Client Education for Postoperative Care
General Postanesthesia Instructions
General Postsurgical Instructions
Postoperative Care of Patients with Drains
Postoperative Care of Patients with a Bandage, Splint, or Cast
After completion of this chapter, the reader will be able to:
• Provide instructions to the owner describing the proper care of a patient after general anesthesia.
• Provide instructions to the client describing proper care of a patient with postoperative drains.
• Describe client education for postoperative care of a patient with a bandage, splint, or cast.
• Provide instructions to the owner describing proper care of a patient after the following surgical procedures:
Discharge Instructions
The role of the veterinary technician does not end when the patient is ready to go home; the owner (client) must be taught how to care for the animal properly. The responsibility for explaining the patient’s aftercare to the owner is typically assigned to the veterinary technician. This is a logical policy because the technician has been the postoperative caregiver and understands the patient’s needs and reactions. Every patient cannot be treated in the same manner. The approach to providing the prescribed treatments is dictated by the patient’s reaction and willingness to cooperate. The veterinary technician assigned to care for the patient has determined which restraint techniques work, what method to use to administer oral medication, and how effective the analgesic drugs have been for the patient. Areas to discuss with the client include timing of drug administration, wound care, and daily walks. For example, antibiotics and analgesics may be administered with a meal. The wound care should be delayed for about an hour after the analgesic is given. This technician knows the patient, can advocate for the patient, and can best educate the owner on how to care for the patient.
Postoperative education can begin before the actual procedure is started. Providing the client with a generalized handout on the procedure (Figure 10-1) can give him/her the opportunity to become familiar with the condition. By having information on the causes, signs, and follow-up care, the client will feel more actively involved. Many clients then come to the discharge with questions of their own.
FIGURE 10-1 Example of a client handout explaining dystocia in dogs and cats. (From Morgan R: Small animal practice: client handouts. St Louis, 2010, Saunders/Elsevier.)
In addition to the verbal discussion, written instructions explaining how to care for the postoperative patient should be sent home with the client. The hospital often has generic instructions that are prepared for all routine postoperative patients. Special instructions are added for certain nonroutine surgical procedures or medical conditions. However, each patient is an individual, and each client appreciates and deserves an explanation of the specific observations of the pet’s reactions and the specific care techniques used. The veterinary technician personally discharging the pet to its owner can provide this communication. It is best to explain the discharge instructions in a quiet area of the clinic. The client’s full attention needs to be directed to the technician’s instructions, so the animal should not be brought to the client until all the information has been provided. Alternatively, the veterinary technician can write out special instructions and add these to the generic instructions (Figure 10-2).
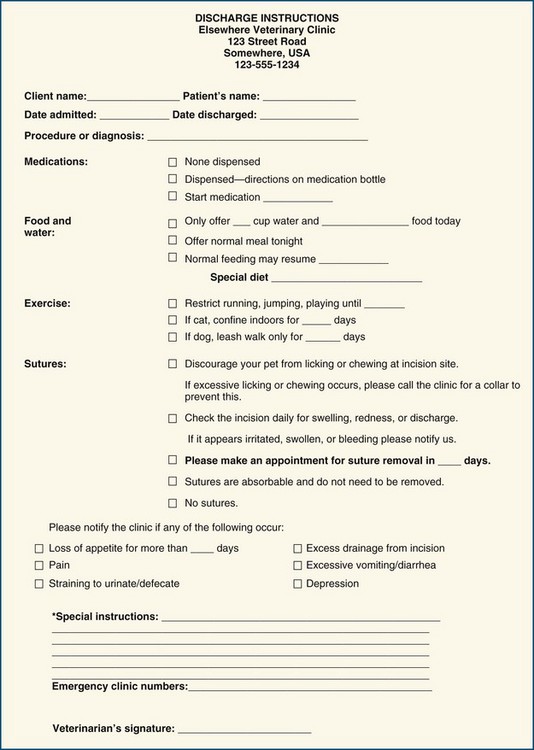
FIGURE 10-2 Example of general postoperative instructions for clients (owners) after a veterinary patient’s discharge.
Regardless of the type of procedure that was performed, the technician must be certain that all the client’s questions have been answered. In a busy hospital a technician may discharge ten animals who have undergone spay procedures in a single day. It is easy to talk at the client rather than with them. The technician should include the owner in the discussion by asking non-leading questions to make sure the information has been understood. “What time will you be feeding Fluffy tonight?” allows for more interaction than “You understand what time to feed Fluffy, right?” The client’s response to the first question allows the technician to gauge the client’s understanding of postoperative feeding.
General Postanesthesia Instructions
All patients that have been under sedation or general anesthesia should go home with instructions regarding their care for at least the first 24 hours. The instruction sheet should address (1) confinement, (2) feeding, (3) medications, (4) signs of possible adverse reactions, and (5) how to reach the hospital or 24-hour emergency clinic. If possible, a contact person, such as the technician, should also be listed. This helps personalize the treatment and makes the client feel more comfortable contacting the clinic with questions or concerns.
The client may need to confine the pet to a recovery crate or room. The pet may still be sedated and unable to walk normally. The pet may need to be accompanied or carried up and down stairs. Other pets in the household may disturb the patient, and it may be preferable to have the patient isolated from other animal housemates for a specified time. Over the long term it may be necessary to keep cats inside and to walk dogs only with a leash.
The owner needs instructions regarding when and how much to feed the animal after returning home. The time to resume the normal feeding schedule should also be addressed. The technician should take the time to discuss the possibility of nausea after anesthesia. The owner should be instructed to start with water first and then offer smaller meals more frequently to the patient. Special diets may be prescribed and may be introduced gradually. The technician should give detailed examples of how to mix the new food in with the old to prevent gastrointestinal (GI) upset. Also, the owner should be given some helpful suggestions on how to make the new food more palatable—heating, adding water, and so on. Specific instructions regarding the special diet should be written in the space provided on the postoperative form.
Medications may be sent home with the patient. Specific instructions regarding their administration are written on the label of the medication bottle. The instructions are repeated on the discharge instructions with more details, including whether the medication should be administered with food or on an empty stomach. In addition, the necessity of giving one medication at a separate time from other medications can be explained to the owner at discharge. Colored labels can be preprinted and placed on the medication bottles to help the owner remember specific requirements. Also, possible side effects of the medication should be addressed.
Animals under anesthesia or sedation may experience undesirable side effects. GI motility may be slowed down (ileus), which may cause inappetence, vomiting, constipation, or bloating. Lethargy, ataxia, and/or depression may be a symptom of prolonged recovery from anesthesia. These symptoms should be discussed with the client or listed on the instruction sheet. The informed owner will be an observant advocate for the patient.
Finally, instructions should be clearly provided regarding how to reach the hospital or a referral emergency center 24 hours a day.
General Postsurgical Instructions
In addition to the postoperative instructions already mentioned, the client is instructed on the need to observe the patient’s surgical site. The integrity of the surgical site should be monitored at least twice daily. The number of sutures should be counted. The client should observe for swelling, redness, and discharge. If sutures are missing or if excessive swelling, discharge, or redness is noted, the owner should be instructed to call the veterinary hospital. The owner is encouraged to call for advice regarding the management of the patient and any changes involving the surgical site. If possible, the owner should be shown pictures of a normally healing incision and then pictures of seromas, hematomas, and inflamed incisions. This knowledge will allow the owner to better understand the terms and conditions being described.
Specific instructions on confining the pet should be discussed with the owner. Each situation is unique, and residences vary, for example, in the presence and number of stairs to the outside. Other pets in the household may necessitate new routines regarding feeding, litter boxes, and walks outside. Children may need to be restricted from handling the pet until the patient is fully recovered. During the pet’s recuperative phase at home, the family’s routines and lifestyle will be disrupted, which can be stressful. The technicians should remind the client that the pet cannot articulate their pain or discomfort; it becomes vitally important for the client to track changes, improvements, or declines in behavior. These small clues can help the veterinary staff determine whether the animal is progressing as anticipated or there might be underlying complications.
If the animal is sent home with an Elizabethan collar (E-collar) or a BiteNot Collar (BiteNot Products, Inc., San Francisco), the technician needs to stress the importance of leaving the collar in place. Removing the collar for even a short period of time can lead to disaster; it only takes a matter of seconds for the animal to remove the skin sutures or completely open the incision. The owner should also be advised that the collar will not prevent the other animals in the household from licking the site and causing damage. An E-collar can also impede the animal’s ability to eat or drink. Even properly fitted collars can touch the floor around the food bowl before the animal can reach the food with its mouth or can hit the bowl itself and prevent eating. If this occurs, the animal should be provided with elevated bowls and/or bowls with a smaller diameter.
If possible, before leaving the hospital, appointments are scheduled for rechecks, suture removal, and drain removal. The hospital should also have a policy on calling the client to check on the animal’s progress. Many clients assume that abnormal behavior is common after surgery. Having the technician call 24 hours after discharge and then at a preset time (times) after that can put clients at ease; they will also be more likely to voice what they may feel are minor concerns.
Postoperative Care of Patients with Drains
Many surgical procedures involve the implanting of drains. These devices are temporarily placed to channel unwanted fluid or gas from a wound or body cavity. Often the patient is sent home with a passive drain. The owner is required to clean the discharge from the drain site and ensure that the drain is not disturbed by the patient. Clear and detailed instructions regarding drain care are important. Owners should also be informed that the discharge from an unbandaged drain can get on to furniture, carpet, and clothing. In multi-pet households the owner should also be reminded that the E-collar will not prevent the other animals from licking at the site or removing the drain.
The owner needs a demonstration of as well as written instructions regarding the care of the surgical site with the drain. Warm soaks to loosen and remove dried serous discharge will be necessary (Figure 10-3). The skin may need to be protected from the development of a moist dermatitis caused by contact with the discharge. A thin film of petroleum jelly can be spread over the area where the discharge tends to dry to the skin. The petrolatum serves as a protective barrier and facilitates skin cleaning.

FIGURE 10-3 Care of postoperative drains. Clean the area where the drain exits the wound with a warm compress of gauze. Apply warm soaks to the area to soften the discharge. Once the discharge is soft and loose, wipe the area clean.
Inadequate cleaning of discharge can prevent the drain from functioning and block further discharge. Fluid then becomes trapped under the wound or in the body cavity. This will slow the healing process or compromise a successful outcome in other ways. The veterinary technician must emphasize to the client the importance of proper and thorough cleaning of the drain site.
The client also needs instructions about effective restraint of the pet while the drain is being cleaned. The technician who has been caring for the patient knows the most effective means to restrain the patient safely and effectively. If possible, this technician should be present when the patient is discharged. These “customized” instructions can be written on the discharge information form in the area for special instructions.
If the pet pulls out the drain, the owner should report this to the clinic. The owner should search for any parts or pieces of the drain. These pieces can help the veterinary technician determine whether a portion of the drain is still in the patient. If a piece of the drain remains deep in the wound or body cavity, it will need to be surgically retrieved.
Postoperative Care of Patients with a Bandage, Splint, or Cast
When a bandage, splint, or cast has been applied to a limb, the pet should be kept quiet. Cats are confined indoors and restricted from jumping. Dogs may need to be confined in a recovery crate. Play with other dogs and humans in the household must be suspended. Dogs are walked only by leash.
Weekly in-hospital rechecks should be scheduled. The owner is instructed to examine the pet carefully each day and note the condition of the bandage and the extremity (Box 10-1). Toes should be checked for smell, warmth, and color. Foul odor can indicate tissue damage under the bandage; if swelling is occurring the toes will move apart, or if the bandage is too tight, the toes may become cyanotic or extremely pale. In the event that any abnormalities are noted, the owner should be instructed to contact the hospital for bandage removal and or replacement. The client should be made aware of the serious complications that can arise from a damaged bandage.
The owner is given instructions regarding how to protect the cast, bandage, or splint from wet grass, snow, puddles, and other sources of moisture. A plastic bag taped to the limb can effectively cover and protect the bandage (cast, splint) while the pet is outside. Empty fluid bags are made of heavy plastic that holds up well to repeated use. The bag should be removed as soon as the pet is back inside because the animal’s body heat can create condensation within the bag, leading to a moist bandage.
Postoperative Instructions for Common Procedures
While the mouth is healing after a tooth extraction, the pet will have a soft-food diet, such as canned, semi-moist pet food or dry food soaked in water until mushy. The socket will heal in 1 to 2 weeks. During the healing phase the pet may be gradually returned to his/her usual dry-food diet.
The client should watch for a number of specific signs. For the first day the owner may see the water in the bowl tinged red after the pet drinks. If this does not subside, the veterinarian should be notified. Long-term bleeding from the mouth indicates delayed healing, infection, or a coagulation problem. The pet rubbing or pawing at its face is an indication of pain, and the veterinarian should be notified. Crying out while eating or refusing to eat any hard food after several days to weeks have passed indicates an ongoing problem. The patient that refuses to eat will not heal promptly or properly.
Feeding Tube Placement
An enteral feeding tube may be placed for many reasons to aid in the patient’s nutritional support (see Chapter 8). This tube may stay in place for many weeks. Because of the critical support the feeding tube provides and the possible long-term need for it, the client caring for the patient at home requires detailed instructions on the tube’s use and care (Box 10-2; Figure 10-4).

Commercially prepared liquid diets (e.g., CliniCare, Jevity) are mandated when the tube has a very small diameter. Gastric and esophageal tubes are often large enough in diameter that pureed canned pet foods can be used in larger patients. It is important that large chunks of food be eliminated during preparation and not be forced down the tube.
Gastrointestinal Enterotomy or Anastomosis
Surgery of the GI tract is indicated to remove foreign body obstructions, collect tissue biopsy samples, remove growths, and resect diseased areas of intestine (e.g., cancer, necrosis, intussusception). Fluid therapy is continued until the animal is drinking and not vomiting. Feeding is resumed after the animal is able to consume water without vomiting. Prophylactic antibiotic therapy is typically discontinued within hours postoperatively.
Animals recovering from GI surgery need to be observed with great care. If the intestinal surgical site does not hold and intestinal contents leak into the abdominal cavity, a serious infection will ensue. This complication, peritonitis, can occur within hours or days after surgery. Peritonitis is an extremely painful condition that responds only slightly to analgesics. The patient will also have a fever, so postoperative monitoring of body temperature is important. If the patient spikes a fever, laboratory procedures (e.g., complete blood count) may be ordered. As peritonitis progresses, fluid accumulates in the abdominal cavity, and the patient appears bloated. An abdominocentesis procedure may be performed to obtain a culture sample, and abdominal ultrasound may be helpful in diagnosing peritonitis.
The owner should be instructed to monitor the patient closely at home immediately following and for several weeks postoperatively for signs of peritonitis (Box 10-3)
Two other postoperative concerns may not appear for weeks or months. First, the intestinal lumen may narrow because of scar formation. Second, a small, slow leak from the enterotomy site can lead to an abdominal abscess. Both complications may cause clinical signs associated with an obstruction. If an abdominal abscess has formed, vomiting, anorexia, lack of bowel movements, and abdominal pain may occur.
Perianal Surgery
Surgery around and involving the anus is indicated for removal of tumors, débridement and drainage of fistulas and anal sacs, and removal of anal sacs. In addition to the general postsurgical instructions, special instructions should be given to the client (Box 10-4).
Cystotomy
One major concern following bladder surgery is bladder distension. To prevent the bladder from becoming overly distended, the patient needs to be able to and allowed to empty his/her bladder frequently. See Box 10-5 for postoperative instructions for the owner of a pet with a procedure involving surgical incision of the bladder (cystotomy).
Feline Declaw (Onychectomy)
An onychectomy is a painful procedure regardless of the method used. Pain management preoperatively, perioperatively, and postoperatively will ensure that the patient recovers quickly and with few complications. Owners need to understand that jumping must be forbidden, because the force of even the smallest jump could damage the paws. This may mean confining the cat to a small bathroom or even a kennel during the healing processes. Even though the site of the phalange removal is covered or closed, it still needs to be treated like any other surgical incision. The paws should be checked daily for swelling, redness, discharge, and odor. Clay or clumping litter should be replaced as it can leave material in the surgical site (Box 10-6).
Aural Hematoma
Aural hematomas are typically messy, and the bandaging can be quite distressing to the owner. The technician needs to stress the importance of treating the underlying cause of the hematoma as well as keeping the pinna clean (Box 10-7).
Box 10-7 Client Postoperative Instructions Following an Aural Hematoma
1. The area where the drain exits the pinna needs to be cleaned of discharge. Warm water and a clean face towel or gauze work well. The drains usually stay in for 2 to 3 weeks (Figure 10-5).

2. Some animals may also need to have an infected ear canal treated with topical drops and ear cleansers. The pinna may be sore to the touch, so take extra care when instilling medication into the ear canal.
3. Some patients may have their head wrapped in a bandage. The same observations outlined earlier for extremity bandages apply to head bandages. Watch for soiling, slipping, moisture, foul odor, and skin irritation along the edges of the bandage.
Lateral Ear Canal Resection or Ablation
The ear canal is ablated, or surgically removed, when it is so chronically diseased that medical treatment is unable to establish a healthy canal. This surgery is a last resort. The theory is that if the diseased part is removed, the pain and discomfort will disappear. Part or all of the ear canal can be removed. If the entire ear canal is removed, the pet may be rendered deaf in that ear.
The pet is usually not released to the owner’s care until the need for daily bandage changes has passed and all drains have been removed. Postoperative infection may be caused by preexisting disease or contamination during surgery. Facial nerve paralysis is a well-recognized complication that usually resolves within 2 weeks. In some patients the vestibular system can be adversely affected when the entire ear canal is ablated. In these cases the pet exhibits a head tilt, nystagmus, and difficulty walking. Overall, many complications may occur, and intensive nursing care in the hospital setting is needed for a variable time after ear canal resection or ablation surgery.
The patient typically tries to scratch at the surgical site. An Elizabethan collar is an important piece of equipment used to help protect the integrity of the surgical site. Postoperative pain often drives the pet to self-trauma. Lateral ear canal resection or ear canal ablation tends to be very painful. Administration of analgesic medication and close observation of the surgical site are the owner’s primary directives.
Orthopedic Procedures
The client with a pet that underwent orthopedic surgery should receive postoperative instructions specific to that procedure. The animal may need additional support such as a bandage, cast, or non–weight-bearing sling. Exercise and even moderate activity may be severely restricted for weeks or months. Extensive pain management may also be indicated. See Box 10-8 for general home care instructions following orthopedic procedures.
Box 10-8 Client Postoperative Instructions Following an Orthopedic Procedure
1. The pet will need to be confined. Dogs are walked only by leash. Cats must stay indoors during the recuperative period. Excessive activity and exercise can slow the healing process by allowing weight bearing too early or causing excessive movement of the affected joint or fracture site.
2. Dogs especially may need help standing and walking. A bath towel can be placed under the abdomen or chest to act as a sling (Figure 10-6).

FIGURE 10-6 Towel sling. Place a towel under the dog’s abdomen. Pull up with one or both arms. The towel sling takes some of the weight off the dog’s hind end, allowing the animal to walk more easily.
3. If a bandage or cast has been applied, the owner receives specific instructions regarding its care (see Box 10-1).
4. If the patient has an external fixation device, the stainless steel pins and connecting pieces need particular attention, as follows:
• The site where the pin exits the skin will not heal while the pin is in place. Dried discharge is cleaned from the area once or twice daily as needed. An antimicrobial ointment can be applied to the skin around the exit site.
• The connecting pieces are covered with tape to prevent sharp edges from catching on furniture or the opposite limb.
Cesarean Section
After a cesarean section, the mother and newborns are kept apart until all have completely recovered from anesthesia. The neonates are at risk of being crushed if introduced to a mother that is still heavily sedated or ataxic. Even when fully recovered, the mother may reject the newborns. The staff must watch the mother carefully for any sign of aggression toward the neonates.
The newborns should be weighed at least once daily. Each one should be steadily gaining weight every day. If any newborn is not gaining weight, it should have extra time by itself on the mammary glands. If the newborn is not nursing, the owner should be shown how to supplement the neonate’s feeding with milk replacer (e.g., KMR, Esbilac).
The mother’s surgical incision is at risk of irritation and injury from her licking or the newborns’ suckling. The owner should inspect the incision daily. A bloody, mucous discharge is expected from the vulva for several days postsurgically. The color of the discharge may change from red to brown as the days pass. A foul odor to the discharge is not normal, and the hospital should be notified.
It is common for the new mother to have loose stools after giving birth. The mother’s appetite should be good. It is important that the new mother have plenty of high-calorie food because she must eat enough for herself and all her offspring. The new mother that is not eating will not heal promptly and cannot produce enough milk to feed the newborns.
The owner should be shown how to express milk from each mammary gland to check it for milk production and color and consistency. Colostrum (the first milk, generally rich in antibodies) is usually slightly yellow and sticky. After the newborns have nursed for approximately 24 hours, the milk becomes thinner and whiter. If the mammary glands stop releasing milk or become painful or red, or if the milk is thick or discolored (any color other than white), the owner must contact the veterinarian. The mother will need to be treated, and the newborns will need to be fed milk replacer. The veterinary technician often must instruct clients on how to bottle-feed or tube-feed the newborns.
Pet supply stores carry milk replacers for puppies and kittens. Bottles with nipples of appropriate size for the newborn should be purchased at the same time. Milk replacers come in canned as well as powdered forms. The process of tube or bottle feeding neonates can be very labor intensive. The technician should discuss the pros and cons of both options with the owner. Detailed description and hands-on demonstrations will be necessary to ensure that the young animals get the proper nutrition with minimal complications.
There are several veterinary textbooks dedicated to the pediatric patient; Small Animal Pediatrics: The First 12 Months of Life is one example.
Key Points
1. As the primary caregiver in the hospital setting, the veterinary technician is the best team member to discharge the patient to the owner’s care.
2. Instructions for all postanesthesia patients address confinement, feeding, medication, possible adverse reactions, and hospital contact information.
3. The client should receive written instructions as well as a demonstration of cleaning steps for passive drains.
4. To prevent distraction, all discharge instructions should be given in a quiet area where there will be minimal distractions. The pet and owner should not be reunited until after all home care has been thoroughly discussed.
5. It is important to ask non-leading questions to assess the client’s understanding of home care.
6. The client should be given a point of contact person, typically that of the technician, so that he/she feels more comfortable calling with questions.
7. The technician or other staff member should call the owner 24 hours after discharge to see how the patient is doing and then again at set intervals during the recovery.
8. Patients with a bandage, cast, or splint need to be strictly confined. The owner must understand the importance of this measure.
9. The owner needs to report any change in the appearance or position of the bandage, splint, or cast to the veterinary hospital.
10. Within a week, the patient that has undergone one to several tooth extractions should be pain free, and the tooth sockets should be almost healed.
11. If a patient is sent home with an E-collar, the owner must make sure that the animal is able to eat and drink normally.
12. Owners in multi-pet households should be reminded that the E-collar will not prevent the other animals from licking the patient’s incision and causing damage.
13. A feeding tube may be needed for several weeks, so the owner must care for the tube properly.
14. To assess the necessity of maintaining the feeding tube, the patient must have food available when it is ready to eat.
15. The patient exhibiting signs of unrelenting pain hours to days after gastrointestinal surgery most likely has peritonitis.
16. The heavier and older the cat, the longer it will take for the cat to recover from declaw surgery. Confining the cat to an indoor lifestyle is ideal after onychectomy because the animal no longer has the ability to defend itself.
17. Insufficient confinement of the patient after an orthopedic procedure is the most common reason for delayed healing.
18. The bladder of the patient recovering from a cystotomy should be kept small by allowing the patient to void every few hours.
19. After aural hematoma surgery, passive drains usually remain in place for several weeks. The pinna may heal with scar tissue and significant wrinkling.
20. The patient recovering from a cesarean section must heal and also raise a litter. The newborns’ feeding may have to be supplemented with milk replacer.
1. Which of the following statements is true regarding postoperative at-home nursing care?
a. The general principles are the same regardless of what specific surgery was performed, such that every patient can be treated exactly the same when he/she leaves the hospital.
b. Only the veterinarian who performed the procedure should explain postoperative nursing care to the owners at discharge.
c. The veterinary technician knows the patient, can advocate for the patient, and can educate the owner regarding what postoperative techniques work the best for that specific animal.
d. Well-written instructions make verbal discharge instructions unnecessary.
e. It is best to have the patient in the examination room when discharge instructions are given to the owner.
2. Which of the following may be clinical signs of prolonged recovery from anesthesia?
3. How often should the surgical site be observed once the patient is discharged to the owners?
e. The surgical site does not need to be observed after the patient leaves the hospital, because the patient would not be released if this were necessary.
4. When checking the surgical site, which of the following should be noted?
5. Serous discharge tends to accumulate where a surgical drain exits the skin. What can be done to prevent this accumulation from occluding the drainage site and thereby preserve the intended function of the drain?
a. Application of warm soaks around the exit site.
b. Application of a thin film of petroleum jelly.
6. True or False: When a dog has a bandage, splint, or cast on a limb, it should be walked only by leash.
7. True or False: A plastic bag may be continuously kept over a bandage, splint or cast to prevent it from getting dirty or damaged.
8. If a feeding tube becomes clogged, which of the following techniques usually resolves most occlusions?
9. True or False: If a large enough feeding tube is placed, chunks of kibble can be administered.
10. Which of the following may occur after an intestinal resection and anastomosis?
b. Narrowing of the intestinal lumen at the anastomosis site.
c. Slow leak from the anastomosis site leading to an abdominal abscess.
11. All of the following are indications of post–tooth extraction complications except:
12. How long should hematuria be expected following a cystotomy?
e. Any hematuria following a cystotomy is abnormal, and the veterinarian should be alerted immediately.
13. Why should the typical clay, clumping cat litter be avoided for the first few weeks after a declaw procedure?
a. Most cats refuse to use clumping litter after a declaw.
b. Most cats are so clean that they refuse to use clay litter after a declaw.
c. The clay granules tend to stick to the surgical site and can become embedded in the healing wound, leading to pain and infection.
14. What is another name for a declaw procedure?
15. Which of the following statements regarding ear canal ablations is true?
a. Postoperative infection may occur.
b. Facial nerve paralysis is a common complication that usually resolves within 2 weeks.
c. Head tilt, nystagmus, and difficulty walking are signs of a compromised vestibular system.
16. Which of the following statements regarding postoperative care of cesarean section patients is true?
Bassert JM, McCurnin DM, eds. McCurinin’s clinical textbook for veterinary technicians, ed 7, St Louis: Elsevier, 2010.
Peterson, ME, Kutzler, M. Small animal pediatrics: the first 12 months of life. St Louis: Saunders; 2011.
Piermattei, DL, Flo, GL, DeCam, CE. Brinker: Piermattei and Flo’s handbook of small animal orthopedics and fracture repair, ed 4. St Louis: Elsevier; 2006.
Sirois, M. Principles and practice of veterinary technology, ed 3. St Louis: Mosby; 2011.
Wortinger, A. Nutrition for the veterinary technician and nurse. Ames, Iowa: Wiley-Blackwell; 2007.