31 The Hindlimb of the Ruminant
The angular appearance of the hindquarters of cattle is due in part to the robust formation of the pelvic girdle, much of which is outlined below the skin, and in part to the weak development of the muscles of the croup. The sacral tuber is palpable to the side of the lumbosacral space even though it fails to reach the height of the sacral crest. (Its occasional elevation above the crest prompts suspicion of sacroiliac dislocation.) This tuber is joined to the much more prominent coxal tuber (“hook bone”) by the iliac crest, which is only thinly—and incompletely—covered by the gluteus medius (Figures 31–1 and 31–2). The triangular ischial tuber (“pin bone”) is raised considerably above the pelvic floor and projects largely or wholly above the vulva. Its subcutaneous dorsal angle is joined by the sacrotuberous ligament; because the edge of this ligament is not covered by muscle, it is readily palpable (Figure 31–3/1′).
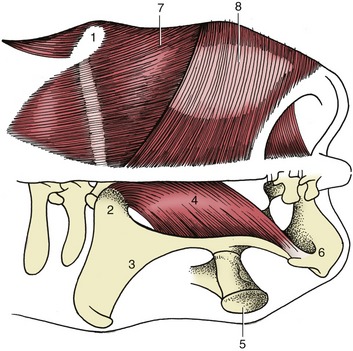
Figure 31–1 Dorsal view of the bovine croup; the muscles on the left side have been removed. 1, Coxal tuber; 2, sacral tuber; 3, ilium; 4, sacrosciatic ligament; 5, greater trochanter of femur; 6, ischial tuber; 7, gluteus medius; 8, biceps.
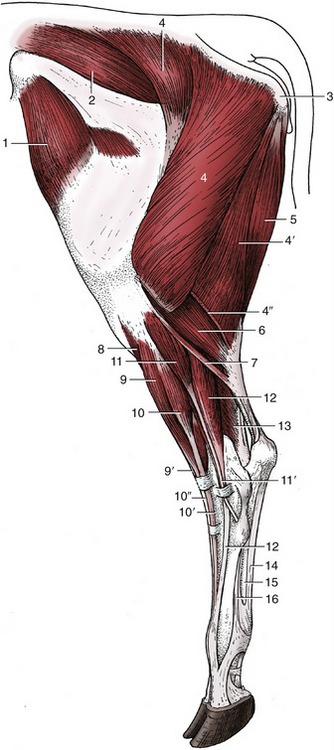
Figure 31–2 Muscles of the bovine left hindlimb; lateral view. 1, Tensor fasciae latae; 2, gluteus medius; 3, ischial tuber; 4, 4′, 4″, biceps, transected at 4″; 5, semitendinosus; 6, lateral head of gastrocnemius; 7, rudimentary soleus; 8, tibialis cranialis; 9, 9′, peroneus tertius; 10, 10′, 10″, long digital extensor; 11, 11′, peroneus longus; 12, lateral digital extensor; 13, lateral digital flexor; 14, tendon of superficial digital flexor; 15, combined tendon of deep digital flexors; 16, interosseous.

Figure 31–3 Right bovine thigh. 1, Ischial tuber; 1′, sacrotuberous part of sacrosciatic ligament; 2, greater trochanter of femur; 3, coxal tuber; 4, biceps; 5, lateral vastus; 6, patella; 7, flank fold.
The line connecting coxal and ischial tubers reveals the slope of the pelvis. An angle larger than usual is associated with a more upright pelvic inlet; a smaller angle (flattened rump) requires the femur to be carried more vertically, which is a conformation thought to predispose to concussive trauma of the hip joint. Neither inspection nor palpation directly reveals the position of this joint, which must be deduced by reference to the palpable greater trochanter; this is situated lateral and slightly caudal to the femoral head, below the intertuberal line (Figure 31–3/2). The disturbance of this relationship suggests fracture of the neck or dislocation of the head of the femur. Dislocation may occur in several directions and is thought to be facilitated by the relative weakness or occasional absence of the sole intraarticular ligament (ligamentum capitis). Most commonly the trochanter is displaced dorsocranially to project above the intertuberal line. This joint is nominally a ball-and-socket joint, but the extension of the femoral articular surface onto the semicylindrical neck makes it evident that flexion and extension must be the principal movements. However, the degree of outward rotation of the thigh that accompanies flexion ensures that the stifle is carried free of the abdomen. The cavity of the joint may be reached if a needle is inserted directly in front of the trochanter and is advanced medially and slightly cranially. The deep location and contractions of the muscle pierced en route make the procedure difficult to accomplish successfully.
The most striking features of the regional muscles are the relative weakness of the gluteal group and the absence of vertebral origins of the semitendinosus and semimembranosus. The gluteus superficialis is wholly incorporated within the biceps to form the combination sometimes known as gluteobiceps. The gluteus medius possesses a well-defined deep division (gluteus accessorius) with its own insertion tendon that enjoys the protection of a synovial bursa where it passes lateral to the greater trochanter. This bursa is occasionally inflamed. The biceps fills the caudolateral part of the thigh and has a wide insertion spread between the fascia lata, patella, lateral patellar ligament, and, via the crural fascia, the tibia and calcaneus. A large bicipital bursa intervenes between the lateral epicondyle of the femur and the part of the insertion proceeding to the patellar ligament. The bursa, which may communicate with the stifle joint cavity is sometimes the site of a painful inflammation, most often encountered in cattle required to rest on bare concrete. The insertions of the semitendinosus and semimembranosus and the actions of the group follow the usual pattern.
The adductor muscles of the medial thigh, the deep group about the hip joint, and the quadriceps femoris require no special notice. The tensor fasciae latae at the cranial margin of the thigh is a guide to the location of the subiliac lymph node.
THE STIFLE, LEG, AND HOCK
The stifle joint resembles that of the horse in possessing three patellar ligaments and an asymmetrical trochlea (Figure 31–4, B). The patella, patellar ligaments, and tibial tuberosity can be palpated on the cranial surface; two palpable “dimples” at the proximal end of the tuberosity separate and conveniently identify the three ligaments. The prominent femoral epicondyle, collateral ligament (and its attachment to the rudimentary fibula; Figure 31–4, A/9), and, more cranially, the common origin of the long digital extensor and peroneus tertius (Figure 31–4/5) are palpable on the lateral aspect. As in the horse, the intermediate patellar ligament, the patella, a medial fibrocartilage, and the medial patellar ligament combine to form a loop that passes over the expanded proximal end of the medial ridge (Figure 31–4, B/11) of the femoral trochlea. Although relatively little muscular effort keeps the loop in place (which prevents flexion of the stifle), the mechanism is by no means as efficient as that of the horse, in which the stifle can be fully locked. Lateral and medial luxations of the patella are occasionally reported. Dorsal dislocation, better described as fixation, is more common; indeed it is relatively prevalent among working bullocks of the Indian subcontinent. The condition is usually intermittent and, if not relieved spontaneously, may be treated by section of the medial patellar ligament.
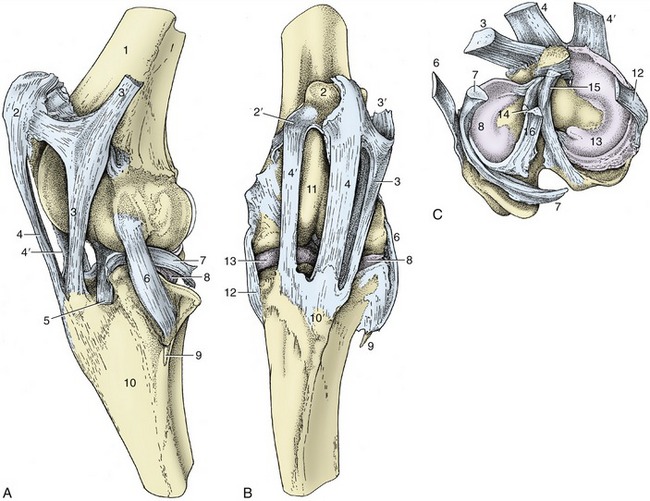
Figure 31–4 The left bovine stifle joint. A, Lateral view. B, Cranial view. C, The menisci and ligaments attaching on the proximal end of the left tibia. 1, Femur; 2, patella; 2′, fibrocartilage of patella; 3, lateral patellar ligament; 3′, attachment of biceps; 4, intermediate patellar ligament; 4′, medial patellar ligament; 5, combined tendon of long digital extensor and peroneus tertius; 6, lateral collateral ligament; 7, tendon of popliteus; 8, lateral meniscus; 9, fibula; 10, tibia; 10′, tibial tuberosity; 11, medial ridge of femoral trochlea; 12, medial collateral ligament; 13, medial meniscus; 14, cranial cruciate ligament; 15, caudal cruciate ligament; 16, meniscofemoral ligament.
The femoropatellar and medial femorotibial joint cavities always communicate, but the lateral femorotibial joint does not communicate with either of the other two. Two puncture sites are therefore in use. One, between the medial and intermediate patellar ligaments a short distance proximal to the tibia, gives access to the femoropatellar space; the other, in the extensor groove of the tibia, cranial to the common tendon of the long digital extensor and peroneus tertius, provides access to the lateral femorotibial compartment.
The tibia is the only weight-bearing bone of the leg (crus). Its medial surface, including the prominent medial malleolus, is subcutaneous; the remaining surfaces are covered by muscle (see Figure 31–6). The distal articular surface (cochlea) presents two sagittal grooves separated by a ridge; each groove is bounded externally by the corresponding malleolus. The fibula is much reduced. A proximal rudiment, generally drawn into a distal point, is fused with the lateral condyle of the tibia and receives the lateral collateral ligament of the stifle. The distal rudiment is a separate (and palpable) quadrilateral bone (lateral malleolus; Figure 31–5/2) that articulates securely with the tibia by means of an interlocking spike and groove. It also takes part in the formation of the hock joint.
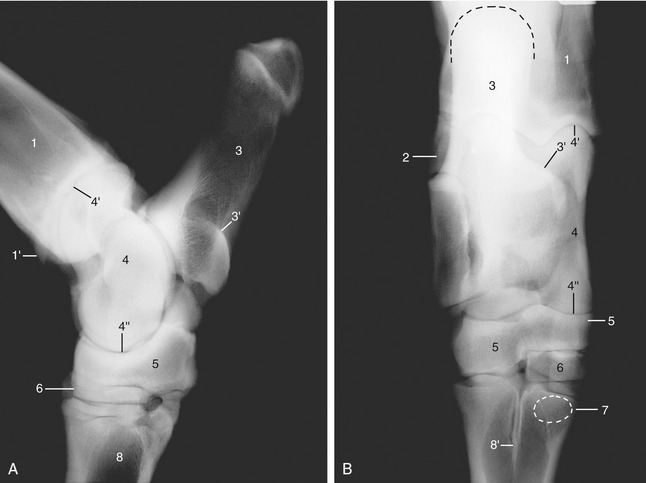
Figure 31–5 Lateral (A) and dorsoplantar (B) radiographs of the bovine hock. 1, Tibia; 1′, medial malleolus; 2, lateral malleolus (distal end of fibula); 3, calcaneus; 3′, sustentaculum tali; 4, talus; 4′, 4″, proximal and distal trochlea of talus; 5, fused central and fourth tarsal bones; 6, fused second and third tarsal bones, in B superimposed on small first tarsal bone (not labeled); 7, position of sesamoid bone in interosseous; 8, metatarsal bone; 8′, median septum.
The tarsal skeleton is formed by the following elements: calcaneus and talus in the proximal row; fused central and fourth bones in the intermediate row; and fused second and third bones and a small independent first bone in the distal row (see Figure 2–60). In marked contrast to that of the horse, the talus carries a trochlea at each end (as in artiodactyls generally; Figure 31–5/4′,4″). The proximal trochlea articulates with the tibial cochlea and malleolar bone, forming the tarsocrural joint; the distal trochlea articulates with the calcaneus behind and the fused central and fourth tarsal bones distally, forming the proximal intertarsal joint. Both joints allow flexion and extension, the principal movements at the hock; the proximal joint has the greater excursions. The calcaneus, more slender than the equine bone, has an additional articulation with the lateral malleolus. The tuber calcanei (point of hock) is slightly expanded. The combined central and fourth tarsals (Figure 31–5/5) span the breadth of the hock. The part provided by the fourth tarsal extends into the distal row and articulates with the metatarsal bone. It is related to the fused second and third bones on its medial side. The small first tarsal lies on the plantar aspect of the joint. The surfaces of the distal elements that concur in the formation of the distal intertarsal and tarsometatarsal joints are relatively flat and permit minimal movement. A small discoid sesamoid bone on the plantar surface of the metatarsal bone is embedded in the proximal part of the interosseous (Figure 31–5/7).
Few of the many ligaments are individually important. The joint is supported on each side by collateral ligaments whose long components may be palpated in their full extents from the respective malleolus to the metatarsus. The long plantar ligament (palpable on the plantaromedial aspect) follows the plantar border of the calcaneus and extends beyond this to the metatarsus; it unites the bones on the plantar aspect that would otherwise be pulled apart by the powerful muscles attaching on the point of the hock.
The tarsocrural and proximal intertarsal articulations share a common and relatively capacious cavity. When enlarged, the capsule pouches noticeably on the dorsomedial aspect of the hock, medial to the tibialis cranialis tendon and directly distal to the medial malleolus. It can be punctured more safely than in the horse because the pouch is not overlain by a vein. The other joints are rarely of clinical concern.
The conformation of the hindlimb, particularly the hock, is important in the selection of animals for breeding. The points of the hock should be vertically below the ischial tubers in both lateral and caudal views. If they are too close the animal is said to be “cow-hocked,” and its feet assume a wide stance. An adaptation to an overlarge udder is one cause of an exaggerated approximation of the points of the hocks. (The opposite bowlegged conformation brings the feet close together.) The normal angle of the hock joint (viewed from the side) is about 140°, which gives the metatarsus a slightly forward inclination. When the angle is noticeably smaller, the hock sinks and the animal is said to be “sickle-hocked”; when it exceeds the normal, the animal is said to be “straight-hocked,” a defect that may lead to “weak pasterns” because of the reduced angle at the fetlock joint. Abnormal postures of the hock cause faulty footing and risk damage to the tendons and synovial structures of the digits.
The muscles of the leg are divided into the usual craniolateral and caudal groups. Among the former, the tibialis cranialis and peroneus tertius broadly resemble those of the horse (Figure 31–2/8,9); the peroneus tertius, though largely tendinous, is yet significantly fleshier than its equine equivalent. The long digital extensor resembles the common extensor of the forelimb in possessing two bellies: one supplies the tendon proper to the medial digit, while the tendon of a second, smaller one splits to reach both digits. There is also a lateral extensor (Figure 31–2/12), proper to the lateral digit. All extensor tendons are of necessity held in place by (two) stout, palpable retention bands where they descend over the flexor surface of the hock; equally necessarily, synovial sheaths protect them here. The proximal retinaculum is easily palpated even in heavy, thick-skinned cows. The group is completed by a peroneus longus muscle (Figure 31–2/11) that arises near the lateral collateral ligament of the stifle and descends on the lateral side of the leg. It then crosses over the tendon of the lateral digital extensor to wind around to the plantar aspect of the hock where it inserts. Some inward rotation of the foot is produced by its contraction.
The gastrocnemius (Figure 31–2/6) arises by twin heads from the caudal surface of the femur and forms a muscular swelling at the upper end of the leg before narrowing abruptly to the strong tendon that inserts on the point of the hock.
The superficial digital flexor, though more muscular than that of the horse, is very tendinous and relatively inextensible (Figure 31–6/14). It arises between the heads of the gastrocnemius, winds around the medial surface of that muscle’s tendon, and spreads to cap the point of the hock. The edges of the cap attach here, but the bulk of the tendon continues down the plantar surface into the foot. The crural segment, acting in concert with the peroneus tertius, links the movements of the stifle and hock joints. (This needs to be kept in mind when attempting to correct the relatively common breech position of a fetus that presents the tail and flexed hocks.) An extensive subtendinous (calcanean) bursa protects the tendon both where it wraps around the gastrocnemius and again over the point of the hock. Occasionally a subcutaneous bursa (hygroma) develops over the tendon here.
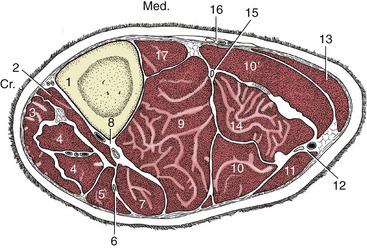
Figure 31–6 Transverse section of the left bovine leg. 1, Tibia; 2, tibialis cranialis; 3, peroneus tertius; 4, long digital extensor; 5, peroneus longus; 6, peroneal nerve; 7, lateral digital extensor; 8, cranial tibial vessels; 9, deep digital flexors; 10, 10′, lateral and medial heads of gastrocnemius; 11, biceps; 12, caudal cutaneous sural nerve and lateral saphenous vein; 13, semitendinosus; 14, superficial digital flexor; 15, tibial nerve; 16, saphenous vessels and nerve; 17, popliteus.
The gastrocnemius and superficial flexor are in a continuous (reflex) state of contraction in calves with “spastic paresis.” In these animals the hock and stifle are maximally extended, and the affected limb is used stiffly with only the toes of the hoofs touching the ground (Figure 31–7). Section of the tendons (or of the [tibial] nerve branches to the gastrocnemius) gives relief. Although there is no proof of inheritance, it is generally agreed that it is unwise to breed from affected animals even after surgical “cure.”

The deep digital flexor (Figure 31–6/9) has three heads. Two come together in the leg to form a thick tendon that passes over the plantar surface of the hock medial to the calcaneus and is protected by the tarsal synovial sheath. The tendon is bound down by the flexor retinaculum and other deep fasciae so that, when distended, the sheath bulges only at its ends, proximal and distal to the joint. The thin tendon of the third head tunnels through the dense medial tarsal fascia, within its own synovial investment, to join the major tendon in the metatarsus. The popliteus has no special features.
Most locomotor and cutaneous structures of the hindfoot are very similar to their forelimb counterparts and need not be described. However, the metatarsal bone is noticeably longer than the metacarpal and is quadrilateral in transverse section, which gives the hind cannon a deeper appearance in lateral view (see Figure 31–14). The higher incidence of disease in the digits of the hindlimb, especially the lateral one, has not been fully explained.
THE BLOOD VESSELS AND LYMPHATIC STRUCTURES OF THE HINDLIMB
The femoral artery continues the external iliac artery beyond the vascular lacuna. It passes between the medial muscles of the thigh to reach the flexor surface of the stifle, where it is renamed the popliteal artery. This soon divides into cranial and caudal tibial arteries (Figure 31–8/10,11). One branch of the femoral, the saphenous artery (Figure 31–8/7), runs on the surface of the gracilis and is often used for taking the pulse of cows; it is most easily found by sliding the hand from behind, between the udder and thigh. This vessel is responsible for the vascularization of the caudal part of the leg and follows the common calcanean tendon to the hock, where it gives rise to medial and lateral plantar arteries.
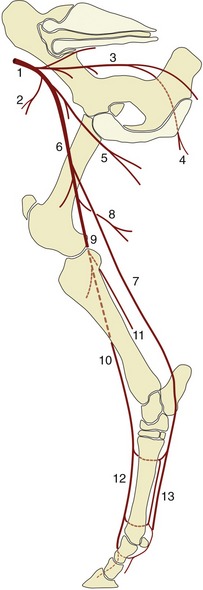
Figure 31–8 The principal arteries of the bovine right hindlimb, medial view. 1, External iliac a.; 2, deep circumflex iliac a.; 3, internal iliac a.; 4, caudal gluteal a.; 5, deep femoral a.; 6, femoral a.; 7, saphenous a.; 8, caudal femoral a.; 9, popliteal a.; 10, cranial tibial a.; 11, caudal tibial a.; 12, dorsal metatarsal aa.; 13, medial and lateral plantar and metatarsal (closer to the bone) aa.
The cranial tibial artery (Figure 31–6/8), which may be regarded as the continuation of the femoral trunk, runs embedded between the crural muscles to reach the flexor (dorsal) surface of the hock joint under cover of the long digital extensor tendon. The caudal tibial artery is of minor local significance.
Renamed the dorsal metatarsal artery (Figure 31–8/12), the main trunk now sends a perforating artery through the upper part of the metatarsal bone before continuing in the dorsal groove of this bone. A second perforating artery is released toward the fetlock. The perforating branches join the plantar arteries and are also connected by small deeper vessels. The plantar arteries resemble the corresponding forelimb vessels. One branch of the medial plantar artery crosses the plantar surface of the medial tendon of the superficial flexor proximal to the fetlock and is here liable to injury. This branch continues into the interdigital space, where it anastomoses with the main trunk. The anastomosis is substantial and winds around below the proximal interdigital ligament, where it is encountered in amputation of a digit. The axial surfaces of the digits are supplied by branches arising from the anastomosis; the abaxial surfaces are supplied by direct continuations of the plantar arteries.
The very number and frequent anastomoses of other side branches deprive them of individual significance.
The veins are divided between a deep system satellite to the arteries and a few superficial vessels that follow independent courses (Figure 31–9). The superficial vessels comprise the medial and lateral saphenous veins and their tributaries. The larger lateral saphenous vein (Figure 31–9/9) arises from two tributaries: one ascends with the extensor tendons and superficial peroneal nerve and crosses on the dorsolateral aspect of the hock, and the other ascends with the lateral plantar artery from a subcutaneous origin on the lateral digit and follows the flexor tendons under cover of the deep fascia to cross the joint plantarolaterally. The lateral saphenous vein (Figure 31–9/9) raises a ridge below the skin as it crosses to the caudal border of the leg and then follows the curvature of the gastrocnemius, eventually to open into the femoral vein. The medial saphenous vein (Figure 31–9/5) is also formed by two tributaries. The more important caudal one takes its origin from the abaxial aspect of the medial digit, ascends with the medial plantar artery, and passes the hock plantaromedially. The medial saphenous vein ascends together with the palpable saphenous artery on the medial aspect of the leg; above the stifle it dips between the gracilis and sartorius muscles to join the femoral vein.
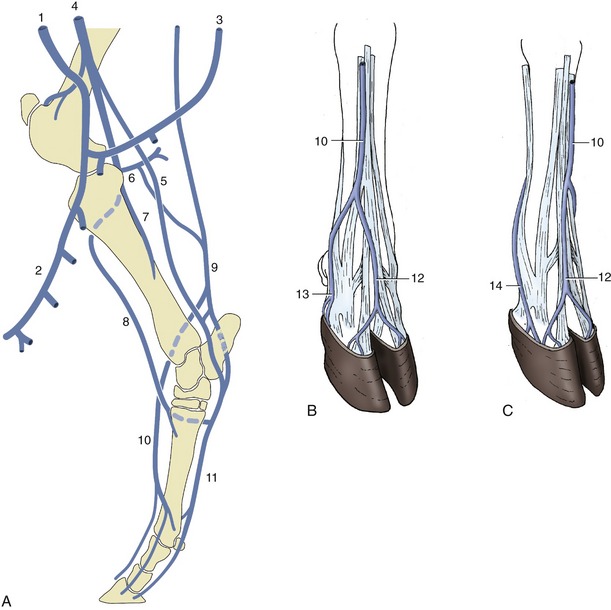
Figure 31–9 The major veins of the bovine hindlimb. A, Right limb, medial view. B, Right hindfoot, dorsolateral view. C, Left hindfoot, dorsomedial view. 1, External pudendal v.; 2, mammary v.; 3, ventral labial v.; 4, femoral v.; 5, medial saphenous v.; 6, caudal femoral v.; 7, caudal tibial v.; 8, cranial tibial v.; 9, lateral saphenous v.; 10, cranial tributary of lateral saphenous v.; 11, medial and lateral plantar vv.; 12, dorsal common digital v. III; 13, plantar v. of lateral digit; 14, plantar v. of medial digit.
The superficial veins (Figure 31–9, B-C) may be raised by application of a tourniquet below the hock for injection of local anesthetic so that the digits may be desensitized.
The lymph nodes include the popliteal node within the popliteal fossa and the very large subiliac node described with the abdominal wall (Figure 31–10/9,10). A small coxal node ventral to the coxal tuber and a group of gluteal nodes on the lateral surface of the sacrosciatic ligament are also commonly present (Figure 31–10/2,5). An ischial node (Figure 31–10/6) that lies on the ligament just dorsal to the lesser sciatic foramen can be inspected in the split carcass by incision of the ligament from within the pelvis. A tuberal node (Figure 31–10/7) lies medial to the ischial tuber within the ischiorectal fossa.

Figure 31–10 The lymph nodes of the bovine pelvis and hindlimb. 1, Lateral iliac lymph node; 2, coxal lymph node; 3, medial iliac and sacral lymph nodes; 4, deep inguinal lymph node; 5, gluteal lymph node; 6, ischial lymph node; 7, tuberal lymph node; 8, superficial inguinal (mammary) lymph node; 9, popliteal lymph node; 10, subiliac lymph node; 11, linea alba.
The popliteal node collects from the distal part of the limb, including most of the leg, and sends its efferent vessels along two routes: one follows the sciatic nerve to the ischial node, while the second accompanies the femoral vessels to the large, deep inguinal node (Figure 31–10/4) at the side of the pelvic inlet. The subiliac node drains the skin over the thigh and stifle in addition to the flank; its efferents also go chiefly to the deep inguinal node. The smaller nodes are only of local significance.
THE NERVES OF THE HINDLIMB
The lumbosacral plexus and its branches adhere to the common pattern. The obturator nerve (L4–6) crosses the ventral surface of the sacroiliac joint, runs medial to the shaft of the ilium, and passes through the obturator foramen to reach the adductor muscles of the thigh. It is vulnerable where it lies against bone, and the most common cause of injury is compression during parturition. Conduction is rarely completely interrupted in this injury; cows can still stand and walk on rough ground even when both nerves have been damaged. However, they cannot prevent their feet sliding sideways on smooth floors and, once down, are often unable to rise (Figure 31–12). It must be said that the role of obturator nerve injury in postparturient paralyses (the “downer cow” syndrome) has probably been exaggerated; insufficient attention has been directed toward traumatic or ischemic injury to the adductor muscles ventral to the pelvis as alternative or aggravating causes. These muscles may suffer from direct compression or through constriction of their blood supply in prolonged recumbency.

The femoral nerve (L4–6) (Figure 31–11, A) ramifies in the quadriceps after detaching the saphenous branch, which supplies skin over the medial aspect of the limb from midthigh to midmetatarsus. Damage to this nerve is occasionally encountered in newborn calves that were delivered by strong traction on the hindlimbs. An affected limb is unable to bear weight; the diagnosis is confirmed by the loss of sensation in the appropriate area.
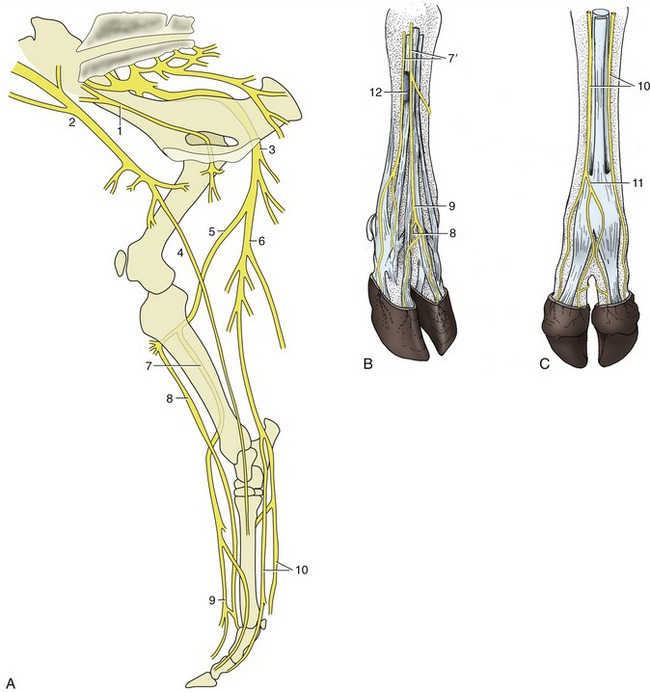
Figure 31–11 Nerves of the right bovine hindlimb. A, Medial view. B, Right hindfoot, dorsolateral view. C, Right hindfoot, plantar view. 1, Obturator n.; 2, femoral n.; 3, sciatic n.; 4, saphenous n.; 5, common peroneal n.; 6, tibial n.; 7, superficial peroneal n.; 7′, lateral and middle branches of superficial peroneal n.; 8, deep peroneal n.; 9, dorsal common digital n. III; 10, medial and lateral plantar nn.; 11, plantar common digital n. III; 12, cranial tributary of lateral saphenous vein.
Leaving the pelvis, the sciatic nerve (L6–S2) winds around the dorsal and caudal aspects of the hip joint before supplying the caudal muscles of the thigh. Its course between the biceps and semimembranosus, a few centimeters caudal to the femur, exposes it to risk of damage from careless intramuscular injection. Before reaching the gastrocnemius, it divides into tibial and common peroneal nerves, which share responsibility for the innervation of all structures below the stifle, except the medial skin territory of the saphenous nerve. The sciatic nerve may also be damaged at the birth of an over-large or ill-positioned calf. When the injury is severe, the affected limb hangs loose, and the stifle and hock joints are extended, the digital joints flexed, and the foot knuckled. Cutaneous sensation is lost over most of the extremity.
The tibial nerve (L6–S2) passes between the heads of the gastrocnemius and at once detaches branches to the caudal muscles of the leg (Figure 31–11, A), including those that are severed in the treatment of spastic paresis (see earlier). Severe lesions of this nerve are manifested by overflexion of the hock and overextension of the fetlock, resulting in a vertical pastern. As the digital extensors are not affected, the hoofs are correctly set down as the animal walks and they continue to bear their share of weight at rest. The anomalous attitude of the joints is exaggerated at the walk.
The common peroneal nerve (L6–S2) crosses the gastrocnemius under cover of the biceps to become palpable (and vulnerable) where it passes behind the lateral collateral ligament of the stifle joint. It then sinks between the peroneus longus and the lateral digital extensor before dividing into deep and superficial branches. The larger superficial peroneal nerve crosses deep to the peroneus longus to enter the foot. The deep peroneal nerve supplies the dorsal crural muscles, among which it is embedded, and also enters the foot. Paralysis of the common peroneal is betrayed by overextension of the hock and overflexion of the more distal joints (Figure 31–13).

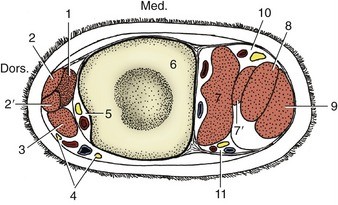
Figure 31–14 Transverse section of the bovine left cannon. 1, Extensor brevis; 2, 2′, long digital extensor; 3, lateral digital extensor; 4, branches of superficial peroneal nerve and cranial tributary of lateral saphenous vein; 5, deep peroneal nerve and dorsal metatarsal artery (continuation of cranial tibial); 6, metatarsal bone; 7, interosseous; 7′, band from interosseous to superficial digital flexor; 8, deep digital flexor; 9, superficial digital flexor; 10, 11, medial and lateral plantar nerves and vessels.
Unless passively set down correctly, the limb rests on the dorsal surface of the flexed digits. The animal eventually learns to compensate for this defect by flicking the foot forward before placing it on the ground.
The same considerations apply to the digital nerves of the hindfoot as to those of the forefoot. In very brief summary, the dorsal aspect of the foot is the province of the peroneal nerve, and the plantar aspect is the province of the tibial nerve; there is some overlapping to the sides (Figure 31–14).