5 Orofacial Complex: Form and Function
This chapter discusses primarily the physiological form of the teeth and periodontium, with consideration of the coverage of form and function in Chapter 4 and the coverage of orofacial structures in other chapters on muscles and joints.
Form and Function
The phrase form and function reflects a concept of interrelation of the shape or attributes of something with its function. In dentistry the phrase may indicate the entire masticatory system, acting as a biomechanical engine for the reduction of food. If so, then arguably it may be possible to try to make a case that each of the components of the masticatory system has some kind of physiological relationship to its individual functions and to that of the whole system, including its maintenance. These relationships have a spectrum of possible associations: speech and jaw motion1; arch form and mathematical function2; integration of form, function, and esthetics in mandibular anterior ceramic veneers3; morphological and functional analysis of the orofacial complex4; and the condylar disk as the controlling factor in the form of the condylar head.5 The search for the meaning of form and function continues.
Form Follows Function
For some clinicians the general principle that becomes operant is form follows function, which means, for example, that in restorative dentistry, the dependent relationship between the original biomechanical behavior of stress concentrations in incisor teeth6 and the nature of the materials used to restore these teeth is addressed. Thus the term form not only means shape but also biomechanical attributes that contribute to the maintenance of function. Other examples include the dependent relationship between esthetics and optimum occlusion,7 physical forces and the periodontal ligament,8 and arch form and beta function,2 as well as the controversial interrelationship between the morphology and function of the discomuscular apparatus of the human temporomandibular joint. Although the function of implant-supported restorations seems to be generally achieved, the esthetics and biocompatibility of the materials used (i.e., design and fabrication of restorative components with dimensions that closely resemble natural tooth anatomy and esthetics) remain a challenge.9,10
Articulation of Teeth
Anyone who has carved a set of Ivorine teeth, even to the dimensions set forth in Table 1-1, can attest to the difficulty of aligning the carved teeth into what might be thought to be only one proper articulation of the teeth on an articulator. Form and function are not a template by which it is possible to draw a straight-line correlation between the shape of a tooth and all of its functions. A restored crown of a maxillary central incisor should meet standards of function and esthetics (see Figure 1-1).
Physiological Form of the Teeth and Periodontium
The form of the teeth is consistent with the function they are to perform and with their position and arrangement in the structures involved in oral motor behavior, especially mastication. To attempt to relate form and function in all the structures involved in such functions is beyond the scope of this book, and the reader is referred to several of the publications listed in the references and bibliography of this chapter.
Fundamental Curvatures
It can be assumed that the form of the teeth and their arrangement are related to incising or crushing food without causing damage to the supporting structures; for them to be otherwise might be inconsistent with the survival of the species. Some of the form must also relate to that of the jaws and face and to occlusal forces that dictate that the teeth be at various angles and positions in the dental arches. Beyond assumptions or teleological approaches to the morphology of the teeth, the relationships of tooth form to the form of the supporting structures, including the gingiva, must be considered in terms of clinical significance. Thus food impaction may occur as a result of gingival enlargement and of the driving of food between the teeth because of improper marginal ridges and/or contact areas, irrespective of teleological considerations of tooth morphology.
Although a great deal has been said about the relationship of the health of the gingiva to the contours of the teeth, as indicated in the references included at the end of this chapter, such appraisals are generally descriptive, involve restorations, and are retrospective observations. To conclude that the gingival tissues around a tooth (natural or restored) need neither stimulation nor protection suggests that the true significance of buccolingual crown contours has not been evaluated. In no instance has the influence of axial contours, which begin with the height of the contour of buccal and lingual surfaces, been tested in relation to such functions as chewing efficiency or occlusal stability. And even though the significance of buccolingual crown contours to gingival health relative to gingival stimulation, self-cleansing mechanisms, and gingival protection has been seriously questioned, the significance of other contours has also been questioned. Dental plaque accumulates on teeth in the absence of adequate oral hygiene, and gingivitis occurs in spite of “self-cleansing” mechanisms.11 The influence of a primitive diet does not appear to prevent gingivitis. However, plaque formation and gingivitis may be related more to bacterial attachment mechanisms, bacterial toxins, and food substrates than to physical form. It should not be concluded from such observations that curvatures have nothing to do with the function and health of the masticatory system. The effect of overcontouring or undercontouring of surfaces of the teeth may be related more to occlusal mechanisms than to self-cleansing mechanisms and be of more significance to food self-cleansing efficiency and/or musculature in one patient than in another. The role of protective reflexes in relation to the contours of the teeth is not known. Even though the significance of tooth forms has yet to be clarified, ideas about form and function that have been held should be understood, and liberties with form avoided. The following are considered:
These headings include form, which has been considered to have a direct or primary bearing on the protection of the periodontium. Many other details of tooth form may have an indirect bearing on the stability of the teeth through their contribution to the maintenance of efficiency during function. Some of these details are cusp forms, the proportions of various measurements of the crowns and roots, root form, and anchorage and angles at which teeth are set in the jaws. It has been suggested that when well-formed teeth are in normal alignment with normal gingival contour (Figures 5-1 and 5-2), the efficient use of the toothbrush during home care of the teeth is enhanced.11
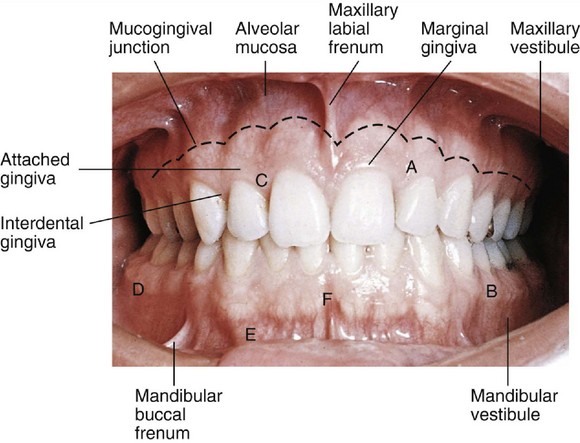
Figure 5-1 Clinical appearance of gingiva. A, Attached gingiva above and interdental papilla below; B, mucogingival line separating attached gingival from mucosa; C, free gingival margin; D, posterior vestibular fornix; E, anterior vestibular fornix or mucobuccal fold; F, frenum area.
(From Bird DL, Robinson DS: Torres and Ehrlich modern dental assisting, ed 9, St Louis, 2009, Saunders.)
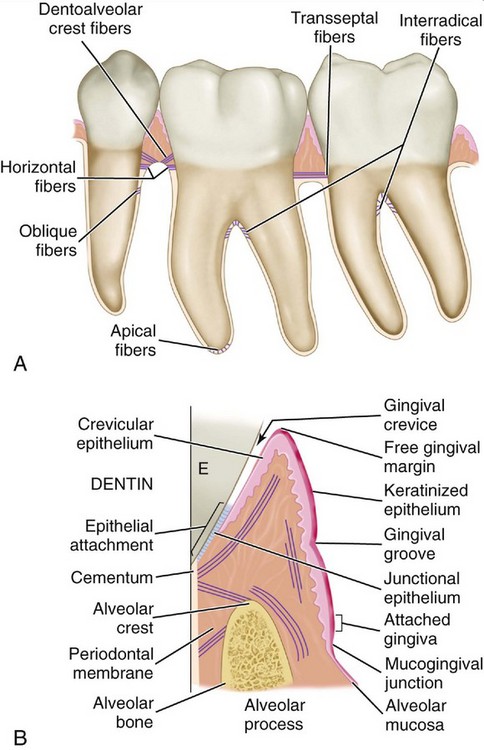
Figure 5-2 A, Principal fibers of the supporting structures. B, Schematic representation of periodontal structure at the junction of the enamel, cementum, and dentin showing attachment of gingival tissue to the tooth via the junctional epithelium. E, Enamel.
(From Ramfjord SR, Ash MM: Periodontology and periodontics, Philadelphia, 1979, Saunders.)
Proximal Contact Areas
Soon after the alignment of all of the teeth in their respective positions in the jaws takes place, a positive contact relation of one tooth with another in each arch should be established mesially and distally (Figure 5-3). Except for the last molars (third molars, if present), each tooth has two contacting members adjoining it. The last molar is in contact only with the tooth mesial to it. Although the areas of contact are still very circumscribed, especially on anterior teeth, these are areas and not mere points of contact (Figure 5-4). Actually, the term contact point, which is often used to designate the contact of teeth in the same arch, is a misnomer. When the individual is quite young and the teeth are newly erupted, some of the teeth come close to having point contacts only when the contacting surfaces are nearly perfect curvatures. Examples of the few contacts made by such rounded surfaces are contacts located distally on canines and mesially on first premolars, maxillary and mandibular.
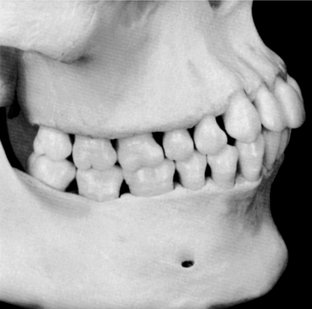
Figure 5-3 Proximal “contacts” vary in size in relation to type of teeth and wear of these areas. Note flat contacts in molar region compared with absence of flattening in relation to space between canine and premolar. The form of the interproximal spaces is altered by wear of contact areas, extrusion of teeth, or tipping of teeth.

The proper contact relation between neighboring teeth in each arch is important for the following reasons: it serves to keep food from packing between the teeth, and it helps stabilize the dental arches by the combined anchorage of all the teeth in either arch in positive contact with each other (Figures 5-5 and 5-6; see also Figure 5-3). Except for the third molars, each tooth in the arch is supported in part by its contact with two neighboring teeth, one mesial and one distal. The third molars (and the second molars if no third molar is present) are prevented from drifting distally where there is no contacting tooth by the angulation of their occlusal surfaces with their roots and by the angle of the direction of the occlusal forces in their favor. This is explained more fully in later chapters.
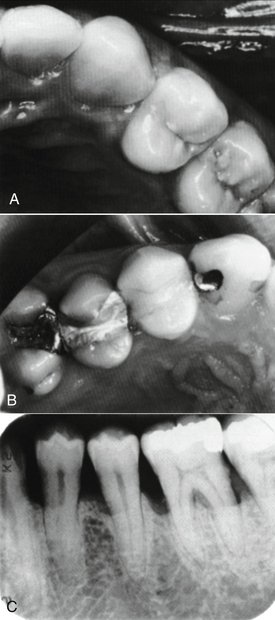
Figure 5-5 Contact areas. A, “Contacts” without evidence of dysfunction. B, “Restored” contact areas associated with dysfunction from food impaction. C, Loss of contacts associated with bone loss due to periodontal disease.
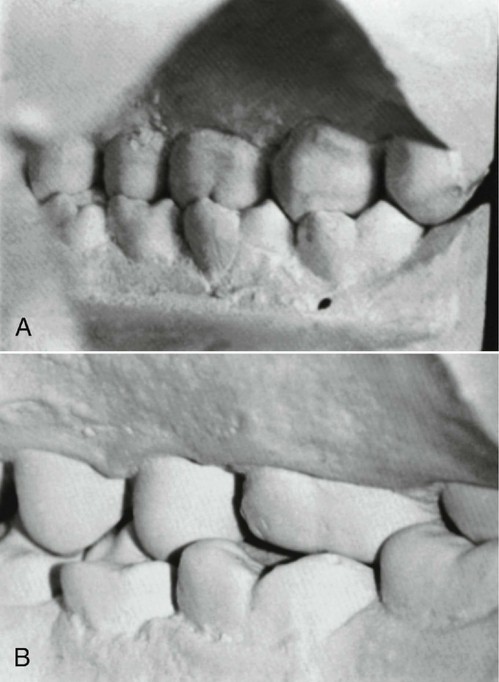
Figure 5-6 Relationship of cusps to embrasures in some dentitions. A, Casts in the intercuspal position and teeth in “normal” occlusion. B, Other casts in intercuspal position with alignment of the teeth preventing normal contact relations between cusps and embrasure areas.
If, for any reason, food is forced between the teeth past the contact areas, the result may be pathological. The gingival tissue, which normally fills the interdental spaces, may become inflamed (gingivitis) and ultimately involve deeper periodontal structures with loss of bone and attachment (periodontitis).
Excessive occlusal forces on an individual tooth may occur when normal forces are no longer distributed over several teeth, as may happen when teeth are lost or when normal forces become excessive with loss of supporting structures as a result of periodontal diseases.
Contact areas must be observed from two aspects to obtain the proper perspective for locating them: the labial or buccal aspect, and the incisal or occlusal aspect (Figures 5-7 and 5-8).
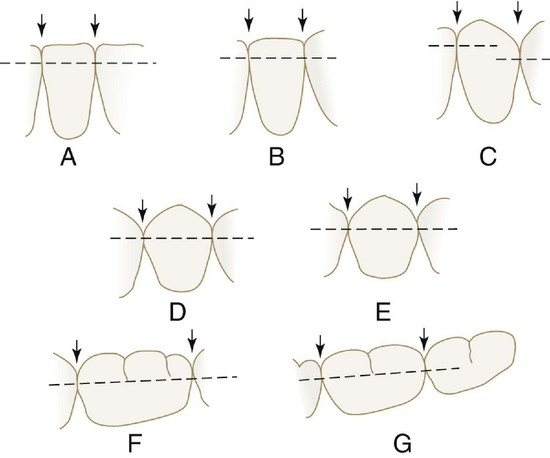
Figure 5-7 Contact levels found normally on mandibular teeth. Arrows point to embrasure spaces. A, Central and lateral incisors. B, Central and lateral incisors and canine. C, Lateral incisor, canine, and first premolar. D, Canine and first and second premolars. E, First and second premolars and first molar. F, Second premolar and first and second molars. G, First, second, and third molars.
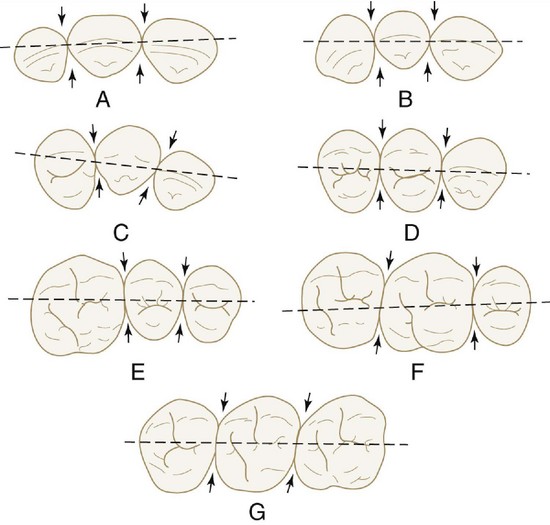
Figure 5-8 Outline drawings of the maxillary teeth from the incisal and occlusal aspects with broken lines bisecting the contact areas. These illustrations show the relative positions of the contact areas labiolingually and buccolingually. Arrows point to embrasure spaces. A, Central incisors and lateral incisor. B, Central and lateral incisors and canine. C, Lateral incisor, canine, and first premolar. D, Canine, first premolar, and second premolar. E, First molar, second premolar, and first molar. F, Second premolar, first molar, and second molar. G, First, second, and third molars.
The labial or buccal view will demonstrate the relative positions of the contact areas cervicoincisally or cervico-occlusally. The center of the area from this aspect is gauged by its relation to the length of the crown portion of the tooth (Figure 5-9).
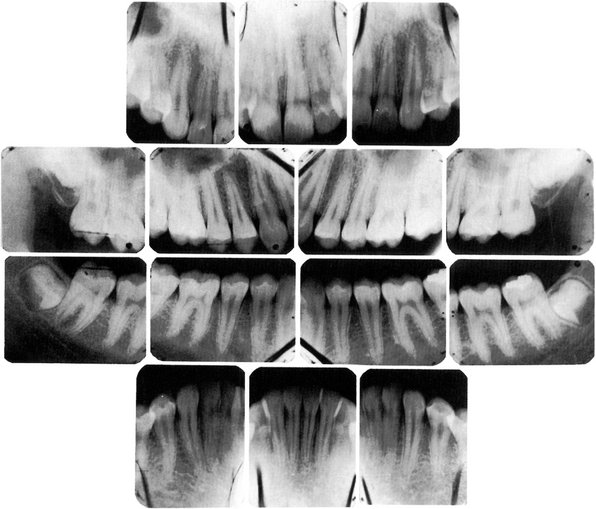
Figure 5-9 Radiograph demonstrating form of alveolar crest, contact areas, and relation to form of the crown.
The incisal or occlusal view will show the relative position of the contact areas labiolingually or buccolingually. In this instance, the center of the area may be located in its relation to the labiolingual or buccolingual measurement of the crown (Figure 5-10; see also Figure 5-8). The point at which the contact area is bisected also depends on the outline of the form of the crown from the incisal or occlusal aspect. This outline is governed by the alignment of the tooth in the arch and also by the occlusal relation with its antagonists in the opposing arch. The mandibular first molar is an excellent example (Figure 5-11; see also Figure 5-10). The contact and embrasure design for this tooth is explained later when the incisal and occlusal aspects of the teeth are considered.


Interproximal Spaces (Formed by Proximal Surfaces in Contact)
The interproximal spaces between the teeth are triangularly shaped spaces normally filled by gingival tissue (gingival papillae). The base of the triangle is the alveolar process, the sides of the triangle are the proximal surfaces of the contacting teeth, and the apex of the triangle is in the area of contact. The form of the interproximal space will vary with the form of the teeth in contact and will depend also on the relative position of the contact areas (Figures 5-12 through 5-14). Normally, a separation of 1 to 1.5 mm exists between the enamel and alveolar bone. Thus the distance from the CEJ (cervical line) to the crest of the alveolar bone as seen radiographically (see Figure 5-9) is 1 to 1.5 mm in a normal occlusion in the absence of disease.
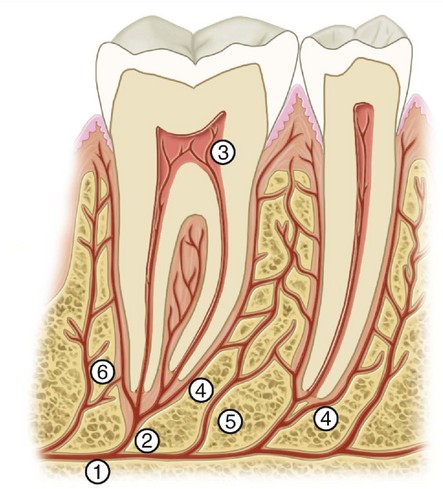
Figure 5-12 Schematic drawing of distribution of the periodontal blood vessels and interdental papillae. 1, Inferior alveolar artery; 2, dental arteriole; 3, pulpal branches; 4, periodontal ligament arteriole; 5 and 6, interalveolar arterioles.
(From Ramfjord SR, Ash MM: Periodontology and periodontics, Philadelphia, 1979, Saunders.)
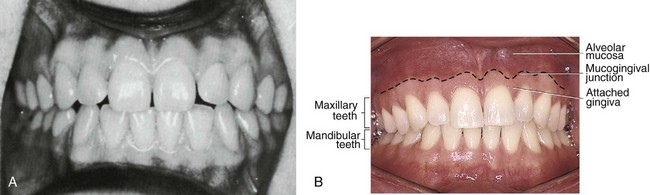
Figure 5-13 The form of the gingiva is related to the form of the teeth, contact areas, spacing between the teeth, and effects of periodontal disease and dental caries. A, Interdental papillae do not fill the interproximal areas in several places because of spacing between the teeth. B, Clinically normal gingivae; the form is different because of the form of the teeth, including contact areas.
(From Bath-Balogh M, Fehrenbach MJ: Illustrated dental embryology, histology, and anatomy, ed 2, St Louis, 2006, Saunders.)
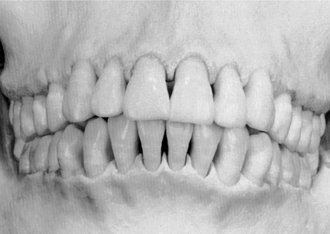
Figure 5-14 The form of the teeth, position and wear of contact areas, type of teeth, and level of eruption of the teeth determine the form of the interproximal “spaces.” These factors also determine the interproximal shape of the crest of alveolar bone.
Proper contact and alignment of adjoining teeth allows proper spacing between them for the normal bulk of gingival tissue attached to the bone and teeth. This gingival tissue is a continuation of the gingiva covering all of the alveolar process. The surface keratinization of the gingiva and the density and elasticity of the gingival tissues help maintain these tissues against trauma during mastication and invasion by bacteria.
Because the teeth are narrower at the cervix mesiodistally than they are toward the occlusal surfaces and the outline of the root continues to taper from that point to the apices of the roots, considerable spacing is created between the roots of one tooth and the roots of adjoining teeth. This arrangement allows sufficient bone tissue between one tooth and another, which anchors the teeth securely in the jaws. It also simplifies the problem of space for the blood and nerve supply to the surrounding alveolar process and other investing tissues of the teeth (see Figure 5-12).
The type of tooth also has a bearing on the interproximal space. Some individuals have teeth that are wide at the cervices, constricting the space at the base. Others have teeth that are more slender at the cervices than usual; this type of tooth widens the space. Teeth that are oversize or unusually small will likewise affect the interproximal spacing. Nevertheless, this spacing conforms to a plan that is fairly uniform, provided that the anatomical form is normal and the teeth are in good alignment.
Embrasures (Spillways)
When two teeth in the same arch are in contact, their curvatures adjacent to the contact areas form spillway spaces called embrasures. The spaces that widen out from the area of contact labially or buccally and lingually are called labial or buccal and lingual interproximal embrasures. These embrasures are continuous with the interproximal spaces between the teeth (see Figure 5-10). Above the contact areas incisally and occlusally, the spaces, which are bounded by the marginal ridges as they join the cusps and incisal ridges, are called the incisal or occlusal embrasures. These embrasures, and the labial or buccal and lingual embrasures, are continuous (Figure 5-15; see also Figure 5-8). The curved proximal surfaces of the contacting teeth roll away from the contact area at all points, occlusally, labially or buccally, and lingually and cervically, and the embrasures and interproximal spaces are continuous, as they surround the areas of contact.
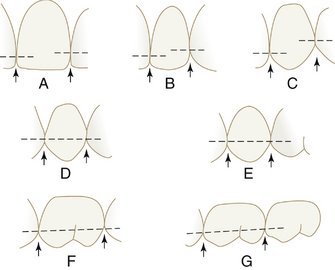
Figure 5-15 Outline drawings of the maxillary teeth in contact, with dotted lines bisecting the contact areas at the various levels as found normally. Arrows point to embrasure spaces. A, Central and lateral incisors. B, Central and lateral incisors and canine. C, Lateral incisor, canine, and first premolar. D, Canine and first and second premolars. E, First and second premolars and first molar. F, Second premolar, first molar, and second molar. G, First, second, and third molars.
The form of embrasures serves two purposes: (1) it provides a spillway for food during mastication, a physiological form that reduces the forces brought to bear on the teeth during the reduction of any material that offers resistance; and (2) it prevents food from being forced through the contact area. When teeth wear down to the contact area so that no embrasure remains, especially in the incisors, food is pushed into the contact area even when teeth are not mobile.
The design of contact areas, interproximal spaces, and embrasures varies with the form and alignment of the various teeth; each section of the two arches shows similarity of form. In other words, the contact form, the interproximal spacing, and the embrasure form seem rather constant in sectional areas of the dental arches. These sections are named as follows: the maxillary anterior section, the mandibular anterior section, the maxillary posterior section, and the mandibular posterior section. All embrasure spaces are reflections of the form of the teeth involved. Maxillary central and lateral incisors exhibit one embrasure form, the mandibular incisors another, and so on.
Maxillary posteriors and mandibular posteriors apparently require an embrasure design geared for their sections. In some cases, the constancy has to be attained by a tooth form adaptation (Figure 5-16). The canines, for instance, are shaped so that they act as a catalyst in these matters between anterior and posterior teeth. A line bisecting the labial portion of either canine seems to create an anterior half mesially that resembles half of an anterior tooth and a posterior half that resembles a posterior tooth. The mesial contact is at one level for contact with the lateral incisor, but the distal contact form must be at a level consistent with the contact form of the first premolar, whether maxillary or mandibular (see Figure 5-15, C).
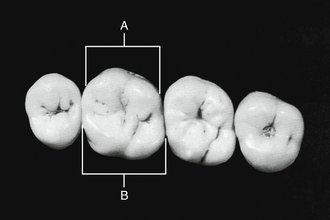
Figure 5-16 Calibration of maxillary first molar. A, Calibration at prominent buccal line angles that functions by deflecting food material during mastication. B, Calibration of lingual contour from contact area mesially to contact area distally. There are no prominent line angles, but the development of the mesiolingual cusp has widened the rounded lingual form. Thus the two lingual embrasures are kept similar in size, even though the tooth makes contact with two teeth that are dissimilar lingually. This way, the lingual gingival tissue interproximally is properly protected by the equalization of lingual embrasures.
Contact Areas and Incisal and Occlusal Embrasures from the Labial and Buccal Aspect
It is advisable to refer continually to the illustrations of contacts and embrasures during the reading of the descriptions that follow. Locate the illustration of interest (see Figure 5-15, A) while reading the details concerning contact area levels in the following paragraphs.
MAXILLARY TEETH
Central Incisors
The contact areas mesially on both central incisors are located at the incisal third of the crowns. Since the mesioincisal third of these teeth approaches a right angle, the incisal embrasure is very slight.
Central and Lateral Incisors
The distal outline of the central incisor crown is rounded. The lateral incisor has a shorter crown and has a more rounded mesioincisal angle than the central incisor. The form of these two teeth coming into contact with each other therefore opens up an embrasure space distal to the central incisors larger than the small one mesial to the central incisors. A line bisecting the contact areas distal to the central incisor and mesial to the lateral incisor approaches the junction of the middle and incisal thirds of each crown.
Lateral Incisor and Canine
The distal contact area on the lateral incisor is approximately at the middle third. The mesial contact area on the canine is at the junction of the incisal and middle thirds. The form of these teeth creates an embrasure that is more open than the two previously described.
Canine and First Premolar
The canine has a long distal slope to its cusp, which puts the distal crest of curvature at the center of the middle third of the crown. The contact area is therefore at that point. This is an important observation to be made clinically. As mentioned, it is at this point in the dental arch that the canine, situated between the anterior and posterior segments, becomes a part of both (see Figure 5-15, B and C).
The first premolar has a long cusp form also, which puts its mesial contact area rather high up on the crown. Usually it is just cervical to the junction of the occlusal and middle thirds. The embrasure between these teeth has a wide angle.
First and Second Premolars
The contact areas of the first and second premolars are similar to those just mentioned, although usually a little cervical to the junction of the occlusal and middle thirds of the crowns. The form of these teeth creates a wide occlusal embrasure.
Note that the design of the interproximal spaces changes also with the form and dimensions of the teeth in contact.
Second Premolar and First Molar
The position of the second premolar and first molar contact areas cervico-occlusally is about the same as that found between the premolars.
First and Second and Second and Third Molars
The two contact and embrasure forms for the first and second and second and third molars may be described together, since they are similar. The distal outline of the first molar is round, a fact that puts the contact area approximately at the center of the middle third of the crown. Here again, it must be emphasized that contact levels on maxillary molars (and even on premolars to some extent) tend to be centered in the middle third of the anatomical crown.
The mesial contact area of the second molar also approaches the middle third of the crown. The occlusal embrasure is generous as a consequence, even though the cusps are not long.
The contact and embrasure design of the second and third molars is similar to that of the first and second molars. The molars become progressively shorter from the first through the third. Again, the dimensions of the tooth crowns affect the contact and embrasure design.
MANDIBULAR TEETH
Central Incisors
The mesial contact areas on the mandibular central incisors are located at the incisal third of the crowns. At the time of the eruption of these teeth, the mesial and distal incisal angles are slightly rounded, and the mamelons are noticeable on the incisal ridges. Soon, however, incisal wear reduces the incisal ridge to a straight surface, and the mesial and distal angles approach right angles in sharpness. This is due partly to wear at the contact areas (see Figures 5-7 and 5-14). In many instances, the contact areas extend to the mesioincisal angle. Therefore a small incisal embrasure occurs mesially between the mandibular central incisors unless wear through usage obliterates it.
Central and Lateral Incisors
The distal contact areas and the incisal embrasures on the central incisors and the mesial contact areas and incisal embrasures on the lateral incisors are similar to those just described. Because the mandibular central and lateral incisors are small mesiodistally and supplement each other in function, the design of their crowns brings about similar contact and embrasure forms.
Note the slender Gothic arch–like spaces that circumscribe the interproximal spaces between the mandibular anterior teeth.
Lateral Incisor and Canine
The positions of the contact areas distally on the lateral incisor and mesially on the canine are approximately the same, cervicoincisally, as the other two just described. The teeth are in contact at the incisal third close to the incisal ridges. However, the mesioincisal angle of the canine is more rounded than the others, which form opens up a small incisal embrasure at this point.
The interproximal spacing between lateral and canine is very similar in outline to the two interproximal spaces just described.
Canine and First Premolar
The distal slope of the cusp of the mandibular canine is pronounced and long, which places the distal contact area on this tooth somewhat cervical to the junction of its incisal and middle thirds.
The first premolar has a long buccal cusp, and although its crown is shorter than that of the canine, the mesial contact area has about the same relation cervico-occlusally as that found distally on the canine and is just cervical to the junction of the occlusal and middle thirds. Thus the whole arrangement places these contact areas level with each other.
The occlusal embrasure is quite wide and pronounced because of the cusp forms of the two teeth. The interproximal space has been reduced by the lowering of the contact areas cervically, comparing favorably to the design for posterior mandibular teeth.
First and Second Premolars
From the buccal aspect, the crowns of the first and second premolars are similar. The buccal cusp of the second premolar is not quite as long as that of the first premolar. The contact of these teeth is nearly level with that of the canine and first premolar. The slope of the cusps creates a large occlusal embrasure. The interproximal space is a little smaller than that between the canine and first premolar.
Second Premolar and First Molar
The contact and embrasure design for the second premolar and first molar is similar to that just described for the premolars. The mesiobuccal cusp of the first molar is shorter and more rounded than the cusp of the second premolar, which varies the embrasure somewhat, and since the crown of the molar is a little shorter, it reduces the interproximal space to that extent.
First and Second and Second and Third Molars
The two contact and embrasure designs of the first and second and second and third molars may be described together, since they are similar.
The proximal surfaces—that is, the distal surface of the first molar, mesial surface of the second molar, distal surface of the second molar, and mesial surface of the third molar—are quite round. The occlusal embrasures are therefore generous above the points of contact, even though the cusps are short and rounded.
Because the molars become progressively shorter from the first to the third, the centers of the contact areas also drop cervically. A line bisecting the contact areas of the second and third molars is located approximately at the center of the middle thirds of the crowns.
The interproximal spaces have been reduced considerably because of their shortened form.
Contact Areas and Labial, Buccal, and Lingual Embrasures from the Incisal and Occlusal Aspects
To study the relative positions of contact areas and the related labial, buccal, and lingual embrasures and also to get proper perspective, the eye must be directed at the incisal surfaces of anterior teeth and directly above the surface of each tooth being examined in series (Figure 5-17; see also Figures 5-8, 5-10, and 5-11). Posterior teeth are examined in the same manner. Look down on each tooth or group of teeth by facing the occlusal surfaces on a line with the long axis.
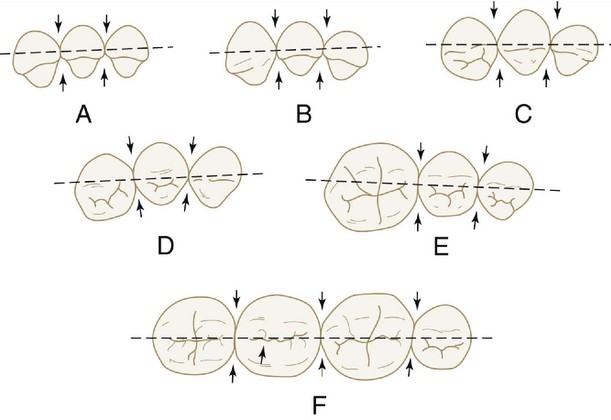
Figure 5-17 Contact relation of mandibular teeth labiolingually and buccolingually when surveyed from the incisal and occlusal aspects. Arrows point to embrasure spaces. A, Central incisors and lateral incisor. B, Central and lateral incisors and canine. C, Lateral incisor, canine, and first premolar. D, Canine, first premolar, and second premolar. E, First premolar, second premolar, and first molar. F, Second premolar and first, second, and third molars.
The problem at this point is to discover the relative positions of contacts in a labiolingual or buccolingual direction and to observe the embrasure form facially and lingually created by the tooth forms and their contact relations.
A generalization may be established in locating contact areas faciolingually. Anterior teeth will have their contacts centered labiolingually, whereas posterior teeth will have contact areas slightly buccal to the center buccolingually. This buccal inclination must be carefully studied and must not be overemphasized.
Except for the maxillary first molar, all crowns converge more lingually than facially from contact areas. The maxillary first molar is the only tooth wider lingually than buccally (see Figure 5-16). Its formation makes a necessary adjustment of the mesiolingual embrasure when the tooth form of maxillary posteriors changes from the maxillary premolar form to the purely rhomboidal form of maxillary second and third molars. This situation is discussed more fully later on.
The narrower measurement lingually rather than facially causes wider embrasures lingually compared with facial embrasures. Compare the two types of embrasures displayed by maxillary central and lateral incisors.
MAXILLARY TEETH
See Figures 5-8 and 5-10, A.
Central Incisors
The contact areas of the central incisors are centered labiolingually. The labial embrasure is a V-shaped space created by the labial form of these crowns. The lingual embrasure widens out more than the labial embrasure because of the lingual convergence of the crowns (see Figure 5-10, A). Note the centering of the labioincisal edge with respect to the crown outline of these teeth, and the narrowness of the lingual surfaces in comparison with the broad labial faces.
Central and Lateral Incisors
The contact areas of the central and lateral teeth are centered labiolingually also.
Lateral Incisor and Canine
The contact area of the lateral incisor and canine is centered labiolingually on both canine and lateral incisors. The lingual embrasure is similar to that of the central and lateral incisors, but the labial embrasure is changed somewhat by a definite convexity at the mesiolabial line angle of the canine.
Canine and First Premolar
The contact area of the canine and first premolar is centered on the distal surface of the canine but is a little buccal to the center on the mesial surface of the first premolar. The embrasure design lingually is marked by a concavity in the region of the distolingual line angle of the canine and by a developmental groove crossing the mesial marginal ridge of the first premolar.
First and Second Premolars
The contact areas of the first and second premolars are nearly centered buccolingually. The embrasures buccally and lingually are regular in outline, although slightly different in design.
The prominence of the mesiobuccal and distobuccal line angles of the premolars is in direct contrast to the even taper of these teeth lingually, as viewed from the occlusal aspect. This form demonstrates a slight variation between buccal and lingual embrasures.
Second Premolar and First Molar
As usual, a line bisecting the contact areas of the second premolar and first molar is nearly centered on the distal surface of the second premolar. The area on the mesial surface of the first molar is located farther buccally than other contact areas on the maxillary posterior teeth. The contact areas are wider on molars because of the greater width buccolingually of the molar teeth.
The buccal embrasure between these teeth and the location of the mesial contact area of the first molar are influenced by the prominence of the mesiobuccal line angle of the maxillary first molar and the matching prominence of the distobuccal line angle of the maxillary second premolar. The lingual embrasure is kept standard for the molar area by the enlargement of the mesiolingual cusp of the first molar. Occasionally, this cusp carries a small conformation lingually as part of the change in form (fifth cusp, or cusp of Carabelli). Usually, the mesiolingual cusp of the maxillary first molar is rounded out, with no more than a developmental groove showing that an extra cusp formation may have been intended.
The mesiolingual lobe of this tooth is always large, however, causing the tooth to be wider lingually from its mesiolingual line angle to its distolingual line angle than it is from the mesiobuccal line angle to the distobuccal line angle. If it were not for this fact, the rhomboid form of the first molar in contact with the tapered form of the second premolar would open up a lingual embrasure of extremely large proportions. The large mesiolingual lobe makes up for the change in occlusal outline from premolar form to molar form, keeping the conformity of the lingual embrasures (see Figure 5-16).
First and Second and Second and Third Molars
The contact and embrasure forms of the first and second and second and third molars may be described together, since they are similar. Although the mesiobuccal line angles of the second and third molars are not as sharp as that of the first molar, they are prominent nevertheless.
The distobuccal line angles of all the maxillary molars are indistinct and rounded, so that the buccal embrasure forms are shaped and characterized mainly by the prominent mesiobuccal line angle. The mesiolingual line angles of the second and third molars are rounded and in conjunction with the rounded distolingual line angles; the lingual embrasures between first, second, and third molars present a regular and open form (see Figure 5-8, F and G).
The contact areas are broad and centered buccolingually. The embrasures are uniform. Note the generous proportions of the buccal embrasures.
MANDIBULAR TEETH
See Figures 5-10, 5-11, and 5-17.
Central Incisors and Central and Lateral Incisors
The contact areas and embrasures of the central incisors and the central and lateral incisors may be described together, since they are similar.
Although these teeth are narrow mesiodistally, their labiolingual measurements are not much less than those of the maxillary central and lateral incisors. The mandibular central incisors come within a millimeter or so of having the same labiolingual diameter as that of the maxillary central incisors; the mandibular lateral incisors have a labiolingual diameter as great if not greater than that of the maxillary lateral incisors.
The contact areas are centered labiolingually, and the embrasures are uniform. Although the mesiodistal dimensions are less, the outline form of the incisal aspects of the mandibular central and lateral incisors is similar to that of the maxillary central and lateral incisors in that the lingual outlines have a rounded taper in comparison with broader, flattened labial faces.
Lateral Incisor and Canine
The contact areas of the lateral incisor and canine are centered, and the lingual embrasure is similar to those just described. The labial embrasure is influenced by the prominence of the mesiolabial line angle of the canine. Note that the maxillary canine presents the same characteristic.
Canine and First Premolar
The canine and first premolar contact areas are approximately centered, and the buccal embrasure is smooth and uniform in outline. The lingual embrasure is opened up somewhat by a slight concavity on the canine distolingually and by a characteristic developmental groove across the marginal ridge of the first premolar mesiolingually.
First and Second Premolars
The contact areas of the first and second premolars are nearly centered buccolingually but are broader than those found mesial to them, because the distal curvature of the first premolar describes a larger arc than the mesial curvature and the mesial contacting surface of the second premolar is relatively broad and describes a shallower curved surface than that of the distal surface of the first premolar.
Because of the lingual convergence of the first premolar and the narrow lingual cusp form, the lingual embrasure is as wide as the one mesial to it.
Second Premolar and First Molar
The second premolar and first molar contact areas are wide and almost centered. The extent of the contact areas is sometimes increased by a slight concavity in the outline of the mesial surface of the first molar below the marginal ridge. The mesial contact area of the first molar is located farther buccally than any of the other contact areas on mandibular posterior teeth. It must be remembered that the same situation holds true in the upper dental arch when the contacts of the maxillary first molars and second premolars are described.
The prominence of the first molar at the mesiobuccal line angle is readily apparent. The mesial outline of the crown tapers to the lingual, forming a generous lingual embrasure in conjunction with the smooth curvature of the second premolar distolingually.
First and Second Molar
The contact areas of the first and second molars are nearly centered buccolingually, although they are not so broad as the contact just described. This variation is brought about by the design of the first molar distally. The distal contact area of the first molar is confined to the distal cusp, which does not present the broad surface for contact with the second molar that was found mesially in contact with the second premolar. This form, along with the rounded outline at the distobuccal line angle, opens up both embrasures wider than those found immediately mesial.
The outline of the first molar crown just lingual to the distal contact area presents a straight line and an occasional concavity.
The second molar outline buccally and lingually on both sides of the mesial contact area is uniformly rounded.
Second and Third Molars
The contact areas of the second and third molars are broad, and they are nearly centered buccolingually. When the third molar is normally developed, it is similar in outline to the second molar from the occlusal aspect. The buccal and lingual embrasures between these teeth are almost alike in form and extent.
A straight line may be drawn through the contact areas of the second premolar and the three molars, and it will come very near to bisecting all of the contact areas. These four mandibular teeth are set in a line that is almost straight (see Figures 5-10, B, and 5-17, F).
Facial and Lingual Contours at the Cervical Thirds (Cervical Ridges) and Lingual Contours at the Middle Thirds of Crowns
The teeth are unique in that their static outside form is physiological. Even the maxillary teeth, which are firmly set in their alveoli, when moving through food material activated by mandibular movement, change their functional crown form from a static to a dynamic form. All details of tooth form have some effect on the stabilization of the tooth in the arch.
Examinations show that all tooth crowns, when viewed from mesial or distal aspects, have rather uniform curvatures at the cervical thirds and at the middle thirds labially or buccally or lingually, depending on the teeth being examined (Figure 5-18, A, D, and E). As has already been discussed briefly, concepts about the importance of these contours in relation to protection and stimulation of the gingiva have been challenged. However, the evidence does not contradict the possibility that food impaction or trauma can occur as a result of “faulty” contours (undercontouring). It is, rather, that inflammatory periodontal disease is caused primarily by bacterial plaque and that buccal and lingual contours do not appear to be related to plaque removal during mastication. Thus in the absence of oral hygiene measures, the self-cleansing mechanisms of the musculature and suggested cleansing action of coarse food are not adequate to remove plaque sufficiently well to prevent gingivitis. However, the relative importance of contour on trauma, food impaction, and, occasionally, the initiation of a localized inflammatory response cannot be overlooked. The buccal and lingual contours can deflect food material away from the gingival margins during mastication (Figure 5-18, A). Undercontoured surfaces can lead to food impaction (Figure 5-18, B), but the significance of overcontouring (Figure 5-18, C) has yet to be clarified, although overcontouring does not appear to be beneficial. Marginal adaptation of the gingiva and home and professional cleaning are of far greater significance for gingival health.
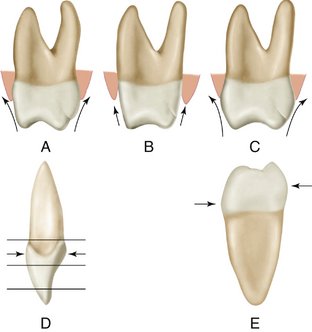
Figure 5-18 Schematic drawings of curvatures labially, buccally, and lingually. A, Normal curvatures as found on maxillary molar. Arrow shows theoretical path of food during mastication. B, If molar shows little or no curvature, there is possibility for food impaction. C, Molar with curvature in excess of normal. The significance of such an excess in curvature has not been firmly established. D, Normal cervical curvatures as found on maxillary incisors. The crests of curvature are opposite each other labiolingually. E, Curvatures as found on mandibular posterior teeth.
The cervical third formation of the crowns is the area of soft tissue attachment. The epithelial attachment of soft tissue to the teeth, soon to be described more fully, is entirely within the area of the cervical third of the crowns. The cervical curvatures are often spoken of as cervical ridges. However, cervical curvature is a more descriptive term, because few of these areas are pronounced enough to be called ridges and yet rarely is a normal tooth seen with no curvature at all.
In young persons, and some older ones, most of the curvature lies beneath the gingival crest. In older persons, the CEJ may be visible or may be just under the gingival crest, with most of the prominent curvature exposed.
Gradual recession of the gingivae throughout life may be a normal occurrence. However, root exposure may lead to cemental caries, cervical sensitivity, and abrasion with improper tooth brushing.
All protective curvatures are most functional when the teeth are in proper alignment. It should be quite plain that when teeth are malposed, their curvatures are displaced and may be ineffective.
The curvatures are rather uniform at the cervical third or lingual third of all of the maxillary teeth and on the buccal portion of mandibular posterior teeth (Figures 5-19 through 5-21).
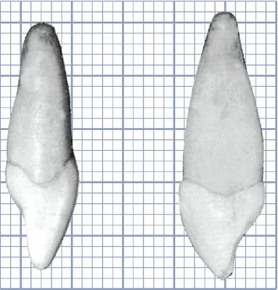
Figure 5-19 The maxillary central incisor exhibits a curvature of approximately 0.5 mm labially and somewhat less lingually at the cervical third of the crown. Many specimens show equal curvature on the two sides. The maxillary canine exhibits approximately the same curvature. Note the limitation of the curvature at the cingulum area above the cervical line.(Grid = 1 sq mm.)
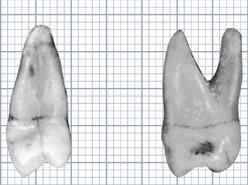
Figure 5-20 The maxillary first premolar has a curvature of approximately 0.5 mm buccally and lingually. The crest of curvature buccally is located at the cervical third of the crown and lingually at the middle third. The maxillary first molar has curvatures of the same degree at similar points on both sides. (Grid = 1 sq mm.)
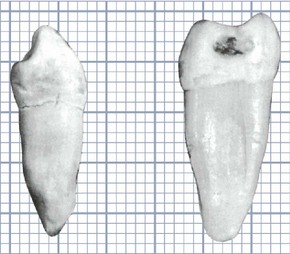
Figure 5-21 Mandibular first premolar and first molar. Both teeth have a curvature of approximately 0.5 mm buccally at the cervical third of the crown and a curvature of approximately 1 mm lingually, with the crest of curvature at the middle third. (Grid = 1 sq mm.)
The normal curvature from the CEJ to the crest of contour is approximately 0.5 mm in extent. When the long axis of the tooth is placed vertically, it is found that this curvature is fairly constant and may be recognized as average or normal for the maxillary teeth, labially or buccally and lingually, and for the mandibular posterior teeth on the buccal surfaces. The curvature, lingually, of mandibular posterior teeth extends about 1 mm beyond the cervical line. Here, however, the extreme curvature does not contribute to the stasis of food material at the cervix because of the activity of the tongue in keeping the lingual surfaces of these teeth clean.
Figure 5-19 shows that the maxillary central incisor and canine have curvatures, labially and lingually, that are almost identical. Because the canines have a more massive development of the cingulum, clinical observation only gives an impression of greater curvature. This is an optical illusion that is dispelled when the outline of the canine is properly compared with that of other teeth on a graph.
The maxillary premolar and molar show the same limited curvatures. The crest of curvature, lingually, on all posterior teeth is at or near the middle third of the crowns.
When curvatures are found that are greater in extent than 0.5 mm, rarely is the curvature as much as 1 mm, except lingually on mandibular posterior teeth and often lingually on maxillary posterior teeth. In these instances, the crest of contour is found at the middle third of the crowns instead of at the cervical third (see Figure 5-21). These crests are always lingual.
The eye is easily confused at times when viewing certain aspects of the teeth because of the abrupt sweep of curvatures as they travel from the cervical line toward occlusal and incisal surfaces (i.e., the buccal surfaces of mandibular posterior teeth, the lingual surfaces of posterior maxillary teeth, or the lingual surfaces of canines). When the actual photographs are placed on a background of squares (Figure 5-22), with the long axis of each tooth positioned vertically, we readily see that the extent of curvature from the cervical line to the crest of curvature facially or lingually is slight. Quite often, in restorative procedures, it is greatly overestimated and reproduced.
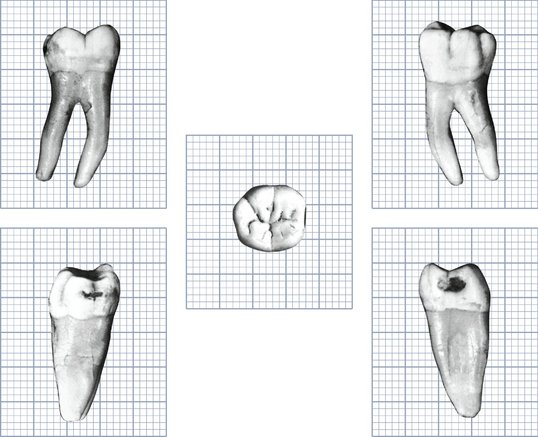
Figure 5-22 Photographs of a natural specimen of a mandibular first molar, taken with a lens capable of two-diameter registrations. Cutouts of these photos were placed on graphs depicting squared millimeters. The result is an accurate graph in millimeters of tooth outlines from five aspects. (Grid = 1 sq mm.)
Figure 5-23 shows a mandibular central incisor and canine from the mesial aspect. Here, the curvature at the cervical third is less than that of the other teeth in the mouth, occasionally appearing so slight that it is hardly distinguishable. The canine often has little more curvature immediately above the cervical line than the mandibular central or lateral incisor.
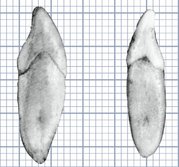
Figure 5-23 Mandibular central incisor and canine. The central incisor curvature labially and lingually is less than 0.5 mm in extent, and the crest of curvature is near the cervical line. The canine also exhibits less than 0.5-mm curvature, although the crest of curvature is higher up on the crown; however, it is still within the confines of the cervical third. (Grid = 1 sq mm.)
SUMMARY OF PHYSIOLOGICAL CONTOURS OF TOOTH CROWNS, FACIALLY AND LINGUALLY
All tooth crowns exhibit some curvature above the cervical line. Again, this slight bulge at the cervical third is sometimes called the cervical ridge. Although the extent of curvature will vary in different individuals, apparently it is not normal for the curvatures on permanent teeth to extend out as much as 1 mm beyond the cervical line; usually the curvature will be less.
The curvatures on the labial, buccal, and lingual surfaces of all maxillary teeth and on the buccal surfaces of mandibular posterior teeth are rather uniform; the average curvature, as mentioned before, is about 0.5 mm.
Mandibular posterior teeth have a lingual curvature of approximately 1 mm, with the crest of curvature at the middle third of the crown instead of at the cervical third. Occasionally maxillary posterior teeth have similar curvatures on the lingual aspect. (Compare the lingual curvatures in Figures 5-20 and 5-21.)
Mandibular anterior teeth show less curvature on the crown above the cervical line than any of the other teeth. Usually it is less than 0.5 mm, and occasionally it is so slight that it is hardly distinguishable. The mandibular canines may show a little more curvature than central and lateral incisors.
Regardless of whether theories explaining the functional significance of these contours are correct, there is little doubt that they are important. If this were not so, there would be more variance in the presence or the extent of curvature. The curvatures as described seem to be as standard and as constant as any anatomical detail can be.
The Height of Epithelial Attachment: Curvatures of the Cervical Lines (Cementoenamel Junction [CEJ]) Mesially and Distally
The epithelial attachment seals the soft tissue to the tooth. It is a remarkable system capable of adjustment to local physiological changes, but it is vulnerable to physical injury. Careless treatment can cause breaks in the attachment, making the tooth liable to further physical or pathological injury. The teeth can be injured by careless probing during clinical examination, by improper scaling during prophylactic treatment, by tooth preparation techniques in operative procedures, and so forth.
The height of normal gingival tissue, mesially and distally, on approximating teeth is directly dependent on the heights of the epithelial attachment on these teeth. Normal attachment follows the curvature of the CEJ if the teeth are in normal alignment and contact. This does not mean that the CEJ and the epithelial attachment are at the same level, but it does mean that they tend to follow the same curvature, even though the epithelial attachment may be higher on the crown on its enamel surface (Figure 5-24). A comparison of the curvatures of the CEJ mesially and distally on the teeth is therefore in order. Measurements and comparisons are shown in Figures 5-25 and 5-26; see also Table 1-1.
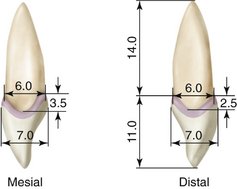
Figure 5-24 Curvatures of the cervical line (cementoenamel junction) mesially and distally on the maxillary central incisor, demonstrating the points of measurement in determining the relation between the curvatures of the cervical line mesially and distally. Other points of measurement of the crown and root, when one observes the mesial and distal aspects, are outlined and are considered average measurements for a mandibular central incisor. The shaded area in the form of a band on the enamel follows the cervical curvature and represents the epithelial attachment of gingival tissue to the enamel of the crown. The unit of measurement in the figure is millimeters.
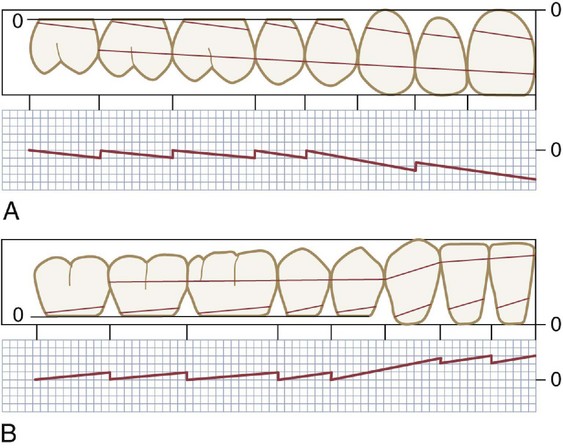
Figure 5-25 Schematic drawing of the crowns of maxillary and mandibular teeth with associated graphs of the average extent of curvatures of the cervical line mesially and distally. A, Maxillary teeth. B, Mandibular teeth. Compare the graph of cervical curvatures with a line drawn through the center of contact areas. Note that the graph tends to run somewhat parallel to this line. (Grid = 1 sq mm.)
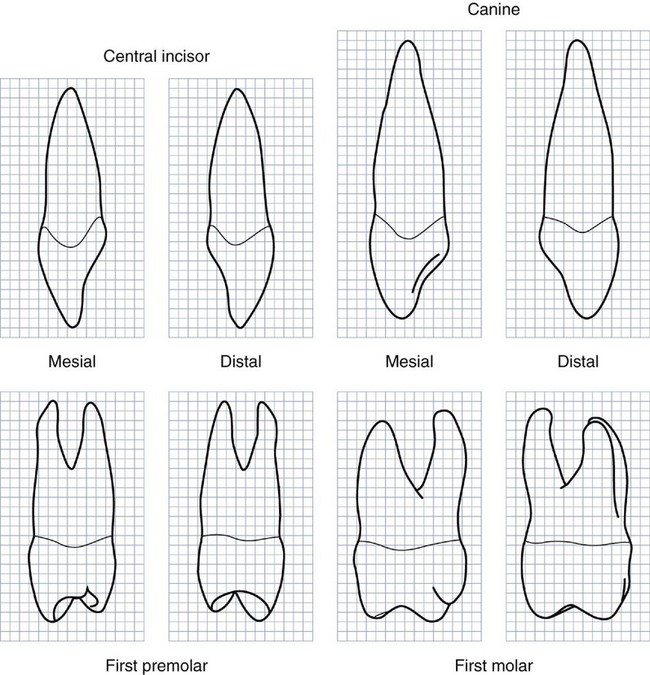
Figure 5-26 Graphs of typical forms of maxillary teeth accenting the outlines of cervical lines mesially and distally. (Grid = 1 sq mm.)
The extent of curvature seems to depend on the height of the contact area above the crown cervix and also on the diameter of the crown labiolingually or buccolingually. The crowns of anterior teeth, which are narrower and longer from these aspects, show the greatest curvature (see Figure 5-25). In the use of the words height and above, the supposition is made that in either the maxillary or the mandibular arch the occlusal surfaces of the teeth are above the cervices. Any point approaching the incisal edge or occlusal surface of a crown is considered above the cervix, and the height is increased as it approaches occlusal levels.
Periodontal attachment that follows the curvature of the CEJ mesially and distally seems to be about as high on mandibular anterior teeth as on their counterparts that are larger in the maxillary arch. Although the crowns of the mandibular anterior teeth average 1 mm less in labiolingual diameter (the lateral incisors excepted), the contact areas are higher accordingly, being near the incisal edges on centrals and laterals. Consequently, measurements usually show less than 1-mm variation in mesial and distal curvatures between maxillary and mandibular anterior teeth.
Posterior teeth show little variation in either arch. Figure 5-25 is a diagrammatic drawing of the outlines of the teeth on one side of the arch when viewed from the labial and buccal aspects. These outlines have been placed so that a direct comparison can be made with the graphs below them. The graphs demonstrate the relative height of individual attachments in the average normal case. They are based on cases having upper central incisors with crowns 10.5 to 11 mm in length. Unless the teeth were very large or very small, the graphs would not vary from those illustrated by more than 0.5 mm.
The curvature of the cervical line of most teeth (CEJ) is approximately 1 mm less distally than mesially. The greater curvature is found at the median line on central incisors, maxillary and mandibular. The height of attachment is dependent on the height of the contact areas of the two teeth creating the interproximal space. If the mesial curvature of the central incisor is calibrated at 3.5 mm, the distal curvature is about 1 mm less, or 2.5 mm.
The six anterior teeth, both maxillary and mandibular, when compared with posteriors, exhibit the greatest curvature. Because the canine crowns function distally as posterior teeth, their curvatures distally represented by the CEJ are slight, being about 1 to 1.5 mm on the average. Premolars and molars have rather uniform but slight curvatures. The contact levels are low in relation to total crown length; consequently, these teeth do not have high periodontal attachments interproximally. The average premolar or molar has a curvature mesially of only 1 mm or less, with no curvature or even a minus curvature distally (Figure 5-27).
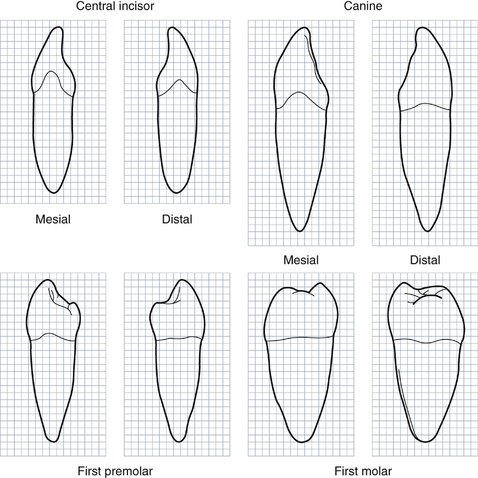
Figure 5-27 Graphs of typical forms of mandibular teeth accenting the outlines of cervical lines mesially and distally. (Grid = 1 sq mm.)
From the operator’s point of view, anterior teeth especially must be carefully approached (when attachment is normal) as, for example, in preparing them for restoration. Posterior teeth have curvatures that are less critical.
A summary of the height of periodontal attachment interproximally indicates the attachment to be highest at the median line on central incisors. In distal progression the height of attachment decreases along with the decrease in curvature of CEJs until the mesial surface of the first premolar is reached. From this point distally through third molars, curvatures are slight.
The possibility of injury to mesial and distal periodontal attachment during tooth preparation should be considered. The height of attachment must be ascertained by careful probing and by the continuous observation of landmarks during the operation. Improper usage of impression materials must also be avoided.
To secure scientific data regarding comparative curvatures, it was necessary to examine many tooth specimens. It was found that, usually, a graph of the cementoenamel curvatures from the median line distally could be staggered, as in Figure 5-25. It is noticed that in the posterior teeth, the variation in curvature is slight and the amount of curvature is minor, with the variance ranging from 1 mm mesially toward the occlusal surface to a slight curvature in the opposite direction. (Note the distal aspect of the mandibular first molar in Figure 5-27.)
Figures 5-26 and 5-27 are graphs of maxillary and mandibular teeth demonstrating typical cervical curvatures mesially and distally.
1. Ostry DJ, Vatikiotis-Bateson E, Gribble PL. An examination of the degrees of freedom of human jaw motion in speech and mastication. J Speech Lang Hear Res. 1997;40:1341.
2. Braun S, et al. The form of the human dental arch. Angle Orthod. 1998;68:29.
3. Nixon RL. Mandibular ceramic veneers: an examination of diverse cases integrating form, function, and esthetics. Pract Periodontics Aesthet Dent. 1995;7:17.
4. Watanabe M, et al. Morphological and functional analysis of dento-orofacial complex in monozygotic twins with Duchenne type muscular dystrophy. J Jpn Orthod Soc. 1990;49:522.
5. McDonald F. The condylar disk as a controlling factor in the form of the condylar head. J Craniomandib Disord. 1989;3:83.
6. Magne P, Versluis A, Douglas WH. Rationalization of incisor shape: experimental-numerical analysis. J Prosthet Dent. 1999;81:345.
7. Sorensen DA. Form follows function-based rationale for esthetic dentistry. J Indiana Dent Assoc. 1998;77:25.
8. McCulloch CA, et al. Role of physical forces in regulating the form and function of the periodontal ligament. Periodontology. 2000;24:56.
9. Daftary F. Dentoalveolar morphology: evaluation of natural root form versus cylindrical implant fixtures. Pract Periodontics Aesthet Dent. 1997;9:469.
10. Daftary F. Prosthetically formulated natural aesthetic implant prostheses. Pract Periodontics Aesthetic Dent. 1994;6:75.
11. Ramfjord SR, Ash MM. Periodontology and periodontics. Philadelphia: Saunders; 1979.
Ash MM, Karring T. Periodontal and occlusal considerations in operative dentistry. In: Horsted-Bindslev P, Mjor IA, editors. Modern concepts in operative dentistry. Copenhagen: Munksgaard, 1988.
Beaudreau DE. Tooth form and contour. J Am Soc Psychosom Dent Med. 1973;3:36.
Becker C, Kaldahl WB. Current theories of crown contour, margin placement and pontic design. J Prosthet Dent. 1981;45:268.
Butler PM, Joysey KA, editors. Development, function and evolution of teeth. New York: Academic Press, 1978.
Douglas WH. Form, function and strength in the restored dentition. Ann R Austral Coll Dent Surg. 1996;13:35.
Farer J, Isaacson D. Biologic contours. J Prev Dent. 1974;1:4.
Herlands RE, et al. Forms, contours and extensions of full coverage restorations in occlusal reconstruction. Dent Clin North Am. March 1962;6:147.
Lindhe J, Wicen PO. The effects on the gingivae of chewing fibrous foods. J Periodont Res. 1969;4:193.
Maeda Y, et al. Biomechanical study of temporomandibular joint on its form and function. Part I: Condyle morphology in frontal section. J Osaka Univ Dent Sch. 1993;33:65.
Morris M. Artificial crown contours and gingival health. J Prosthet Dent. 1962;12:1146.
Nissan HF, Ride RA, Noble WH. Physiologic design criteria for fixed dental restorations. Dent Clin North Am. 1971;15:543.
Perel ML. Periodontal considerations of crown contours. J Prosthet Dent. 1971;26:627.
Ryder JA. On the mechanical genesis of tooth forms. Proc Acad Natl Sci Phila. 1878;30:45.
Sackett BP, Gildenhuys RR. The effect of axial crown over-contour on adolescents. J Periodontol. 1976;47:320.
Volchansky A. The role of clinical crown height and gingival margin position in oral disease. Diastema. 1979-1980;7:17.
Wade AB. Effect on dental plaque of chewing apples. Dent Pract. 1971;21:194.
Wheeler RC. Complete crown form and the periodontium. J Prosthet Dent. 1961;11:722.
Youdelis RA, Weaver JD, Sapkos S. Facial and lingual contours of artificial complete crown restorations and their effects on the periodontium. J Prosthet Dent. 1973;29:61.
 site for additional study resources.
site for additional study resources.