialism, some assessments are designed for particular areas of practice while others can be applied across most areas. Assessment manuals often provide guidance about when using it would be inappropriate; for example using a self-report assessment with a client who has limited insight. Occupational therapists also work in a variety of settings including hospitals, clinics and in clients’ homes. There may be some practical limitations that restrict the available range of assessments for use, for example if the equipment is not easily portable.
Occasionally an occupational therapist may be asked to assess an individual only to provide a report, for example in a compensation claim. However, usually assessments are a means to an end: to begin, review or end a programme of intervention. It is therefore important that practitioners consider what to do with the information that they gather.
Standardised assessments provide a structure for organising information into a logical format, and may provide information for interpreting the findings. Practitioners may also have gathered information from one or several assessments. Taking time to formulate all the information gathered through the assessment process into a conceptualisation of the individual is an important step in the assessment process and vital to enable appropriate planning of an intervention. The conceptualisation, drawn from the information gathered, will provide a portrait of a client’s occupational life and their needs. This information should be considered as a whole. In a collaborative therapeutic relationship the practitioner should then return to their client, share their understanding and confirm whether or not the client views the situation in a similar way (see Chapter 9 for further information as this issue is often much easier to suggest than to truly achieve). Sharing and confirming your understanding is an important step towards developing shared goals.
Report writing is a useful way of synthesising the findings of assessments, provides a document in the clinical records to demonstrate occupational therapy’s intervention and can be used to compare future assessment findings (see Chapter 6). Some assessments provide a quantitative summary of findings (for example the Assessment of Motor and Process Skills (AMPS) (Fisher 1999), but a narrative interpretation of findings is also useful to describe what this means for the client.
The type of information required
The type of information required will also influence the type of assessment used. Practitioners wishing to gain a broad understanding of a client may decide to use a general screening tool. Alternatively, where more detailed information is desired about client’s specific abilities, a structured observational measure may be more appropriate. Which assessment is ultimately selected depends on a variety of issues including client ability, timing and the form of assessment the practitioner wishes to undertake.
The ability of the client to participate in the assessment process
Clients who are non-verbal or have very low levels of concentration will be unable to participate in interviews; clients who are unable to read will not be able to complete self assessment forms without assistance, etc.
The timing of the assessment
An assessment at the start of therapy will initially be broad in nature: practitioners will frequently conduct a screening procedure or initial interview to ascertain whether or not a client requires occupational therapy, and if so broadly what the issues are. Towards the end of therapy assessments are likely to be much more focused to measure (whether narratively or numerically) what difference (if any) occupational therapy intervention has made.
Forms of assessment
Several different forms of assessment exist and have been mentioned within the chapter so far. Each method of assessment has its strengths and weaknesses.
Case note review
Frequently clients have already seen several health-care professionals before they meet an occupational therapist. Looking through multidisciplinary notes (where available) is an excellent way in which to gain some extra knowledge about a client before a practitioner sees them for the first time. Frequently case notes are interdisciplinary, and there may not be separate case notes held by each professional discipline. Either way there are often medical case notes that are held separately and these can contain additional valuable background information.
Some practitioners prefer not to look at case notes before they meet a client, and may suggest this to students. The rationale for this is that it is best to form your own initial impressions without having your assessment tainted by the clinical information and reasoning of others. However, there is no evidence to suggest that reading case notes before meeting a client significantly affects practitioners’ opinion of them, and if a practitioner was aware of the potential of forming an unhelpful attitude towards clients they can consciously try to avoid doing so (Creek 2002). There are several other reasons why reviewing a client’s notes before meeting them is very sensible:
Observation
Observation is an essential assessment skill for every practitioner. Observational assessments can be either structured or unstructured. An excellent example of an unstructured observational assessment process, and the richness of information that can be gained through this process, is recounted in the book ‘Dibs in search of self’ (Axline 1964). This section outlines various forms of observational assessments commonly used in practice.
Whilst all forms of observation could be categorised as structured or non-structured, more detailed categorisations also exist and are useful ways of considering the various forms of observation. Creek (2002) outlines three types of observation: general observation, observation of specific performances and observation of set task performance. Using the theoretical framework of the Model of Human Occupation, observation can also be used to understand both the performance and participation levels of clients’ occupational functioning.
An observation of performance skills could include assessing a client’s dressing ability post stroke. Whilst an observation of occupational participation could include assessing a client with multiple sclerosis working in their office to see if any adaptations are required. As well as unstructured observations of a client’s skill level, the practitioner may also wish to conduct a structured observation of a client’s communication and interaction or motor and process skills. Two well-known assessments developed from the Model of Human Occupation enable practitioners to do this and provide extremely detailed information about clients actual abilities (Fisher 1999, Forsyth et al 1998) (see Vignette 6.3).
Vignette 6.3
Mrs Harris is a 78-year-old widow, she lives alone and has no local family. After a recent home visit, the district nurse has referred Mrs Harris to the community rehabilitation team. The district nurse was concerned that Mrs Harris is not looking after herself and her home environment is deteriorating. The occupational therapist in the team is asked to visit to carry out a functional assessment.
During the visit it quickly becomes apparent that Mrs Harris is a poor historian and has limited insight into the difficulties she is experiencing, she does not know why the district nurse has asked for this assessment. When discussing her daily routine Mrs Harris reports going to the shops every morning, coming home to do some housework before cooking her own lunch. There is only out-of-date food in the fridge and no signs of recent cooking even though it is early afternoon. The occupational therapist decides that in order to get an objective assessment of Mrs Harris’ abilities she should carry out an AMPS assessment (Fisher 1999). This is suggested to Mrs Harris, who agrees.
The environmental location of both participation and performance skills are highly dependent on the environment in which they occur: how a client completes an activity can significantly differ between an occupational therapy department and a client’s home for example. This differentiation in skill level may be due to environmental differences (for example the kitchen in the occupational therapy department is at a more suitable height for the client than their own kitchen at home), but it can also be due to volitional differences.
Volition is most easily understood as the thoughts and feelings that a person has about what they have done, are doing, and will be doing in the future (Kielhofner 2008). Volitional deficits can have a significant effect on a clients’ functioning. Some clients may be able to accurately articulate these issues, others (such as people with severe mental illness or learning difficulties) will find this harder. In these cases it is useful to carry out an observational assessment.
Whilst it can therefore be very important to observe a client in the environment in which the activity will normally take place, it can also be useful, depending on the reason for the assessment, to observe a client in a variety of settings. This variation in environment can be used to good effect to demonstrate a client’s occupational potential. The Volitional Questionnaire (de les Haras et al 2007) (a structured assessment developed from the Model of Human Occupation) provides an excellent method of measuring volition through observation. This assessment can be used to good effect when a practitioner wishes to understand in greater depth why a client performs better in one environment than another, or to demonstrate the significance of this altered behaviour to other members of the clinical team.
Interviews
At their most basic level interviews are where a practitioner asks questions from a client in order to gain a better picture of their occupational performance. Like observation, interviews can generally be categorised as unstructured or structured.
Unstructured interviews
Unstructured interviews are those where the practitioner is not following a standardised interview assessment or formal information-gathering schedule.
Unstructured interviews may vary in their formality and presentation. At their most informal a practitioner may conduct an unstructured interview whilst participating in another task. An example of this is the ‘interview’ that occurs when a client and practitioner are jointly preparing a meal, doing the dishes, or driving somewhere in a car. Participating in such activities can make information sharing for some clients much easier and often a practitioner is able to elicit more information from a client whilst participating in such tasks than they would ever manage to gain if they had formally sat down in a room together with the specific aim of talking!
Of course it will often be appropriate and feasible to sit down together to interview a client. In these situations, even when the interview is unstructured, it is important to consider factors that will improve the interview process. These factors can be broadly categorised as expectations (of both practitioner and client) and environment (where the interview will take place), and are equally relevant and worthy of consideration when carrying out structured assessments.
Clients should be informed in advance of the reason for an interview, the time and location that it will take place, and the length of time a client should expect it to take (Creek 2002). Practitioners should also have gained the client’s agreement to be interviewed.
The physical and social environment where an interview is to take place should be closely considered. Interviews should be carried out in a peaceful setting, free from distractions and interruptions. Let other people know that an interview is taking place so that unnecessary interruptions are avoided. Consideration should be given to the seating arrangements of both parties: a 90 ° angle of seats that are comfortable and allow the feet of both client and participant to be flat on the floor is ideal (see Figure 6.1). Seats should be the same height so neither party is looking up or down on the other. It is important that clients are as relaxed as possible during interviews, so practitioners need to employ all their skills in the therapeutic use of self (see Chapter 9).
Structured interviews
Structured assessments have a relatively fixed format. They may form the basis of an initial assessment developed by a department or service which contains a list of questions that are asked of all clients who enter the service. Alternatively a practitioner may wish to gather particular information about occupational functioning and may use a structured assessment from a conceptual model of practice. One such example is the Occupational Circumstances Interview and Rating Scale (Forsyth et al 2005) which is developed from the Model of Human Occupation and now has specific formats and guiding questions for physical, general mental health and forensic settings (see Vignette 6.5). It is important to read the instructions for all structured assessments carefully: some require the use of precise words in questions, whilst others (including the majority of those associated with the Model of Human Occupation) provide examples of questions to use, but have specific guidelines for scoring the assessment. Familiarity with structured interview assessments is essential to enable the interview to flow smoothly. They can feel awkward to use at first, due to a lack of experience, but frequent use helps practitioners to feel more comfortable with them, which in turn helps the interview to flow more like a good conversation.
Vignette 6.5
Potter House is a new residential rehabilitation unit built in the community as an intermediary step between hospital and independent tenancy as part of the neuro-rehabilitation service. The multi-professional team has been asked to consider appropriate assessments to be used at monthly intervals during a client’s stay in the unit. It is planned that residents will be in the unit for between 3 and 12 months.
The practitioner considers that it will be important to gain a comprehensive picture of a client’s occupations in self care, work and leisure pursuits; she wants to be able to identify areas of need and priorities for the client. She is particularly aware that while in hospital clients tend to follow the routine of the busy ward and priorities tend to be set by the clinical team. This has led to clients finding it difficult on discharge as they feel overwhelmed with the responsibility of planning for the future. The occupational therapist decides to utilise the COPM (Canadian Occupational Performance Measure) (Law et al 2005b). She recognises that this assessment gathers information about a client’s self perception of their occupational performance and facilitates clients’ setting their own priorities for rehabilitation. She anticipates that through supporting clients in setting their own goals the transition to independence may be assisted.
Self-report questionnaires and checklists
Self-report questionnaires and checklists are commonly used in practice. They can be generic (such as measures of depression (e.g. Kroenke and Spitzer 2002) or anxiety (Beck and Steer 1990)) or occupation specific (such as measures of client’s self assessment of occupational interests (Kielhofner and Neville 1983) or time use (Smith et al 1986)). Whilst questionnaires and checklists do not provide a depth of information about a client, they can be very useful methods of gathering specific information.
When deciding whether or not to use a self-report method of assessment consideration should be given to the client’s eyesight quality, as well as reading, comprehension and concentration levels.
Assessments that combine information-gathering methods
Some assessment measures do not ‘fit’ nicely into either observation, interview or self-report categories, as they use a combination of methods to gather information. Two examples of such measures are the Model of Human Occupation Screening Tool (MOHOST) (Parkinson 2006) and the Canadian Occupational Performance Measure (Law et al 2005).
Vignette 6.4
James is a long-term client of the mental health services, he lives independently in the community supported by his keyworker (a community psychiatric nurse). The keyworker is concerned that he is isolated and has no social network. She has discussed her concerns with the occupational therapist (Beth); they plan a joint visit for James’ next appointment.
However on introducing James to Beth he immediately refuses to work with her, James explains that he has seen occupational therapists in the past and they always wanted him to join sports and art groups, he tells her he has no interest in these activities. Beth asks him about what he does enjoy, he tells her about his interest in computers. Beth explains that if he were to agree to work with her she would initially interview him using the OCAIRS (Occupational Circumstances Assessment Interview and Rating Scale) (Forsyth et al 2005). Beth explained that this would help her to fully understand what is important to him and what, if any, difficulties he was having. Beth told James she would then share her assessment with him and then they would be able to discuss what they could work on together. She guaranteed that as James was not interested in sports or art group she would not ask him to attend these. Beth recognized that by using this interview as an initial assessment her intervention could be tailored to James’ specific needs and they could work in collaboration to set meaningful goals.
The MOHOST was developed by a group of clinicians in the United Kingdom who worked with clients who were very low functioning. The practitioners wished to use a broad screening assessment to gather information about clients’ general occupational functioning difficulties, but found the interview structure of assessments such as the OCAIRS (Forsyth et al 2005) too intense and challenging for this client population. Over time and in collaboration with academic colleagues they developed the MOHOST. Whilst primarily an observational measure, information can also be gathered through case note review, interview and even third-party information gathering from relatives or other care staff to inform the scoring of the MOHOST.
The Canadian Occupational Performance Measure (Law et al 2005) combines an interview format with a self report rating of satisfaction and importance. This assessment is closely linked with the Canadian Occupational Performance Model and Engagement and addresses the three occupational performance areas covered by the model: self-care, productivity and leisure (see Vignette 6.5).
Standardised or non-standardised assessments?
Standardised assessments
Assessments can be standardised in two main ways: in terms of their process, materials and scoring instructions, and by normative standardisation (that is by providing statistics that outline what healthy ‘normal’ individuals could expect to score on the assessment) (de Clive Lowe 1996). De Clive Lowe (1996) outlined the importance of standardised assessments for occupational therapists. Standardised assessments can provide objective information about the health status or occupational functioning of a client. Such objectivity is important as it provides a very useful outcome measurement of a client’s progress and can form the basis of decision making that is more defensible than a practitioner’s judgement alone (Stewart 1999). Further, and as previously discussed, human memory is very fallible (Schacter 1999) and self reporting is recognised to be a very subjective process, with tenuous reliability and open to numerous biases. All of these reasons provide a sound rationale for using standardised assessments. Taking these factors into account Laver Fawcett (2002) rightly concluded that, ‘Inadequate, and even inaccurate, decisions may be made from non-standardised assessments and can have negative consequences both for the care of an individual and, where the effectiveness of occupational therapy intervention cannot be reliably demonstrated, for service provision as a whole’ (p. 135). Given this, why do non-standardised assessments continue to be used in practice?
Non-standardised assessments
Non-standardised assessments continue to form a part of practitioners’ assessment toolkit for a variety of reasons, some of which are more defensible than others! These include:
Non-standardised assessments lend themselves to those serendipitous moments in therapy when a client shares some information during the course of intervention that helps the practitioner to understand the client’s occupational performance in a new or more profound manner. Further, there is no standardised measure that can help a practitioner to understand what it means to a client to be affected by the illness or disability they themselves are experiencing. However, this does not mean that due care and attention should not be made to the process of gathering this sort of information. Kielhofner (2008) outlines three strategies that support the dependability of the information gathered by unstructured means: evaluating context, triangulation and validity checks.
Evaluating context
The circumstances in which a client shares information often influences the degree of confidence a practitioner has in the information received: Information shared by a child who is refusing to go to school may be interpreted quite differently if given in the presence of their school teacher than in a one-to-one interview scenario.
Triangulation
Information that is yielded in a non-structured assessment should be checked, using an alternative source, for accuracy: This can be achieved by observing the client do the activity they discussed or by asking another person who knows them well (e.g. nurse or spouse) for their perspective of the situation.
Validity checks
It is important that practitioners ensure that their understanding of information shared is accurate. This can be done by:
Thus, whilst Laver Fawcett’s (2002) argument that lack of use of standardised assessments, where they are already developed, could place practitioners and clients at risk is true; sound reasons to use non-standardised assessments also exist (Kielhofner 2008). The challenge for the discerning practitioner is to have the skill to know when to use each to their best effect.
Summary
This chapter has described what, why, where and when practitioners should consider undertaking assessments in practice. Basic information about the various types of assessments and the appropriate stages at which assessments could be carried out were presented. More contemporary issues, such as whether or not a top-down approach to conducting assessments is appropriate, were also discussed. It was suggested that, whilst objective evidence of the superiority of a top-down assessment approach over a more traditional assessment strategy is still lacking, there are well-grounded theoretical arguments that support the use of an assessment strategy that commences with the selection of an occupation-focused conceptual model of practice and initially uses assessments drawn from the model.
Axline VM. Dibs in Search of Self. Toronto, Canada: Ballantyne Books, 1964.
Beck AT, Steer RS. Beck Anxiety Inventory. Oxford, UK: The Psychological Incorporation, 1990.
Chia. The use of non standardised assessments in occupational therapy with children who have disabilities: a perspective. The British Journal of Occupational Therapy. 1996;59(8):363-364.
Cohn ES, Schell BAB, Neistadt ME. Overview of Evaluation. Crepeau EB, Cohn ES, Schell BAB, editors. Willard and Spackman’s Occupational Therapy, 10th ed., Philadelphia, PA: Lippincott Williams and Wilkins, 2003.
Creek J. Assessment. In: Creek J, editor. Occupational Therapy and Mental Health. Edinburgh, UK: Churchill Livingstone; 2002:93-118.
Creek J. Occupational Therapy Defined as a Complex Intervention. London: College of Occupational Therapists, 2003.
de Clive-Lowe S. Outcome measurement, cost effectiveness and clinical audit: the importance of standardised assessments to occupational therapists in meeting these new demands. British Journal of Occupational Therapy. 1996;59(8):357-362.
de las Heras C, Geist R, Kielhofner G, et al. The Volitional Questionnaire (VQ) (V.4.1) The Model of Human Occupation. Chicago, IL: Clearing House, 2007.
Fisher AG. Assessment of Motor and Process Skills, 3rd edn. Fort Collins: Three Star Press. 1999.
Forsyth K, Kielhofner G. The model of human occupation: integrating theory into practice and practice into theory. EAS Duncan, editor. Foundations for Practice in Occupational Therapy, 4th edn. Edinburgh: Churchill Livingstone. 2006:69-107.
Forsyth K, Salamy M, Simon S, et al. A users guide to the Assessment of Communication and Interaction Skills (ACIS). In Model of Human Occupation. Clearinghouse, Department of Occupational Therapy, College of Applied Health Sciences. Chicago: University of Illinois at Chicago; 1998.
Forsyth K, Deshpande S, Kielhofner G, et al. The Occupational Circumstances Assessment Interview and Rating Scale (OCAIRS) Version 4.0, The Model of Human Occupation. Chicago, IL: Clearing House, 2005.
Gilovich T, Griffin D, Kahneman D, editors. Heuristics and Biases: The Psychology of Intuitive Judgment. Cambridge, UK: Cambridge University Press, 2002.
Health Professions Council. Standards of Proficiency: Occupational Therapists. 2007.
Iwama M. The Kawa Model. London: Culturally Relevant Occupational Therapy. Churchill Livingstone/Elsevier, 2006.
Kielhofner G. A model of human occupation: theory and application, 3rd ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2008.
Kielhofner G, Neville A. The Modified Interest Checklist. 1983. Available at http://www.moho.uic.edu/images/Modified%20Interest%20Checklist.pdf Accessed on 2 November 2007
Kramer P, Hinojosa J, Royeen CB. Perspectives in Human Occupation: Participation in Life. Philadelphia, PA: Lippincott Williams & Wilkins, 2003.
Kroenke K, Spitzer RL. The PHQ-9: A new depression and diagnostic severity measure. Psychiatric Annals. 2002;32:509-521.
Laver Fawcett A. Assessment. Turner A, Foster M, Johnson SE, editors. Occupational Therapy and Physical Dysfunction, 5th edn. Edinburgh: Churchill Livingstone. 2002:107-144.
Law M, Baptiste S, Carswell A, et al. Canadian Occupational Performance Measure. Canadian Association of Occupational Therapists, 2005.
Law M, Baptiste S, Carswell A, et al. Canadian Occupational Performance Measure. 2005. Questions and Answers. http://www.caot.ca/copm/questions.html#1 Accessed on 4 November 2007
McMillan I. Assumptions underpinning a biomechanical frame of reference in occupational therapy. Duncan EAS, editor. Foundations for Practice in Occupational Therapy, 4th edn., Edinburgh, UK: Elsevier, 2006.
Mathiowetz V. Role of physical performance component evaluations in occupational therapy functional assessment. American Journal of Occupational Therapy. 1993;47(3):225-230.
Miller G. The magical number seven, plus or minus two. The Psychological Review. 1956;63:81-97.
Paley J, Cheyne H, Dalgleish L, et al. Nursing’s ways of knowing and dual process theories of cognition. Journal of Advanced Nursing. 2007;60(6):692-701.
Parkinson S, Forsyth K, Kielhofner G. The Model of Human Occupation Screening Tool (MOHOST) Version 4.0, The Model of Human Occupation. Chicago, IL: Clearing House, 2006.
Schacter DL. The seven sins of memory: Insights from psychology and cognitive neuroscience. American Psychology. 1999;54:182-203.
Smith N, Kielhofner G, Watts J. The relationship between volition, activity pattern and life satisfaction in the elderly. American Journal of Occupational Therapy. 1986;40:278-283.
Stewart S. The use of standardised and non-standardised assessments in a social service setting: implications for practice. The British Journal of Occupational Therapy. 1999;62(9):410-423.
Townsend E, Polatjko HJK. Enabling Occupation II: Advancing an Occupational Therapy Vision for Health, Well-being, & Justice through Occupation. Ottawa: Canadian Association of Occupational Therapists, 2007.
Trombly CA. Occupation: purposefulness and meaningfulness as therapeutic mechanisms. American Journal of Occupational Therapy. 1995;49(11):960-972.