4 Forensics, Comparative Anatomy, Geometries, and Form and Function
This chapter includes brief discussions of forensic dentistry, comparative dental anatomy, and some relationships of form to function in the permanent dentition. The limited space allotted to these subjects should not suggest that they lack importance. The literature on these subjects is extensive, and the reader should review the references cited for additional information.
Forensic Dentistry
Forensic dentistry (odontology) is the field within the greater disciplines of dentistry and forensic science that evaluates, manages, and presents dental evidence in legal proceedings in the interest of justice.1 Forensic dental casework often involves identification of unidentified or missing individuals, human remains, or victims of mass fatality incidents, including natural and accidental disasters. This is accomplished by comparison of a victim’s dentition and supporting structures with dental records of known individuals. The latter records may be obtained from private dental offices, prison or military dental databases, or records retained by the Federal Bureau of Investigation through its National Crime Information Center’s Missing, Unidentified, and Wanted Persons files in a Web environment.2
Since forensic odontology is one of several forensic specialties, the forensic dentist’s role often interfaces with those of the anthropologist, criminologist, toxicologist, pathologist, and law enforcement official involved with a case. Only a brief summary is given here with general references added to cited references for further reading.
JAWS AND TEETH
Unlike the static, genetically determined friction ridges found on the human hand and foot (commonly referred to as fingerprints and footprints) each individual’s dentition is fluid and changes throughout life as the deciduous teeth are exfoliated and the permanent dentition erupts. In addition, the teeth are subject to dental and periodontal disease, the oral manifestations of systemic diseases that may affect the individual, and alterations of dental structures related to techniques of restoration and replacement that are employed by the dental practitioner.
Historically, despite this potential for an ever-changing dentition, inspection of the teeth and jaws has been used as a legally accepted method of human identification. Significant cases in which identification has been resolved by means of examination of dental evidence include identification of Revolutionary War hero Dr. Joseph Warren, the prominent Boston murder victim Dr. George Parkman, and Adolph Hitler.3
Paramount to the success of a forensic dental comparison between antemortem and postmortem dental records is the requirement that both sets of records provide the maximum amount of dental information for analysis. Thus, dentists are encouraged to document all dental anomalies, existing restorations, and missing teeth in their written, photographic, and radiographic records.
CHRONOLOGICAL AGE
The determination of dental maturity and tooth development has been considered in Chapter 2. As indicated there, the determination of chronological age is possible with some reasonable degree of accuracy. When it is employed in conjunction with evaluation of the stage of development of osseous tissues,4 the two methods can be used to determine an estimated age for an individual less than 20 years old. This is accomplished by entering data from both methods into an electronic encyclopedia on maxillofacial, dental, and skeletal development.5
Chronological age determination is a central issue in population studies, and racial and sex differences in tooth development and eruption patterns are acknowledged.6,7 Dental age assessment is also important in the forensic dental evaluation of human remains or living individuals. Aging of the dentition has been employed in forensic dental casework involving estimation of age of unidentified individuals.8,9
Separation of victims of multiple fatality incidents by age facilitates the narrowing of searches for eventual identification by comparison of medical and dental records. Dental evaluation of illegal immigrants, who may present authorities with misinformation concerning their age, is important in cases in which protection of unaccompanied minors is a concern.2
A variety of dental age estimation procedures have been employed. Some are useful in the analysis of radiographic changes associated with development of the dentition of children.10 Others use dental radiographs to determine the dental chronological age in living or deceased adult individuals.11,12
Estimation of the age of an adult may also be based on six characteristics first identified by Gustafson in 195013 by his observation of ground sections of extracted teeth. These six variables include attrition of the occlusal or incisal surfaces, degree of deposition of secondary dentin (evaluation of the size of the pulp chamber and canal), deposition of apical cementum, attachment level of the periodontium, root resorption, and radicular translucency.
In addition, biochemical methods that assess the ratios of levorotatory and dextrorotatory isomers of the long-lived, metabolically stable amino acid aspartate have been employed in both living and deceased subjects to age tissues in which this substance is found. Through a racemization process the L form of aspartic acid is slowly transformed into its stereoisomer, which is the D form of the amino acid. As enamel and dentin age, levels of the D form of aspartic acid increase in these calcified dental structures. These values can be measured and related to known levels for age estimation.14
DENTAL DNA
Each individual’s unique genetic information is contained within the nuclear and mitochondrial deoxyribonucleic acid (DNA) molecules of their cells. Only identical twins share the same DNA. Nuclear DNA is transmitted from either parent, whereas mitochondrial DNA is derived only through a maternal route. As a unique biological molecule, DNA offers the forensic scientist a means of positively identifying an individual when this material can be obtained from tissues or bodily fluids recovered at a crime scene or from human remains or other forensic evidence.
The most widely used method for forensic analysis of DNA material is the restriction fragment length polymorphism (RFLP) technique. This laboratory procedure requires that large amounts (>100 ng) of DNA be used in the analysis. The polymerase chain reaction (PCR) technique is employed when this cannot be accomplished because of degradation of the DNA molecule submitted as evidence, when only small amounts (<100 pg) of DNA are available for analysis, or when the DNA sample is fragmented.15 The PCR method amplifies the amount of DNA available for analysis by copying a specific locus of genetic material.16 Since only small amounts of DNA evidence need be evaluated using PCR technology, a positive identification may still be effected when human remains have been left unburied for long periods or have been incinerated, or when DNA trace evidence is obtained from saliva, blood, or fluid samples.
The calcified and pulp tissues within a tooth often present the forensic scientist with the most uncontaminated and protected DNA samples for analysis. Thus, even small amounts of DNA recovered from these tissues often may be analyzed using the PCR method when other means of identification have been lost or degraded as evidence.17,18
In addition, the sex of a decedent can be determined through DNA analysis of the sex-linked amelogenin gene. A DNA sample from the victim can be compared directly with one obtained from the clothing or other personal effects of a putative subject of interest or indirectly with a sample from the parents or siblings of the individual one is attempting to identify.19
BITE MARKS
When the dentition of a human or animal impresses the surface of an object during the act of biting, a pattern mark is often imprinted on that surface (Figure 4-1, A). Like a tool mark left as forensic evidence, the pattern left by the teeth can be evaluated and compared to the dentition that allegedly caused it (Figure 4-1, B). Whether the bite mark pattern involves the skin of a victim or suspect or remains on the surface of an inanimate object, to be probative, it must have class and individual characteristics consistent with a mark caused by teeth.

Figure 4-1 Forensic bite marks. A, Forehead bite marks. B, Bite marks related to maxillary dental cast.
(Courtesy Dr. David Ord.)
Class characteristics of a bite mark include the size and shape of the pattern. In most cases this should be consistent with the dental arch size of the suspected biter (human or animal) and retain a circular shape consisting of two half arches (maxilla and mandible) separated by a space (temporomandibular joint). One arch should be larger in its greatest dimension, representing the greater arch length of the maxilla.
Individual characteristics associated with a bite mark involve the patterns routinely made by specific teeth. In the human dentition these include the following:
It is generally accepted that no two individuals have an identical dentition based on variations in the arrangement, spacing, size, and shape of specific teeth and dental arches. Currently, however, neither quantitative values nor databases have been established for the dentition that are similar to those described for fingerprint and DNA analysis and comparison. Thus, although bite mark evidence has been admissible in the federal and state courts of the United States based on the Frye rule and decisions related to the Federal Rules of Evidence,20,21 this evidence is often used in an exculpatory manner.
Guidelines have been established and are continually reviewed and revised to provide the forensic odontologist with evidence gathering and analytical procedures to be followed to ensure that recovered bite mark evidence is admissible in court and supports corroborative evidence in the case.22
Comparative Dental Anatomy
To understand the human dentition, it is helpful to compare the dentitions of other vertebrates. In doing so, it should become clear that the dentition in humans is different in many ways from that of other vertebrates in form and function. However, it should be equally clear that the presence of related characteristics in a wide range of vertebrates suggests a plan common to all.
Only a brief summary of the topic is presented here, starting with a simple form of tooth, the single cone or lobe, and then combinations of lobes forming more complicated teeth that are found in highly developed animals and in humans. Additional material on the subject may be found in the references and bibliography presented at the end of this chapter.
Figure 4-2 graphically illustrates a theory of the following four phylogenetic classes of tooth forms23-25:
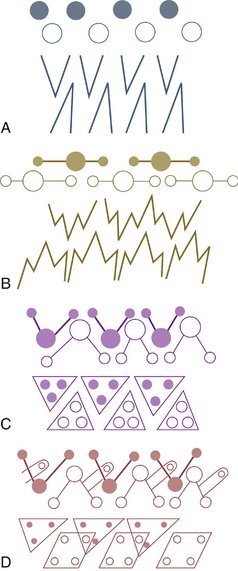
Figure 4-2 Classification of cusp forms. A, Haplodont. B, Triconodont. C, Tritubercular molar. D, Quadritubercular molar. The solid black dots represent upper molar cusps. The circles represent lower molar cusps.
(From Thompson AH: Comparative dental anatomy, ed 2, revised by M Dewey, St Louis, 1915, Mosby.)
The haplodont class is represented schematically by the simplest form of tooth, the single cone (Figure 4-2, A). This type of dentition usually includes many teeth in both jaws and is seen where jaw movements are limited to simple open and close (hinge) movements (Figure 4-3). No occlusion of the teeth occurs in this class, since the teeth are used mainly for prehension or combat.26,27 Their main function is the procurement of food. Jaw movements are related to and governed by tooth form in all cases.

Figure 4-3 The Mississippi alligator. An interesting commentary on the anatomy of the alligator: because of the alligator’s physical problems, the upper jaw is the mobile one. The lower jaw, closer to the ground, is static.
(From Kronfeld R: Dental histology and comparative dental anatomy, Philadelphia, 1937, Lea & Febiger.)
The triconodont class exhibits three cusps in line in posterior teeth as indicated in Figure 4-2, B. Anthropologically, the largest cusp is centered with a smaller cusp located anteriorly and another posteriorly. Purely triconodont dentitions are not seen, although certain breeds of dogs28 and other carnivores have teeth reflecting the triconodont form (Figure 4-4). Nevertheless, dogs and other animals carnivorous by nature are considered to be in the third category (Figures 4-5 through 4-8), namely, the tritubercular class.29,30 The three-cusp arrangement of the triconodont class and the more efficient three-cornered tritubercular molar arrangement are both consistent with the teeth’s bypassing each other more or less when the jaw is opened or closed. However, the quadritubercular class reflects an occlusal contact relationship between the teeth of the upper and lower jaws. Articulation of the jaws and teeth is consistent with jaw movements and functions of these classes of teeth.

Figure 4-4 Permanent dentition of Canis familiaris.
(Modified from Tims HWM: Notes on the dentition of the dog, Anat Anz Bd 11:537, 1896.)
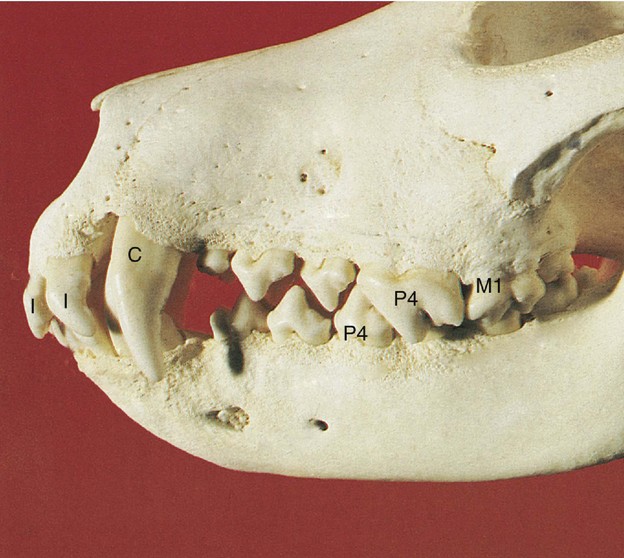
Figure 4-5 Jaws of a dog (collie). The premolars are tritubercular and widely spaced; the upper carnassial (fourth premolar, P4) articulates with the lower carnassial (first molar, M1). I, Incisor; C, canine.
(From Boyd J: Color atlas of clinical anatomy of the dog and cat, ed 2, St Louis, 2001, Mosby.)
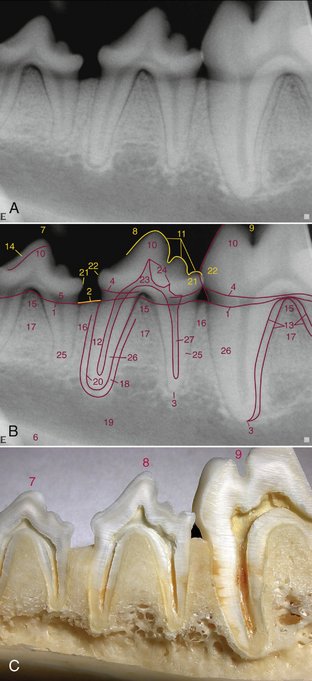
Figure 4-6 Normal radiographic anatomy of a dog (unspecified). A, Radiograph of a left mandibular fourth premolar tooth along with partial images of the third premolar (on left) and the first molar (on right). B, Anatomical features outlined for identification. C, A sectioned specimen showing internal anatomy.
(From DuPont GA, DeBowes LJ: Atlas of dental radiography in dogs and cats, St Louis, 2009, Saunders.)
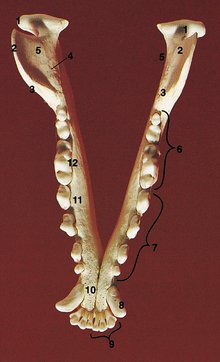
Figure 4-7 Occlusal view of the mandible of a dog (collie). The mandible is long and slender. The cutting edges of the four premolars (7) and three molars (6) are arranged in a sagittal plane. 9, Incisor; 8, canine.
(From Boyd J: Color atlas of clinical anatomy of the dog and cat, ed 2, St Louis, 2001, Mosby.)
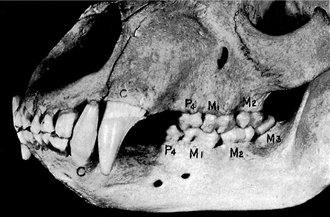
Figure 4-8 The bear. The extent of development of teeth and jaws and occlusion is often used to rate animal form. Compare with Figure 4-9. C, Canine; P, premolar; M, molar.
(From Kronfeld R: Dental histology and comparative dental anatomy, Philadelphia, 1937, Lea & Febiger.)
Animals that have dentitions similar to that of humans are anthropoid apes. This group of animals includes the chimpanzee, gibbon, gorilla, and orangutan (Figures 4-9 and 4-10). The shapes of individual teeth in these animals are amazingly close to their counterparts in the human mouth. Nevertheless, the development of the canines, the arch form, and the jaw development are quite different.
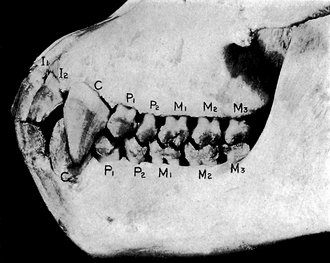
Figure 4-9 The ape. I, Incisor; C, canine; P, premolar; M, molar.
(From Kronfeld R: Dental histology and comparative dental anatomy, Philadelphia, 1937, Lea & Febiger.)
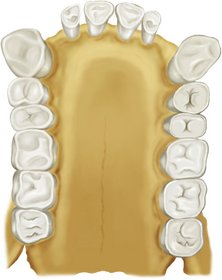
Figure 4-10 Occlusal view of the upper jaw of an orangutan. The arch is square, and the canines, premolars, and molars stand in a straight sagittal line. Note the diastema between lateral incisor and canine.
(From Kronfeld R: Dental histology and comparative dental anatomy, Philadelphia, 1937, Lea & Febiger.)
The multiplication and fusion of lobes during tooth development are demonstrated graphically when human teeth are viewed from the mesial or distal aspects. Anterior teeth, which are used for incising or apprehending food, reflect the single cone, whereas the posterior or multicusped teeth, which are used for grinding food in addition to having a shearing action, appear to be two or more cones fused (Figure 4-11). Although the schematic form of the teeth from the mesial or distal aspects is that of a single cone in anterior teeth, or what seems to be an indication of a fusion of two or more cones in posterior teeth, close observation causes one to come to the conclusion that each tooth crown, regardless of location, appears to be a combination of four or more lobes. Each lobe represents a primary center of formation.
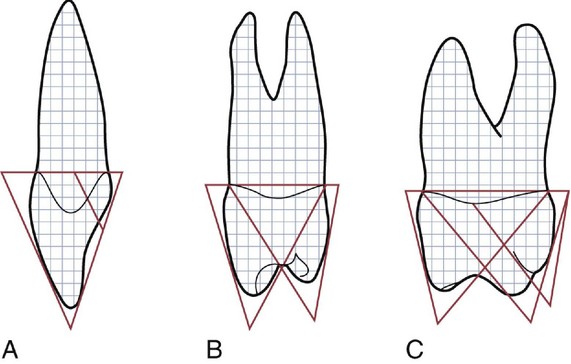
Figure 4-11 The functional form of the teeth when outlined schematically from the mesial or distal aspects is that of the fusion of two or three cones. A, Maxillary incisor. B, Maxillary premolar. C, Maxillary first molar. Note that the major portion of the incisor in view is made up of one cone or lobe.
All anterior teeth show traces of four lobes, three labially and one lingually, the lingual lobe being represented by the cingulum. Each labial lobe of the incisor terminates incisally in rounded eminences known as mamelons. These mamelons are prominent in newly erupted incisors. Soon after eruption they are worn down by use unless, through misalignment, they escape incisal wear. Maxillary central incisors often show traces of the fusion of three lobes on the labial face by visible markings in the enamel called labial grooves (Figures 4-12, A; 4-13; and 4-14).
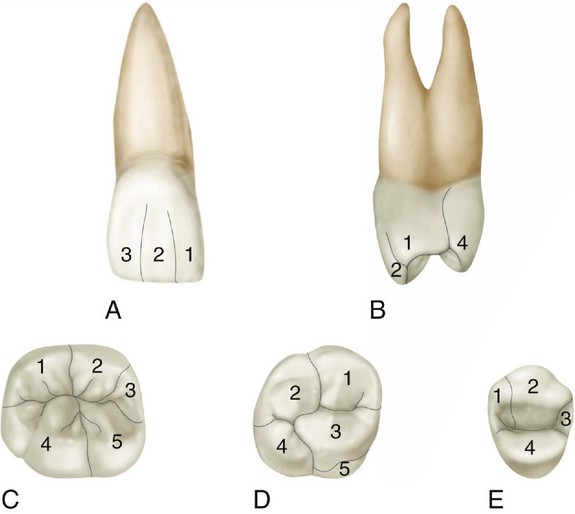
Figure 4-12 General outlines of some of the lobes. A, Labial aspect of maxillary central incisor, showing the labial grooves marking the division of the lobes. 1, Mesial lobe; 2, labial lobe; 3, distal lobe. The lingual lobe, or cingulum, is not in view (see Figure 4-13, A, 4). B and E, Mesial and occlusal aspects of maxillary first premolar. 1, Mesial lobe; 2, buccal lobe; 3, distal lobe; 4, lingual lobe. C, Occlusal aspect of mandibular first molar. 1, Mesiobuccal lobe; 2, distobuccal lobe; 3, distal lobe; 4, mesiolingual lobe; 5, distolingual lobe. Lobes on molars are named the same as cusps. D, Occlusal aspects of maxillary first molar. 1, Mesiobuccal lobe; 2, distobuccal lobe; 3, mesiolingual lobe; 4, distolingual lobe; 5, fifth lobe (fifth cusp).
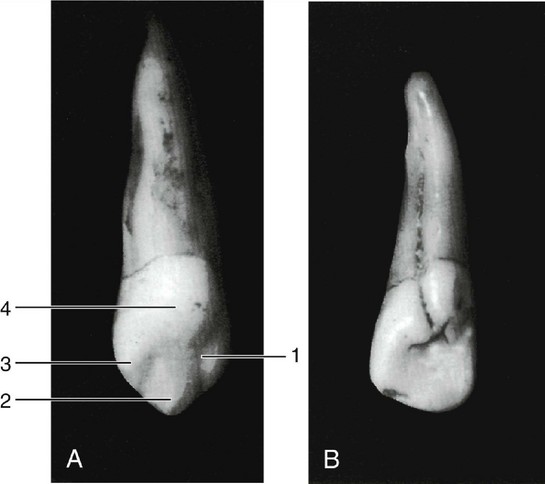
Figure 4-13 A, Lingual aspect of maxillary canine, with primary centers marked. 1, Mesial lobe; 2, central lobe (cusp); 3, distal lobe; 4, lingual lobe (cingulum). B, Incomplete formation demonstrated by a developmental groove distolingually on a maxillary lateral incisor. This groove will sometimes harbor fissures at various points along its length, especially in the coronal portion. A tooth with this handicap is more subject to caries.
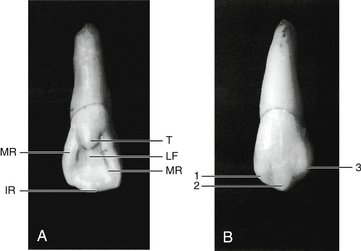
Figure 4-14 A, Maxillary lateral incisor, which shows prominences at the centers of calcification. T, Tubercle, prominence equal to a small cusp at the cingulum; LF, lingual fossa; MR, marginal ridges; IR, incisal ridge with a prominent enamel rise. B, Maxillary canine showing evidence of lobe formation. 1, Mesial lobe; 2, labial lobe; 3, distal lobe.
In the anterior teeth, the four lobes are called the mesial, labial, distal, and lingual lobes. In premolars they are called mesial, buccal, distal, and lingual lobes, or as in the case of the mandibular second premolar, which often has two lingual cusps, the mesial, buccal, distal, mesiolingual, and distolingual lobes, making five in all (see Figure 10-17).
The molar lobes are named the same as the cusps (e.g., mesiobuccal lobe). The tip of each cusp represents the primary center of formation of each lobe.*
It is possible, of course, to find a variation in the number of lobes in molars. Tubercles of enamel may be found in addition to the primary lobes. When present, they are usually smaller than and supplementary to the major lobes.
TOOTH FORM AND JAW MOVEMENTS
In general terms, the primates are bunodont and relatively isognathous and therefore have limited lateral jaw movement. Bunodont refers to tooth-bearing conical cusps. Isognathous means equally jawed; anisognathus means unequally jawed. Humans are not perfectly isognathous (i.e., the maxillary arch overlaps horizontally the mandibular arch). The shape of the glenoid (mandibular) fossae (see Figure 15-1) is correlated also with tooth form and jaw movements. A number of living and extinct species demonstrate a number of dental forms, from the bunodont to the selenodont (i.e., molars with crescent-shaped cusps) types. Each type is accompanied by an increased mobility of the mandible in a lateral direction and increased anisognathism. When the incisal point is viewed from the front during mastication, the mandible moves up and down without lateral deviation in dogs, cats, pigs, and all other animals with bunodont articulations. Lateral movement increases in a number of animals to the extreme lateral excursions seen in the giraffe, camel, and ox. In relation to the latter type of movement, it has been proposed that where the condyle is greatly elongated transversely and very flat, great lateral movement occurs during mastication, associated with selenodont molars, and a great degree of anisognathism. Also of interest for the gnathologist is the putative correlation between the directions of the ridges and grooves and a radius drawn to the center of the glenoid fossa.
It has been suggested that the simplest type of jaw movement is opening and closing without lateral excursion and coexistent with the simple bunodont molar. With increasing complexity of movement, an apparent increase in the complexity of enamel folding, ridges, and crests occurs, which might be consistent with the hypothesis of the mechanical genesis of tooth forms.31 Correlations between the forms of the teeth, joints, muscles, skull, bones, and jaw movement appear to be consistent with the functions of each species.
GEOMETRIES OF CROWN OUTLINES
In a general way, all aspects of each tooth crown except the incisal or occlusal aspects may be outlined schematically within one of three geometric figures: a triangle, trapezoid, or rhomboid. To one unfamiliar with dental anatomy, it may seem an exaggeration to say that curved outlines of tooth crowns can be included within geometric figures. Nevertheless, it seems very plausible to consider fundamental outlines schematically to assist in visualization (see Figures 4-15 and 4-16).
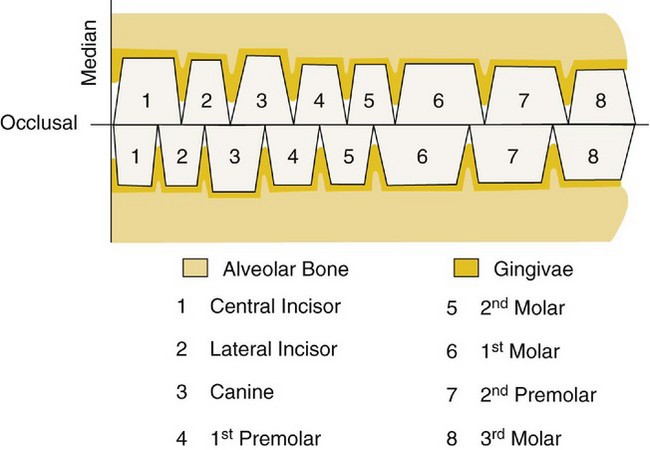
Figure 4-15 Schematic drawing of facial (labial and buccal) aspects of the teeth only, illustrating the teeth as trapezoids of various dimensions. Note the relations of each tooth to its opposing tooth or teeth in the opposite arch. Each tooth has two antagonists except number 1 below and number 8 above.
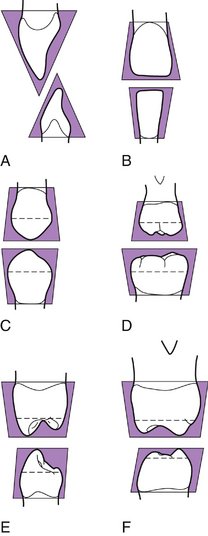
Figure 4-16 Outlines of crown forms within geometric outlines—triangles, trapezoids, and rhomboids. The upper figure in each square represents a maxillary tooth, the lower figure a mandibular tooth. Note that the trapezoidal outline does not include the cusp form of posteriors actually. It does include the crowns from cervix to contact point or cervix to marginal ridge, however. This schematic drawing is intended to emphasize certain fundamentals. A, Anterior teeth, mesial or distal (triangle). B, Anterior teeth, labial or lingual (trapezoid). C, Premolars, buccal or lingual (trapezoid). D, Molars, buccal or lingual (trapezoid). E, Premolars, mesial or distal (rhomboid). F, Molars, mesial or distal (rhomboid).
Facial and Lingual Aspects of All Teeth
The outlines of the facial and lingual aspects of all the teeth may be represented by trapezoids of various dimensions. The shortest of the uneven sides represent the bases of the crowns at the cervices, and the longest of the uneven sides represent the working surfaces, or the incisal and occlusal surfaces, the line made through the points of contact of neighboring teeth in the same arch (Figure 4-15). Disregarding the overlap of anterior teeth and the cusp forms of the cusped teeth in the schematic drawing, the fundamental plan governing the form and arrangement of the teeth from this aspect seems apparent.
The occlusal line that forms the longest uneven side of each of the trapezoids represents the approximate point at which the opposing teeth come together when the jaw is closed in the intercuspal position or centric occlusion. The viewer must not become confused at this point and think that all of each tooth actually makes contact at the occlusal level. The illustration is made to help in visualizing the fundamental shape of the teeth from the labial and buccal aspects (Figure 4-16).
This arrangement brings out the following fundamentals of form:
MESIAL AND DISTAL ASPECTS OF THE ANTERIOR TEETH
The mesial and distal aspects of the anterior teeth—central incisors, lateral incisors, and canines, maxillary and mandibular—may be included within triangles. The base of the triangle is represented by the cervical portion of the crown and the apex by the incisal ridge (see Figure 4-16, A).
MESIAL AND DISTAL ASPECTS OF THE MAXILLARY POSTERIOR TEETH
The outlines of the mesial and distal aspects of all maxillary posterior teeth (premolars and molars) can be included within trapezoidal figures. Naturally, the uneven sides of the premolar figures are shorter than those of the molars (see Figure 4-16, E and F). Notice that in this instance the trapezoidal figures show the longest uneven side representing the base of the crown instead of the occlusal line, as was the case in showing the same teeth from the buccal or lingual view. In other words, the schematic outline used to represent the buccal aspect of premolars or molars is turned upside down to represent the mesial or distal aspects of the same teeth. Figure 4-16 compares maxillary parts C and D with E and F.
The fundamental considerations to be observed when reviewing the mesial or distal aspects of maxillary posterior teeth are as follows:
It has been found necessary to emphasize the fundamental outlines of these aspects through the medium of schematic drawings, because the correct anatomy is overlooked so often. The tendency is to take for granted that the tooth crowns are narrowest at the cervix from all angles, which is not true. The measurement of the cervical portion of a posterior tooth is smaller than that of the occlusal portion when viewed from buccal or lingual aspects only; when it is observed from the mesial or distal aspects, the comparison is just the reverse; the occlusal surface tapers from the wide root base.
MESIAL AND DISTAL ASPECTS OF THE MANDIBULAR POSTERIOR TEETH
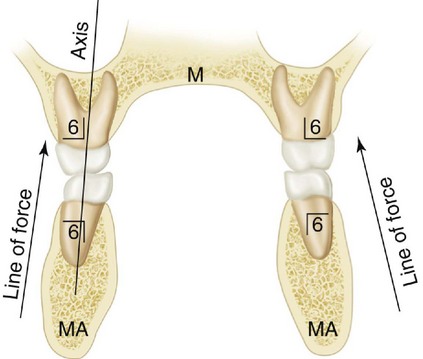
Finally, the mandibular posterior teeth, when approached from the mesial or distal aspects, are somewhat rhomboidal in outline (see Figure 4-16, E and F). The occlusal surfaces are constricted in comparison with the bases, which is similar to the maxillary posterior teeth. The rhomboidal outline inclines the crowns lingual to the root bases, which brings the cusps into proper occlusion with the cusps of their maxillary opponents. At the same time, the axes of crowns and roots of the teeth of both jaws are kept parallel (Figures 4-17 and 4-18). If the mandibular posterior crowns were to be set on their roots in the same relation of crown to root as that of the maxillary posterior teeth, the cusps would clash with one another. This would not allow the intercuspal relations necessary for proper function.
Summary of Schematic Outlines
Outlines of the tooth crowns, when viewed from the labial or buccal, lingual, mesial, and distal aspects, are described in a general way by triangles, trapezoids, or rhomboids (Figure 4-16, A through F).
Form and Function of the Permanent Dentition
The relationship between the form of the teeth and function is usually discussed in terms of type of food in the diet of humans, jaw movements, and protection of the periodontium and stimulation of the gingiva. It is also recognized that the teeth not only contribute to the digestion of food but also are important in speech and personal appearance.
The primary function of the teeth is to prepare food for swallowing and to facilitate digestion. The teeth have their respective forms to facilitate prehension, incision, and trituration of food. The dentition, joints, and muscles in humans have the form and alignment to enable the mastication of both animal and vegetable foods. This type of dentition is referred to as omnivorous.
The shapes of incisal and occlusal surfaces of the teeth are related not only to the function they perform but also to the movements of the mandible required to carry out chewing of a variety of foods. In contrast to the facts regarding many animals, only up-and-down jaw closure is possible because of the interlocking conical form of the teeth, temporomandibular joint (TMJ) morphology, and lack of muscles to carry out lateral movements. To understand more completely the form and function of teeth, the protective aspects of form and their functional relationships are considered.
Alignment, Contacts, and Occlusion
When the teeth in the mandibular arch come into contact with those in the maxillary arch in any functional relation, they are said to be in occlusion. The term occlusion is also used to designate the anatomical alignment of the teeth and their relationship to the rest of the masticatory system. Malocclusion is a term usually used to describe deviations in intramaxillary and/or intermaxillary relations of the teeth and/or jaws. Occlusion is considered in more detail in Chapter 16.
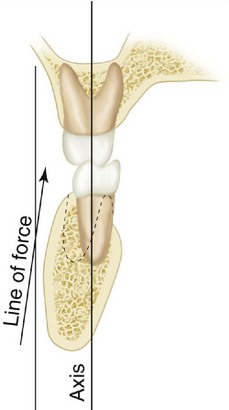
As demonstrated in Chapter 1, especially relative to Table 1-1, a very low probability exists of drawing at random one tooth of each class and type from a large sample of natural teeth with the expectation of being able to place them in proper alignment and articulation, as in Figure 1-16Figure 1-17Figure 1-18 in Chapter 1. This fact should indicate the complexity of the process of development and eruption of the teeth into a normal occlusion, which means minimally the proper alignment, and arrangement of the teeth within each jaw and the interdigitation of the teeth between the jaws.32 In addition, each tooth (including implants) in the arch should be placed in its most advantageous angle to withstand the forces brought to bear on it. The angles of the teeth are considered in Chapter 16 (see Figure 16-20). A general restorative principle states that occlusal forces in dental restorations should be directed along the long axis of the teeth (see Figure 4-17). Although this concept seems appropriate, it is not evidence based (i.e., no randomized clinical trial results support the concept). Unfortunately, at this time, no acceptable method of testing the hypothesis is available (i.e., no dynamic clinical biomechanical method, including telemetry, has determined the vector forces generated between teeth during function). However, some evidence suggests that tangential loading (see Figure 4-18) results in reduced chewing forces and that negative feedback from receptors in the periodontium mediate chewing forces. Receptor thresholds for axially directed forces appear to be higher than those for tangentially directed forces and suggest a positive feedback control on axially directed tooth forces. To position dental implants correctly, an intraoral appliance is used to guide the placement of the implant into a position and angulation consistent with angulations of opposing teeth or those suggested in Box 16-1 and Figure 16-20.
The buccal and lingual contours of the teeth have an influence on the way in which food is directed to and away from the gingival tissues. When a tooth is normally positioned, the gingival margin and sulcus have a physiological relationship to the tooth in function. Food impaction, impinging trauma from tough foods, and accumulation of dental plaque may be the consequence of malposed teeth or overcontouring or undercontouring of restorations involving buccolingual surfaces. The exact relationship between the contouring of restorations and gingival health is not clear. Ideas concerning the relationship of faulty buccal contours (undercontouring) to the initiation of gingivitis have been challenged. Plaque control by toothbrushing may be more important than simple deviations of the contour. However, overcontoured and undercontoured restorations should be avoided. Overcontouring of facial and lingual surfaces may inhibit natural cleaning by the tongue, cheeks, and passage of food and may require special toothbrushing methods.
INTERPROXIMAL FORM
Proximal contacts of approximating teeth in the arch protect the soft tissues (gingiva) between the teeth and are referred to as the interproximal spaces (Figures 4-19 and 4-20; see also Figure 5-1). The gingiva, which normally fills this pyramidal-like space and extends from the alveolar bone to and around the proximal contacts of the teeth (see Figure 5-2, B) may not fill these spaces (Figure 4-21). In the absence of correct proximal tooth contacts and marginal ridges, food impaction may occur.
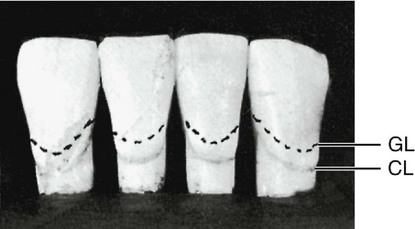
Figure 4-19 The mandibular centrals and laterals contact each other at the incisal third. The form of each tooth, plus the location of the contact areas, creates narrow pointed spaces between the teeth that differ from other interproximal spaces in other segments of the arches. GL, Variable gingival line representing the gingival level; CL, cervical line as established by the cementoenamel junction.

Figure 4-20 Contact design and interproximal (sometimes called interdental) spaces illustrated by the mandibular canine and first and second premolars. Note the variation in contact areas in relation to crown length.
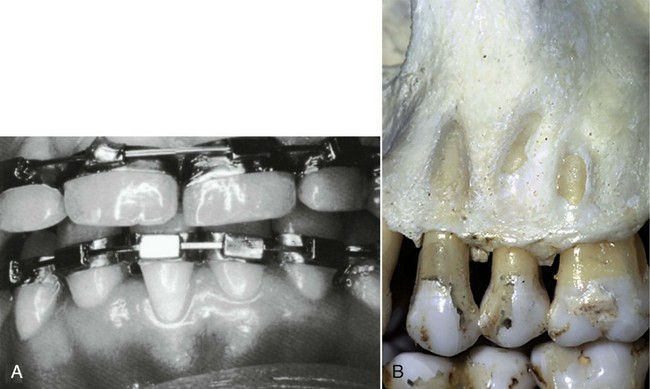
Figure 4-21 Influence of malalignment of teeth on form of gingival line and bone. A, Change in gingival line (free gingival margin) of central incisor. B, Absence of bone over root of tooth in labioversion (fenestration).
(B from Perry DA, Beemsterboer PL: Periodontology for the dental hygienist, ed 3, St Louis, 2007, Saunders.)
The gingiva within the interproximal space is called the gingival or interdental papilla (see Figure 5-1). Normally, the gingiva covers part of the cervical third of the tooth crowns and fills the interproximal spaces (see Figures 4-21 and 5-1). The gingival line follows the curvature but not necessarily the level of the cervical line. The cervical line is defined as the cementoenamel junction and has been considered in Chapter 2. The gingival line and the cervical line must not be thought of as being identical; although they normally follow a similar curvature, they are seldom at the same level on the tooth. The cervical line is a stable anatomical demarcation, whereas the gingival line merely represents the gingival level on the tooth at any one period in the individual’s life, and this level is variable (e.g., gingival recession). Misalignment of the teeth may change the gingival line, which may not be conducive to the health of the tissue (e.g., partial absence of bone over the root of a tooth as in dehiscence [cleft] or fenestration [window]) (see Figure 4-21, B).
Even when the teeth are in good alignment, unless the proper relation is kept between the width of each tooth at the cervix and the width at the point of contact with neighboring teeth, the spacing interdentally is changed. This is an important point to observe in clinical examinations and to maintain in approximating restorations (e.g., do not reduce the interproximal space at the expense of the interdental gingival papilla).
When considering the form of the teeth from the mesial and distal aspects, it is possible to observe a curvature on the crowns at the cervical third above the cervical line, labially or buccally and lingually. It is called the cervicoenamel ridge (see Figure 1-19), or simply cervical ridge, with the location added (buccocervical ridge, and so forth). As already indicated, this ridge should not be overcontoured or undercontoured in full-crown restorations.
ROOT FORM
The length and shape of the root (or roots) of each tooth must be viewed as important; the canine, for instance, because of its position and the work required of it, would be torn out of its socket or at least displaced by forces brought to bear on it if the root were not of extra size and length. Fracture would be imminent if the root were not larger than that of other single-rooted teeth. The root form therefore is associated with the overall form of the tooth and the work it has to do.
The angle at which the incisal and occlusal surfaces of the tooth crowns are placed with respect to the root bases is also important. The mesial view of an anterior tooth will show that the incisal ridge or cusp is centered over the root (see Figure 1-4). The mesial view of an upper first molar, which is a multicusped tooth, demonstrates the same principle. The points on the occlusal surface that are contacted by opposing teeth will prove to be well within the confines of the root base of the crown. The measurement from cusp tip to cusp tip buccolingually is much less than the buccolingual diameter of the root base (see Figure 1-4). Note the flare of the roots for stabilization.
The length and shape of the roots, the angles at which the incisal and occlusal surfaces are placed with respect to the roots, sufficient dimensions for strength, and an efficient design for thorough work with resistance against lines of force suggest their importance to occlusal stability.
OCCLUSAL CURVATURE
When occlusion is considered, the concept of what constitutes normalcy arises. Although this is considered conceptually in Chapter 16, it is appropriate to give a brief definition here. Normal implies a situation that is found commonly in the absence of disease or disorders and that exhibits an associated range of values that reflects the adaptive physiological range of a dynamic biological system, including the masticatory system.31 Therefore one must be careful not to attach rigid biomechanical significance to observations that are not yet evidence based (i.e., verified by appropriately designed clinical trials). It is also important not to reject clinical procedures based on statistically significant differences when the biological significance of the difference cannot be determined.
It can be observed that the occlusal and incisal surfaces of all the crowns taken together in either arch do not contact a flat plane. For example, when the teeth are viewed from a point opposite the first molars buccally, a line following the occlusal and incisal surfaces describes a curve. Graf von Spee described this curvature of natural teeth originally in the German literature in 1890, and for that reason, it is called the curve of Spee (Figure 4-22). No acceptable scientific evidence exists that the occlusion should be spherical (i.e., that each cusp and incisal edge touch or conform to a segment of the surface of a sphere). This kind of curvature suggested by the lingual inclination of the mandibular molars is the basis for the curve of Wilson (i.e., the curvature of the mandibular teeth is concave and that of the maxillary teeth convex). A template for these curvatures cannot be used to set teeth in complete dentures or to perform full-mouth oral rehabilitation. The degree of anterior-posterior curvature is related to the amount of anterior guidance that is needed to obtain posterior disclusion of the teeth in lateral and protrusive mandibular movements.

1. Herschaft EE. Forensic dentistry. In Neville BW, et al, editors: Oral and maxillofacial pathology, ed 2, Philadelphia: Saunders, 2002.
2. Herschaft EE, et al, editors. Manual of forensic odontology, ed 4, Albany, NY: American Society of Forensic Odontology, 2007.
3. Bowers CM. Forensic dental evidence: an investigator’s handbook. San Diego: Elsevier; 2004.
4. Lampe H, Roetzcher K. Age determination from the human skeleton. Med Law. 1994;13:623.
5. Reich KJ, Demirjian A. A multimedia tool for the assessment of age remains: the electronic encyclopedia for maxillo-facial, dental and skeletal development. In Reichs KJ, editor: Forensic odontology, ed 2, Springfield, IL: Charles C Thomas, 1998.
6. Kasper K, Senn D: Reliability of third molar development on a north Texas Hispanic population: a comparison study for age estimation, Proceedings of the American Academy of Forensic Sciences, vol 10, Colorado Springs, CO, February 2004, American Academy of Forensic Sciences (abstract F19).
7. Loevy HT. Maturation of permanent teeth in black and Latino children. Acta Odontol Pediatr. 1983;4:59.
8. Willems G. A review of the most commonly used dental age estimation techniques. J Forensic Odontostomatol. 2001;19:9.
9. Pretty IA. The use of dental aging techniques in forensic odontological practice. J Forensic Sci. 2003;48:1127.
10. Moorrees CF, Fanning EA, Hunt EE. Age variation of formation stages for ten permanent teeth. J Dent Res. 1963;42:1490.
11. Mincer HH, Harris EF, Berryman HE. The ABFO study of third molar development and its use as an estimator of chronological age. J Forensic Sci. 1993;38:379.
12. Kvaal SI, Sellevold BJ, Solheim T. A comparison of different non-destructive methods of age estimation in skeletal material. Int J Osteoarchaeol. 1994;4:36.
13. Gustofson G. Age determination on teeth. J Am Dent Assoc. 1950;41:45-54.
14. Ohtani S, Abe I, Yamamoto T. An application of D- and L-aspartic acid mixtures as standard specimens for the chronological age estimation. J Forensic Sci. 2005;50:1298.
15. Wagner GN. Scientific methods of investigation. In: Stimson PG, Mertz CA, editors. Forensic dentistry. Boca Raton, FL: CRC Press, 1997.
16. Sweet DJ. Bitemarks as biological evidence. In: Dorion RBJ, editor. Bitemark evidence. New York: Marcel Dekker, 2005.
17. Sweet DJ, Sweet CH. DNA analysis of dental pulp to link incinerated remains of homicide victim to crime scene. J Forensic Sci. 1995;40(2):310-314.
18. Sweet DJ, Hildebrand CH. Recovery of DNA from human teeth by cryogenic grinding. J Forensic Sci. 1998;43:1199.
19. Sweet DJ. Why a dentist for identification? Dent Clin North Am. 2001;45:241.
20. Frye v United States, 293 F 10 13 (DC Cir 1923).
21. Daubert v Merrell Dow Pharmaceuticals, 509 US 579, 113 S Ct 2786, 125 LEd2d 469 (1993).
22. American Board of Forensic Odontology: guidelines for bite mark analysis. J Am Dent Assoc. 1986;112:383.
23. Osborn HF. Evolution of mammalian molar teeth. In: Gregory WK, editor. Biological studies and addresses. New York: Macmillan, 1907.
24. Gregory WK. The origin and evolution of human dentition. Baltimore: Williams & Wilkins; 1906.
25. Thompson AH. Comparative dental anatomy. revised by Martin Dewey., ed 2. 1915. Mosby, St Louis.
26. Kronfeld RL. Dental histology and comparative dental anatomy. Philadelphia: Lea & Febiger; 1937.
27. Ferguson MW. Review of the value of the American alligator (Alligator mississippensis) as a model for research in craniofacial development. J Craniofac Genet Dev Biol. 1982;1:123.
28. Tims HWM. Notes on the dentition of the dog. Anat Anz Bd. 1896;11:537.
29. Cope EE. On the tritubercular molar in human dentition. J Morphol. 1888;2:7.
30. Wortman JL. Origin of the tritubercular molar. Am J Sci. 1902;13:93.
31. Ryder JA. On the mechanical genesis of tooth-forms. Proc Acad Nat Sci Philadelphia. 1878.
32. Ash MM, Ramjford SP. Occlusion, ed 4. Philadelphia: Saunders; 1995.
Ash MM. Physiology of the mouth. In Bunting RW, editor: Oral hygiene, ed 3, Philadelphia: Lea & Febiger, 1954.
Barker BC. Dental anthropology: some variations and anomalies on human tooth form. Aust Dent J. 1973;18:132.
Cooke WP. Value and use of temporary teeth. Br J Dent Sci. 1923;66:267.
Farer JW, Isaacson D. Biologic contours. J Prev Dent. 1974;1:4.
Fixott RH. Forensic odontology. Dent Clin North Am. 2001;45(2, theme issue):217.
Gale GL. Dentistry, bite marks, and investigation of crime. J Cal Dent Assoc. 1996;24:28.
Graf H. Occlusal forces during function. In: Graf H, editor. Occlusion: research in form and function (symposium report). Ann Arbor: University of Michigan, 1975.
Hellman M. The relationship of form to position in teeth and its bearing on occlusion. Dent Items Interest. 1920;42:161.
Humphreys HF. Function in the evolution of man’s dentition. Br Dent J. 1921;42:939.
Lindhe J, Wicen PO. The effects on the gingiva of chewing fibrous foods. J Periodont Res. 1969;4:193.
Perel ML. Periodontal considerations of crown contours. J Prosthet Dent. 1971;26:627.
Ramfjord SP, Ash MM. Periodontology and periodontics. Philadelphia: Saunders; 1979.
Russell ES. Form and function. New York: Dutton; 1917.
Shaw DM. Form and function of teeth: a theory of maximum shear. J Anat Physiol. 1917;13:97.
Wheeler RC. Complete crown form and the periodontium. J Prosthet Dent. 1961;11:722.
Youdelis RA, Weaver JD, Sapkos S. Facial and lingual contours of artificial complete crown restorations and their effect on the periodontium. J Prosthet Dent. 1973;19:61.
 site for additional study resources.
site for additional study resources.